
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ. , 05 January 2024
Sec. Special Educational Needs
Volume 8 - 2023 | https://doi.org/10.3389/feduc.2023.1183994
This article is part of the Research Topic Educational Approaches for Promoting Neurodivergent Health, Well-Being, and Thriving Across the Life Course View all 9 articles
 Marianne Pugatch1*†
Marianne Pugatch1*† Nathan J. Blum2William J. Barbaresi3
Nathan J. Blum2William J. Barbaresi3 Jonathan Rowe4Mark Berna1
Jonathan Rowe4Mark Berna1 Sean Hennigan1
Sean Hennigan1 Alison Giovanelli1
Alison Giovanelli1 Carlos Penilla1Kathleen P. Tebb1Megan Mott5Vikram Kumaran6
Carlos Penilla1Kathleen P. Tebb1Megan Mott5Vikram Kumaran6 Sara Buckelew1James C. Lester4Elizabeth Ozer1,7
Sara Buckelew1James C. Lester4Elizabeth Ozer1,7Background: Attention deficit hyperactivity disorder (ADHD) affects about 13% of adolescents and is associated with substance use-related morbidity and mortality. While evidence on effective interventions to reduce alcohol use among adolescents with ADHD is limited, parent-teen communication about alcohol use has been found to be protective. Other approaches, such as educational interventions, hold promise to reduce alcohol-related harms in adolescents with ADHD. Digital technology offers an innovative approach to health behavior change, expanding access to services and may promote learning for neurodiverse youth, including teens with ADHD. INSPIRE, a narrative-centered game-based behavior change environment designed to promote self-regulation and self-efficacy to prevent risky alcohol use has been found to engage a general adolescent population. The goals of this pilot study are (1) to examine the engagement of youth with ADHD in INSPIRE; and (2) to examine if INSPIRE fosters parent-teen communication.
Method: Adolescents diagnosed with ADHD aged 14–16 were recruited from developmental medicine clinics and invited to a focus group offered via Zoom. Participants completed a pre-survey, interacted with the INSPIRE game, and answered a post-survey as well as open-ended questions about their gaming experience during the focus group. Engagement was measured through both self-report using subscales from the User Engagement Scale and computer data; survey and qualitative data collected information on parent-teen communication. Univariate statistics described adolescent characteristics, Rank-sum and Fisher’s exact tests examined relationships among variables, and qualitative analysis identified themes in open-ended questions.
Results: Of adolescent participants (N = 40), 45% identified as female, 17.5% Black, 7.5%, Hispanic, and 62.5% White. Post-survey mean engagement subscales of Usability (on a 5-point scale) was 3.67 (SD = 0.74), and Satisfaction was 3.63 (SD = 0.75). Computer data indicated that participants played the game for a median of 24 min. Adolescents shared that playing the game strengthened refusal skills and their ability to navigate social gatherings with alcohol. Post-survey, 63% planned to share information from INSPIRE with a parent.
Conclusion: Findings suggest that INSPIRE may support facilitating youth with ADHD to learn the developmental competencies needed to mitigate risk and thrive. INSPIRE warrants further testing to explore its impact on alcohol use in youth with ADHD.
Attention deficit hyperactivity disorder (ADHD) affects approximately 8–10% of school-age children (Barbaresi et al., 2004) and 13% of adolescents (Centers for Disease Control and Prevention., 2016; Bitsko et al., 2022), often persisting into adulthood (Barbaresi et al., 2018). Individuals with ADHD encounter challenges throughout the life course related to lower educational and occupational attainment, difficulties in relationships, substance abuse, and a five-fold increased risk of death by young adulthood (Dalsgaard et al., 2015). Substance use is highly prevalent in youth with ADHD (Ohlmeier et al., 2008). Adolescents with ADHD may struggle disproportionately with substance use across the life course due to barriers to quality healthcare (Wright et al., 2015), including insufficient resources, challenges in obtaining health information, as well as gaps in the receipt of diagnosis from providers and schools (Fridman et al., 2017). Co-occurring substance use is a significant risk factor for many challenging adult outcomes. Youth with ADHD who start using alcohol and other drugs earlier are more likely to have alcohol-related problems and to develop substance use disorders (Charach et al., 2011; Lee et al., 2011; Harstad et al., 2020). The maturing neural circuitry during adolescence heightens the impact of alcohol exposure on regions of the brain sensitive to drugs and those regions involved in reward (Barkley, 1997; Sisk and Foster, 2004; Sibley et al., 2014). Thus, adolescence is an important sensitive period for alcohol and substance use in life course health development, and interventions to prevent or delay alcohol use in youth with ADHD have the potential to dramatically improve adult outcomes and to support thriving across the life course.
The Society for Developmental-Behavioral Pediatrics ADHD practice guideline recommends clinicians engage in substance use prevention strategies with adolescents but notes an absence of evidence on effective interventions in this group. The guideline recommends that clinicians utilize interventions that were developed for adolescents in general (Barbaresi et al., 2020). Consistent with the Bright Futures Guidelines for screening and counseling for substance use for adolescents (American Academy of Pediatrics, 2017), behavior change interventions that show promise include brief interventions indicating a small to moderate effect for up to 1 year (Steele et al., 2020; Tanner-Smith and Lipsey, 2015; O’Connor et al., 2018).
Research on alcohol and substance use prevention has identified the importance of parents1 to support healthy behavior in adolescents. Several factors, including parental modeling, good parent-child relationship quality, parental involvement and support, and general communication, are associated with delaying early alcohol initiation and reduced levels of later drinking by adolescents (Ryan et al., 2010; Cox et al., 2018). Among adolescents with ADHD, a potentially important protective factor includes frequent alcohol-specific communication with parents, while a risk factor includes permissive parental messages regarding alcohol use (Booth-Butterfield and Sidelinger, 1998; Reimuller et al., 2011). Recent literature indicates that parents of adolescents with ADHD lack knowledge regarding the facilitation of alcohol-specific conversations (Harstad et al., 2020).
With the goal of enhancing wellbeing across the life course, there has been a recent call to develop innovative technology interventions to promote health behavior change in adolescents and young adults (Harris et al., 2017; Ozer and Lester, 2020; Wong et al., 2020). In general adolescents engage in high rates of video game play and find digital technologies appealing (Anderson and Jiang, 2018), including in healthcare settings (Wozney et al., 2018). Pediatric digital health interventions to promote and maintain behavior change have been found to be impactful (Hieftje et al., 2013) and their effect is larger than that of educational interventions alone (Cushing and Steele, 2010). The growing interest in supporting the health and wellbeing of youth with ADHD by leveraging digital technologies that already captivate their attention (Fogler et al., 2017; Davis et al., 2018) provides a unique opportunity.
