 Dorottya Árva
Dorottya Árva Zoltán Vokó
Zoltán Vokó Mária Sápi
Mária Sápi Zsuzsa Cselkó
Zsuzsa Cselkó Zsuzsa Rákosy
Zsuzsa Rákosy
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 09 January 2024
Sec. Educational Psychology
Volume 8 - 2023 | https://doi.org/10.3389/feduc.2023.1240909
Background: In Hungary, as in other European countries, substance and behavioral addictions are an increasing problem among children and adolescents. Schools play a vital role in providing the knowledge and skills needed to prevent addictions. However, various factors influence the overall effectiveness of such efforts. To design more effective preventive interventions, it is necessary to evaluate existing programs and identify possible points to intervene. Our aim was to assess the current state of addiction prevention in Hungarian schools, identify barriers, and explore facilitators that contribute to the successful implementation of addiction prevention.
Methods: A nationwide cross-sectional survey-based quantitative study was performed to investigate the implementation of addiction prevention in Hungarian elementary schools (N = 2,892). With the participation of 37 teachers from 21 elementary schools, a focus group-based qualitative study was conducted to investigate teachers’ perspectives on such programs and ways to improve them.
Results: Among the addiction topics, alcohol (61.9%), smoking (73.6%), and drug use (71.3%) were the most covered themes. Problematic use of the internet and electronic devices was addressed in 60.9% of the schools, while gaming and gambling were addressed in only 18.9%. Of schools, 55.1% reported having regular programs to support pupils’ mental health, and this differed significantly by school type and size. Logistic regression analysis revealed that the type of school, the support for teachers’ work, and the diversity of implementers were significantly associated with the quality of implementation of addiction prevention. The qualitative study showed that addiction prevention is hindered by inappropriate family or teacher models, increased workloads, and challenges in collaborating with colleagues and parents. According to the teachers, they can do the most for the health of children at school, but they need support for effective implementation.
Conclusion: Our results indicate the importance of school characteristics in addiction prevention implementation and call for the support and empowerment of teachers and greater organizational capacity to ensure the effectiveness of school-based addiction prevention activities. By understanding these barriers and facilitators, policymakers and educators can develop evidence-based strategies to improve the effectiveness of prevention programs.
Substance use such as smoking, drinking alcohol and cannabis use often begin during adolescence (Inchley et al., 2020; Brener et al., 2022) and can be associated with acute and/or long-term health problems (Lee and Henry, 2022) and with premature mortality (MacArthur et al., 2016; Turhan et al., 2017). It can have detrimental effects on school performance, contribute to aggressive behavior, increase the likelihood of engaging in risky sexual behavior and contribute to the development of mental health disorders, including depression, anxiety or psychosis and self-harm (Silins et al., 2014; Marconi et al., 2016; Esmaeelzadeh et al., 2018; Bozzini et al., 2021; Wiese et al., 2023). In the United States, the latest Adolescent Behaviors and Experiences Survey from 2021 (Brener et al., 2022) revealed concerning trends: one in three 9–12th graders used some form of substance, such as alcohol, tobacco (e.g., cigarette, cigar, smokeless tobacco or electronic vapor product) or cannabis, or misused opioid prescription drugs. The one-month prevalence of alcohol consumption was recorded most commonly (20%), followed by tobacco use of any type (16%). The use of electronic vapor products (15%) accounted mainly for the latter. Students reported using cannabis (13%) and prescription opioid misuse (4%) less frequently. Similar rates have been recorded in the Monitoring the Future project for 2022 (Monitoring the Future, 2022). A parallel pattern is evident in Europe and Canada, as indicated by the latest findings of the Health Behaviour in School-aged Children (HBSC) study from 2018 (Inchley et al., 2020): 37% of children aged 15 drank alcohol, while 15% smoked cigarettes and 7% used cannabis in 30 days prior the survey. Moreover, 14% of 15-to 16-year-olds in Europe reported using e-cigarette (ESPAD Group, 2020).
Other behaviors with addictive potential, such as internet, smartphone, and social media use; online communication; playing digital games and gambling, also begin or become widespread during adolescence (Derevensky et al., 2019; ESPAD Group, 2020; Inchley et al., 2020). These behavioral addictions are also associated with various health harms and mental health problems (van den Eijnden et al., 2018; Derevensky et al., 2019; Sohn et al., 2019; Dahl and Bergmark, 2020; Emond and Griffiths, 2020; Vannucci et al., 2020; Kelly and Leung, 2021). Problematic use of technology and games that bear the risk of addiction was also detectable in this age group, although fortunately in lower proportions. Generally, fewer than one in ten teenagers was reported to be affected in Europe [1.5%–8.2% for problematic internet use (Weinstein and Lejoyeux, 2010; De-Sola Gutiérrez et al., 2016), 7% for social media use (Inchley et al., 2020), 1.4% for problem gambling (ESPAD Group, 2020), and approximately 2% for gaming problems (Paulus et al., 2018)], and rates of similar magnitude were detected in the US (Gentile, 2009; Liu et al., 2011), although estimates can show significant differences depending on the measures used. Notably, however, rates of both internet-based activities and problematic use increased during the COVID-19 pandemic (Kovačić Petrović et al., 2022).
Several factors represent risks for substance use and abuse and the development of the above-detailed behavioral addictions. Examples of individual risk factors are the presence of mental health issues [behavior or conduct problems, attention deficit and hyperactivity, depressive symptoms, anxiety and aggressive behavior (Weinstein and Lejoyeux, 2010; Koo and Kwon, 2014; Peeters et al., 2018; Derevensky et al., 2019; Bozzini et al., 2021; Busch and McCarthy, 2021; Kelly and Leung, 2021; Nawi et al., 2021; Wartberg et al., 2021; Lozano-Blasco et al., 2022)], specific personality traits [impulsivity and novelty-seeking (Koo and Kwon, 2014; Kelly and Leung, 2021; Nawi et al., 2021)] or poorer social and personal skills [e.g., social competence, problem-solving, decision-making, self-control, impulse control, emotion regulation and self-esteem (Griffin et al., 2001; Lochman and Wells, 2002; Lam, 2014; De-Sola Gutiérrez et al., 2016; Paulus et al., 2018; Peeters et al., 2018; Nawi et al., 2021; Wartberg et al., 2021)]. There exist family-related risks such as the experience of maltreatment, attachment problems, substance use in the family, absence of a parent and low parental education or control (Weinstein and Lejoyeux, 2010; Paulus et al., 2018; Derevensky et al., 2019; Bozzini et al., 2021; Nawi et al., 2021; Lozano-Blasco et al., 2022). School and social environment of children also play an important role: low school connectedness, poor academic performance (Derevensky et al., 2019; Bozzini et al., 2021; Nawi et al., 2021; Lozano-Blasco et al., 2022) along with high perceived drug accessibility and substance use among friends and peers (Bozzini et al., 2021; Nawi et al., 2021) also represent a higher risk.
On the other hand, there are factors that protect against substance use and addiction. On the individual level these include enhanced psychosocial competencies such as assertiveness (Evren et al., 2014; Lozano-Blasco et al., 2022), effective coping (Koo and Kwon, 2014; Das et al., 2016; Throuvala et al., 2019), and resilience (Zeleeva and Petrova, 2016; Robertson et al., 2018; Derevensky et al., 2019). Family cohesion and secure attachment can also decrease the risk of addictions (Derevensky et al., 2019; Bozzini et al., 2021). In relation to the school and social context, the protective factors are academic motivation, successful adjustment to school, school engagement and positive school climate (Koo and Kwon, 2014; Das et al., 2016; Dunne et al., 2017; Derevensky et al., 2019; Bozzini et al., 2021; Lozano-Blasco et al., 2022) along with anti-substance policy (Bozzini et al., 2021).
Schools play a pivotal role in curbing addictive behaviors. The implementation of prevention programs within the school environment can serve to bolster individual protective factors while mitigating the influence of risk factors associated with school and family. Furthermore, this contributes to the reduction of health disparities (Pulimeno et al., 2020; Herke et al., 2022). Both the European Union (EU) and the United States have adopted a comprehensive strategy for health promotion in schools to address substance and behavioral addictions (European Monitoring Centre for Drugs and Drug Addiction, 2019; Centers for Disease Control and Prevention, n.d.). These strategies typically encompass a multifaceted combination of health education, counseling and support services, prevention campaigns, awareness initiatives, and regulations. Universal school-based interventions designed for addiction prevention, targeting all students irrespective of their risk profiles, have shown promise in averting addictive behaviors. Effective interventions focus on enriching knowledge and fostering protective factors, such as students’ psychosocial skills and mental well-being (Das et al., 2016; Throuvala et al., 2019; Pulimeno et al., 2020). Creating a positive school atmosphere and establishing safe school areas have proven to be effective intervention points as well (Das et al., 2016; Spanemberg et al., 2020). These forms of school-based interventions align with the United Nations International Standards on Drug Use Prevention (United Nations Office on Drugs and Crime and the World Health Organization, 2018) and have been particularly beneficial for elementary school students (Griffin and Botvin, 2010; Onrust et al., 2016).
Nonetheless, the implementation of the aforementioned interventions can be influenced by various school characteristics including teacher competencies, school and class size, institutional resources, and organizational structures (Herke et al., 2022). Drawing from Domitrovich’s Multi-Level Model, it becomes evident that these contextual factors play a significant role in influencing the implementation quality of school-based interventions (Domitrovich et al., 2008). This model proposes that the quality of implementation depends not only on the characteristics of the intervention itself, but also on its support system [including, for example, the training of implementers (Domitrovich et al., 2008)]. Implementation of interventions is further influenced by the macro-level factors (e.g., policy environment), school-level factors (e.g., the school size, organizational health, resources, and personnel expertise) and individual-level factors [e.g., attitudes to the intervention (Domitrovich et al., 2008)]. Although, the impact of school size and location on implementation is not yet clear; smaller schools may be more amenable to certain interventions, while others may demonstrate the opposite trend, or they may fare differently in rural or suburban communities compared to urban settings (Domitrovich et al., 2008; Bast et al., 2017). The literature lacks information regarding how universal addiction prevention is implemented in schools with various types of funding. Findings also demonstrate that religious education can beneficially affect adolescent mental health (Estrada et al., 2019), alcohol use and binge drinking (Isralowitz and Reznik, 2015). Additionally, insights from a British Cohort Study underscored the pivotal role of education type or status within the socioeconomic context (Bann et al., 2016). Attending private schools was linked to long-term positive health outcomes and better health-related behaviors, such as lower smoking rates (Bann et al., 2016). The United Nations International Standards on Drug Use Prevention offer expert insights into factors that could ensure the effectiveness of universal school-based substance use prevention (United Nations Office on Drugs and Crime and the World Health Organization, 2018). Notably, regarding the school-level factors, the support system and the intervention (Domitrovich et al., 2008), it emphasizes the support of teachers through training in fostering social competencies via interactive classroom activities or engaging students in discussions about substance use risks. Collaborative efforts with mental health professionals and healthcare facilities are also highlighted as advantageous. To examine the importance of these institutional characteristics in the implementation of addiction prevention programs we applied national data from Hungary.
