 Marie H. Martin
Marie H. Martin Elizabeth S. Rose
Elizabeth S. Rose Eiman Jahangir
Eiman Jahangir Douglas C. Heimburger2,5
Douglas C. Heimburger2,5
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ. , 16 November 2023
Sec. Higher Education
Volume 8 - 2023 | https://doi.org/10.3389/feduc.2023.1200389
This article is part of the Research Topic Research and Discussions in Critical Discourses and Remedies in Global Health Education View all 20 articles
Introduction: Responding to a growing need for health care professionals equipped with global expertise in local and international settings, an innovative global health medical school course was developed that combines rigorous didactics, mentorship, cross-cultural training, and international experiences to build students’ cultural humility and clinical skills.
Methods: Recognizing that global health service trips and courses can unintentionally exacerbate inequities and power imbalances, this course was evaluated using the four principles of Melby et al.’s Guidelines for Implementing Short-term Experiences in Global Health. These principles include skill building in cross-cultural effectiveness and cultural humility, bidirectional participatory relationships, local capacity building, and long-term sustainability.
Results: The course was developed with long-standing global partners and includes a capstone project that is intended to strengthen local capacity with benefits to the site and student. Student course evaluations, supervisors’ observations of students, and supervisor feedback forms indicate that this course achieves these principles. Furthermore, there is evidence that students developed cultural humility, acquired foundational science knowledge and relevant skills, and changed their medical practice.
Discussion: This approach could serve as a model for institutions seeking to enhance training in global health for medical students.
Experience in global health is increasingly viewed as an essential component of medical and public health training (Drain et al., 2009; Rowson et al., 2012). There has been a growing demand by students in high-income countries (HIC) for educational opportunities that build skills for research in global contexts, clinical knowledge for service delivery in low-income settings, cross-cultural competencies, and tools to address global health inequities (Macfarlane et al., 2008; Merson and Page, 2009). The rise in global health interest across academic, business, and government sectors has driven expansion of opportunities for global health education and cultural humility training in medical schools (Drain et al., 2007). Moreover, there are increasing demands for health care providers who can effectively engage people with international backgrounds and provide care with a high degree of cultural competence regardless of setting (Crump and Sugarman, 2010).
Responding to these needs, the Vanderbilt Institute for Global Health (VIGH) and the Vanderbilt University School of Medicine (VUSM) developed a global health integrated science course for third- and fourth-year medical students to develop competencies aimed at providing high quality and equitable health care to diverse patients in both local and global contexts. The course also seeks to build and enhance sustainable, bi-directional partnerships for health care, particularly in low-resourced settings. This immersive, foundational month-long course includes clinical experience in low- and middle-income countries (LMICs), mentoring, a capstone project and paper, and digital didactic modules and discussions that explore topics on global health epidemiology, equity, healthy policy, and health systems.
Global health service trips and courses can unintentionally exacerbate inequities and power imbalances (Eichbaum et al., 2021). To address this issue, frameworks have been developed to guide educators in mindful design of courses and short-term experiences in global health (STEGH) (Melby et al., 2016; Shah et al., 2019; Prasad et al., 2022). These principles promote STEGH elements that encourage sustainable and ethical engagement with local collaborators. This course utilizes many of the principles outlined as best practices in developing and implementing STEGHs. We expand the use of an equity framework to evaluate an existing global health program that has been in existence for ten years. As an established framework, Melby et al. has been frequently utilized to reinforce global health equity standards.
After a decade of offering this global health clinical immersion course, we sought to formally evaluate and understand how it aligns with best practice principles. We selected Melby et al.’s (2016) Guidelines for Implementing Short-term Experiences in Global Health as the framework to evaluate the course. The principles in this framework include skill building in cross-cultural effectiveness and cultural humility, bidirectional participatory relationships, local capacity building, and long-term sustainability. In this paper, we describe outcomes of the evaluation in relation to these four principles based on student course evaluations and LMIC supervisor feedback. Using these principles, we aimed to understand the impact of this course on students, clinical partners, and LMIC communities. We were also interested in exploring whether a similar curricular approach could be broadly implemented by medical schools with similar resources and global networks, or adapted by medical schools with limited resources, in order to enhance collaborative, sustainable global health education.
In this international clinical rotation course, students participated in patient care at long-standing partner sites in low- and middle-income countries. Sustained engagement with these sites for more than a decade has provided reliability in the clinical experience and maintained global health partnerships. Partner sites include an urban tertiary care teaching hospital (Jordan), a rural district hospital (Kenya), and a rural health clinic (Guatemala). Beyond these sites, students can propose an “alternate site,” such as at a teaching hospital in Peru or a clinic run by a non-governmental organization in India, if the site better meets the student’s learning objectives. From 2012 to 2022, 121 students participated in this course with 68% of students rotating with one of our partner sites.
