 Jessica Hayton
Jessica Hayton Karl Wall
Karl Wall Dagmara Dimitriou
Dagmara Dimitriou
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ. , 12 December 2019
Sec. Special Educational Needs
Volume 4 - 2019 | https://doi.org/10.3389/feduc.2019.00149
Dressing is a fundamental independent living skill often haphazardly acquired via visual observation. For children with vision impairment and children with Down Syndrome (where vision impairment is a component), dressing skill acquisition can be delayed due to a reduced/absent visual modality. Independent living skills is an aspect of habilitation practice and training, designed to maximise independence in children and young people with vision impairment and prepare them for adulthood. This paper, presented in two parts, first details a systematic (UK based) survey exploring fastening use across a clothing sample of birth-adult clothing (N = 12,967). Study 1 presents a frequency distribution exploring types of fastenings used on clothing items from birth-adulthood. The data are fundamental in exploring the likelihood of fastening exposure across developmental phases. Further, Study 1 details the process behind developing a novel dressing skill intervention. Informed by Study 1, Study 2 qualitatively explored the effectiveness of an original resource/group-based intervention over a 10-week period. Eighteen children were recruited for the study, namely children with vision impairment (n = 9) and children with Down Syndrome (n = 9) aged 5–11 years. Collective and illustrative case studies are presented based on emergent themes from intervention observations. The findings reveal areas for consideration by Habilitation Specialists and the multidisciplinary team surrounding children with vision impairment and/or Down Syndrome as this may inform Habilitation Plans, and Educational Health Care Plan reports. The implications of this study extend beyond dressing skill development in children with vision impairment and/or Down Syndrome and inform resource development and subsequent practice when working with children with special educational needs and disabilities.
Habilitation is the process of maximising independence in children with vision impairment, particularly supporting the achievement of motor, sensory, psychological, and cognitive milestones (Hayton and Dimitriou, 2019). Habilitation is a triangulated, practical approach consisting of mobility, orientation and independent living skills and, in England, is a provision for all children and young people with special educational needs and disabilities from birth-25 years (Department for Education and Department of Health, 2015). Independent living skills are associated with daily living and are expressed through adaptive behaviours (Oakland and Harrison, 2008). This means that a child with vision impairment will demonstrate functioning and independence in their display of adaptive behaviour. Independent dressing skill acquisition is essential for participation in everyday life (Bardin, 2014), and the ability to perform this task in a variety of appropriate settings that are familiar and unfamiliar (i.e., home, education, and public) is adaptive behaviour.
For children with vision impairment, the acquisition of independence skills can be affected due to restricted/absent learning via observation (incidental learning) and developmental delay in motor domains. Children with a disability are at higher risk of developing vision impairment 1(10.5 vs. 0.16%; Salt and Sargent, 2014). Children with Down Syndrome are at elevated risk of vision impairment including cataract, refractive errors, and strabismus (independent of refractive error) (Cregg et al., 2003; Creavin and Brown, 2009; Salt and Sargent, 2014). This means that access to incidental learning in this population may also be compromised. Children with vision impairment and children with Down syndrome can experience developmental delay in cognition and motor skill acquisition which can relate directly to a delay in acquiring independent living skills. Further, intellectual disability is characteristic of Down syndrome, manifesting in areas such as attention, working memory, planning, and inhibition (Costanzo et al., 2013). Intellectual disability could therefore affect successful independent dressing in children with Down syndrome, however low IQ is not considered a predictor of delayed motor skill acquisition and adaptive behaviours at a young age (~4 years). Rather the impact of intellectual disability on independent self-care skills becomes apparent as chronological age increases (e.g., 21 years) (Carr, 2000, 2005).
Successful independent dressing for all children requires the acquisition of transferable pre-requisite motor skills suitable for all independent living skill areas (Klein, 1983; Swallow and Huebner, 1987; Fairnham et al., 2002). These include gross motor skills including cephalo-caudal development (from the head to toes, demonstrated by sitting and reaching), proximal-distal development (control from the joints closest to the midline of the body to fingers and toes), and medial-lateral development (culminating in fine motor control particularly of the hands and fingers) (Klein, 1983; Hayton, 2012). The pre-requisite skills outlined in this literature are based, in turn, on an assumed linearity of child development in the transition from gross to fine motor skill development (see: Klein, 1983; Fairnham et al., 2002; Martin and Fabes, 2009; Sugden and Wade, 2013). The acquisition and refinement of such transferable skills are necessary for successful, independent dressing and can be demonstrated in a variety of ways (e.g., pincer grasp for zipping can be demonstrated by pulling the lid from a yoghurt pot). For children with Down syndrome, physical motor delay including dexterity, and bi-manual co-ordination may be more apparent when compared to children with vision impairment, due to hypertonia associated with the condition (Pereira et al., 2013).
Independent dressing also includes demonstration of pre-requisite motor and spatial skills such as “body awareness”—whereby the child understands their body as a whole and sum of parts (e.g., the hand as part of the arm); and directional awareness. Directional awareness is also an essential preparatory aspect of the development of independent dressing skills, as the intrinsic concepts of “left/right,” “up/down” for example are necessary to complete dressing activities. For children with vision impairment and children with Down syndrome, these concepts are taught systematically (through Habilitation and/or key partners in the multidisciplinary team surrounding the child), combining auditory instruction and tactile experience (e.g., Cuturi et al., 2016) in lieu of observational/incidental learning. The acquisition of pre-requisite skills varies from child to child (including typically developing children), as noted by van Herwegen et al. (2011) and is particularly pronounced in clinical populations such as those with Down syndrome and/or vision impairment. Although these groups are at low incidence in relation to prevalence rate, there is a high heterogeneity of variance that is present even when individuals share the same diagnosis (McLinden et al., 2016). Taking individual variation into account for developing independence skills, parents/caregivers are encouraged to dress/undress their child until they are confident that the child has the competency to successfully and independently dress/undress (Fairnham et al., 2002).
Achieving independent dressing skills is not prescribed at a particular chronological age for any child, regardless of need. In the typically developing context, the age and stage expected to achieve independent dressing skills remains unclear. Ideally, independent dressing is a skill to be mastered by all children before entering primary school (~5 years of age; Public Health, 2015) however this is largely anecdotal as published literature is lacking. The common consensus appears to be that independence skills should be encouraged when the child (regardless of need) demonstrates: readiness to learn, an understanding of the task in hand, and a motivation toward achieving the skill (Miller et al., 2011). In the field of vision impairment, independent dressing skills are taught once pre-requisite skills (including readiness and motivation, established via verbal/non-verbal communication) are observed (see Fairnham et al., 2002). This shift from dependence to independence could be characterised by an increase in chronological age, maturation or skill. For children with Down syndrome and children with vision impairment this readiness for independent dressing may occur at a later age in comparison to sighted peers (Bardin, 2014). This is arguably due to developmental delay, which is a common characteristic of children with sensory impairments (Thomas and Knowland, 2014). In relation to atypicality and for the purpose of this paper, developmental delay is defined as a difficulty in reaching developmental milestones considered characteristic of chronological age based on standardized measures (Riou et al., 2008; Thomas and Knowland, 2014).
It is postulated that children with vision impairment follow the same motor development trajectory as their sighted peers, yet are delayed in achieving milestones by ~3 months (Sugden and Wade, 2013). Although developmental delay may not always be apparent in individuals with vision impairment, it is argued that there may be a relationship between vision impairment and developmental delay. This is because of the restriction/inability to learn incidentally, meaning that independence skills are not haphazardly observed and learned in the same way as sighted peers (Lewis and Iselin, 2002; Favela et al., 2018). Resultantly, development of independence skills in children with vision impairment requires systematic and formal habilitation training. Research has revealed that at around 5 years of age, children with Down syndrome demonstrate delays in independent self-care activities, particularly those that require fine motor skills (Mancini et al., 2003; Dolva et al., 2004). Further for children with Down Syndrome, it is also acknowledged that low muscle tone, intellectual disability, and cognitive impairments may delay independence skills (All Party Parliamentary Group on Down Syndrome, 2012). The over-expression of genes in chromosome 21 affects global development of the child (cognitive, physical, social) meaning that children with Down syndrome can take twice as long as a typically developing child in achieving motor milestones Luz Carvalho and Vasconcelos, 2011; Malak et al., 2013. In context, this means that a sighted child could visually attend to a zip, observing how it was fastened/unfastened, and copy behaviour. Contrastingly, a child with reduced/absent vision has restricted access to this stimulus. Therefore, a child with a vision impairment and/or additional needs (i.e., Down syndrome) requires systematic (Habilitation) training and instruction to attend to and manipulate objects within their environment, potentially compensating for the lack of incidental learning (Hayton et al., 2018).
From birth through to adolescence, the style, type, and range of clothing items increase during children's development. This is apparent in the UK, where this study took place. Typically, babies/young infants are dressed in all-in-one body suits (typically with popper/press-stud fastenings). The sizes of the fastenings available on items of clothing are commensurate to the size of the infant; however, in the case of body suits, the popper fastenings are too small for the developing infant to manipulate. Infants do not have the necessary motor skills to carry out this task, and so this assumes that dressing and manipulating fastenings are dependent on a competent adult. The sizes of fastenings change as the child's size increases yet dressing remains dependent on adult support, unless an adult actively involves the child in the dressing sequence (Swallow and Huebner, 1987; Kellegrew, 2000). Throughout these developmental stages, parents/caregivers have a responsibility to provide appropriate clothing for their child (e.g., Summers et al., 2008). An assumption was made in this study that in Westernised cultures, the availability and types of children's clothing are targeted toward parents rather than children. This means that the choice of clothing is determined by commercial availability, but parents/caregivers ultimately prescribe item purchase. As parents play a crucial role in initiating and supporting the development and acquisition of independence skills, parental influence resulting from culture, expectations, and willingness can affect skill development (Taverna et al., 2011; Greenaway et al., 2017; Ayllón et al., 2019).