The few youth alcohol prevention digital technology interventions in the literature are primarily in design and development phases (Lyk et al., 2020; Prediger et al., 2021; Nicholas et al., 2022; Osilla et al., 2023). One innovative example of this technology in a general adolescent population is INSPIRE2 (Ozer et al., 2020). INSPIRE is a narrative-centered behavior change environment designed to reduce risky alcohol use by promoting the acquisition of knowledge of alcohol risk, self-efficacy, and self-regulation skills. INSPIRE is grounded in social cognitive theory (Bandura, 1986) which has been applied across the life course to diverse populations (Ozer, 2022). According to Social Cognitive Theory, personal efficacy, beliefs in one’s capabilities to organize and execute specific courses of action, plays a pivotal role in determining behavior (Bandura, 1982; Ozer and Bandura, 1990). Perceived self-efficacy is a strong predictor of behavior; people tend to avoid activities they believe they cannot carry out and engage in activities they judge themselves capable of handling. The INSPIRE game is designed to increase players’ ability to set goals, adopt problem-solving strategies, reason about the consequences of their actions, and reflect on their observed outcomes to adjust their future behaviors. In INSPIRE, players enhance their self-efficacy through mastering a series of increasingly challenging scenarios and exploring alternative strategies for handling alcohol-related situations in the branching storyline. The interactive narrative has been designed to foster increased self-regulation, a key component of social cognitive theory, through setting and monitoring goals, gaining strategic knowledge (ways of refusing alcohol) and declarative knowledge (the risks and potential consequences of consuming alcohol), and reflecting upon prior decisions (Ozer et al., 2020). INSPIRE has several in-game tools to support enhancing self-regulation and players are encouraged to make decisions aligned with their stated goals by stopping and thinking about how their choices may support these goals.
In INSPIRE, players adopt the role of a teenage protagonist who “relives” the events and decisions of a high-school get-together involving alcohol. Players interact with a cast of virtual characters who model various health behaviors. The outcomes for the protagonist, his/her friends, and the storyline are actively shaped by the player’s decisions. Once adolescents leave the game and return to their life, it is hypothesized that having acquired knowledge of alcohol and practiced behavioral competencies in a simulated environment with peer pressure, they are better prepared to translate their behavior to make healthy choices around alcohol use in their life.
An essential step to promote learning and behavior change through digital technology tools is to engage adolescents in the intervention (Couper et al., 2010; Giovanelli et al., 2023). The INSPIRE game was iteratively developed with input from over 200 adolescents, including obtaining their perspectives on characters, dialog, and usability of game techniques. INSPIRE has been shown to foster engagement in a general population of adolescents (Ozer et al., 2020), but it has not been studied in youth with ADHD. The primary aim of this research is to examine the engagement of youth with ADHD in the INSPIRE game using both quantitative and qualitative methods. A secondary aim of this pilot study is to examine if the intervention supports adolescent communication with parents regarding alcohol use after the INSPIRE game.
This pilot study took place over 6 months (February to August 2022) with participants recruited from a large children’s hospital in the Mid-Atlantic Region. The electronic health records for adolescents seen in the Division of Developmental and Behavioral Pediatrics and/or by physicians or psychologists in the Hospital’s ADHD program were queried to identify patients who met the following eligibility criteria: (1) Age 14.5 to 16 years; and (2) visit diagnosis of ADHD (any subtype). As the study is focused on the engagement in INSPIRE of adolescents with ADHD, records were excluded if the child had a diagnosis of autism spectrum disorder, pervasive developmental disorder, or intellectual disability. Participants who were non-English speaking were also excluded. Parents were notified of the opportunity for youth to participate by email (if an email address was available) or regular mail. Recruitment occurred in 3 waves of emails/letters. Due to the under-recruitment of females in the first two waves, the third wave of recruitment only included females.
This study involving human participants was reviewed and approved by the Institutional Review Board (IRB) at the University of California San Francisco. The participants’ parents provided their written informed consent, and participants provided assent to participate in this study.
Families of eligible youth who received the recruitment letter or email were asked to contact the study team (MP) if the adolescent was interested in partnering with the study team to learn about developing an interactive computerized game for teenagers that focused on teenage health and wellbeing and particularly decreasing alcohol use. Parents and youth were informed that participation through Zoom would take approximately 1 hour and involved completing a pre-survey, interacting with the INSPIRE game, answering a post-survey, and then participating in a brief group discussion of four open-ended qualitative questions.3 Two study team members (MP and SH) led participants in the Zoom focus group, guiding participants through the multiple methods of data collection, and utilizing PowerPoint slides to provide linkage to the pre-post surveys, the INSPIRE gaming platform, and qualitative questions. If during gameplay, an adolescent experienced a technical issue, the study research associate (SH) and the on-call study computer scientist and researcher (MB) would support the adolescent in troubleshooting and resolving the issue. Adolescents received a $25.00 gift card for their participation.
INSPIRE enables youth to actively participate in unfolding storylines to enhance self-efficacy for navigating potentially risky social situations and self-regulation skills (Ozer et al., 2020). During the study, subjects played the INSPIRE game which also served as a data collection tool. As the participants play INSPIRE, detailed computer logs of in-game behaviors are time-stamped and recorded, called trace log data. Trace log data enable an understanding of how adolescents engaged with the game and enacted behavior change-related decisions (Ozer et al., 2020) by capturing the player’s actions in the game. This granular view of in-game behaviors at the event level provides a window into participants’ engagement.
Trace log data provides information on time spent playing the game, such as:
1. Total time playing the game in minutes.
2. Time spent choosing goals for the protagonist’s behavior during the game. At the outset of the game, players select three goals for the evening (e.g., stay in control, have a chill night with friends, do not get in trouble) that apply to the events of the storyline and are intended to guide adolescent’s decision making during problem-solving episodes in the unfolding storyline.
3. Time spent engaging with “knowledge objects” in the game. There are three knowledge objects labeled: (1) “Cookies,” which impart information about the comparative caloric value of cookies to alcohol; (2) “Guitar,” which imparts information about the effects of alcohol on the teen brain; and (3) “Keys,” which impart information about alcohol use and accidents.
Trace log data tracks the number of times a player clicks on knowledge objects and what goals the player chooses for the protagonist’s goals for the evening. Trace log data also records whether the player decides to have the protagonist accept alcohol during the game.
The pre-game survey included:
• Adolescent self-report measures including demographic variables of adolescent age, gender identity, race, ethnicity (Ozer et al., 2020), and parent educational level. Adolescents were asked about the frequency and quantity of current and past alcohol use (Centers for Disease Control and Prevention., 2016), as well as the use of medication for ADHD.
• Questions regarding the frequency of parent-teen communication regarding alcohol:
How do you think your parents or caregivers feel about you drinking alcohol occasionally? with three item options to choose from, 1. Not disapprove, 2. Disapprove, 3. Strongly disapprove (Miech et al., 2020). How often do you have a discussion with your parent(s) or caregivers about alcohol use? with five possible item answers, including About once every few weeks, About once every few months; About once a year; Never have had a conversation with them about alcohol use, and Unsure.
The post-game survey included:
• Questions from the validated and reliable User Engagement Scale (UES) (O’Brien and Toms, 2010; Wiebe et al., 2014; O’Brien et al., 2018), including the satisfaction subscale with items reflecting involvement and novelty (O’Brien and Toms, 2010; O’Brien et al., 2018). Items adolescents were asked on satisfaction included Playing the game was worthwhile and The gaming experience was fun, measured on a five-point Likert scale with a 3 indicating the game was satisfying. Satisfaction (5 items; α = 0.89). Adolescents were also asked questions from the Perceived Usability subscale of the UES with items reflecting cognitive and affective dimensions about ease of game use. Items adolescents were asked on usability included I felt frustrated while playing the game and, The gaming experience was demanding, measured on a five-point Likert scale with a 3 indicating the game was easy to use. Usability (7 items; α = 0.85).