This course includes a structured curriculum with pre-departure training, online video lectures, journal articles, 40+ hours of weekly on-site clinical activity in inpatient, outpatient, and community settings, remote mentoring, and online discussion boards. Didactic activities and clinical immersion are guided by eight course competencies (Table 1). The course materials provide students an understanding of diseases and challenges in LMICs through the foundational sciences including epidemiology, equity, ethics, health policy, and health systems (Dahlman et al., 2018). While course didactics focus primarily on health systems and disparities, students rotate in a variety of specialty clinical areas depending on site-specific resources. In certain sites, students engage in language training provided by a third party, which augments their experience and efficacy at the clinic and in the community.
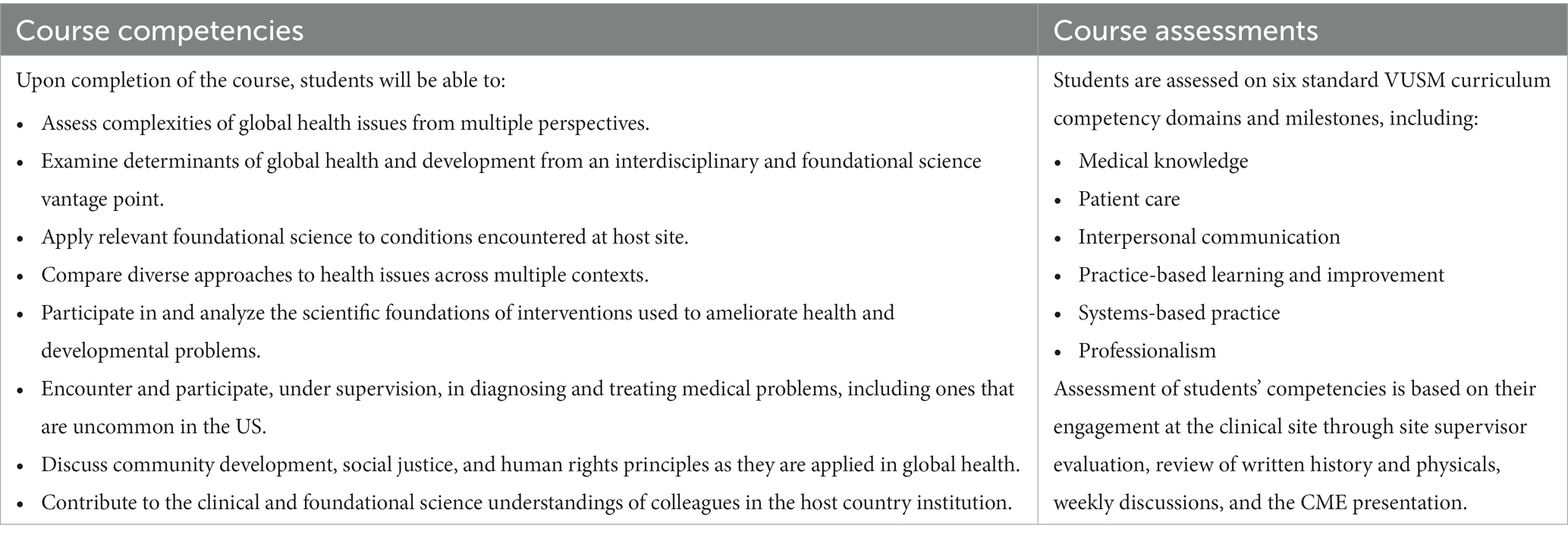
Table 1. Global health immersion course competencies and milestones.
At the end of each course, students submit course evaluations and host-site clinical supervisors (either physicians or clinical officers, depending on the facility) submit observational assessments of students as well as course feedback forms. Supervisors rank a student’s behavior on selected Accreditation Council for Graduate Medical Education (ACGME) milestones1 as well as the impact of the student on the environment using a four-point scale from below average (1) to exceptional (4) and write comments about the student’s performance. Student evaluations included questions with four- and six-point Likert scales for students to indicate perceived quality, agreement, frequency, or importance of the question topic. Students further described their experiences in free-response fields. We calculated means and standard deviations for quantitative data. We used consensus to categorize qualitative data based on Melby et al.’s principles. Over the ten years this course has been implemented, there have been slight changes (e.g., questions added or removed) in measurement tools resulting from modifications in the medical school assessment processes, which impacted the number of students that completed each item.
