 Adeline Dozois1
Adeline Dozois1 Catalina González Marqués2Kaushila Thilakasiri3Adebisi Anthonia Adeyeye4
Catalina González Marqués2Kaushila Thilakasiri3Adebisi Anthonia Adeyeye4 Joseph Leanza5
Joseph Leanza5 Megan Rybarczyk5Timothy Depp6Travis Wieland7
Megan Rybarczyk5Timothy Depp6Travis Wieland7 Naz Karim8Monalisa Muchatuta9
Naz Karim8Monalisa Muchatuta9 Fahad Ali8Ahmed Amer10
Fahad Ali8Ahmed Amer10 Stephanie Chow Garbern8
Stephanie Chow Garbern8 Shama Patel11*
Shama Patel11*- 1Department of Emergency Medicine, Atrium Health Carolinas Medical Center, Charlotte, NC, United States
- 2Department of Emergency Medicine, Brigham and Women's Hospital, Boston, MA, United States
- 3Ministry of Health Sri Lanka, Oxford University Hospitals NHS Trust, Colombo, Sri Lanka
- 4College of Medicine, University of Lagos, Lagos, Nigeria
- 5Department of Emergency Medicine, University of Pennsylvania, Philadelphia, PA, United States
- 6Department of Emergency Medicine, University of South Carolina, Greenville, SC, United States
- 7UW Health University Hospital and Beloit Memorial Hospital, Madison, WI, United States
- 8Department of Emergency Medicine, Alpert Medical School of Brown University, Providence, RI, United States
- 9Department of Emergency Medicine, SUNY Downstate Medical Center, Brooklyn, NY, United States
- 10Department of Emergency Medicine, Kings County Hospital Center, Brooklyn, NY, United States
- 11Department of Emergency Medicine, University of Florida, Jacksonville, FL, United States
One of the tenets of global emergency medicine (GEM) is to create equitable relationships between high-resource and resource-denied countries to promote emergency care for all. Health interventions proposed by those working in GEM too often lack input from local and indigenous communities result in “voluntourism,” research authorship inequity, under-representation and under-valuation of technical expertise and lived experience of leaders from resource-denied countries. We present a decolonization toolkit with specific recommendations that target and disrupt counter-productive power dynamics in GEM education. We held a workshop at the 2022 Society for Academic Emergency Medicine Annual Meeting to collectively develop strategies to address inequalities and increase diversity in GEM education. GEM practitioners were divided into small groups representing five thematic areas and asked to identify specific action items to address inequities related to their theme. Following the workshop, a group of authors reviewed small group responses and data was divided into themed qualitative matrices and recommendations were revised based on targeted literature review. Five thematic areas discussed included access, awareness and cultural humility, language, representation, and recognition. Specific recommendations and action items were created to address inequities related to these themes which can be applied by individuals and institutions in both HICs and LMICs. Despite being a relatively new academic discipline, GEM has replicated colonial structures that are prevalent in global health. However, using targeted recommendations described in our toolkit, individuals, and institutions can build a new framework for GEM that actively combats structural vulnerabilities and academic inequities.
1. Introduction
“History is written by the victors,” with the legacy of colonialism woven through the economics, politics, culture, history, and health of colonized societies. Consequently, global health policies and interventions often validate non-local perspectives and ignore indigenous expertise as well as local, historical, and socio-cultural factors. Global health has colonial roots, since its inception as “tropical medicine,” which emerged primarily to support the functioning of the extractive colonial apparatus via maintaining the health of the occupying Westerners. By focusing narrowly on pathologies impacting colonists, tropical medicine became a reinforcing mechanism of power structures imposed by occupying peoples (Birn, 2009; Packard, 2016). Later, tropical medicine evolved into “international health,” with continued focus on health conditions and hazards affecting HICs and then to the field of global health today (Smith, 2013).
Global Emergency Medicine (GEM), a relatively new sub-specialty at the intersection of global health and emergency medicine (EM), aims to support the delivery of emergency care globally through capacity strengthening, education, and clinical care in resource-limited areas and humanitarian emergencies (Birn, 2009; Markel, 2014; Packard, 2016; Kivlehan et al., 2022). Despite being a relatively new academic discipline, GEM has replicated similar colonial structures prevalent throughout the broader global health field, including unequal authorship representation, lack of locally driven projects, and poor representation of experts from low- and middle-income countries (LMICs)1 in organizational leadership.
While a growing body of literature identifies and calls to challenge colonial power structures and “decolonize global health,” few publications offer practical strategies on how to combat these inequities, particularly for educational initiatives. To address this gap, we created a Toolkit with recommendations and action items to equip individuals and academic institutions with strategies to disassemble colonial power structures in GEM education.
