 Marianne Rorije
Marianne Rorije Saskia Damen
Saskia Damen Marleen J. Janssen
Marleen J. Janssen Alexander Minnaert
Alexander Minnaert- 1Department of Inclusive and Special Needs Education, Faculty of Behavioral and Social Sciences, University of Groningen, Groningen, Netherlands
- 2Royal Kentalis, Kentalis Academy, Utrecht, Netherlands
This systematic review revealed how children and youths with congenital deafblindness (CDB) exhibit autonomy characteristics and how caregivers perform autonomy support, which Erikson described as part of the first three stages of psychosocial development. This review comprises 22 studies that explicitly addressed one or more autonomy characteristics or autonomy support tasks. The results demonstrated that children and youths with CDB exhibited most characteristics of Erikson’s first stage (e.g., explorative behavior in their nearby environment and with objects within reach) and caregivers predominantly fulfilled autonomy tasks in the first stage (e.g., being present and near the child). In addition, children and youths with CDB exhibited independent acts at the second stage, although these were often limited to asking for or refusing concrete objects in the here-and-now situation. The limited degree to which the children with CDB exhibited autonomy characteristics from the second and third stages seems to co-occur with their struggle to develop symbolic communication. Additionally, the review revealed that caregivers supported autonomy by remaining present and nearby, even when autonomy support tasks from the second and third stages might be more appropriate in supporting the autonomy of children and youths with CDB (e.g., the second stage’s autonomy support task to balance between offering the child protection and encouragement, and the third stage’s task to support the child in taking initiative and setting goals). We recommend the use of a longitudinal video-feedback intervention that both supports the children’s and youths symbolic communication skills and supports caregivers in finding a balance between being present and nearby and fostering the autonomy characteristics of children and youths with CDB.
1. Introduction
Autonomy refers to the experience of acting with a sense of choice, volition, and room for self-determination (Reis et al., 2000; Ryan and Deci, 2000; Deci et al., 2009). An autonomous individual can exert influence and has control in their everyday situations (Barron, 2001). The development of autonomy is fundamental during childhood and an evident psychosocial task in adolescence (Van Petegem et al., 2019) to safeguard a person’s well-being and smooth development.
Children and youths with congenital deafblindness (CDB), who encounter a combination of visual and hearing disabilities from birth or before the onset of language development (Dammeyer, 2012), have a typical psychological need for autonomy, just like all people. However, their teachers have expressed difficulties and feelings of incompetence in supporting this need (Haakma, 2015). Haakma et al. (2017a) found a lack of autonomy support among teachers of youths with CDB, possibly related to time restraints and overprotectiveness. Due to their impairments, children and youths with CDB are relatively more dependent on their parents’ or caregivers’ stimulation to explore and be active (Marks, 1998). A potential risk of this greater dependency is that parents or caregivers may offer too much support, even when it is unnecessary. This may result in a lack of autonomous motivation and passivity in the child with CDB and, in the long run, culminate in learned helplessness (Marks, 1998). Moreover, autonomy skills are essential for further social development (Bruce et al., 2016). Altogether, there is a need for research on what is known about autonomy development and autonomy support among children and youths with CDB.
Hence, this study aimed to review the literature on how children and youths with CDB demonstrate autonomy. In addition, we aimed to obtain more in-depth knowledge and understanding of the autonomy support given to them, since we assume that autonomy is an integrated concept and is not entirely self-contained. Given that an individual’s environment should support their need for autonomy (Ryan and Deci, 2000) and children and youths with CDB often lack such support (Marks, 1998; Haakma, 2015), we also expected that examples of autonomy support performed by caregivers would provide a better understanding of how autonomy can be facilitated in children and youths with CDB.
Before analyzing the literature, we searched for a theoretical model that described autonomy development and autonomy support. Erikson’s eight stages of psychosocial development (Erikson, 1950, 1968) emerged as a suitable model (see Table 1) since it focuses on autonomy as a main developmental stage in psychosocial development and defines both developmental characteristics seen in the individual and support tasks for the social environment. Schlesinger (2000) applied Erikson’s theory to analyze the psychosocial development of individuals with deafness and found that caregivers struggle to provide appropriate autonomy support, most often due to communication and language barriers between the child and the caregivers. To our knowledge, the applicability of Erikson’s theory to the autonomy development of children and youths with CDB has yet to be examined.
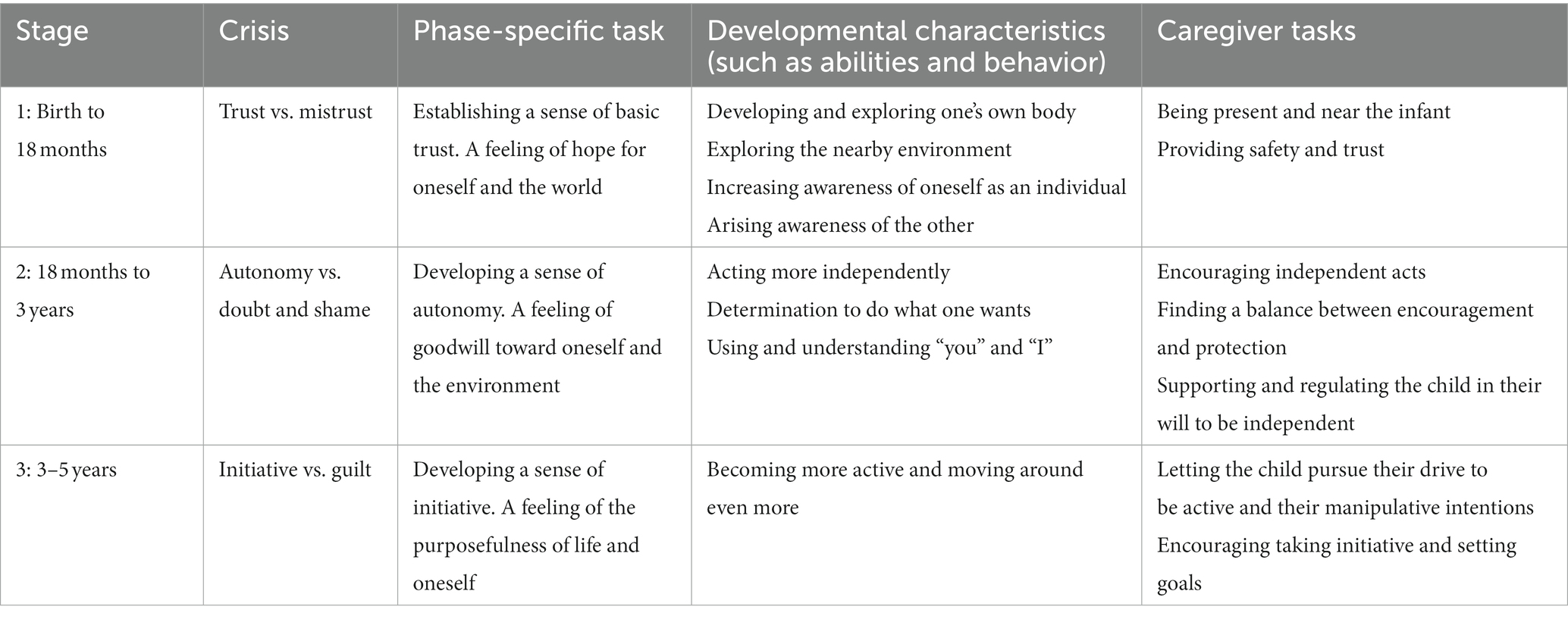
Table 1. Overview of developmental characteristics and caregiver tasks related to autonomy development in Erikson’s first three stages of psychosocial development.
Receiving appropriate support from the environment is one of Erikson’s key conditions for individuals to succeed at each of the eight stages of psychosocial development, also defined as the eight psychosocial crises (Erikson, 1968). In this context, a psychosocial “crisis” refers to a turning point in one’s life, a crucial period of increased vulnerability and profound growth (Erikson, 1968). To resolve the crisis, Erikson describes developmental characteristics for the individual at each stage and support tasks for people in the social environment, including caregivers. Erikson (1968) indicates that the stages are related and developmental characteristics can already be present in an earlier stage (i.e., on an unconscious level). According to Erikson, the outcome of one stage can have a negative or positive influence on the following stage.
We will present several aspects of Erikson’s first three stages related to autonomy development and autonomy support with the goal of understanding fundamental steps in the autonomy development of children and youths with CDB. See Table 1 for an overview of the developmental characteristics and caregiver tasks in the first three stages. To obtain a comprehensive understanding of autonomy development, we focused in depth on the second stage: “autonomy vs. doubt and shame.” In addition, we included feasible precursors of autonomy development described in the first stage: “trust vs. mistrust.” Erikson (1968) stated that this is a fundamental stage for succeeding in subsequent stages. Finally, we included the third stage—"initiative vs. guilt”—since we interpreted particular developmental characteristics and caregiver tasks in this stage as the continuation of autonomy development.
In Erikson’s first stage, an infant’s development of senses, body parts, and gross motor skills supports their individuation. The infant performs small actions, such as grasping their own feet or their caregiver’s hand. In this stage, the infant also experiences their ability to affect the immediate environment by expressing basic emotions (e.g., by crying or laughing), although the infant is still not conscious of this ability. Furthermore, the infant develops a drive to be active and explore the nearby environment and the infant becomes increasingly aware of “the other.” In this first stage, the caregivers’ tasks are to be present and nearby, to provide safety and trust.
During the second stage, a child becomes more conscious of acting independently as an autonomous creature. Erikson (1950) describes how the still highly dependent child begins to experience their autonomous will with the support of their environment. In this stage, the child prepares to stand more firmly on one’s own feet. Additionally, the child learns to categorize their world using concepts like “I” and “you” and “me” and “mine” (Erikson, 1968). Discovering the outer world helps the child develop even further and occurs in tandem with physical development: the child grows, becomes stronger, walks independently, and develops language (Erikson, 1968). A negative consequence of this stage can be that a child becomes determined to get what they want. In addition, the child might dominate and control their parents in areas where co-regulation is lacking (Erikson, 1968).
The caregivers’ task in the second stage is to encourage the child to “stand on his own feet” (Erikson, 1950, p. 252) with a feeling of independence and free will. At the same time, caregivers must help the child avoid misusing their willpower, which can lead to shame and early doubt (Erikson, 1968).
Whereas the first two stages emphasized obtaining one’s own will and resisting dependency, the third stage of initiative adds the quality of undertaking. The child becomes more active and the outside world becomes even more important, including increasing interactions with siblings and peers (Erikson, 1968). This state of being active dominates the child’s behavior during this stage; the child must establish a sense of initiative, which leads to a feeling of purposefulness in life. The caregivers should encourage the child to take initiative, set goals, and pursue these goals. Sometimes they must restrain their child slightly, but they should not act in a discouraging way (Erikson, 1950, 1968).
We used the developmental characteristics and caregiver tasks embedded in Erikson’s first three stages of psychosocial development as a framework to analyze the literature systematically to discover how children and youths with CDB exhibit these characteristics and caregivers perform their support tasks. The following two research questions guided the literature review: (1) How do children and youths with CDB exhibit autonomy characteristics at the first three stages of psychosocial development? and (2) How do caregivers perform autonomy support tasks at the first three stages of psychosocial development?
