 Sonja Mohr
Sonja Mohr Birgit Küfe1
Birgit Küfe1 Jennifer Guse
Jennifer Guse- 1Dean’s Office for Student Affairs, Faculty of Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Department of Medical Psychology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Higher education has changed significantly since the beginning of the COVID-19 pandemic. Medical education programs with extensive practical and interactive components faced major challenges to protect students, faculty and patients. In response to COVID-19, many medical schools worldwide shut down undergraduate medical education and converted most of their teaching to digital formats. The aim of this paper is to assess the attitude towards and adoption of the novel learning environment among undergraduate medical students during COVID-19. Two studies were conducted to analyze specific aspects of the adaption of digital teaching during the digital summer semester 2020 (study 1), and to compare student satisfaction and their feeling of preparedness for exams in the digital semester compared to traditional semesters (study 2). Results show that there are numerous pros and cons of digital teaching. Pros were the large flexibility and large-scale availability of digital teaching materials. Cons were the lack of interactions with peers, professionals, and patients in practice. Results also show that female students as well as year 1 students seemingly coped better with the digital learning environment. Students with childcare or job obligations also benefited from the large flexibility. While student satisfaction decreased in the digital semester, they did not feel less prepared for exams. Cross-sectional comparisons revealed that student satisfaction and agreement gradually decreased in the comparison of the different cohorts with fourth year students being the least satisfied and showing the least agreement regarding the feeling of preparedness for exams. Altogether, our results indicate that students were able to cope with digital teaching, but clearly, some groups of students were able to better adapt to the novel learning environment. This might demand the introduction of tailored educational support services for different groups of students during COVID-19 as they progress through medical school.
Introduction
The coronavirus disease (COVID-19) pandemic and its consequences have an impact on private, professional and social life of the general population and specific groups (Vindegaard and Benros, 2020). Higher education has changed significantly since the beginning of the pandemic. Particularly, study courses with extensive practical and interactive components such as medical education faced major challenges to protect students, faculty and patients, and flatten the curve by social distancing while ensuring the educational mission at the same time. Undergraduate medical education usually applies many different formats in teaching (i.a., bedside-teaching, laboratory courses, practical training) and in assessment (i.a., Multiple-Choice-Questions, Objective Structured Clinical Examinations, mini-clinical evaluation exercise) (Holzinger et al., 2020; Vanderbilt et al., 2013). In response to COVID-19, many medical schools worldwide shut down undergraduate medical education and converted most of their teaching to digital formats (Rose, 2020). In addition, the exams changed significantly. For example, all Objective Structured Clinical Examinations (OSCE) were converted into Multiple Choice tests. This rapid change of the learning environment may cause several effects among medical students. Both, positive and negative effects of the learning environment on health profession education have been reported (Gruppen et al., 2019; Weiss et al., 2013) and strategies to improve the learning environment in undergraduate medical education to promote students’ well-being were recommended before the pandemic began (Wasson et al., 2016; Dyrbye et al., 2020). Learning environments that are perceived as unsupportive are typically associated with high levels of depression, burnout or exhaustion and medical students’ level of mental health decreases the further they progress in their undergraduate medical education (Brazeau et al., 2014; Dyrbye et al., 2010; Schwenk et al., 2010).
The definition of the learning environment by Gruppen et al. (2019) serves as an important background for this study: “Learning environment refers to the social interactions, organizational cultures and structure, and physical and virtual spaces that surround and shape the learners’ experience, perceptions and learning.” The rapid change to digital formats and asynchronous teaching resulted in a dramatic decrease of social interactions. The organizational culture in medical education depends on a direct interaction between physicians and students, especially in clinical teaching. The organizational structure of medical education with its complex and multifaceted class schedules could be relatively easily arranged for digital teaching, because a unique digital tool for the administration of curricula already existed at the University Medical Center of Hamburg-Eppendorf. Using this platform, the Faculty could control the virtual space that shapes the students’ experiences. However, the physical environment of students could no longer be controlled and might be an important aspect of how students’ handled the situation.
There is limited evidence on how a pandemic and its consequences affect medical education. However, some previous studies provide some insight that has to be considered in the context of the present paper. A study during the SARS pandemic showed that the elimination of routines and the massive reduction in social contact often led to boredom, frustration, and a sense of isolation from the outside world (Hawryluck et al., 2004; Reynolds et al., 2008). A few studies targeting higher health education were published early on in the COVID-19 pandemic: Chen et al. (2021) showed that the rapid introduction of synchronous e-learning initially worsened the learning of dental students. Consequently, asynchronous formats and the recording of lectures were introduced. This was well received by students, because they could use the recorded material for review. In a qualitative study, Khalil et al. (2020) assessed medical students’ perspectives on synchronous online learning. Results also show that the utilization of recorded lectures was well perceived. Another important benefit was time efficiency of online learning. Students also reported methodological (e.g., timing and lecture duration), technical (e.g., internet connectivity and sound quality), and behavioral challenges (e.g., lack of interaction and individual learning style).
The aim of this study is to assess the attitude towards and adoption of the novel learning environment among a large sample of undergraduate medical students during COVID-19 (study 1). Therefore, students’ perceptions of positive and negative effects of the online teaching formats compared to the diverse face-to-face teaching formats were assessed. Second, the aim was to find out how the novel learning environment affected students’ satisfaction, and their view on preparedness for exams (study 2).