In designing and implementing the course and evaluation tools, we used Melby et al.’s principles to create and assess how the course aligned with best practices for STEGH. The principles were applied in the following ways:
Principle 1 – skills building in cross-cultural effectiveness and cultural humility: in the months prior to departure, students complete training in cultural humility, ethics of engagement, professionalism, risks of traveling abroad, and understanding culture shock. Additionally, students develop learning objectives to supplement site- and module-specific objectives. Weekly mentoring calls with Vanderbilt faculty focus on ethical and culturally appropriate engagement and course reflections help students continue to process their experiences abroad.
Principle 2 – foster bidirectional participatory relationships: course leaders and local clinical staff (including physicians, clinical officers, nurses, laboratory technicians and/or community health workers) support bilateral collaboration, reverse innovation, and reciprocal opportunities. In bidirectional exchanges, students are peer mentors for visiting medical students from their host site. During the course, students work in collaborative, interprofessional teams depending on the site (including various cadres of clinical and non-clinical staff) and are assessed on teamwork and systems-based practice.
Principle 3 – promote sustainable local capacity building and health systems strengthening: students contribute to strengthening long-term capacity in health care, public health, and health systems through their capstone project. During the first weeks of the course, students collaborate with their clinical supervisor and other clinical staff (which may include physicians, clinical officers, nurses, laboratory technicians and/or other allied health professionals) to identify a project that is beneficial to the LMIC host site. Each student capstone project is focused on increasing knowledge and/or skills of an identified disease or condition during weekly continuing medical education sessions held at the local facility.
Principle 4 – community-led efforts focused on sustainable development: at most sites, students participate in community health activities led by the clinic including health education classes at local schools, water and sanitation workshops, and cooking classes. To ensure applicability and sustainability of the course, course leaders regularly monitor and evaluate the impact of this STEGH.
Ethics approval was received from Vanderbilt University Medical Center (#221706).
Between 2012 and 2022, 85 students and 30 clinical supervisors completed course evaluations, and these formed the basis of our analysis. Based on the four principles outlined by Melby et al. (2016), our data indicate that the structure and content of this course aligns with suggested best practices for STEGH.
Student course evaluations suggest that students gained cultural humility through pre-departure modules and workshops and in clinical rotations (Table 2). Students (94%) agreed that the pre-departure training prepared them for the immersion experience. In questions related to developing cultural humility, students (99%) agreed that the clinical environment consistently reflected sensitivity to issues of culture, gender, race, religion, and sexual orientation and/or identity.
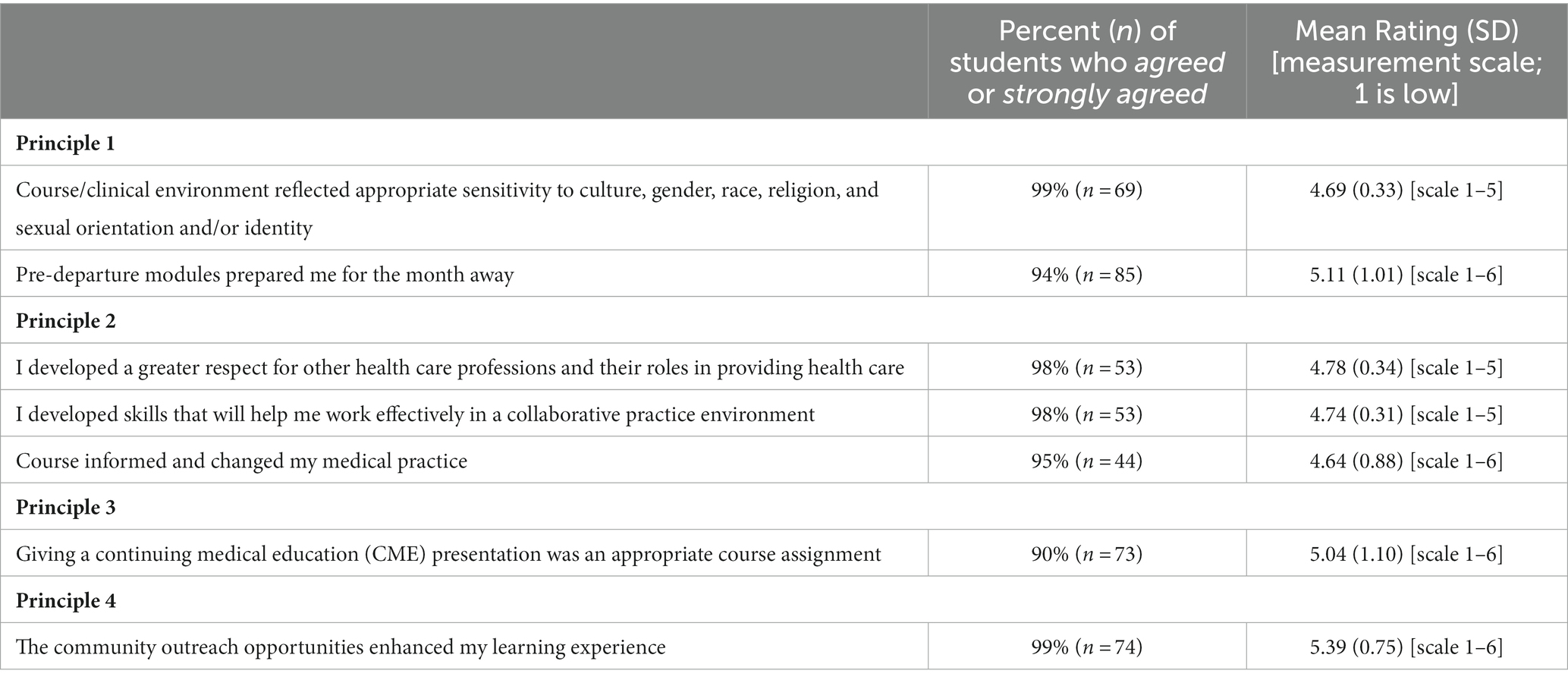
Table 2. Student course evaluation questions.