• The following questions on character relatedness (Ozer et al., 2020):
1. How much was Max (the protagonist) like you? on a three-point scale ranging from Not at all like me to Very much like me.
2. Please choose the approach that best describes how you selected the dialog choices that Max made while exploring the narrative with discreet choices, including:
I chose dialog for myself if I were in Max’s situation.
I chose dialog that I thought Max would choose, based on what I know about him.
I chose dialog options that seemed most interesting to watch unfold.
• One item about information the adolescent would share with parents is, Is there information learned from this game that you will discuss with a parent or caregiver? with three answers No, Some, and A lot.
Following gameplay and completion of the post-survey, the study team (MP and SH) led participants in qualitative data collection consisting of a brief discussion of four open-ended questions developed by INSPIRE study team members. Adolescents were reminded that the information shared was confidential and would be anonymized. Questions were designed to elicit feedback and understand what adolescents learned in the game that might contribute to the further development of the game as well as to provide important information about the secondary aim of the research study—what adolescents might share with a parent post-game play. Questions included:
• Share one experience from the INSPIRE game that you might like to share with others.
• Name one thing from INSPIRE game that a teen participant playing the game might share with a parent.
• Name one thing from the INSPIRE game that a teen participant playing the game might share with a friend.
The two study team members (MP, SH) recorded notes by hand. Post focus group, the study team members compared and reached a consensus for qualitative notes. Anonymized focus group notes and summary documents were compiled (SH).
Trace log data capturing students’ time-stamped interactions were downloaded from the INSPIRE software. The data was cleaned, and a set of descriptive variables were distilled from the logs to enable an analysis of participant engagement with the game. Data were coded through R and transferred to and analyzed in Stata statistical software (Baum, 2006). Descriptive statistics were run, and alcohol risk prevention was modeled by looking at the relationships between survey data (reported alcohol use in real life, parent disapproval of alcohol) and acceptance of in-game alcohol. T-tests, Rank-sum tests, Kruskal–Wallis tests and Fisher’s exact tests were used to examine bivariate relationships.
Qualitative data analysis involved two coders analyzing responses to open-ended questions posed to adolescent participants. Coding was grounded in a content analysis that reflected research questions, including respective codes for (1) engagement and (2) conversations with parents about alcohol. Other codes were mapped to social cognitive theory (e.g., vicarious learning, mastery, self-regulation, and self-efficacy). Coders individually reviewed transcripts, met to compare, discuss, and reach a consensus on identified codes, and then developed themes (Beebe, 2001).
Of 1,929 families sent emails or letters, 73 (about 4%) responded with interest. Of those who responded, 49 (67%) consented to play the INSPIRE game. Forty-six youth participated in 10 focus groups between February 2022 and August 2022. Forty adolescents (55%) age 14–16 years were included in the final analysis (Figure 1).
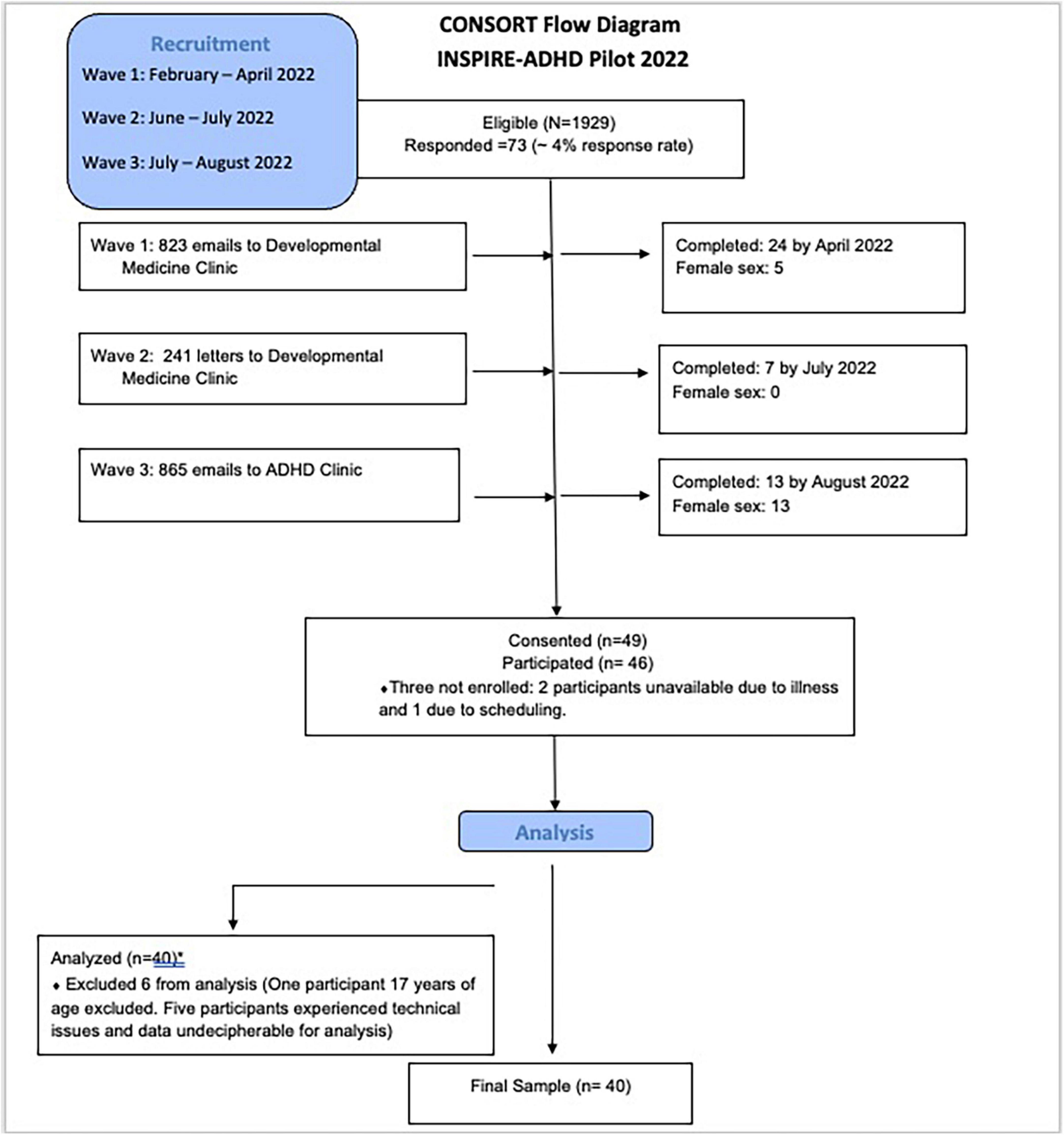
Figure 1. Consort flow diagram for pilot study of INSPIRE in adolescents diagnosed with ADHD.