Materials and Methods
Setting
Both studies are cross-sectional surveys conducted at the University Medical Center Hamburg-Eppendorf (UKE), Germany. Undergraduate medical education in Germany encompasses either traditional study courses or reform study courses as full education programs with a duration of 6 years including a practical year at the end. The Medical Faculty in Hamburg is one of the larger faculties in Germany with cohorts consisting of approximately 370 medical students per year and launched the longitudinal integrated medical degree program iMED in 2012. Altogether, the reformed integrated curriculum iMED consists of 19 modules. In each semester, medical students attend two modules in a given order. Each module lasts for 6 weeks. A week of exams follows each module in the first three semesters. From the fourth semester onward, exams are conducted in the last week of the semester after both modules have been completed. At UKE, students are invited to participate in the end-of-semester evaluation from the very beginning of the program. Participation in the anonymous online-questionnaire is voluntary, but highly recommended. More precisely, the whole population of medical students is eligible to participate in the evaluation each semester. The actual samples are made up of participants who have voluntarily chosen to participate.
Study 1
In study 1, students participated in an additional voluntary evaluation 6 weeks into the semester (May, 2020) as well as at the end of the semester (July, 2020). The online survey was conducted from May 28, 2020 to June 7, 2020 (t1), and from July 14, 2020 to July 30, 2020 (t2). During this period and before (since mid-March 2020), the German government announced several public health measures to suppress the spread of COVID-19 by increasing social distancing. The following measures were predominantly used: the closure of schools, daycare, playgrounds and non-essential shops, and the prohibition to meet more than one person from another household. Lectures and seminars were held in a digital format–presentations with audio recordings in the majority of cases–to diminish interpersonal contact and protect patients, students and faculty.
This study utilized a mixed-methods design following a sequential explanatory strategy (Creswell, 2014). In this, a set of new self-developed or adapted items was integrated in the questionnaires. In this process, the student council was consulted to ensure that all relevant aspects of digital teaching were captured in the questionnaire. The items in the formative evaluation (May, 2020) targeted the identification of technical issues as well as the technical application of digital teaching methods. Students were also asked to assess whether presentations with audio recordings were inferior, superior or equivalent to face-to-face teaching in lectures, seminars, bedside teaching, and practical training. At the end of the semester, an assessment of the positive and negative perceptions of digital teaching was implemented in the questionnaire (see Table 1). Additionally, students were asked to describe positive and negative aspects of the digital teaching compared to usual teaching in an open-ended question. The integration of this qualitative source of data at t2 was needed to better understand how students handled the first digital semester at our Faculty. Also, the sequential analysis of follow-up qualitative data helped explain the quantitative results.

TABLE 1. Descriptive statistics of items regarding positive and negative perceptions of digital teaching (study 1).
Study 2
In study 2, end-of-semester evaluations of the digital semester as well as two previous summer semesters were compared. Response rates are usually above 90%. The questionnaire to evaluate all study modules is comprised of self-constructed items that cover general perceptions of the module and the study program as well as subject-specific items since the implementation of iMED in 2012. In this paper, three items regarding the module or study program in general were analyzed: Every semester, students are asked to rate their current satisfaction with iMED as well as the completed module. In addition, students were asked to assess whether they knew what they had to learn for the exams. All items are assessed using a 6-point Likert scale ranging from 1 = not at all to 6 = absolutely.
Participants Study 1
Study 1 participants were 959 medical students (62% female) who completed the formative evaluation (population = 1,544 students; response rate = 62%) in May 2020. At the end of the semester in July 2020, 1,425 students (58% female) participated in the evaluation (population = 1,501 students; response rate = 95%). 50% (May 2020) and 56% (July 2020) of students were between 21 and 25 years old respectively. Four different cohorts of students participated in the evaluation (July 2020): 338 (24%) first year students (second semester), 338 (24%) second year students (fourth semester), 430 (30%) third year students (sixth semester), and 319 (22%) fourth year students (eighth semester).
Participants Study 2
Participants were N = 4,215 medical students who participated in the end-of-semester evaluation in the summer semester 2018 (n = 1,382, population = 1,476 students; response rate 94%), summer semester 2019 (n = 1,408, population = 1,477 students; response rate 95%) and summer semester 2020 (n = 1,426, population = 1,501; response rate 95%). 58% were female. The majority of students (55%) was between 21 and 25 years old. In each of the three semesters, four different cohorts of students participated in the evaluation.
Quantitative Analysis
Perceptions of students were compared using either Kruskal-Wallis tests or Mann-Whithney U tests due to skewed distributions. In study 1, a Bonferroni correction was applied due to multiple testing, resulting in a significance level of 0.006 (0.05/8). In study 2, a Bonferroni correction was applied resulting in a significance level of 0.017 (0.05/3). Effect size calculations were conducted to determine the magnitude of the differences. According to Cohen’s guidelines (Cohen, 1988), r = 0.10 was considered to be a small effect, r = 0.30 as a medium effect, and r = 0.50 as a large effect. In terms of the effect size eta-squared, η2 = 0.01 was considered as a small effect, η2 = 0.06 as a medium effect, and η2 = 0.14 as a large effect.
Qualitative Analyses
In study 2, all comments by the students were analyzed using an inductive category formation in MAXQDA 2018 (VERBI GmbH). Two top-level codes, namely positive and negative effects of digital teaching, were set beforehand. Initially, one coder (BK) worked through two modules to build a coding frame containing categories associated with one of these top-level codes. Afterwards, all documents were completely worked through by two coders to share the workload (BK, SM). In a next step, all codes in all categories were screened to identify discrepancies in category attribution and to consolidate ambiguous categories. This coding and counting process of the qualitative data enabled the connection to quantitative data.
Ethical Considerations
The study was realized in accordance with the Declaration of Helsinki (World Medical Association, 2013). Participation in the studies was voluntary. The permission to evaluate teaching and learning is granted in the Hamburg higher education act (section 111 subsection 2, Hamburgisches Hochschulgesetz, HmbHG). At our faculty, data analyses and dissemination processes are regulated in the “Statutes of evaluation of teaching and learning at the Medical Faculty, University of Hamburg.” When entering iMED, students officially consent to the procedures of the web-based evaluation. The consent is voluntary, and over 99% of students give it. The anonymity of students is guaranteed.