In open-ended responses on course evaluations, most students (78%) described how the opportunity to learn and practice medicine in another setting enhanced their cultural humility, knowledge, and skills (Table 3). Students’ clinical experiences and engagements with patients helped them understand the ways that one’s culture impacts their perception of health care. Through this new understanding, students wrote about becoming more culturally sensitive in their clinical practice. Students described the unique perspectives they gained that included caring for the whole person and the community.
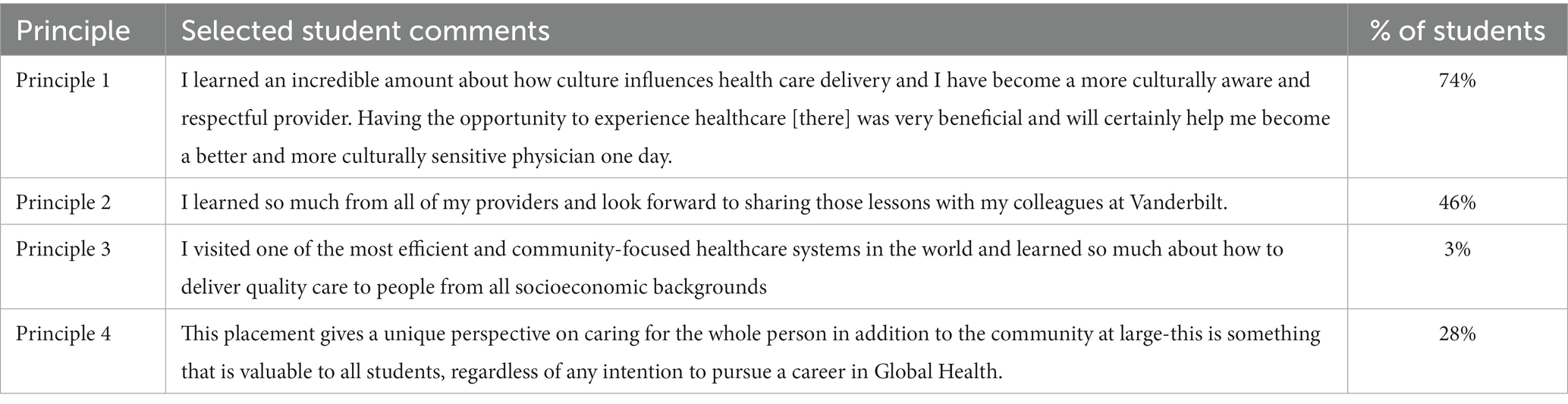
Table 3. Percentage of students’ comments that align with each principle (some comments aligned with multiple principles).
Almost all supervisors rated students’ depth of knowledge (97% of supervisors gave top ratings), performance in learning and improvement (97%), and their approach to learning (93%) highly (Table 4).