2. Methods
2.1. Data collection process
We conducted a systematic multi-step literature search to find the literature on autonomy development and autonomy support at the first three stages of psychosocial development in children and youths with CDB from birth up to age 23. We formulated two sets of keywords, described in Table 2: the first set of keywords refer to deafblindness and the second set of keywords refer to characteristics of Erikson’s first three stages of psychosocial development.

Table 2. Two sets of keywords.
The flow diagram in Figure 1 illustrates the steps we took to comply with the Preferred Reporting Items for Systematic Review and Meta-Analysis (the PRISMA 2020 statement; Page et al., 2021). We began the electronic search in ERIC, using a combination of the two sets of search terms to find relevant articles. We also searched the APA PsycINFO, Scopus, and Web of Science databases. The complete search (on articles published from January 2000 to August 12, 2023) resulted in 3984 papers. Initially, we conducted the search on articles published from January 2000 to August 2021; that resulted in 3286 papers, 20 of which we eventually included. In August 2023, we applied an identical multi-step literature search to articles published from August 13, 2021 to August 21, 2023; this extended search resulted in 698 papers, two of which were finally included. The flow diagram in Figure 1 illustrates the complete search (January 2000 to August 2023). The steps taken in this complete search will be explained in the upcoming paragraphs. For reasons of transparency and replication purposes, the separate flow diagrams of the two searches can be found in Supplementary Appendices A, B.
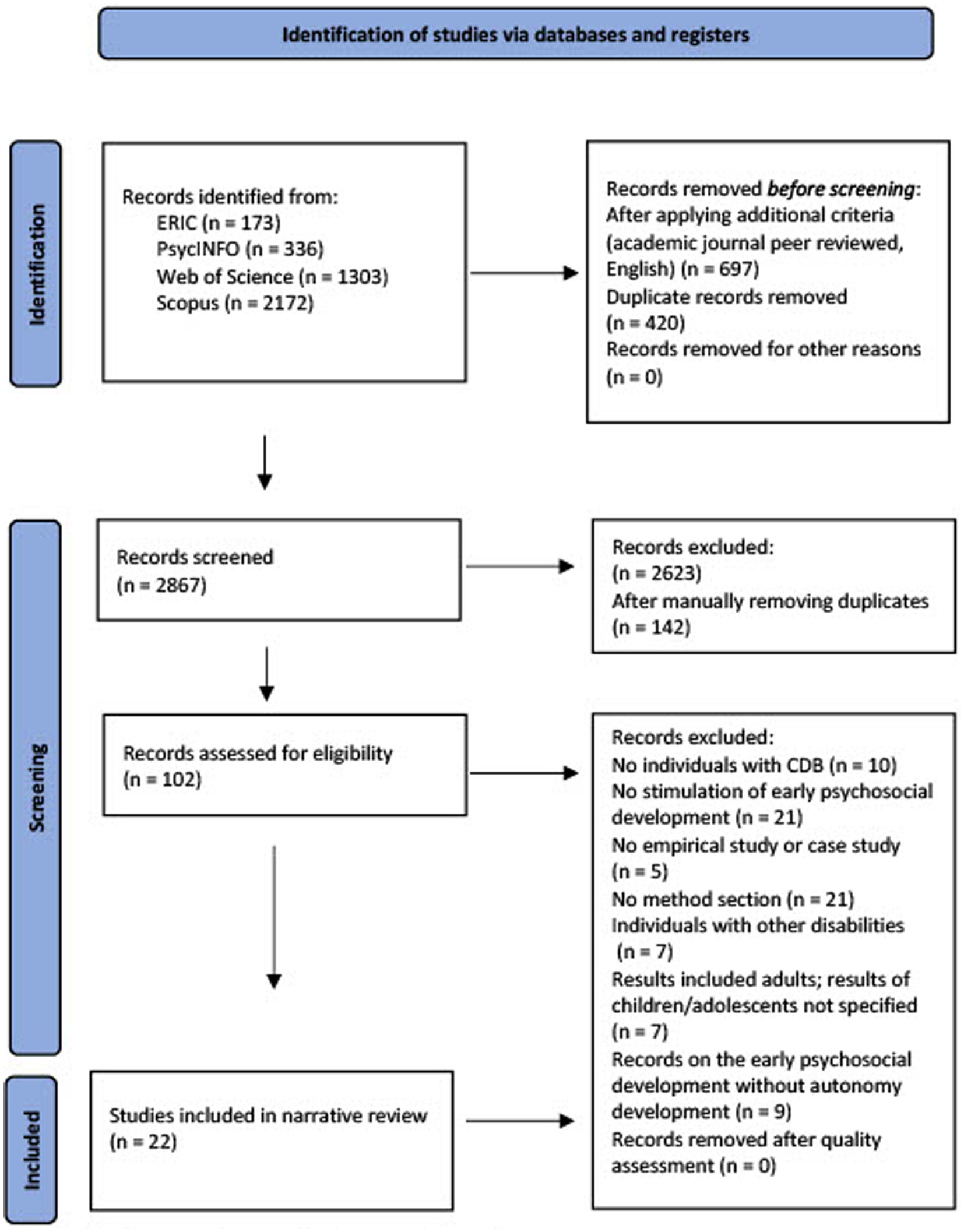
Figure 1. Flow diagram of study selection according to the PRISMA statement.
2.2. Inclusion and exclusion criteria
We then applied additional criteria to the 3,984 papers: they had to be published in a peer-reviewed academic journal and written in English. After applying these criteria and automatically removing duplicates, 2,867 papers remained. Further criteria were applied to the title and abstract: they needed to involve individuals with CDB or deafblindness during childhood and focus on their early psychosocial development, and the paper must have been published as an empirical study or case study. Applying these criteria led to the exclusion of 2,623 papers. After manually removing the duplicates from the remaining 244 papers, 102 papers remained.
Next, we applied several exclusion criteria to the full text of the papers. We excluded those with the following characteristics: (1) papers that did not describe the research method; (2) papers that addressed one or more characteristics of psychosocial development but did not explicitly link this to autonomy development; (3) papers that, in addition to children and youths with CDB, also addressed children and youths with other disabilities and neither explicitly addressed nor discussed, or did not relate the findings to children and youths with CDB; and (4) papers that included adults with CDB in their studies but did not explicitly mention the results of children and youths separately. Twenty-two papers remained for the next phase: i.e., quality assessment.
2.3. Quality assessment
We assessed the quality of the remaining 22 papers by applying QualSyst, a pragmatic systematic review tool to evaluate the quality of studies. According to Kmet et al. (2004) this tool is potentially suitable for a systematic review. The tool consists of two checklists for assessing quality: a 14-item checklist for quantitative studies with a maximum score of 28 points, and a 10-item checklist for qualitative studies with a maximum score of 20 points. For each item, the assessor indicates the extent to which the study met the quality criteria by choosing one of the following response options: “Yes, fully” (2 points), “Yes, partially” (1 point), or “No” (zero points). The checklist for quantitative studies also included “Not applicable” as an additional response option. Scores are displayed as percentages that indicate whether the methodological quality is strong (>80%), good (70–80%), adequate (50–70%), or poor (<50%). We used the following formula to calculate percentages: we divided the score by the maximum score, subtracted the items that were not applicable, and then multiplied that total by 100. To safeguard at least adequate methodological quality, we excluded studies with a final percentage of <50% from further analysis.
Application of the QualSyst tool by the first author resulted in two studies with an outcome of 60% and one studies with an outcome of 55%. The first and second authors discussed these three studies and decided not to exclude them. Thus, all 22 papers were included in the narrative review. Of those 22 studies, 13 were quantitative (with a mean score of 83%, assessed as strong). The mean score of the nine qualitative studies was 69%, assessed as adequate (Kmet et al., 2004).
2.4. Inter-rater reliability
All papers found in the database search (except duplicates) were fully assessed for appropriateness by the main reviewer (first author) using the previously mentioned criteria based on title and abstract. A second reviewer (a PhD candidate in special-needs education) independently assessed a random subset of 20% of the articles (n = 574) to verify that the inclusion and exclusion criteria had been applied accurately (Liberati et al., 2009).
Subsequently, an inter-rater reliability analysis was performed using Cohen’s Kappa statistic to determine consistency among the reviewers. There was substantial agreement, with a Kappa value of 0.64 (Fleiss, 1981) and a 96.5% agreement. An example of a discrepancy between the reviewers was the assessment of a paper about gestures by Bruce et al. (2007): the second reviewer rejected it because it seemed that the paper only focused on describing the type of gestures made by individuals with CDB, but the first author accepted the paper after noticing that the descriptions of gestures also included the intentions with which these were made, which revealed the participants’ requests and therefore their independent acts.
The first author analyzed the remaining 22 papers for narrative review and did a within-study analysis of relevant characteristics: measured variables related to autonomy development in Erikson’s first three stages, sample information, research design (including type of data, methodology, and study description), research aim, and results. The first author discussed the analysis with the second author until they reached consensus.
2.5. Data analysis
We examined how the 22 remaining papers described the developmental characteristics and caregiver tasks in Erikson’s first three stages (as formulated in Table 1). For each of Erikson’s characteristics and tasks, we then noted how the studies describe them (i.e., the corresponding “manifestations”). It is noteworthy that one developmental characteristic (“using and understanding ‘you’ and ‘I’”) and one caregiver task (“supporting and regulating the child in their will to be independent”) did not appear in the reviewed papers.
In addition, one manifestation that appeared in four studies—“expressing preferences”—was difficult to link to a specific child characteristic. We agreed that it is a manifestation of child characteristics at stage 2 (autonomy vs. doubt or shame), but we were unsure whether to consider it a manifestation of “acting more independently” or “determination to do what one wants.” The final decision was to assess this for each study separately. If a study emphasized the child’s determination in expressing their preferences, it was interpreted as a manifestation of “determination to do what one wants.” If the child’s determination was not described clearly enough, “expressing preferences” was interpreted as “acting more independently.”
Some of the caregiver strategies described in the studies as supporting the autonomy of children and youths with CDB could not be clearly linked to Erikson’s caregiver tasks. This was the case for autonomy-supportive teaching strategies, described in the study by Haakma et al. (2017b). Although these strategies did not appear to be exclusive manifestations of a specific caregiver task since they could be used for other purposes, the purpose for which these teacher strategies were applied in the included studies were related to one of Erikson’s caregiver tasks (“encouraging independent acts”) and was manifested as “fostering relevance” and “showing respect.”
For stage 1, we formulated two additional caregiver tasks: “supporting the child’s exploration” and “providing intensity regulation.” Erikson did not define these tasks for caregivers of typically developing children. Nevertheless, we could extract these caregiver tasks from seven studies and link them to stage 1 (establishing trust) and as precursors for autonomy development. We defined these tasks as important for caregivers of children and youths with CDB. Due to their impairments, children and youths with CDB need more help to explore the environment and they generally need more time for regulation and processing during exploration and interaction than typically developing children.
In the results, we distinguish between manifestations of developmental characteristics and caregiver tasks related to autonomy development or autonomy support (see Tables 3, 4). Furthermore, we distinguish between papers that describe observational contexts and studies of intervention contexts. An observational context demonstrates the naturally present skills or support, and an intervention context shows what is feasible when some intervention is provided. In addition, we classified the papers in the chronological order of Erikson’s three stages in each table. Tables 3, 4 focus on manifestations of developmental characteristics and manifestations of caregiver tasks and only include information about the papers. See Supplementary Appendices C, D for an extensive overview of the papers’ characteristics.