2. Toolkit preparation
The Society of Academic Emergency Medicine (SAEM) Global Emergency Medicine Academy (GEMA) held a workshop at the 2022 SAEM Annual Meeting to collectively develop strategies to address inequalities and increase diversity in GEM education. GEM practitioners were divided into small groups representing five thematic areas, which were developed previously by committee consensus and adapted from existing toolkits for decolonizing global health (Huq et al., 2021; University of Washington International Clinical Research Center, 2021). Groups were given a description of each theme and specific prompts for reflection (Table 1), after which groups identified specific barriers and action items for GEM education (Table 2). Following the workshop, a small group of authors reviewed the responses and data divided into themed qualitative matrices and recommendations based on targeted literature review of each specific theme.
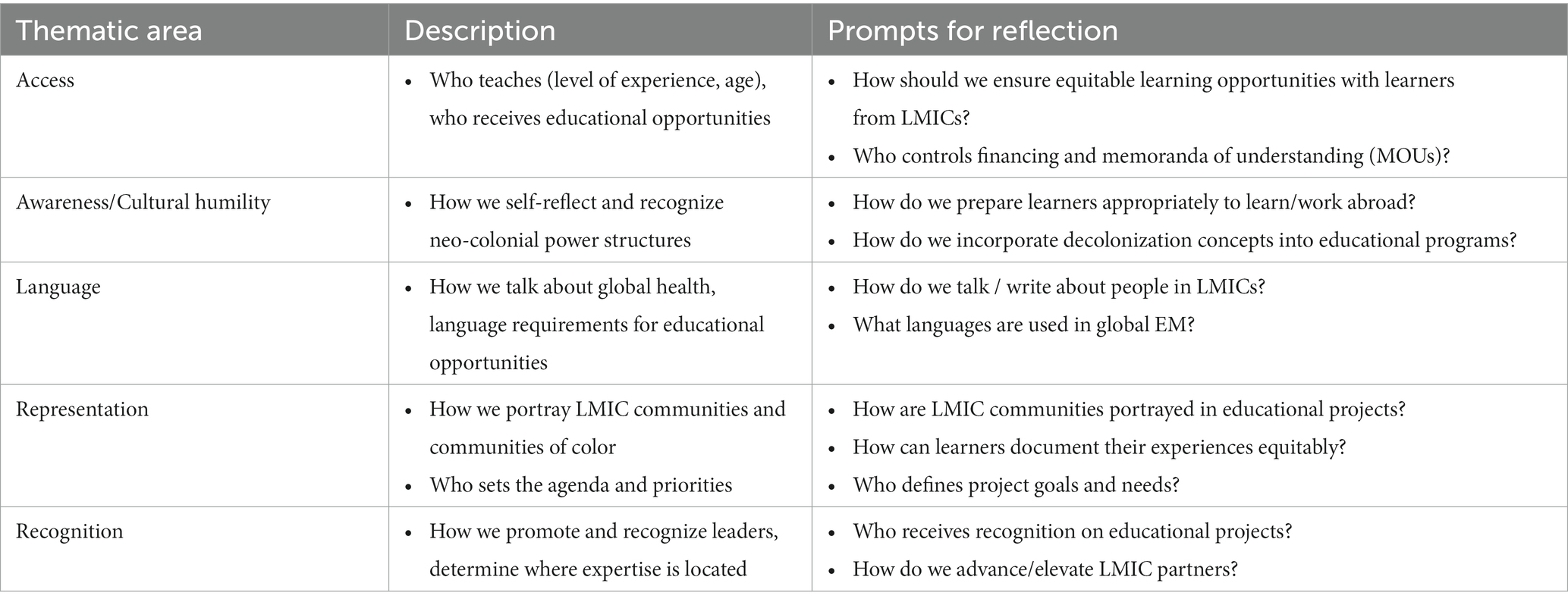
Table 1. Reflection prompts based on thematic areas.