Results
Study 1
The results of the formative evaluation 6 weeks into the semester showed that students agreed to the statement that they were able to use the digital teaching offers with their technical equipment as well as their internet connection (N = 945, M = 5.17, SD = 1.12, Mdn = 6). Students also strongly agreed that they were able to make use of the different digital teaching methods (presentations with audio recordings: N = 946, M = 4.98, SD = 1.17, Mdn = 5; video conference: N = 796, M = 4.78, SD = 1.35, Mdn = 5; videos: N = 845, M = 4.73, SD = 1.40, Mdn = 5). 52% of students felt that presentations with audio recordings were superior to face-to-face lectures. In contrast, the majority of students felt that presentations with audio recordings were inferior regarding seminars (60%), bedside teaching (79%), and practical training (80%).
Several items regarding the adaption of digital teaching were assessed in study 1 (July, 2020). None of the items were normally distributed. The largest approval was found regarding the appreciation of the possibility to use digital teaching material repeatedly (see Table 1). Sixty percent of students stated they very often or often made use of this possibility. All items regarding positive perceptions of digital teaching were negatively skewed. Perceptions of negative aspects were somewhat heterogeneous resulting in rather bimodal distributions with larger groups of students disagreeing or agreeing to the statements, respectively.
Within this study, four different cohorts of students participated in the evaluation (year 1 students/second semester; year 2 students/fourth semester; year 3 students/sixth semester; year 4 students/eighth semester). In a next step, differences between students of different cohorts were analyzed (see Supplementary Table S1). Figure 1 illustrates that first year students were seemingly able to cope with the negative aspects of digital teaching the best, because they agreed the least with these statements. First year students also agreed most to the positive aspects of digital teaching. In contrast, second year students agreed most to negative aspects of digital teaching, and disagreed most to positive aspects of digital teaching, respectively. Kruskal-Wallis tests were statistically significant (p < 0.006) in all but two comparisons (see Supplementary Table S1). There were no statistically significant differences regarding the items “I appreciate the use of digital teaching offers independently of time and location” as well as “I appreciate the possibility to use digital teaching material repeatedly.” Post-hoc tests served to show which groups were different from each other. Effect sizes of post-hoc tests were rather small, but the most substantial differences were found between first and second year students. The effect sizes of these pairwise comparisons in the post-hoc test varied between r = 0.14 and r = 0.23.
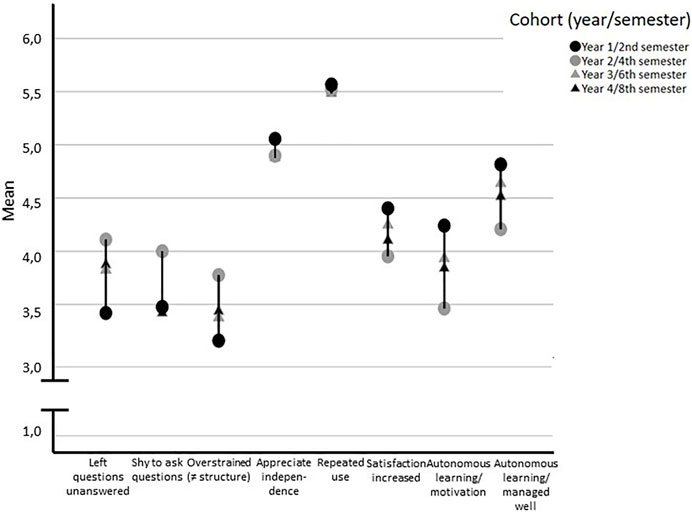
FIGURE 1. Drop-line chart showing the difference of positive and negative perceptions of digital teaching between four cohorts.
Analysis of gender differences showed that female students’ perceptions were different from male students’ perceptions in the majority of items (see Figure 2; Supplementary Table S2). After a Bonferroni correction for multiple comparisons, three statistically significant differences were detected (p < 0.006). Male students agreed more to the statement that the lack of a time frame and structure in the digital teaching made them feel overstrained, representing a small effect (r = 0.13). In contrast, female students agreed more to the statement that digital teaching increased their study satisfaction (r = 0.09) as well as the statement that digital teaching motivated them to continuously pursue autonomous learning (r = 0.10).
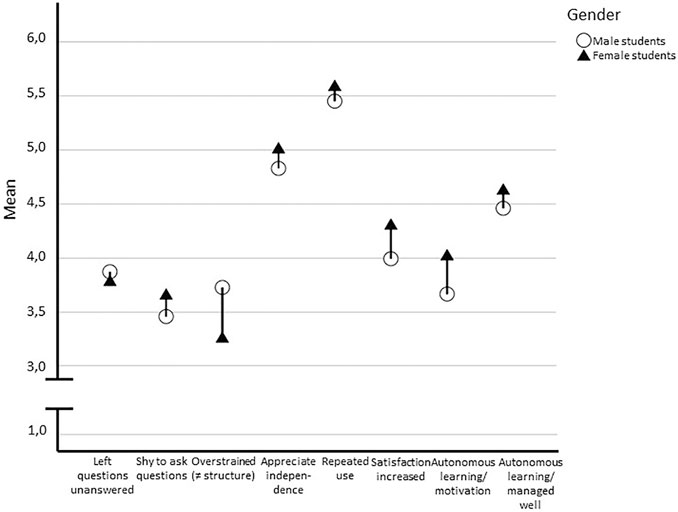
FIGURE 2. Drop-line chart showing the difference of positive and negative perceptions of digital teaching between male and female students.