Parental influence combined with exposure to and availability of fastenings on children's clothing may affect gross and fine motor skill development associated with successful independent dressing. For example, high exposure to zip fastenings may lead to a better zip fastening ability. This concept underpinned the current investigation. Independent dressing also involves the demonstration of transferable gross and fine motor skills. These include the refinement of the pincer grasp (pinching the index finger and the thumb), and sufficient finger strength (Klein, 1983; Fairnham et al., 2002). The exposure to different types and sizes of clothing fastenings may affect children's development and refinement of these pre-requisite skills; however, a degree of causality is implied. This is where a child can only master task B (e.g., fastening a zip) after successfully mastering task A (pre-requisite skills) (Warren, 1982).
The purpose of this two-part novel study was to contextualise the types of clothing available from infancy to early adolescence (aged 0–14 years) and adulthood, using the information to design and test intervention materials supporting the independent dressing skills in children with vision impairment and children with Down Syndrome. This study is complementary to the first empirical study investigating dressing skill acquisition in children with vision impairment and children with Down syndrome from a Habilitation perspective (Hayton et al., 2018). Previous work (see Fairnham et al., 2002) is largely experience-based, grounded in rehabilitation techniques (developed for adult populations) and not formally tested. Study 1 detailed a fastenings survey conducted to provide a basis for understanding possible exposure to and availability of particular clothing fastenings. The primary aim of the survey was to identify the most popular items of children's clothing and the fastenings available. Investigating the availability and use of clothing fastenings was considered important in contextualising the gross and fine motor control needed to operationalize independent dressing skills. The findings of Study 1 informed Study 2 in terms of supporting the design of novel intervention materials supporting independent dressing skills in children with vision impairment and children with Down syndrome. Study 1 offers quantitative findings, whereas Study 2 is an observation-based qualitative case study account of the effectiveness of the intervention.
Study 1 served two functions. First, the survey revealed the frequencies of fastenings present across the range of clothing (from infancy to adulthood). This demonstrated the variety and potential complexity of clothing as chronological age increases. As Habilitation practice supports the development of independence from childhood to adulthood, it was considered appropriate to understand the characteristics of clothing as children and young people transition toward adulthood. Second, the most common fastenings, as revealed by the survey, were selected for the development of novel intervention resources suitable for the development of gross and fine motor skills (suitable for dressing) in children with vision impairment and children with Down syndrome.
Study 1 used a cross-sectional survey design examining clothing items and fastenings from birth to adulthood. This afforded a snapshot relative to fastening use at a time point which then informed the design of intervention materials. Frequency distribution represented the survey data. The recording and presentation of quantitative values are based on how many times each fastening appeared. The method was approved by the research team and the survey was run by the main researcher. First, a sample of the full spectrum of items of children's clothing were examined (N = 1,569 items) across the age range “birth-14 years.” The sample was drawn from the 5 most popular children's clothing stores (with online and offline purchasing options) in the United Kingdom (UK), based on an internet search. The search was compared to an online forum for parents (Mumsnet). This ensured that the stores chosen were representative of consumer habits and preferences in this sample. The online forum is a global platform; however, the results were refined to specific clothing stores within the UK. This ensured that the results would be representative of the clothing likely to be worn by children within the UK (despite the global availability of clothing online) and inform the development of intervention materials.
Second, a sample of male and female adult clothing was also examined (N = 11,398). This contextualised the likelihood of clothing fastening occurrence in adult populations. This supported the aim of Habilitation work, notably preparing a child for the transition to adulthood. The exploration of available clothing and fastenings in adult ranges indicated the potential fastenings that children and young people might utilise once reaching adulthood. This bears importance as dressing skill development and acquisition is based on the opportunity to experience and manipulate items of clothing. The adult sample of clothing was drawn from one department store (with online and offline purchasing options) and one “online-only” store (consistently ranked number 1 for adult clothes in the UK from Media Outlets such as Newspapers, Fashion Magazines/Media Blogs). Due to the difficulty of clearly establishing a “top 5” for adult clothes (largely resultant from gendered items, i.e., stores for males only and the number of stores available), the surveyed stores represented the broadest availability of adult clothing encompassing the full range of budget to “high-end” fashion.
The examined items of clothing (birth-adult) were all available online. Every identified form of available children's clothing were refined to “most popular” (i.e., most commonly purchased, determined by the ‘sort/filter' option on all websites) as this reflected consumer habits (i.e., purchase) and preferences. Unlike the child sample, online clothing for adults was pre-filtered to “male/men” and “female/women.” The clothing items were also pre-categorised according to type. Notably, the types and range of clothing available in the adult sample was far greater than types available for children and young people. For example, in children's clothing, the category “trousers” encompassed jeans, chinos, dress trousers and joggers (sports-wear). In adult clothing, “trousers” pertained to dress trousers/office wear. The remaining types e.g. jeans, chinos and joggers in adult ranges (male and female) were separated under different headers. Similarly, in girl's clothing “dresses” was a catchall term for a variety i.e., day dresses and party dresses, whereas in the adult sample, the dress category was split into length (mini-, midi- and maxi-dresses) and occasion (e.g., party, evening, casual, bridesmaid). This demonstrated how clothing types expand and undergo dynamic changes in the transition across development. It is important to understand these changes when developing Habilitation interventions due to the purpose of maximising independence from child- to adulthood.
After filtering items to most popular, 30% of each identified and available type of clothing (e.g., trousers, skirts, blouses [female) and shirts (male)] on each online store was recorded. 30% of each clothing type was chosen as it was considered to sufficiently reflect the clothing within each group. Duplicates of the same item were excluded using visual inspection. This was because the style of the item and fastenings (if present) remained the same. Product duplication cases were not recorded. Seasonality was a potential confound, as changes occur according to seasonal suitability. The survey examined Autumn/Winter/Spring collections for children and adults. The survey could not account for fashion trend, as this fluctuates and is beyond the control, influence and scope of this project.
All clothing items were split into types (using each website filter option for children's clothes as they were distinguished by age; adult clothes were pre-filtered to type) and the total number of each type available on the website was recorded using website records. From this total number, 30% was calculated of each clothing type, as it was understood that observation that a sample of this size would be reasonably generalizable across the availability of children's and adult clothing. This was due to the replication of many items.
The survey assessed only functional fastenings, i.e., those that require manipulation in the dressing sequence to put on/secure/take off an item of clothing. Fastenings used for aesthetic purposes only (i.e. decorative buttons that could not be fastened/unfastened), were not recorded. The fastenings (and descriptions) identified in the surveyed sample are presented in Table 1.
Table 1. Descriptions of identified fastenings on children's clothes.
Table 1 included the recording of “Slip-on” clothing (i.e., t-shirts and trousers) occurred despite not technically being considered as a fastening. This is because the joining of material is not needed to secure an item. Slip-on items were part of the most popular surveyed items. Omission of the slip-on category would not reflect the availability of children/adult's clothing or the shopping habits of consumers. The inclusion of slip-on items more accurately reflected the most popular items of clothing bought, and subsequently the clothing types that the children/adults were potentially exposed to. Slip-on clothing reduces exposure to fastenings, and potentially may hinder the development of gross/fine motor fastening skills. This is because children do not need to complete additional stages to independently dress and secure their clothing. This means that the gross motor skill of pulling on or pushing off clothing may be better developed than the fine motor skill of fastening with requires more dexterity and control.
The recorded frequencies of fastenings (Figure 1) on the most popular items of children's clothing indicated, it was assumed, the types of fastenings that infants and children are exposed to from birth-14 years of age, across the UK. The splitting of the age groups at 2 years is arguably associated with the developmental variation and progression of fastening exposure. The split of the age in the online shopping stores sorting filters showed an overlap between the two groups however was uncontrollable due to website filtering. The recorded frequencies of fastenings on adult clothing were considered representative of the types of fastenings that children and young people were likely to engage with once transitioning into adulthood. These frequencies are considered important when mapping an intervention protocol to support children and young people with independent dressing skills.
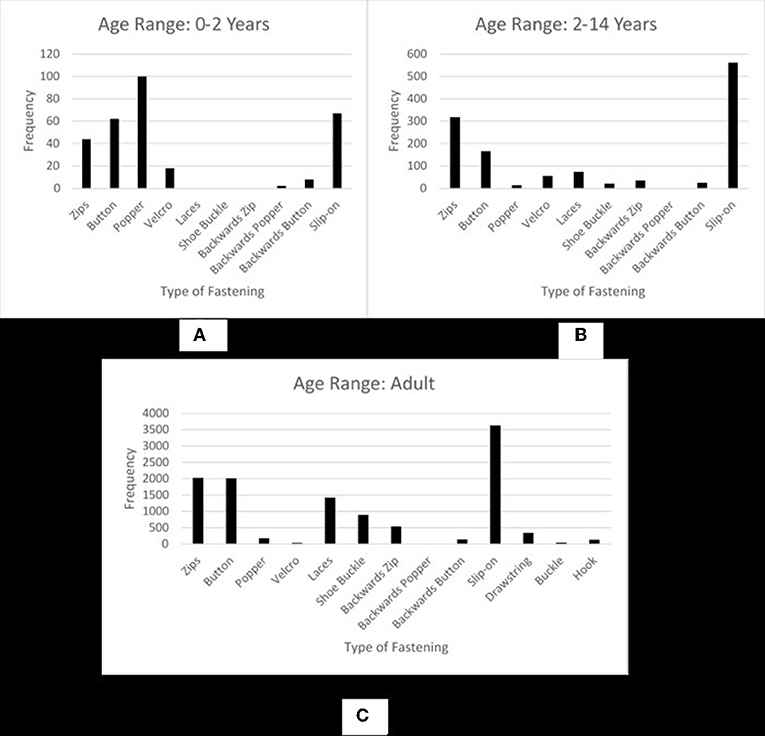
Figure 1. Recorded frequencies of fastenings on children's clothing 0–2 years (A), 2–14 years (B), and adult clothing (C).
Figure 1 shows how fastenings and frequencies differ according to chronological age/size. Figure 1A reveals that the most common fastening for children aged 0–2 years is poppers. For children aged 2–14 years (Figure 1B), and adults (Figure 1C), the most frequent fastening is zips (frequency of 318 and 2017, respectively). The observable differences in Figure 1, show how fastenings change across development. Table 2 displays the frequency of fastenings across both child groups and the adult sample.