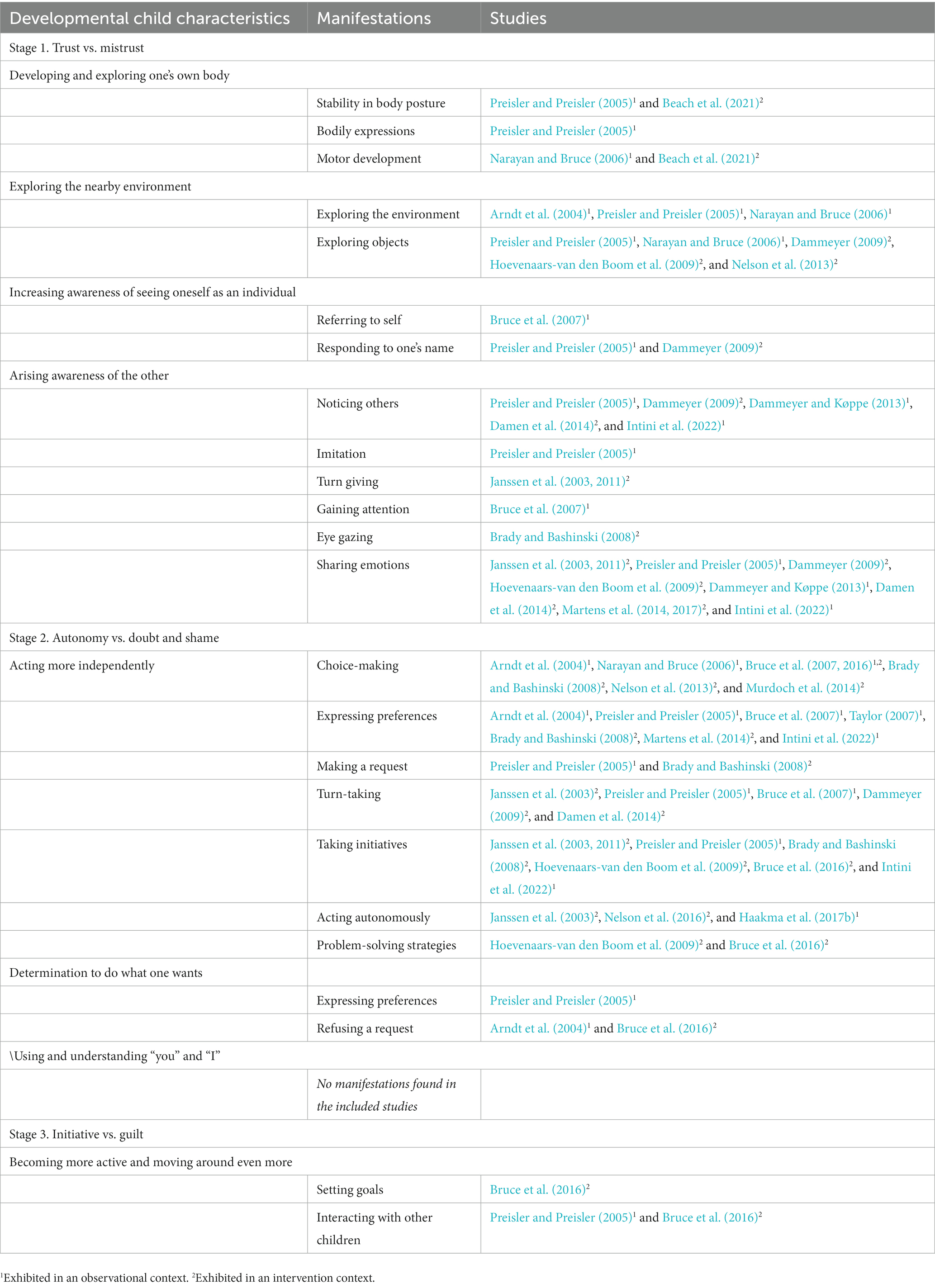
Table 3. Overview of developmental characteristics of Erikson’s first three stages, measured in children and youths with congenital deafblindness in the included studies.
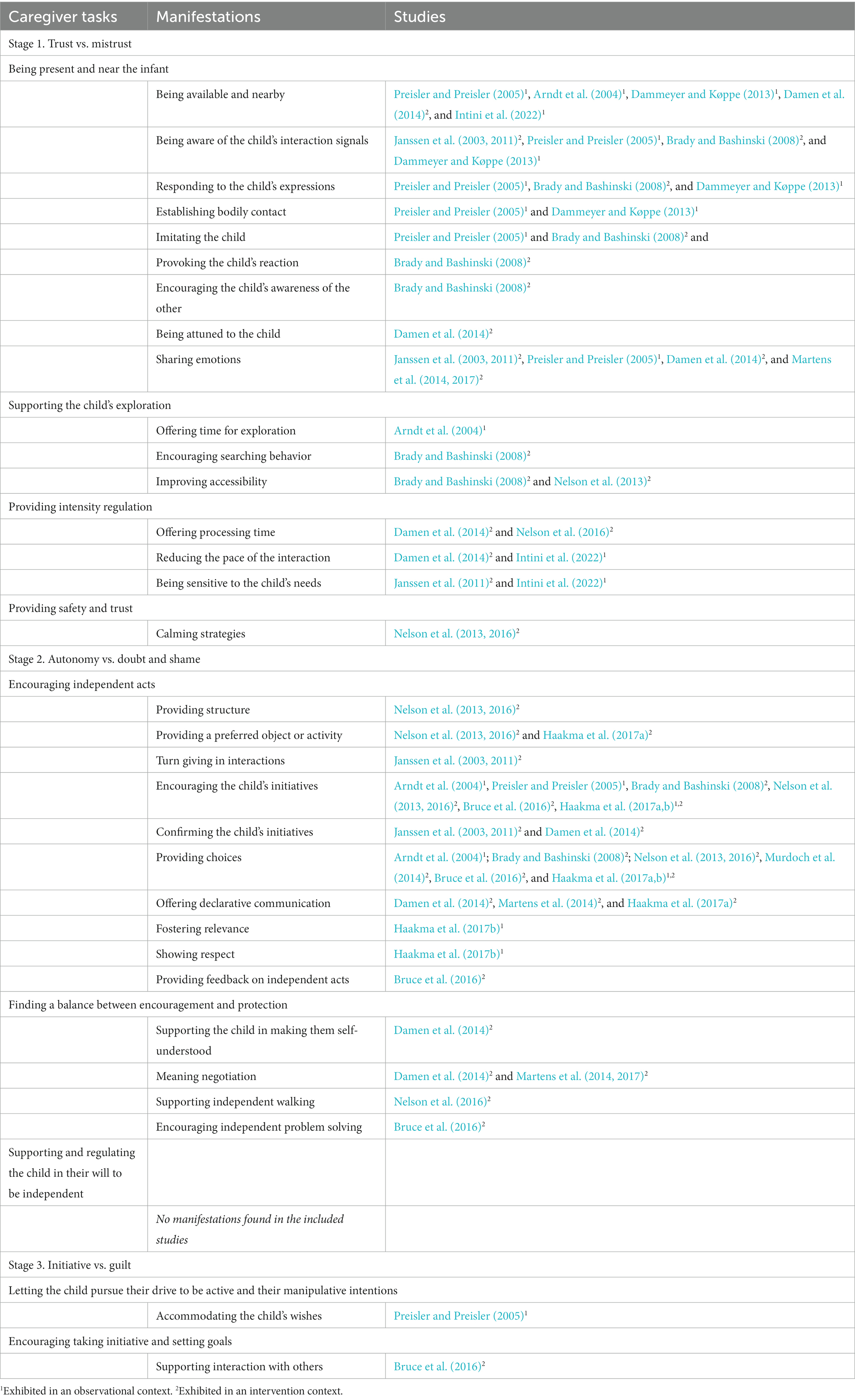
Table 4. Overview of caregiver tasks at Erikson’s first three stages, measured in children and youths with congenital deafblindness in the included studies.
3. Results
One hundred-seven children and youths with deafblindness were involved in the 22 included studies. The children and youths were between 6 months and 23 years, with a mean age of 7.5 years. Four studies referred to the participants as children and youths with deafblindness and did not specify whether it was acquired or congenital, although the onset was during childhood (Taylor, 2007; Nelson et al., 2013, 2016; Murdoch et al., 2014). The majority of the studies (i.e., 14 out of 22) were performed in an intervention context, including seven video-feedback interventions (Janssen et al., 2003, 2011; Damen et al., 2014; Martens et al., 2014, 2017; Bruce et al., 2016; Haakma et al., 2017a). The other eight studies were performed in an observational context: five used observations (Arndt et al., 2004; Preisler and Preisler, 2005; Bruce et al., 2007; Dammeyer and Køppe, 2013; Haakma et al., 2017b), and three used questionnaires or interviews for data collection (Narayan and Bruce, 2006; Taylor, 2007; Intini et al., 2022).
All developmental characteristics and caregiver tasks in Erikson’s first three stages, as described in Table 1, were found in the 22 included studies, except for the characteristic, “using and understanding ‘you’ and ‘I,’ and the caregiver task ‘supporting and regulating the child in their will to be independent.” We also found two additional caregiver tasks: “supporting the child’s exploration” and “providing intensity regulation.”
No studies specifically mentioned Erikson’s theory or referred directly to one of the three stages of psychosocial development. However, all the studies explicitly addressed one or more manifestations of developmental characteristics or caregiver tasks within one of the three stages related to autonomy development or autonomy support.
3.1. Developmental characteristics
3.1.1. Stage 1. Trust vs. mistrust
3.1.1.1. Developing and exploring one’s own body
This most fundamental developmental characteristic was described as “stability in body posture” (Preisler and Preisler, 2005; Beach et al., 2021), “bodily expressions” (Preisler and Preisler, 2005), and “motor development” (Narayan and Bruce, 2006; Beach et al., 2021). Preisler and Preisler (2005) described this characteristic in six children with CDB. Five children were filmed every 4 months for 2 years, starting at the age of 13 months; in another case study, parents recorded their child from the age of 6 months to 7 years. The children expressed themselves by using their bodies in interaction with others. Preisler also observed in a 13-month-old boy that more stability in body posture and the ability to sit and stand contributed to more interactions with the environment.
A study by Beach et al. (2021) compared the outcomes of a parental self-report questionnaire about their child’s motor development in the home environment. Twenty-eight parents of a child with CDB and 32 parents of a child without disabilities completed this questionnaire (all children aged 1–3 years). Beach et al. found that more children without disabilities than children with CDB exhibited motor milestones. Examples of milestones related to stability in their body posture are standing without support and “cruising” and gross motor milestones such as rolling over and crawling. Moreover, significant differences were found in the age of motor milestones; the children without disabilities achieved the milestones at an earlier age than the children with CDB. In a study by Narayan and Bruce (2006), teachers and parents of eight children with CDB (aged 4–12 years) also reported delays in the children’s gross motor skills, such as their abilities to use their arms and legs to move.
3.1.1.2. Exploring the nearby environment
Erikson’s second characteristic, “exploring the nearby environment,” was described as “exploring the environment” in the studies by Arndt et al. (2004), Preisler and Preisler (2005), and Narayan and Bruce (2006). In these studies, proximity senses (e.g., the olfactory sense and sense of touch) appeared to play an important role in the children’s exploration.
Preisler and Preisler (2005) observed another manifestation of “exploring the nearby environment”: “exploring objects.” During two years of observation, all six participants with CDB (aged 6 months to 3 years at the study’s onset) started to feel, taste, smell, and test the qualities and functions of objects in many ways.
