 Raúl Piñuñuri1
Raúl Piñuñuri1 Catalina Muñoz-Castillo2
Catalina Muñoz-Castillo2 Eduardo Herrera-Aliaga2Ximena Rodríguez-Palleres1Carolina Pino-Astorga1*
Eduardo Herrera-Aliaga2Ximena Rodríguez-Palleres1Carolina Pino-Astorga1* Lisbell D. Estrada2
Lisbell D. Estrada2- 1Escuela de Nutrición y Dietética, Facultad de Ciencias de la Salud, Universidad Bernardo O’Higgins, Santiago, Chile
- 2Hospital de Simulación y Laboratorios, Facultad de Ciencias de la Salud, Universidad Bernardo O’Higgins, Santiago, Chile
Introduction: During the COVID-19 pandemic, tele-simulation emerged as an educational alternative, being useful for the development of Nutritional Care Process (NCP) skills. The importance of this study lies in knowing the impact of tele-simulation on perception and learning for the NCP. The aim of this research was to know the academic performance and the student’s perception of their ability to apply a dietary anamnesis.
Materials and methods: A quantitative, longitudinal, three-temporal study was conducted with a purposive sample of 25 Nutrition and Dietetics students during 2021. All students performed three tele-simulations with a standardized patient, in relation to the NCP.
Results: The mean response among the three tele-simulations developed on perception in tele-simulation with a standardized patient was 4.6 (Scale 1–5). The aspect with the best perception of the students was observed in relation to the feasibility and viability of the tele-simulation. The students improved in disciplinary aspects such as the investigation of the culinary technique, representativeness and quantification of the intake through the application of the NCP.
Conclusion: Tele-simulation with standardized patient is viable as a teaching-learning methodology for the application of the PNC. It is possible to demonstrate a higher performance in the nutritional interview.
Introduction
Clinical simulation is a teaching, learning and evaluation methodology that offers advantages in the training of health professionals compared to traditional methods (Nestel et al., 2011; Corvetto et al., 2013; Abas and Juma, 2016; Herrera-Aliaga and Estrada, 2022). Seeks the learner’s interaction with environments that mimic reality, in order to acquire skills necessary for clinical performance (Fraser et al., 2012); conceives practical and perfectible learning, involving emotions, analysis and reflection on one’s own performance (Cleary et al., 2020), through an experiential experience, which implies a meaningful and, therefore, long-term learning (Herrera-Aliaga and Estrada, 2022). Simulation allows better problem solving using clinical reasoning (Armijo-Rivera et al., 2020) and allows the student to increase his self-confidence in relation to learning (Abas and Juma, 2016).
In simulation, the participation of standardized patients is common, constituting a widely accepted tool for teaching and with important benefits for the student in health science field (McNaughton and Anderson, 2017), including in nutrition and dietetics field (O’Shea et al., 2019). The standardized patient is defined as an actor or trained person who simulates a health condition, which increases the fidelity of the experience (McNaughton and Anderson, 2017; O’Shea et al., 2019). The standardized patient generates “standard responses” and allows the development of various skills such as attitudinal and procedural, which are necessary for optimal professional preparation and for interaction with real users (McNaughton and Anderson, 2017).
The COVID-19 pandemic generated the massive incorporation of “remote” methodologies, multiplying the use of tele-simulation or online simulation (MacKenna et al., 2021), which corresponds to a relatively recent modality for health education and consists of linking, through the internet, of an instructor and a trainee in a simulated scenario (McCoy et al., 2017). There are successful applications of this methodology especially in the area of laparoscopic surgery (Henao et al., 2013; McCoy et al., 2017; Jarufe et al., 2018). When the on-site participation of students and instructors is not possible, remote training is possible in specific situations, being able to use standardized patients for that purpose, maintaining the same principles of a face-to-face simulation: Brief, Scenario and Debriefing. This methodology was incorporated in the University, in the Nutrition and Dietetics Program in the context of the pandemic, for the development of the necessary skills to carry out the food anamnesis, which is part of the Nutritional Care Process (NCP; Buchholz et al., 2018, 2020).