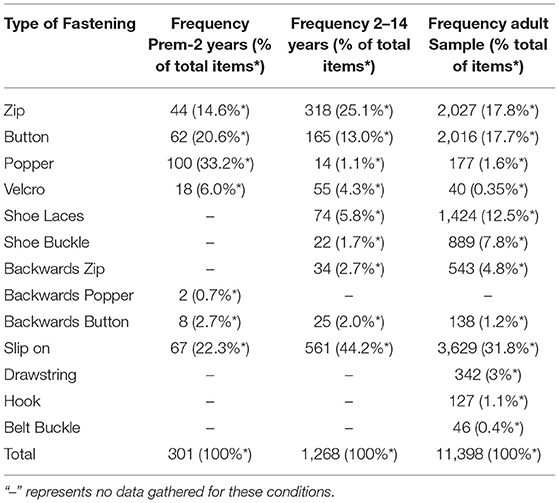
Table 2. Frequency of clothing fastenings for children aged between 0-2 years, 2–14 years and adults.
Table 2 identified the different types, variety and availability of clothing fastenings available, relative to age. The greater variety in fastening type/availability was in the adult sample. Arguably, this represented a broader choice in adult clothing. The frequency results revealed that as a child transitions into adulthood, zips, buttons and laces would become more frequent forms of fastening within the adult category (although slip-on was still available).
Study 1 demonstrated that chronological age (and, arguably, physical size) linked to more variety in clothing fastenings. Clothing type increases across development; i.e., from all-in-one body suits to trousers, chinos, jeans and active wear. The fastenings used to secure items in place become more dynamic and, arguably, more complex in adult clothing. The survey revealed a dramatic increase in style (e.g., adult options being “mini,” “midi,” and “maxi” dresses compared to “dresses” for children) and type (e.g., jeans and chinos for adults compared to “trousers” for children). Arguably, this supports the notion that dressing is a developmentally-centred independent living skill, and the progression and complexity of independent dressing skills extends into adulthood. This is in-line with the basic principle of Habilitation, whereby children and young people with VI are trained formally and systematically in adaptive behaviours, supporting transition into adulthood.
The survey supported the assumption that independent dressing skills extends across the lifespan. The reported frequencies indicated a need to develop fastening abilities that are transferable across the different fastening domains. This is because the type and range of fastenings increased according to chronological age. This is prior to consideration of physique in comparison with chronological age. Therefore, it is important to note that the chronological age associated with children's clothing does not always reflect the size of the child. For example, a child aged 8 years old may wear clothes “sized” 10 Years. This means that although chronological age is a label generally associated with the average size of children that age, it does not mean that the size of the clothes will always necessarily match the chronological age of the child. Clothing choice is arguably more reflective of physiological size (which extends into sizing for adult ranges), in terms of what will fit, as opposed to chronological age. It could be argued that slip-on items of clothing and shoes can override the need to develop fastening skills in childhood, however the purpose of habilitation is to equip children and young people with the skills that they presently need, but also train and develop skills that are required through adolescence and into adulthood. Furthermore, the need to independently develop dressing skills is crucial for Habilitation but also is essential knowledge for transference of skill ability if these adults become parents themselves.
There are limitations to this survey. First, clothing changes seasonally and annually, therefore the survey only offers a snapshot in time regarding the availability of fastenings on clothing items. Second, surveyed items were available only in the UK, and so are not necessarily generalizable beyond this context. Third, examined items were based on popular clothing stores and the child samples compared with an online parental forum. This means that the sample was limited, as it did not account for differences in cultural dress nor socio-economic status. Families with higher or lower incomes may choose different stores that may supply different items. Similarly, annual income would influence adult choice. This could then shift the likelihood of exposure to different fastening types. Future research could account for this by using questionnaires and interviews with families to fully assess environmental influences that could contribute to clothing choice.
The survey has also informed the assumption that gross and fine motor skill development are essential for manipulation and the successful fastening of clothing items. Despite identification of independent dressing skills in Habilitation practice and it being legislated in England, little systematic, and empirical evidence supports how dressing can be developed and achieved in children with vision impairment. Extending beyond the survey findings, a further search explored whether there are any commercial resources to support dressing skills in children with vision impairment, to no substantial avail. Resultantly, the survey data informed the development of a novel intervention resource suitable for training independent dressing skills in children with vision impairment (Study 2).
The survey data informed development of novel intervention resources, particularly fastenings chosen. A lack of commercial availability for resources suitable for children with vision impairment led to the design and creation of a novel resource to support independent dressing skills; the Interactive Puzzle Game. The interactive puzzle game was an oversized jigsaw puzzle containing zips, buttons, poppers, and shoelace fastenings as per the popular fastening types yielded from the survey. A benefit of training zips, buttons and poppers is that they can all be found on one item of clothing (an outdoor coat), thus removing the need for multiple items of clothing.
Particular emphasis was on the results of children's clothing, as the intervention was designed for children with vision impairment and children with Down syndrome aged 5–11 years. Further, it is argued that early intervention should occur with resources that a child would naturally engage with/be exposed to, but also equip the child with transferable skills for adulthood. The likelihood of exposure to particular fastenings could impact dressing skill development in children in their current context. The purpose of designing and testing resources was to aid contextualisation of this assumption, support dressing skill development, and transfer of skills through early intervention, preparing for transition to adulthood.
Using thematic analysis and collective case studies (detailed in section Qualitative Data Analysis) Study Two, qualitatively explored the effectiveness of the novel intervention materials in developing independent dressing skills in children with vision impairment and children with Down syndrome over a 10-week period. This approach was chosen to explore participant behaviours in response to the intervention and attempt to encapsulate the real-world nature of conducting an intervention in relation to answering the main research question. The main research question for Study 2 was “To what extent can novel resources support fastening skill development in children with vision impairment and children with Down syndrome?”
Prior to conducting Study 2, the novel intervention materials were created and piloted for reliability and face validity (Hayton, 2017). Amendments such as colour contrast and material choice were made to the interactive puzzle game to support suitability for children with vision impairment and children with Down syndrome. Dimensions such as size and shape of the materials were not altered, and these were found suitable for children of this age. The interactive puzzle game was tested using observation and a case study approach. Children acted as their own control, due to the large heterogeneity of variance present in children with disabilities. Development of resources led to the qualitative assessment of intervention effectiveness, presented here in Study 2.
Eighteen participants were recruited (n = 9 vision impaired; age range 5;04–10;02 years). The age range represented that of Primary School in the UK, responding to a delay in dressing skill acquisition as part of school readiness (Public Health, 2015). Participants with vision impairment were recruited from a specialist school in London, UK. Participants with Down syndrome were recruited from a voluntary organisation in London, UK. All participants were recruited due to their inability to fasten items of clothing. Children with vision impairment and children with Down syndrome were matched on chronological age +/– 2 months. Recruitment was school/organisation-based as the intervention ran in these settings.
Ethical approval was granted by UCL Institute of Education Ethics Committee. Informed consent for the whole study was obtained for each setting (school/organisation) and from each participant's parent/caregiver. Child assent (verbal and/or gestured e.g., thumbs up) was obtained prior to the intervention taking place, and before each session. This was done to ensure that the child was happy to take part on each day that the group-based intervention ran and to ensure that the voice of the child was heard throughout. Consent to publish case study data was obtained by parents/caregiver of the child participants.
All children with vision impairment spoke English as a first language. Some children with vision impairment were bilingual and two children used Makaton (a form of sign language) to support communication. Children with Down syndrome all had English as a first language, and some used Makaton to support communication as they had limited speech. For children with vision impairment, the types of diagnosis varied, although some shared a diagnosis. Table 3 indicates the diagnoses of the full sample (children with vision impairment and children with Down syndrome, based on Medical History information provided by parents/caregiver). Confirmation of visual status was via the Class Teacher as they had access to clinical information and parental permission to disclose. As some parents did not speak English as a first language, the class teacher communicated or confirmed diagnosis. Table 3 also states co-morbidities for the children with vision impairment. The parents of children with Down syndrome did not provide information about comorbidity.
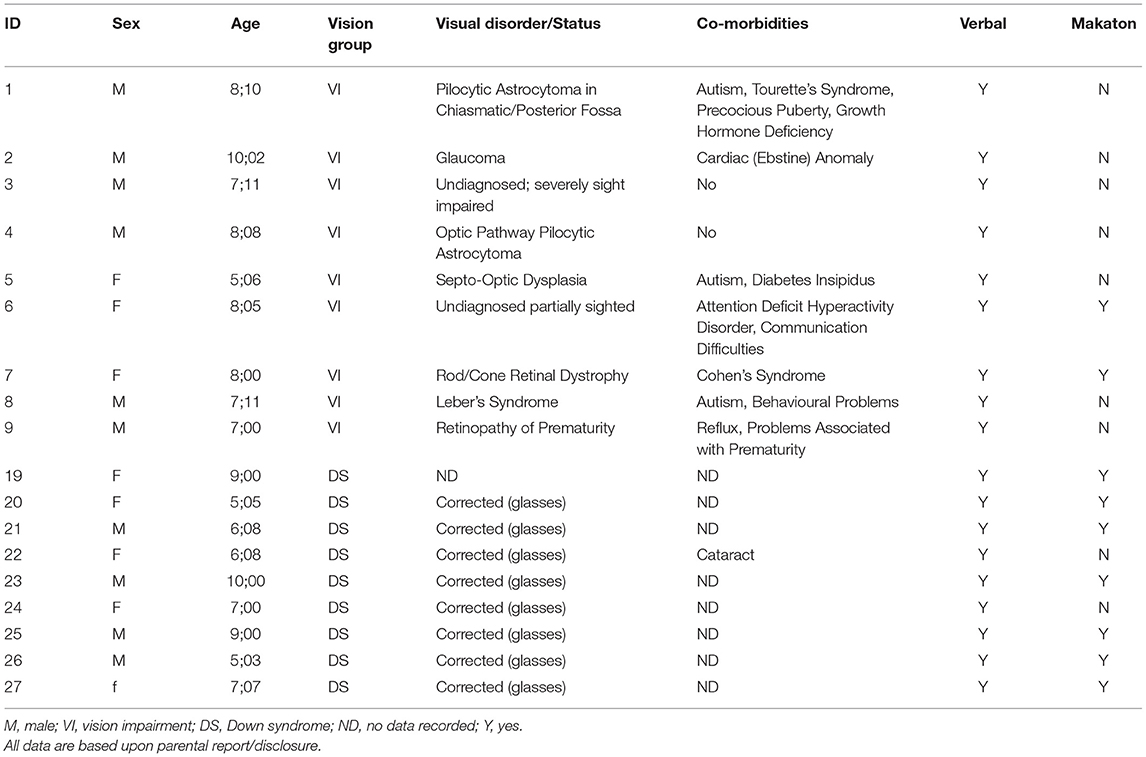
Table 3. Characteristics of children with vision impairment and children with Down syndrome.