In Hungary, elementary schools are responsible for the first 8 years of the ten-year compulsory school education starting from age 6 [primary and lower secondary education in a single structure (Motiejūnaitė-Schulmeister et al., 2022; Scholaro Database, n.d.)]. The regulation of school health promotion [a macro-level factor in Domitrovich’s model (Domitrovich et al., 2008)] establishes that all children must be involved in Holistic Health Promotion (HHP) in schools (signifying both state, church and private schools) accounting for health promotion activities adapted to their biological, social and age-specific characteristics (Országgyűlés-Hungarian Parliament, 2003, 2011; Emberi Erőforrások Minisztériuma (EMMI) – Ministry of Human Capacities, 2012). These activities are aimed at promoting healthy diet, health promoting physical activity, improvement of health literacy and health competencies above the enhancement of mental health to prevent the development of behavioral addictions and substance use among others [e.g., early school leaving, violence (Emberi Erőforrások Minisztériuma (EMMI) – Ministry of Human Capacities, 2012)]. The elements of HHP are in accordance with the WHO health-promoting school approach (Bessems et al., 2020; World Health Organization and United Nations Educational Scientific and Cultural Organization, 2021). This regulation prescribes the evidence-based and recommended methods of universal addiction prevention that were listed above. However, the incorporation of these regulations into the Hungarian National Core Curriculum (NCC) (Magyar Kormány-Hungarian Government, 2020) is only partial, as health promotion is treated merely as an adjunct to physical education (Lipták and Tarkó, 2021). There are no selective nor indicated addiction programs in the current NCC, and it is unclear how universal school programs address the risk and the protective factors of addiction (Lipták and Tarkó, 2020). The number of school hours dedicated to health promotion is minimal, and the curricula do not include outcome requirements related to addictions. This is particularly significant considering that the rates of both individuals who had ever smoked (53%) and the one-month prevalence of cigarette smoking (28%) among 15- to 16-year-old Hungarian adolescents exceeded the European rates by 30%–40% in 2019 (ESPAD Group, 2020). The proportion of individuals who had ever tried alcohol was found to be one of the highest (over 90%) in Europe (ESPAD Group, 2020). Moreover, the proportion of Hungarian 15-year-olds who had been drunk at least twice was also among the highest compared to other European countries (Inchley et al., 2020). Developing skills and fostering positive attitudes toward healthy lifestyle choices from an early age is of utmost importance to address these unfavorable national epidemiological indicators. However, to successfully accomplish this goal, it is crucial to gain a comprehensive understanding of the addiction prevention currently being implemented in schools and the factors influencing its implementation.
Our aim was to examine the state of the art of health promotion programs targeting universal addiction prevention in Hungarian elementary schools, and to identify potential areas for improvement to inform stakeholders and policy development. Furthermore, we investigated how institutional characteristics of schools, including school-level factors and the quality of the intervention support system such as the funding, and size along with the diversity of program implementers and the support of teachers influence the quality implementation of addiction prevention programs in a nationwide quantitative study. We also explored teachers’ opinions and perspectives on possible ways to facilitate the implementation and to improve the effectiveness of school-based addiction prevention activities in Hungary through qualitative data. This niche study provides the first national data on the subject while offering lessons of international relevance.
This was a mixed-methods research project run from October 2019 to February 2020. The project consisted of a survey-based quantitative study providing data on the implementation of universal addiction prevention in Hungarian elementary schools [providing primary [International Standard Classification of Education (ISCED) 1: grades 1–4] and lower secondary education [ISCED 2: grades 5–8] in a single structure (Motiejūnaitė-Schulmeister et al., 2022; Scholaro Database, n.d.)] and a focus group-based qualitative study examining teachers’ views on such programs and on ways to improve them.
The survey-based study was part of an overarching evaluation of the implementation of HHP [prescribed by the Ministry of Human Capacities Decree of 2012 (Emberi Erőforrások Minisztériuma (EMMI) – Ministry of Human Capacities, 2012)] in Hungarian elementary schools. The Ministry of Human Capacities emailed an invitation to participate in the evaluation to the principals of all Hungarian elementary schools (N = 3,601). The email contained basic information on the study and the link to the online survey, which was open between 7 and 21 February 2020. All schools providing a complete answer to the survey during the data collection period were included in the study. Participation by schools was voluntary and anonymous, and respondents were asked to provide data on their institution only with no personal data included.
The original survey evaluating the implementation of the whole spectrum of HHP activities in schools consisted of 32 questions. According to the purpose of our research, we used data from 14 of these questions. The questions can be divided into three blocks according to their focus.
The first block of questions focused on the basic characteristics of schools, measuring three parameters. The type of school by funding was measured with a single-choice question (state/private/church). The school size was given by the number of pupils enrolled. Three categories were then created for the analyses: small: ≤ 150 children, medium: 151–450 children, and large: ≥ 451 children (Andl, 2020; Balogh, 2023). Finally, the regional location of the school was determined by using data from its county of operation. The official administrative regional structure was used except for merging Pest county and Budapest into one region called Central Hungary (Hungarian Central Statistical Office, 2023a).
The second block of questions focused on the institutional conditions and support for HHP implementation. A dichotomous question evaluated whether a school health promotion program was integrated into the school’s pedagogical program. It was followed by a multiple-choice question that listed the developers of the school health promotion program (teacher/school physician/school health-visitor/school psychologist/parents’ working group/pupil). For the analysis, answers were grouped into three categories: (1) only teacher was selected, (2) other developer(s) in addition to teacher(s) were selected, and (3) no developer from the list was selected.
The diversity of program implementers was measured with the number of different types of program implementers chosen in a multiple-choice question listing five potential partners involved in the implementation of the school health promotion program (school personnel/persons working for the school on a contract [e.g., school health-visitors and physicians]/parents with an educational background in medicine or health sciences/external expert speakers/organizations or associations providing programs approved by experts).
The ways in which the schools supported teachers in their health promotional activities were examined by 3 questions. One multiple-choice question targeted the available support for teachers through training opportunities. Several options were listed from which three groups relevant for the analysis were created: (1) available training only provided health-related information, (2) both training providing health-related information and programs to help build teachers’ resilience, coping strategies and mental well-being were available, and (3) any other answer. Another question examined the types of support for teachers’ work with pupils in need of help for mental health (individual counseling for pupils with a mental health professional/consultation about pupils with a mental health professional/both/none). Finally, a question examined the frequency of community-building and recreational events for teachers (more than once a year/once a year/never).
The third block of questions monitored the presence of effective school-based universal addiction prevention methods. The topics covered by the school health promotion program were evaluated with a multiple-choice question (smoking/alcohol/drug/internet gaming disorder and problem gambling/problematic use of internet and electronic devices/online and offline bullying), as well as the methods of building social competence (cooperative teaching method/interactive teaching method/assertive communication techniques). A 10-point Likert scale (from fully disagree to fully agree) measured whether regular programs supporting students’ mental health were provided in schools and whether pupils’ environment, such as the school atmosphere and facilities (e.g., classrooms, corridors, schoolyard) were friendly and safe. Answers to these three questions were then grouped into three categories: (1) disagree: 1–5 points, (2) moderately agree: 6–8 points, and (3) fully agree: 9–10 points.
Pearson’s chi-squared tests were used in univariate analyses to test the associations of the elementary school characteristics with the institutional conditions of HHP implementation, as well as the addiction prevention programs provided. In some cases, the associations between institutional conditions and the provided programs were also tested by Pearson’s chi-squared test and non-parametric trend test.
In addition, we used a multiple logistic regression model to investigate factors that predict schools’ performance in implementing universal addiction prevention. The participating schools were divided into two groups for this analysis based on the quality of their program implementation (good-, or low-quality). Schools with a school health promotion program included in the pedagogical program were considered good-quality performers if:
1. their program covered at least three of the above-listed topics related to addiction prevention, and
2. they used at least one of the above-listed methods of building social competence, and
3. fully agreed that the school provided regular programs supporting students’ mental health, and
4. fully agreed that the school atmosphere was friendly and safe, and
5. fully agreed that school facilities were friendly and safe, and
6. they provided at least one type of support for teachers who worked with pupils needing help for mental health.
The model investigated the relationship between basic characteristics (school type by funding, school size) and institutional conditions (support for teachers through training, number of types of program implementers) with implementation quality while correcting for the regional location. The likelihood ratio test (LR test) was used to determine whether the model fit better by representing the number of types of program implementers as a categorical or a continuous variable. The statistical analyses were performed with STATA/SE 16.1 software.
We aimed to explore the various views of Hungarian elementary school teachers involved or interested in addiction prevention. Therefore, we aimed to involve teachers from different regions of the country. Additionally, we assumed that the general socioeconomic conditions of the area where teachers’ workplaces were located may affect their perceptions on addiction prevention in schools as it is associated with substance use behaviors (OECD, 2021). Therefore, we recruited participants from a convenience sample of 21 schools located in two counties from two regions: in Borsod-Abaúj-Zemplén, one of the most deprived Hungarian counties (Nándori, 2021), and in Pest county, more specifically in its western part (Buda region), one of the wealthiest parts of the country (Kis and Goda, 2013). Principals, who were informed about the study by telephone and email, were asked to inform any interested colleagues about how they could take part. Eligibility criteria were as follows: teachers with valid employment contracts could be included, and employees in administrative services with no direct contact with students were excluded from the study. Given the available resources, we planned to conduct four focus group discussions.
A total of 37 teachers (15 from 10 schools of Borsod-Abaúj-Zemplén, 22 from 11 schools of Pest county; 8 primary school, and 29 lower secondary school teachers; 34 women, and 3 men) participated in this study.
Participation was voluntary and subject to written consent. The four discussions lasted between 75–120 min with 7 and 8 teachers in the groups from Borsod-Abaúj-Zemplén county, and 8 and 14 teachers from Pest county. Each focus group was held in person, outside the school grounds in a community space of the county (e.g., in a municipal community center). The discussions were led by a facilitator with the presence of an assistant (who intervened only if the guide was not followed). The facilitators were selected to have experience in focus group techniques and were provided with instructions about the focus group discussion guide prior to data collection. The Ethical Review Board of the National Korányi Institute of Pulmonology (Reg. No. 14/2019) granted approval for the study.
Questions of the focus group discussion guide were developed by two members of the research team. Questions were finalized through triangulation with other members of the team in order to ensure they were appropriate for the research aims and non-directive. In order to ensure comparability between focus groups, we have selected the most important questions (including the ones below) to be asked in each group. These questions focused on the factors influencing implementation and could provide guidance on how to support it. In this study, answers to the following questions were analyzed:
• What are your thoughts on improving addiction prevention and communicating the importance of related mental health promotion in your own work?
• What are the most significant barriers to these programs in your school?
• How can such a program be implemented in schools?
• What message could be used to persuade the teaching staff to support the program?
The discussions were audio-recorded and transcribed verbatim, and the Classic Analysis Strategy of Krueger and Casey (2015), with roots in grounded theory, was then applied to the transcripts. In this inductive approach, the constant comparative method is used to code responses to questions, then findings are structured around repeatedly emerging themes. For the analysis, we aimed to involve a person experienced in using this method, who was also familiar with the focus of the study, so we involved a member of the research team (also helping in the development of the guide) as an analyst. The first draft of the qualitative findings was presented to trainers to check that the emphases were in the right places and that irony and emotion had been captured correctly by the analyst working only from the transcripts. The refined results were reviewed and finalized with the help of a newly involved member of the research team to improve coherence and clarity.
We involved two female facilitators from outside the research team. They had experience in interviewing, worked as a trainer, coach and facilitator with companies, and specialized in communication skill-building. The analyst was a member of the research team, a female doctor specialized in preventive medicine and public health, working in her specialty in a public hospital, with previous experience in processing focus group data with the applied method. Neither facilitators, nor the analyst had any interest regarding the results of the study.