The NCP is a “systematic method that allows problem solving for nutrition professionals based on reasoning, critical thinking and scientific evidence to make decisions and guarantee comprehensive, quality, adequate, timely, safe, rigorous and effective” (Ichimasa, 2015; Carbajal et al., 2020). It has application in the clinical or public health field, adapting to the physiological, pathological, psychological and social needs of the individual (Hammond et al., 2014; Carbajal et al., 2020), and is considered essential for professional performance. It consists of four consecutive stages: i. Assessment, ii. Diagnosis, iii. Intervention, and iv. Monitoring or Follow-up (Buchholz et al., 2018). In the assessment, the antecedents such as the clinical, social and nutritional history, biochemical and physical examinations are collected, and anthropometric measurements are made, which also implies verifying and interpreting the nutritional information (Bueche et al., 2008a,b; Petermann et al., 2017; Carbajal et al., 2020). At this stage, surveys are applied through food anamnesis (Petermann et al., 2017), which aim to identify dietary alterations, know the habits and food intake of patients (Troncoso-Pantoja et al., 2020). The most common methods used are the 24-Hour Dietary Recall (24hDR) and Food Frequency Questionnaire (FFQ). The 24hDR is for the patient to remember everything they ingested the day before, both solid and liquid foods, so that the nutritionist can quantify the intake (Foster and Bradley, 2018). The FFQ consists of knowing the frequency of consumption of certain foods during a certain period of time (Troncoso-Pantoja et al., 2020). NCP is related to better results in nutritional intervention in the treatment of malnutrition due to excess in the adult population (Petermann et al., 2017) and children (Kim et al., 2019). In addition, it improves the productivity and communication and interaction of the health team (Ichimasa, 2015; Carbajal et al., 2020). Therefore, the NCP should be addressed in the training of students of the discipline, since its proper application can impact the clinical results of the patient (Petermann et al., 2017; Kim et al., 2019).
As a research problem, tele-simulation is a relatively recent incorporation and its impact on students’ perception and learning is not known. In this research, a tele-simulation experience with a standardized patient was implemented in third year students of the Nutrition and Dietetics Program. The objective of this research was to know the academic performance and the student’s perception of their ability to apply a dietary anamnesis through 24hDR thought the tele-simulation methodology.
Materials and methods
The present investigation corresponds to quantitative, longitudinal study in three times, between the months of June to November 2021.
Participants
It was carried out with an intentional non-random sample of students from the Nutrition and Dietetics Program of the University, the inclusion criterion corresponded to being in the third year of this program. 25 students participated, of which 24 were female (96%), the mean age was 24 years (range 20–46). The average of the University Selection Test (PSU) of the sample at the time of entry to the program (years 2017–2018), was 475 points (maximum 850 points) and the average score of Secondary Education Notes (NEM) was 505 points (maximum 850 points). 58.3% of the students come from the periphery/rural of the Metropolitan Region of Chile.
Procedures
The students had to apply the 24HR, through tele-simulation with a standardized patient. The study was developed in phases, beginning with the planning of the activity, in which experts in the disciplines and in the simulation methodology participated. Twelve scenarios were designed, with minimal variations to ensure standardization, focusing on nutritional assessment skills. A standardized patient profile was defined with a clinical history and a biographical profile. The diets and their energy contributions in all scenarios were calculated based on current exchange portions for the Chilean population (Zacarías et al., 2018). The standardized patients were professional actors, with experience in simulation, and who had special preparation to perform the telesimulation, for example, they knew in advance the cases to be represented and were trained to interact virtually with the students. The standardized patients represented the patient cases, according to the clinical history profile, age, health condition and type of diet of the case.
A second phase consisted of student participation in three tele-simulations (I, II and III) with a standardized patient. Each tele-simulation was separated by 1 month. The students received prior information about the telesimulation and the expected performance. Each tele-simulation consisted only of the development of one of the 12 previously constructed scenarios. For the interaction between the student and the standardized patient, the Zoom© platform was used; the teacher supervised the activity without audio or camera activated to facilitate the interaction. Each student performed three 24hDR, the designated time for each was 20 min. Before starting the tele-simulation, a fiction and confidentiality contract was established, a psychologically safe environment was established, explaining the details and (brief) instructions to the student. The student then applied the 24hDR. At the end, the teacher conducted a classical structured debriefing (MacKenna et al., 2021), in which the standardized patient also participated.
Instruments
The instruments applied were: A. Survey of perception of the tele-simulation methodology with a standardized patient; B. Dichotomous checklist of performance in the application of 24hDR; and C. Self-perception survey of the ability to apply 24hDR (pre and post tele-simulation). The instruments A, B and C were designed and evaluated by the authors. For instruments A and C, a Likert-type scale from 1 to 5 was used, with 1 being “strongly disagree” and 5 “strongly agree.” The instrument A was adapted from a previous version, which assessed presential simulation (Cronbach’s Alpha = 0.84), and its reliability for tele-simulation was evaluated (Cronbach’s Alpha = 0.89). The instrument B consisted of a dichotomous checklist of performance in the application of the 24hDR was based on the structure of the survey itself, for example: meal times, schedules, culinary techniques, type and quantity in home measurements of food, among others, which have been described as part of the NCP (Petermann et al., 2017; Kim et al., 2019; Troncoso-Pantoja et al., 2020). The teachers evaluated the performance of the activity as “completed” only if the student completely and correctly performed the described activity; therefore, if the student performed it partially, it was evaluated as “not completed.” In addition, it was evaluated if the students analyzed the calories contributed according to the diet mentioned by the standardized patient and finally if they analyzed the food qualitatively. The results are expressed as a percentage of students who correctly perform the evaluated aspect.
Data analysis
The variables are expressed as mean and standard deviation. The analysis of change before and after the intervention was carried out through the Mann-Witney test for paired samples. While the analysis between the different applications was carried out through Kruskal Wallis. The disciplinary aspects were evaluated as the percentage of correct responses over total responses, they were analyzed with Fisher’s Test and later the association strength with the Cramér’s V Coefficient (Cramér’s V) was analyzed. The results were considered significant when p < 0.05. STATA Software version 13.1 for Mac was used.