The individual characteristics of both samples in Table 3 are incorporated into the research design to aid contextualization of skill development/developmental changes over the course of the novel audio-tactile intervention period, detailed next.
Two materials were used in this study; the interactive puzzle game (used to support the development of independent dressing skills) and the observation schedule (used to record skill progression for each child).
The size of the puzzle pieces was commensurate to the size of a child's hand to aid fastening manipulation (too large/small puzzle pieces might affect manipulation of the fastenings and/or the child's ability to hold each item). Affixed to each piece was either a zip, button, popper or shoelace fastening. The three most frequent fastenings identified by the survey in the 2–14 years age range were zips, buttons, poppers, and therefore they were chosen for the interactive puzzle game. Further, due to the increase in lace fastening availability in the adult sample, laces were also chosen for the interactive puzzle game to support the child's transition into adulthood.
The affixed button and popper fastenings were offered in three sizes (small, medium, large). This was purposive to support the development of fine motor skills suitable for independent dressing. Velcro was used on the reverse of the fastening/on each puzzle piece to make the puzzle pieces interchangeable, and to increase handling opportunities for the children. Colour contrast was also considered an important aspect in the design process, as some children with vision impairment have a sensitivity to or difficulty with processing colours with very high or low contrast.
The development of the interactive puzzle game (Hayton, 2012, 2017) was based on the practical aspect of fastening and unfastening. The use of the puzzle and systematic verbal instructions (relative to task completion; i.e., “pinch the tail of the zip”) afforded the opportunity to transfer fastening skills from the abstract (e.g., the puzzle pieces in front of the child) to the actual (fastening/unfastening personal clothing items). The ability to first practice abstractly was considered important for the development of independent dressing skills. This was because the puzzle game afforded the opportunity to practise fastening/unfastening without being constricted in clothing or reducing movement.
In addition to removing the potential distress caused by constriction in their own clothing, the opportunity to practice using the fastenings separate from their own clothing was considered more appropriate for three reasons: the first being that incrementally and systematically developing independent dressing skills meant that anxiety and stress were reduced. This was because transference onto the child's personal items (an outdoor coat) occurred at the stage that they demonstrated readiness and confidence. Second, taking time to develop, refine and subsequently “master” the skill before transference reduced pressure regarding task completion. This is because directly requesting a child to “fasten their coat” for example could appear a colossal task. However, framing the same task in an informal, playful and step-wise activity could increase motivation, alleviating potential embarrassment and stress. Third, some children may not have access to, or wear, lace-up shoes and so developing this skill in the abstract meant that if required, the ability to transfer the acquired skill subsequently prepared the child for adolescence/adulthood. The skills of fastening and unfastening were gradually refined over the course of the intervention, culminating (where possible) to transference on personal clothing items.
An observation schedule was devised to support the recording of skill development. The schedule was based on a task analysis principle used in Habilitation practice. The previously piloted observation schedule (participants, N = 65 university students; interrater validity was found to be Kappa = 0.97, p < 0.001) split the tasks of unfastening and fastening into small yet observable stages (see Hayton, 2017; Hayton et al., 2018). Each type of fastening process required its own continuous sequence, and so a continuum-based approach to recording skill acquisition was devised for zips, buttons, poppers, and laces. The observation schedule stages are continuum-based, meaning that stage 4 can only be independently acquired after stage 3, for example.
Each step in each fastening sequence was categorised as “gross” and/or “fine” as this pertained to the motor skill requirement for each nuanced stage. For example, “pinching the base of the zip (fine)” vs. “pulls zip slider up 100% [gross and fine, due to the combination of pinching (fine) and pulling (gross)].” Participants were also scored on the indications of their vocalisations (sounds/speech). This was based on the premise that, if a child could not physically complete a stage of fastening yet is aware of the next stage, they would pre-empt the stage by using speech. The noting of these behaviours is important for Habilitation practice, as pre-empting the next step in the sequence is indicative of the development of the skill itself. For children who struggle with motor skills, the verbal indication and subsequent praise/reinforcement can support motor skill development.
Records were made for assistance or scaffolded support. Assistance was characterised as either physical support (hand-over-hand) or verbal support (giving instructions). Assistance was only provided at the child's request, and the child also specified the type of support that they wanted i.e. “Can you help me with your hands?” was a request for physical, and “Can you tell me what comes next?” was a report for verbal. These were two particularly articulated expressions for help, and requests varied according to the needs of each child.
Upon receipt of informed consent from all parties (schools/organisation, parents/caregivers, and children), parents/caregivers were invited to complete a medical history questionnaire for their child within 2 weeks. During these 2 weeks, preparation for the commencement of the group-based intervention began. This involved briefing support staff (involved in working with the child participants) regarding the nature, purpose, and process of the intervention. Timetables, rooms, and calendars were arranged during this time to ensure consistency and collaboration between each setting and the researcher.
Next, familiarisation with the child participants in each setting occurred. The intention was to build a familiar and supportive working relationship. The mean time for familiarisation for children with vision impairment was 10 min per participant. The mean time for familiarisation for children with Down syndrome was 2 h, but this was with the whole group, as requested by the Group Leader who was aware of the social/emotional needs of the children.
Participant screening then occurred by asking each child to fasten a zip, a button and a popper. None of the eighteen participants were able to independently complete this task, so all were considered suitable for the intervention. The intervention schedule was prepared to accommodate pre-, during- and post-intervention observations. The intervention schedule demonstrated a gradual development in skill development, from the abstract (the interactive puzzle game in front of the child) to the actual (fastening their own coats), over 10-weeks. During pre-intervention observations, each child was presented with each piece and asked to name the fastening and show the researcher how it worked. This was marked against the observation schedule to establish a baseline for each child.
The group-based intervention was conducted twice per week for 20 min for 10 weeks. The sessions were purposefully short to hold attention and avoid frustration. Each session followed the same principles: welcome, introducing the session and what was going to happen, practicing, ending the session with each child saying their favourite part of the session. The repetitive structure was purposeful to maintain a structured and consistent environment optimising skill development. The pace of each session was determined by each child, but support was scripted prior to the intervention. Child-led, researcher-facilitated sessions meant that the children had most control over their choices (fostering play and incidental learning) and that they did not feel pressurised. Set resources in each session restricted choice (so as not to overwhelm) but each child mostly controlled their engagement. The researcher ensured that each child attempted each fastening once per session, with or without scaffolded support. The intervention sessions ran at times appropriate for dressing (i.e., before play-time). This was to keep the skill relevant to the time of day when dressing/undressing would naturally occur.
Progress of each child was recorded using the observation schedule at weekly intervals (last session per week) for 10 weeks. Table 4 shows the group structure and number of absences per participant.
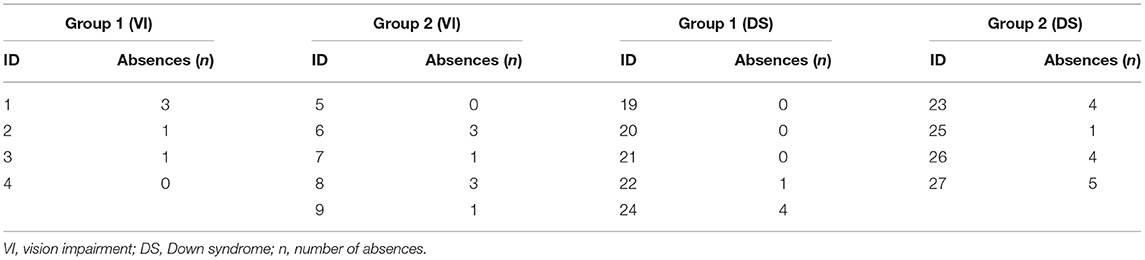
Table 4. Assigned groups and number of absences (out of 20 intervention sessions).
Participants knew that they were being observed, but also that there was no pressure to fastening all items. Transparency and honest communication with the children were considered crucial to support them/alleviate anxiety. Post-intervention follow-up sessions were made 1 and 3 months after the intervention ceased. Observations were made for each child attempting each fastening, without scaffolded support. This was because the longer-term effects of the intervention were observed. The skill ability of each child was recorded, as were reports of practice in the home environment. Unfortunately, the children with Down syndrome did not participate in the post-intervention follow-up due to time restrictions.
All intervention and post-intervention sessions were audio-recorded, and observation notes were made after every session. Verbatim transcriptions of the sessions and the observation notes were coded to support a theoretical thematic analysis, following the 6-phase guide proposed by Braun and Clarke (2006). Familiarisation with data was completed first. Open-coding of eighteen case studies (n = 9 vision impairment were then completed by hand (as pre-set codes were not considered appropriate). As codes emerged they were independently checked by a staff member and were discussed and modified. Discussion and modification of codes led to establishing sub-themes of broader categories and themes were identified based on the significance in the transcripts. Themes were then reviewed to ensure that data supported them and there were no instances of overlap; themes were coherent and distinct.
Two broad themes emerged: clinical diagnosis and intervention performance and behaviours that could affect intervention performance. Within the first theme, subthemes emerged which were over/under performance in response to the intervention, based on the characteristics of diagnosis and the possible effect of chronological age. Within the second theme, subthemes were varied. These included: multi-tasking behaviour (present or absent in the sample and maintaining on-task focus or not); attention seeking behaviour (including negative strategies such as physical aggression to peers (pushing), spitting on/licking the researcher and participants purposefully positioning themselves as close to the researcher as possible), familiarization with the researcher (including co-operative behaviour due to familiarisation and avoidant/wary behaviour due to seeing the researcher as a “professional”) and parental influence (overprotection when parents were present). These themes informed the development of collective case studies to generally explore the development of fastening/unfastening skills in children with vision impairment and children with Down syndrome. Within the collective case study approach, instrumental case studies are used to offer insight into the intricacies of developing fastening/unfastening skills in children with vision impairment and children with Down syndrome. The sampling choice of each case is considered meaningful in fully answering the research question. This means that some of the cases chosen demonstrate the real-world nature of delivering an intervention to support children with vision impairment and children with Down syndrome.
