 Christopher Campbell1
Christopher Campbell1 Ley Fraser
Ley Fraser- 1Faculty of Education, University of Manitoba, Winnipeg, MB, Canada
- 2Department of Sociology and Criminology, University of Manitoba, Winnipeg, MB, Canada
On March 11th, 2020, the World Health Organization (WHO) declared the worldwide outbreak of COVID-19 as a pandemic. On the following day, the Ontario government (Canada’s most populous province) ordered all public schools to close. By Monday, March 16th, 2020, all public schools (and most private schools) in Canada announced plans to physically shutter schools, with a shift to remote and online learning to follow soon after. This unprecedented shift in learning environment for young Canadians came at a time when the onset of the COVID-19 pandemic was creating a challenging environment for the mental health of all Canadians. While all students may have struggled to cope, 2SLGBTQ + students faced an unusually complex shift, as their school and home environments may have contributed differentially to the social supports and acceptance (related to their 2SLGBTQ + identity or identities) that their cisgender heterosexual peers routinely experience in their social surroundings. In this paper, we explore the relationship between school attachment, parental involvement and positive mental health in 2SLGBTQ + youth using data collected as part of the Second Annual School Climate Survey on Homophobia, Biphobia, and Transphobia in Canadian Schools.
Introduction
Early in the pandemic, researchers recognized the need for high-quality data on mental health, particularly among vulnerable populations; and highlighted data collection as a priority area to mitigate the mental health impacts of COVID-19 (Holmes et al., 2020). Early research conducted by Statistics Canada found significant reductions in mental health (Findlay and Arim, 2020) and life satisfaction ratings (Statistics Canada, 2020b), particularly among younger Canadians (Arim et al., 2020; Statistics Canada, 2020a).
Isolation and disrupted social networks also hit Canadian youth hard. More than a third (37%) of young Canadians felt more disconnected from their community (such as friends and support networks); 80% said their opportunities for social connections were more difficult (Kishchuk, 2020). The same study reported greater stresses on education as well; youth found it difficult to learn and expressed worry about the impact of COVID-19 on their education (Statistics Canada, 2020a). Further, COVID-19 more acutely affects 2SLGBTQ + people1.
Egale Canada (Egale Canada, 2020a,b) surveyed Canadians over 18 years of age and found COVID-19 disproportionately impacted the finances and mental health of LGBTQI2S [sic] people. At the time of the survey over half (53%) of LGBTQI2S households had been affected by lay-offs and reduced hours, compared to 39% of overall Canadian households (Egale Canada, 2020a). And low mental health in LGBTQI2S people was nearly double that of the general population [41% of LGBTQI2S people reported their mental health was fair/poor compared to 21% of overall Canadian sample (Egale Canada, 2020b)]. Prokopenko (2020), among others (Fish et al., 2020; Public Health Agency of Canada, 2020) identifies that public health measures pose unique threats to LGBTQ2 + [sic] people (for example, LGBTQ2 + youth who may be required to isolate at home with homophobic, biphobic, or transphobic family members). The Trevor Project (Green et al., 2020) echoes these concerns for LGBTQ [sic] youth, highlighting how the combined impacts of COVID-19 are detrimental to mental health of LGBTQ youth specifically by decreasing positive social connections and access to supports. Modifications to the education system cut off access to school-based supports and positive social connections outside the home, as well as recreational activities and any supportive adults present in these various areas (e.g., coaches, counselors) (Green et al., 2020).
While the above research gives preliminary insights on the impact of COVID-19 on the health and wellbeing of 2SLGBTQ + youth, it does not address the specific situation of 2SLGBTQ + youth within school settings. Specifically, what is missing (and what this current study offers) is an analysis which ties together positive mental health, and social supports (school attachment and parental support) for school-age 2SLGBTQ + youth during the COVID-19 pandemic.
Research on positive mental health is less common than research on mental health disorders and illness; this divide is particularly conspicuous among research on 2SLGBTQ + youth where emphasis is often on negative mental health indicators such as depression/depressive symptoms, anxiety, suicidality, and stress (Veale et al., 2016; Peter et al., 2017; Watson et al., 2018). This research is valuable and necessary; naturally, there is an inverse relationship between negative and positive mental health (White et al., 2018) and negative mental health is particularly pervasive in the 2SLGBTQ + community (Kelleher, 2009; Lefevor et al., 2019). However, the absence of a mental health disorder (or overall negative mental health markers) does not necessarily indicate positive mental health (Bariola et al., 2017). While many studies seek to measure or mitigate negative mental health outcomes, equally important is a focus on fostering positive mental health in 2SLGBTQ + youth. Our current research examines the effect of social supports (school attachment and parental supports) specifically on positive mental health measures.
Emerging research shows broad benefits of social support for 2SLGBTQ + youth. Contemporary studies have shown social and school-based supports are protective factors for 2SLGBTQ + youth: supporting their mental health, promoting self-esteem, and positive identity development, reducing suicidality, and even mediating the negative impacts of bullying (Spencer and Patrick, 2009; Saewyc et al., 2014; Veale et al., 2017; Day et al., 2019, 2020; Hatchel et al., 2019; Reisner et al., 2020). Parental support also moderates psychological distress for 2SLGBTQ + youth (Antonio and Moleiro, 2015; Hatchel et al., 2019). Given this literature, there is potential for social supports to not only moderate negative experiences but contribute to the positive mental health of 2SLGBTQ + youth.
School attachment (also called belongingness) has been linked to a number of positive mental health outcomes such as life satisfaction, as well as more broadly to positive education and general wellbeing (Allen and Bowles, 2012). School attachment is such a useful measure of adolescents’ wellbeing that some researchers have proposed its addition to overall mental health screening of school age youth (Moffa et al., 2016). For 2SLGBTQ + youth, feeling a sense of belonging and attachment to school may be particularly important for overall positive mental health if they have unaccepting environments elsewhere (Fish et al., 2020). For example, social and recreational institutions outside of school may address homo/trans/biphobia with varying effectiveness (or not at all), leading 2SLGBTQ + youth to belong to fewer groups related to their various interests. School is where 2SLGBTQ + youth, like other youth, will spend most of their time. While it is important to prevent school environments having a negative impact on 2SLGBTQ + youths’ mental health (Allen et al., 2020) it would be remiss of the research community to neglect the potential for school to contribute to positive mental health.
