 Alexandra Delmas
Alexandra Delmas Benjamin Clement
Benjamin Clement Pierre-Yves Oudeyer
Pierre-Yves Oudeyer Helène Sauzéon1,3*
Helène Sauzéon1,3*- 1Equipe Flowers, Inria, Talence, France
- 2Ensta Paris-Tech, Paris, France
- 3Laboratoire Handicap, Activité, Cognition et Santé (EA4136), Université de Bordeaux, Bordeaux, France
Coupled with Health Education programs, an e-learning platform—KidBreath—was participatory designed and assessed in situ (Study 1) and was augmented and tested with an Intelligent Tutoring System (ITS) based on Multi-Armed Bandit Methods (Study 2). For each study, the impact of KidBreath practice was assessed in children with asthma in terms of pedagogical efficacy (knowledge of the illness), pedagogical efficiency (usability, type of motivation and level of interest elicited), and therapeutic effect (illness perception, system's expectation and judgement in disease self-management, child's implication in study). For the Study 1, asthma children aged 8 to 11 years used the tool at home without time pressure for 2 months according to a predefined learning sequence defined by the research team. Results supported pedagogical efficacy of KidBreath, with a significant increase of general knowledge about asthma after use. It also featured a greater learning gain for children knowing the least about the illness before use. Results on pedagogical efficiency revealed a great intrinsic motivation elicited by KidBreath showing a deep level of interest in the edutainment activities. Study 2 explored an augmented version of KidBreath with learning optimization algorithm (called ZPDES) after its use during 1 month. Pedagogical efficacy was less conclusive than Study 1 because less content was displayed due to algorithm parameters. However, the ITS-augmented KidBreath use showed a strong impact in pedagogical efficiency and therapeutic adherence features. Even if implementation improvements must be done in future works, this preliminary study highlighted the viability of our methods to design an ITS as serious game in health education context for all chronic diseases.
Introduction
According to World Health Organization (WHO), asthma is the most common chronic disease among children1, with a low illness control (Rabe et al., 2004; Gustafsson et al., 2006). One reason for asthma children's multiple hospital stays lies is the lack therapeutic adherence (to have a positive attitude toward good health practices) (Morris and Schulz, 1992). Only 50% of children with asthma are generally known adherent (Bauman et al., 2002). One of the key factors behind a low level of therapeutic adherence usually lies in the patient's lack of knowledge concerning the illness and its medication (Lieberman, 2001; de Benedictis and Bush, 2007; Kharrazi et al., 2008; Naimi et al., 2009).
To improve therapeutic adherence mechanisms, Health education—related to the concept of Health Literacy2–is generating a plethora of research questions to be answered by multidisciplinary teams, including the fields of Education, Health, and Technology-Enhanced Learning (TEL) (Nutbeam, 1998, 2008; Mitic et al., 2012). Therapeutic education aims to help patients suffering from chronic illnesses acquire and maintain self-management skills concerning the awareness and regulation of their illness in their daily life. In order for this apprenticeship to be the most efficient, it has to rely strongly on patients' background and past experiences with the illness (Mitic et al., 2012). A systematic review revealed benefits of educational interventions for self-management for improving health results (Guevara et al., 2003).
Within the TEL community, numerous educational devices and interactive systems were developed to help teachers make children learn better as well as to increase their motivation to learn (Hirsh-Pasek et al., 2015). Massive Open Online Courses (MOOCs)S created using a variety of technological devices and methods, currently spread knowledge worldwide by using a distant, high number of learners to one teacher, asynchronized learning environment. Nowadays, the majority of such online learning systems became much simpler online tools delivering personalized transmedia content to targeted learners, instead of more traditional reading materials students ought to go through. New systems are far from the complex teaching aids initially used in traditional classroom settings. Computer Assisted Education (CAE) systems have evolved as learning tools providing students with encoded set of exercises and associated solutions (Huertas and Juárez-Ramírez, 2013). CAE systems usually provide problems with a single correct answer, hence when the problem arises, a more complex scenario cannot be completely evaluated, especially when a single problem may have a lot of potential correct answers. The effectiveness of CAE systems was shown, but there is still a gap to be filled for more complex topics. This is why the Intelligent Tutoring Systems (ITS) have proved to match and even surpass CAE system performance (Glickman and Dixon, 2002). As learners generally study structurally-similar courses in a linear manner (which accounts for nearly 90% of school dropout behaviors), ITS were created to make learning more accessible and efficient to learners, as well as to define specific pedagogical goals and metrics to be used in education research (Anderson et al., 1995; Koedinger et al., 1997; Nkambou et al., 2010). In the past decades, such systems aimed to automatically evaluate students' learner models. A learner model can be defined by a set of beliefs a teacher can form about a student's level in a specific learning context. Among such beliefs are a set of knowledge and skills to acquire on a target domain and a student's learning preferences.