To minimize the effect of the perspectives of facilitators and the analyst, we applied the following credibility strategies: during data collection the use of the guide, and the presence and notifications from the assistant helped trainers each to avoid directive questioning. Additionally, we have planned the design in such a way, so that the analyst does not meet the participating teachers. In this way, we aimed to avoid the generation of assumptions based on informal conversations, that can bias the interpretation of transcripts. For the review of the draft of the results, we asked another member of the research team with the least prior knowledge and preconceptions: who joined after the first draft of results was prepared and who was not involved in any similar fieldwork before.
Of the 3,601 elementary schools in Hungary, 2,892 completed the national survey. According to their size, 805 were small, 1,297 were medium, and 790 were large schools (small: ≤ 150 children, medium: 151–450 children, large: ≥ 451 children), and regarding their type by funding: 2,330 were state, 158 were private and 404 were church schools.
The school health promotion program was included in the pedagogical program in more than two-thirds (68.5%) of schools. Table 1 summarizes the remaining institutional conditions and support for the implementation of school health programs. The number and diversity of participants involved in the program development were significantly associated with the school size (p < 0.001). Two-thirds of the schools supported teachers with health-related information and skill development training. The type of training differed by school size (p = 0.004). The majority (74.2%) of institutions supported teachers by providing both individual counseling for pupils and consultations for teachers when a pupil was in need of help for mental health. The level of this support related significantly to both school type and school size (p = 0.002 and p < 0.001, respectively). Almost two-thirds (63.2%) of the schools organized community-building and recreational events for the teachers more than once a year (Table 1).
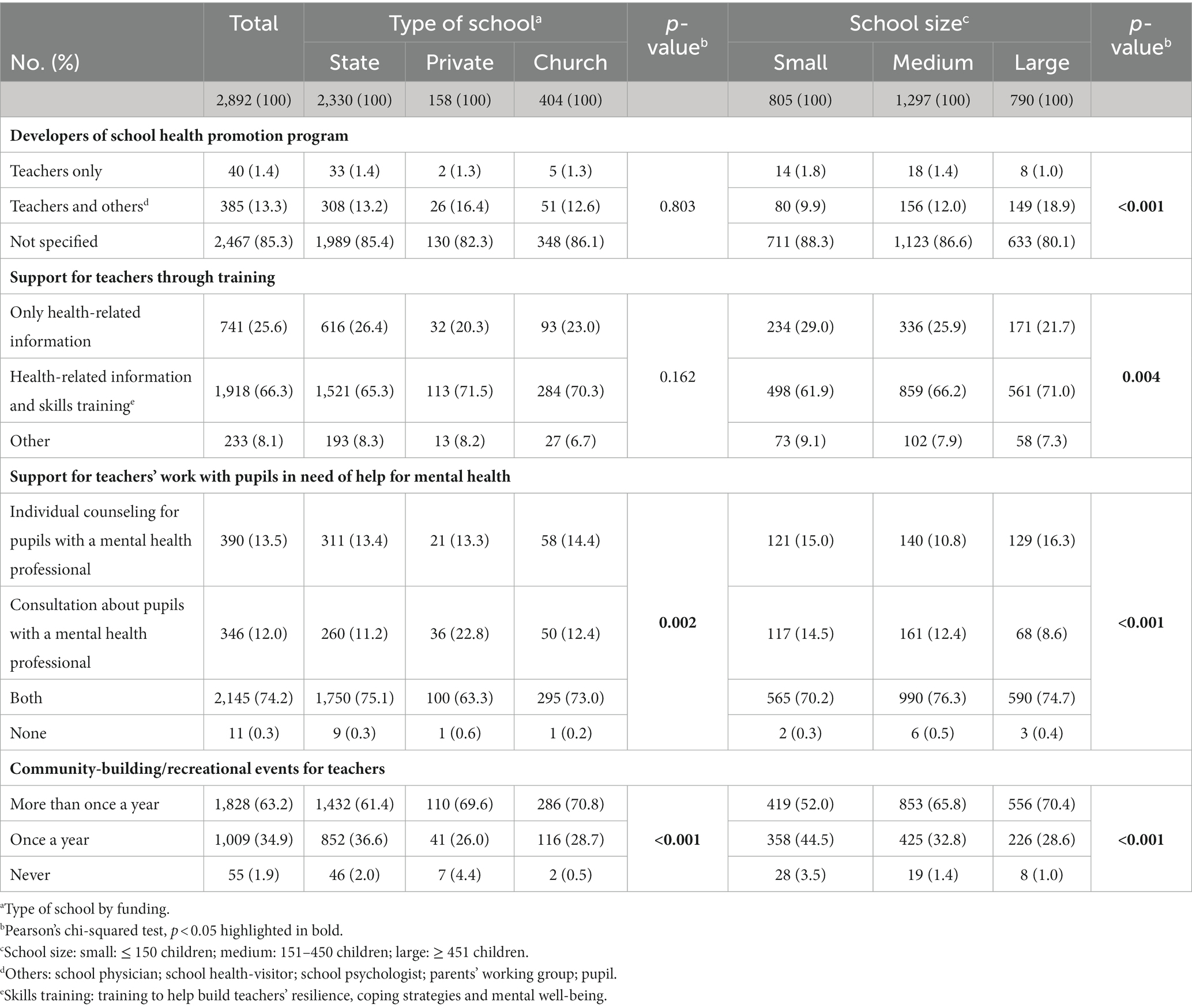
Table 1. Institutional conditions and support for the implementation of school health promotion programs in Hungarian elementary schools.
Table 2 shows the associations between the different school types and the implementation of universal addiction prevention. Among the addiction topics, alcohol (61.9%), smoking (73.6%), and drug use (71.3%) were the most common themes in the schools. State schools were more likely to implement these programs than church or private schools. Problematic use of internet and electronic devices was addressed in 60.9% of the schools, while gaming and gambling were covered in only 18.9% of the participating institutions. Half (50.9%) of the institutions organized programs to prevent online and offline bullying. In the cases where the implementation was linked to the size of the school, larger schools implemented these prevention programs more frequently.
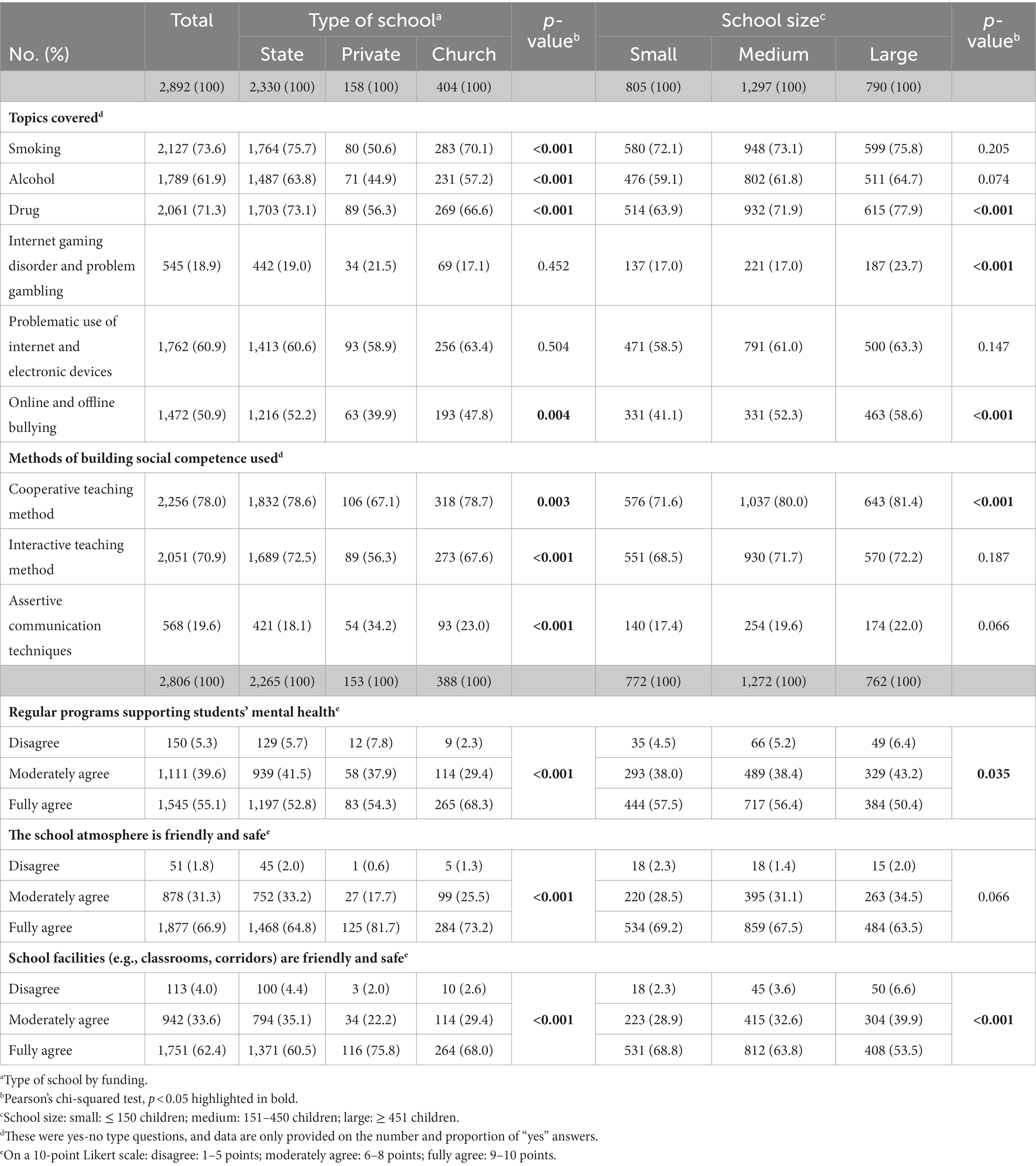
Table 2. Universal addiction prevention in Hungarian elementary schools.
The school health promotion program was mostly delivered by school personnel (64.5%), by someone in a legal relationship with the school (76.9%), or by external experts (66.9%) (data not shown in the tables). The number of addiction prevention topics covered was significantly associated with the diversity of implementers (p < 0.001, Figure 1).