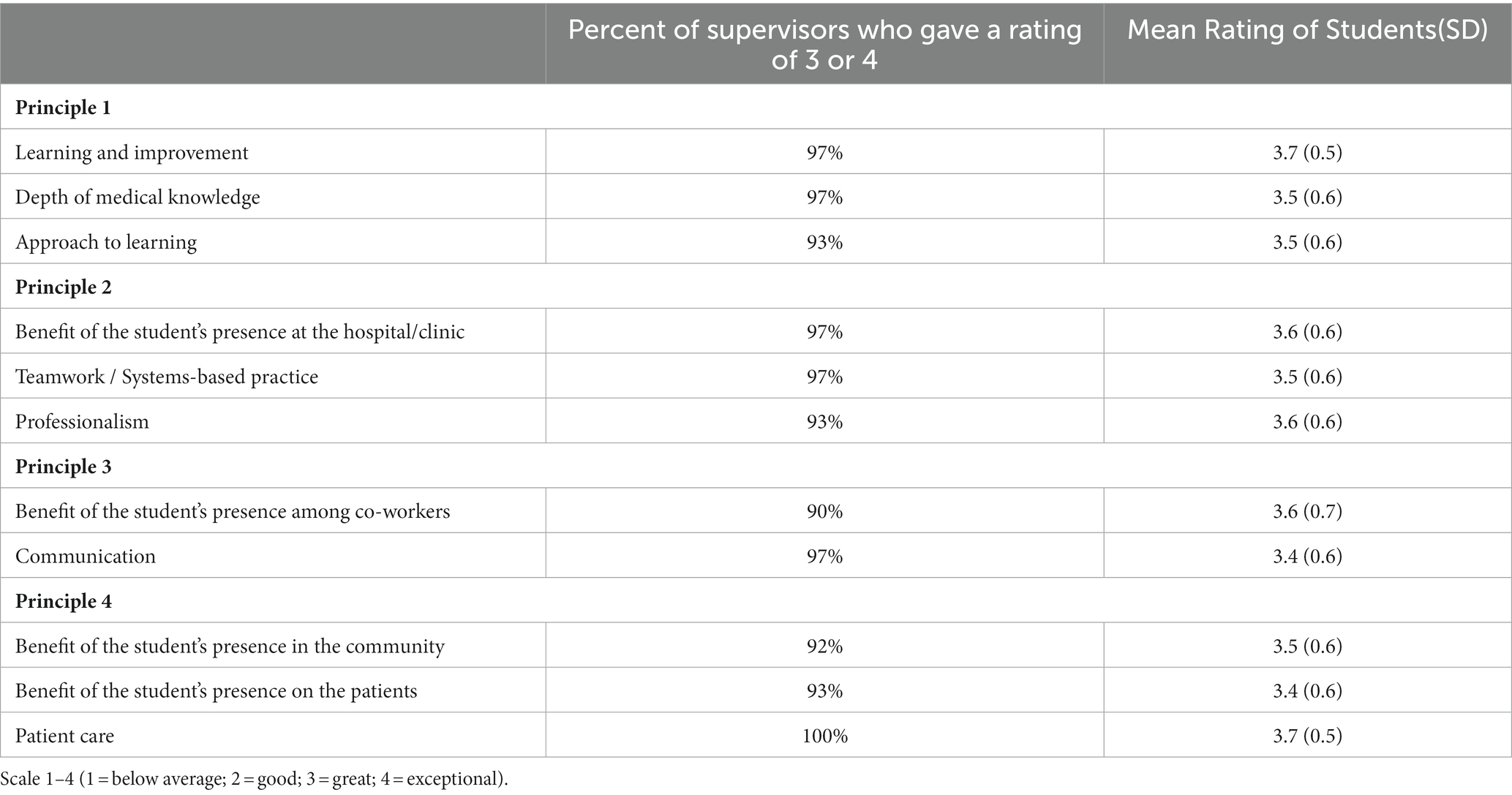
Table 4. Clinical supervisors’ perceptions (n = 30) of students’ performance and presence.
Nearly half (48%) of supervisors’ comments described students’ progression of learning. Comments included “willingness to learn,” “active engagement in seeking further details,” possessing a “strong understanding of medical knowledge,” and “very participatory, showing her interest in helping and learning new things, we are very happy to have had her in the clinic.”
All students agreed that the clinical experience contributed to their development as a physician. They agreed that they developed skills to work in collaborative practice (98%) and a greater respect for other health care professions and their roles in providing health care (98%). Students (95%) reported that their STEGH informed their medical practice, and 95% indicated they will use information from the experience in their careers.
In open-response questions, nearly half of students (46%) reflected on applying lessons and ideas from their clinical experience abroad to their practice at home. Students reflected on expanding their clinical knowledge through learning from incredible physicians and forming meaningful professional and personal relationships. They learned from an array of providers and built lifelong partnerships with their clinical team. They discussed sharing what they learned with colleagues once they were back at school.