Considering the massive expansion of the world wide web high-tech devices home usage and the known benefits of young learners' usage of video games in learning contexts, the field of TEL soon welcomed a new sub-field called serious games (Malone, 1980; Cordova and Lepper, 1996; Bergeron, 2006; Kam et al., 2008; Hirsh-Pasek et al., 2015), which were games designed in a traditional video game landscape, but including some pedagogical goals (Kapp, 2012). They are specifically aimed at using intrinsic gaming mechanisms to foster long term learning retention (Whyte et al., 2015). According to the Social Cognitive Theory, intrinsic motivation requires the presence of an intrinsic contentment to involve oneself in a specific activity for one's own benefit (Touré-Tillery and Fishbach, 2014; Kaloti-Hallak et al., 2015).
The main focus was to study the potential benefits of using a serious game designed following a Participatory Design (PD) approach for supporting a therapeutic education intervention amongst children with asthma. Our main contributions are the following:
- The KidBreath assessment in real-life setting (use at home) for its impact in terms of pedagogical efficacy, pedagogical efficiency, and therapeutic effect (Study 1);
- The assessment of the added value of an ITS embedded in KidBreath with a field study according to similar evaluation criteria to those used in study 1 in order to move the field with an automatized learning personalization in health education (Study 2).
Study 1: Field Study for Assessment of KidBreath
Related Work: E-Education for Asthma Children
In order to promote therapeutic adherence, therapeutic educational programs were designed in workshops that could include one or several health practitioners. To foster educational impact in long-term use, researchers (Rikkers-Mutsaerts et al., 2012) carried out internet-based self-management for children with asthma, which included asthma information, news, frequently asked questions and interactive communication with a specialized nurse (Gibson et al., 2002). In another study, the intervention included just internet-based management and education received though the web site with tele-monitoring (Chan et al., 2007). Jan and colleagues studied over a 12 week-period the impact of Internet-based interactive asthma educational and monitoring program, composed of basic information asthma child-related, an electronic diary, an action plan for the patients, and a retrieval analysis system to review the accumulated data on symptoms score (Jan et al., 2007). After using these web-based educational programs from 3 months to 1 year, all studies showed that the quality of life and treatment use were improved but not for asthma control.
According to TEL field, gamification is widely used as an approach due to its known benefits on different aspects of learning (Malone and Lepper, 1987; Cordova and Lepper, 1996; Shaffer, 2006). It refers to the use of game-based mechanisms in a non-gaming context to engage users, to increase their motivation, and to improve learning (Deterding et al., 2011; Kapp, 2012; Hamari et al., 2014). Nowadays, a majority of such tools are designed specifically for the treatment of chronic illness in terms of illness prevention and illness awareness. However, few were evaluated scientifically in terms of knowledge acquisition process and day-to-day management in mid to long term use (Lieberman, 2001; Shegog et al., 2001; Beale et al., 2007; Charles et al., 2007; Kato et al., 2008). These serious games are reported as providing benefits to minimize the pain while hospital staff changed the bandages for burned victims (Sharar et al., 2007; Hoffman et al., 2008), increasing self-esteem, self-management, and foster health practice for diabetes patients (Brown et al., 1997; Lieberman, 2001), and improving self-esteem and compliance for teenage patients suffering from cancer (Beale et al., 2007; Kato et al., 2008).