Case studies are used to explore the individual characteristics and behavioural responses to the intervention materials. Two broad themes emerged from the observations of participants with vision impairment and children with Down syndrome. The themes related to: (1) clinical diagnosis and intervention performance and (2) behaviours that could affect intervention performance. The instrumental case studies presented are grouped in accordance with the themes.
P3 was a notable case within the intervention due to the severity of his diagnosed condition and his performance during the intervention period.
P3 was a 7-year-old boy diagnosed with Juvenile Onset Battens Disease. Vision impairment is a characteristic of this condition, as well as developmental regression (including motor skills) and loss of speech. Additional comorbidities were not reported. P3 was quiet and reserved in the sessions. However, he would say “yes” or “no” and ask for assistance when he needed it. This demonstrated that he was still able to communicate efficiently with the researcher and his peers in the sessions.
P3 preferred to work alone and did not ask for much assistance throughout the intervention period. He mastered the zip condition by week 5, the button and popper condition by week 4 and the lace condition by week 5. This was considered remarkable, accounting for the severity of his diagnosis and anecdotal reports (from teachers) regarding regression. P3 would collect as many fastening pieces as he could, unfasten/fasten as fast as possible and place them to his side (creating a tower). He would repeat this behaviour throughout the sessions, displaying incredible focus toward attempting every piece available in every session. P3 was able to transfer the acquired skills onto his own outdoor coat. He was able to put on a shoe and fasten the laces, yet his own shoes did not have laces.
The performance of P3 over the intervention period did not seem to correspond with the severity of his diagnoses. Theoretically, P3 should have performed worse than was observed over the intervention period due to developmental regression associated with the condition (von Tetzchner et al., 2013). Furthermore, P3 maintained task mastery in all fastening conditions 1 and 3 months post-intervention. The case of P3 suggests that at the time that the research occurred, he was still able to acquire and maintain new motor skills suitable for independent dressing.
The case of P5 further explores the possible relationship between diagnosis and performance. P5 was not diagnosed with developmental motor skill regression, and so her poor performance could not necessarily be explicitly related to her diagnosis in the same manner, however could link to her being younger than other participants.
P5 was a 5-year-old girl, diagnosed with septo-optic dysplasia, and registered blind. Additional needs included Autism and diabetes insipid us. P5 had also experienced neonatal abstinence syndrome (withdrawal) as an infant and as a result, resided with her grandparents. P5 was a very polite and softly spoken child. She enjoyed group work but would get frightened if there were any loud or unexpected noises occurring inside/outside the workroom (e.g., crying, screaming, banging).
Compared to all participants, P5 required the most assistance over the intervention period. A teaching assistant would sit beside her and support her (mimicking the researcher). This was done to maximise the opportunity for P5's independent fastening abilities. P5 did not master any fastening. However, she did appear to reach her own level of mastery during the intervention period. This was not transferable to her own outdoor coat/shoes. P5 preferred the button condition as opposed to the others, avoiding other fastenings given the choice. Subsequently she needed encouragement to try the other fastenings in every session. She would attempt the other conditions once or twice but swiftly requested a big button because she liked the feel of it. P5 was the youngest recruited participant in the group with vision impairment, and this may have had more of an effect on her performance through the intervention period than her medical diagnoses.
The cases of P3 and P5 indicated that despite clinical diagnoses, performance in the fastening activities were variable. From P5's case, it is arguable that chronological age may also affect task performance, but from the sessional observations, the performance of both P3 and P5 did not appear to correspond with the characteristics of their diagnoses. This set of case studies arguably demonstrated variation according to task performance and clinical diagnosis.
The following case studies examined different behaviours that may impact on task performance. It was initially thought that the development of independent dressing skills in relation to fastening would have required participants to specifically focus on the task alone and avoid distraction. P2 demonstrates this was not always the case. P2 exhibited multi-tasking behaviour and this possibly may have supported his motor skill development over the intervention procedure.
P2 was a 10-year-old male diagnosed with glaucoma and retinal detachment. P2 did not have verbal communication difficulties but would often mimic or “parrot” words or phrases that were said throughout the sessions.
He was a very inquisitive and chatty child and would often tell jokes within the sessions whilst unfastening/fastening to make the participants and the researcher laugh. He was incredibly motivated toward task completion, often asking if fastening a coat was like fastening a seatbelt, because he had recently learned how to do that. He would constantly ask such questions whilst attempting to unfasten/fasten different materials.
P2 mastered buttons by week 8 and poppers by week 6 of the intervention. He became so comfortable with the button and popper conditions that he would hold remarkably detailed conversations about “wanting to be a dentist” and warning the researcher about the risks of eating too many Easter eggs; “I don't want you to pop!.” He would maintain these conversations whilst continually and successfully unfastening/fastening buttons and poppers. This ability to do two arguably complex things at once with such ease demonstrated multi-tasking behaviour and confidence.
P2 struggled with laces and zips. He was motivated toward fastening zips, due to an awareness that the other members of his group could fasten them. He would become frustrated and say “silly zip” frequently throughout sessions. For fastenings that he struggled with (i.e., zips and laces), he would start conversations about how to successfully unfasten/fasten (correctly) while attempting the pieces.
Observing P2 revealed that when attempting to insert the tail into the slider, he would turn his hands in toward his stomach, meaning that he could not insert the tail due to approaching from the wrong angle. To correct him, he was asked to hold his hands in the correct position for 3 repetitions of 10 s.
P2 would then ask questions and talk about the task whilst he was doing this. As he could be easily distracted, focusing on the action for 10 s would sometimes make him laugh, and so we would start again, for him to remember where to position his hands. Although P2 did not master zips and laces, he continued to attempt these fastenings, and hold conversations about them. P2 never displayed de-motivation toward the tasks. He was able to transfer button and popper skills onto his own outdoor coat, overriding the need to fasten the zip.
The case of P2 demonstrated that engaging with the intervention materials did not necessarily mean a singular focus on the task in hand. For two fastenings, he was able to develop unfastening/fastening skills whilst speaking about related or unrelated concepts. For fastenings that required more fine motor control, and perhaps concentration, he struggled. Potential reasons for this are speculative.
Contrastingly, the following case studies (P19 and P23) examine different aspects of behaviour and performance, where both participants have limited language and communication difficulties. Running group-based interventions meant that participants worked together whilst the researcher divided attention according to individual need(s). Participants generally understood this and requested help when they needed support. This attitude, however, was not always shared. The case of P19 illustrated how attention-seeking behaviours manifest, and the potential negative impact that this may have on a group dynamic.
P19 was a 9-year-old girl diagnosed with Down syndrome. She did have communication problems and used Makaton to support her limited speech. She was very confident, preferred to work directly with the researcher, and would exhibit notable behaviours to ensure this.
P19 was present in the group settings, however would snatch the materials out of the other participants' hands or push them out of the way to have the researcher's attention/sit closer. The researcher explicitly informed her that this was unacceptable behaviour. Despite cooperating with the request, a limited attention span led to the exhibition of cyclical behaviours between defiance and compliance. This was much to the annoyance of the other children in the group.
P19 could be very heavy handed with other participants and the researcher. If she felt ignored, she would grab the researcher's arm or hand and try to drag the researcher away. The researcher would remain in the same position, calmly inform her that the behaviour was unacceptable and continue assisting the other participants.
Generally, P19 responded positively to verbal instructions provided by the researcher regarding her behaviour but would not respond to additional adults (including her mother). She would physically push these people away and move to position herself directly next to the researcher.
She often needed reminded of her behaviour and “kind hands” to participate in the sessions. She responded to this and so was present in the full 10-week intervention. Due to her disruptive behaviour, interruptions could have negatively influenced others in the group. Despite interruption, P19 mastered buttons by week 3 and poppers by week 9. She did not master zips and laces during the intervention, but plateaued relative to her skill by week 6.
The case of P19 demonstrated that some children exhibit negative behavioural strategies to gain attention of a supporting adult. Had the sessions have been uninterrupted, the performance of P19 and potentially others may have been better. Negative behaviours manifest differently and can be facilitated or enhanced through unfamiliarity and prior experience of working with professionals. Despite the incorporation of a familiarisation period in the research design to alleviate anxieties/concerns, the case of P23 illustrates how avoidant behaviour and wariness of supporting adults may affect performance.
P23 was a 9-year-old boy diagnosed with Down syndrome. He was very wary of new people, especially those who he considered “professionals” or teachers who were there to help him. He was very reserved, spending most of his time interacting with his mother rather than the intervention group. He would actively avoid any adult who he perceived to be “support.” Resultantly, P23 would often be uncooperative in the sessions and required gentle introduction to the fastenings. He appeared suspicious of the tasks, as if he was aware that assessments were occurring, so he would mainly attempt unfastening/fastening when he felt comfortable.
Over the 10-week period, he was absent for 4 sessions, meaning that in total he only had 6 weeks of intervention. Despite this, he reached task mastery for buttons and poppers by week 7. He showed improvement over the intervention period for the zip and lace condition, however did not reach task mastery. His mum was very encouraging for the development of independent dressing however, would frequently explain that he was not keen on people helping him specifically.
The avoidant behaviour of P23 could be framed in two ways. The first is that his avoidance is related to shyness and perhaps anxiety, as the voluntary organisation (from which he was recruited) was specifically targeted at different forms of supporting therapy for children with Down syndrome and assessing the impact of these therapies. Yet, framing P23's behaviour in a different light may suggest that due to a motivation toward independence, being surrounded by “supporting” adults may not be conducive to attaining it. The following case (P25) examines the link between participant behaviour (wariness and anxiety) and the potential impact of parental presence in the sessions.
P25 was a 9-year-old boy diagnosed with Down syndrome. He had some spoken language difficulties and used Makaton frequently to support his communication. His mother sat with him for every session.
He was very wary and anxious toward new activities. When initially offered interactive puzzle pieces he would say that he could not do it because it was too difficult, or he was scared. He would say this before he had attempted unfastening/fastening. To support his confidence the researcher verbally encouraged him to try whilst physically (and slowly) showing him how the fastenings worked. He would then engage with the task, overcome his initial anxieties and become excited with his attempts.