Parental support is naturally related to, and can interact with, school attachment and overall effects on mental health (Reisner et al., 2020). Many 2SLGBTQ + youth drop below their peers in mental health and related risky behaviors (e.g., problem drinking) during adolescence, a key time when parental support can shape youth trajectories (Needham and Austin, 2010). This support might also directly affect 2SLGBTQ + youths’ day-to-day environment at school, as many parents advocate for their children when school issues arise.
For 2SLGBTQ + youth, having the social support of their parents can help mitigate the stresses of coming out and other challenges a young 2SLGBTQ + person faces in society (Grossman et al., 2021). Bouris et al. (2010) meta-analysis of parental support and 2SLGBTQ + youth outcomes found support from both parents contributed to positive mental health. This finding was in the minority of studies examined by Bouris et al. (2010) which examined positive mental health; like other research on 2SLGBTQ + youth mental health (Keyes, 2006; Saewyc et al., 2014) most of the studies in the meta-analysis examined the relationship between parental supports and negative mental health outcomes. The research described in this paper adds to the limited material on positive mental health in 2SLGBTQ + youth while also examining the under-researched Canadian population of 2SLGBTQ + youth.
Ideally 2SLGBTQ + youth would have both parental support and a strong attachment to the school environment in which they spend their days. However, during COVID-19 students’ physical time at school has waned there is a unique opportunity to examine how this change (which naturally brings them into more contact with family) might affect their positive mental health, and what positive mental health looks like for 2SLGBTQ + youth.
Keyes (2002) maintains that positive mental health encompasses subjective wellbeing and can be categorized by three components—emotional, psychological, and social wellbeing. Emotional wellbeing is based on personal feelings of self, such as the presence of positive affect, the absence of negative affect, and an overall satisfaction with life. Psychological and social wellbeing move beyond these immediate individual feelings (of emotional wellbeing) to the aspects of wellbeing which encourage the development of happiness. Researchers can assess these individual aspects of wellbeing independently, and taken together they form an operational definition of positive mental health.
Naturally, the COVID-19 pandemic affected all Canadians’ mental health (Findlay and Arim, 2020), as social environments became smaller and more limited, and the uncertainty of jobs and schooling shifted with new developments. Canadian youth expressed concerns about the local and global impacts (concerned more about vulnerable groups than themselves), as well as specifically engaging behaviors (such as communication with friends and/or family) that could bolster their mental health (Arim et al., 2020).
However, there are always limits to the resources available to an individual for the maintenance of positive mental health, and even more so during a pandemic. Parenting was under specific pressure, and negative home situations or treatment of children could be amplified during these times (Brown et al., 2020). And the 2SLGBTQ + community was hit especially hard by the pandemic (Egale Canada, 2020a). This could affect the independent supports 2SLGBTQ + youth have outside of the home (e.g., community organizations under greater strain or unable to offer certain services), as well as affecting their informal supports (as their peers within the 2SLGBTQ + community could be the source of greater worry or concern as well as themselves). 2SLGBTQ + youth living in an unsupportive homes (Fish et al., 2020), isolated from their school environment, faced unique circumstances- particularly in the early days of the pandemic when countries around the globe were still scrambling to adapt and offer new supports.
For the current study we analyze how the first wave of COVID-19, when schools moved to remote, has affected the positive mental health of 2SLGBTQ + students. We recognize that few researchers have been able to collect large-scale datasets on 2SLGBTQ + youth during the pandemic, and even fewer have pre-pandemic and “first wave” pandemic data focused on 2SLGBTQ + experiences in schools. Through fortuitous timing, we collected our data before and during the first wave (Peter et al., 2021).
Below, we empirically assess the impact of the COVID-19 pandemic on 2SLGBTQ + students’ positive mental health, and the extent to which parental involvement and feelings of school attachment mediate this zero-order relationship. We used the following research questions to inform our work:
1. What impact, if any, did the pandemic have on the positive mental health of 2SLGBTQ + students?
2. Does parental involvement and school attachment influence the positive mental health of 2SLGBTQ + students?
3. How does parental involvement and school attachment moderate the relationship with positive mental health pre-pandemic and during the first wave of the pandemic?
Data
In this study, we use data from the second National Climate Survey on homophobia, biphobia, and transphobia in secondary schools (i.e., middle school and high school). Survey participation also included cisgender-heterosexual students. However, for the purposes of this study we selected only the data from students who identified themselves as 2SLGBTQ+.
Participants completed the survey between April 2019 and May 2020 as part of a national study conducted by researchers from the University of Manitoba and the University of Winnipeg, in partnership with Egale Canada. We recruited participants in three ways. First, through directed recruitment activities via youth organizations for Canadian 2SLGBTQ + youth. Second, by advertising the survey website through various social media outlets. And third, through Canadian school boards/districts who agreed to distribute the survey link to their students. Some school boards/districts received encouragement and endorsement from their provincial government’s Ministry of Education. The survey took approximately 20–25 min to complete and received ethics approval from the researchers’ respective universities.
A total of 1,312 2SLGBTQ + students completed the survey (overall N = 3, 558, for participants of all identities who completed the survey). We asked participants to select as many gender and sexual identity options as applied to them (note: because participants could choose multiple identity signifiers, the percentages from these questions do not sum to 100).
Over half the sample (56%) identified as girl/woman, with smaller proportions identified as boy/man (16%), or non-binary (15%). Bisexual was the most selected sexual identity (43%), followed by lesbian (26%) and queer (21%) See (Table 1) for a complete list of identities reported.