Clinical supervisors (97%) reported that students were a benefit to the clinic. Most supervisors (97%) rated students’ performance in teamwork and systems-based practice highly and 93% rated students highly in professionalism. In addition to our students going abroad for clinical rotations, we foster bidirectional participatory relationships through established memoranda of understanding (MOU) for bidirectional educational exchanges with several of our long-term LMIC partner institutions. These exchanges support medical students from partner teaching hospitals to rotate at VUSM. Our students reciprocate the peer mentoring they receive during the course and help orient visiting students. We recognize there are other ways to further enhance bidirectional partnership, but these are the ones highlighted in this case.
Many comments from supervisors about student performance focused on collaboration and engagement with patients and the clinic. Comments that exemplified this collaboration included, “a team player, proactive and was always seeking alternative opinion for the benefit of the patients” as well as “attentive to the needs and concerns of her teammates”.
During the rotation, students collaborate with their site supervisor to identify a capstone project of mutual benefit that will strengthen local capacity. Students then build out the project, which is generally in the form of a continuing medical education (CME) presentation to clinic staff. Most of students (90%) felt the presentation was an appropriate course assignment and a way to use their skills to give back to the clinic.
In feedback forms, 90% of supervisors reported that the students’ presence was a benefit to the clinical staff. Nearly all supervisors (97%) noted that students communicated well with clinic staff and patients, although some supervisors noted language barriers and suggested that students improve their proficiency. Overall, supervisors commented that students positively contributed to strengthening aspects of the clinical group. One supervisor noted that their student was “ready and willing to learn and also share his knowledge with the rest of the team,” and another supervisor commented that “she has added depth and insight to our program.”
To further support capacity strengthening, VUSM faculty have visited sites to collaborate with clinical providers and provide additional CME opportunities. At one site, regular remote (virtual) case study conferences between LMIC clinical officers at the rural hospital and VUSM faculty physicians provide opportunities for the clinical officers to discuss and receive guidance on difficult cases from VUSM specialists. Additionally, VUSM faculty and site supervisors have presented together at international global health conferences, which helped broaden opportunities for capacity strengthening at those sites.
Particularly at clinics where we have long-standing partnerships, students participate in a variety of community outreach initiatives. Over the years, students have engaged in mobile ultrasound clinics, cataract camps, nutrition and cooking classes, dental hygiene classes at schools, sexual and reproductive education for adolescent females, and water and sanitation workshops. Students (99%) agreed that community outreach opportunities enhanced their learning experiences.
In open-response questions, 28% of students highlighted community engagement. For some students, these community experiences were a cornerstone of their learning and taught them about community-focused healthcare and how to deliver quality care. They learned how a community-based approach to health care could be integrated into the health care system and discussed the positive impact these experiences would have on their career.
The course has expanded opportunities beyond the month to include collaboration on global health case competitions, which have brought international partners to Vanderbilt to judge student proposals to address pressing issues in their communities in countries. Some of these cases have included efforts to improve non-communicable disease care through expansion of Lwala's health services in rural Kenya and to improve health outcomes through expansion of access to emergency services in rural Guyana. Medical students have also integrated the course into research immersions that span multiple months which has allowed for co-creation of research and co-authorship of publications (Starnes et al., 2018, 2021; Heerboth et al., 2020; Banerdt et al., 2021a,b).
Supervisors observed that the student’s presence benefitted the community (92%) and patients (93%). All supervisors rated their students’ performances in patient care highly. Through comments about students’ clinical performance, supervisors indicated that students engaged deeply with patients and the community. Such comments included “able to navigate the cultural nuances of medical care in rural Kenya,” “fostered a special doctor-patient connection,” and “actively participated in areas that seek to improve patient care.” Many students worked with community outreach teams to engage in community health promotion activities outside clinical time. Engagements in these community-led efforts were often mutually beneficial. One supervisor noted that the student “both gained from and contributed a lot to the [community] environment.”
This global health course was evaluated using Melby et al.’s four principles to ensure that it was aligned with best practices in the field. While frameworks like Melby et al. have been used to develop global health programs, we have not found these frameworks to be used in global health program evaluation. This paper seeks to expand use of equity frameworks to ensure cross-cultural effectiveness, mutual benefit, sustainability, and positive community impact in STEGHs.
In this evaluation, we found during the ten years that we have partnered globally with partners on the course, there have been positive outcomes for both US medical students and their host communities as evaluated by their LMIC supervisors. Based on qualitative and quantitative data, the course appears to be effective in addressing the four guiding equity principles. Student course evaluations, supervisors’ observations of students, and supervisor feedback forms indicate that students developed cultural humility, acquired foundational science knowledge and relevant skills, and were likely to change their future medical practice habits. Clinical supervisors’ observations and feedback revealed that students’ engagements with the clinic, staff, patients, and community were beneficial.