If P25's mother perceived him to be slow or unsuccessful she would put her hands over his and complete the task for him, without verbal instruction/explanation. The researcher gently advised that the mother removed her assistance until he asked for help, as this was the nature of the intervention. This was usually effective until P25 attempted another fastening. When attempting different fastenings, the mother would then complete the task for P25, until reminded otherwise. Then, when P25 asked for physical help (“can you help with your hands?”), the researcher assisted with light hand-over-hand (researcher's hand over child's) support and systematic verbal instruction to support. This modelled the behaviour to both P25 and his mother so that she would be able to assist if/when necessary.
Once P25 became more comfortable with the researcher, he would move away from his mother (who was still present) and toward the researcher. He preferred the button condition because he found this easier to achieve, mastering this skill by week 3. He mastered poppers by week 5 but did not master zips and laces by the end of the intervention.
The case of P25 illustrated how initial anxiety toward a task can be overcome with gentle guidance and listening to the voice of the child. In addition, the case of P25 demonstrated how parental presence might have affected the effectiveness of the intervention procedure.
The cases in Study 2 demonstrated the variation of skill ability within and between children with vision impairment and children with Down syndrome. The illustrative case studies were purposefully chosen to contextualise and offer a fuller picture regarding the characteristics of children in response to the novel intervention. The variation in the cases presented demonstrated the heterogeneity of variance of children with vision impairment and children with Down syndrome when participating in the same task (McLinden et al., 2016).
Within the first established theme of clinical diagnosis and intervention performance, the two case studies showed that severity of condition does not always manifest negatively. Based on clinical reports, P3 should have performed poorly in the intervention because of the developmental motor skill regression associated with his condition. This, however, was not apparent at time of testing. In fact, P3 performed consistently better in comparison to the rest of the group with vision impairment and the group with Down syndrome. This could support Habilitation strategies pertaining to the child displaying readiness and motivation to learn new skills (Fairnham et al., 2002). P3's case potentially reveals that there can be a disparity between clinical and functional assessments. Therefore, information regarding performance in uncontrolled/naturalistic (functional) environments (e.g., school/home contexts) should be equally as important or understood as assessment performance in controlled/ideal (clinical) settings. This is consistent with Habilitation practice, as clinical vision assessments inform a practitioner toward the condition and prognosis, whereas functional vision assessments inform the practitioner as to how the child uses their available vision in a natural environment.
The case of P5 also illustrated the concept of diagnosis and performance. Septo-optic dysplasia can be associated with developmental delay relation to motor milestones (Signorini et al., 2012) but was not reported in the questionnaire for this participant. This means that, in terms of motor skill development, P5 may be delayed but was not experiencing motor regression. P5 had a comorbid diagnosis of Autism and diabetes. Of note is the overlap between characteristics of Septo-optic dysplasia and Autism in relation to self-stimulating behaviours such as repetitive head movements and hand fluttering/flapping (Williams et al., 2013), she also demonstrated eye-poking. It was subsequently difficult to ascertain whether task performance was directly related to the primary diagnosis of vision impairment, or whether comorbid conditions were also having an effect. Assuming all diagnoses could affect task performance in various ways, it is crucial to understand that P5 was not motivated toward skill development. She neither demonstrated nor vocalised a desire to achieve the independence skill, although big buttons were her favourite fastening because they were “easy.” She received the most 1:1 support in the sessions yet did not master any fastening. Rather, she reached her own level during the intervention phase and did not increase in skill ability from Week 5. This could also have related to her chronological age, as she was the youngest recruited child with vision impairment.
The second emergent theme was related to behaviour; particularly the exhibition of multi-tasking behaviour, negative attention-seeking behaviour, and relationships with adults (i.e., the researcher and parental influence). The case of P2 was the sole example of multi-tasking to the extent of holding completely unrelated conversations whilst correctly and independently fastening/unfastening buttons and poppers. As each session was analysed, this became an apparent theme despite it presenting at an individual level. The behaviour of P2 is notable as there is a general assumption within Habilitation that children should remain directly “on-task” in terms of language and skill but this was not necessary in this case. P2 appeared confident in his skill ability in fastening/unfastening buttons and poppers. The automaticity of which the skills were correctly demonstrated supported this. His reticence and “on-task-only” language for fastenings he struggled with, indicated that language and focus may bear more importance to develop an emerging skill, rather than practice a newly acquired one. However, one particularly pertinent case does not yield generalizable findings. This is merely indicative of the types of behaviour that children can exhibit whilst developing independence skills.
Further behaviours emerged within the sample with Down syndrome, as characterised in P19. Examined literature in the field (see Walz and Benson, 2002; Næss et al., 2017) generally acknowledged more pro-social behaviours in children with Down syndrome, but this case demonstrated this is not always consistent. The physicality of these attention-seeking behaviours was notable and concerning; from a safety perspective the researcher was in a position of safeguarding and trust, so such interruptions were problematic to ensure the safety of the group. Further, these disruptions reduced amount of time “on-task” in the group setting, subsequently reducing the opportunity to learn and develop the skills. As each child consented to take part in each session, this could not be reduced to “withdrawing,” especially as P19 was, in effect, predominantly demanding the attention of the researcher. Perhaps the explanation of this behaviour was that P19 did not want to engage in a group setting, preferring 1:1. Speculatively, this could be the case for children who are used to having consistent 1:1 support as part of their Educational Health Care Plan provision. The slower development of fastening skills could therefore be understood in two ways; disruption led to lack of opportunity to learn the skill, and global developmental delay associated with Down syndrome would have an effect regardless of behaviour. These two concepts are not mutually exclusive, as cognitive impairments can manifest in disruptive behaviour (see Capone et al., 2006).
The role of adults requires consideration in the development of fastening skills; understanding that children with vision impairment and children with Down syndrome will have substantial adult input from birth/early infancy. Medical intervention, routine appointments and multiple testing with various practitioners and professionals are part of their everyday life. Scepticism toward unfamiliar, intervening, adults is to be expected. Despite the intention to help/support these children, it cannot and should not be assumed that they will gladly receive it. Adopting a child-directed intervention therefore afforded an element of child-control about the situation, particularly how they chose to engage with the intervention materials. The case of P23 encapsulated the initial wariness of adults and showed how, over time, he became more respondent, engaged, and subsequently developed fastening skills. Researchers, practitioners and professionals should be aware of the role that they play in each child's life, and how this can affect their emotional state/task performance. Parents also play a crucial role, and, as parents being considered the first Habilitation specialists, their input is vast and various. Parental overprotection, however, can be prevalent in parents of children with vision impairment and children with Down syndrome (e.g., Alesi and Pepi, 2015; Munro et al., 2016). This was demonstrated in P25 where the mother, quite naturally, wanted to support her child with a difficult task. Her support manifested in completing the activity for the child, contradicting the intervention aim of promoting independence. Literature regarding parental support in dressing supports this behaviour, where parents will complete the task for speed/ease. However, this reduces time and opportunity for skill development. P25 mastered buttons and poppers over the intervention, but not laces and zips. Speculatively, his performance may have differed had he the full opportunity to develop his skills. However, this is an accurate reflection of real-world situations, whereby parents/caregivers are uncomfortable in seeing their child struggle.
The cases presented encapsulate the real-world nature of conducting an intervention in children with vision impairment and children with Down syndrome. The cases revealed that the intervention was suitable for skill development, but individual profiles contribute to the overall effectiveness of the intervention. Heterogeneity of variance is therefore a fundamental aspect to incorporate in research design for children with disabilities (Warren, 1984). Generalisations to broader populations of vision impairment and Down syndrome cannot and should not be made to truly incorporate heterogeneity of variance. The inability to generalise is a limitation of Study 2, further, of 18 cases made only 6 were presented.
Dressing is an essential independent living skill often taken for granted. There are few empirically-based studies exploring the development of independence skills in children with vision impairment and fewer with children with Down syndrome. This project was underpinned by habilitation theory and practice, using a step-wise task analysis approach to intervention design and implementation. By reporting frequencies of fastenings at different ages a structured intervention relative to participant age and stage was designed. This is important as a habilitation programme systematically trains independence skills over developmental phases that are age and stage appropriate to each individual child (Wall, 2019), accommodating the notion that the developmental age of the child may be lesser than their chronological age as a result of developmental delay (vision impairment) and/or intellectual disability (Down syndrome). This bespoke individualized approach to developing independence skills may support parents, Habilitation Assistants/Specialists and the multidisciplinary team surrounding the child nationally and internationally. Both presented studies are complementary to the development of independent dressing skills in children with vision impairment and children with Down syndrome. This paper reveals the intricate detail that is employed when designing systematic Habilitation training, and the effectiveness of running a bespoke intervention. The current paper also demonstrated how habilitation could be extended to support children with Down syndrome. This in line with the Special Educational Needs Code of Practice England (Department for Education and Department of Health, 2015) which entitles all children with special educational needs and disabilities to access Habilitation provision.
Findings revealed that the 10-week intervention was effective to a certain extent in children with vision impairment and children with Down syndrome. However, participant absences and behaviours (anxiety, attention seeking, and parental overprotection) in the group with Down syndrome arguably limited the effectiveness and transference onto personal clothing items. Of the sample, only 3 children with vision impairment were able to transfer acquired skills onto personal items of clothing (outdoor coat and shoes). No children with Down syndrome were able to transfer skills onto personal clothing items. Further, absence and the inability to follow-up the study with the children with Down syndrome was an unforeseeable yet compromising factor for the intervention outcome. The case study data reveals a greater depth to the development of independence skills, highlighting that heterogeneity of variance within the sample and participant (and adult/peer) behaviours that might affect skill development. This paper is original in applying child-centred habilitative principles to developing independent fastening skills, as previous literature adopted rehabilitation, adult-focussed techniques (e.g., Klein, 1983; Fairnham et al., 2002), which are incompatible in application to child development.