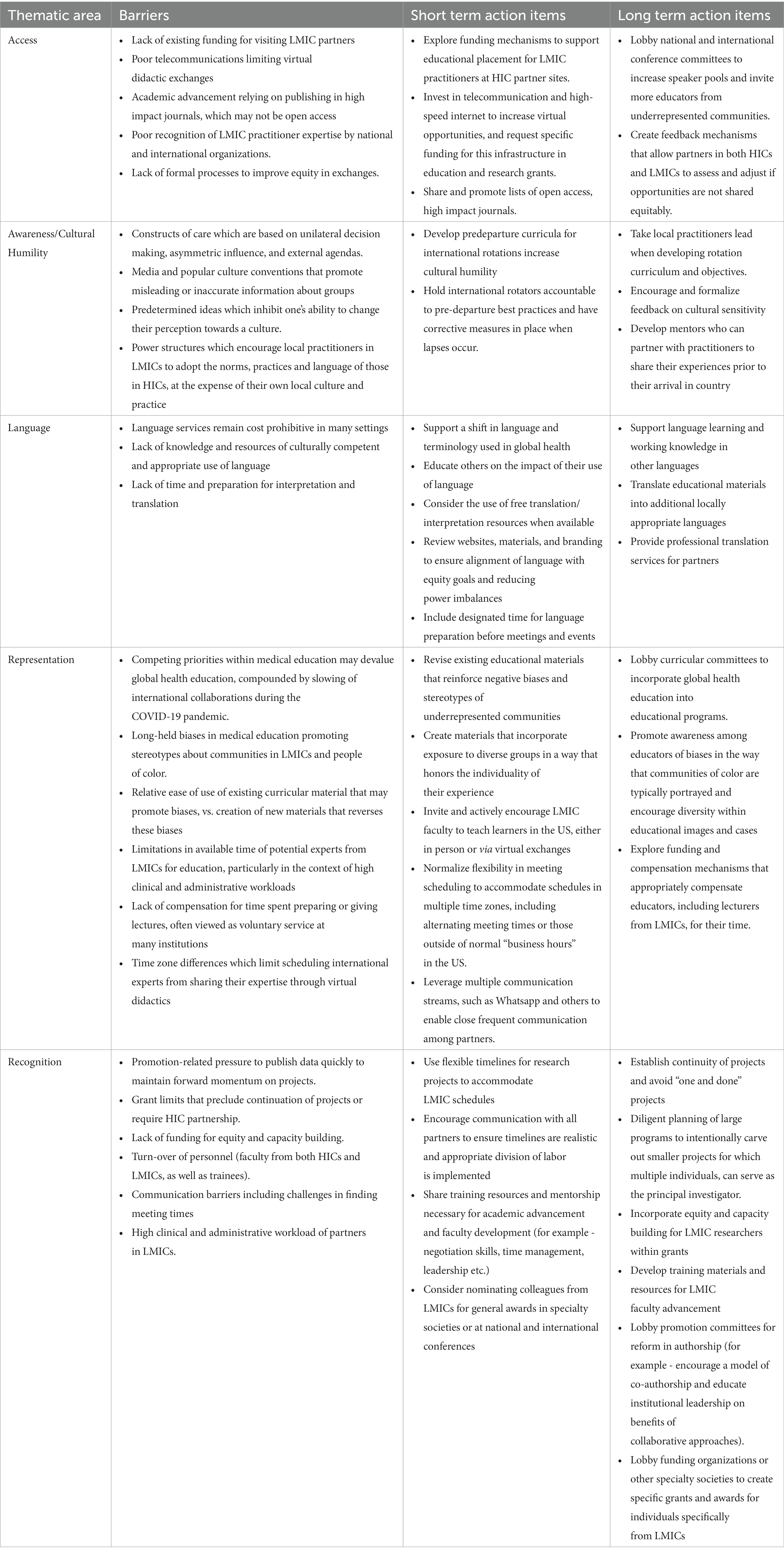
Table 2. Barriers, short term, and long-term action items.
3. Toolkit
3.1. Access
Access to educational opportunities varies widely based on trainees’ origination from HIC or LMIC and are skewed towards those from HICs. Many HIC institutions offer international opportunities for trainees in LMICs. Similar exchange experiences are often unavailable to trainees and academics from LMICs despite documented benefits (Bodnar et al., 2015). Barriers to LMIC partners visiting HICs are related to strict HICs licensing and clearance criteria limiting international visitors, further exacerbated by COVID-19 travel restrictions. Additionally, the costs associated with transportation and housing in HICs are often prohibitive.
Many trainees from HICs who visit LMICs expect to serve in a teaching role, either due to institutional suggestions or because of their own internal biases regarding the superiority of the education granted to them. Alternatively, scholars from LMICs, from trainees to well-established senior faculty, are much less frequently asked to serve as educators in HICs, even when they may hold the greatest experience. This common unidirectional model of HIC trainees traveling to LMIC sites perpetuates the colonial mentality present in GEM by viewing those from LMIC’s as less capable or knowledgeable than those trained in HICs.
EM has long been on the vanguard in developing free-open access medical education (FOAMed). What began as an experimental way to share knowledge with peers not able to afford access to content from traditional publishers, has become a structured part of medical education with increased recognition as an equitable method of knowledge sharing between communities (Chan et al., 2020). However, in practice FOAMed continues to be primarily accessed by users in HICs. Increased creation of content specifically for users in LMICs and publication of content in languages other than English is much needed (Burkholder et al., 2018). Limited access to mobile devices, particularly among gender minorities (Jennings and Gagliardi, 2013), as well as high-speed internet may also drive decreased FOAMed utilization in LMICs (Burkholder et al., 2018), as a result creators should ensure content is available to be viewed offline and promote investments in wireless technology as part of funded projects. Additionally, a shift in remote learning brought on by COVID-19 has accelerated opportunities for sharing didactic lectures and other live educational experiences on virtual platforms. Similarly, researchers from HICs conduct research in LMICs, however, final results are often published behind high-cost journal paywalls making access difficult for LMIC colleagues.