The course provides an opportunity for students to view diseases in LMICs through the lenses of population science, epidemiology, public health, and health systems. The course also encourages a bidirectional participatory relationship and capacity strengthening through local mentorship by clinicians and CME presentations by students. The combination of robust didactics, mentoring, and international clinical experience lays a strong foundation for future clinicians.
While there are multiple stakeholders of interest in evaluation of this course, our data only capture perspectives of HIC medical students and their LMIC supervisors. In the qualitative analysis of supervisors’ comments, a few supervisors had multiple students and comments were redundant or contained similar phrasing, which resulted in larger tendencies for certain trends. Additionally, not all students and supervisors provided complete course evaluations, so response bias could have influenced the results. Because communities and clients in the LMIC settings were not surveyed, we cannot measure specific impacts of the course, but LMIC supervisor feedback was used as an attempt to understand impact locally. Future studies could expand data collection to include these stakeholders. Questions and scales in the tool were slightly modified over time because of changes in the medical school evaluation approach, which decreased the amount of longitudinal data available. To compare responses across survey questions and instruments, percentages were used to quantify the data. Furthermore, course evaluations were originally developed for quality improvement purposes, so many questions focused on the relevance of didactic materials and activities as well as travel and site logistics to understand students’ needs. Additionally, during the ten years of course implementation, several improvements were made: pre-departure preparation was expanded to enhance training in cultural humility and global health ethics; online discussion boards among students at multiple sites were added; and course elements, including objectives, module videos and readings, and assessments were updated to address evolving student interests and global health topics. Despite these changes, the data was consistent from year to year.
This innovative clinical global health medical school rotation course with long-standing partners in international low-resourced settings addresses guidelines for implementing STEGH. Based on the data available from HIC student course evaluations and LMIC supervisor evaluations, we find that this model appears to be effective and impactful in preparing students for an increasingly globalized world. Future studies would benefit from evaluating the impact of this STEGH on the communities, local staff, and local students (if applicable) as well as the longer-term impact of the course on alumni. In particular, data collection focused on Principle 3 (sustainability), of which we had limited data would add further insight to the impact of this course on communities. Additionally, the course itself could be enhanced through deepening communication and partnerships with clinical sites, furthering bidirectional student exchanges, and continuing to prepare students through robust pre-departure training. While much can be gained through an intensive one-month global health course, more sustained engagement through advanced clinical training and research will likely improve skill development and strengthen bilateral partnerships That said, we believe that this could serve as a model in developing international clinical rotations to address growing interest in global health training in medical schools.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was reviewed by the Vanderbilt University IRB, which determined that the study posed minimal risk to participants and met 45 CFR 46.104 (d) category (1) for exempt review. Vanderbilt University IRB study #221706.
MM, ER, EJ, and DH contributed to the conception or design of the evaluation. ER collected and analyzed the data. MM and ER wrote the first draft of the manuscript. EJ and DH edited the manuscript. All authors contributed to the article and approved the submitted version.
We wish to thank the following supporters who played an integral role in the creation and implementation of this course: Daniel Guiles, Natasha Halasa, Douglas Morgan, Brent Savoie, Lwala Community Alliance, Jordan University Hospital, and Primeros Pasos Clinic. We also thank former Senior Associate Dean Bonnie Miller and the Vanderbilt University School of Medicine leadership for their support of this course. Additionally, we are grateful for LaToya Ford, Annesa Dey, Meira Kowalski, and Yujia Ji who helped with data collection and analysis.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^ACGME milestones include Patient Care PC2A & PC7A; Interpersonal and Communication Skills IPCS7B & IPCS7B.1; Medical Knowledge MK2A, MK2B, MK7A, MK7B, & MK7C; Practice-based Learning and Improvement PBLI3 & PBLI3A; Systems-Based Practice SBP2A; AND Professionalism PR1B.