Regarding impacts for asthma children, only one serious game was studied, i.e., Bronkie the Bronchiasaurus (Lieberman, 1997, 2001). It is a Nintendo video game. The story tale revolves around a prehistoric world covered in dust. One of the main vacuum cleaners had the misfortune to break, therefore letting dust settles all over the ground. Players can perform the following tasks: take their inhaler regularly and in a safe manner, try to avoid asthma attacks provoked by close-contact to dust and fumes, and keep following their quest. In order to progress to the next stage of the quest, children also ought to answer a set of questions about asthma correctly (multiple choice questions on one's respiratory system, asthma self-management, identification of main triggers, instant recognition of first symptoms and how to act in case of emergencies, knowledge of the medicine's active principles, etc.). Lieberman's research team led several studies on the impact of the videogame on therapeutic adherence. One of them asked young asthma patients to play for 40 min at the hospital, complete questionnaires about asthma before and after use, as well as answering a phone interview 1 month later. Results showed an increase in self-esteem and self-efficacy, patients' ability to communicate about illness with their parents, and their general knowledge about asthma and self-regulation (Lieberman, 2001). Despite the great interest of this singular serious game for asthma children, several limitations could be pinpointed. First, all the assessment has been done within a hospital rather than in mainstream environments (such as a child's home) as the best place for health education. Second, there is no mention of how the learning modules of the games were linked and validated with the current therapeutic learning programs involved. For example, none of the proposed activities attempted to capture children's learning curves or the establishment of new daily routines after using the tools. Third, the learning benefit has been assessed for a short-term window, so near/far effects of the serious game have not been documented. Therefore, to overcome these limitations, study 1 aimed to detail design process of a new serious game, i.e., KidBreath, for home's use by asthma children and to assess its pedagogical impact over short-term (1 month) and long term (2 months) period.
KidBreath Design (Details in the Supplementary Material, Appendix 1)
Participatory Design
Our thereby designed e-learning platform, KidBreath proposes asthma-related edutainment activities to asthma patients aged 8 to 10. Complying to user-centered design approaches, a Participatory Design (PD) methodology was selected (Muller and Kuhn, 1993; Sanders, 2002; Melonio and Gennari, 2012). PD aims to build interactive tools by including end-users and relevant stakeholders (for gathering plural experience and expertise) as design partners in various parts of the design process in order to guaranty the conformity of the requirements elicitation process to the user's needs. The team of design partners may be formed of a set of target users (i.e., asthma patients aged 8 to 10) and indirect actors within the learning process (i.e., parents, therapeutic educators, health specialists, or designers). While the use of the PD approach revealed beneficial in several health education studies, none seemed to have been previously applied to the use of serious games for health education in a child population.
The public safety aspects of this project were overseen by the Therapeutic Education Center in Bordeaux Aquitaine (Centre d'Education Thérapeutique de Bordeaux Aquitaine), a health association. Health specialists and young patients both helped in the design of the edutainment activities. Their participation included the creation of a public health education program concerning asthma, iteratively validated by experts and patients during the various steps of the design process. Prior to launching the experimental study, several administrative authorizations were gathered in terms of ethics (COERLE3 within the INRIA), web usage and data gathering (CNIL4), National education services (DSDEN5) in addition to every child's parental consent form.
To ensure pedagogical benefits of such a tool, KidBreath was evaluated on non-asthma children with the age of our target users – 8 to 9 years old—from a local primary school. Here, learning activities could be chosen (Figure 1) and experiments were conducted in school for 2 weeks to assess the tool impact in terms of pedagogical efficacy (knowledge asthma-related) and efficiency (curiosity, motivation, usability, user experience) (Delmas et al., 2018). Results showed a significant increase of general knowledge about asthma after use, revealing the pedagogical efficacy of KidBreath. Results on pedagogical efficiency revealed intrinsic motivation generated during the study and a good usability of the tool with children showing a deep level of interest in the edutainment activities. Taken together, results were supportive of KidBreath as future device for health education relative to asthma.