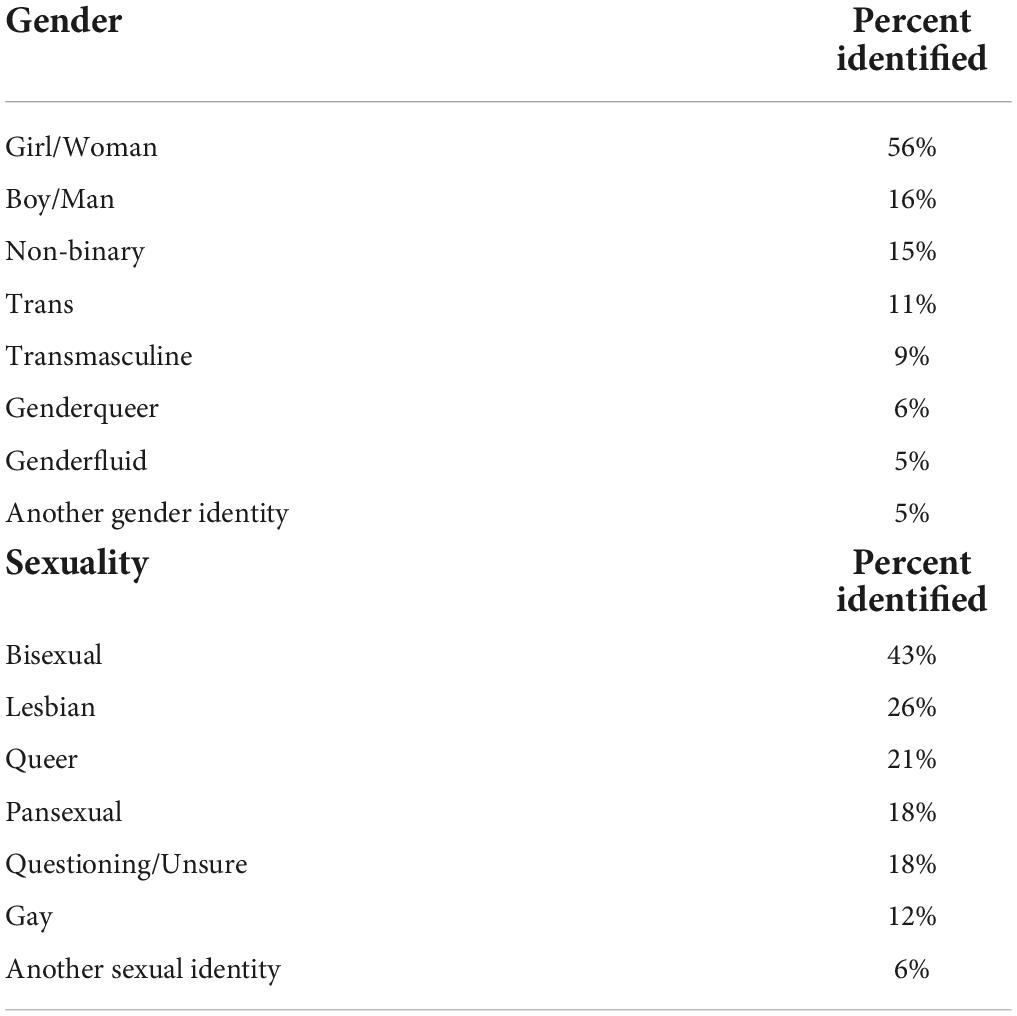
Table 1. Canadian students’ gender and sexual identities.
Geographically, a third of participants (31%) were from Ontario (Canada’s largest province), followed by 20% from Atlantic Canada, 18% from the prairie provinces, 16% from British Columbia, 14% from Québec, and less than 1% from the territories. Participants’ average age was 16 years old (M = 16.40, SD = 1.53).
Measures
We describe the rationale for dividing the data and the variables we used to test our research questions below, and list univariate descriptives and bivariate correlations in Table 2.
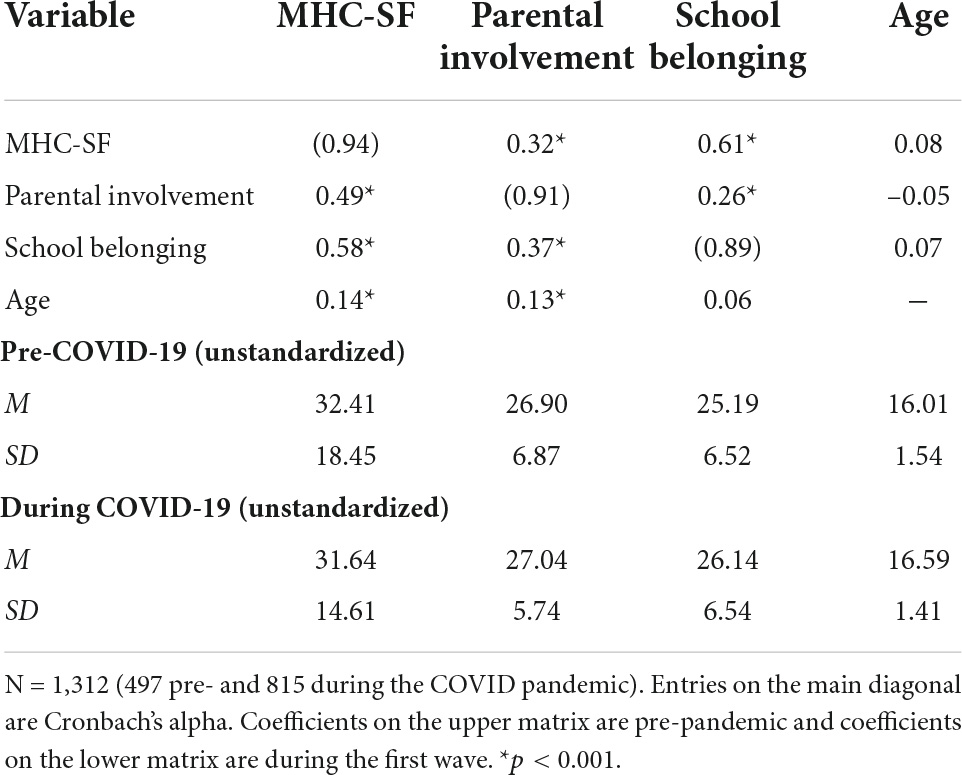
Table 2. Descriptive statistics and intercorrelations.