Several other studies referred to “exploring objects.” Narayan and Bruce (2006) noted explorative behavior toward objects in eight children with CDB (aged 4–12 years). For example, they paid attention to several objects and preferred familiar objects to new ones. In a study by Hoevenaars-van den Boom et al. (2009), semi-standardized assessment revealed explorative behavior toward objects in five participants with CDB (aged 5–23 years). Their behavior was limited to the manipulation of objects with the support of the assessor. Dammeyer (2009) measured the manipulation of objects as well. This intervention study showed that five children with CDB (aged 5–8 years) manipulated objects more often when their cochlear implants (CIs) were switched on than when their CIs were switched off. Two intervention studies by Nelson et al. (2013, 2016) found an increase in “exploring objects” behavior among four students with deafblindness (aged 4–13 years) when one-to-one assistants supported this behavior during a three-part intervention package that was applied to improve their active participation.
3.1.1.3. Increasing awareness of oneself as an individual
This third developmental characteristic was described as “referring to self” and “responding to one’s name.” An observational study by Bruce et al. (2007) of seven children with CDB (aged 4–8 years) found that the children used a gesture for “Self” to label themselves, and one child also used this gesture when her name was called. Dammeyer (2009) described how the parents of a 5-year-old girl with CDB reported that 3 years after the CI was implanted, she turned around when she heard her name.
3.1.1.4. Emerging awareness of the other
The included studies described six manifestations of this fourth developmental characteristic: “noticing others,” “imitation,” “turn-giving,” “gaining attention,” “eye gazing,” and “sharing emotions.”
Preisler and Preisler (2005) observed the manifestation “noticing others” in four children with CDB. The children were between 6 months and 4 years of age during the observations. One child showed interest in other people, as he wanted to touch the fingers and hands of others. The other three children made sounds and smiled when they noticed their parents.
Dammeyer and Køppe (2013) observed that a 4-year-old child with CDB increased attention to their caregiver after the contact between child and caregiver was established. “Noticing others” was also found in Dammeyer (2009) study, which reported an increased awareness of others and increased social interaction after the CIs were switched on for five children (aged 5–8 years). Additionally, the parents of a 5-year-old girl and an 8-year-old boy mentioned that their children’s CIs improved their ability to notice others (Dammeyer, 2009). The effect study of the High Quality in Communication (HQC) video-feedback intervention by Damen et al. (2014) demonstrated increased intersubjective behaviors related to noticing others in interactions between a 19-year-old with CDB and his caregivers.
Intini et al. (2022) conducted parent interviews about several themes with three mothers and one parent couple of a child or youth with CDB (aged 4–23). They reported an example of “noticing others” and others’ feelings. The mother of an 8-year-old boy mentioned his ability to notice her and her feelings, for example, by asking her when she is sad. The study also described a mother’s experiences with her 4-year-old child’s ability to notice others. Where this was initially absent, it gradually developed, and the child can now notice and recognize others. The ability to notice others was also mentioned by another parent of a 23-year-old.
Preisler and Preisler (2005) also noted a second manifestation of “emerging awareness of the other” (i.e., “imitation”) in three children aged 16 months, 3 years, and 5 years. The children imitated their parents’ interactions in multiple ways, such as imitating the parents’ sounds, gestures, or body movements.
Janssen et al. (2003, 2011) observed a third manifestation (i.e., “turn-giving”) in effect studies of the Diagnostic Intervention Model (DIM)/Contact Program, a video-feedback intervention to foster harmonious interactions between children and youths with CDB and their caregivers. During the intervention, turn-giving improved in interactions between caregivers and five participants with CDB aged 3–19 years (Janssen et al., 2003) and between a 5-year-old participant and their caregiver (Janssen et al., 2011).
The fourth manifestation, “gaining attention,” was noted by Bruce et al. (2007) in the actions of seven children with CDB. The children gained their caregivers’ attention in different ways, such as reaching, directing or taking the caregiver’s hand, and touching the body.
The intervention study by Brady and Bashinski (2008) found examples of the fifth manifestation, “eye gazing.” This includes the children’s body orientation and searching behaviors with their hands toward objects or others. This was noted in five of the nine children with CDB (aged 3–7 years) at the end of the intervention. The study’s authors applied adapted prelinguistic milieu teaching (A-PMT) to improve the children’s intentional prelinguistic communication.
Several studies also noted occurrences of a sixth manifestation, “sharing emotions.” Dammeyer (2009) found that emotional response improved among five children with CDB (aged 5–8 years) after their CIs were switched on. In their observational study, Dammeyer and Køppe (2013) found an increased emotional response in a 4-year-old child with CDB. The authors associated the child’s increased emotional response with the child’s and teacher’s body movements (e.g., a short distance between the hands and more face-to-face orientation). The semi-standardized assessment by Hoevenaars-van den Boom et al. (2009) revealed reciprocity between children and youths with CDB and others. Finally, Intini et al. (2022) interviewed the mother of a 4-year-old child with CDB, who mentioned her son’s ability to share when he is upset or happy. However, it seems he cannot share when he is sad.
Two single-case experiments by Martens et al. (2014, 2017) found that two youths with CDB (aged 20 and 22 years) increased their sharing of emotions after their caregivers started participating in the video-feedback Intervention Model for Affective Involvement (IMAI). The IMAI-based intervention also resulted in improved expressions of the youths’ positive emotions (e.g., laughing, flapping with arms, and vocalizing joyful sounds).
Effect studies of two other interventions—the DIM/Contact Program (Janssen et al., 2003, 2011) and the High Quality in Communication (HQC) intervention (Damen et al., 2014)—found comparable results related to sharing emotions. During the phase of the effect study in which the DIM/Contact Program was offered, all seven participants (aged 3–19) improved their sharing of emotions (Janssen et al., 2003, 2011). When his caregivers were implementing the HQC intervention, the 19-year-old youth with CDB shared more emotions through facial expressions and by making signs of the emotion (Damen et al., 2014).
The final example of “sharing emotions” was seen in the study by Preisler and Preisler (2005). The study observed a 3-year-old child with CDB expressing emotions toward his mother.
3.1.2. Stage 2. Autonomy vs. doubt and shame
3.1.2.1. Acting more independently
The first developmental characteristic of the second stage is “acting more independently.” Seven manifestations of this were found in the included studies: “choice-making,” “expressing preferences,” “turn-taking,” “taking initiatives,” “acting autonomously,” “problem-solving strategies,” and “making a request.”
“Choice-making” was exhibited in multiple studies of children aged 4–12 years with deafblindness. Arndt et al. (2004) observed that a 12-year-old child with CDB could choose an activity when a choice was offered. The studies by Narayan and Bruce (2006), Brady and Bashinski (2008), and Nelson et al. (2013) described children’s selection response as tapping on an object. Additionally, a 4-year-old child with CDB was observed using eye gazing as a means of expressing choices (Nelson et al., 2013).
The teachers and parents in Narayan and Bruce (2006) study described even more choice-making behaviors, such as using pictures or a choice board, vocalizing, referring to objects, reaching toward an object, signing, and using symbols. However, three parents reported that they were sometimes uncertain whether their child chose something deliberately and whether the child understood the choice made.
Several studies observed choice-making behavior in relation to food. In the observational study by Bruce et al. (2007), one child with CDB was offered a choice of two snacks and he licked the bag of his choice. An intervention study by Murdoch et al. (2014) observed choice making during mealtime. The study showed that the choice determination of a 14-year-old with deafblindness improved when the fragrances of the meals were added to the choice-making process.
Finally, the intervention study by Bruce et al. (2016) focused on improving the self-determination skills of students with CDB. Three younger students (aged 6–10 years) learned to make toy choices during dyadic interaction sessions with the support of three older students with CDB.
Multiple studies (Bruce et al., 2007; Brady and Bashinski, 2008; Martens et al., 2014; Intini et al., 2022) observed another manifestation of acting more independently: “expressing preferences.” Several children (aged 3–8 years) and one youth (aged 22 years), all with CDB, protested or rejected an object or action, pushed the caregiver away, or became angry when they did not get what they want. The study by Intini et al. (2022) described another example of an 8-year-old boy with CDB. His mother mentioned his ability to express whether he wants to go his room or to play with his iPad.
Taylor (2007) also observed “expressing preferences.” The author, a teacher of a 14-year-old with deafblindness, consulted him about his likes and dislikes at school. He expressed his preferences for objects by choosing “like” or “not like” on a communicative speech device. He could not further explain his preference.
In contrast, a 15-year-old with CDB who joined a sports camp showed that she could express and explain her preferences (Arndt et al., 2004). Prior to running on the court, she discussed with her interpreter her desire to run continuously instead of taking breaks. Additionally, a boy with CDB (aged 3 years) in Preisler and Preisler (2005) study expressed his preferences by showing his mother how he wanted her to act. For example, he used facial expressions and body movements to show her how he wanted her to rock him back and forth.
“Turn-taking” as a manifestation of “acting more independently” was exhibited by one of the young children with CDB in Bruce et al. (2007) study. The child positioned the teacher’s hand in the receiving mode when she wanted to lead. Preisler and Preisler (2005) also found that the turn-taking of a child with CDB improved over time. Turn-taking was present during the first observation (when the child was 16 months old), although it was subtle and not always clear. At age 3, he took part in turn-taking games with his parents by making movements and vocalizations. Preisler observed comparable turn-taking behavior (i.e., movements and vocalizations) in another child, aged 3. Furthermore, the children in Dammeyer (2009) study (aged 5–8 years) demonstrated more turn-taking when their CIs were switched on than when they were switched off.
This behavior was also observed in youths. Turn-taking improved in the dyadic interaction between caregivers and one 19-year-old during the HQC intervention (Damen et al., 2014) and between caregivers and one child (aged 10 years) and one youth (aged 16 years) during the DIM/Contact Program (Janssen et al., 2003).
Preisler and Preisler (2005) observed children taking initiatives in several cases. For example, two children with CDB (aged 2 and 3 years) initiated contact with their parents (e.g., by repeated body movements). Unfortunately, the parents did not always notice their child’s actions as initiatives. In another of Preisler and Preisler (2005) observations, a child played peek-a-boo games with their mother and sibling, initially started by the mother. After a while, the child initiated the peek-a-boo game herself.
“Taking initiatives” was also measured as a result of several interventions. Two effect studies (Janssen et al., 2003, 2011) involving the DIM/Contact Program found that the initiatives of five children (aged 3–10 years) and two youths (aged 16 and 19 years) improved during the intervention. In the study by Bruce et al. (2016), three older students with CDB (aged 14–18 years) demonstrated more initiative during the intervention in which they participated in dyadic interaction sessions with younger students with CDB. Brady and Bashinski (2008) found that nine children (aged 3–7 years) increased their “taking initiatives” behavior during the A-PMT intervention: their initiated communication increased, and their prompted communication decreased. Finally, Hoevenaars-van den Boom et al. (2009) observed communicative initiatives made by five participants with CDB (aged 5–23 years).
“Acting autonomously” is another manifestation of “acting more independently.” For instance, the observational study by Haakma et al. (2017b) examined the engagement of four students with CDB (aged 12–17 years) while their teachers provided autonomy support. The students’ self-initiated actions were one of the observed characteristics of active positive engagement. Three of them exhibited active positive engagement when the teachers provided autonomy-supportive teaching, and the fourth exhibited this behavior twice, even at the moment when the teacher did not provide autonomy-supportive teaching.