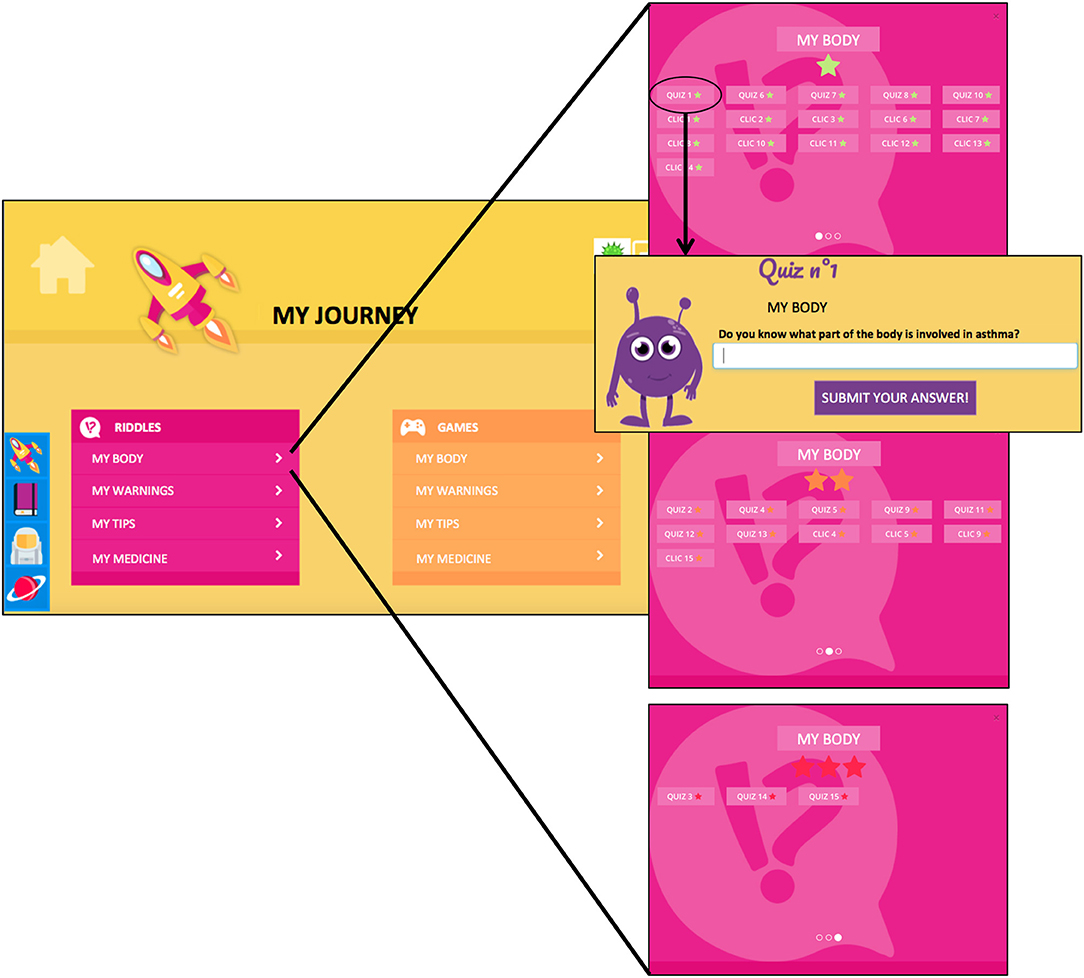
Figure 1. Visualization of the ≪ My Journey ≫ interface in a choice-condition (Left). By clicking on the first theme in Riddles Tab (My Body), learning activities associated were displayed for each level of difficulty (Right), where the first one is a quiz.
KidBreath Contents
Based on pedagogical techniques used in Patient Therapeutic Education workshops (ANAES, 2002; Nguyen et al., 2003) KidBreath prototype is divided into four main units: “My Journey,” “On Discovering the Galaxy,” “My Diary,” and “My profile” (Figure 1).
My Journey (rocket icon): progressive learning units on the four knowledge sub-domains of asthma (general disease knowledge, biomedicine, symptomatology, and treatments) consists of quizzes and MCQ in a “Riddles” tab, and mini-games in the “Games” tab as shown is Figure 1-left. In order to facilitate the interface understanding and usability a dual mode of entry (text and sound) is proposed where online characters read aloud both questions and answers (Figure 1-right). The unit's sub-activities were defined as such: My Body (Biomedicine), My Warnings (Symptoms), My Tips (General disease Knowledge), and My Medicine (Treatments).