Selecting pre-pandemic and first wave data
In Canada, education and healthcare delivery is a provincial/territorial responsibility, which meant there was no nationally unified response to the COVID-19 pandemic across the country. However, between March 7th and March 16th, 2020, every province had closed its doors to in-person learning, and this continued until the end of May at the earliest (when the survey was out of field).
As such, we chose March 16th as the COVID-19 school closure date. We classified the 497 students who took part in the survey prior to this date as “pre-COVID-19,” and those who took part on March 16th or later as part of the first wave COVID-19 pandemic grouping (n = 815). Between March 7th and 16th only four 2SLGBTQ + students completed the survey, which means that the arbitrariness of the cut-off date should not pose any statistical problems. Readers should note that the first-wave data shows very early impressions of the lockdown and its’ effects; participants naturally had no idea how long lockdown would extend. Uncertainty about the length of lockdown and mixed messaging about the growing pandemic may contribute to any differences in this group, as well as the experience of lockdown itself. In addition, while school closure is the common experience by which we divided our datasets, participants hail from across Canada with varying experiences of the early pandemic.
Positive mental health
We asked participants to rate the statements of Keyes’35 Mental Health Continuum-Short Form (MHC-SF) on a 6-point Likert scale (0 “Never,” 5 “Every day”). The scale included emotional (e.g., [felt] “happy”), social (“That you had something important to contribute to society”) and psychological (e.g., “That you like most parts of your personality”) health statements corresponding to the sub-scales.
We computed the14 MHC-SF variables in aggregate to form a positive mental health index (α = 0.94), which we standardized to z-scores (i.e., a mean of 0 and a SD of 1) for easier interpretation. Keyes, 2002, 2006 states researchers can achieve positive mental health measures through a categorical or a continuous assessment. However, converting a continuous quantitative measure to categorical can result in a loss of statistical power (Aiken et al., 1991). In our analysis we use only the continuous assessment of positive mental health.
School attachment
We asked participants to rate ten statements on attachment to their school environment, and reverse-coded the half of the scale which used negative statements so that higher values in aggregate showed a greater sense of belonging. Participants rated each statement on a 4-item Likert scale (1 “strongly disagree,” 4 “Strongly Agree”).
The ten statements ranged from those showing some level of positive school attachment (e.g., “I feel like a real part of my school”) to a lack of attachment (e.g., “I wish I were in a different school”). We created an aggregate mean score from the sum of these ten statements to form a school attachment index (α = 0.89), and then standardized the aggregates to z-scores.
Parental involvement
We used nine statements rated on a 4-point Likert scale (1 “strongly agree,” 4 “strongly disagree”) to assess how participants perceived their parents’ involvement in their lives [e.g., “my parent(s)/guardian(s) encourage me to be confident”]. We calculated an aggregate mean score for each participants to form an overall index (α = 0.91) and mean-centered into standard scores.
Analytic procedures
We conducted several multiple regression analyses using PROCESS v. 3.2 (model 2) within SPSS v. 27 (Hayes, 2018). The model we used includes two interaction terms (parental involvement and school attachment) between the focal predictor (pre-COVID-19/COVID-19) and positive mental health. We used the “pick-a-point method” (Montoya, 2018) to further probe the interaction terms by analyzing the conditional effects of the predictor on positive mental health (θX→Y) at selected values of parental involvement (w) to test the null hypothesis that TθX→Y | (W = w) = 0. In other words, our null hypothesis states there would be no conditional effect of the presence of the pandemic (pre-COVID-19/COVID-19) on the positive mental health of 2SLGBTQ + students.
Since W (the first moderator) is a quantitative variable, we selected three points to examine the conditional effect of X on Y: the mean (average parental involvement), and one standard deviation above and below the mean. We also calculated conditional effects on the second interaction term (Z) at the mean level of school attachment as well as one standard deviation above and below the mean. We plotted the moderating effects using unstandardized coefficients to aid in interpreting the differences in the various slopes; we set percentile bootstrapping confidence intervals to 10,000 to yield more valid approximations (Preacher and Hayes, 2008). Before running the moderation analyses, we performed assumption testing to check for normality, linearity, multivariate outliers, and homogeneity of variance of covariance matrices (no serious violations found; Tabachnick and Fidell, 2007).
Results
Our results show the presence of the first wave of the COVID-19 pandemic had a significant inverse impact on the positive mental health of 2SLGBTQ + students (B = –0.177, SE = 0.05, p = 0.001) with the first wave group showing less positive mental health than the group who took part pre-COVID. We found significant main effects for parental involvement (B = 0.178, SE = 0.04, p < 0.001), school attachment (B = 0.619, SE = 0.04, p < 0.001), and age (B = 0.039, SE = 0.02, p = 0.02). The interaction between the COVID-19 pandemic proxy variable and parental involvement was significant (B = 0.125, SE = 0.05, p = 0.01) as was the interaction between the pandemic measure and school attachment (B = –0.207, SE = 0.05, p < 0.001), suggesting that the impact of the COVID-19 pandemic on the positive mental health of 2SLGBTQ + students was influenced by their level of school attachment as well as their level of parental involvement. Together, the variables accounted for approximately 41% of the variance in positive mental health [R2 = 0.408, F(6, 1,108) = 127.39, p < 0.001].
We used the pick-a-point approach of probing the simple slopes for the interaction terms to assess the association between the onset of the COVID-19 pandemic and positive mental health for low (–1 SD below the mean), average (mean), and high (+ 1 SD above the mean) level of parental involvement across the same relative levels of school attachment (Figure 1). The gap between slopes pre- and during COVID-19 is the widest among 2SLGBTQ + students with high school attachment (SA) and low parental involvement (PI) (Z+1: θ X→Y |(W = –1.0) = –0.510, p < 0.001), but we also found significant differences for all students with high SA regardless of level of parental involvement. 2SLGBTQ + students with low PI also reported lower positive mental health during the first wave of the COVID-19 pandemic than those with low PI who took part prior to the pandemic, for those with average SA overall (Z0: θ X→Y | (W = –1.0) = –0.303, p < 0.001). We also found this difference between students with average parental involvement (PA) and SA (Z0: θ X→Y | (W = 0) = –0.177, p = 0.003).