Fastening variation noticeably increased in the 2–14 years clothing sample. This is important as rapid social, emotional, cognitive and motor skill development occurs within the age range of “2–14 years” (particularly until the age of six (Shonkoff and Meisels, 2011). This means that the emerging independent dressing skills might have a link to these areas of development, specifically in terms of pre-requisite and actual gross/fine motor skill acquisition. The impact of these developmental changes may be enhanced by high exposure to certain fastenings. The development of fastening skills in children may be a conscious expression of awareness of the dressing procedure in terms of; the systematic nature of the dressing sequence, an understanding of the fastenings used and why they are important, and, the strategies employed to achieve successful dressing. These are fundamental concepts to maintain through development into adulthood, as the survey supported the increase in complexity and range of fastenings. Motivation, readiness, and age/stage appropriateness can only account for a portion of task mastery. Exposure, opportunity and task mastery are also influenced by parental choice for clothing. A preference for slip-on (as indicated in Table 2) potentially limits a child's exposure/development which could explain initial reduced skill ability in Study 2. This means that a child's limited exposure to clothing items with functional fastenings would imply a limited opportunity to familiarise, practise and refine their fine motor skills for fastening.
The 10-week intervention afforded opportunity for familiarisation, manipulation, and skill acquisition of fastenings that the children might not have had previous exposure to in the home context. If a child is not afforded the opportunity to fasten/unfasten due to a predominant exposure to slip on clothing, it is less likely that fastening skills would develop. In addition, if a parent/caregiver chose to fasten/unfasten any item of clothing instead of providing the child with an opportunity to manipulate the materials, independent dressing skills may also be delayed. This means that to develop independent living skills generally, a child must have exposure to particular objects and opportunities for developing the skill. Allowing time for rehearsal and subsequent skill development is also essential (Bardin, 2014). As parents are considered to be the first habilitation specialists they play a crucial and fundamental role in supporting independent living skill development (Kellegrew, 2000; Tadić et al., 2013; Bathelt et al., 2019). Their choices reflect upon the opportunities for development of independence skills and adaptive behaviour, although sometimes their view of their child's abilities is discordant with what their child can actually achieve (Tadić et al., 2013). It ought to be further acknowledged that the children (becoming adults) may then become parents. This means that developing popper-fastening skills would be a skill transferable to parenthood, applied to their own children's development.
In the Habilitation context and with focus on dressing, understanding current trends, potential exposure, awareness of fastenings, and the dressing sequence is essential when designing a practical intervention accessible to parents and the multi-disciplinary team surrounding the child. The advantage of using a web-based search (Study 1) was that data recording and filtering (based on consumer habits) was simple and replicable. This could not necessarily be achieved in a physical outlet. The disadvantage was that recording relied heavily on the quality of product description/images. It was found that where one aspect of the recording failed (e.g., product description), the other aspect (e.g., product images) provided sufficient, recordable information. The fastening frequencies based on consumer habits offered reasonable justification for the interactive puzzle game to include zips, buttons, poppers and shoelaces based on likelihood of exposure. However, it is important to note that high fastening exposure does not necessarily entail high fastening experience/task mastery.
Further information that could inform Study 2 and influence skill development pertained to sibling data. Recording participant's siblings and their ages can inform the research as it takes account of other fastenings that the participant may be exposed to within the home environment. For example, if the participant has younger siblings aged “0–2 years,” it could be assumed that the participant will have a greater likelihood of exposure to popper fastenings, as well as the popular fastenings associated with participant age. If the participant has older siblings, aged up to 14 years, or adult (e.g., 18 years), it could be assumed that the participant likely has a higher exposure to broader, more diverse and complex clothing and fastenings. If the participant has both younger and older siblings, their potential exposure may extend further, across all age groups. This exposure may suggest an association between fastener exposure frequency and the independent dressing skill ability associated with fastening/unfastening.
The training of motor skill and evaluation of changes was based on Habilitation practice and the case for early intervention. One grounding principle of habilitation is the development of independent living skills (once the child/young person demonstrates readiness to learn) that should transfer and support independence skills into adulthood. This study revealed a snap-shot in time regarding the effectiveness of a 10-week intervention demonstrating how gross/fine motor skill acquisition in relation to fastening skills developed. Potential issues surrounding this approach is that first, motor skills need practice and time in order to learn and maintain skill development. In the sample of children with vision impairment, there was evidence suggesting that fastening skills plateaued or marginally increased 1 and 3 months after the intervention ceased. This suggested an effect, however more detail is required to understand further input/training, if any, in home and educational settings. A follow-up longitudinal study is needed to track skill development and transference through childhood, into adolescence and adulthood. Further, the measure of progression/skill acquisition in this paper is bespoke to the intervention as a result of lack of nuanced task-analysis based measures of independence skills. Future work could combine this measure with existing measures [e.g., The Oregon Project USA (Anderson et al., 2007) and the scientifically evaluated Developmental Journal for babies and young children with visual impairment (Dale et al., 2019)] could benefit future work.
There are strengths and limitations to both studies, addressed in interim discussions and here, but overall the intervention appeared to be suitable and useful for the development of fastening skills in children with vision impairment and children with Down syndrome. Future work could explore and contextualise fastening use and global availability, examining trends and accounting for cultural dress. This would add to the existing survey, and arguably further supplement the development of intervention materials cross-culturally in relation to the development of independent living skills and adaptive behaviour.
In conclusion, dressing is a necessary yet complex and time-consuming skill to acquire. For children with visual needs, mastering the task can take longer due to the inability or reduced capacity to learn through observation. This paper showed that an informed and purposive child-centred Habilitation intervention can increase fastening skill ability within a 10-week period in children with vision impairment and children with Down syndrome. These developed (or emerging) transferable skills supports each child's transition into adolescence and adulthood. The systematic and purposive design lends itself to further replication and investigation. This study offers an original, practical solution for parents and professionals toward the development of the fundamental independent living skill of dressing in children with vision impairment and children with Down syndrome.
The datasets generated for this study will not be made publicly available The ethics form states that only processed data will be made available. Datasets are not public available to maintain confidentiality/anonymity of the participants (Study 2). Anonymised vignettes/further case studies/detail are presented in Hayton (2017).
The studies involving human participants were reviewed and approved by UCL Institute of Education Ethics Committee. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
JH, DD, and KW contributed conception and design. JH acquired, analysed, and interpreted the data. JH wrote article drafts, DD and KW reviewed the first draft.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors would like to acknowledge Professor Chloe Marshall (UCL Institute of Education) for her helpful comments on previous versions of this manuscript. The child clothing sample 0–14 years (Study 1) and case studies (Study 2) first appeared in a thesis (Hayton, 2017). This is the only form of which these data have appeared and the thesis is available online.
SEND, Special Educational Needs and Disabilities.
Alesi, M., and Pepi, A. (2015). Physical activity engagement in young people with down syndrome: investigating parental beliefs. J. Appl. Res. Intellect. Disabil. 30, 71–83. doi: 10.1111/jar.12220
All Party Parliamentary Group on Down Syndrome (2012). Down Syndrome: Good Practice Guidelines for Education. Visit Down Syndrome Education International's Web Site. Available online at: https://www.dseinternational.org/en-gb/reports/2012/appg-down-syndrome-education-guidelines/ (accessed December 4, 2019).
Anderson, S., Boigon, S., Davis, K., DeWaard, C., and South Oregon Education Service District (2007). The Oregon Project for Preschool Children Who are Blind or Visually Impaired, 6th Edn. Medford, OR: South Oregon Education Service.
Ayllón, E., Moyano, N., Lozano, A., and Cava, M. J. (2019). Parents' willingness and perception of children's autonomy as predictors of greater independent mobility to school. Int. J. Environ. Res. Public Health 16:732. doi: 10.3390/ijerph16050732
Bardin, J. A. (2014). “Independent living,” in ECC Essentials: Teaching the Expanded Core Curriculum to Students With Visual Impairments, eds C. B. Allman and S. Lewis. (New York, NY: American Printing House for the Blind).
Bathelt, J., de Haan, M., and Dale, N. J. (2019). Adaptive behaviour and quality of life in school-age children with congenital visual disorders and different levels of visual impairment. Res. Dev. Disabil. 85, 154–162. doi: 10.1016/j.ridd.2018.12.003
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Capone, G., Goyal, P., Ares, W., and Lannigan, E. (2006). Neurobehavioral disorders in children, adolescents, and young adults with Down syndrome. AJMG 142, 158–172. doi: 10.1002/ajmg.c.30097
Carr, J. (2000). Intellectual and daily living skills of 30-year-olds with Down's syndrome: continuation of a longitudinal study. J. Appl. Res. Intellect. Disabil. 13, 1–16. doi: 10.1046/j.1468-3148.2000.00003.x
Carr, J. (2005). Stability and change in cognitive ability over the life span: a comparison of populations with and without Down's syndrome. J. Intellect. Disabil. Res. 49, 915–928. doi: 10.1111/j.1365-2788.2005.00735.x
Costanzo, F., Varuzza, C., Menghini, D., Addona, F., Gianesini, T., and Vicari, S. (2013). Executive functions in intellectual disabilities: a comparison between Williams syndrome and Down syndrome. Res. Dev. Disabil. 34, 1770–1780. doi: 10.1016/j.ridd.2013.01.024
Creavin, A. L., and Brown, R. D. (2009). Ophthalmic abnormalities in children with down syndrome. J. Pediatr. Ophthalmol. Strabismus 46, 76–82. doi: 10.3928/01913913-20090301-06
Cregg, M., Woodhouse, J. M., Stewart, R. E., Pakeman, V. H., Bromham, N. R., Gunter, H. L., et al. (2003). Development of refractive error and strabismus in children with Down syndrome. Investig. Ophthalmol. Vis. Sci. 3, 1023–1030. doi: 10.1167/iovs.01-0131
Cuturi, L. F., Aggius-Vella, E., Campus, C., Parmiggiani, A., and Gori, M. (2016). From science to technology: orientation and mobility in blind children and adults. Neurosci. Biobehav. Rev. 71, 240–251. doi: 10.1016/j.neubiorev.2016.08.019
Dale, N. J., Sakkalou, E., O'Reilly, M. A., Springall, C., Sakki, H., Glew, S., et al. (2019). Home-based early intervention in infants and young children with visual impairment using the developmental journal: longitudinal cohort study. Dev. Med. Child Neurol. 61, 697–709. doi: 10.1111/dmcn.14081
Department for Education Department of Health (2015). SEND Code of Practice: 0 to 25 Years. GOV.UK. GOV.UK. Available online at: https://www.gov.uk/government/publications/send-code-of-practice-0-to-25 (accessed December 4, 2019).