Within a learning activity, the system proposed one determined learning process where (1) the character asked questions concerning asthma; (2) the child answered by free recall-questions to be imputed via a keyboard (for quizzes), via multiple-choice questionnaires or via mini-games, with the possibility to confirm or overturn before final validation; and (3) instantaneous feedback was provided to the child through the game. The character indicated the correct answer (correct or incorrect) along with detailed explanations and facts the children ought to know already (the same feedback was used whether the child answered correctly or not to take into account answers provided randomly).
On Discovering the Galaxy (planet icon): discovery animated videos units on asthma, which composed of answers to the questions frequently asked by the children having participated to KidBreath design and everyday-life situations children may encounter, their consequences on asthma regulation and prevention, and how to avoid critical development of asthma.
My Diary (book icon): proposes to keep track of the child's achievements within KidBreath.
My profile (cosmonaut icon): gathers every bit of information concerning the child-user.
From the KidBreath conception, the following field study explored the impact of its usage in asthma children, where main research contributions are an evaluation in real-life setting (use at home) of an asthma-related serious game designed with a PD and therapeutic education pedagogical methods in terms of pedagogical efficacy (knowledge around the illness), pedagogical efficiency (intrinsic motivation during learning), therapeutic efficacy (illness perception and therapeutic adherence during use).
Methods
Participants
We recruited volunteers' asthma families after explained user study. Some families were recruited in the health association where they carried out therapeutic educational programs during workshops, and others were called after they accepted when their practitioner told them the goal of the project (working in the association). Consequently, 14 asthma families were recruited and including 8 males, 6 females, aged from 7 to 11 years. All the children exhibited a moderate asthma severity (i.e., between the stage 2 and 3 out of 4 of asthma severity, with a use of daily background inhaler) according to physicians of health association.
Inclusion and exclusion criteria have been established. First, children participating in the study had to have been born between 2006 and 2010. These years were included because children younger don't know read, and children older are in middle school. Second, they had not to be home schooled, and shall know basic computer uses. Third, in order to avoid bias due to literacy issues, only French-speaking children not suffering from cognitive impairments and having no literacy or numeracy conceptual issues were eligible. Four, as the study took place in three sessions at the children's home, only children participating to all sessions were considered for the study. For this reason, final analyses therefore accounted for 14 control children.
Regarding ethics, all child-related data, the study's protocol and the entire set of data collected during the experimental study were pre-validated and registered with the following ethics comities:
• INRIA's ethics comity for experimental studies on humans (COERLE n°2016-010)6
• CNIL7 user studies database
• The head of office of the departmental administration office for education (SDEN)8
• The director of the public school where the study took place.
Consent forms were also filled by all children and their parents (or guardians) prior to using KidBreath.
Material
For controlling learning path across participants, learning units were displayed in a predefined sequence. The riddles were firstly activated by theme category (Biomedical, Symptoms, General Knowledge, Treatments), in respect of the exercises type (quiz, MCQ), of the difficulty level (1: easy, 2: medium, 3: hard) and of ID number of activity. After the riddles completion, the Games became active by theme category (Biomedical, Symptoms, General Knowledge, Treatments), in respect of the difficulty level (1: easy, 2: medium, 3: hard) and number of activity. Figure 1 illustrated this sequence as if the user completed activities displayed from top to bottom and from left to right.
When the participant pressed the button “next” after the correction, the next activity displayed. They could switch to other units, but if he wanted return to play in “My journey,” the learning activity in progress was also displayed.
Procedure and Measurement
Because KidBreath is a web application available for computers, tablets and smartphones, each child was told to use KidBreath at least 10 min per week over 2 months on their own device, after giving to them URL address and instructions. The study was divided into 3 assessment sessions over a 2-month period: pre-intervention session (initial assessment), post-intervention session after 1-month use of KidBreath (mid-point assessment) and post-intervention session after 2-month (end-point assessment). Between each month (M0.5 and M1.5), participants received by regular mail one questionnaire (i.e., adherence questionnaire) having to-be filled before the next experimenter visit (planned 2 weeks after) (Table 1).