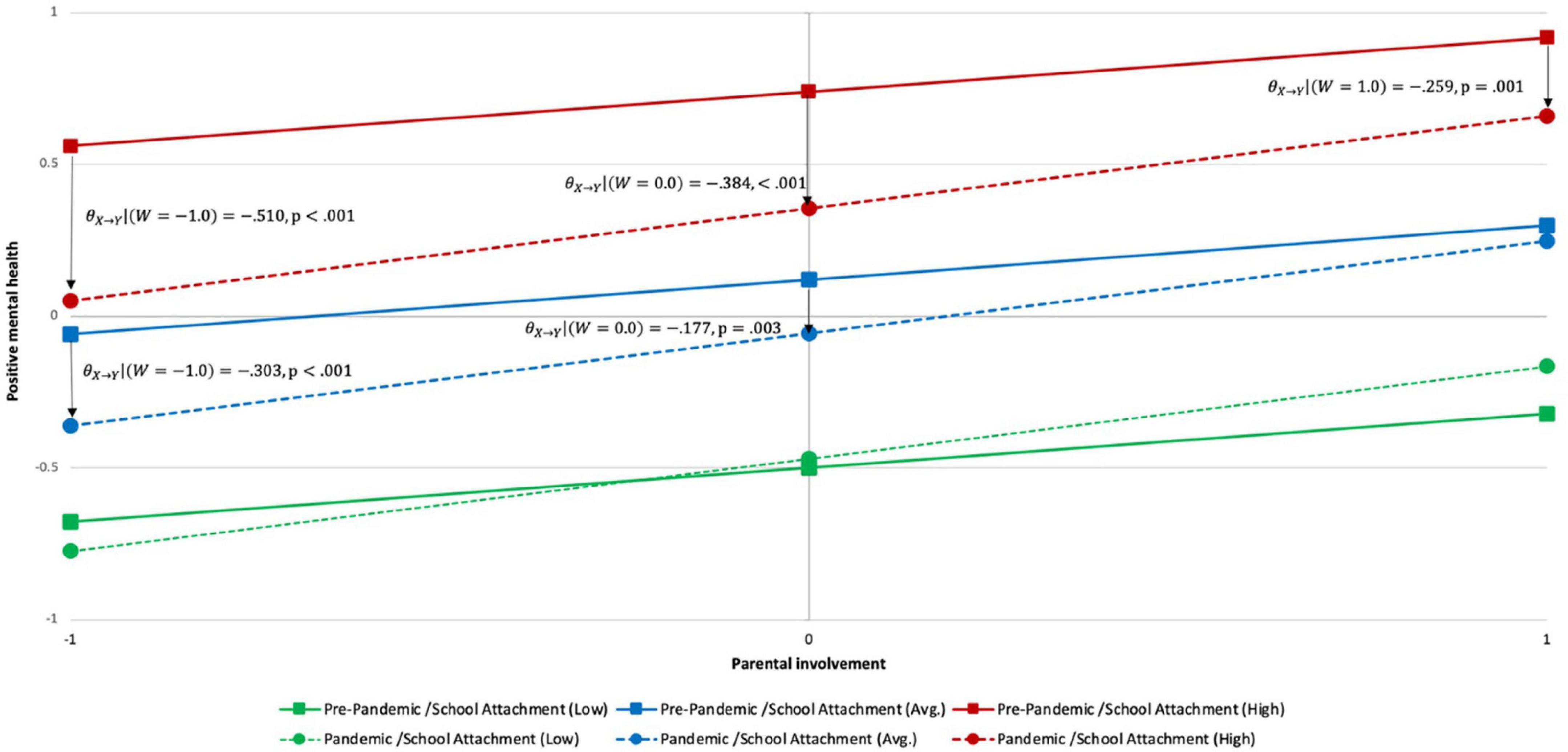
Figure 1. Pre-Pandemic and pandemic slopes between parental involvement and positive mental health by level of school attachment among 2SLGBTQ + students.
The presence of the COVID-19 pandemic did not result in any significant change in the positive mental health of 2SLGBTQ + students with average SA and high PI, nor on 2SLGBTQ + students with low SA across all levels of parental involvement. Students with these characteristics had similar positive mental health scores in the group who took part before the pandemic and the group who took part during the first wave.
While not a significant difference, 2SLGBTQ + students with low SA and high PI scored higher as a group (albeit still well below average) on positive mental health during the first wave of the COVID-19 pandemic than 2SLGBTQ + students with the same characteristics who took part prior to the pandemic.
Discussion
Note that we are comparing two groups measured at different points in time (before and after the first wave of the COVID-19 pandemic). The reader should not infer that the positive mental health of a specific group of 2SLGBTQ + students “changed” over the course of the pandemic. Rather, we surveyed one population on the same criteria (2SLGBTQ + students in Canadian schools) and split the sample to compare the experiences of those 2SLGBTQ + students who happened to take part before and after a momentous world event.
In our analysis, we incorporated a two-term moderation to explore the effects of the COVID-19 pandemic on positive mental health among 2SLGBTQ + students. In our estimation, there are four important takeaways from the results of the study.
First, the gap between the slopes for 2SLGBTQ + students pre-COVID-19 or during COVID-19 is the widest among participants with low PI and high SA. More specifically, the mean value of positive mental health (Y) for low PI, high SA 2SLGBTQ + students who completed the survey prior to the COVID-19 pandemic was above average (Y = 0.56), but was at an average level of positive mental health (Y = 0.05) for students with the same characteristics who took part when secondary schools across the country were delivering education remotely.