Other studies also found improvements in “acting autonomously.” One 10-year-old child with CDB improved during the DIM/Contact Program as the child became more independent in dressing (Janssen et al., 2003). Intini et al. (2022) interviewed the mother of a 4-year-old child with CDB, who mentioned that her child could for example undress himself, but had difficulties with other autonomous acts. A 5-year-old child with deafblindness in another intervention study (Nelson et al., 2016) exhibited autonomous acts, such as exploring tactile books. That child also became more independent and confident in walking. Although he was physically able to walk independently during the baseline of the study, he waited for his one-to-one assistant to hold his hand. During the intervention, the assistant supported him in feeling the features of the environment so he could make an internal map of his surroundings.
Another manifestation of “acting more independently” is “problem-solving strategies.” For instance, five study participants with CDB (aged 5–23 years) asked for help during the semi-standardized assessment, which the authors interpreted as a problem-solving strategy (Hoevenaars-van den Boom et al., 2009). In another study, Bruce et al. (2016) observed “problem-solving strategies” in three older students with CDB (aged 14–18 years) who offered choices to three younger students and took the lead in the interactions.
“Acting more independently” was also demonstrated in the form of “making a request.” In Preisler and Preisler (2005) observation study, a 3-year-old child with CDB asked his mother for something to drink. “Making a request” was also observed in Brady and Bashinski (2008) intervention study, when eight of the nine children with CDB (aged 3–7 years) opened their palms to the caregiver to request a particular object. Four of the children exhibited this behavior at the beginning of the intervention, and eight children in that study exhibited this behavior at the end of the intervention.
3.1.2.2. Determination to do what one wants
The second developmental characteristic of stage 2 is “determination to do what one wants.” The studies described two manifestations of this: “expressing preferences” and “refusing a request.”
Preisler and Preisler (2005) described an example of “expressing preferences” in a 3-year-old boy with CDB who wanted to move in a certain way during playful interactions with his mother. He was persistent and discontent until the mother performed similar movements.
Two studies noted instances of “refusing a request.” The intervention study by Bruce et al. (2016) noted it in the actions of two younger students with CDB (aged 8 and 10 years). The children brought toys to the interaction session with two older students, and they stuck with those toys despite the older students’ attempts to shift their attention to another toy. Arndt et al. (2004) also described “refusing a request” in their observation study: during a sports camp, a 15-year-old with CDB refused to run when the instructor was standing in front of her and subsequently ignored the instructor.
3.1.2.3. Using and understanding “you” and “I”
This last developmental characteristic was not observed in any of the included studies.
3.1.3. Stage 3. Initiative vs. guilt
“Becoming more active and moving around even more” is the sole developmental characteristic in stage 3. Two manifestations were observed in the included studies: “interacting with other children” and “setting goals.”
The studies by Preisler and Preisler (2005) and Bruce et al. (2016) describe instances of “interacting with other children.” Bruce et al. (2016) observed that three older students with CDB (aged 14–18 years) interacted with each other while participating in an intervention that aimed to improve their social skills during dyadic interaction sessions with three younger students with CDB (aged 6–10 years). Preisler and Preisler (2005) described examples of children with CDB who showed interest in their siblings. For example, a 3-year-old child with CDB initiated contact with her siblings and wanted to play peek-a-boo with them.
“Setting goals” was observed by Bruce et al. (2016) when the three older students with CDB improved this characteristic during evaluation sessions with their teachers. They learned to set goals for interaction sessions with three younger students with CDB. The goals involved becoming more active in the interaction and guiding the younger students.
3.2. Caregiver tasks
3.2.1. Stage 1. Trust vs. mistrust
3.2.1.1. Being present and near the infant
This is the first caregiver task in stage 1. The included studies described nine manifestations of it: “being available and nearby,” “being aware of the child’s interaction signals,” “responding to the child’s expressions,” “establishing bodily contact,” “being aware of the child’s interaction signals,” “imitating the child,” “provoking the child’s reaction,” “encouraging the child’s awareness of the other,” “being attuned to the child,” and “sharing emotions.”
Several studies described the first manifestation, “being available and nearby.” For example, the observation study by Arndt et al. (2004) looked at the interpreters for four youths with CDB (aged 12–23 years). The interpreters’ availability and proximity appeared to be important in unfamiliar situations (e.g., new activities or meeting a less familiar sports instructor). The study by Intini et al. (2022) mentioned that parents were aware of the importance of being available and nearby. For example, the parents of a 4-year-old with CDB described that they were constantly nearby when their child had her therapy sessions. The effect study by Damen et al. (2014) also described this manifestation. During that study’s HQC intervention, three caregivers of a 19-year-old with CDB became more available and nearby as they changed their position toward him. This enabled them to have enduring tactile contact.
Preisler and Preisler (2005) study of parents of six children with CDB (aged 6 months to 3 years) found four manifestations of this caregiver task: “being available and nearby,” “being aware of the child’s interaction signals,” “responding to the child’s expressions,” and “establishing bodily contact.” The parents were available, nearby, and aware of their child’s interaction signals by watching and responding to their child’s body and sound expressions. However, the study described one example in which the manifestations appeared difficult to perform. There, the parents struggled to establish contact during the first year of the child’s life because they did not yet know that she had hearing loss and moderate visual impairment. Moreover, the parents believed that their daughter was not aware of them.
Dammeyer and Køppe (2013) observational study of body movements between a teacher and a 4-year-old child with CDB found the same four manifestations. The teacher initiated a free-play activity to establish contact by calling the child’s name, making eye contact, and touching his hands. When bodily contact was established, the teacher and the child responded to each other’s body movements, including face-to-face orientation and closeness of active body parts.
“Being aware of the child’s interaction signals” was also measured in two DIM/Contact Program effect studies (Janssen et al., 2003, 2011). In those studies, 15 caregivers received video-feedback coaching to improve their interaction with five children and youths with CDB (aged 3–19 years). In total, 15 dyads of a caregiver and a child or youth with CDB participated. The coaching increased the caregivers’ awareness of the youths’ interaction signals.
Caregivers of nine children with CDB (aged 3–7 years) in Brady and Bashinski (2008) intervention study performed the manifestations “being aware of the child’s interaction signals” and “responding to the child’s expressions.” During the A-PMT intervention, the caregivers became more sensitive and aware of the child’s interaction signals (e.g., the child’s searching behaviors) and were more responsive to the child’s expressions by immediately responding to the child’s acts.
The caregivers in that study (Brady and Bashinski, 2008) also performed another manifestation: “imitating the child.” The caregivers imitated the children’s motor and vocal acts to increase their intentional communication. Two parents in the study by Preisler and Preisler (2005) also imitated their children’s acts during the author’s observations.
The caregivers in Brady and Bashinski (2008) study also performed two more manifestations: “provoking the child’s reaction” and “encouraging the child’s awareness of the other.” In the first case, one caregiver performed an action the child found funny, paused for a while, and then repeated it to provoke a reaction. In the latter case, the caregiver aimed to encourage the child’s awareness of herself by placing a desired toy near her face. Then, the caregiver slowly increased the distance between herself and the toy, so the child shifted her attention from the toy to the caregiver.
Another manifestation—"being attuned to the child”—was described by Janssen et al. (2003, 2011) in two effect studies of the DIM/Contact Program. The caregivers made fewer initiatives and there were fewer simultaneous turns in seven dyads. According to Janssen et al. (2003, 2011), these changes suggest that the attunement improved. Additionally, Damen et al. (2014) describe improvements to “being attuned to the child” in three caregivers of a 19-year-old with CDB during the HQC intervention.
“Sharing emotions,” the final manifestation of “being present and near the infant,” was measured in five of the included studies. In Preisler and Preisler (2005) study, the parents of two children (aged 13 months and 3 years) performed “sharing emotions” during dyadic interactions with their children. Two studies by Janssen et al. (2003, 2011) found that the DIM/Contact Program improved mutual sharing of emotions in nine dyads.
Damen et al. (2014) also measured meaningful effects on the number of shared emotions between a youth with CDB and his three caregivers. During the HQC intervention, the caregivers worked on improving sharing emotions in a way that was accessible to him. Initially, when they noticed he was smiling, they replied by smiling. However, he was unaware of this since he was blind. Therefore, the communication partners practiced sharing emotions tactilely, using tactile signs and body touch.
“Sharing emotions” also improved through the IMAI-based intervention, according to Martens et al. (2014, 2017). Both studies found positive effects on affective involvement, including the sharing of positive emotions, between caregivers and two youths with CDB (aged 20 and 22 years) when caregivers applied several strategies to affirm positive expressions and to share positive and negative emotions (e.g., by co-actively imitating the youths’ movements). The caregivers in both these studies mentioned that affective involvement was easy to implement. Furthermore, the caregivers in the 2014 study indicated that sharing positive emotions was easier than sharing negative emotions.
3.2.1.2. Supporting the child’s exploration
The second caregiver task of stage 1 is “supporting the child’s exploration.” Three manifestations of this were found in the included studies: “offering time for exploration,” “encouraging searching behavior,” and “improving accessibility.”
In their observation study, Arndt et al. (2004) described “offering time for exploration.” Before the start of a new sports activity they observed, interpreters provided exploration time to two participants with CDB (aged 12 and 23 years), such as letting them explore the sports equipment.
During the A-PMT intervention (Brady and Bashinski, 2008), caregivers performed “encouraging searching behavior.” For example, they provided an object to one of the children with CDB (aged 3–7 years) who required the caregiver’s help. The caregiver gradually increased the distance from the child, so the child needed to reach out to the caregiver. The manifestation “improving accessibility” was also seen during the A-PMT intervention, as the caregivers made the activities more tactile.
Nelson et al. (2013) also observed “improving accessibility” by the caregivers of two children with deafblindness (aged 4 and 6 years). They changed the activities, so the children had more space and opportunity to explore (e.g., adjusting the child’s wheelchair made the child more able to touch the activity materials).
3.2.1.3. Providing intensity regulation
This third caregiver task of stage 1 was performed in the form of three manifestations: “offering processing time,” “reducing the pace of the interaction,” and “being sensitive to the child’s needs.”
The caregivers in the intervention study by Nelson et al. (2016) offered a 5-year-old child with CDB breaks during the activity, which the authors interpreted as an example of “offering processing time.” The effect study by Damen et al. (2014) also provided examples of “offering processing time” and “reducing the pace of the interaction.” During the HQC intervention, the caregivers gave a 19-year-old more time to process and respond to their gestures. The caregivers also decreased the speed of their gestures.
The interviews conducted by Intini et al. (2022) included a mother who reduced the interaction pace by giving her 4-year-old child with CDB all the time she needed. The interviews also provided an example of “being sensitive to the child’s needs.” Another mother mentioned that if needed, she tries to find steps to break down the process of what her 8-year-old is doing.
The caregiver in Janssen et al. (2011) effect study on the DIM/Contact Program was also observed “offering processing time” and “being sensitive to the child’s needs.” The 5-year-old child with CDB demonstrated behaviors such as picking at his sweater or rubbing his legs. These behaviors were interpreted as the child’s way of regulating the intensity of the interaction with the caregiver. During the intervention, the caregiver became more aware of and sensitive to these behaviors and offered time for regulation.