Lastly, differences between age groups were analyzed. This additional analysis is called for, because the cohort is oftentimes not a strong predictor of the age group due to the complex admission procedures in Germany (e.g., applicants can be put on a waiting list for up to 7 years to get into university). In our study, the age group was not strongly associated with the cohort (r = 0.252, p < 0.000). Therefore, differences between age groups regarding all eight items on the adaption of digital teaching were analyzed. Results show that two statistically significant differences between age groups were detected (p < 0.006; see Supplementary Table S3). Older students agreed more to the statement that digital teaching increased their study satisfaction (M = 4.75, SD = 1.52, Mdn = 5; H = 30.26, p < 0.000, η2 =0.02). In addition, older students agreed the least that digital classes left more questions unanswered for them than face-to-face teaching (M = 3.38, SD = 1.74, Mdn = 4; H = 21.55, p < 0.000, η2 =0.014).
At the end of the semester, students were asked for positive and negative aspects of digital compared to face-to-face teaching in a free text format. Four hundred seventeen (29%) students responded to this free-choice question. These students mentioned 705 aspects of which 50% were positive (n = 357 codings within 13 sub-codes) and roughly 50% were negative (n = 349 codings within 12 sub-codes). All sub-codes including their frequencies are presented in Table 2.
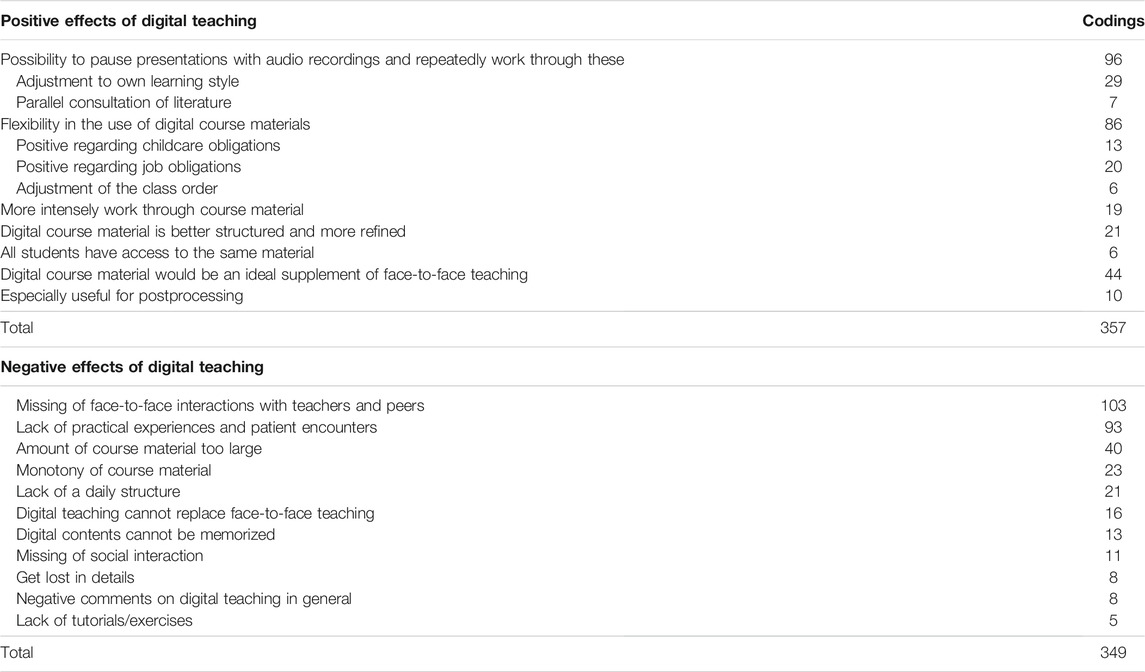
TABLE 2. Codes and categories of study 1 qualitative data including frequencies.
One theme stood out within the positive code, namely the possibility to pause presentations with audio recordings and repeatedly work through these (n = 132 codings). Especially, students appreciated the fact that this format allowed them to adjust their studies to their own learning style.
“It’s great to have your own schedule. If you need a break, you just pause the presentation. You can listen to the presentation repeatedly while consulting relevant literature.”
The second most important positive aspect was the large flexibility in the use of digital course materials (n = 125 codings). Students appreciated the fact that they could access the materials whenever and wherever they wanted. Within this sub-code, 33 students emphasized the advantages of this format for students with other responsibilities like childcare or part-time jobs.
“It’s just positive. Self-regulated learning and this freedom enabled me to better structure my obligations as a student, mother and employee.”
Within the negative code, many students described how they missed the face-to-face interaction with teachers and peers (n = 103 codings). The students argued that asynchronous interaction (e.g., via e-mail) had negative effects on their learning. Some students mentioned that they were reluctant to ask questions via e-mail or in video conferences.
“The lack of interaction and the lack of the possibility to develop questions within a conversation stand in the way of sustainable learning.”
The second most important negative effect was the lack of practical experiences and patient encounters (n = 93 codings). Many students were disappointed and emphasized that they were unable to improve their competence because of the missing application of theoretical knowledge in practice.
“I have the feeling that a lot less knowledge got stuck due to the lack of practical teaching.”
Study 2
In study 2, end-of-semester evaluations of the digital semester as well as two previous semesters were compared (Table 3). Results of a Kruskal-Wallis test showed that the feeling of preparedness for exams was not associated with the semester [H (2) = 5.96, p = 0.051]. Results regarding the difference in satisfaction with iMED showed that satisfaction was associated with the semester [H (2) = 14.47, p = 0.001]. Post-hoc tests revealed that satisfaction was lower in the digital semester compared to both other semesters, representing small effects. The same was found for the satisfaction with the module: students were the least satisfied in the digital semester compared to the two previous semesters [H (2) = 38.93, p > 0.001]. The pairwise comparisons were also small in effect size.

TABLE 3. Descriptive statistics of study 2.