Banerdt, J. K., Mateyo, K., Wang, L., Lindsell, C. J., Riviello, E. D., Saylor, D., et al. (2021b). Delirium as a predictor of mortality and disability among hospitalized patients in Zambia. PLoS One 16:e0246330. doi: 10.1371/journal.pone.0246330
Banerdt, J. K., Mateyo, K., Yan, Y., Liu, D., Zuo, Y., Di Gravio, C., et al. (2021a). Risk factors for delirium among hospitalized patients in Zambia. PLoS One 16:e0249097. doi: 10.1371/journal.pone.0249097
Crump, J. A., and Sugarman, J. (2010). The working group on ethics guidelines for Global Health training (WEIGHT). Global health training ethics and best practice guidelines for training experiences in global health. Am. J. Trop. Med. Hyg. 83, 1178–1182. doi: 10.4269/ajtmh.2010.10-0527
Dahlman, K. B., Weinger, M. B., Lomis, K. D., Nanney, L., Osheroff, N., Moore, D. E., et al. (2018). Integrating foundational sciences in a clinical context in the post-clerkship curriculum. Med. Sci. Educ. 28, 145–154. doi: 10.1007/s40670-017-0522-1
Drain, P. K., Aron Primack, D., Hunt, D., Fawzi, W. W., Holmes, K. K., and Gardner, P. (2007). Global health in medical education: a call for more training and opportunities. Acad. Med. 82, 226–230. doi: 10.1097/ACM.0b013e3180305cf9
Drain, P. K., Holmes, K. K., Skeff, K. M., Hall, T. L., and Gardner, P. (2009). Global health training and international clinical rotations during residency: current status, needs, and opportunities. Acad. Med. 84, 320–325. doi: 10.1097/ACM.0b013e3181970a37
Eichbaum, Q. G., Adams, L. V., Evert, J., Ho, M.-J., Semali, I. A., and van Schalkwyk, S. C. (2021). Decolonizing global health education: rethinking institutional partnerships and approaches. Acad. Med. 96, 329–335. doi: 10.1097/ACM.0000000000003473
Heerboth, S. A., Hennessey, C., Omondi, B., Wafula, M., Mbeya, J., Rogers, A., et al. (2020). Knowledge of obstetric and neonatal danger signs among community health workers in the Rongo Sub-County of Migori County, Kenya: results of a community-based cross-sectional survey. Afr. J. Reprod. Health 24, 121–132. doi: 10.29063/ajrh2020/v24i1.13
Macfarlane, S. B., Jacobs, M., and Kaaya, E. E. (2008). In the name of global health: trends in academic institutions. J. Public Health Policy 29, 383–401. doi: 10.1057/jphp.2008.25
Melby, M. K., Loh, L. C., Evert, J., Prater, C., Lin, H., and Khan, O. A. (2016). Beyond medical “missions” to impact-driven short-term experiences in global health (STEGHs): ethical principles to optimize community benefit and learner experience. Acad. Med. 91, 633–638. doi: 10.1097/ACM.0000000000001009
Merson, M. H., and Page, C. (2009). The dramatic expansion of university engagement in Global Health: implications for U.S. policy. Washington, DC: Centre for Strategic and International Studies.
Prasad, S., Aldrink, M., Compton, B., Lasker, J., Donkor, P., Weakliam, D., et al. (2022). Global health partnerships and the Brocher declaration: principles for ethical short-term engagements in global health. Ann. Glob. Health 88:31. doi: 10.5334/aogh.3577
Rowson, M., Smith, A., Hughes, R., Johnson, O., Maini, A., Martin, S., et al. (2012). The evolution of global health teaching in undergraduate medical curricula. Glob. Health 8, 35–38. doi: 10.1186/1744-8603-8-35
Shah, S., Lin, H. C., and Loh, L. C. (2019). A comprehensive framework to optimize short-term experiences in global health (STEGH). Glob. Health 15, 1–8. doi: 10.1186/s12992-019-0469-7
Starnes, J. R., Chamberlain, L., Sutermaster, S., Owuor, M., Okoth, V., Edman, W., et al. (2018). Under-five mortality in the Rongo Sub-County of Migori County, Kenya: experience of the Lwala community Alliance 2007-2017 with evidence from a cross-sectional survey. PLoS One 13:e0203690. doi: 10.1371/journal.pone.0203690
Starnes, J. R., Wamae, J., Okoth, V., Ressler, D. J., Were, V., Were, L. P. O., et al. (2021). Population-based socio-demographic household assessment of livelihoods and health among communities in Migori County, Kenya over multiple timepoints (2021, 2024, 2027): a study protocol. PLoS One 16:e0256555. doi: 10.1371/journal.pone.0256555
Keywords: global health, medical education, foundational science, international rotation, health equity
Citation: Martin MH, Rose ES, Jahangir E and Heimburger DC (2023) Ten-year evaluation of an immersive global health medical school course using a four-principle equity framework. Front. Educ. 8:1200389. doi: 10.3389/feduc.2023.1200389
Edited by:
Benedicta Ayiedu Mensah, University of Ghana, GhanaReviewed by:
Martin Nyaaba Adokiya, University for Development Studies, GhanaCopyright © 2023 Martin, Rose, Jahangir and Heimburger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie H. Martin, bWFyaWUuaC5tYXJ0aW5AdnVtYy5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.