Specific Recommendations:
1. Partnerships with physician exchanges should be bi-directional with opportunities created for both HICs and LMICs with equal allocation of resources for visitors from LMICs. GEM educators in HICs should aggressively lobby departmental leadership for improved funding and expanded responsibility for visiting rotators.
2. Build repositories of free or low-cost quality medical education available all learners.
3. Empower LMICs colleagues to generate context-specific content and allow for ease of distribution to the GEM community.
4. Improve access to research findings among LMIC practitioners by aiming to publish research and educational projects in open-access journals whenever possible.
5. Work to create feedback mechanisms and space for critical reflection to allow all stakeholders to identify and resolve inequalities in partnerships (Sayeed and Taylor, 2020; Sridhar et al., 2023).
3.2. Awareness/cultural humility
Cultural humility represents an individual commitment to self-critique and openness to others’ self-definition (Tervalon and Murray-García, 1998). Moving from a mindset of cultural “competence” to one of cultural humility is an important step in the evolution of global work, especially when learning, teaching or caring for patients in another culture than one’s own. The historic frame of cultural competence implies the existence of a discrete set of facts which, when mastered, supply the practitioner with skills needed to navigate a culture different from their own (Hook et al., 2013). In contrast, cultural humility suggests that cultural understanding lies beyond a discrete skill or set of facts, especially as it applies to specific individuals within a culture (Betancourt et al., 2003). Cultural humility works to respect that the lived experience may be different within and between cultures. While a broad understanding of cultural norms is important, a perspective of cultural humility encourages a posture of respect and openness to external perspectives, while working to create space for individual voices to see individuals within their singular histories, perspectives, and held beliefs (Tsuchida et al., 2023). This understanding can ideally underpin partnerships and patient care between individuals from different backgrounds.
Specific recommendations:
1. Prepare for work by learning about the local language, culture, beliefs, social, economic, and demographic factors.
2. Preparations will aid understanding of general patterns but will not replace knowledge of individuals within their particular histories and backgrounds.
3. Prioritize decision-making from LMIC partners with ideas and content creation led by LMICs colleagues.
3.3. Language
Language is an essential mechanism for communicating solutions to global health challenges but is challenged and shadowed by colonial language perpetuating colonial structures, biases, and prejudices. Words such as “beneficiary,” “third world,” “global south,” and “developing,” result in a loss of agency and create and/or perpetuate inequitable power structures. Additional examples include “helping” rather than “partnering” or “in the field” rather than the actual location in another country (e.g., a classroom or a clinic). Turning the focus around to represent the realities more accurately - i.e., “resource-denied” rather than “resource poor” can vastly change power dynamics facilitating the breakdown of colonial structures and acknowledges the exploitative history that has often led to imbalances of resources (University of Washington International Clinical Research Center, 2021). Changes in language should permeate all aspects of global health work. Due to the fluidity of language, the understanding of how specific terminology either reinforces or disrupts harmful power structures will change over time, and should be led by indigenous and formerly colonized peoples who are most likely to be harmed by it (Hommes et al., 2021; Opara, 2021). Furthermore, non-verbal communication such as pictures or other graphics must not perpetuate colonial structures and power inequities (Huq et al., 2021).
It is not by chance that the most common languages in global health are traditionally colonial languages: English and French, with most journals, text books, and other educational materials today being published in English (Hommes et al., 2021). Choice of primary language should be an open discussion with local partners, and care should be taken to avoid comments about language ability, which are common microaggressions in global work (University of Washington International Clinical Research Center, 2021). Additionally, interpretation should be offered and expected in conversations, and individuals should not be excluded based on language abilities. The choice of working language(s), as well as the words and designations used within those languages, should be discussed throughout partnerships in global health to ensure mutual respect and equity.
Specific recommendations:
1. Promote the consistent use of language that seeks to reduce power imbalances, avoid dehumanizing, derogatory, and patronizing terminology, developed through local partnership and collaboration.
2. Institutions should critically analyze their language, branding, photos, graphics and other media - with a focus on both verbal and non-verbal communication - and align their messaging with locally appropriate language and imagery.
3. Provide environments that support all partners’ primary language(s) and accommodate for translation both in their home country and abroad.
4. The research community should provide resources that allow for publications to be published in authors’ primary language(s) and offer interpretation.
5. Institutions offering experiential curricula for students/trainees should incorporate primary language(s) of sites as well as principles and best practices in cross-cultural communication.
3.4. Representation
Although race is a social construct with biologic consequences, rather than a meaningful biologic/scientific construct, medical education often does not reflect this understanding (Amutah et al., 2021). Reviews of medical school curricula have shown significant misrepresentations of race, using imprecise or antiquated labels to convey complex biologic or genetic trends, or presenting racial and ethnic differences in disease prevalence without context (Amutah et al., 2021). Medical school curricula suffer from a lack of representation of people of color in both textbooks and didactic instruction. In medical illustrations, white, male, cis-gender patients often serve as the default example, and when patients of other races, genders, and sexual orientation are presented it is often to illustrate associations between disease and specific ethnic and racial categories (Nieblas-Bedolla et al., 2020; Ilic et al., 2022). This can lead to race-based diagnostic bias that pathologizes race (Amutah et al., 2021). Unsurprisingly, a substantial number of US medical students and trainees hold false beliefs about racial and ethnic differences (Hoffman et al., 2016).