The impact of the pandemic and the corresponding move to remote learning had the largest effect on these students’ mental health and wellbeing. It is impossible to know for sure why we saw this difference. However, one plausible explanation is that 2SLGBTQ + students with low parental involvement and high school attachment felt more isolated with the shift to remote learning (with a pronounced impact on their mental health and wellbeing) as their parents did not provide involvement at home that compensated for the loss of their in-person school to which they were highly attached. Fish et al. (2020) support this explanation. In their study of LGBTQ youth during the onset of the pandemic, being “stuck at home with unsupportive parents” was particularly difficult for youth when coupled with the loss of access to supportive school environments (including friends, staff, and gay-straight alliance clubs).
Second, parental involvement is an important protective factor against poor mental health. Overall, the group differences we observed suggest that COVID-19 had a more severe effect on the positive mental health of 2SLGBTQ + students with low PI than those with high PI—a finding that is supported by other research (Poteat et al., 2011; Antonio and Moleiro, 2015; Hatchel et al., 2019).
In addition, though the positive mental health of 2SLGBTQ + students with high SA and high PI was significantly lower for those measured during the pandemic, the mean score of positive mental health remained quite high for the latter (Y = 0.66). There was also only a nominal difference between the pre-COVID-19 and COVID-19 groups’ positive mental health scores for those with average SA and high PI (Y = 0.29 vs. Y = 0.25, respectively). 2SLGBTQ + students with low SA and high PI actually reported higher positive mental health scores when measured during the first wave of the pandemic (Y = –0.16) compared to pre-pandemic scores for students with those characteristics (Y = –0.32).
The absence of a significant conditional effect between the presence of COVID-19 and positive mental health is a good thing for these last two scenarios. The interruptions brought by the pandemic either had no impact on positive mental health or improved it, in the case of students with low SA and high PI.
Third, school attachment also matters to the positive mental health of 2SLGBTQ + students. While parental involvement can protect the mental health and wellbeing of their children, it can only do so to a point. One striking finding (best illustrated in Figure 1) is that regardless of COVID-19 or the level of parental involvement, 2SLGBTQ + students with high school attachment report above average positive mental health. Thus, even at its lowest point (i.e., 2SLGBTQ + students during the first wave of the pandemic with low PI), students with high SA did better than participants with low SA and high PI. Other research shows the key role of school attachment, which is generally lower among 2SLGBTQ + students (Poteat et al., 2011; Peter et al., 2015). For instance, research has found that 2SLGBTQ + students’ sense of school belonging mediates the relationship between peer victimization and depression (Hatchel et al., 2018) and lowers suicidal ideation and attempts (Bariola et al., 2017). Unsurprisingly, experiences of discrimination and harassment in school lowers 2SLGBTQ + students’ school attachment (Diaz et al., 2010; Peter et al., 2015; Hatchel et al., 2019), which negatively impacts students’ grades, attendance, and the importance they place on education (Poteat et al., 2011; Peter et al., 2015).
Finally, taken together our findings confirm the joint importance of both parental involvement and school attachment (regardless of the pandemic) in maximizing the positive mental health of 2SLGBTQ + students. These results are encouraging, especially when we consider that COVID-19 will not last forever. If we look at pre-pandemic positive mental health scores, there is a standard score difference of 1.5 on positive mental health when we compare 2SLGBTQ + students with high SA and high PI (Y = 0.92) vs. those with low SA and low PI (Y = –0.62). The research literature supports the importance of both parental involvement and school attachment for 2SLGBTQ + youth (Poteat et al., 2011; Antonio and Moleiro, 2015; Hatchel et al., 2019).
Limitations
While the results are suggestive, we did not have panel data (meaning it is not the same students who completed the survey pre-pandemic and then during the first wave of the pandemic). By analyzing trend data, we are unable to calculate the net change and gross change of the outcome measure. In other words, it is possible that random differences between the specific students in each group contributed to the different mean positive mental health scores measured before the pandemic and during the first wave of COVID-19. With panel data researchers can control for such differences because they conduct the second part of their research with the same participants. However, panel data has its own limitations including fatigue or familiarity with the survey measures and attrition (participants dropping out over the course of the survey).
It is unreasonable to suggest that future research correct for this limitation. We do not expect that a large sample of 2SLGBTQ + students exists where researchers administered a survey before the pandemic and are able to contact the same group for further study.
Conclusion
The COVID-19 pandemic has had unprecedented impacts on the positive mental health of youth, their education, and the lives of students. While the extent of these impacts will not be fully known for some time, early indications suggest that marginalized populations, including 2SLGBTQ + youth, are experiencing these effects more acutely. Our results confirm that the pandemic has negatively affected the positive mental health of 2SLGBTQ + youth, an effect moderated by level of school attachment as well as the degree of parental involvement. More specifically, we saw the largest difference in positive mental health between 2SLGBTQ + students with high school attachment and low parental involvement. When this group took part during the first wave, their mean positive mental health was lower than that of 2SLGBTQ + students with the same characteristics measured pre-pandemic.
One exception to the general downward trend of positive mental health among 2SLGBTQ + students during the pandemic was among those with low school attachment and high parental involvement. Students from this group who took part after the cessation of in-person schooling reported higher positive mental health than students with those characteristics reported pre-pandemic. This suggests high parental involvement supports the positive mental health of 2SLGBTQ + youth, but with limited effects; students with high school attachment had higher positive mental health, which reveals how important school attachment is for 2SLGBTQ + youth. The implications of this for schools is clear and speaks to the importance of finding ways to ensure 2SLGBTQ + youth receive adequate support, at both home and school.
Data availability statement
The datasets presented in this article are not readily available because the use of the data provided to participants in the consent form includes only the release of aggregate results. Requests to access the datasets will be directed to the full report of results, which can be found at https://egale.ca/awareness/still-in-every-class/. Further enquiries about the Second Annual School Climate Survey of Homophobia, Biphobia, and Transphobia in Canadian Schools can be obtained by emailing TP, dHJhY2V5LnBldGVyQHVtYW5pdG9iYS5jYQ==.