Dolva, A.-S., Coster, W., and Lilja, M. (2004). Functional performance in children with Down syndrome. Am. J. Occup. Ther. 58, 621–629 doi: 10.5014/ajot.58.6.621
Fairnham, M., Johnston, C., Kain, S., Kaine, N., McCauley, A., and Steele, E. (2002). Do It Yourself: Encouraging Independence in Children Who Are Blind. Sydney, NSW: Vision Australia.
Favela, L. H., Riley, M. A., Shockley, K., and Chemero, A. (2018). Perceptually equivalent judgments made visually and via haptic sensory-substitution devices. Ecol. Psychol. 30, 326–45. doi: 10.1080/10407413.2018.1473712
Greenaway, R., Pring, L., Schepers, A., Isaacs, D. P., and Dale, N. J. (2017). Neuropsychological presentation and adaptive skills in high-functioning adolescents with visual impairment: a preliminary investigation. Appl. Neuropsychol. Child. 6, 145–157. doi: 10.1080/21622965.2015.1129608
Hayton, J., and Dimitriou, D. (2019). What's in a word? Distinguishing between habilitation and re-habilitation. Int. J. Orientation Mobility 10, 1–4. doi: 10.21307/ijom-2019-007
Hayton, J., Wall, K., and Dimitriou, D. (2018). Get your coat: examining the development of independent dressing skills in young children with visual impairment, down syndrome and typically developing children. Int. J. Inclusive Educ. 1–16. doi: 10.1080/13603116.2018.1456568
Hayton, J. A. (2012). ‘Get Your Coat': Developing the Independent Living Skill of Dressing in Visually Impaired Children (Dissertation). Institute of Education.
Hayton, J. A. (2017). Get Your Coat: Examining the Development of Independent Dressing Skills in Young Children With Visual Impairment in Comparison With Young Children With Down Syndrome and Typically Developing Children (Thesis). UCL Institute of Education, London United Kingdom. Available online at: http://discovery.ucl.ac.uk/1541120/1/Jessica%20Hayton%20Thesis.pdf (accessed December 4, 2019).
Herwegen, J. V., Rundblad, G., Davelaar, E. J., and Annaz, D. (2011). Variability and standardized test profiles in typically developing children and children with williams syndrome. Br. J. Dev. Psychol. 29, 883–94. doi: 10.1111/j.2044-835X.2010.02015.x
Kellegrew, D. H. (2000). Constructing daily routines: a qualitative examination of mothers with young children with disabilities. Am. J. Occup. Ther. 54, 252–59. doi: 10.5014/ajot.54.3.252
Klein, M. D. (1983). Pre-Dressing Skills: Skill Starters for Self-Help Development. Tucson, AZ: Communication Skill Builders.
Lewis, S., and Iselin, S. A. (2002). A Comparison of the independent living skills of primary students with visual impairments and their sighted peers: a pilot study. J. Vis. Impairment Blindness 96, 335–44. doi: 10.1177/0145482X0209600505
Luz Carvalho, R., and Vasconcelos, D. A. (2011). “Motor behavior in Down syndrome: atypical sensoriomotor control.” in: Prenatal Diagnosis and Screening for Down Syndrome, ed S. Dey S. INTECH Rijeka (London). Available online at: https://www.intechopen.com/books/prenatal-diagnosis-and-screening-for-down-syndrome/motor-behavior-in-down-syndrome-atypical-sensoriomotor-control
Malak, R., Kotwicka, M., Krawczyk-Wasielewska, A., Mojs, E., and Szamborski, W. (2013). Motor skills, cognitive development and balance functions of children with Down syndrome. Ann. Agric. Environ. Med. 20, 803–806.
Mancini, M. C., Carvalho e Silva, P. C., Gonçalves, S. C., and de Medeiros Martins, S. (2003). Comparison of functional performance among children with Down syndrome and children with age-appropriate development at 2 and 5 years of age. Arquivos Neuro-psiquiatria 61, 409–415 doi: 10.1590/S0004-282X2003000300016
McLinden, M., Douglas, G., Cobb, R., Hewett, R., and Ravenscroft, J. (2016). ‘Access to learning'and ‘learning to access': analysing the distinctive role of specialist teachers of children and young people with vision impairments in facilitating curriculum access through an ecological systems theory. Br. J. Vis. Impairment 34, 177–195 doi: 10.1177/0264619616643180
Miller, O., Wall, K., and Garner, M. (2011). Quality Standards: Delivery of Habilitation Training (Mobility and Independent Living Skills) for Children and Young People with Visual Impairment. Available online at: http://www.ssc.education.ed.ac.uk/resources/vi&multi/habilitation.pdf (accessed July 10, 2019).
Munro, M. P., Garza, M. M., Hayes, J. R., and Watt, E. A. (2016). Parental Perceptions of Independence and Efficacy of Their Children with Visual Impairments. SFA ScholarWorks. Available online at: http://scholarworks.sfasu.edu/jhstrp/vol1/iss1/3 (accessed July 9, 2019).
Næss, K. B., Nygaard, E., Ostad, J., Dolva, A.-S., and Lyster, S.-H. (2017). The profile of social functioning in children with Down syndrome. Disabil. Rehabil. 39, 1320–1331. doi: 10.1080/09638288.2016.1194901
Oakland, T., and Harrison, P. L. (2008). “Adaptive behaviors and skills: an introduction,” in Adaptive Behavior Assessment System-II, eds T. Oakland and P. L. Harrison (Burlington, MA: Academic Press), 3–18.
Pereira, K., Basso, R. P., Lindquist, A. R. R., Da Silva, L. G. P., and Tudella, E. (2013). Infants with Down Syndrome: Percentage and Age for Acquisition of Gross Motor Skills. Res. Dev. Disabil. 34, 894–901. doi: 10.1016/j.ridd.2012.11.021
Public Health (2015). Improving School Readiness: Creating a Better Start for London. GOV.UK. GOV.UK. Available online at: https://www.gov.uk/government/publications/improving-school-readiness-creating-a-better-start-for-london (accessed December 04, 2019).
Riou, E. M., Ghosh, S., Francoeur, E., and Shevell, M. I. (2008). Global developmental delay and its relationship to cognitive skills. Dev. Med. Child Neurol. 51, 600–606. doi: 10.1111/j.1469-8749.2008.03197.x
Salt, A., and Sargent, J. (2014). Common visual problems in children with disability. Arch. Dis. Childhood 99, 1163–68. doi: 10.1136/archdischild-2013-305267
Shonkoff, J. P., and Meisels, S. J. (2011). Handbook of Early Childhood Intervention. Cambridge: Cambridge University Press.
Signorini, S. G., Decio, A., Fedeli, C., Luparia, A., Antonini, M., Bertone, C., et al. (2012). Septo-optic dysplasia in childhood: the neurological, cognitive and neuro-ophthalmological perspective. Dev. Med. Child Neurol. 54, 1018–24. doi: 10.1111/j.1469-8749.2012.04404.x
Suddath, C. (2010). A Brief History of: Velcro. Time. Time. Available online at: http://content.time.com/time/nation/article/0,8599,1996883,00.html (accessed December 4, 2019).
Sugden, D., and Wade, M. G. (2013). Typical and Atypical Motor Development. London: Mac Keith Press.
Summers, J., Larkin, D., and Dewey, D. (2008). Activities of daily living in children with developmental coordination disorder: dressing, personal hygiene, and eating skills. Human Mov. Sci. 27, 215–29. doi: 10.1016/j.humov.2008.02.002
Swallow, R.-M., and Huebner, K. M. (1987). How to Thrive, Not Just Survive: a Guide to Developing Independent Life Skills for Blind and Visually Impaired Children and Youths. New York, NY: American Foundation for the Blind.
Tadić, V., Cooper, A., Cumberland, P., Lewando-Hundt, G., and Rahi, J. S. (2013). Development of the functional vision questionnaire for children and young people with visual impairment: the FVQ_CYP. Ophthalmology 120(12), 2725–2732. doi: 10.1016/j.ophtha.2013.07.055
Taverna, L., Bornstein, M. H., Putnick, D. L., and Axia, G. (2011). Adaptive behaviors in young children: a unique cultural comparison in Italy. J. Cross Cultural Psychol. 42,445–465 doi: 10.1177/0022022110362748
Thomas, M. S., and Knowland, V. C. (2014). Modeling mechanisms of persisting and resolving delay in language development. J. Speech Language Hearing Res. 57, 467–483. doi: 10.1044/2013_JSLHR-L-12-0254
von Tetzchner, S., Fosse, P., and Elmerskog, B. (2013). Juvenile neuronal ceroid lipofuscinosis and education. Biochim. Biophys. Acta 1832, 1894–1905. doi: 10.1016/j.bbadis.2013.02.017
Wall, K. (2019). “Habilitation and rehabilitation,” in The Routledge Handbook of Visual Impairment: Social and Cultural Research, ed J. Ravenscroft (London :Routledge), 333–359.
Walz, N. C., and Benson, B. A. (2002). Behavioral phenotypes in children with Down syndrome, Prader-Willi syndrome, or Angelman syndrome. J. Dev. Phys. Disabil. 14, 307–321. doi: 10.1023/A:1020326701399
Warren, D. (1982). “The development of haptic perception. essay,” in Tactual Perception: A Sourcebook, eds W. Schiff and E. Foulke. (Cambridge: Cambridge University Press).
Warren, D. H. (1984). Blindness and Early Childhood Development. New York, NY: American Foundation for the Blind
Keywords: habilitation, vision impairment, down syndrome, independent living skills, adaptive behaviour, dressing, SEND
Citation: Hayton J, Wall K and Dimitriou D (2019) Let's Get It On: Dressing Skill Development in Children With Vision Impairment and Children With Down Syndrome. Front. Educ. 4:149. doi: 10.3389/feduc.2019.00149
Received: 12 July 2019; Accepted: 29 November 2019;
Published: 12 December 2019.
Edited by:
Susana Castro-Kemp, University of Roehampton London, United KingdomReviewed by:
Mats Granlund, Jönköping University, SwedenCopyright © 2019 Hayton, Wall and Dimitriou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica Hayton, amVzc2ljYS5oYXl0b25AdWNsLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.