Data on representation of immigrant communities in medical education is more limited but is thought to be at high risk for negative bias due to the intersectionality between race, ethnicity, and migration (Hall et al., 2015). Similar to non-white populations in the US, when patients who are immigrants or refugees are presented as cases in pre-clinical medical education, it is often to illustrate a potential tropical disease not typically seen in the US, which can lead to diagnostic bias towards “exotic diseases” in these groups and against more common conditions that may be unrelated to their immigrant status. Meanwhile, refugee and immigrant communities face unique health challenges related to access to care, language barriers, and global health epidemiology. Increased exposure to global health curricula, particularly those focused on cultural humility and immigrant health, can better equip healthcare workers to address healthcare disparities in migrants and refugees (Gruner et al., 2022).
Specific recommendations:
1. Medical education should increase exposure to global health for trainees from HICs, including perspectives of LMIC communities and communities of color. Specific attention should be paid to address underlying themes of “white saviorism” that are pervasive in discussions of global health partnerships and international aid.
2. GEM educators should beware of reinforcing biases against immigrant communities and communities of color that are pervasive within medical education. Immigrants and people of color should be included in case-based learning, including in cases unrelated to ethnicity or country of origin.
3. Experts in EM should be given national and international opportunities to share their specialized knowledge regardless of their country of origin. Educational exchanges involving didactics should encourage educators from both HICs and LMICs to share their specific knowledge and experiences with learners.
4. Ensure that local collaborators’ perspectives and priorities are considered throughout research or educational projects, and increase opportunities for trainees and faculty from LMICs to publish and take an active role in research.
3.5. Recognition
EM is a relatively new specialty with the majority of specialty-specific advancement and influential societies based in HICs where the specialty first originated in the 1960s–1980s (Alagappan et al., 2007). This creates an environment where work done by LMIC experts is usually not acknowledged on the global stage due to the early stage of EM development in many LMICs. There is sometimes pressure on LMIC experts to partner with HIC experts to bring attention to work that they developed and led in their home countries.
In particular, authors from LMICs are underrepresented in the broader global health literature, most notably in the lead author positions (first and last author) which have the greatest impact on academic advancement and grant funding (Sumathipala et al., 2004; Ghani et al., 2020). Within GEM specifically, recent analysis of studies within the annual Global Emergency Medicine Literature Review (GEMLR) from 2016 to 2020 found that in research conducted in LMICs, authors affiliated with high-income countries (HICs) were represented more often and were more likely to be in lead author positions than those from LMICs. Additionally, evidence of author “parasitism,” in which a study conducted in a LMIC had no authors from the study country was not uncommon (Garbern et al., 2022).
There are limited opportunities for development of leadership and other academic skills for EM faculty from LMICs (Keiller et al., 2022), where newly trained faculty often have heavy clinical workloads, lack protected time for developing medical education skills, and lack mentorship to advance their careers. Therefore, LMIC faculty may feel poorly equipped to lead academic and training program advancements in their home countries (Douglass and Williams, 2019). Improving the availability of these resources could lead to more visibility and thus more recognition of LMIC experts.
Having LMIC faculty hold joint academic appointments at HIC institutions, in a similar manner as many HIC faculty do with LMIC institutions, can increase opportunities for LMIC leaders in education and academia to be recognized. Reversing the often uni-directional flows of academic funding and knowledge, promoting the unique and valuable perspectives of indigenous scholars, can lead to more equitable global health partnerships (Adams et al., 2016; Karim et al., 2020; Eichbaum et al., 2021).
Specific Recommendations:
1. Decolonization in GEM should be mindful of structures within academia that promote inequities in authorship and attempts made to challenge those structures. When developing manuscripts, attempt meaningfully engagement with LMIC partners and credit them with either first or last author positions. Because factors affecting academic advancement can vary widely by institution and country, HIC authors should also be aware of how authorship position is viewed by the institutions of their partners and advocate for the importance of partnerships to promotion committees.
2. Increase recognition of partners from LMICs for their work through nominations for national and international awards. Physicians from LMICs should be considered for nomination awards granted by organizations based in all income countries. This recognition can start with nomination for existing awards; however, specialty societies should consider creating awards specifically geared towards partners from LMICs.
3. Share and develop resources on skills necessary for academic advancement and faculty development that are culturally and context appropriate.
4. Discussion
Despite its colonial legacy, tremendous opportunity exists to center the field of GEM on practices informed by the core principles of equity and justice. With a broad global literature base examining philosophical and sociological approaches to decolonization, it is now up to practitioners of GEM to translate knowledge into action. As the GEM community has begun to critically analyze the colonial legacy within its specialty, Access, Representation, Cultural Humility, Language, and Recognition stand out as impactful themes.