Ethical aspects
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Bernardo O’Higgins University Ethics Committee (project code N° 75/2021, approved on 14 May 2021), safeguarding ethical principles and the signing of informed consents was established, which explained the nature, risks and importance of the research.
Results
Perception of tele-simulation with standardized patient
It was observed that the average of responses on perception in the tele-simulation I with a standardized patient was 4.7 (Scale 1–5), while the II and III were 4.6 and 4.4, respectively, (Table 1). The aspect with the best perception in the three tele-simulations was the viability and feasibility of performing the tele-simulation.
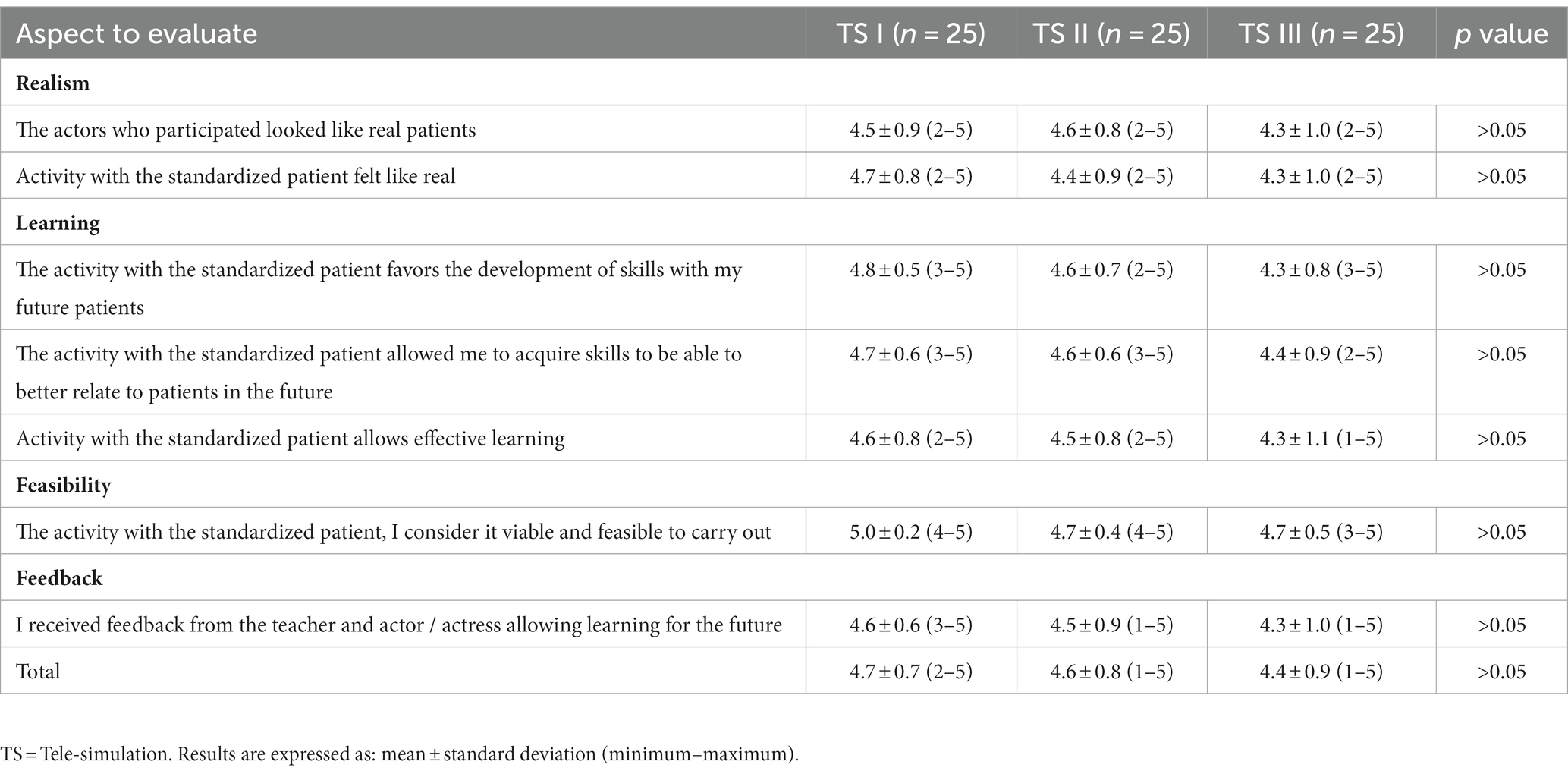
Table 1. Perception of tele-simulation with standardized patient.