3.2.1.4. Providing safety and trust
One manifestation of this final caregiver task of stage 1 was observed in the intervention studies by Nelson et al. (2013, 2016): “calming strategies.” The assistants applied multiple strategies to soothe the four students with deafblindness (aged 4–13 years) during school activities. The strategies included giving hugs, stroking the head or arms, or offering comfort items like a vibrating pillow. The strategies appeared to help the children continue the activity. In the 2016 study by Nelson et al., calming strategies were needed less often when the child developed more self-regulation and participated more actively.
3.2.2. Stage 2. Autonomy vs. doubt and shame
This second stage includes three caregiver tasks: “encouraging independent acts,” “finding a balance between encouragement and protection,” and “supporting and regulating the child in their will to be independent.” The included studies described observations of the first two tasks, but no observations of the third task.
3.2.2.1. Encouraging independent acts
The included studies described 10 manifestations of this task: “providing structure,” “providing a preferred object or activity,” “turn-giving in interactions,” “encouraging the child’s initiatives,” “confirming the child’s initiatives,” “providing choices,” “offering declarative communication,” “fostering relevance,” “showing respect,” and “providing feedback on independent acts.”
In two studies by Nelson et al. (2013, 2016) “providing structure” was performed by the assistants of four students (aged 4–13 years) as an anticipatory strategy. The assistants provided structure by using a calendar or picture schedule of the activities and supported the students’ participation by creating meaningful, enjoyable, and interactive activities. This last strategy was interpreted as an example of the manifestation “providing a preferred object or activity.”
Brady and Bashinski (2008) also described this manifestation in their study. During the intervention period, the caregivers provided desired objects or actions to nine children with CDB (aged 3–7 years). The needs-supportive behavior intervention study by Haakma et al. (2017a) examined teachers’ autonomy-supportive teaching in four students with CDB (aged 12–17 years). Providing interesting learning activities was one of the teachers’ autonomy-supportive strategies, which the authors interpreted as another example of “providing a preferred object of activity.”
In their effect studies, Janssen et al. (2003, 2011) measured “turn-giving in interactions.” After participating in the DIM/Contact Program, the caregivers of four children and youths with CDB demonstrated increased turn-giving, which positively affected the children’s and youths’ interactive behaviors.
We also interpreted “encouraging the child’s initiatives” as another manifestation of “encouraging independent acts.” Interpreters in the observation study by Arndt et al. (2004) performed this manifestation by providing communication breaks to four participants with CDB (aged 12–23 years) during continuous sports activities. Continuous activities, such as tandem biking, are activities in which both hands are engaged and therefore unsuitable for manual or tactile communication. Offering communication breaks gave the participants an opportunity to ask or say something to the interpreter using sign language.
The teachers in the intervention study by Bruce et al. (2016) also performed “encouraging the child’s initiatives” as they prompted three older students with CDB in their dyadic interaction with three younger students. The teachers gave the older ones prompts for opening and closing the interaction.
Brady and Bashinski (2008) and Nelson et al. (2013, 2016) found comparable results in their intervention studies. All three studies described caregivers who encouraged the child’s initiatives by prompting (Brady and Bashinski, 2008) or providing touch cues as anticipatory strategies (Nelson et al., 2013, 2016). Furthermore, Nelson et al. (2016) observed that a 5-year-old child with deafblindness took more initiatives to explore objects as the assistant offered more hand-under-hand support and decreased hand-over-hand manipulation during activities.
The descriptive study by Haakma et al. (2017b) found that teachers encouraged the initiatives of students with CDB, which positively affected their engagement. Haakma et al. (2017a) also noticed this manifestation in the intervention study.
“Confirming the child’s initiatives” was interpreted as another manifestation of “encouraging independent acts.” It was performed by caregivers who participated in the DIM/Contact Program (Janssen et al., 2003, 2011) and the HQC intervention (Damen et al., 2014).
Another manifestation, “providing choices,” was observed in several studies. Arndt et al. (2004) observed it in the behavior of interpreters for participants with CDB during a sports camp. For example, one interpreter offered a 12-year-old with CDB the choice between doing the activity alone or with the interpreter. In the intervention study by Bruce et al. (2016), older students offered a choice of toys to younger students with CDB (aged 6–10 years). “Providing choices” was also observed in Brady and Bashinski (2008) intervention study involving caregivers of nine children with CDB. For example, the caregiver presented two preferred objects to a child, placed the child’s hand on the object, pulled the object out of reach, maintained contact, and asked in sign language, “Which one do you want?”
In addition, “providing choices” was observed in two studies by Haakma et al. (2017a,b). It was used as an autonomy-supportive teaching strategy applied by four teachers of students with CDB. One teacher in the observation study (Haakma et al., 2017b) offered choices to a 15-year-old student during a computer activity, by letting her choose words with a sign language dictionary program. A teacher in the intervention study (Haakma et al., 2017a) created a new reference object method where all the objects hung on a coat rack. This gave the 13-year-old student a better overview of activities and made choice-making easier.
In the study by Murdoch et al. (2014), fragrances were added to meals to support the mealtime choices of a 14-year-old with deafblindness. “Providing choices” also appeared as an anticipatory strategy in studies by Nelson et al. (2013, 2016) as part of a three-part intervention package that was evaluated. Four one-to-one assistants provided choices to four students with deafblindness, such as letting them choose between two tactile activities to make it more meaningful.
“Offering declarative communication”—another manifestation of “encouraging independent acts”—was found in several studies. Haakma et al. (2017a) mentioned communicating in an open manner to four students with CDB as an example of an autonomy-supportive strategy, which this study interpreted as “offering declarative communication.” Damen et al. (2014) effect study of the HQC intervention found improvement in “offering declarative communication” between a 19-year-old with CDB and his caregivers. The caregivers applied strategies that supported him to talk about more topics, including those that happened in the past. Similar strategies were observed in the effect study of the IMAI-based intervention (Martens et al., 2014). There, the caregivers of a 22-year-old with CDB created opportunities to communicate about interests and feelings through sensory play. However, caregivers rated this as rather difficult to implement.
Two other manifestations of “encouraging independent acts” were found in Haakma et al. (2017b) observation study: “fostering relevance” and “showing respect.” In the publication of the study, no concrete examples were given of how this was offered.
Finally, Bruce et al. (2016) observed “providing feedback on independent acts,” another manifestation of “encouraging independent acts,” during feedback sessions between three older students with CDB and their teachers. After each of the six dyadic interaction sessions, older students received feedback from their teachers to improve their interaction with the three younger students with CDB. In the next dyadic interaction session, they had the opportunity to apply one of the suggestions discussed in the feedback sessions.
3.2.2.2. Finding a balance between encouragement and protection
We found four manifestations for the second caregiver task of stage 2: “finding a balance between encouragement and protection.” The manifestations were “supporting the child in making them self-understood,” “meaning negotiation,” “supporting independent walking,” and “encouraging independent problem-solving.”
“Supporting the child in making them self-understood” was observed in Damen et al. (2014) effect study of the HQC intervention. Three caregivers applied numerous strategies to improve meaning-making with the youth. One caregiver started checking whether the 19-year-old with CDB felt understood by asking YES/NO? in sign language, followed by immediately sharing her interpretation of what he seemed to have tried to say. By responding to the YES/NO question, he appeared to be able to clarify whether the caregiver understood him correctly.
Caregivers in the effect studies of the HQC intervention (Damen et al., 2014) and the IMAI-based intervention (Martens et al., 2014, 2017) performed another manifestation: “meaning negotiation.” The studies defined “meaning negotiation” as the caregiver’s attempt to obtain more information about the meaning and intention of the signs expressed by the youth with CDB. The caregivers also offered the youth the opportunity to respond. Damen et al. (2014) found improvement in meaning negotiation. Martens et al. (2014, 2017) did not describe the results related to meaning negotiation for the caregivers and two youths with CDB. The caregivers did indicate that they found meaning negation rather difficult to implement.
Nelson et al. (2016) described another manifestation of “finding a balance between encouragement and protection”: “supporting independent walking.” In their intervention study, the assistant supported the independent walking of a 5-year-old child with deafblindness by attaching a string to the child’s cane. Through the string, the child could feel the assistant’s presence and practice walking more independently.
The teachers participating in Bruce et al. (2016) intervention study performed the final manifestation: “encouraging independent problem-solving.” The older students with CDB could contact the teachers for help during the interaction sessions with the younger students with CDB. The teachers were nearby but outside the interaction space to encourage the older students’ independent problem-solving skills. The teachers placed mats on their sides to mark the interaction space more clearly and this worked as a barrier to easily seeking help.
3.2.2.3. Supporting and regulating the child in their will to be independent
This last caregiver task of the second stage was not observed in any of the included studies.
3.2.3. Stage 3. Initiative vs. guilt
The third stage consists of two caregiver tasks: “letting the child pursue their drive to be active and their manipulative intentions” and “encouraging taking initiatives and setting goals.” The first task was observed as “accommodating to the child’s wishes” in one of Preisler and Preisler (2005) case studies. For example, the mother and her 3-year-old child with CDB were in a situation in which they had different wishes. The child wanted to watch a television program, and his mother wanted to play with him. Finally, after 25 min of interaction, the child and his mother came to a solution: they sat next to each other and watched the television program together.
“Supporting interaction with others,” i.e., a manifestation of the second task (“encouraging taking initiatives and setting goals”), was seen in the intervention study by Bruce et al. (2016). The teachers supported the interaction between the older and younger students with CDB and the interaction among the older ones during feedback sessions.
4. Discussion
Using the perspective of Erikson’s first three stages of psychosocial development, we aimed to systematically analyze the scientific literature on how children and youths with CDB exhibit characteristics of autonomy development and how caregivers perform autonomy support. We found a similar pattern for both the autonomy characteristics and the autonomy support tasks. Most autonomy characteristics and autonomy support tasks were found at the first two stages of psychosocial development, and the characteristics and tasks of the third stage were exhibited infrequently. In the next paragraphs, we will first answer the two research questions.
The first research question asks, “How do children and youths with CDB exhibit autonomy characteristics at the first three stages of psychosocial development?” In the first stage, in which precursors of autonomy development are seen, children and youths with CDB exhibited explorative behavior of their bodies. They also explored their environment and objects, but this was limited to their nearby environment and objects within reach. Additionally, children and youths with CDB showed an awareness of the other, for example, when they demonstrated turn-giving and shared their emotions in dyadic interactions. However, such other awareness was most often demonstrated in intervention studies and to a lesser extent in observational studies.
At the second stage, the core stage of autonomy development, our review revealed that children and youths with CDB exhibited independent acts, although these were often limited to asking for or refusing concrete objects. More complex autonomy characteristics, such as “determination to do what one wants,” and “using and understanding ‘you’ and ‘I’” were not exhibited (or less frequently so) in the included studies.
The second research question asks, “How do caregivers perform autonomy support tasks at the first three stages of psychosocial development?” In the first stage, caregivers supported the child’s autonomy predominantly by being present and near the child. We found two additional caregiver support tasks at this stage—"supporting the child’s exploration” and “providing intensity regulation”—that Erikson did not describe. In the second stage, caregivers performed autonomy support, most often in the form of supporting independent acts. In addition, the caregivers provoked independent acts from the children and youths with CDB by offering them prompts. When we looked at all the included studies together, we noticed that caregivers did not perform (or performed to a lesser extent) the more complex tasks of the second stage, such as “finding a balance between encouragement and protection” and “supporting and regulating the child in their will to be independent.” The findings will be further discussed in the following paragraphs.