Of the adolescent participants (n = 40), 35% self-identified as female, and 45% self-identified as female sex at birth. The race-ethnicity of the participants included 17.5% African American or Black, 7.5% Hispanic or Latino, 62.5% White, and 12.5% of multiple race-ethnicities. More than half (62.5%) of the adolescent participants reported taking a prescription medication given by a doctor for their ADHD; of the adolescent participants who took medication, 68% reported that they took prescription medications for ADHD that day (Table 1).

Table 1. Characteristics of adolescents with ADHD (N = 40).
Of the teens who participated in the study, 25% reported having ever used alcohol. This use did not vary by gender, age, or race-ethnicity. About 90% of adolescents with ADHD reported that their parents disapproved of occasional drinking.
In the post-game survey, 70% of the adolescents reported that Max, the main protagonist in the game, was somewhat or very much like them. Eighty percent of adolescents with ADHD reported playing the game as themselves (I chose dialog options I would have selected for myself if I were in Max’s situation).
Pre-game, 65% of adolescents reported never communicating with their parents about alcohol or only speaking about alcohol with parents once a year. Post-game, 62.5% reported that they would share at least some information from the INSPIRE game with their parents.
Engagement, measured by the self-report subscales of the User Engagement Scale, indicated that participants’ mean usability, which assesses ease of use of the game, was 3.67 (SD = 0.74), and satisfaction was 3.63 (SD = 0.75) on a 5-point Likert scale. Usability and satisfaction did not differ by the age, sex, or race-ethnicity of the participants (Prob > | Z| = 0.2) for all non-parametric Rank-sum tests (Table 2).
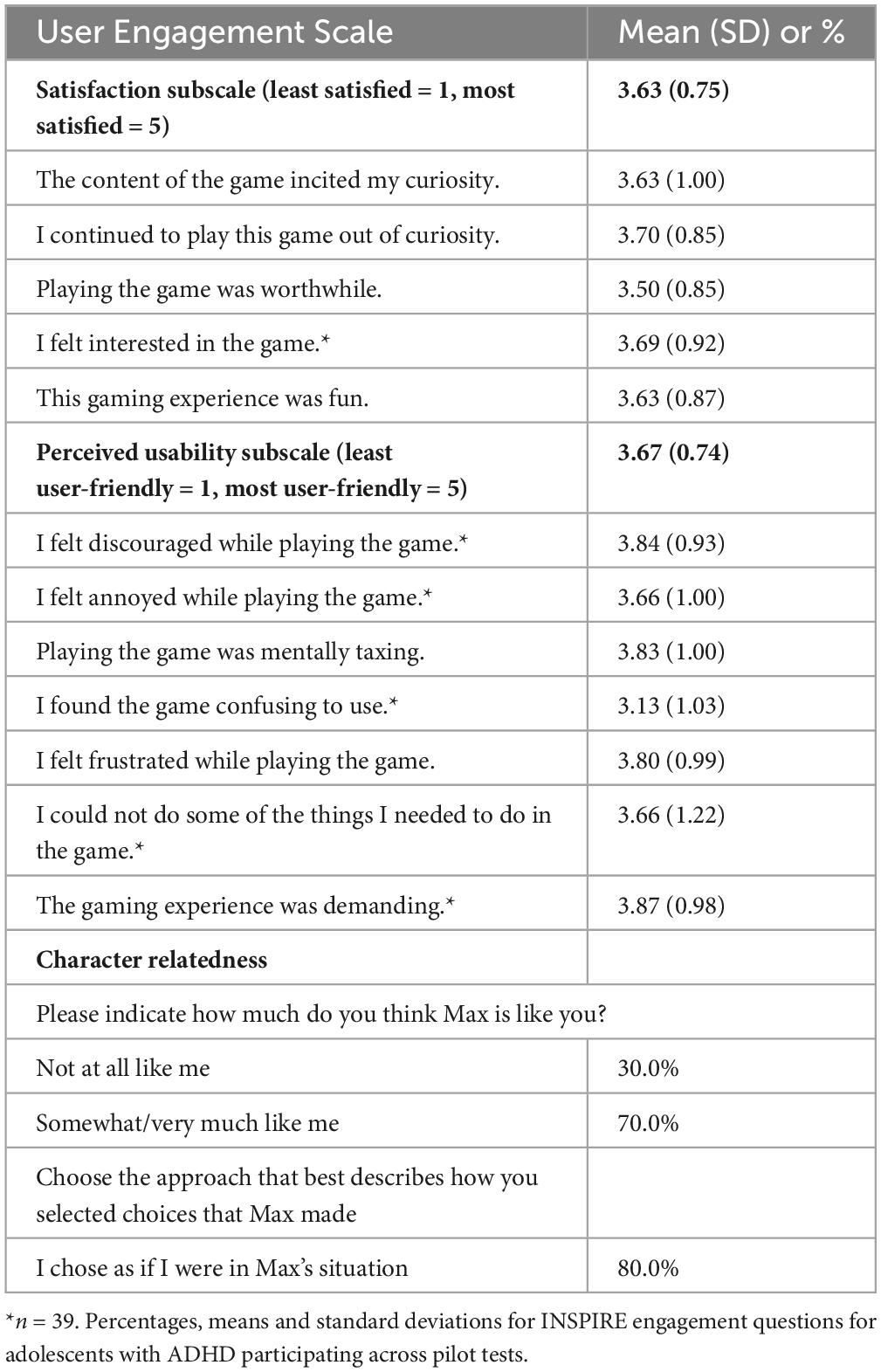
Table 2. Survey results of engagement N = 40.
Engagement, as measured by trace log data, includes the users’ total time spent playing the game, choosing goals, making dialog choices, and both the time and number of clicks by users on knowledge items. Trace log data indicated adolescents (n = 39) completed playing the game in 24.3 [6.6] minutes.4 The time it took adolescents with ADHD to complete the INSPIRE game did not differ by age, sex, or race-ethnicity, (Prob > | Z| = 0.7) for all non-parametric Rank-sum tests (Table 3).