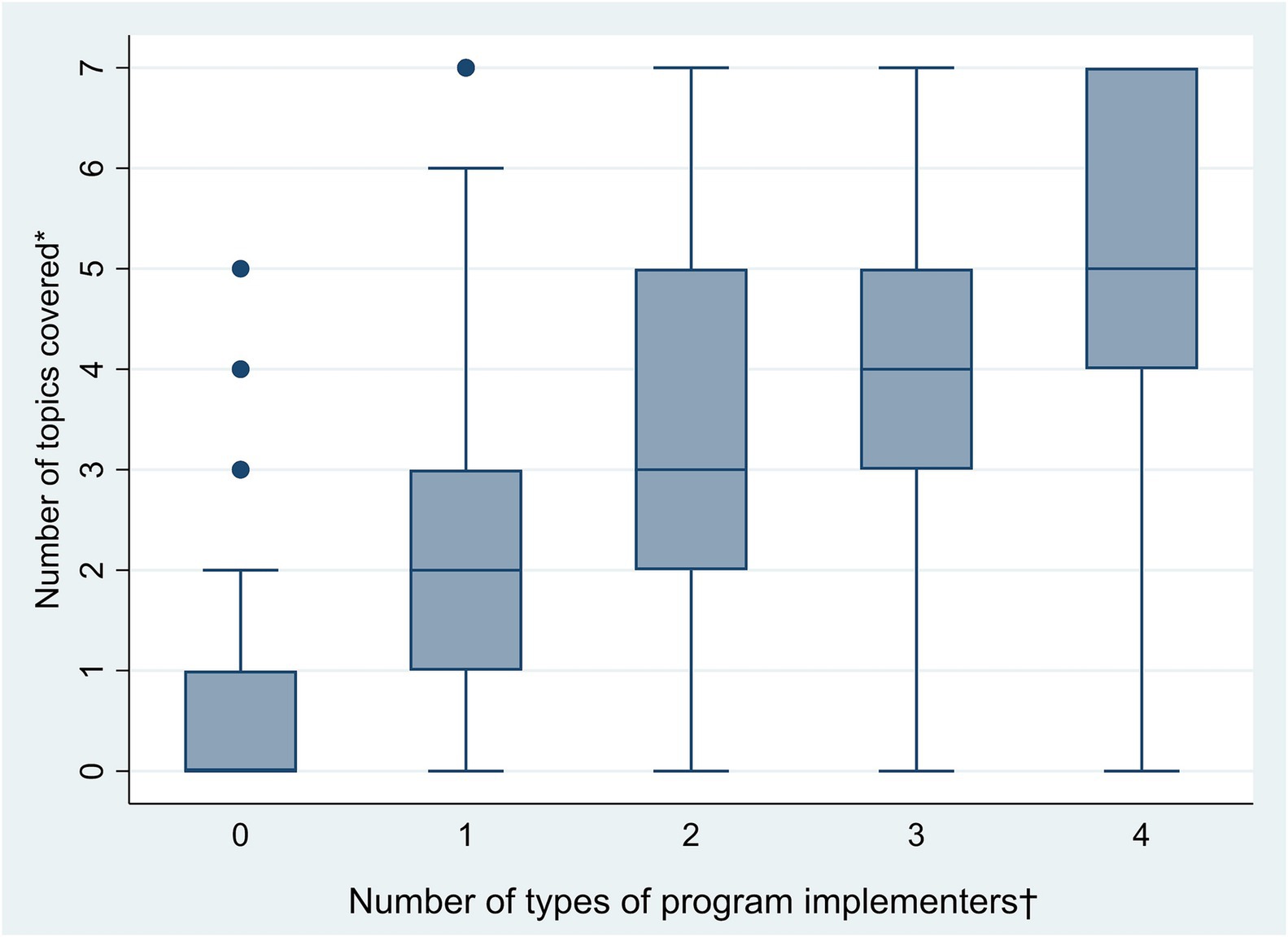
Figure 1. Box- and whisker plot showing the association between the number of topics covered by universal addiction prevention programs in Hungarian elementary schools and the diversity of implementers. * From the seven topics of addiction prevention and mental health programs listed in the questionnaire: smoking/alcohol/drug/internet gaming disorder and problem gambling/problematic use of internet and electronic devices/body image disorders/online and offline bullying. † From the five partners listed in the questionnaire: school personnel/persons working for the school on a contract (e.g., school health-visitors and physicians)/parents with an educational background in medicine or health sciences/external expert speakers/organizations or associations providing programs approved by experts. The bottom of the boxes indicates the lower quartile, the top the upper quartile, and the line within it is the median. Whiskers are at lower/upper quartile ± interquartile range or minimum/maximum value, whatever is more extreme.
In addition to specific addiction prevention programs, the use of either cooperative or interactive teaching methods to develop social skills was common in most schools (78.0% and 70.9%, respectively), but state and large schools were most likely to do so.
Over half of the schools reported having regular programs to support pupils’ mental health and having a safe and friendly school atmosphere and facilities. These differed significantly by school type and size, with the highest proportions of church and small schools (Table 2).
In the majority of the participating institutions, the environment for pupils was reported to be friendly and safe with private and small schools providing them the most frequently (Table 2). The presence of such a mental health-supporting environment was also significantly related to the frequency of dedicated opportunities for community building within the teaching staff (p < 0.001). Schools that organized community-building activities several times a year were more likely to have friendly and safe school atmosphere and facilities (Table 3).
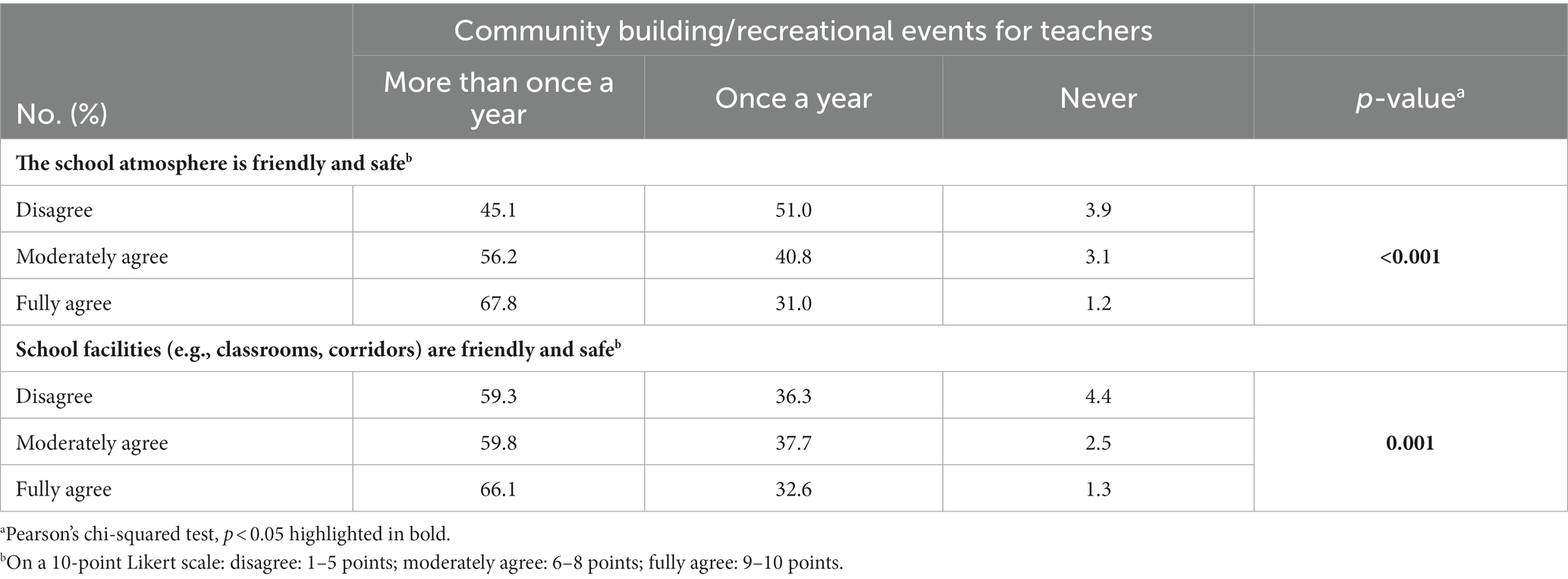
Table 3. Associations between the frequency of community-building/recreational events for teachers and the friendliness and safety of the school atmosphere and facilities in Hungarian elementary schools (N = 2,806).
Among the participating schools, 20.4% were found to be good-quality performers and 79.6% low-quality performers with respect to universal addiction prevention. There was no evidence that the logistic regression model with the number of types of implementers represented by a categorical variable would fit better; therefore, it was included as a continuous variable (LR test p = 0.8).
The type of school by funding, support for teachers’ work, and the number of types of implementers were significantly associated with the quality of implementation (Table 4). The odds of good-quality performance was twice as high in state schools than in private schools and it was 25.0% lower in large schools than in small schools, but the difference was not statistically significant. Compared to schools with support containing only health-related information, the odds was less than 0.5 for schools providing support that did not include health-related information. In schools where the support involved information provision complemented by skills training, the odds of good-quality performance was 14.5% higher than in the reference category, although the difference was not statistically significant. Each additional number of implementers increased the odds of good-quality performance by 11.1%.
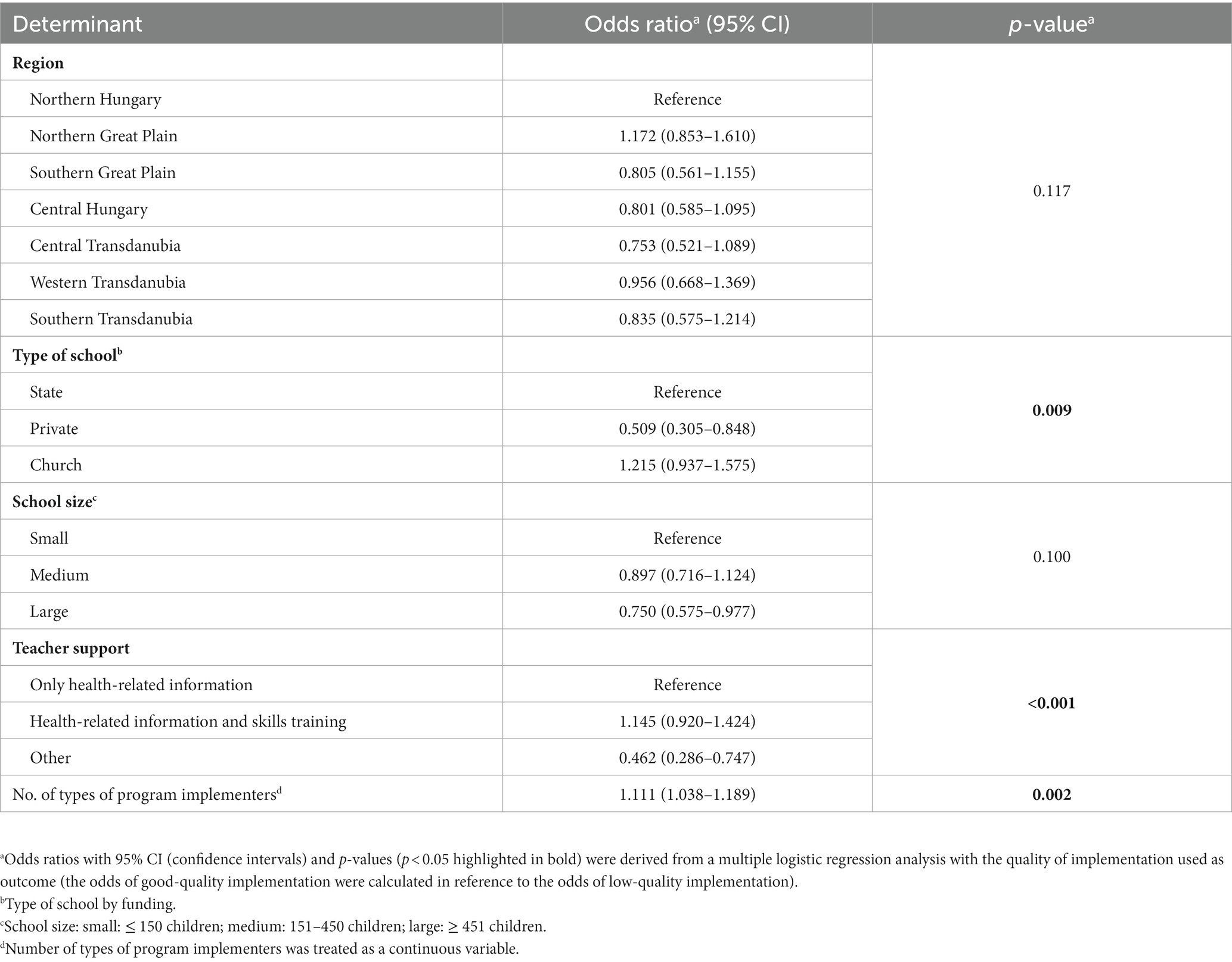
Table 4. Associations of good-quality implementation of universal addiction prevention in Hungarian elementary schools with the school’s regional location, type by funding, and size, the support for teachers and the diversity of program implementers (N = 2,806).