We hope that this toolkit can serve as a starting point, a guide, and an impetus for change. While use of the toolkit is not meant to be prescriptive, we provide some suggested methods to implement the toolkit. Regarding the end-user, the toolkit may be used for both individual or group activities to critically examine the current state of existing educational projects and serve as a guide to direct future more equitable initiatives. We encourage representation from all partners to ensure diverse voices are heard and a truly collaborative rather than uni-directional strategy exists to overcome barriers. Our current work is limited by the composition of our writing group which disproportionately includes authors affiliated with institutions in the US, and we acknowledge that there may be additional strategies or considerations missing from our HIC-weighted perspective. As a result, revisiting the toolkit regularly is suggested, perhaps on a semi-annual basis and with increasing involvement of practitioners from LMICs, to track progress and ensure accountability to stated goals, and create additional themes as relevant to one’s own work as they arise using the toolkit’s framework.
With respect to Access and Representation, we strongly endorse bidirectional knowledge transfer, educational and travel opportunities, freely accessible medical education, and research, emphasizing the expertise and perspectives of EM leaders in LMICs. Some recent examples demonstrating positive changes in the GEM field include resources from the African Federation of Emergency Medicine (AFEM) (African Federation of Emergency Medicine, 2021). AFEM provides comprehensive EM educational and clinical resources that are open access, free, and implemented worldwide. An additional two examples are found within the University of California San Francisco (UCSF) specialty-independent Health, Equity, Action, and Leadership (HEAL) (Heal Initiative, 2023) fellowship, which aims to develop bidirectional education, interprofessional exchange, and partnership-based sustainable work over multi-year assignments. Simultaneously, UCSF has created a Center for Health Equity in Surgery and Anesthesia, which focuses on local and global health equity featuring bidirectional research, advocacy, education, and training (Center for Health Equity in Surgery and Anesthesia, 2023). These frameworks, put into practice by AFEM and UCSF, can be easily molded to other global health initiatives.
Considering Cultural Humility and Language, we encourage practitioners and institutions to reconceptualize how GEM academic projects are conducted. Practitioners should develop cultural competence while simultaneously aspiring to the ideals of cultural humility. We simultaneously recommend equitable usage of working languages and interpretation so that all patients, communities, and partners have an equal voice. We therefore recommend care in employing verbal and non-verbal communication that encourages agency, equity, and is defined by those that it describes.
Finally, with respect to Recognition, we recommend an approach that understands differing cultural contexts surrounding professional advancement, encourages equal access to research opportunities and accolades, collaboratively shares and develops skills, and seeks to both fund and recognize individuals from LMICs for their achievements. While authorship inequity is reflective of deep systemic inequities in GEM research and funding, the GEMLR group recently took an important step toward promoting authorship equity by implementing an article scoring criteria to award additional points if authors have an affiliation in the country where the research was performed. Future steps might include further emphasis on author blocks that contain local researchers in the first and last author positions and ensuring LMIC scholars have equitable representation on global health and GEM journal editorial boards.
Lastly, we encourage thoughtful, respectful dialog to promote more equitable, meaningful partnerships.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
CG, SG, and MM: substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work. JL, MR, KT, TD, AdA, TW, NK, FA, AhA, SP, CG, AD, SG, and MM: drafting the work or revising it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank the participants below who attended the Society of Academic Emergency Medicine 2022 Annual Meeting session “Who Benefits From Global Health Education? Creating an Action List to Decolonize Global Emergency Medicine Education” for their insights and contributions to this toolkit. These members include: Uche Anigbogu, MD, Michaela Banks, MD, MBA; Andrew Beck MD MS, Torben K. Becker, MD, PhD, Morgan C. Broccoli, MD, MPH, MSc, Taylor Burkholder, MD, MPH, Cameron Callipari, MD, Suven Cooper, MD MPH, Mariame Fofana, MD, Czestochowa Francois MD, MPH, Megan Horne, MD, Brianna Hurdle MD, Trevia Jackson MD, Farha Khan MD, Elise Klesick, DO, Samantha Lawson, MD, Adam Laytin, MD MPH, J. Austin Lee MD MPH, Rmaah Memon, MD, Elizabeth Morrison MD, Sonya Naganathan, MD, MPH, Sarah Newhall, MD, Thomas Parks Remcho, BS, Amanda Michelle Ritchie, MD, BScN, Rachel Shing MD, Vicken Totten, MD.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^We use the term LMIC instead of other terms such as the “global south.” All terms have limitations and to an extent may perpetuate power imbalances, but we must choose a term, within the limited language and have chosen LMIC.
References
Adams, L. V., Wagner, C. M., Nutt, C. T., and Binagwaho, A. (2016). The future of global health education: training for equity in global health. BMC Med. Educ. 16, 296–297. doi: 10.1186/s12909-016-0820-0
African Federation of Emergency Medicine . (2021). AFEM. Available at: https://afem.africa/resources/ (Accessed April 30, 2023).