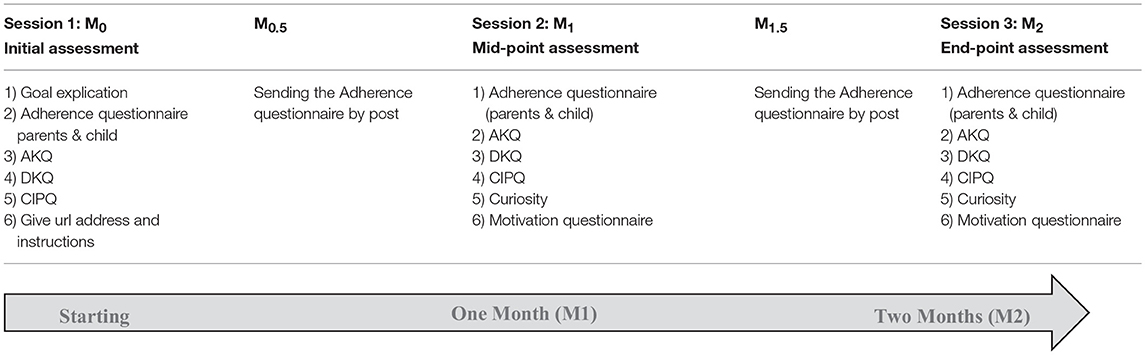
Table 1. Procedure and timeline of assessment sessions of KidBreath.
Pedagogical efficacy measurement
Before and after using KidBreath, the Asthma Knowledge Questionnaire (AKQ) (Al-Motlaq and Sellick, 2011) was completed by all children. This English-speaking (true or false) questionnaire for asthma patients is generally divided into 24 affirmations about asthma. Once translated into French, a third option was added to all queries (“I don't know”) to remove uncertainty about the child's random choice of an answer (Nguyen et al., 2003).
In order to check whether the children's knowledge could be correlated to their own general knowledge or the sole use of KidBreath informative content, children were asked to fill a Diabetes Knowledge Questionnaire (DKQ)9 questionnaire on diabetes. This French-speaking questionnaire was adapted for a better understanding by 8 and 9-year-old children—items 4, 8, 9, 12, and 13 were removed, others were reformulated, the option “I don't know” was included—leaving us with a 10 items single choice questionnaire.
Pedagogical efficiency measurement
The pedagogical efficiency was probed thanks to questionnaires assessing elicited motivation and curiosity, respectively.
–Motivation. To the kind of motivation elicited in children when they use KidBreath. Vallerand's questionnaire (Vallerand et al., 1989, 1992), based on Deci and Ryan's Self-Determination Theory (1985) and commonly used to ascertain the elicitation of intrinsic and extrinsic motivation (e.g., Desrochers et al., 2006) was selected. Once adapted to a public of children users playing a serious game, children had to answer a 21 items questionnaire on their experience during play. Items were visualized by groups of three representing one of the following type of motivation subcomponent:
• Amotivation (AM). The student is amotivated when he doesn't see how the results applied are related to his actions. This shows a lack of motivation.
• Extrinsic Motivation (EM). This kind of motivation is divided into three subcomponents, i.e., External regulation (behavior is regulated through rewards; e.g., passing a grade or a level with honors), Introjection (learner begins to internalize external constraints; e.g., show his smarts to others), and Identification (the chosen ways to achieve external means, such as helping a friend suffering from asthma).
• Intrinsic Motivation (IM) including three subcomponents, i.e., To Know (epistemic need to know and understand, satisfaction of learning for its own sake), Accomplishments (interact with the environment to feel competent, focus on the process of achieving rather than on the outcome), and Feelings (engage in learning to experience stimulating feelings (e.g., sensory pleasure, excitement, fun).
Scores on motivation span from 0 to 3 in each category of items, presented randomly to children as to avoid learning effects.
–Curiosity. Children's level of elicited curiosity were computed by questioning (Gordon et al., 2015): the child was directed to ask as many questions as wishes on a specific topic without the answers being given by the interviewer (Harris, 2012). After using KidBreath children went through this process, asking for additional information on asthma for KidBreath to answer in the future. Scores on curiosity finally range from 0 to the maximum of questions asked.