At first glance, our review confirmed the reciprocity between the children’s and youths’ autonomy characteristics and the caregivers’ autonomy support tasks, as described by Erikson: children and youths with CDB mainly showed characteristics of the first two stages and caregivers supported these characteristics. However, it is unclear whether the limited support in the third stage meant that caregivers were more attuned to the child’s need for support at lower stages of autonomy development, or that children and youths with CDB could not fully exhibit or develop their autonomy characteristics at the highest stage because they lacked appropriate autonomy support from the caregivers. We suggest the latter, as it seems that caregivers found it difficult to shift from providing trust to supporting the full autonomy of children and youths with CDB. Caregivers appeared to frequently prompt independent acts and remained present and nearby, even in situations when the tasks from the subsequent stages would probably be more appropriate in supporting the autonomy of children with CDB who already performed independent acts. This assumption also aligns with the teacher and caregiver behavior observed in the studies by Marks (1998) and Haakma et al. (2017b). In these studies, caregivers were rather overprotective and lacked sufficient time to support the autonomy of children and youths with CDB.
Another explanation for the limited autonomy characteristics and limited support tasks at the third stage can be found when we consider the specific challenges children and youths with CDB and their caregivers encounter in social and communicative interactions. This is in line with the result of Schlesinger (2000) study of children with deafness, which showed how these children’s difficulties in communication negatively affected their autonomy development. Our review found that most children and youths with CDB were able to express their autonomy within the here-and-now situation, but they were not able to express their wishes beyond this situation. According to Bruce (2005), these difficulties are related to their challenges with “distancing,” i.e., the ability to distinguish themselves from others, distinguish themselves from objects, and distinguish objects from representation. Bruce (2005) states that caregivers can support an understanding of distancing in children and youths with CDB by using strategies like hand-under-hand guidance and exploration of objects.
In addition, children and youths with CDB may find it difficult to understand that they can express their wishes and opinions, which is a prerequisite to actions such as choice-making. Narayan and Bruce (2006) showed that making a meaningful choice can be difficult for these children as the parents participating in this study questioned whether their child with CDB understood the choices they made.
Only one of the included studies (Arndt et al., 2004) demonstrated higher levels of communication in children and youths with CDB that enabled them to express their autonomy beyond the current situation and, for example, explain why they wanted something. Most children and youths with CDB in the included studies did not exhibit symbolic communication: they expressed themselves through body movements with objects and communicated using their proximity senses, particularly their sense of touch. This level and type of pre-symbolic communication require caregivers to be near the children and sensitive to their children’s communication signals (Miles, 1997; Bruce, 2005); that explains why “being present and nearby” was a common support strategy described in the included studies and why the caregivers who participated in intervention studies used tactile approaches. Examples of such approaches are hand-under-hand support or tactile sharing of emotions. However, other caregivers expressed difficulty with using tactile interaction and communication approaches. In addition, some caregivers in the included studies found it difficult to interpret the children’s and youths’ communication signals, including autonomous initiatives. This may also lead the child or youth to attempt fewer initiatives.
Although we did not find the autonomy characteristic “using and understanding ‘you’ and ‘I’” in the included studies, Dammeyer (2009) showed that having a CI had a positive impact on the ability of children with CDB to see themselves as individuals and notice others. Specific challenges in the intersubjective communication development of children and youths with CDB may explain why the autonomy characteristic “using and understanding ‘you’ and ‘I’” was not found in the included studies. According to Damen et al. (2015) and Wolthuis et al. (2019), most children and youths with CDB encounter difficulties in exhibiting higher levels of “intersubjectivity” because of challenges in social interaction with other people. Intersubjectivity is a term used for “self-and-other awareness” of which “understanding ‘you’ and ‘I’” is a characteristic feature. Additionally, this autonomy characteristic can be considered part of symbolic communication, although it can emerge in children and youths with CDB who use pre-symbolic communication. Another explanation for the difficulty in “using and understanding ‘you’ and ‘I’” is found in Bruce (2005) finding that children and youths with CDB have difficulties understanding the concept of “distancing.”
In this review, we applied Erikson’s three stages of psychosocial development to describe how children and youths with CDB exhibited autonomy characteristics and caregivers performed autonomy support tasks. Therefore, it is worth discussing the applicability of Erikson’s framework to children and youths with CDB and their caregivers, especially as he established this framework to describe typically developing children and caregivers. Erikson describes how caregivers of typically developing children follow their child’s natural psychosocial development. A characteristic or skill occurs at a certain age, and subsequently, the parent performs behavior in favor of the child to further develop a specific task.
The descriptions of caregiver support we found in our review suggest that caregivers of children and youths with CDB need to be more supportive since the overall development of these children and youths occurs less spontaneously than that of typically developing children and youths. When we compared the descriptions of autonomy support provided by caregivers of children and youths with CDB at the first stage, we also discovered two additional caregiver tasks in five studies related to supporting these children’s and youths’ exploration and regulation. These additional tasks may be related to the way children and youths with deafblindness perceive the world. Due to their disabilities, they lack information about their environment and depend on what they can reach within their immediate vicinity (Aitken, 2000). Hence, children and youths with CDB need another person to support them in exploration, such as offering them sufficient exploration time (Janssen et al., 2012), and making the environment accessible (Miles, 1997). Using touch to obtain an overview of situations can be difficult and time-consuming (Dammeyer et al., 2015). Moreover, tactile information can be overwhelming (Costain, 2020), which can explain why they need a sensitive caregiver to notice when they need a break for regulation. Although children and youths with CDB need their caregivers to provide more active and specific autonomy support, in general, Erikson’s first three stages seem applicable to describing both the autonomy characteristics of children and youths with CDB and the autonomy support tasks of their caregivers.
4.1. Limitations and recommendations for future research
The first limitation of our study is that only one of the 22 included studies (Preisler and Preisler, 2005) was longitudinal and the others did not study changes in children’s and youths’ behavior over time in the short and long term. Therefore, our findings are limited to how children and youths with CDB exhibit autonomy characteristics at a specific age and do not provide insight into how autonomy develops in these children and youths.
Another limitation of our study is that the children and youths with CDB who exhibited the autonomy characteristics in the included studies had a mean age of 7.5 years, which was mostly older than the ages at which Erikson (1950, 1968) asserts that typically developing children develop these autonomy characteristics. These age differences make it challenging to compare the autonomy characteristics of children and youths with CDB to those of typically developing children and youths. However, the six children in the study by Preisler and Preisler (2005) had similar calendar ages as the typically developing children Erikson described, and three of those children (aged 3–4 years) exhibited characteristics of the third stage.
The methodological quality of some of the included studies is another limitation. We assessed the quality with the QualSyst tool (Kmet et al., 2004) and found an overall lower quality of the qualitative studies than that of the quantitative studies. Moreover, three qualitative studies were assessed with a score 60% (Arndt et al., 2004; Preisler and Preisler, 2005), and one study was assessed with 55% (Taylor, 2007), defined as adequate (50–70%), These studies, particularly those by Arndt et al. (2004) and Preisler and Preisler (2005), provided rich examples of developmental characteristics and caregiver support tasks. Within these studies, however, limited information was provided on the way data collection was carried out. This restricts replication of these studies and comparison of their results with other studies. Accordingly, the methodological quality of qualitative studies in this domain is a matter of concern.
Two other limitations concern the applicability of Erikson’s theory. First, although we found autonomy characteristics and autonomy support tasks related to the first three stages, none of the studies specifically mentioned Erikson’s theory of psychosocial development and only three studies explicitly focused on the autonomy of children and youths with CDB (Bruce et al., 2016; Haakma et al., 2017a,b). Since none of the studies specifically focused on applying Erikson’s theory, it is possible that the children and youths exhibited more autonomous skills and their caregivers more autonomy support than was described. Therefore, we cannot determine with complete certainty whether these behaviors were indeed not exhibited. Second, the caregiver tasks as formulated by Erikson are mainly descriptive and mostly follow the child, and these tasks have not always proved to be specific enough for caregivers of children and youths with CDB. Therefore, we had to attribute the child and caregiver variables measured in the included studies to developmental characteristics and caregiver tasks of the first three stages.
We conclude this study with recommendations for research and practice based on our findings. Our study revealed that children with CDB exhibit characteristics of autonomy and caregivers support this autonomy. However, we could not determine precisely how autonomy develops in these children and youths and how caregivers support their development, as Erikson described in the first three stages of psychosocial development. Thus, our first recommendation is to study the development of autonomy in children and youths with CDB over time.
Another recommendation concerns the application of Erikson’s theory. Based on our findings, some modifications would make this theory more suitable for studying autonomy and autonomy support in children and youths with CDB and their caregivers. Examples of modifications are the addition of the deafblind-specific caregiver tasks we found at the first stage and the description of deafblind-specific manifestations of autonomy characteristics and support tasks.
Our third recommendation also relates to the application of Erikson’s theory in practice. In line with Erikson’s assumptions, the autonomy characteristics and autonomy support tasks in stage 1 and the less complex characteristics and tasks in stage 2 remain important to succeed in further autonomy development. Thus, we recommend that caregivers of children and youths with CDB be present and nearby to provide safety and trust, support exploration and regulation, and support their independent acts. The review also identified what is needed to further develop the more complex autonomy characteristics of stages 2 and 3 through appropriate autonomy support from the caregivers at these stages. This autonomy support should comprise caregivers’ ability to balance between offering the child encouragement and protection, supporting and regulating the child’s independent will, letting the child be active, encouraging their initiative, and setting goals.
Another recommendation for practice is to strengthen autonomy development in children and youths with CDB by improving their communication skills, especially symbolic communication. Improving symbolic communication may support their expression of autonomy. In addition, we recommend strengthening caregivers’ autonomy support skills, as we found that caregivers experienced challenges in supporting the autonomy development of children and youths with CDB. Such challenges were also found in previous studies in the domain of communication.
To improve communication and autonomy development in children and youths with CDB and to strengthen the autonomy and communication support skills of their caregivers, we recommend developing and evaluating a longitudinal video-feedback (VF) intervention with this purpose, by means of a tactile approach. In previous studies, VF coaching enhanced caregivers’ skills in fostering communication with individuals with CDB (Damen et al., 2020). In VF interventions, the interaction between a caregiver and a child, student, or client is video recorded and subsequently analyzed by the caregiver and a professional coach or therapist. The aim of VF interventions is to improve the caregivers’ interaction skills by letting them reflect on their own behavior and observing how the caregiver’s behavior affects the child, student, or client (Fukkink, 2008; Damen et al., 2020). As far as we know, there are no VF interventions that focus on training and coaching caregivers in supporting symbolic communication and autonomy development in children and youths with CDB. More research into this area might pave the way to improve both the children’s and youths’ autonomy development and the provision of appropriate autonomy support by their caregivers.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
MR, SD, MJ, and AM contributed to conceptualization and design of the study. MR conducted the literature research, study selection process, and data collection. MR and SD conducted the analysis. MR worked on drafts of the manuscript with support of SD. MR wrote the manuscript with support provided first by SD, and second by AM and MJ. All authors contributed to the manuscript revision and read, and approved the submitted version.
Funding
This work was supported by ZonMw/InVision, grant number 94312003.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2023.1228905/full#supplementary-material
References
Aitken, S. (2000). “Understanding deafblindness” in Teaching children who are deafblind. Eds. M. Buultjens, C. Clark, J. T. Eyre and L. Pease (London, UK: David Fulton Publishers), 1–35.