Within each semester, four different cohorts of students participated in the evaluation (year 1 students/second semester; year 2 students/fourth semester; year 3 students/sixth semester; year 4 students/eighth semester; see Supplementary Table S4). In this analysis, the digital summer semester 2020 stood out in different ways. In both previous summer semesters (2018 and 2019) first year students were the most satisfied and agreed most in all three items. Student satisfaction and agreement gradually decreased in the comparison of the different cohorts with fourth year students being the least satisfied and showing the least agreement regarding the feeling of preparedness for exams. Kruskal-Wallis tests were statistically significant in all comparisons. Medium sized effects were detected in the comparisons of cohorts in 2018 and 2019 (see Supplementary Table S4). Post-hoc tests of these results revealed that the largest effect sizes of pairwise comparisons of the cohorts were found between first and fourth year students (r = 0.28–0.35). In 2020, we identified a different pattern. First year students’ satisfaction with the module and the program was lower than in previous semesters, resulting in scores approximately on the level of third year students. First year students also felt less prepared for exams than in previous semesters. Effect sizes were rather small in 2020 compared to the previous semesters (see Supplementary Table S4). Pairwise comparisons of post-hoc tests also revealed smaller effects (r = 0.13–0.21). All means of the different cohorts in all three semesters are presented in Figure 3.

FIGURE 3. Drop-line chart showing the difference of satisfaction and feeling of preparedness for exams between four cohorts.
In a next step, differences regarding gender and age were analyzed. Therefore, data of the three different semesters were split to investigate each semester separately. A statistically significant difference between male and female students was found with female students being more satisfied with the module in the digital semester (female students: n = 808, M = 4.66, SD = 1.05, Mdn = 5; male students: n = 516, M = 4.44, SD = 1.25, Mdn = 5; U = 192,247.5, z = −2.518, p = 0.012, r = 0.06). None of the other comparisons of male and female students were statistically significant (see Supplementary Table S5).
Since the age group was not strongly associated with the cohort/semester (r = 0.274, p < 0.000), the differences between students in the four age groups were additionally analyzed. Results showed that age group was associated with the three items. Several statistically significant differences between students of different age groups were detected, however effect sizes were small (see Supplementary Table S6). Students in the age group <21 years were the most satisfied with the study program in all three semesters. Students in the age group >31 years were the least satisfied with the study program in all three semesters. The same pattern of satisfaction was found regarding the item “satisfaction with module.” However, a statistically significant difference was only detected for the summer semester 2019. The only statistically significant differences between students in different age groups regarding the item “feeling of preparedness for exams” was found in the summer semester 2019. Students in the age group <21 years felt the most prepared while students between 21 and 25 years as well as students >31 years felt less prepared for exams. All pairwise comparisons in follow-up post-hoc analyses of statistically significant effects represented small to medium effect sizes.
Discussion
Overall, the results indicate that students coped well with the usage of the digital teaching offers. Unlike the results of Khalil et al. (2020) suggest, technical challenges were not prevalent in the present study. It depended on the teaching format whether students rated digital teaching offers superior or inferior to non-digital teaching: More than half of the students even appreciated presentations with audio recordings more than non-digital lectures whereas the majority evaluated digital practical training, bedside-teaching, and seminars inferior compared to non-digital formats. It is no wonder that lectures with audio recordings that can be replayed as much as one needs to comprehend the contents are appreciated most by students (Khalil et al., 2020; Chen et al., 2021). In all probability, the content availability has never been this convenient before.
Meaningful (Online) Learning Experiences
The reported inferiority of certain digital teaching offers could be explained by a lack of meaningful learning experience (Rusticus et al., 2014). Meaningful learning experiences as one scale of the Medical School Learning Environment Survey developed by (Marshall, 1978) and modified by (Feletti and Clarke, 1981) represents the degree to which students perceive that the educational experience is relevant to the practice of medicine. The extreme reduction of social interaction can also be identified as a negative aspect of digital teaching and learning. The qualitative findings of this study corroborate this assumption: The students argued that the lack of interactions had negative effects on their learning.
Online Learning Style
Both quantitative and qualitative results of the present study add to the body of research on (online) learning style of medical students. Students stated that the online format allows them to adjust their studies to their own learning style (Khalil et al., 2020). Seemingly, students with childcare or job obligations did profit the most. A recent study among undergraduate dental students reported that performing digital learning activities in an office or study room was an important factor to maintaining a high quality of life (Silva et al., 2021). In general a suitable environment that allows an adequate level of concentration (McCutcheon et al., 2015) is crucial for improved academic performance (Kirschner et al., 1997). Students with childcare or job obligations as well as older students might be more likely to have such a learning environment than younger students due to financial resources. As mentioned before, another positive factor might be the opportunity to manage their numerous obligations on their own terms. Altogether, the flexibility and control within the novel learning environment in terms of the possibility to use digital teaching material repeatedly and independent of time and location was most appreciated by the students.
The Role of Sample Characteristics
Three sample characteristics were analyzed in this study: medical education level, gender, and age group. Interestingly, first year students disagreed most to the negative aspects of digital teaching, and agreed most to the positive aspects of digital teaching, respectively. The background of these results could be the structure of the undergraduate medical curriculum with predominantly preclinical subjects, which can be more easily studied with the help of presentations with audio recordings, and few practical training in the first year (Chenot, 2009; Hense et al., 2021; Rheingans et al., 2019). Furthermore, prior research among undergraduate medical and dental students found that students adopted a different learning approach (Lee at al., 2020; Wickramasinghe and Samarasekera, 2011) and increased levels of stress (Erschens et al., 2018) with the entry to clinical training. This might account for our findings that second year students (fourth semester) agreed most to negative aspects of digital teaching, and disagreed most to positive aspects of digital teaching, respectively. At the University Medical Center of Hamburg-Eppendorf, the large cohort of approximately 370 students is divided into four groups after the third semester, and students enter the second stage of the program in which the complexity as well as clinical teaching offers are increased (Rheingans et al., 2019). This might be an explanation why second year students perceptions stand out in the analysis.