The results were structured around five themes. We illustrated the themes with quotes and typed both in italics.
Anxiety and the lack of emotional safety were identified as predictors of experimenting with addictive substances and devices. “Emotional security is what these children lack.” According to teachers’ observations, the likelihood of developing addictions is higher in cases where an imbalanced mental state is affected by impulses that can lead to addiction. Factors that may also play a role in the development and maintenance of addiction include the home environment, particularly the pattern set by parents and/or the child’s environment, and the cognitive abilities of the student: “Addiction prevention should start much earlier, during fetal development, e.g., if a pregnant mother smokes.” Teachers believed that not only the parents but also the schools and teachers were responsible for children developing appropriate health behavior.
Health education was also mentioned as essential for students and their parents to improve their knowledge of addictions and how to prevent them. It is important for students to be able to avoid being manipulated: “There is a very severe industry – one that reinforces addictions – and there is significant marketing going on for their attention, for their time”.
It is also necessary for parents to be able to provide better support to their children: “Parents have good intentions but often they do not know what they are putting in the hands of their children”.
According to teachers, the person in the classroom can do the most for the mental health of children in school. They confirmed that they are attentive to identifying when a pupil is experiencing a difficult situation in their social relationships that may require help. Teachers felt that it was part of their professional duty to address children’s mental health, recognizing that children can only be expected to perform well in school if they are emotionally balanced, and committed to doing so: “It is absolutely our job to deal with this. What’s wrong with a child who performed well before and now is not? What happened? There must be a psychological reason for that.”
Teachers expressed their conviction that they can provide meaningful help if they address students’ problems with the right approach: “It is important to have a trusting relationship with the children.” Sometimes they have to compensate for the lack of attention from parents, but there are also occasions when parents need to be advised on how to deal with their child.
Many factors can obstruct the implementation of addiction prevention in schools. Pupils’ workloads are increasing: “Kids today cannot be kids.” Children, parents and teachers are overworked. The expectations towards teachers are too high, these expectations change at a rapid pace, and some teachers do not agree that they should be involved in addiction prevention: “There should be a change of attitude, also on the part of the teachers, so that they feel it is their problem as well.” The classrooms are overcrowded, which makes health promotion activities very challenging. Among the hindering factors, teachers’ lack of material and methodological tools were mentioned: despite teachers’ sense of duty and attentiveness, they said that the tools and competences that they had acquired during their studies thus far with which they could support children’s mental health and help them develop their coping strategies were limited. Divisive behavior by the teaching staff, and the inappropriate family or teacher models were also highlighted as barriers: “A teacher who wants to convince children of anything as a smoker is not an authentic teacher”.
In addition, difficulties of cooperating with colleagues and with parents were both mentioned. Teachers need support from other professionals in schools, such as psychologists and teaching assistants. However, it seemed difficult for them to share responsibility for supporting children’s mental health, as they considered the less intense presence of these other professionals as an important limitation in their ability to do so. Teachers’ relevant statements included, “In many cases, there is no time to wait for support from other professionals to take action, something must be done immediately to restore the student’s mental balance.” and “The children do not approach the psychologist with the same trust as the one they see every day.” The difficulty of cooperating with parents was also mentioned as a major constraint. In some cases, parents consider school to be a knowledge-only institution rather than an educational institution and they reject teachers’ efforts to shape behavior: “They will educate [their child], you teach. But I cannot because there are such discipline problems”.
Based on the teachers’ perspectives, introducing an addiction prevention program requires the school leadership to be committed to supporting children’s mental health and to coordinate, manage, and monitor activities in this area and provide feedback on effectiveness. Sample comments were, “the school management should be committed because this is a joint task” and “the result must also be advertised.” A cooperative attitude and mutual support from the teaching staff are also essential. Additional help is needed in the form of good practices to build cooperation with fellow teachers and with parents as well. Participants believed that teachers’ work is facilitated when pupils know and follow the school rules. The maintenance of teachers’ mental well-being was also emphasized: “A basic requirement for the development of children’s mental health is the mental health balance of the teacher.” This can be supported, among other things (e.g., skills training), by social recognition/acknowledgment of the teacher.
Collaboration with other teachers at school was also mentioned as important and that would facilitate preventive work: “Together we can make a much more powerful difference in shaping the mental health of pupils.” Thus, the engagement of fellow teachers in the program was also mentioned as crucial. This can be facilitated and strengthened if teachers become personally involved in the program: if they understand that the methods used to develop children’s mental health also support their own health and burnout prevention or if the new methods are also introduced and tried out among the staff: “bringing the games into the staff-room” Additionally, creating programs that involve the children of fellow teachers also seemed useful for teachers so they become emotionally involved. It was also deemed important and very helpful to establish a dialogue with parents, such as through joint programs; in this way, addressing children’s mental health could become a common goal. The same applied to children’s discipline and compliance, which were seen as two crucial factors of effective work at school. These factors were influenced most by the patterns that students bring from home, as well as consistent and clear school rules.
This was a mixed-methods research project that examined the implementation of addiction prevention and its influencing factors in elementary schools on a national level for the first time in Hungary. We have demonstrated - based on data provided by school principals - that the quality implementation of the aforementioned school program is closely linked to institutional characteristics of schools, namely to the nature of support and training provided to teachers in this domain, to the diversity of program implementers, and to the type of schools by funding. Furthermore, our focus group-based study provided insights into the challenges associated with program implementation, particularly from the perspective of teachers who serve as vital stakeholders. By analyzing their perspectives, we were able to corroborate our survey-based findings regarding the significance of institutional factors, including the presence of committed leadership that not only provides comprehensive training but also actively engages and supports teachers both individually and as a community.
In addition to the family, the school serves as a vital institutional setting for young individuals, exerting a significant influence on their physical, psychological, and social development. Empowering children and adolescents to avoid harmful substances, such as alcohol and tobacco, and maladaptive technology use requires multidisciplinary efforts and knowledge (World Health Organization and United Nations Educational Scientific and Cultural Organization, 2021). Our findings have also shown that collaborating with a greater variety of partners enhances the quality of addiction prevention implementation. Furthermore, we found that schools with a higher number of program implementers can address a wider, more diverse range of addiction-related topics in their curricula. This result reinforces the standards provided in the International Standards on Drug Use Prevention (United Nations Office on Drugs and Crime and the World Health Organization, 2018). Cooperation among teachers, parents, and other professionals was also mentioned in the focus-groups as an important supporting factor of effective implementation. This collaborative approach is in line with the WHO and UNESCO endorsed framework on establishing health-promoting schools (World Health Organization and United Nations Educational Scientific and Cultural Organization, 2021) and it has been demonstrated to be effective in practice (Das et al., 2016).
School size can influence the implementation of school health programs, but its effect is contradictory and depends on the nature of the programs and the type of school (Bast et al., 2017). In our model, school size was not shown to be associated with the quality of program implementation. However, our univariate analysis detected differences in terms of institutional support of implementation by school size in favor of large schools. This may be explained by the Hungarian regulatory frameworks, which determine the number of health professionals who can be employed by the schools. For example, schools with fewer than 800 pupils can only employ one school health-visitor [a specialist with similar tasks to a school nurse (National Public Health Centre, n.d.)] and one school physician on a part-time basis (Népjóléti Minisztérium (NM) – Ministry of Welfare, 1997), and one part-time school psychologist is allowed per 500 pupils (Magyar Kormány-Hungarian Government, 2013). In this respect, larger schools are in a better position, as the presence of a full-time school health-visitor and psychologist creates opportunities for their involvement in both program design and implementation. The study by McIsaac et al. (2013) also highlighted the importance of enhancing organizational capacity for effective implementation of health promotion activities.
Different school types by funding also have different resources, which, as our quantitative data showed, can influence the implementation quality and the provision of addiction prevention. State and church schools were found to perform better than private schools in quality implementation according to our model. Church schools may be in a better position in the context of mental health promotion. These institutions are obliged by their church to maintain contact with the local parish and its pastors and/or to employ an institutional pastor who is responsible for the support of the whole school: pupils, staff and parents (A magyarországi evangélikus egyház zsinata – Synod of the Evangelical Church in Hungary, 2005; A Magyarországi Református Egyház-Reformed Church of Hungary, 2013; Katolikus Egyház - Catholic Church, 2015). This regulatory framework may be reflected in our results, which showed the highest proportion in the provision of regular programs supporting pupils’ mental health in church schools (68.3% vs. 52.8 and 54.3% in state and private schools, respectively).
We controlled our analysis for regional differences in the quality of implementation of addiction prevention, and our results did not show any independent effect of region. However, it is important to acknowledge that implementation differences may still exist at the level of smaller administrative units. Previous studies from other countries have shown that different regions may have varying levels of investment and commitment to school health promotion, which can impact the effectiveness and quality of implementation. Additionally, regional variations in socioeconomic conditions and support from the Regional Education Authority can also influence the quality of implementation of school health promotion initiatives (Darlington et al., 2018; Pereira and Sanchez, 2018).
Support of teachers with health-related information was shown to be an important facilitator of the implementation quality. Parallel with this, in our focus groups, the enhancement of children’s health literacy was mentioned as an important task, which requires adequate health-related information. These are in line with previous studies showing that competent and trained teachers are the keys to promoting and supporting young people’s health by facilitating social and emotional skill building (Durlak et al., 2011). Our survey results indicated that teachers still lack sufficient, complex health education and skill development training and support in one-third of schools. These issues were also reflected in the outcomes of our focus group-based study underlining the importance of skill development. Similar hindering factors of the effectiveness of school-based addiction prevention programs than those, mentioned in our focus-groups, were already detected in Hungary (Paksi and Demetrovics, 2011). It was found that although the number of these programs has been increasing since the early 2000s, most programs are short, mainly restricted to health education without social–emotional skill learning, and are often led by external presenters with frontal-type education (Paksi and Demetrovics, 2011). The frontal type of education does not meet the new methodological needs of the Z and Alpha generations, and its motivational approaches are not or only partially effective (Fromann, 2017).
Additional results from our project further underscored the significance of school characteristics. Consistent with multiple prior studies (Gottfredson and Gottfredson, 2002; Elliott and Mihalic, 2004; Forman et al., 2009; McIsaac et al., 2013; Garcia et al., 2023), it has been demonstrated in our focus-groups that ensuring effective implementation relies on dedicated leadership, along with the provision of support for the school staff acting as implementers and by greater organizational capacity (good communication and willingness to cooperate). Additionally, our survey-based study showed that educational institutions that invest in the well-being of the teaching community more than once a year have significantly greater success in creating a school environment that supports mental health, which is also an important school-based protective factor (Franco et al., 2022). The focus group discussions provided a possible explanation for this association, as teachers emphasized that they can generally do the most for children’s mental health based on the trust between them and the children, and the maintenance of their own mental health was mentioned as key for effective work. The latter is in line with previous findings on the importance of teachers’ mental health (Lever et al., 2017). It was also mentioned as beneficial for these processes if school leaders prioritize the mental health of pupils and teachers and provide the necessary training and supportive environment for teachers. This further underlines the need for teachers’ skills training, as this could not only help them facilitate pupils’ skill building (as mentioned above) but also provide them with help maintaining their own mental well-being. Community building can also have this two-sided beneficial effect by facilitating cooperation in the implementation tasks and improving mental health.