Academic performance
High achievement percentages were observed in most of the items, which present significant differences between tele-simulations (Table 2). Additionally, in the aspects that were significant, the association strength was evaluated in each tele-simulation according to the aspect evaluated. The major associations were: the quantification of what was consumed (Cramér’s V = 0.44); explain the procedure to the patient (Cramér’s V = 0.37); and, the reinforcement as regards the ingredients and preparations consumed during the day (Cramér’s V = 0.37). In the evaluated aspects that they represented with a medium association strength, we have: the support provided in the face of the patient’s questions regarding their diet, from the technical and emotional point of view (Cramér’s V = 0.35); the quantification measures what the patient consumed in two meal times (Cramér’s V = 0.34); if the student asked “if yesterday was representative of her usual diet” (0.31); and, the student was consulted for the culinary technique (Cramér’s V = 0.31).
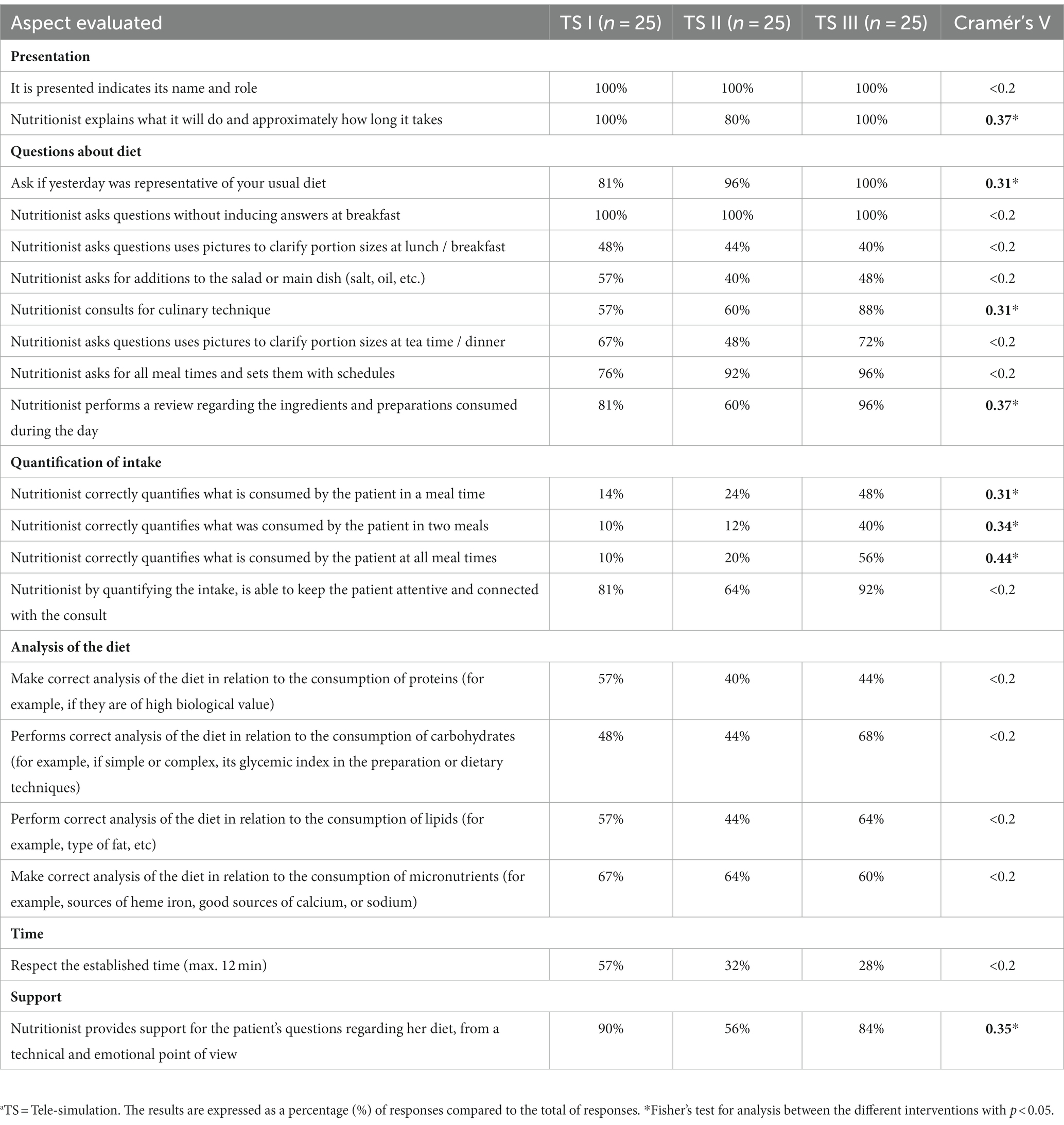
Table 2. Academic performance in the application of 24hDR.
Students’ self-perception of the ability to apply a food anamnesis (24hDR)
When comparing the responses before and after the tele-simulation, significant differences were only found in the tele-simulation III showing an improvement in self-perception, regarding the ability to use an adequate verbal and non-verbal language, the comparisons of the responses before and after in each tele-simulation they did not show significant differences (Table 3).