Alagappan, K., Schafermeyer, R., Holliman, C. J., Iserson, K., Sheridan, I. A., Kapur, G. B., et al. (2007). International emergency medicine and the role for academic emergency medicine. Acad. Emerg. Med. 14, 451–456. doi: 10.1197/j.aem.2007.01.003
Amutah, C., Greenidge, K., Mante, A., Munyikwa, M., Surya, S. L., Higginbotham, E., et al. (2021). Misrepresenting race - the role of medical schools in propagating physician Bias. N. Engl. J. Med. 384, 872–878. doi: 10.1056/NEJMms2025768
Betancourt, J. R., Green, A. R., Carrillo, J. E., and Ananeh-Firempong, O. (2003). Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Public Health Rep. 118, 293–302. doi: 10.1093/phr/118.4.293
Birn, A. E. (2009). The stages of international (global) health: histories of success or successes of history? Glob. Public Health 4, 50–68. doi: 10.1080/17441690802017797
Bodnar, B. E., Claassen, C. W., Solomon, J., Mayanja-Kizza, H., and Rastegar, A. (2015). The effect of a bidirectional exchange on faculty and institutional development in a global health collaboration. PLoS One 10:e0119798. doi: 10.1371/journal.pone.0119798
Burkholder, T. W., Bellows, J. W., and King, R. A. (2018). Free open access medical education (FOAM) in emergency medicine: the global distribution of users in 2016. West. J. Emerg. Med. 19, 600–605. doi: 10.5811/westjem.2018.3.36825
Center for Health Equity in Surgery and Anesthesia . (2023). University of California San Francisc. Available at: https://globalsurgery.org/ (Accessed August 30, 2023).
Chan, T. M., Stehman, C., Gottlieb, M., and Thoma, B. (2020). A short history of free open access medical education. The past, present, and future. ATS Schol. 1, 87–100. doi: 10.34197/ats-scholar.2020-0014PS
Douglass, K., and Williams, A. (2019). Faculty development program for emergency medicine physicians in India: a pilot program. AEM Educ. Train. 3, 33–38. doi: 10.1002/aet2.10125
Eichbaum, Q. G., Adams, L. V., Evert, J., Ho, M. J., Semali, I. A., and van Schalkwyk, S. C. (2021). Decolonizing Global Health education: rethinking institutional partnerships and approaches. Acad. Med. J. Assoc. Am. Med. Coll. 96, 329–335. doi: 10.1097/ACM.0000000000003473
Garbern, S. C., Hyuha, G., González Marqués, C., Baig, N., Chan, J. L., Dutta, S., et al. (2022). Authorship representation in global emergency medicine: a bibliometric analysis from 2016 to 2020. BMJ Glob. Health 7:e009538. doi: 10.1136/bmjgh-2022-009538
Ghani, M., Hurrell, R., Verceles, A. C., McCurdy, M. T., and Papali, A. (2020). Geographic, subject, and authorship trends among LMIC-based scientific publications in high-impact Global Health and general medicine journals: a 30-month bibliometric analysis. J. Epidemiol. Glob. Health. 11, 92–97. doi: 10.2991/jegh.k.200325.001
Gruner, D., Feinberg, Y., Venables, M. J., Shanza Hashmi, S., Saad, A., Archibald, D., et al. (2022). An undergraduate medical education framework for refugee and migrant health: curriculum development and conceptual approaches. BMC Med. Educ. 22:374. doi: 10.1186/s12909-022-03413-8
Hall, W. J., Chapman, M. V., Lee, K. M., Merino, Y. M., Thomas, T. W., Payne, B. K., et al. (2015). Implicit racial/ethnic Bias among health care professionals and its influence on health care outcomes: a systematic review. Am. J. Public Health 105, e60–e76. doi: 10.2105/AJPH.2015.302903
Hoffman, K. M., Trawalter, S., Axt, J. R., and Oliver, M. N. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc. Natl. Acad. Sci. U. S. A. 113, 4296–4301. doi: 10.1073/pnas.1516047113
Heal Initiative . (2023). GEMLR. Available at: https://www.gemlr.org (Accessed April 30, 2023)
Hommes, F., Monzó, H. B., Ferrand, R. A., Harris, M., Hirsch, L. A., Besson, E. K., et al. (2021). The words we choose matter: recognising the importance of language in decolonising global health. Lancet Glob. Health 9, e897–e898. doi: 10.1016/S2214-109X(21)00197-2
Hook, J. N., Davis, D. E., Owen, J., Worthington, E. L., and Utsey, S. O. (2013). Cultural humility: measuring openness to culturally diverse clients. J. Couns. Psychol. 60, 353–366. doi: 10.1037/a0032595
Huq, M., Irvine, L., and Burgess, R. (2021). Decolonize Global Health working group at the UCL Institute for Global Health. Decolonising Global Health & Development Toolkit. Available at: https://www.ucl.ac.uk/teaching-learning/sites/teaching_learning/files/decolonising_global_health_toolkit.pdf (Accessed August 30, 2023).