In addition, gender differences were revealed in the analysis. While male students felt more overstrained, female students seemingly coped better with the digital learning environment. A study in relation to the COVID-19 pandemic by Salfi et al. (2020) also showed that women in the Italian population seemed to cope better with the ongoing lockdown measures. Nevertheless, our findings do not refer to mental health issues, but to the handling of educational challenges. In this regard, our findings are interesting, because it was shown that women “define themselves as higher in relational interdependence than men, and men define themselves as higher in independence/agency than women” (Guimond et al., 2006, p. 221). Findings of other studies in medical education on how motivation affects medical students suggest that male and female student’ quantity and quality of motivation differ: female students have higher autonomous motivation than male students, and male students have higher controlled motivation than female students (e.g., Kusurkar et al., 2013). The absence of perceived approval from others as well as the fact that any external reinforcement was missing during the digital, asynchronous teaching might have led male students to feel more overstrained than female students. Nevertheless, future studies will be needed to further analyze how female students coped with the lack of social interaction despite the fact that relational interdependence is evidently more important to women.
Additionally, a few differences between age groups were detected in study 1. On the one hand, older students agreed more to the statement that digital teaching increased their study satisfaction. On the other hand, this group of students agreed more that digital teaching left more questions unanswered for them than face-to-face teaching. Older students might have to face more job and family obligations. The very flexible, asynchronous digital teaching makes it easier for this group to manage their several obligations, which might have resulted in their higher study satisfaction.
In-Person vs. Distance Medical Education
Results of study 2 showed that satisfaction with the integrated study course iMED decreased during distance medical education compared to previous in-person medical education summer semesters. Interestingly, students did not feel less prepared for exams. This might be because exams were organized in a multiple-choice format only. Nonetheless, students’ quantitative ratings as well as their written statements indicate that many questions were left unanswered due to missing interaction and practical experiences. It has been reported that students’ perceptions of the medical school learning environment is associated with satisfaction (Genn, 2001). In the comparison of four different cohorts, a particular pattern was detected in the digital semester (2020). Differences between cohorts in terms of the satisfaction with the module were smaller than in previous semesters. Fourth year students felt the least prepared for exams. In this advanced stage of medical education, the practical study components are usually particularly high (Hense et al., 2021; Rheingans et al., 2019) and are probably the most difficult to learn digitally. Altogether, the finding that satisfaction seemingly decreased during the course of medical school could be associated with the fact that the mental health of students also changes throughout the course of the semesters and is increasingly characterized by distress (Dyrbye et al., 2009).
Only one statistically significant difference between male and female students was detected in study 2 with female students being more satisfied with the module in the digital semester. This finding is in accordance with the findings of study 1 in which females were also found to have more positive perceptions of digital teaching and learning. The comparison of age groups revealed a remarkable difference in the satisfaction with the study program: Younger students were the most satisfied and older students were the least satisfied. The fact that older students were the least satisfied might be associated with multiple obligations of older students (e.g., job, family), although this group explicitly pointed out the advantages of digital learning in study 1.
Limitations
Both studies have several limitations. The cross-sectional design does not allow causal statements. The representativeness is limited due to the implementation at a single institution. In study 1, there were differences in terms of response rates. Students are used to complete an extensive evaluation at the end of each semester. Also, at the end of the semester all exams are completed for both modules of the semester. This might be the reason why students were not as committed to evaluate the module 6 weeks into the semester as usual. Consequently, the response rates were different. In addition, despite many statistically significant associations, effect sizes were small, which may be due to the big sample size that increases the likelihood for the p value to become statistically significant.
Nevertheless, we assume that those limitations could be compensated partially. A particular strength of both studies is the high response rate and the consideration of quantitative and qualitative data (Frambach et al., 2013). The approach of conventional content analysis can be used when existing theories or literature are limited. The information comes directly from the participants without predefined categories (Hsieh and Shannon, 2005; Patton, 2014). Quantifying the qualitative data can also facilitate the process of assigning meaning through pattern recognition by identifying consistencies and inconsistencies in the data, especially when analyzing large data sets (Neale et al., 2014; Monrouxe and Rees, 2020). Another limitation is the lack of results on mental health of students that could amplify the reasoning of the present study.
Conclusion
Altogether, our results indicate that the attitude towards the novel learning environment in medical education is comprised of negative as well as positive aspects. Despite several advantages in terms of the flexibility and large-scale availability of digital teaching materials, medical students were seriously affected by the lack of interactions with peers, professionals, and patients in practice. This corroborates the results of previous studies that were conducted during the SARS pandemic (Hawryluck et al., 2004; Reynolds et al., 2008). Participation in activities via telephone or video meeting could not compensate for the negative emotional states (Jeong et al., 2016). Since the undergraduate medical education is very structured (Chenot, 2009) this effect might account in parts for the negative perception of the students. At the same time, the structured curriculum enables the Faculty to more easily make digital learning materials accessible. Furthermore, social support in terms of peers and faculty as well as physical space for gathering is considered one important domain of system-level factors that influence learner well-being (Dyrbye et al., 2020).
In particular, the differences regarding gender, age group, and semester might demand the introduction of tailored educational support services for students during COVID-19 as they progress through medical school. This has to be acknowledged by Universities, since there is not a single strategy that will match all students’ needs. In addition, longitudinal studies are needed as the pandemic continues to monitor the perceived impact of the novel learning environment.