Our study underlines the importance of institutional characteristics in implementing school-based universal addiction prevention. The training and mental health support of teachers and their collectives are important intervention points that should be invested in by local and national policymakers to increase the effectiveness of addiction prevention and to empower teachers. In addition, strengthening staff cohesion, teacher–teacher and parent–teacher dialogue and cooperation is essential not only during the introduction of new programs and methods but also to ensure their sustainability (Bast et al., 2017).
Hungary has the second-highest rate of preventable deaths among the 36 OECD Member States (OECD, 2019). The leading causes of avoidable mortality are cardiovascular diseases and cancer (OECD, 2019), for which the main risk factors are alcohol consumption and smoking. It is particularly significant in this regard that the rate of alcohol and cigarette use among Hungarian adolescents is high and above the European average (ESPAD Group, 2020). However, there are several challenges to implementing effective school-based universal addiction prevention interventions in this country. One is to ensure that teachers are properly encouraged to do the difficult work of introducing these pedagogical methods and programs that promote pupils’ mental health outside the different projects and supported in doing so. Effective implementation is further hampered by the aging of the Hungarian teacher population and high rates of turnover, stress, and burnout among teachers (Mihály, 2002; Paksi et al., 2015; Bacsa-Bán, 2019; Hajdu et al., 2022), which were further aggravated by the COVID-19 pandemic. The worsening trend in children’s mental health, the significant increase in children’s psychiatric illnesses (Képviselői Információs Szolgálat Infojegyzet, 2022) and the steep rise in the number of children with severe learning disabilities over the past 20 years (Hungarian Central Statistical Office, 2023b) are also aggravating factors. Among these conditions, it is of crucial importance to enhance the attractiveness of the teaching profession, to motivate talented individuals able to cope with these difficulties. Part of this task for the coming years is to modify teachers’ training curricula in order to ensure that newly qualified teachers are equipped with the knowledge and pedagogical methods in health promotion that facilitate the development of skills and that are adapted to the learning needs of new generations. Furthermore, integrating a comprehensive health education program into the National Core Curricula that adheres to standards is also essential. This will enable students to gain the knowledge, attitudes, skills, and experiences needed to lead a healthy lifestyle which will not only benefit them personally but also contribute to the overall well-being of society.
In addition to the above-described factors, school-based local planning and involvement in decisions about implementation can further enhance the success of school-based programs (Payne et al., 2006; Payne, 2009) with program/method integration into school routines and school curricula (Rohrbach et al., 1993; Mihalic et al., 2008). It is also essential to prioritize actions that involve input from multiple stakeholders for the nationwide improvement of addiction prevention in schools. Health Services, Counseling, Psychological Services specialists (e.g., school health-visitors, physicians, psychologists) are important partners in school health promotion (CDC, n.d.). Capacity must be built in the current service so that its members can actively participate in designing and implementing school health promotion programs and support such activities of teachers, regardless of the schools’ characteristics. Equal support for all schools, regardless of size and funding would ensure that every student has access to quality health promotion which can significantly enhance the chances of students achieving health-promoting behavior.
Notably, our results have limitations. Due to the cross-sectional nature of the project, it can only provide a detailed description of universal addiction prevention in Hungarian elementary schools at a given point in time. The survey method did not allow schools to provide a detailed description of their health promoting activities. However, a relatively short, easy-to-complete questionnaire seemed the best method to gather comparable data at a national level. An additional limitation is that the survey was completed by principals of schools, which may result in some distortions in the data provided compared to the actual implementation of the programs in schools and classrooms. More accurate data on implementation could be obtained if the questionnaire was also completed by teachers, school health service professionals, psychologists and by students as well (in older age groups) above principals in schools. This method would also make it possible to examine the consistency of data from different sources of information and to identify possible discrepancies. Another limitation is the lack of information on the actual number of school health services specialists and psychologists working in the institutions at the time of the survey. We could only infer their number from the school sizes and the related regulations; however, there may have been vacancies. As participation in the focus groups was voluntary, sampling bias cannot be excluded in our qualitative data. The opinions and perceptions of teachers’ who were willing to discuss the issues of addiction prevention in school are not generalizable on a national level. In addition, this sampling method did not allow the potential role of school type and school size in the qualitative results to be explored. Member checking to improve credibility of the results was not possible in this study, due to our indirect contact with participants (we only communicated with the teachers through the principals).
The use of alcohol, tobacco, and illicit substances typically first occurs in adolescence, while maladaptive technology use or technology addiction can arise from early childhood, as children today are born and grow up in environments in which digital technologies are widely available (Benedetto and Ingrassia, 2021). Both substance and behavioral addictions can lead to significant impairment in personal, family, social, educational or other important life domains and represent high mental and physical health burdens. We have demonstrated that good-quality implementation of school-based universal addiction prevention programs is closely linked to the provision of training for teachers that includes health education and social skills training, to greater diversity of program implementers and to schools being run by the state or a church. Additionally, from our focus group-based study, we could reinforce our results on the importance of institutional factors, such as committed leadership, providing training, and engaging and supporting teachers individually and as a community. These results may inform policymakers, schools, teachers, adolescents, and their parents about which factors to invest in to improve the school-based universal addiction prevention.
The datasets presented in this article are not readily available because the data analyzed in this study was obtained from the Ministry of Human Capacities, Hungary. This authority disposes all rights upon providing access to these datasets. Requests to access the datasets should be directed to ZR, enN1enNhLnJha29zeUBhb2sucHRlLmh1.
The studies involving humans were approved by The Ethical Review Board of the National Korányi Institute of Pulmonology, Budapest, Hungary. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
DÁ: validation, data curation, writing the original draft, review and editing, and visualization. ZV: formal analysis, visualization, and validation. MS: review and editing of the original draft. ZC: methodology, formal analysis, and review and editing. ZR: conceptualization, methodology and investigation along with writing the original draft and review and editing it, supervision, and project administration. All authors contributed to the article and approved the submitted version.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Scientific Foundations of Education Research Program of the Hungarian Academy of Sciences (SZKF-12/2021), WHO-BCA 2019-2020 (2019/881133-0), Central Budget of Hungary for 2019 (according to Act L of 2018, Annex 1, Chapter XX. Ministry of Human Capacities, Title No. 20.22.28. “Tasks related to the National Public Health Strategy”). The contributions of the first author (DÁ) were supported by the ÚNKP-22-3-I-SE-11 New National Excellence Program of the Ministry for Culture and Innovation from the source of the National Research, Development and Innovation Fund.
Thank you to Annamária Somhegyi for her help in designing the questionnaire and conducting the survey. We greatly appreciate the efforts of the colleges of the Ministry of Human Capacities in helping send the questionnaire to the schools. We give special thanks to school principals and teachers for giving their time to participate in this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
A magyarországi evangélikus egyház zsinata – Synod of the Evangelical Church in Hungary . (2005). Évi viii. Törvény Az Egyház Intézményeiről [act viii of 2005 on the institutions of the Church] [Accessed 2023 26.02]. Available at: https://zsinat.lutheran.hu/torvenyek/hatalyos-toervenyek/2005.%20evi%20VIII.%20toerveny%20az%20egyhaz%20intezmenyeirol.pdf/view.
A Magyarországi Református Egyház-Reformed Church of Hungary . (2013). Évi V. Törvény a Magyarországi Református Egyház 1995. Évi I. Köznevelési Törvényének Átfogó Módosításáról/act V of 2013 on the comprehensive amendment of the public education act I of 1995 of the reformed Church of Hungary/[Accessed 2023 02.26]. Available at: http://refpedi.hu/sites/default/files/hir_kepek/2013_%20evi_%20VI_%20KOZNEVELESI%20TV_EGYSEGES%20SZERKEZET.pdf.
Andl, H. (2020). A Kisiskolák És Lehetőségeik [small schools yand their opportunities]. Educatio 29, 409–424. doi: 10.1556/2063.29.2020.3.6
Bacsa-Bán, A. (2019). A Szakmai Pedagógusok (Pedagógusi) Pálya Elhagyásának Vizsgálata Több Dimenzióban. Opus et Educatio 6:6. doi: 10.3311/ope.312
Balogh, M. A Demográfiai Változások Hatása a Közoktatásra [the impact of demographic changes on public education]. Önkormányzat és közoktatás; (2023); Szekszárd (2009).
Bann, D., Hamer, M., Parsons, S., Ploubidis, G. B., and Sullivan, A. (2016). Does an elite education benefit health? Findings from the 1970 British cohort study. Int. J. Epidemiol. 46, 293–302. doi: 10.1093/ije/dyw045
Bast, L. S., Due, P., Ersbøll, A. K., Damsgaard, M. T., and Andersen, A. (2017). Association of School Characteristics and Implementation in the X: it study—a school-randomized smoking prevention program. J. Sch. Health 87, 329–337. doi: 10.1111/josh.12500
Benedetto, L., and Ingrassia, M. (2021). “Digital Parenting: Raising and Protecting Children in Media World,” in Parenting - Studies by an Ecocultural and Transactional Perspective. IntechOpen.
Bessems, K., Bartelink, N., and Prevo, L.. She monitoring report 2020: Country-specific results of Hungary. Denmark: Schools for Health in Europe Network Foundation (SHE), (2020).
Bozzini, A. B., Bauer, A., Maruyama, J., Simões, R., and Matijasevich, A. (2021). Factors associated with risk behaviors in adolescence: a systematic review. Braz J Psychiatry 43, 210–221. doi: 10.1590/1516-4446-2019-0835
Brener, N. D., Bohm, M. K., Jones, C. M., Puvanesarajah, S., Robin, L., Suarez, N., et al. (2022). Use of tobacco products, alcohol, and other substances among high school students during the Covid-19 pandemic—adolescent behaviors and experiences survey, United States, January–June 2021. MMWR Suppl. 71, 8–15. doi: 10.15585/mmwr.su7103a2
Busch, P. A., and McCarthy, S. (2021). Antecedents and consequences of problematic smartphone use: a systematic literature review of an emerging research area. Comput. Hum. Behav. 114:106414. doi: 10.1016/j.chb.2020.106414
CDC . School health services [cited 2023 26.02]. Available at: https://www.cdc.gov/healthyschools/schoolhealthservices.htm.
Centers for Disease Control and Prevention . What works in schools (Accessed 2023 01.06). Available at: https://www.cdc.gov/healthyyouth/whatworks/index.htm.