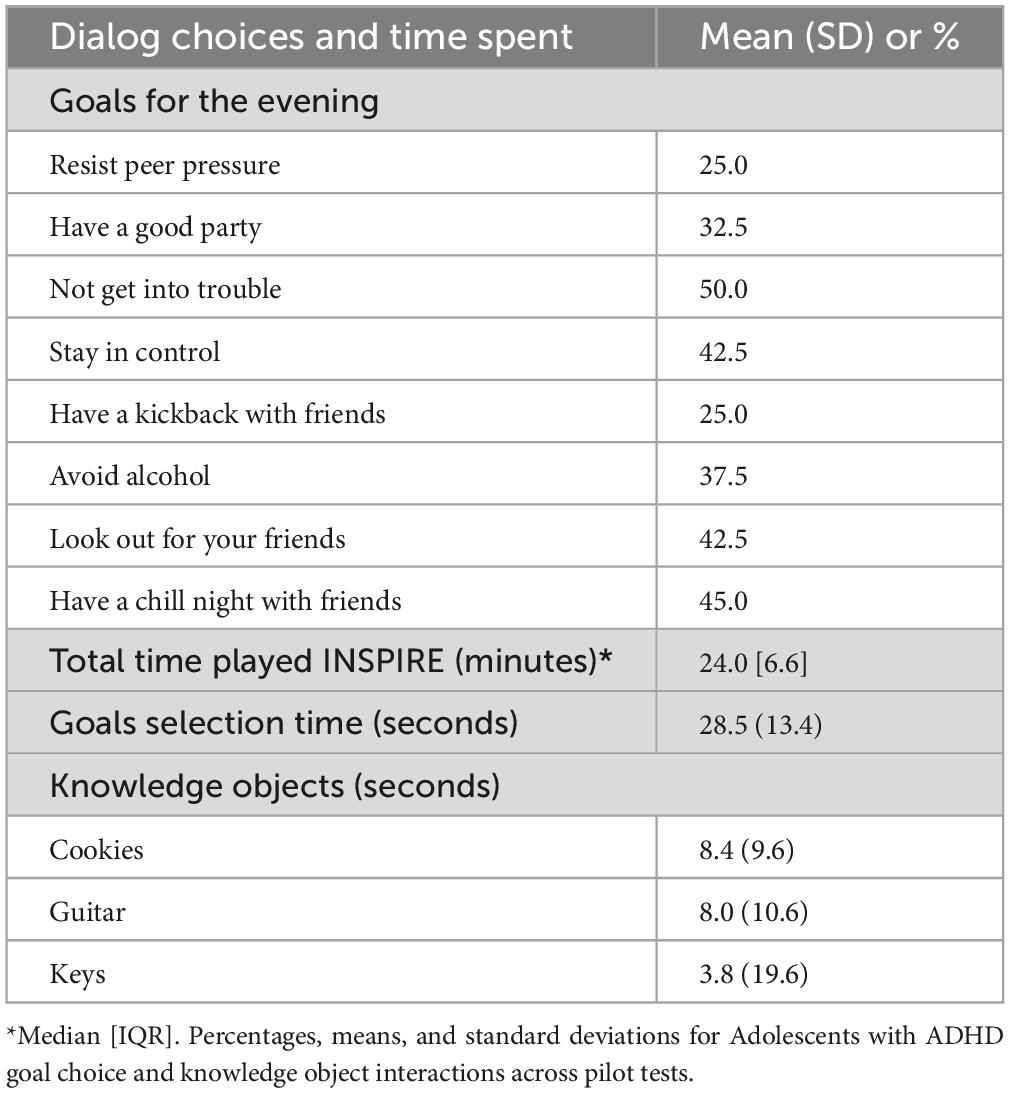
Table 3. Trace log data results of engagement (N = 40).
Participants engaged with three knowledge objects (cookies, guitar, and keys). The participants clicked on the knowledge objects between 0 and 9 times with a mean of 3.8 (1.9) clicks.
At the outset of the game, adolescents with ADHD chose their top three goals for the evening. The top two were “Do not get in trouble” (50%) and “Have a chill night with friends” (45%). “Look out for your friends” and “Stay in control” (42.5%) were tied for the third most chosen goals for the evening. Goal selection time took between 5.3 and 82.4 seconds.
Among these adolescents with ADHD, 22.5% made dialog choices to accept in-game alcohol use. Further, 50% of those teens who ever drank alcohol in real life accepted alcohol in the game compared to only 13.3% of those who never reported drinking alcohol in the real world (Fisher’s exact p = 0.029).
The focus group qualitative questions yielded information that deepened our understanding of what adolescents with ADHD learned from INSPIRE, querying about what they might share with others, including friends and parents. Enhancing the quantitative survey item on discussions with parents, the open-ended questions provided additional insight into the content of what they would share with parents and how collaborative parent-teen communication may further foster the acquisition of key developmental competencies (Table 4). Four themes were identified in the qualitative data, displayed in Table 4. First, adolescents discussed how the game facilitates parent-teen communication, particularly with regard to navigating social situations. A second theme was the adolescents’ engagement in the game through their relatedness to the virtual characters, as demonstrated by the strength of their emotional affinity to the INSPIRE characters. Third, adolescents discussed vicarious learning in a virtual environment, commenting on how “real” their emotions felt, including anxiety when responding to the main protagonist experiencing peer pressure to drink alcohol. Fourth, adolescents’ discussed building mastery in a virtual environment through experiences involving alcohol-risk situations.
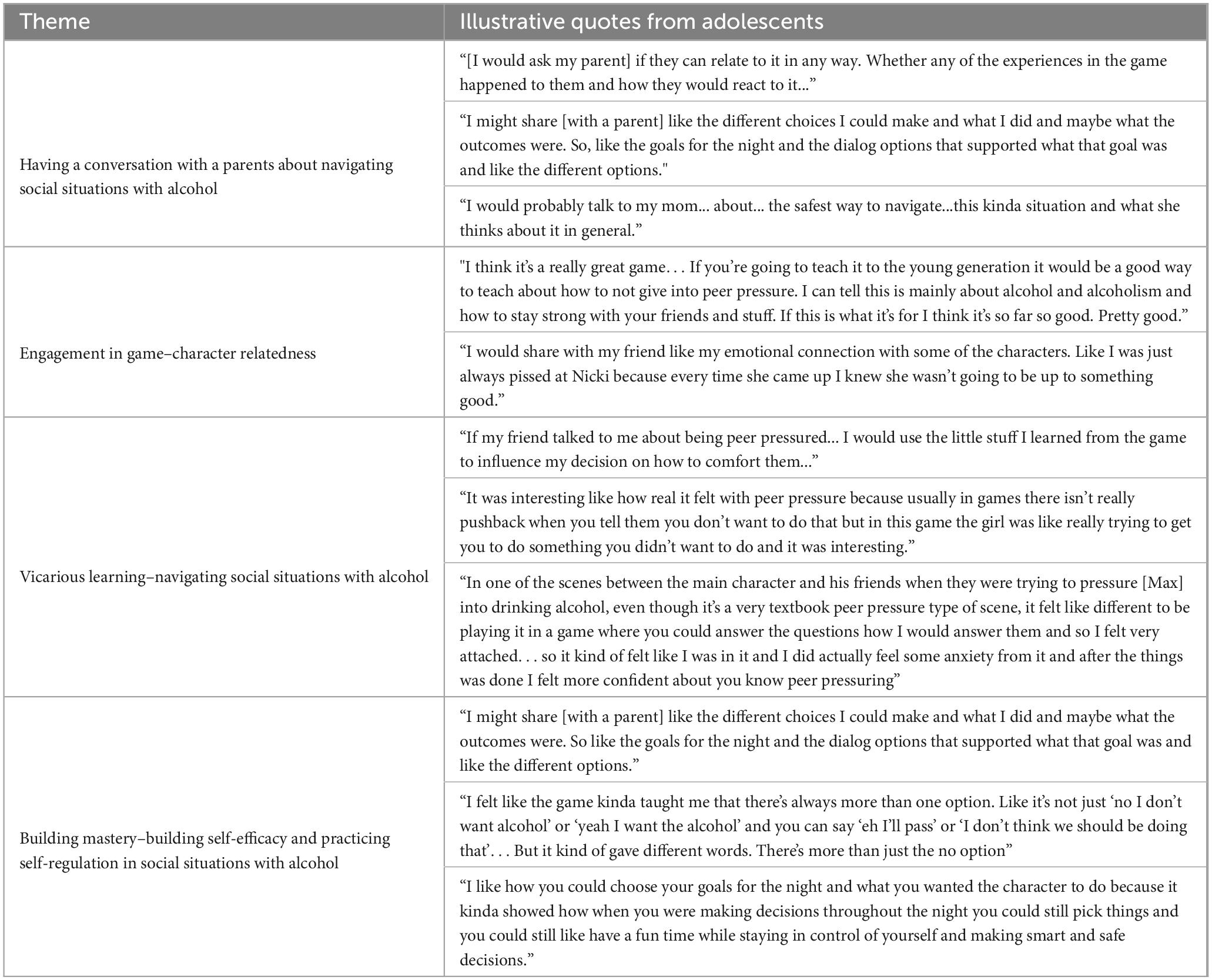
Table 4. Qualitative results: engagement with inspire and information shared with a parent.