Ethics statement
The studies involving human participants were reviewed and approved by the Psychology/Sociology Research Ethics Board at the University of Manitoba [Protocol# P2018:107 (HS22224)]. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
CC and TP: analysis and writing. LF: writing and editing. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by Egale Canada, with partial funding provided by the Dean’s Office discretionary research fund, Faculty of Arts, University of Manitoba.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
- ^ * 2SLGBTQ+ is an acronym for Two Spirit (2S), Lesbian, Gay, Bisexual, Transgender, Queer, and Questioning plus (+) other marginalized sexual or gender identities (e.g., asexual, gender non-binary, etc.). In this study, we list Two Spirit first to acknowledge and recognize that Indigenous peoples are the first peoples of Canada. We use 2SLGBTQ+ in our reporting except when referencing research that uses a different acronym.
References
Aiken, L. S., West, S. G., and Reno, R. R. (1991). Multiple Regression: Testing and Interpreting Interactions. Newbury Park, CA: Sage Publications.
Allen, B. J., Andert, B., Botsford, J., Budge, S. L., and Rehm, J. L. (2020). At the margins: comparing school experiences of nonbinary and binary-identified transgender youth. J. Sch. Health 90, 358–367. doi: 10.1111/josh.12882
Allen, K. A., and Bowles, T. (2012). Belonging as guiding principle in the education of adolescents. Aust. J. Educ. Dev. Psychol. 12, 108–119. doi: 10.3389/fpubh.2021.604668
Antonio, R., and Moleiro, C. (2015). Social and parental support as moderators of the effects of homophobic bullying on psychological distress in youth. Psychol. Sch. 52, 729–742. doi: 10.1016/j.jadohealth.2016.03.018
Arim, R., Findlay, L., and Kohen, D. E. (2020). The Health and Behavioural Impacts of COVID-19 on Youth: Results From the Canadian Perspectives Survey Series 1. Ottawa: Statistics Canada.
Bariola, E., Lyons, A., and Lucke, J. (2017). Flourishing among sexual minority individuals: Application of the dual continuum model of mental health in a sample of lesbians and gay men. Psychol. Sex. Orientat. Gend. Divers. 4, 43–53. doi: 10.1037/sgd0000210
Bouris, A., Guilamo-Ramos, V., Pickard, A., Shiu, C., Loosier, P. S., Dittus, P., et al. (2010). Systematic review of parental influences on the health and well-being of lesbian, gay, and bisexual youth: Time for a new public health research and practice agenda. J. Prim. Prev. 31, 273–309. doi: 10.1007/s10935-010-0229-1
Brown, S. M., Doom, J. R., Lechuga-Pena, S., Watamura, S. E., and Koppels, T. M. (2020). Stress and parenting during the global covid-19 pandemic. Child Abuse Negl. 110:104699. doi: 10.1016/j.chiabu.2020.104699
Day, J. K., Fish, J. N., Grossman, A. H., and Russell, S. T. (2020). Gay-straight alliances, inclusive policy, and school climate: lgbtq youths’ experiences of social support and bullying. J. Res. Adolesc. 30, 418–430. doi: 10.1111/jora.12487
Day, J. K., Ioverno, S., and Russell, S. T. (2019). Safe and supportive schools for lgbt youth: Addressing educational inequities through inclusive policies and practices. J. Sch. Psychol. 74, 29–43. doi: 10.1016/j.jsp.2019.05.007
Diaz, E. M., Kosciw, J. G., and Greytak, E. A. (2010). School connectedness for lesbian, gay, bisexual, and transgender youth: In-school victimization and institutional supports. Prev. Res. 17:15. doi: 10.1037/e597072010-005
Egale Canada (2020a). Impact of COVID-19: Canada’s LGBTQI2S Community in Focus. Toronto: Egale Canada.
Egale Canada (2020b). Second National Report: Impact of COVID-19 on Canada’s LGBTQI2S Community: Egale Canada, Innovative Research, and African-Canadian Civic Engagement Council.
Findlay, L., and Arim, R. (2020). Canadians Report Lower Self-Perceived Mental Health During the COVID-19 Pandemic. Ottawa: Statistics Canada.
Fish, J. N., McInroy, L. B., Paceley, M. S., Williams, N. D., Henderson, S., Levine, D. S., et al. (2020). “I’m kinda stuck at home with unsupportive parents right now”: LGBTQ youths’ experiences with covid-19 and the importance of online support. J. Adolescent Health 67, 450–452. doi: 10.1016/j.jadohealth.2020.06.002
Green, A., Price-Feeney, M., and Dorison, S. (2020). Implications of COVID-19 for LGBTQ Youth Mental Health and Suicide Prevention. New York, NY: The Trevor project.
Grossman, A. H., Park, J. Y., Frank, J. A., and Russell, S. T. (2021). Parental responses to transgender and gender nonconforming youth: associations with parent support, parental abuse, and youths’ psychological adjustment. J. Homosex. 68, 1260–1277. doi: 10.1080/00918369.2019.1696103
Hatchel, T., Espelage, D. L., and Huang, Y. (2018). Sexual harassment victimization, school belonging, and depressive symptoms among lgbtq adolescents: Temporal insights. Am. J. Orthopsychiatry 88, 422–430. doi: 10.1037/ort0000279
Hatchel, T., Merrin, G. J., and Espelage, D. (2019). Peer victimization and suicidality among lgbtq youth: The roles of school belonging, self-compassion, and parental support. J. LGBT Youth 16, 134–156. doi: 10.1080/19361653.2018.1543036
Hayes, A. F. (2018). Introduction to Mediation, Moderation, and Conditional Process Analysis a Regression-Based Approach, 2nd Edn. New York, NY: Guilford Press.
Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., et al. (2020). Multidisciplinary research priorities for the covid-19 pandemic: A call for action for mental health science. Lancet Psychiatry 7, 547–560. doi: 10.1016/S2215-0366(20)30168-1
Kelleher, C. (2009). Minority stress and health: implications for lesbian, gay, bisexual, transgender, and questioning (LGBTQ) young people. Couns. Psychol. Q. 22, 373–379. doi: 10.1080/09515070903334995
Keyes, C. L. M. (2002). The mental health continuum: from languishing to flourishing in life. J. Health Soc. Behav. 43, 207–222. doi: 10.2307/3090197
Keyes, C. L. M. (2006). Mental health in adolescence: Is america’s youth flourishing? Am. J. Orthopsychiatry 76, 395–402. doi: 10.1037/0002-9432.76.3.395
Kishchuk, O. (2020). COVID-19 & Canadian Youth: Impacts, Perspectives & the Recovery. Report Based on a National Survey of 1000 Canadians Aged 15 to 30: Abacus Data and Coalition of National Youth Serving Agencies. Ottawa: Abacus data.