Dahl, D., and Bergmark, K. H. (2020). Problematic internet use: a scoping review-longitudinal research on a contemporary social problem, 2006-2017. Nordisk Alkohol Nark 37, 497–525. doi: 10.1177/1455072520941997
Darlington, E. J., Violon, N., and Jourdan, D. (2018). Implementation of health promotion Programmes in schools: an approach to understand the influence of contextual factors on the process? BMC Public Health 18:163. doi: 10.1186/s12889-017-5011-3
Das, J. K., Salam, R. A., Arshad, A., Finkelstein, Y., and Bhutta, Z. A. (2016). Interventions for adolescent substance abuse: an overview of systematic reviews. J. Adolesc. Health 59, S61–S75. doi: 10.1016/j.jadohealth.2016.06.021
Derevensky, J. L., Hayman, V., and Lynette, G. (2019). Behavioral addictions: excessive gambling, gaming, internet, and smartphone use among children and adolescents. Pediatr. Clin. N. Am. 66, 1163–1182. doi: 10.1016/j.pcl.2019.08.008
De-Sola Gutiérrez, J., Rodríguez de Fonseca, F., and Rubio, G. (2016). Cell-phone addiction: a review. Front. Psychiatry 7:175. doi: 10.3389/fpsyt.2016.00175
Domitrovich, C. E., Bradshaw, C. P., Poduska, J. M., Hoagwood, K., Buckley, J. A., Olin, S., et al. (2008). Maximizing the implementation quality of evidence-based preventive interventions in schools: a conceptual framework. Adv. School Ment. Health Promot. 1, 6–28. doi: 10.1080/1754730x.2008.9715730
Dunne, T., Bishop, L., Avery, S., and Darcy, S. (2017). A review of effective youth engagement strategies for mental health and substance use interventions. J. Adolesc. Health 60, 487–512. doi: 10.1016/j.jadohealth.2016.11.019
Durlak, J., Weissberg, R., Dymnicki, A., Taylor, R., and Schellinger, K. (2011). The impact of enhancing students’ social and emotional learning: a Meta-analysis of school-based universal interventions. Child Dev. 82, 405–432. doi: 10.1111/j.1467-8624.2010.01564.x
Elliott, D. S., and Mihalic, S. (2004). Issues in disseminating and replicating effective prevention programs. Prev. Sci. 5, 47–53. doi: 10.1023/b:prev.0000013981.28071.52
Emberi Erőforrások Minisztériuma (EMMI) – Ministry of Human Capacities . (2012) 20/2012. (viii. 31.) Emmi Rendelet a Nevelési-Oktatási Intézmények Működéséről És a Köznevelési Intézmények Névhasználatáról/Emmi decree 20/2012. (viii. 31.) on the operation of the educational institutions and on the use of names of the public education institutions/ (Accessed 2023 26.02). Available at: https://njt.hu/jogszabaly/2012-20-20-5H.
Emond, A. M., and Griffiths, M. D. (2020). Gambling in children and adolescents. Br. Med. Bull. 136, 21–29. doi: 10.1093/bmb/ldaa027
Esmaeelzadeh, S., Moraros, J., Thorpe, L., and Bird, Y. (2018). Examining the association and directionality between mental health disorders and substance use among adolescents and young adults in the U.S. and Canada-a systematic review and Meta-analysis. J. Clin. Med. 7:543. doi: 10.3390/jcm7120543
ESPAD Group (2020). Espad report 2019: Results from the European school survey project on alcohol and other drugs. Luxembourg: EMCDDA Joint Publications, Publications Office of the European Union.
Estrada, C. A. M., Lomboy, M. F. T. C., Gregorio, E. R., Amalia, E., Leynes, C. R., Quizon, R. R., et al. (2019). Religious education can contribute to adolescent mental health in school settings. Int. J. Ment. Heal. Syst. 13:28. doi: 10.1186/s13033-019-0286-7
European Monitoring Centre for Drugs and Drug Addiction . European prevention curriculum: A handbook for decision-makers, opinion-makers and policy-makers in science-based prevention of substance use. Luxembourg: Publications Office of the European Union (2019).
Evren, C., Dalbudak, E., Evren, B., and Demirci, A. C. (2014). High risk of internet addiction and its relationship with lifetime substance use, psychological and behavioral problems among 10 (Th) grade adolescents. Psychiatr. Danub. 26, 330–339. Epub 2014/11/08.
Forman, S., Olin, S., Hoagwood, K., Crowe, M., and Saka, N. (2009). Evidence-based interventions in schools: developers’ views of implementation barriers and facilitators. Sch. Ment. Heal. 1, 26–36. doi: 10.1007/s12310-008-9002-5
Franco, K., Baumler, E., Torres, E. D., Lu, Y., Wood, L., and Temple, J. R. (2022). The link between school climate and mental health among an ethnically diverse sample of middle school youth. Curr. Psychol. 42, 18488–18498. doi: 10.1007/s12144-022-03016-y
Fromann, R. Játékoslét – a Gamifikáció Világa [Playerlife – the world of gamification]. Budapest: Typotex kiadó (2017).
Garcia, A., Sprang, G., and Clemans, T. (2023). The role of school leaders in cultivating a trauma-informed school climate. Child Youth Serv. Rev. 146:106816. doi: 10.1016/j.childyouth.2023.106816
Gentile, D. (2009). Pathological video-game use among youth ages 8 to 18: a National Study. Psychol. Sci. 20, 594–602. doi: 10.1111/j.1467-9280.2009.02340.x
Gottfredson, D. C., and Gottfredson, G. D. (2002). Quality of school-based prevention programs: results from a National Survey. J. Res. Crime Delinq. 39, 3–35. doi: 10.1177/002242780203900101
Griffin, K. W., and Botvin, G. J. (2010). Evidence-based interventions for preventing substance use disorders in adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 19, 505–526. doi: 10.1016/j.chc.2010.03.005
Griffin, K. W., Epstein, J. A., Botvin, G. J., and Spoth, R. L. (2001). Social competence and substance use among rural youth: mediating role of social benefit expectancies of use. J. Youth Adolesc. 30, 485–498. doi: 10.1023/a:1010449300990
Hajdu, T., Hermann, Z., Horn, D., Hőnich, H., and Varga, J.. A Közoktatás Indikátorrendszere 2021. Budapest: Közgazdaság-és Regionális Tudományi Kutatóközpont, Közgazdaság-tudományi Intézet (2022). Available at: https://kti.krtk.hu/wp-content/uploads/2022/02/A_kozoktatas_indikatorrendszere_2021.pdf.
Herke, M., Moor, I., Winter, K., Hack, M., Hoffmann, S., Spallek, J., et al. (2022). Role of contextual and compositional characteristics of schools for health inequalities in childhood and adolescence: a scoping review. BMJ Open 12:e052925. doi: 10.1136/bmjopen-2021-052925
Hungarian Central Statistical Office . (2023a) Regional atlas–regions [cited 2023 26.02]. Available at: https://www.ksh.hu/regionalatlas_regions.
Hungarian Central Statistical Office . (2023b). Education: Annual Sumary tables: 23.1.1.6 children and students with special educational needs by type of disabilities [Accessed 2023 26.02]. Available at: https://www.ksh.hu/stadat_files/okt/en/okt0006.html.
Inchley, J. C. D., Budisavljevic, S., Torsheim, T., Jåstad, A., and Cosma, A. (2020). Spotlight on adolescent health and well-being. Findings from the 2017/2018 health behaviour in school-aged children (Hbsc) survey in Europe and Canada. International report. Copenhagen: WHO Regional Office for Europe.
Isralowitz, R., and Reznik, A. (2015). Impact of religious education and religiosity on adolescent alcohol use and risk-taking behavior. Relig. Educ. 110, 303–310. doi: 10.1080/00344087.2015.1039388
Katolikus Egyház - Catholic Church . (2015). In: Codex Iuris Canonici -5th ed [internet]. Budapest: Szent István társulat az apostoli szentszék könyvkiadója. Available at: https://torvenykonyv.katolikus.hu/www.vatican.va/archive/cod-iuris-canonici/hu/documents/cic_konyvIII_0796-0806_hu.html.
Kelly, S., and Leung, J. (2021). The new frontier of Esports and gaming: a scoping Meta-review of health impacts and research agenda. Front. Sports Active Living 3:3. doi: 10.3389/fspor.2021.640362
Képviselői Információs Szolgálat Infojegyzet . (2022). Fiatalok Mentális Egészsége. Available at: https://www.parlament.hu/documents/10181/63291245/Infojegyzet_2022_11_fiatalok_mentalis_egeszsege.pdf/a567afa0-d502-aa12-4199-cc843370ea3a?t=1657529636549. (Accessed February 26, 2023).
Kis, M., and Goda, P. (2013). Pest Megye Településeinek Versenyképességi Térképe. In: Új hangsúlyok a területi fejlődésben [Internet]. Szeged: JATEPress; [116–28]. Available at: http://eco.u-szeged.hu/download.php?docID=40048.
Koo, H. J., and Kwon, J. H. (2014). Risk and protective factors of internet addiction: a Meta-analysis of empirical studies in Korea. Yonsei Med. J. 55, 1691–1711. doi: 10.3349/ymj.2014.55.6.1691
Kovačić Petrović, Z., Peraica, T., Kozarić-Kovačić, D., and Palavra, I. R. (2022). Internet use and internet-based addictive Behaviours during coronavirus pandemic. Curr. Opin. Psychiatry 35, 324–331. doi: 10.1097/yco.0000000000000804
Krueger, R. A., and Casey, M. A.. Focus groups: A practical guide for applied research, 5th Edition. USA: SAGE Publications (2015).
Lam, L. T. (2014). Risk factors of internet addiction and the health effect of internet addiction on adolescents: a systematic review of longitudinal and prospective studies. Curr. Psychiatry Rep. 16:508. doi: 10.1007/s11920-014-0508-2
Lee, H., and Henry, K. L. (2022). Adolescent substance use prevention: long-term benefits of school engagement. J. Sch. Health 92, 337–344. doi: 10.1111/josh.13133
Lever, N., Mathis, E., and Mayworm, A. (2017). School mental health is not just for students: why teacher and school staff wellness matters. Rep Emot Behav Disord Youth 17, 6–12. Epub 2017/01/01.
Lipták, M. Z., and Tarkó, K. (2020). Hétköznapi Egészségfogalom–Tévképzetek, Naiv Elméletek, Mítoszok Vagy Laikus Értelmezések [everyday health concept–misconceptions, naive theories, myths or lay interpretations]. Magyar Pedagógia 120, 33–46. doi: 10.17670/MPed.2020.1.33
Lipták, M. Z., and Tarkó, K. (2021). “Az Egészség Megjelenése a Nemzeti Alaptantervekben (1995-2020)” in A Neveléstudomány Válaszai a Jövő Kihívásaira: Xxi Országos Neveléstudományi Konferencia Szeged, 2021 November 18–20: Program, Előadás-Összefoglalók. eds. G. Molnár and E. Tóth (Szeged, Magyarország: MTA Pedagógiai Tudományos Bizottság, SZTE BTK Neveléstudományi Intézet), 265.