This paper describes a novel approach to alcohol risk prevention intervention that shows promise to fill a gap in the literature to mitigate the alcohol risk trajectory for adolescents with ADHD. INSPIRE was engaging for adolescents with ADHD, and their results were similar to those found in a general group of adolescents. Specifically, most teens with ADHD played the game and explored knowledge objects for a similar amount of time to adolescents in a general population. Further, as in a general population, most youth with ADHD chose to play the game as themselves (Ozer et al., 2020). User Engagement Scale results in youth with ADHD were similar to previous general adolescent study populations (mean usability 3.59: and mean satisfaction 3.55 and 3.57) (Ozer et al., 2020; Pugatch et al., 2022). Adolescents with ADHD selected similar goals for the evening as adolescents in the general population (e.g., were most likely to choose “Stay in control” and “Not get in trouble”).
Post-INSPIRE gameplay, adolescents with ADHD were eager to talk with their parents about alcohol risk scenarios, a known protective factor for youth with ADHD (Harstad et al., 2020). Specifically, they expressed wanting to share knowledge and problem-solve about how to deal with peer pressure effectively and to develop skills in personal efficacy and regulation. Consistent with this qualitative data, survey data reinforced adolescents’ desire to communicate with parents about alcohol risks post-game, as a majority of youth reported that they wanted to share information they learned in the game with their parents. Adolescents’ inclination to discuss with parents what they observed in the game, as well as talk through strategies to refuse alcohol and watch out for friends, may facilitate and bolster known alcohol prevention protective factors (e.g., parental support, frequent communication regarding alcohol use, parental modeling) (Ryan et al., 2010; Reimuller et al., 2011; Cox et al., 2018).
Adolescent discussions in the focus groups post-game play suggest that adolescents were incorporating the central points of the intervention. Adolescents with ADHD may learn from the INSPIRE game how to navigate peer pressure with alcohol at a house party, including strengthening refusal skills and practicing setting goals and aligning behavioral choices with these goals.
Of interest, we found significantly different frequencies in game-based drinking behavior depending on past reported alcohol use. Specifically, adolescent participants with ADHD who had ever drunk alcohol in real life were significantly more likely to choose to drink in-game alcohol than those adolescent participants with ADHD who never had drunk alcohol previously outside of the game. This pattern has not yet been examined in a general group of youth playing INSPIRE and would be useful to look at this population as well. In future work, with larger numbers of adolescents with ADHD, analyzing the in-game alcohol use choices of adolescents in real-time with computer log data and examining this subgroup’s alcohol use behavior longitudinally in real life could be instructive. INSPIRE may provide a particularly high-risk group of teens the opportunity to learn to make different choices once they return to their lives.
In this pilot study, it was feasible to recruit the target population of youth with ADHD and technical challenges were mitigated. The youth found the intervention acceptable to play. Triangulation of the engagement subscales, trace log data, and qualitative data demonstrate a strong multidimensional measure of engagement. Another strength of this study is that almost half of the participants were female, an understudied group with ADHD (Hinshaw et al., 2022). We found no differences in engagement across youth characteristics, although due to the small sample size, we could not determine differences across all categories of race and ethnicity. In future work, it will be important to test INSPIRE with a larger, more diverse sample of youth across race, ethnicity, sex, gender, and socioeconomic status to establish equitable access to the most vulnerable adolescents with ADHD. There are many potential advantages to the INSPIRE approach regarding equitable dissemination through the digital online platform. Scalability in clinical preventive services has a broad reach with the potential to reach adolescents with public and private insurance and achieve population-level impact, as well as the flexibility to use across settings with diverse populations. Future research is needed to test if the INSPIRE game impacts adolescents’ self-efficacy and real-life alcohol risk in adolescents with ADHD.
The present study has limitations, including that it is a pilot study examining the engagement of youth with ADHD using descriptive statistics and did not examine the impact of the intervention on alcohol use in real life. Further, it is comprised of a small sample focused on youth with ADHD in developmental medicine clinics in one children’s hospital in the mid-Atlantic US region. Therefore, our findings may not apply to other types of settings or be representative of US youth with ADHD. The low response rate may reflect the broad email and mail recruitment method, suggesting that a more targeted personal approach might yield improved results. We did not receive any responses explicitly declining study participation. While the study encourages youth to share information about alcohol use with parents, specific parent-youth conversations about alcohol, including the frequency of these conversations over time, were not tracked. To further study if INSPIRE facilitates parent-youth conversations about alcohol use, it would be important to quantify and qualify conversations with parents post-game and explore parents’ perceptions of parent-youth conversations about alcohol use pre and post-INSPIRE gameplay.
This pilot study of a strategically timed narrative-centered behavior change environment targets a key developmental period to reduce alcohol use among adolescents with ADHD. The aims of this pilot are primarily to examine the engagement of adolescents with ADHD in INSPIRE and to examine the holistic eco-system of the adolescent. Findings demonstrate that adolescents with ADHD engaged with the game and were motivated to share information with their parents about alcohol-related risks. INSPIRE may provide a digital technology innovation to foster the critical developmental competencies and supportive ecosystems needed to mitigate risk across the life course for neurodivergent adolescents with ADHD. The application of INSPIRE presents a significant opportunity for researchers and providers to partner with adolescents with ADHD and their parents for health. INSPIRE warrants further testing with adolescents with ADHD to explore this narrative-centered game-based behavior change environment’s effectiveness in both preventing and reducing alcohol use.
The datasets presented in this article are not readily available because due to the nature of the study questions and age of the participants, data from this study will not be shared. Requests to access the datasets should be directed to MP bXB1Z2F0Y2hAbHVyaWVjaGlsZHJlbnMub3Jn.
The studies involving humans were approved by the Institutional Review Board (IRB) at the University of California San Francisco. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MP, EO, WB, and NB conceptualized the study, research goals, aims, and methodology. MB, MP, JR, AG, MM, and VK developed the dataset used for the study. MP performed the statistical analysis and took the lead in writing the manuscript. MP and SH were responsible for the administration of the project. All authors reviewed and edited versions of the manuscript and approved the submitted version.
This project is primarily supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under cooperative agreements UA6MC32492, Life Course Intervention Research Network and UA6MC273 & U8DMC45901, Adolescent and Young Adult Health Research Network; and the National Cancer Institute R01CA247705. Additional funding sources include the National Institute of Mental Health (NIMH) [T32MH018261], HRSA-funded Developmental-Behavioral Pediatrics Research Network, UT5MC42432, and the National Science Foundation under grants IIS-1344803 and IIS-1344670.