Arndt, K., Lieberman, L. J., and Pucci, G. (2004). Communication during physical activity for youth who are deafblind: research to practice. Teach. Except. Child. Plus 1.
Barron, K. (2001). Autonomy in everyday life, for whom? Disabil. Soc. 16, 431–447. doi: 10.1080/09687590120045987
Beach, P., Perreault, M., and Lieberman, L. (2021). Affordances for motor development in the home environment for young children with and without CHARGE syndrome. Int. J. Environ. Res. Public Health 18:11936. doi: 10.3390/ijerph182211936
Brady, N. C., and Bashinski, S. M. (2008). Increasing communication in children with concurrent vision and hearing loss. Res. Practi. Pers. Severe Disabil. 33, 59–70. doi: 10.2511/rpsd.33.1-2.59
Bruce, S. M. (2005). The impact of congenital deafblindness on the struggle to symbolism. Int. J. Disabil. Dev. Educ. 52, 233–251. doi: 10.1080/10349120500252882
Bruce, S. M., Mann, A., Jones, C., and Gavin, M. (2007). Gestures expressed by children who are congenitally deaf-blind: topography rate, and function. J. Vis. Impair. Blind. 101, 637–652. doi: 10.1177/0145482X0710101010
Bruce, S. M., Zatta, M. C., Gavin, M., and Stelzer, S. (2016). Socialization and self-determination in different-age dyads of students who are deafblind. J. Vis. Impair. Blind. 110, 149–161. doi: 10.1177/0145482X1611000302
Costain, K. (2020). Tactile hypersensitivity and “overwhelming subjectivity” in the touch experience of people with congenital Deafblindness: implications for a touch-based pedagogy. Front. Educ. 5, 5:582808. doi: 10.3389/feduc.2020.582808
Damen, S., Janssen, M. J., Huisman, M., Ruijssenaars, W. A. J. J. M., and Schuengel, C. (2014). Stimulating intersubjective communication in an adult with deafblindness: a single-case experiment. J. Deaf. Stud. Deaf. Educ. 19, 366–384. doi: 10.1093/deafed/enu006
Damen, S., Janssen, M. J., Ruijssenaars, W. A. J. J. M., and Schuengel, C. (2015). Communication between children with deafness, blindness and deafblindness and their social partners: an intersubjective developmental perspective. Int. J. Disabil. Dev. Educ. 62, 215–243. doi: 10.1080/1034912X.2014.998177
Damen, S., Prain, M., and Martens, M. (2020). Video-feedback interventions for improving interactions with individuals with congenital deaf blindness: a systematic review. J. Deafblind Stud. Commun. 6, 60–69. doi: 10.21827/jdbsc.6.36191
Dammeyer, J. (2009). Congenitally deafblind children and Cochlear implants: effects on communication. J. Deaf. Stud. Deaf. Educ. 14, 278–288. doi: 10.1093/deafed/enn042
Dammeyer, J. (2012). Identification of congenital deafblindness. Br. J. Vis. Impair. 30, 101–107. doi: 10.1177/0264619612443882
Dammeyer, J., and Køppe, S. (2013). The relationship between body movements and qualities of social interaction between a boy with severe developmental disabilities and his caregiver. Intellect. Dev. Disabil. 51, 154–163. doi: 10.1352/1934-9556-51.3.154
Dammeyer, A. N., Strøm, E., Hendar, O., and Eiriksdottir, V. K. (2015). A case study of tactile language and its possible structure: a tentative outline to study tactile language systems among children with congenital deafblindness. Commun. Disord. Deaf Stud Hearing Aids 3, 1–7. doi: 10.4172/2375-4427.1000133
Deci, E. L., Ryan, R. M., and Stone, D. N. (2009). Beyond talk: creating autonomous motivation through self-determination theory. J. Gen. Manag. 34, 75–91. doi: 10.1177/030630700903400305
Fleiss, J. L. (1981). “The measurement of interrater agreement” in Statistical methods for rates and proportions. ed. J. L. Fleiss . 2nd Edn (New York City, United States: John Wiley & Sons.), 38–46.
Fukkink, R. G. (2008). Video feedback in widescreen: a meta-analysis of family programs. Clin. Psychol. Rev. 28, 904–916. doi: 10.1016/j.cpr.2008.01.003
Haakma, I. (2015). Motivation to learn: engaging students with congenital and acquired deafblindness. Doctoral dissertation. The Netherlands: University of Groningen.
Haakma, I., Janssen, M., and Minnaert, A. (2017a). The influence of need-supportive teacher behavior on the motivation of students with congenital deafblindness. J. Vis. Impair. Blind. 111, 247–260. doi: 10.1177/0145482X1711100305
Haakma, I., Janssen, M., and Minnaert, A. (2017b). Intervening to improve Teachers' need-supportive behaviour using self-determination theory: its effects on teachers and on the motivation of students with deafblindness. Int. J. Disabil. Dev. Educ. 64, 310–327. doi: 10.1080/1034912X.2016.1213376
Hoevenaars-van den Boom, M. A. A., Antonissen, A. C. F. M., Knoors, H., and Vervloed, M. P. J. (2009). Differentiating characteristics of deafblindness and autism in people with congenital deafblindness and profound intellectual disability. J. Intellect. Disabil. Res. 53, 548–558. doi: 10.1111/j.1365-2788.2009.01175.x
Intini, M., Garrino, L., Conti, A., Dimonte, V., and Borraccino, A. (2022). Deaf-blindness through the voices and experiences of parents and educators. J. Deaf. Stud. Deaf. Educ. 27, 373–384. doi: 10.1093/deafed/enac014
Janssen, M. J., Huisman, M., Van Dijk, J. P. M., and Ruijssenaars, W. A. J. J. M. (2012). Touching textures in different tasks by a woman with congenital deaf-blindness. J. Vis. Impairm. Blind. 106, 739–745. doi: 10.1177/0145482X1210601104
Janssen, M. J., Riksen-Walraven, J., and Van Dijk, J. P. M. (2003). Contact: effects of an intervention program to foster harmonious interactions between deaf-blind children and their educators. J. Vis. Impairm. Blind. 97, 215–229. doi: 10.1177/0145482X0309700403
Janssen, M. J., Riksen-Walraven, J. M., van Dijk, J., Huisman, M., and Ruijssenaars, W. (2011). Fostering harmonious interactions in a boy with congenital deaf-blindness: a single-case study. J. Vis. Impair. Blind. 105, 560–572. doi: 10.1177/0145482X1110500907
Kmet, L., Lee, R. C., and Cook, L. S. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton, Canada: Alberta Heritage Foundation for Medical Research.
Liberati, A., Altman, D. G., Tetzlaff, J., Moher, D., Mulrow, C., Gotzsche, P. C., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann. Intern. Med. 151:W-94. doi: 10.7326/0003-4819-151-4-200908180-00136
Marks, S. B. (1998). Understanding and preventing learned helplessness in children who are congenitally deaf-blind. J. Vis. Impair. Blind. 92, 200–211. doi: 10.1177/0145482X9809200307
Martens, M. A. W., Janssen, M. J., Ruijssenaars, W. A. J. J. M., Huisman, M., and Riksen-Walraven, J. (2014). Intervening on affective involvement and expression of emotions in an adult with congenital deafblindness. Commun. Disord. Q. 36, 12–20. doi: 10.1177/1525740114526926
Martens, M. A. W., Janssen, M. J., Ruijssenaars, W. A. J. J. M., Huisman, M., and Riksen-Walraven, J. M. (2017). Fostering emotion expression and affective involvement with communication partners in people with congenital deafblindness and intellectual disabilities. J. Appl. Res. Intellect. Disabil. 30, 872–884. doi: 10.1111/jar.12279
Miles, B. (1997). Talking the language of the hands to the hands. The importance of hands for the person who is deafblind. DB-LINK Fact Sheet. Available at: http://search.ebscohost.com.proxy-ub.rug.nl/login.aspx?direct=true&db=eric&AN=ED419331&site=ehost-live&scope=site
Murdoch, H., Gough, A., Boothroyd, E., and Williams, K. (2014). Adding scents to symbols: using food fragrances with deafblind young people making choices at mealtimes. Br. J. Spec. Educ. 41, 249–267. doi: 10.1111/1467-8578.12072
Narayan, J., and Bruce, S. M. (2006). Perceptions of teachers and parents on the cognitive functioning of children with severe mental disability and children with congenital deafblindness. Int. J. Rehabil. Res. 29, 9–16. doi: 10.1097/01.mrr.0000185946.49186.4e
Nelson, C., Greenfield, R. G., Hyte, H. A., and Shaffer, J. P. (2013). Stress, behavior, and children and youth who are deafblind. Res. Pract. Pers. Severe Disabil. 38, 139–156. doi: 10.2511/027494813809330243
Nelson, C., Hyte, H. A., and Greenfield, R. (2016). Increasing self-regulation and classroom participation of a child who is deafblind. Am. Ann. Deaf 160, 496–509. doi: 10.1353/aad.2016.0002
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int. J. Surg. 88:105906. doi: 10.1016/j.ijsu.2021.105906
Preisler, G., and Preisler, G. (2005). Development of communication in deafblind children. Scand. J. Disabil. Res. 7, 41–62. doi: 10.1080/15017410510032145
Reis, H. T., Sheldon, K. M., Gable, S. L., Roscoe, J., and Ryan, R. M. (2000). Daily well-being: the role of autonomy, competence, and relatedness. Personal. Soc. Psychol. Bull. 26, 419–435. doi: 10.1177/0146167200266002
Ryan, R. M., and Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 55, 68–78. doi: 10.1037/0003-066X.55.1.68
Schlesinger, H. S. (2000). A developmental model applied to problems of deafness. J. Deaf. Stud. Deaf. Educ. 5, 349–361. doi: 10.1093/deafed/5.4.349
Taylor, K. (2007). The participation of children with multi-sensory impairment in person-centred planning. Br. J. Spec. Educ. 34, 204–211. doi: 10.1111/j.1467-8578.2007.00480.x
Van Petegem, S., Baudat, S., Zimmermann, G., Zimmer-Gembeck, M., Soenens, B., and Vansteenkiste, M. (2019). Adolescents' responses to parental regulation: the role of communication style and self-determination. J. Appl. Dev. Psychol. 65:101073. doi: 10.1016/j.appdev.2019.101073
Wolthuis, K., Bol, G. W., Minnaert, A., and Janssen, M. J. (2019). Communication development from an intersubjective perspective: exploring the use of a layered communication model to describe communication development in students with congenital deafblindness. J. Commun. Disord. 80, 35–51. doi: 10.1016/j.jcomdis.2019.04.001
Keywords: deafblindness, autonomy development, autonomy support, psychosocial development, Erikson’s developmental stages
Citation: Rorije M, Damen S, Janssen MJ and Minnaert A (2023) Applying Erikson’s theory of psychosocial development to understand autonomy development in children and youths with deafblindness: a systematic literature review. Front. Educ. 8:1228905. doi: 10.3389/feduc.2023.1228905
Edited by:
Cindy H. P. Sit, The Chinese University of Hong Kong, ChinaReviewed by:
Lilly Augustine, Jönköping University, SwedenSusan M. Bruce, Boston College, United States
Copyright © 2023 Rorije, Damen, Janssen and Minnaert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marianne Rorije, bS5yb3JpamVAcnVnLm5s