KidBreath adherence measurement
The KidBreath adherence was probed with a self-made questionnaire. A 4 points Likert scale (score from 0 to 3) was especially self-made for scoring the parents and children's points of views about the system. It was composed of 3 quantitative items: (1) Parents perception of Child engagement at pre-use and post-use of KidBreath: ≪ Do you think your child will be/was cooperative? ≫ (Never/Seldom/Often/More often); (2) Child perception of engagement at pre-use and post-use of KidBreath: ≪ Do you think you will achieve/achieved playing KidBreath weekly for 2 month/since study began? ≫ (Not at all/From time to time/Many times/All the time); (3) Child perception of KidBreath efficacy in pre-use and post-use: ≪ How much do you think KidBreath will help/helped you for better taking your medication, being more careful and having less asthma attacks? ≫ (Not at all/Slightly/Much/Widely).
Therapeutic measurement
It included an assessment of illness perception thanks to Children Illness Perception Questionnaire (CIPQ based on Leventhal's illness representation theory, Leventhal et al., 1984). The CIPQ is a 26-item instrument adapted from the IPQ for adults (Weinman et al., 1996). Like the IPQ, the CIPQ consists of two separate sections: illness beliefs, where the overall score represents the degree to which the illness is perceived as threatening, and children's beliefs regarding the causal aspects of their condition. According to Weinman, Petrie, Sharpe, and Walker, the causality items were not to be regarded as a subscale, so analyses were undertaken only on the first section (Weinman et al., 2000).
Table below summarizes the experimental procedure and timeline of assessment sessions and their content.
Statistical Analyses
All data analyses were performed on IBM SPSS Statistics 20. A significance level of 0.05 was used throughout the analysis process.
Descriptive statistics were computed from raw scores on each questionnaire for each participant. For any mean comparison, the variance equality was checked for performing parametric statistics.
Regarding pedagogical efficacy, results were treated in two steps for catching the short-term effects of KidBreath (initial assessment vs. mid-point assessment) and its long-term effect (initial assessment vs. end-point assessment). For each step, KidBreath's pedagogical efficacy was evaluated using a two-way mixed ANOVA [Time x Disease questionnaire] with pre-post intervention effect on children's AKQ and DKQ scores. Complementary analyses were performed using an independent t-test with pre-post intervention effect for both disease questionnaires. Correlations were performed in order to highlight any possible association between learning gain and scores in pre-use or post-use.
Concerning pedagogical efficiency, KidBreath's effect on motivation was measured according to the results of the Motivation questionnaire [two-way repeated ANOVA with Motivation type (AM vs. EM vs. IM) and Time (M1 vs. M2) as independent variables)]. Curiosity scores were also compared between mid-and end-point assessments as another efficiency measure.
Correlations were performed in order to highlight any possible association between pedagogical efficacy and efficiency measures on the following set of variables: measures associated to asthma-related knowledge (learning-gains scores) and measures associated to elicited motivation scores.
Finally, one-way repeated ANOVAs (Time) were applied on CIPQ scores and those from the KidBreath adherence questionnaire. To complete quantitative data, we added most frequent verbatim reported by parents during interviews.
Results
Pedagogical Efficacy
Individual scores across time
Figures 2A, 3A illustrate the distribution of pre- and post- use learning scores on the AKQ and DKQ questionnaires when coupled with the following relative learning gains [(post-use score – pre-use score) / (post-use score + pre-use score)].
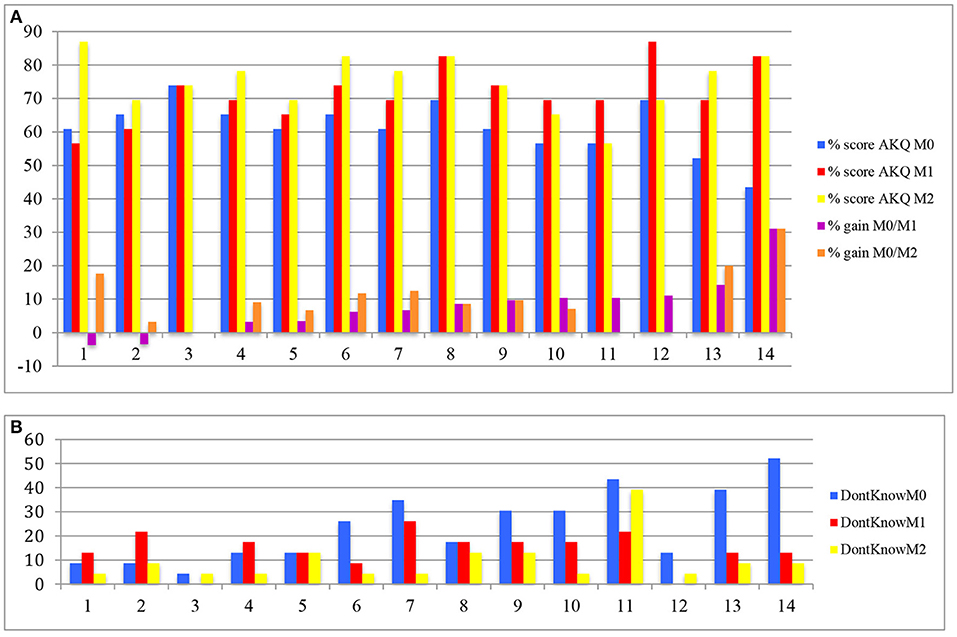
Figure 2. (A) Child's performance (percentage) for AKQ in M0 (pre-use), M1 (mid-point assessment), M2 (end-point assessment) and relative learning gains. (B) Child's performance (percentage) for “I don't know” answers in AKQ for M0 (pre-use), M1 (mid-point assessment), M2 (end-point assessment).