We appreciate the important contributions of the adolescents engaged in this study, the guidance received from Shirley A. Russ, MD of the Life Course Intervention Research Network, and the support of Jaclyn Cacia, Clinical Research Program Manager Developmental-Behavioral Pediatrics Research Network, and Anthony Kung, Senior Research Associate, Adolescent and Young Adult Health Research Network.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
American Academy of Pediatrics (2017). Bright futures: Guidelines for health supervision of infants, children, and adolescents fourth edition. Itasca, IL: American Academy of Pediatrics.
Anderson, M., and Jiang, J. (2018). Teens, social media & technology 2018. Washington, DC: Pew Research.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall, Inc.
Barbaresi, W., Katusic, S., Colligan, R., Weaver, A., Pankratz, V., Mrazek, D., et al. (2004). How common is attention-deficit/hyperactivity disorder? Towards resolution of the controversy: Results from a population-based study. Acta Paediatr. Suppl. 93, 55–59. doi: 10.1111/j.1651-2227.2004.tb03058.x
Barbaresi, W. J., Campbell, L., Diekroger, E. A., Froehlich, T. E., Liu, Y. H., O’Malley, E., et al. (2020). The society for developmental and behavioral pediatrics clinical practice guideline for the assessment and treatment of children and adolescents with complex attention-deficit/hyperactivity disorder: Process of care algorithms. J. Dev. Behav. Pediatr. 2S, S58–S74. doi: 10.1097/DBP.0000000000000781
Barbaresi, W. J., Weaver, A. L., Voigt, R. G., Killian, J. M., and Katusic, S. K. (2018). Comparing methods to determine persistence of childhood adhd into adulthood: A prospective, population-based study. J. Atten. Disord. 22, 571–580. doi: 10.1177/1087054715618791
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 121, 65–94. doi: 10.1037/0033-2909.121.1.65
Bitsko, R. H., Claussen, A. H., Lichstein, J., Black, L. I., Jones, S. E., Danielson, M. L., et al. (2022). Mental health surveillance among children - united states, 2013-2019. MMWR Suppl. 71, 1–42. doi: 10.15585/mmwr.su7102a1
Booth-Butterfield, M., and Sidelinger, R. (1998). The influence of family communication on the college-aged child: Openness, attitudes and actions about sex and alcohol. Commun. Q. 46, 295–308. doi: 10.1080/01463379809370103
Centers for Disease Control and Prevention. (2016). Fact sheets - underage drinking - alcohol. Atlanta, GA: Centers for Disease Control and Prevention.
Charach, A., Yeung, E., Climans, T., and Lillie, E. (2011). Childhood attention-deficit/hyperactivity disorder and future substance use disorders: Comparative meta-analyses. J. Am. Acad. Child Adolesc. Psychiatry 50, 9–21. doi: 10.1016/j.jaac.2010.09.019
Couper, M. P., Alexander, G. L., Zhang, N., Little, R. J., Maddy, N., Nowak, M. A., et al. (2010). Engagement and retention: Measuring breadth and depth of participant use of an online intervention. J. Med. Internet Res. 12, e52. doi: 10.2196/jmir.1430
Cox, M. J., Janssen, T., Lopez-Vergara, H., Barnett, N. P., and Jackson, K. M. (2018). Parental drinking as context for parental socialization of adolescent alcohol use. J. Adolesc. 69, 22–32. doi: 10.1016/j.adolescence.2018.08.009
Cushing, C. C., and Steele, R. G. (2010). A meta-analytic review of ehealth interventions for pediatric health promoting and maintaining behaviors. J. Pediatr. Psychol. 35, 937–949. doi: 10.1093/jpepsy/jsq023
Dalsgaard, S., Ostergaard, S. D., Leckman, J. F., Mortensen, P. B., and Pedersen, M. G. (2015). Mortality in children, adolescents, and adults with attention deficit hyperactivity disorder: A nationwide cohort study. Lancet 385, 2190–2196. doi: 10.1016/S0140-6736(14)61684-6
Davis, N. O., Bower, J., and Kollins, S. H. (2018). Proof-of-concept study of an at-home, engaging, digital intervention for pediatric adhd. PLoS One 13:e0189749. doi: 10.1371/journal.pone.0189749
Fogler, J. M., Burke, D., Lynch, J., Barbaresi, W. J., and Chan, E. (2017). Topical review: Transitional services for teens and young adults with attention-deficit hyperactivity disorder: A process map and proposed model to overcoming barriers to care. J. Pediatr. Psychol. 42, 1108–1113. doi: 10.1093/jpepsy/jsx102
Fridman, M., Banaschewski, T., Sikirica, V., Quintero, J., and Chen, K. S. (2017). Access to diagnosis, treatment, and supportive services among pharmacotherapy-treated children/adolescents with adhd in europe: Data from the caregiver perspective on pediatric adhd survey. Neuropsychiatr. Dis. Treat 13, 947–958. doi: 10.2147/NDT.S128752
Giovanelli, A., Rowe, J., Taylor, M., Berna, M., Tebb, K. P., Penilla, C., et al. (2023). Supporting adolescent engagement with ai-driven digital health behavior change interventions. J. Med. Internet Res. 25, e40306.
Harris, S. K., Aalsma, M. C., Weitzman, E. R., Garcia-Huidobro, D., Wong, C., Hadland, S. E., et al. (2017). Research on clinical preventive services for adolescents and young adults: Where are we and where do we need to go? J. Adolesc. Health 60, 249–260. doi: 10.1016/j.jadohealth.2016.10.005
Harstad, E., Sideridis, G., Kaye, D., Wisk, L. E., Weitzman, E. R., and Levy, S. (2020). Parental perceptions about alcohol use for their adolescent with attention-deficit/hyperactivity disorder. J. Dev. Behav. Pediatr. 41, 366–372. doi: 10.1097/DBP.0000000000000794
Hieftje, K., Edelman, E. J., Camenga, D. R., and Fiellin, L. E. (2013). Electronic media-based health interventions promoting behavior change in youth: A systematic review. JAMA Pediatr. 167, 574–580. doi: 10.1001/jamapediatrics.2013.1095
Hinshaw, S. P., Nguyen, P. T., O’Grady, S. M., and Rosenthal, E. A. (2022). Annual research review: Attention-deficit/hyperactivity disorder in girls and women: Underrepresentation, longitudinal processes, and key directions. J. Child Psychol. Psychiatry 63, 484–496. doi: 10.1111/jcpp.13480
Lee, S. S., Humphreys, K. L., Flory, K., Liu, R., and Glass, K. (2011). Prospective association of childhood attention-deficit/hyperactivity disorder (ADHD) and substance use and abuse/dependence: A meta-analytic review. Clin. Psychol. Rev. 31, 328–341. doi: 10.1016/j.cpr.2011.01.006
Lyk, P. B., Majgaard, G., Vallentin-Holbech, L., Guldager, J. D., Dietrich, T., Rundle-Thiele, S., et al. (2020). Co-designing and learning in virtual reality: Development of tool for alcohol resistance training. Electron. J. E-Learn. 18, 213–228. doi: 10.34190/EJEL.20.18.3.002
Miech, R. A., Johnston, L. D., Bachman, J. G., O’Malley, P. M., Schulenberg, J. E., and Patrick, M. E. (2020). Monitoring the future: A continuing study of american youth (8th- and 10th-grade surveys), 2019. Ann Arbor, MI: Inter-university Consortium for Political and Social Research.