Liu, T. C., Desai, R. A., Krishnan-Sarin, S., Cavallo, D. A., and Potenza, M. N. (2011). Problematic internet use and health in adolescents: data from a high school survey in Connecticut. J. Clin. Psychiatry 72, 836–845. doi: 10.4088/JCP.10m06057
Lochman, J. E., and Wells, K. C. (2002). The coping power program at the middle-school transition: universal and indicated prevention effects. Psychol. Addict. Behav. 16, S40–S54. doi: 10.1037/0893-164X.16.4S.S40
Lozano-Blasco, R., Latorre-Martínez, M. P., and Cortés-Pascual, A. (2022). Screen addicts: a Meta-analysis of internet addiction in adolescence. Child Youth Serv. Rev. 135:106373. doi: 10.1016/j.childyouth.2022.106373
MacArthur, G. J., Harrison, S., Caldwell, D. M., Hickman, M., and Campbell, R. (2016). Peer-led interventions to prevent tobacco, alcohol and/or drug use among young people aged 11–21 years: a systematic review and Meta-analysis. Addiction 111, 391–407. doi: 10.1111/add.13224
Magyar Kormány-Hungarian Government . 5/2020. (I. 31.) Korm. Rendelet a Nemzeti Alaptanterv Kiadásáról, Bevezetéséről És Alkalmazásáról Szóló 110/2012. (vi. 4.) Korm. Rendelet Módosításáról [5/2020. (I. 31.) government decree amending the 110/2012. (vi. 4.) Governement decree on the publication, introduction and application of the National Core Curriculum]. (2020). In: Magyar Közlöny [Internet]. [290–446]. Available at: https://magyarkozlony.hu/dokumentumok/3288b6548a740b9c8daf918a399a0bed1985db0f/megtekintes.
Magyar Kormány-Hungarian Government . (2013). 326/2013. (viii. 30.) Korm. Rendelet a Pedagógusok Előmeneteli Rendszeréről És a Közalkalmazottak Jogállásáról Szóló 1992. Évi xxxiii. Törvény Köznevelési Intézményekben Történő Végrehajtásáról [government decree 326/2013 (viii. 30.) on the implementation of act xxxiii of 1992 in public education institutions on the promotion system for teachers and the status of public servants] [cited 2023 26.02]. Available at: https://njt.hu/jogszabaly/2013-326-20-22.
Marconi, A., Di Forti, M., Lewis, C. M., Murray, R. M., and Vassos, E. (2016). Meta-analysis of the association between the level of Cannabis use and risk of psychosis. Schizophr. Bull. 42, 1262–1269. doi: 10.1093/schbul/sbw003
McIsaac, J.-L. D., Read, K., Veugelers, P. J., and Kirk, S. F. L. (2013). Culture matters: a case of school health promotion in Canada. Health Promot. Int. 32, 207–217. doi: 10.1093/heapro/dat055
Mihalic, S. F., Fagan, A. A., and Argamaso, S. (2008). Implementing the Lifeskills training drug prevention program: factors related to implementation Fidelity. Implement. Sci. 3:5. doi: 10.1186/1748-5908-3-5
Mihály, I. (2002). A Tanári Hivatás És a Munkaerő-Piac [the teaching profession and the labour market]. Új Pedagógiai Szemle. Available at: https://folyoiratok.oh.gov.hu/uj-pedagogiai-szemle/a-tanari-hivatas-es-a-munkaero-piac.
Monitoring the Future . Trends in 30-day prevalence of use of various drugs for grades 8, 10, and 12 combined (2022) (Accessed 2023 17.08). Available at: https://monitoringthefuture.org/wp-content/uploads/2022/12/mtf2022table07.pdf.
Motiejūnaitė-Schulmeister, A., Sicurella, A., and Birch, P. (2022) in The structure of the European education systems 2022/2023: schematic diagrams. ed. P. Birch (European Commission, European Education Culture Executive Agency) Publications Office of the European Union
Nándori, E. S. (2021). Perception of the reasons for living in poverty in Hungary. Hung. Stud. 35, 80–96. doi: 10.1556/044.2021.00156
National Public Health Centre . Egészségvonal: Health care system-health-visitor service [Accessed 2023 26.02]. Available at: https://egeszsegvonal.gov.hu/en/health-care-system/health-visitor-service.html.
Nawi, A. M., Ismail, R., Ibrahim, F., Hassan, M. R., Manaf, M. R. A., Amit, N., et al. (2021). Risk and protective factors of drug abuse among adolescents: a systematic review. BMC Public Health 21:2088. doi: 10.1186/s12889-021-11906-2
Népjóléti Minisztérium (NM) – Ministry of Welfare . 26/1997. (Ix. 3.) Nm Rendelet Az Iskola-Egészségügyi Ellátásról [Nmdecree 26/1997. (Ix. 3.) on School Health Service] [Accessed 2023 26.02]. Available at: https://njt.hu/jogszabaly/1997-26-20-3D.
Onrust, S. A., Otten, R., Lammers, J., and Smit, F. (2016). School-based Programmes to reduce and prevent substance use in different age groups: what works for whom? Systematic review and Meta-regression analysis. Clin. Psychol. Rev. 44, 45–59. doi: 10.1016/j.cpr.2015.11.002
Országgyűlés-Hungarian Parliament . (2003). Évi lxi. Törvény a Közoktatásról Szóló 1993. Évi lxxix. Törvény Módosításáról/act lxi of 2003. Amending act lxxix of 1993 on public education/ [Accessed 2023 28.02]. Available at: https://njt.hu/jogszabaly/2003-61-00-00.
Országgyűlés-Hungarian Parliament . (2011). Évi cxc. Törvény a Nemzeti Köznevelésről/act cxc of 2011 on National Public Education/ [cited 2023 20.02]. Available at: https://njt.hu/jogszabaly/2011-190-00-00.
Paksi, B., and Demetrovics, Z.. Drogprevenció És Egészségfejlesztés Az Iskolában [Drogprevention and health promotion at school]. Budapest: L’Harmattan (2011).
Paksi, B., Veroszta, Z., Schmidt, A., Magi, A., Vörös, A., Endrődi-Kovács, V., et al. Pedagógus-Pálya-Motiváció: Egy Kutatás Eredményei. Budapest: Oktatási Hivatal (2015). Available at: https://viselkedeskutato.hu/index.php?option=com_attachments&task=download&id=53&lang=hu.
Paulus, F. W., Ohmann, S., von Gontard, A., and Popow, C. (2018). Internet gaming disorder in children and adolescents: a systematic review. Dev. Med. Child Neurol. 60, 645–659. doi: 10.1111/dmcn.13754
Payne, A. A. (2009). Do predictors of the implementation quality of school-based prevention programs differ by program type? Prev. Sci. 10, 151–167. doi: 10.1007/s11121-008-0117-6
Payne, A. A., Gottfredson, D. C., and Gottfredson, G. D. (2006). School predictors of the intensity of implementation of school-based prevention programs: results from a National Study. Prev. Sci. 7, 225–237. doi: 10.1007/s11121-006-0029-2
Peeters, M., Koning, I., and van den Eijnden, R. (2018). Predicting internet gaming disorder symptoms in young adolescents: a one-year follow-up study. Comput. Hum. Behav. 80, 255–261. doi: 10.1016/j.chb.2017.11.008
Pereira, A. P. D., and Sanchez, Z. M. (2018). Drug use prevention: factors associated with program implementation in Brazilian urban schools. BMC Public Health 18:334. doi: 10.1186/s12889-018-5242-y
Pulimeno, M., Piscitelli, P., Colazzo, S., Colao, A., and Miani, A. (2020). School as ideal setting to promote health and wellbeing among young people. Health Promot. Perspect. 10, 316–324. doi: 10.34172/hpp.2020.50
Robertson, T. W., Yan, Z., and Rapoza, K. A. (2018). Is resilience a protective factor of internet addiction? Comput. Hum. Behav. 78, 255–260. doi: 10.1016/j.chb.2017.09.027
Rohrbach, L. A., Graham, J. W., and Hansen, W. B. (1993). Diffusion of a school-based substance abuse prevention program: predictors of program implementation. Prev. Med. 22, 237–260. doi: 10.1006/pmed.1993.1020
Scholaro Database . Education system in Hungary (Accessed 2023 28.02). Available at: https://www.scholaro.com/db/countries/hungary/education-system.
Silins, E., Horwood, L. J., Patton, G. C., Fergusson, D. M., Olsson, C. A., Hutchinson, D. M., et al. (2014). Young adult sequelae of adolescent Cannabis use: an integrative analysis. Lancet Psychiatry 1, 286–293. doi: 10.1016/s2215-0366(14)70307-4
Sohn, S. Y., Rees, P., Wildridge, B., Kalk, N. J., and Carter, B. (2019). Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: a systematic review, Meta-analysis and grade of the evidence. BMC Psychiatry 19:356. doi: 10.1186/s12888-019-2350-x
Spanemberg, L., Salum, G. A., and Bado, P. (2020). How can schools be integrated in promoting well-being, preventing mental health problems and averting substance-use disorders in urban populations? Curr. Opin. Psychiatry 33, 255–263. doi: 10.1097/yco.0000000000000591
Throuvala, M. A., Griffiths, M. D., Rennoldson, M., and Kuss, D. J. (2019). School-based prevention for adolescent internet addiction: prevention is the key. A systematic literature review. Curr. Neuropharmacol 17, 507–525. doi: 10.2174/1570159x16666180813153806
Turhan, A., Onrust, S. A., ten Klooster, P. M., and Pieterse, M. E. (2017). A school-based Programme for tobacco and alcohol prevention in special education: effectiveness of the modified ‘healthy school and Drugs' intervention and moderation by school subtype. Addiction 112, 533–543. doi: 10.1111/add.13672
United Nations Office on Drugs and Crime and the World Health Organization . (2018). International Standards on Drug Use Prevention, Second updated edition. Vienna: United Nations Office on Drugs and Crime and the World Health Organization.
van den Eijnden, R., Koning, I., Doornwaard, S., van Gurp, F., and Ter Bogt, T. (2018). The impact of heavy and disordered use of games and social media on Adolescents' psychological, social, and school functioning. J. Behav. Addict. 7, 697–706. doi: 10.1556/2006.7.2018.65
Vannucci, A., Simpson, E. G., Gagnon, S., and Ohannessian, C. M. (2020). Social media use and risky behaviors in adolescents: a Meta-analysis. J. Adolesc. 79, 258–274. doi: 10.1016/j.adolescence.2020.01.014
Wartberg, L., Zieglmeier, M., and Kammerl, R. (2021). An empirical exploration of longitudinal predictors for problematic internet use and problematic gaming behavior. Psychol. Rep. 124, 543–554. doi: 10.1177/0033294120913488
Weinstein, A., and Lejoyeux, M. (2010). Internet addiction or excessive internet use. Am. J. Drug Alcohol Abuse 36, 277–283. doi: 10.3109/00952990.2010.491880
Wiese, A. L., Sease, T. B., Joseph, E. D., Becan, J. E., Knight, K., and Knight, D. K. (2023). Avoidance self-efficacy: personal indicators of risky sex and substance use among at-risk youth. Child Youth Serv. Rev. 147:106846. doi: 10.1016/j.childyouth.2023.106846
World Health Organization and United Nations Educational Scientific and Cultural Organization . Making every school a health-promoting school: global standards and indicators for health-promoting schools and systems. Geneva (2021).
Keywords: universal addiction prevention, mental health, school-based health promotion, implementation, teachers, policy
Citation: Árva D, Vokó Z, Sápi M, Cselkó Z and Rákosy Z (2024) The influence of institutional characteristics on implementing school-based universal addiction prevention: a Hungarian mixed-methods nationwide study on the state of implementation, barriers, and facilitators. Front. Educ. 8:1240909. doi: 10.3389/feduc.2023.1240909
Edited by:
Douglas F. Kauffman, Medical University of the Americas – Nevis, United StatesReviewed by:
Laura Nabors, University of Cincinnati, United States Kit-Aun Tan, Universiti Putra Malaysia, MalaysiaCopyright © 2024 Árva, Vokó, Sápi, Cselkó and Rákosy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zsuzsa Rákosy, enN1enNhLnJha29zeUBhb2sucHRlLmh1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.