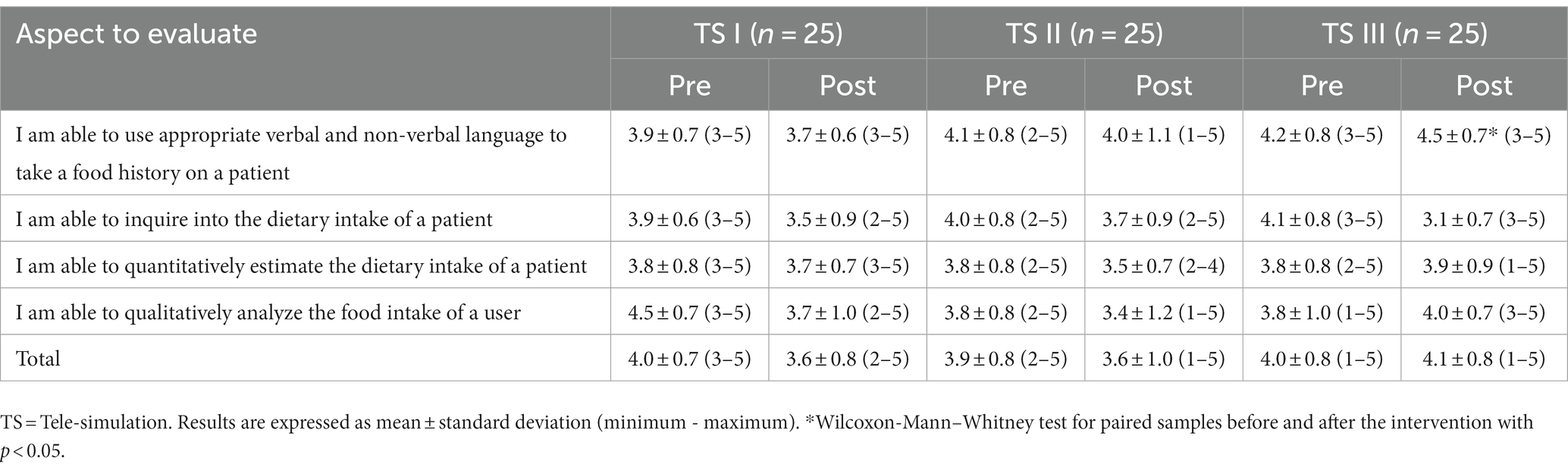
Table 3. Self-perception survey of the ability to apply 24hDR (pre and post tele-simulation).
Discussion
Due to the COVID-19 pandemic, forms of education were modified to adapt to the health needs of distance education (Beshgetoor and Wade, 2007; Dieckmann et al., 2020; MacKenna et al., 2021). A series of technological changes were evidenced to support the new modalities of education, learning and assessment. Given this scenario, the concern was on the impact of these new modalities on academic training beyond how novel they may seem. The incorporation of online simulations or telesimulations was established in our institution as a useful measure to continue learning in the different health disciplines.
Tele-simulation as a teaching-learning-evaluation experience based on remote interaction was perceived by students as a positive experience, highlighting it as a viable and applicable one in contexts where there is a need for social distancing (McCoy et al., 2017). Likewise, the students perceived that the tele-simulation was realistic, and they agreed that it favored the development of professional skills. Although changes are observed in the assessment of the first and third tele-simulation, it does not represent a significant event, which could be explained in the empowerment of the student given the repetitive practice that is an inherent quality of the simulation (McCoy et al., 2017). These results coincide with previous studies, where the simulation was perceived as real, and its ability to promote learning was highlighted (Beshgetoor and Wade, 2007; Sa-Couto and Nicolau, 2020). Another aspect well evaluated by the students was that this methodology allows the development of skills to relate to the patient, being essential in undergraduate teaching since it is one of the most difficult aspects to develop, since for its execution they converge, beyond technical capabilities, communication, active listening, among other skills (Porter et al., 2019).
Also noteworthy is the feedback provided by both the teacher and the simulated patient. Feedback is considered one of the central aspects in simulation-based education, and a constitutive part of all activities where this methodology mediates since it generates an impact on emotions and therefore results in reflective and long-term learning (Ramjan et al., 2016; Herrera-Aliaga and Estrada, 2022). Feedback is essential during debriefing, allowing to deepen learning (Davis, 2019), therefore, the possibility of doing it in online education is recommended on the one hand, and on the other, it is possible to do it while maintaining the same principles when it is done in person (McCoy et al., 2017). Debriefing is a fundamental strategy in simulation and tele-simulation, currently there are several types of debriefing (GAS, CORE, With Good Judgment, etc.), another modality is self-debriefing, which consists of self-management of reflection by students (Mackenna et al., 2021).