Nicholas, J., Mills, B., Hansen, S., Bright, S. J., Boyd, H., Brook, L., et al. (2022). Developing an alcohol and other drug serious game for adolescents: Considerations for improving student engagement. Aust. N. Z. J. Public Health 46, 682–688. doi: 10.1111/1753-6405.13287
O’Brien, H. L., Cairns, P., and Hall, M. (2018). A practical approach to measuring user engagement with the refined user engagement scale () and new ues short form. Int. J. Human-Comput. Stud. 112, 28–39.
O’Brien, H. L., and Toms, E. G. (2010). The development and evaluation of a survey to measure user engagement. J. Am. Soc. Inf. Sci. Technol. 61, 50–69.
O’Connor, E. A., Perdue, L. A., Senger, C. A., Rushkin, M., Patnode, C. D., Bean, S. I., et al. (2018). Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: Updated evidence report and systematic review for the us preventive services task force. JAMA 320, 1910–1928. doi: 10.1001/jama.2018.12086
Ohlmeier, M. D., Peters, K., Te Wildt, B. T., Zedler, M., Ziegenbein, M., Wiese, B., et al. (2008). Comorbidity of alcohol and substance dependence with attention-deficit/hyperactivity disorder (ADHD). Alcohol. Alcohol 43, 300–304. doi: 10.1093/alcalc/agn014
Osilla, K. C., D’Amico, E. J., Smart, R., Rodriguez, A., Nameth, K., and Hummer, J. (2023). Study design to evaluate a web-intervention to prevent alcohol and cannabis-impaired driving and use among adolescents in driver education. Addict. Sci. Clin. Pract. 18:17. doi: 10.1186/s13722-023-00373-2
Ozer, E. M., and Bandura, A. (1990). Mechanisms governing empowerment effects: A self-efficacy analysis. J. Pers. Soc. Psychol. 58, 472–486. doi: 10.1037//0022-3514.58.3.472
Ozer, E. M., and Lester, J. C. (2020). Innovative digital technologies to improve adolescent and young adult health. J. Adolesc. Health 67, S3. doi: 10.1016/j.jadohealth.2020.05.015
Ozer, E. M., Rowe, J., Tebb, K. P., Berna, M., Penilla, C., Giovanelli, A., et al. (2020). Fostering engagement in health behavior change: Iterative development of an interactive narrative environment to enhance adolescent preventive health services. J. Adolesc. Health 67, S34–S44. doi: 10.1016/j.jadohealth.2020.04.022
Prediger, C., Hrynyschyn, R., Stock, C., and Helmer, S. M. (2021). Virtual reality-based alcohol prevention in adolescents: A systematic review. Adolescents 1, 138–150. doi: 10.3390/adolescents1020011
Pugatch, M., Giovanelli, A., Berna, M., Rowe, J., Mott, M., Tebb, K., et al. (2022). “Alcohol use and in-game goals and behavioral choices in a narrative-centered behavior change environment for reducing risky alcohol use,” in Poster presentation in Pediatric Academic Societies (PAS), Denver, CO.
Reimuller, A., Hussong, A., and Ennett, S. T. (2011). The influence of alcohol-specific communication on adolescent alcohol use and alcohol-related consequences. Prev. Sci. 12, 389–400. doi: 10.1007/s11121-011-0227-4
Ryan, S. M., Jorm, A. F., and Lubman, D. I. (2010). Parenting factors associated with reduced adolescent alcohol use: A systematic review of longitudinal studies. Aust. N. Z. J. Psychiatry 44, 774–783. doi: 10.1080/00048674.2010.501759
Sibley, M. H., Kuriyan, A. B., Evans, S. W., Waxmonsky, J. G., and Smith, B. H. (2014). Pharmacological and psychosocial treatments for adolescents with adhd: An updated systematic review of the literature. Clin. Psychol. Rev. 34, 218–232. doi: 10.1016/j.cpr.2014.02.001
Sisk, C. L., and Foster, D. L. (2004). The neural basis of puberty and adolescence. Nat. Neurosci. 7, 1040–1047. doi: 10.1038/nn1326
Steele, D. W., Becker, S. J., Danko, K. J., Balk, E. M., Adam, G. P., Saldanha, I. J., et al. (2020). Brief behavioral interventions for substance use in adolescents: A meta-analysis. Pediatrics 146:4. doi: 10.1542/peds.2020-0351
Tanner-Smith, E. E., and Lipsey, M. W. (2015). Brief alcohol interventions for adolescents and young adults: A systematic review and meta-analysis. J. Subst. Abuse Treat 51, 1–18. doi: 10.1016/j.jsat.2014.09.001
Wiebe, E. N., Lamb, A., Hardy, M., and Sharek, D. (2014). Measuring engagement in video game-based environments: Investigation of the user engagement scale. Comput. Hum. Behav. 32, 123–132.
Wong, C. A., Madanay, F., Ozer, E. M., Harris, S. K., Moore, M., Master, S. O., et al. (2020). Digital health technology to enhance adolescent and young adult clinical preventive services: Affordances and challenges. J. Adolesc. Health 67, S24–S33. doi: 10.1016/j.jadohealth.2019.10.018
Wozney, L., McGrath, P. J., Gehring, N. D., Bennett, K., Huguet, A., Hartling, L., et al. (2018). Emental healthcare technologies for anxiety and depression in childhood and adolescence: Systematic review of studies reporting implementation outcomes. JMIR Ment. Health 5, e48. doi: 10.2196/mental.9655
Keywords: prevention, technology, adolescent, alcohol-related disorders, parenting, attention deficit hyperactivity disorder, ADHD, life course
Citation: Pugatch M, Blum NJ, Barbaresi WJ, Rowe J, Berna M, Hennigan S, Giovanelli A, Penilla C, Tebb KP, Mott M, Kumaran V, Buckelew S, Lester JC and Ozer E (2024) Engagement of adolescents with ADHD in a narrative-centered game-based behavior change environment to reduce alcohol use. Front. Educ. 8:1183994. doi: 10.3389/feduc.2023.1183994
Received: 10 March 2023; Accepted: 11 December 2023;
Published: 05 January 2024.
Edited by:
Emily Hotez, UCLA Health System, United StatesReviewed by:
Roberta Renati, University of Cagliari, ItalyCopyright © 2024 Pugatch, Blum, Barbaresi, Rowe, Berna, Hennigan, Giovanelli, Penilla, Tebb, Mott, Kumaran, Buckelew, Lester and Ozer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marianne Pugatch, bXB1Z2F0Y2hAbHVyaWVjaGlsZHJlbnMub3Jn
†Present address: Marianne Pugatch, Potocsnak Family Division of Adolescent and Young Adult Medicine, Department of Pediatrics, and Pritzker Department of Psychiatry and Behavioral Health, Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, United States
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.