Lefevor, G. T., Boyd-Rogers, C. C., Sprague, B. M., and Janis, R. A. (2019). Health disparities between genderqueer, transgender, and cisgender individuals: an extension of minority stress theory. J. Counsel. Psychol. 66, 385–395. doi: 10.1037/cou0000339
Moffa, K., Dowdy, E., and Furlong, M. J. (2016). Exploring the contributions of school belonging to complete mental health screening. Educ. Dev. Psychol. 33, 16–32. doi: 10.1017/edp.2016.8
Montoya, A. K. (2018). Moderation analysis in two-instance repeated measures designs: Probing methods and multiple moderator models. Behav. Res. Methods 51, 61–82. doi: 10.3758/s13428-018-1088-6
Needham, B. L., and Austin, E. L. (2010). Sexual orientation, parental support, and health during the transition to young adulthood. J. Youth Adolesc. 39, 1189–1198. doi: 10.1007/s10964-010-9533-6
Peter, T., Campbell, C. P., and Taylor, C. (2021). Still in Every Class in Every School: Final Report on the Second Climate Survey on Homophobia, Biphobia, and Transphobia in Canadian Schools. Toronto:Egale Canada.
Peter, T., Edkins, T., Watson, R., Adjei, J., Homma, Y., and Saewyc, E. (2017). Trends in suicidality among sexual minority and heterosexual students in a canadian population-based cohort study. Psychol. Sex. Orient. Gender Divers. 4, 115–123. doi: 10.1037/sgd0000211
Peter, T., Taylor, C., Ristock, J., and Edkins, T. (2015). Pride and prejudice: Factors affecting school attachment among lesbian, bisexual, and heterosexual girls. J. Lesbian Stud. 19, 249–273. doi: 10.1080/10894160.2015.969127
Poteat, V. P., Mereish, E. H., DiGiovanni, C. D., and Koenig, B. W. (2011). The effects of general and homophobic victimization on adolescents’ psychosocial and educational concerns: The importance of intersecting identities and parent support. J. Couns. Psychol. 58, 597–609. doi: 10.1037/a0025095
Preacher, K. J., and Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 40, 879–891. doi: 10.3758/BRM.40.3.879
Prokopenko, E. (2020). Vulnerabilities Related to COVID-19 Among LGBTQ2+ Canadians. Ottawa: Statistics Canada.
Public Health Agency of Canada (2020). From Risk to Resilience: An Equity Approach to COVID-19. Chief Public Health Officer of Canada’s Report on the State of Public Health in Canada 2020. Ottawa: State of Public Health in Canada.
Reisner, S. L., Sava, L. M., Menino, D. D., Perrotti, J., Barnes, T. N., Humphrey, D. L., et al. (2020). Addressing lgbtq student bullying in massachusetts schools: Perspectives of lgbtq students and school health professionals. Prev. Sci. 21, 408–421. doi: 10.1007/s11121-019-01084-4
Saewyc, E. M., Konishi, C., Rose, H. A., and Homma, Y. (2014). School-Based Strategies to Reduce Suicidal Ideation, Suicide Attempts, and Discrimination among Sexual Minority and Heterosexual Adolescents in Western Canada. Int. J. Child Youth Fam. Stud. 5, 89–112. doi: 10.18357/ijcyfs.saewyce.512014
Spencer, S. M., and Patrick, J. H. (2009). Social Support and Personal Mastery as Protective Resources During Emerging Adulthood. J. Adult Dev. 16, 191–198. doi: 10.1007/s10804-009-9064-0
Statistics Canada (2020a). Canadian Perspectives Survey Series 1: Impacts of COVID-19. Ottawa: Statistics Canada.
Statistics Canada (2020b). Study: The COVID-19 Pandemic Takes a Toll on Life Satisfaction. Ottawa: Statistics Canada.
Tabachnick, B. G., and Fidell, L. S. (2007). Using Multivariate Statistics, 5th Edn. Boston, MA: Allyn & Bacon.
Veale, J. F., Peter, T., Travers, R., and Saewyc, E. M. (2017). Enacted stigma, mental health, and protective factors among transgender youth in canada. Transgend. Health 3, 27–216. doi: 10.1089/trgh.2017.0031
Veale, J. F., Watson, R. J., Peter, T., and Saewyc, E. M. (2016). Mental health disparities among canadian transgender youth. J. Adolesc. Health 60, 44–49. doi: 10.1016/j.jadohealth.2016.09.014
Watson, R. J., Peter, T., McKay, T., Edkins, T., and Saewyc, E. (2018). Evidence of Changing Patterns in Mental Health and Depressive Symptoms for Sexual Minority Adolescents. J. Gay Lesbian Ment. Health 22, 120–138. doi: 10.1080/19359705.2018.1427646
Keywords: 2SLGBTQ, school attachment, positive mental health, parental involvement, COVID-19, school closures, students, Canadian schools
Citation: Campbell C, Fraser L and Peter T (2022) The impact of school attachment and parental involvement on the positive mental health of 2SLGBTQ + students during COVID-19. Front. Educ. 7:957543. doi: 10.3389/feduc.2022.957543
Received: 31 May 2022; Accepted: 24 August 2022;
Published: 20 September 2022.
Edited by:
Terrell Lamont Strayhorn, Illinois State University, United StatesReviewed by:
Giuseppe Mannino, Libera Università Maria SS. Assunta, ItalyMark Vicars, Victoria University, Australia
Copyright © 2022 Campbell, Fraser and Peter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ley Fraser, bGZyYXNlckBteXVtYW5pdG9iYS5jYQ==