The tele-simulation led to improvements in academic performance, especially in aspects of skills in the structural items of the 24hDR, such as the ability to quantify specific aspects of the diet (Table 3; Quantification of intake), this point is remarkable given that the 24hDR is part of the assessment and this, in turn, from NCP (Hammond et al., 2014; Carbajal et al., 2020; Troncoso-Pantoja et al., 2020), which shows that tele-simulation with standardized patient contributes to the formation of skills for the execution of this process, however, it is necessary to know how other teaching-learning methodologies impact for the application of 24hDR, which have not been analyzed. Also, little variation is observed in the aspects of the survey that are related to analyzing the patient’s intake, a situation that could be explained since “analyzing” requires metacognition, a more complex ability to acquire, but which can be developed through simulation as an educational methodology (Medina et al., 2017) for which it is interesting to know if, when subjecting the student to more than three tele-simulations, this aspect presents improvements.
When the student’s self-perception survey to execute the 24hDR is analyzed, significant differences are observed in the ability to use an adequate verbal and non-verbal language with the standardized patient, specifically in the tele-simulation III, which coincides with another study where nutrition and dietetics students increase communication skills with simulated patients (Hampl et al., 1999; Henry et al., 2009; Buchholz et al., 2020). Despite not showing significant differences in the other aspects to be evaluated, it is striking to observe that in the subsequent evaluation the assessment decreased, that is, the students felt they had less capacity to apply the 24hDR, which can be explained by the fact that the students reflect on a more critical way about their own performance, which is part of what the simulation aims to achieve (O’Shea et al., 2019).
In summary, the incorporation of standardized patients is a strategy that allows the training of skills in nutrition students (Hampl et al., 1999; Henry et al., 2009) and among the advantages of the implementation of this methodology is the decrease in the use of physical and financial resources compared to a face-to-face instance (McCoy et al., 2017), in addition to maintaining the essence of the clinical simulation methodology that allows the interaction between professional and patient despite physical distancing. In addition, as a substantial aspect, this activity allows the evaluation of learning through ad-hoc instruments, which can later be analyzed and allow the identification of deficiencies and the elaboration of action plans that allow reinforcing content.
However, experience shows some disadvantages related to technological gaps, such as the student’s need to have computer equipment (personal computer, smartphone, web camera) with an internet connection, this implies that the study may not be replicable under the same conditions in other countries or regions with limited access to these technologies. Likewise, the impossibility of training technical skills, such as anthropometry, is also a disadvantage, relegating oneself to face-to-face activities. Another aspect that appears as an opportunity for improvement corresponds to the realism offered by the activity, where it would be necessary to establish technological improvements and teaching skills, so that the experience increases its realism. Also, it requires special emphasis on student self-regulation in relation to their learning processes (McCoy et al., 2017) and the emotions associated with learning (Fraser et al., 2012; Rogers et al., 2019; Pino et al., 2023). Likewise, this instance did not improve aspects of the diet analysis, since they are more complex skills such as clinical reasoning (Miles et al., 2016; Medina et al., 2017).
As limitations of the study, it is worth mentioning the type of sample, which was intentional and not randomized, as well as its size (n = 25), which limits the generalizability of the results. Another limitation emerges from the fact that only three tele-simulations were included in this study, which does not allow for longer observation over time with more interventions; it is possible that in further tele-simulations, different results will emerge, because repetitive exercise improves skills. Finally, it is necessary to incorporate other variables in future studies, for example, how students’ emotions impact on learning, because in the first simulations students present emotions such as “anxiety” or “fear,” which change to “calmness” and other “positive” emotions in successive simulations with standardized patients, according to a recent study (Pino et al., 2023).
Conclusion
It favors the development of clinical skills, despite the physical distance with the patient (McCoy et al., 2017), which also allows giving continuity to the teaching, learning and evaluation processes. In this research, an increase in the performance of nutritional interviewing skills was evidenced. In future research, it is important to evaluate how emotions are related to the development of learning through this methodology, since they can have a significant impact on cognitive processes (Fraser et al., 2012; Rogers et al., 2019).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
RP, CM-C, EH-A, and CP-A participated in the conception of the study, application for funds, methodological design, construction of evaluation instruments, and data interpretation. RP and CP-A carried out the data collection. RP performed the quantitative analysis of the data. RP, CM-C, EH-A, CP-A, XR-P, and LE participated in the writing of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research was carried out with funds from the “Investigación Aplicada a la Docencia” contest of the Universidad Bernardo O’Higgins (UBO/VCMEI 20204).