Ilic, N., Prescott, A., Erolin, C., and Peter, M. (2022). Representation in medical illustration: the impact of model bias in a dermatology pilot study. J. Vis. Commun. Med. 45, 253–262. doi: 10.1080/17453054.2022.2086455
Jennings, L., and Gagliardi, L. (2013). Influence of mhealth interventions on gender relations in developing countries: a systematic literature review. Int. J. Equity Health 12, 85–10. doi: 10.1186/1475-9276-12-85
Karim, N., Rybarczyk, M. M., Jacquet, G. A., Pousson, A., Aluisio, A. R., Bilal, S., et al. (2020). COVID-19 pandemic prompts a paradigm shift in global emergency medicine: multidirectional education and remote collaboration. AEM Educ. Train. 5, 79–90. doi: 10.1002/aet2.10551
Keiller, L., Nyoni, C., and van Wyk, C. (2022). Online faculty development in low- and middle-income countries for health professions educators: a rapid realist review. Hum. Resour. Health 20:12. doi: 10.1186/s12960-022-00711-6
Kivlehan, S. M., Hexom, B. J., Bonney, J., Collier, A., Nicholson, B. D., Quao, N. S. A., et al. (2022). Global emergency medicine: a scoping review of the literature from 2021. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 29, 1264–1274. doi: 10.1111/acem.14575
Markel, H. (2014). Worldly approaches to global health: 1851 to the present. Public Health 128, 124–128. doi: 10.1016/j.puhe.2013.08.004
Nieblas-Bedolla, E., Christophers, B., Nkinsi, N. T., Schumann, P. D., and Stein, E. (2020). Changing how race is portrayed in medical education: recommendations from medical students. Acad. Med. J. Assoc. Am. Med. Coll. 95, 1802–1806. doi: 10.1097/ACM.0000000000003496
Opara, I. (2021). It’s time to decolonize the decolonization movement. Speaking of medicine and health. Published July 29, 2021. Available at: https://speakingofmedicine.plos.org/2021/07/29/its-time-to-decolonize-the-decolonization-movement/ (Accessed August 1, 2023).
Sayeed, S., and Taylor, L. (2020). Institutionalising global health: a call for ethical reflection. BMJ Glob. Health 5:e003353. doi: 10.1136/bmjgh-2020-003353
Smith, R. (2013). Moving from global heath 3.0 to global health 4.0. The BMJ. Published October 8, 2013. https://blogs.bmj.com/bmj/2013/10/08/richard-smith-moving-from-global-heath-3-0-to-global-health-4-0/ (Accessed January 29, 2023).
Sridhar, S., Alizadeh, F., Ratner, L., Russ, C. M., Sun, S. W., Sundberg, M. A., et al. (2023). Learning to walk the walk: incorporating praxis for decolonization in global health education. Glob. Public Health 18:2193834. doi: 10.1080/17441692.2023.2193834
Sumathipala, A., Siribaddana, S., and Patel, V. (2004). Under-representation of developing countries in the research literature: ethical issues arising from a survey of five leading medical journals. BMC Med. Ethics 5:E5. doi: 10.1186/1472-6939-5-5
Tervalon, M., and Murray-García, J. (1998). Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. J. Health Care Poor Underserved 9, 117–125. doi: 10.1353/hpu.2010.0233
Tsuchida, R. E., Doan, J., Losman, E. D., Haggins, A., Huang, R., Hekman, D., et al. (2023). Cultural humility curriculum to address healthcare disparities for emergency medicine residents. West. J. Emerg. Med. 24, 119–126. doi: 10.5811/westjem.2023.1.58366
University of Washington International Clinical Research Center . (2021). Decolonizing Global Health toolkit. Available at: https://globalhealth.washington.edu/sites/default/files/ICRC%20Decolonize%20GH%20Toolkit_20210330.pdf
Keywords: global health, global emergency medicine, decolonization of global health, health equity, global health education HICs and LICs
Citation: Dozois A, González Marqués C, Thilakasiri K, Adeyeye AA, Leanza J, Rybarczyk M, Depp T, Wieland T, Karim N, Muchatuta M, Ali F, Amer A, Garbern SC and Patel S (2023) A toolkit for decolonizing global emergency medicine education. Front. Educ. 8:1214904. doi: 10.3389/feduc.2023.1214904
Edited by:
Ashti A. Doobay-Persaud, Northwestern University, United StatesReviewed by:
Anna Kalbarczyk, Johns Hopkins University, United StatesCopyright © 2023 Dozois, González Marqués, Thilakasiri, Adeyeye, Leanza, Rybarczyk, Depp, Wieland, Karim, Muchatuta, Ali, Amer, Garbern and Patel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shama Patel, c2hhbWEuZC5wYXRlbEBnbWFpbC5jb20=