Data Availability Statement
The datasets presented in this article are not readily available because evaluation data cannot be shared publicly because of internal data protection reasons. The Medical Faculty, in this case represented by the Vice Dean for student affairs, does not allow the non-aggregated publication of student evaluation data. This regulation is specified in §5 of the “Statutes of evaluation of teaching and learning at the Medical Faculty, University of Hamburg.” Requests to access the datasets should be directed to SM, cy5tb2hyQHVrZS5kZQ==.
Author Contributions
All authors contributed to the conception and design of the studies. SM and BK analysed the quantitative and qualitative data. SM and JG wrote the manuscript in consultation with BK and AR. AR supervised the studies.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank all undergraduate medical students for their participation in the voluntary evaluation.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2021.714526/full#supplementary-material
References
Brazeau, C. M., Shanafelt, T., Durning, S. J., Massie, F. S., Eacker, A., Moutier, C., et al. (2014). Distress Among Matriculating Medical Students Relative to the General Population. Acad. Med. 89, 1520–1525. doi:10.1097/acm.0000000000000482
Chen, E., Kaczmarek, K., and Ohyama, H. (2021). Student Perceptions of Distance Learning Strategies during COVID‐19. J. Dent. Educ. 85 (Suppl. 1), 1190–1191. doi:10.1002/jdd.12339
Chenot, J. F. (2009). Undergraduate Medical Education in Germany. Ger. Med. Sci. 7, Doc02. doi:10.3205/000061
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences. New York, NY: Academic Press.
Creswell, J. W. (2014). Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Thousand Oaks, CA: SAGE Publications.
Dyrbye, L. N., Lipscomb, W., and Thibault, G. (2020). Redesigning the Learning Environment to Promote Learner Well-Being and Professional Development. Acad. Med. 95, 674–678. doi:10.1097/ACM.0000000000003094
Dyrbye, L. N., Massie, F. S., Eacker, A., Harper, W., Power, D., Durning, S. J., et al. (2010). Relationship between Burnout and Professional Conduct and Attitudes Among US Medical Students. JAMA 304, 1173–1180. doi:10.1001/jama.2010.1318
Dyrbye, L. N., Thomas, M. R., Harper, W., Massie, F. S., Power, D. V., Eacker, A., et al. (2009). The Learning Environment and Medical Student Burnout: A Multicentre Study. Med. Educ. 43, 274–282. doi:10.1111/j.1365-2923.2008.03282.x
Erschens, R., Herrmann-Werner, A., Keifenheim, K. E., Loda, T., Bugaj, T. J., Nikendei, C., et al. (2018). Differential Determination of Perceived Stress in Medical Students and High-School Graduates Due to Private and Training-Related Stressors. PLoS One 13, e0191831. doi:10.1371/journal.pone.0191831
Feletti, G. I., and Clarke, R. M. (1981). Review of Psychometric Features of the Medical School Learning Environment Survey. Med. Educ. 15, 92–96. doi:10.1111/j.1365-2923.1981.tb02403.x
Frambach, J. M., van der Vleuten, C. P., and Durning, S. J. (2013). AM Last Page. Quality Criteria in Qualitative and Quantitative Research. Acad. Med. 88, 552. doi:10.1097/ACM.0b013e31828abf7f
Genn, J. M. (2001). AMEE Medical Education Guide No. 23 (Part 1): Curriculum, Environment, Climate, Quality and Change in Medical Education-A Unifying Perspective. Med. Teach. 23, 337–344. doi:10.1080/01421590120063330
Gruppen, L. D., Irby, D. M., Durning, S. J., and Maggio, L. A. (2019). Conceptualizing Learning Environments in the Health Professions. Acad. Med. 94, 969–974. doi:10.1097/acm.0000000000002702
Guimond, S., Chatard, A., Martinot, D., Crisp, R. J., and Redersdorff, S. (2006). Social Comparison, Self-Stereotyping, and Gender Differences in Self-Construals. J. Pers Soc. Psychol. 90, 221–242. doi:10.1037/0022-3514.90.2.221
Hawryluck, L., Gold, W. L., Robinson, S., Pogorski, S., Galea, S., and Styra, R. (2004). SARS Control and Psychological Effects of Quarantine, Toronto, Canada. Emerg. Infect. Dis. 10, 1206–1212. doi:10.3201/eid1007.030703
Hense, H., Harst, L., Küster, D., Walther, F., and Schmitt, J. (2021). Implementing Longitudinal Integrated Curricula: Systematic Review of Barriers and Facilitators. Med. Educ. 55, 558–573. doi:10.1111/medu.14401
Holzinger, A., Lettner, S., Steiner-Hofbauer, V., and Capan Melser, M. (2020). How to Assess? Perceptions and Preferences of Undergraduate Medical Students Concerning Traditional Assessment Methods. BMC Med. Educ. 20, 312. doi:10.1186/s12909-020-02239-6
Hsieh, H. F., and Shannon, S. E. (2005). Three Approaches to Qualitative Content Analysis. Qual. Health Res. 15, 1277–1288. doi:10.1177/1049732305276687
Jeong, H., Yim, H. W., Song, Y. J., Ki, M., Min, J. A., Cho, J., et al. (2016). Mental Health Status of People Isolated Due to Middle East Respiratory Syndrome. Epidemiol. Health 38, e2016048. doi:10.4178/epih.e2016048
Khalil, R., Mansour, A. E., Fadda, W. A., Almisnid, K., Aldamegh, M., Al-Nafeesah, A., et al. (2020). The Sudden Transition to Synchronized Online Learning during the COVID-19 Pandemic in Saudi Arabia: A Qualitative Study Exploring Medical Students' Perspectives. BMC Med. Educ. 20, 285. doi:10.1186/s12909-020-02208-z
Kirschner, P., Van Vilsteren, P., Hummel, H., and Wigman, M. (1997). The Design of a Study Environment for Acquiring Academic and Professional Competence. Stud. Higher Educ. 22, 151–171. doi:10.1080/03075079712331381014
Kusurkar, R. A., Ten Cate, T. J., Vos, C. M., Westers, P., and Croiset, G. (2013). How Motivation Affects Academic Performance: A Structural Equation Modelling Analysis. Adv. Health Sci. Educ. Theor. Pract 18, 57–69. doi:10.1007/s10459-012-9354-3
Lee, J., Kim, R. J. Y., and Choi, H. (2020). Most Surface Learning in the Third Year: Dental Student Learning Approaches and Implications for Curriculum and Assessment. J. Dent Educ. 84, 464–472. doi:10.1002/jdd.12043
Marshall, R. E. (1978). Measuring the Medical School Learning Environment. J. Med. Educ. 53, 98–104. doi:10.1097/00001888-197802000-00003
McCutcheon, K., Lohan, M., Traynor, M., and Martin, D. (2015). A Systematic Review Evaluating the Impact of Online or Blended Learning vs. Face-To-Face Learning of Clinical Skills in Undergraduate Nurse Education. J. Adv. Nurs. 71, 255–270. doi:10.1111/jan.12509
Monrouxe, L. V., and Rees, C. E. (2020). When I Say … Quantification in Qualitative Research Quantification in Qualitative Research. Med. Educ. 54, 186–187. doi:10.1111/medu.14010
Neale, J., Miller, P., and West, R. (2014). Reporting Quantitative Information in Qualitative Research: Guidance for Authors and Reviewers. Addiction 109, 175–176. doi:10.1111/add.12408
Patton, M. Q. (2014). Qualitative Research & Evaluation Methods: Integrating Theory and Practice. Thousand Oaks, CA: SAGE Publications.