Acknowledgments
The authors thank the “Vicerrectoría de Vinculación con el Medio e Investigación” of the Bernardo O’Higgins University for the Applied Research Funds for Teaching.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abas, T., and Juma, F. Z. (2016). Benefits of simulation training in medical education. Adv. Med. Educ. Pract. 7, 399–400. doi: 10.2147/AMEP.S110386
Armijo-Rivera, S., Behrens-Pérez, C., Reyes-Aramburu, E. P., Pérez-Villalobos, C., and Bastías-Vega, N. (2020). Simulation contribution to the development of clinical reasoning in undergraduate medical students. Simulación Clínica 2, 19–25. doi: 10.35366/92935
Beshgetoor, D., and Wade, D. (2007). Use of actors as simulated patients in nutritional Counseling. J. Nutr. Educ. Behav. 39, 101–102. doi: 10.1016/j.jneb.2006.10.008
Buchholz, D., Kolm, A., Vanherle, K., Adam, M., Kohlen-berg-Müller, K., Roemeling-Walters, M., et al. (2018). Process models in dietetic care. A comparison between models in Europe. Ernahrungs. Umschau 65, 154–163. doi: 10.4455/eu.2018.034
Buchholz, A. C., Vanderleest, K., MacMartin, C., Prescod, A., and Wilson, A. (2020). Patient simulations improve dietetics students’ and interns’ communication and nutrition-care competence. J. Nutr. Educ. Behav. 52, 377–384. doi: 10.1016/j.jneb.2019.09.022
Bueche, J., Charney, P., Pavlinac, J., Skipper, A., Thompson, E., and Myers, E. (2008a). Nutrition care process and model part I: the 2008 update. J. Am. Diet. Assoc. 108, 1113–1117. doi: 10.1016/J.JADA.2008.04.027
Bueche, J., Charney, P., Pavlinac, J., Skipper, A., Thompson, E., and Myers, E. (2008b). Nutrition care process part II: using the international dietetics and nutrition terminology to document the nutrition care process. J. Am. Diet. Assoc. 108, 1287–1293. doi: 10.1016/J.JADA.2008.06.368
Carbajal, Á., Sierra, J. L., López-Lora, L., and Ruperto, M. (2020). Nutrition care process: elements for its implementation and use by nutrition and dietetics professionals. Rev. Española Nutr. Humana y Dietética 24, 172–186. doi: 10.14306/renhyd.24.2.961
Cleary, T. J., Battista, A., Konopasky, A., Ramani, D., Durning, S. J., and Artino, A. R. Jr. (2020). Effects of live and video simulation on clinical reasoning performance and reflection. Adv. Simul. (Lond.). 5:17. doi: 10.1186/s41077-020-00133-1
Corvetto, M., Bravo, M. P., Montaña, R., Utili, F., Escudero, E., Boza, C., et al. (2013). Simulation in medical education: a synopsis. Rev. Med. Chil. 141, 70–79. doi: 10.4067/S0034-98872013000100010
Davis, A. (2019). Virtual reality simulation: an innovative teaching tool for dietetics experiential education. Open Nutr. J. 9, 65–75. doi: 10.2174/1876396001509010065
Dieckmann, P., Torgeirsen, K., Qvindesland, S. A., Thomas, L., Bushell, V., and Ersdal, H. L. (2020). The use of simulation to prepare and improve responses to infectious disease outbreaks like COVID-19: practical tips and resources from Norway, Denmark, and the UK. Adv. Simul. (Lond.) 5:3. doi: 10.1186/S41077-020-00121-5
Foster, E., and Bradley, J. (2018). Methodological considerations and future insights for 24-hour dietary recall assessment in children. Nutr. Res. 51, 1–11. doi: 10.1016/j.nutres.2017.11.001
Fraser, K., Ma, I., Teteris, E., Baxter, H., Wright, B., and McLaughlin, K. (2012). Emotion, cognitive load and learning outcomes during simulation training. Med. Educ. 46, 1055–1062. doi: 10.1111/j.1365-2923.2012.04355.x
Hammond, M. I., Myers, E. F., and Trostler, N. (2014). Nutrition care process and model: an academic and practice odyssey. J. Acad. Nutr. Diet. 114, 1879–1894. doi: 10.1016/J.JAND.2014.07.032
Hampl, J. S., Herbold, N. H., Schneider, M. A., and Sheeley, A. E. (1999). Using standardized patients to train and evaluate dietetics students. J. Am. Diet. Assoc. 99, 1094–1097. doi: 10.1016/S0002-8223(99)00261-8
Henao, Ó., Escallón, J., Green, J., Farcas, M., Sierra, J. M., Sánchez, W., et al. (2013). Fundamentals of laparoscopic surgery in Colombia using telesimulation: an effective educational tool for distance learning. Biomedica 33, 107–114. doi: 10.1590/S0120-41572013000100013
Henry, B. W., Duellman, M. C., and Smith, T. J. (2009). Nutrition-based standardized patient sessions increased counseling awareness and confidence among dietetic interns. Top. Clin. Nutr. 24, 25–34. doi: 10.1097/TIN.0b013e3181978050
Herrera-Aliaga, E., and Estrada, L. D. (2022). Trends and innovations of simulation for twenty first century medical education. Front. Public Health 10:619769. doi: 10.3389/fpubh.2022.619769
Ichimasa, A. (2015). Review of the effectiveness of the nutrition care process. J. Nutr. Sci. Vitaminol. (Tokyo) 61, S41–S43. doi: 10.3177/JNSV.61.S41
Jarufe, N., Barra, M., and Varas, J. (2018). Regional surgical simulation centers and remote certification (telesimulation). A pioneering innovation in the world conducted by the Society of Surgeons of Chile. Rev. Chil. Cir. 70, 307–308. doi: 10.4067/s0718-40262018000300307
Kim, J., Kim, Y. M., Jang, H. B., Lee, H. J., Park, S. I., Park, K. H., et al. (2019). Evidence-based nutritional intervention protocol for Korean moderate-severe obese children and adolescents. Clin. Nutr. Res. 8, 184–195. doi: 10.7762/cnr.2019.8.3.184
MacKenna, V., Díaz, D. A., Chase, S. K., Boden, C. J., and Loerzel, V. (2021). Self-debriefing in healthcare simulation: an integrative literature review. Nurse Educ. Today 102:104907. doi: 10.1016/j.nedt.2021.104907
McCoy, C. E., Sayegh, J., Alrabah, R., and Yarris, L. M. (2017). Telesimulation: an innovative tool for health professions education. AEM Educ. Train. 1, 132–136. doi: 10.1002/aet2.10015
McNaughton, N., and Anderson, M. (2017). Standardized patients: It’s all in the words. Clin. Simul. Nurs. 13, 293–294. doi: 10.1016/j.ecns.2017.05.014
Medina, M. S., Castleberry, A. N., and Persky, A. M. (2017). Strategies for improving learner metacognition in health professional education. Am. J. Pharm. Educ. 81:78. doi: 10.5688/ajpe81478
Miles, A., Friary, P., Jackson, B., Sekula, J., and Braakhuis, A. (2016). Simulation-based dysphagia training: teaching interprofessional clinical reasoning in a hospital environment. Dysphagia 31, 407–415. doi: 10.1007/s00455-016-9691-0
Nestel, D., Groom, J., Eikeland-Husebø, S., and O’Donnell, J. M. (2011). Simulation for learning and teaching procedural skills: the state of the science. Simul. Healthc. 6, S10–S13. doi: 10.1097/SIH.0b013e318227ce96
O’Shea, M. C., Reeves, N. E., Bialocerkowski, A., and Cardell, E. (2019). Using simulation-based learning to provide interprofessional education in diabetes to nutrition and dietetics and exercise physiology students through telehealth. Adv. Simul. (Lond.) 4:28. doi: 10.1186/s41077-019-0116-7
Petermann, F., Durán, E., Labraña, A., and Celis-Morales, C. (2017). Effect of a structured nutritional consultation on weight loss and eating habits in overweight and obese adults. Rev. Chil. Nutr. 44, 341–349. doi: 10.4067/S0717-75182017000400341
Pino, C., Piñuñuri, R., Muñoz, C., Sepúlveda, K., and Herrera-Aliaga, E. (2023). Analysis of the discourses of debriefing in telesimulation in nutrition and dietetics students: emotions, performance, and assessment of the experience. Rev. Educ. Cienc. Salud 20, 21–28.
Porter, J., Kellow, N., Anderson, A., Bryce, A., Dart, J., Palermo, C., et al. (2019). Patient involvement in education of nutrition and dietetics students: a systematic review. Nutrients 11:2798. doi: 10.3390/nu11112798
Ramjan, L. M., Peters, K., Villarosa, A., Villarosa, A. R., Curmi, C., and Salamonson, Y. (2016). Debriefing as a form of reflection and catharsis for researchers. Nurs. Res. 24, 20–25. doi: 10.7748/nr.2016.e1402
Rogers, T., Andler, C., OʼBrien, B., and van Schaik, S. (2019). Self-reported emotions in simulation-based learning: active participants vs. Observers. Simul. Healthc. 14, 140–145. doi: 10.1097/SIH.0000000000000354
Sa-Couto, C., and Nicolau, A. (2020). How to use telesimulation to reduce COVID-19 training challenges: a recipe with free online tools and a bit of imagination. MedEdPublish. 9:129. doi: 10.15694/MEP.2020.000129.1
Troncoso-Pantoja, C., Alarcón-Riveros, M., Amaya-Placencia, J., Sotomayor-Castro, M., and Maury-Sintjago, E. (2020). Practical guide for applying the dietary method for integrated nutritional diagnosis. Rev. Chil. Nutr. 47, 493–502. doi: 10.4067/S0717-75182020000300493
Keywords: simulation in healthcare, tele-simulation, clinical nutrition, standardized patient, 24-h dietary recall
Citation: Piñuñuri R, Muñoz-Castillo C, Herrera-Aliaga E, Rodríguez-Palleres X, Pino-Astorga C and Estrada LD (2023) Tele-simulation in nutrition and dietetics students, impact on learning and perception: a study pilot. Front. Educ. 8:1127509. doi: 10.3389/feduc.2023.1127509
Edited by:
Stamatios Papadakis, University of Crete, GreeceReviewed by:
Juliany Lino Gomes Silva, State University of Campinas, BrazilYercin Mamani Ortiz, Universidad Mayor de San Simón, Bolivia
Copyright © 2023 Piñuñuri, Muñoz-Castillo, Herrera-Aliaga, Rodríguez-Palleres, Pino-Astorga and Estrada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carolina Pino-Astorga, Y2Fyb2xpbmEucGlub0B1Ym8uY2w=