Reynolds, D. L., Garay, J. R., Deamond, S. L., Moran, M. K., Gold, W., and Styra, R. (2008). Understanding, Compliance and Psychological Impact of the SARS Quarantine Experience. Epidemiol. Infect. 136, 997–1007. doi:10.1017/s0950268807009156
Rheingans, A., Soulos, A., Mohr, S., Meyer, J., and Guse, A. H. (2019). The Hamburg Integrated Medical Degree Program iMED. GMS J. Med. Educ. 36, Doc52. doi:10.3205/zma001260
Rose, S. (2020). Medical Student Education in the Time of COVID-19. JAMA 323, 2131. doi:10.1001/jama.2020.5227
Rusticus, S., Worthington, A., Wilson, D., and Joughin, K. (2014). The Medical School Learning Environment Survey: An Examination of its Factor Structure and Relationship to Student Performance and Satisfaction. Learn. Environ Res 17, 423–435. doi:10.1007/s10984-014-9167-9
Salfi, F., Lauriola, M., Amicucci, G., Corigliano, D., Viselli, L., Tempesta, D., et al. (2020). Gender-Related Time Course of Sleep Disturbances and Psychological Symptoms during the COVID-19 Lockdown: A Longitudinal Study on the Italian Population. Neurobiol. Stress 13, 100259. doi:10.1016/j.ynstr.2020.100259
Schwenk, T. L., Davis, L., and Wimsatt, L. A. (2010). Depression, Stigma, and Suicidal Ideation in Medical Students. JAMA 304 (11), 1181–1190. doi:10.1001/jama.2010.1300
Silva, P. G. D. B., Oliveira, C. A. L., Borges, M. M. F., Moreira, D. M., Alencar, P. N. B., Avelar, R. L., et al. (2021). Distance Learning during Social Seclusion by COVID‐19: Improving the Quality of Life of Undergraduate Dentistry Students. Eur. J. Dent Educ. 25, 124–134. doi:10.1111/eje.12583
Vanderbilt, A. A., Feldman, M., and Wood, I. K. (2013). Assessment in Undergraduate Medical Education: A Review of Course Exams. Med. Educ. Online 18, 1–5. doi:10.3402/meo.v18i0.20438
Vindegaard, N., and Benros, M. E. (2020). COVID-19 Pandemic and Mental Health Consequences: Systematic Review of the Current Evidence. Brain Behav. Immun. 89, 531–542. doi:10.1016/j.bbi.2020.05.048
Wasson, L. T., Cusmano, A., Meli, L., Louh, I., Falzon, L., Hampsey, M., et al. (2016). Association between Learning Environment Interventions and Medical Student Well-Being: A Systematic Review. JAMA 316, 2237–2252. doi:10.1001/jama.2016.17573
Weiss, K. B., Bagian, J. P., and Nasca, T. J. (2013). The Clinical Learning Environment: the Foundation of Graduate Medical Education. JAMA 309, 1687–1688. doi:10.1001/jama.2013.1931
Wickramasinghe, D. P., and Samarasekera, D. N. (2011). Factors Influencing the Approaches to Studying of Preclinical and Clinical Students and Postgraduate Trainees. BMC Med. Educ. 11, 22. doi:10.1186/1472-6920-11-22
Keywords: medical education, learning environment, digital teaching, COVID-19, mixed-methods study
Citation: Mohr S, Küfe B, Rheingans A and Guse J (2021) Attitude Towards and Adoption of the Novel Learning Environment Among Undergraduate Medical Students During COVID-19. Front. Educ. 6:714526. doi: 10.3389/feduc.2021.714526
Received: 25 May 2021; Accepted: 06 October 2021;
Published: 26 October 2021.
Edited by:
Karin Gehrer, Leibniz Institute for Educational Trajectories (LG), GermanyReviewed by:
Jing Yu, Tianjin Normal University, ChinaRining (Tony) Wei, Xi’an Jiaotong-Liverpool University, China
Alexandre Berney, Centre Hospitalier Universitaire Vaudois (CHUV), Switzerland
Copyright © 2021 Mohr, Küfe, Rheingans and Guse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sonja Mohr, cy5tb2hyQHVrZS5kZQ==