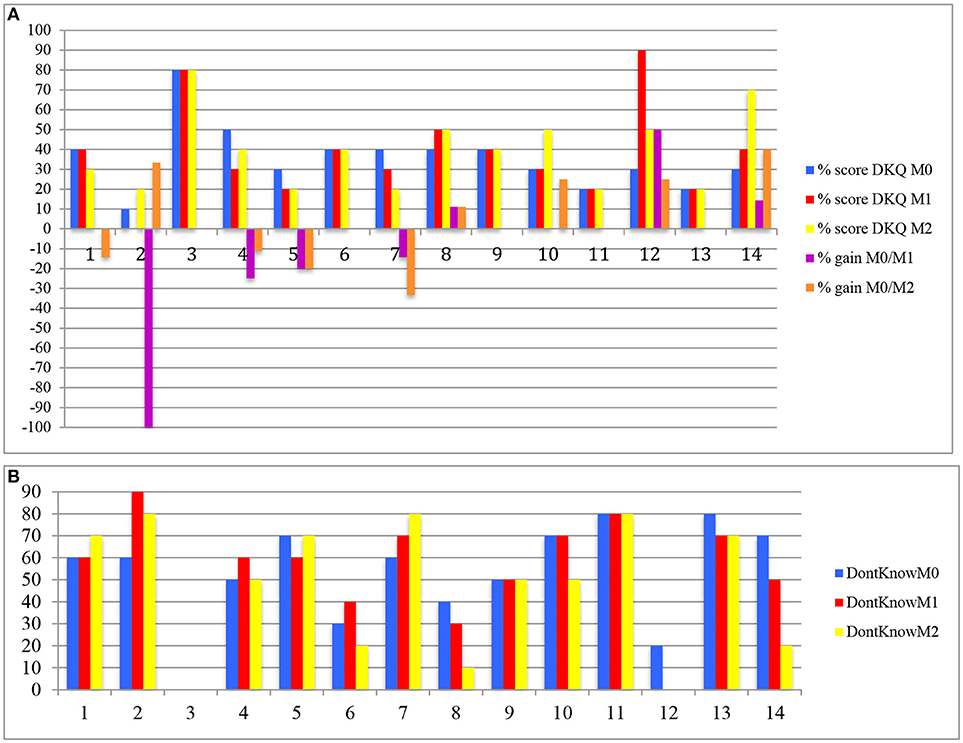
Figure 3. (A) Child's performance (percentage) for DKQ in M0 (pre-use), M1 (mid-point assessment), M2 (end-point assessment) and relative learning gains. (B) “Child's performance (percentage) for I don't know” answers in DKQ for M0 (pre-use), M1 (mid-point assessment), M2 (end-point assessment).
In Figure 2A, learning gains gathered in M1 session are ranked from lowest to highest. A negative correlation was found between the pre-use AKQ scores and the associated relative learning gains (r = −0.70; p = 0.005). Thus, children who knew the least about asthma before using KidBreath benefited the most in terms of asthma-related knowledge gained.
Complementary analyses were carried out to check if children answered in a random way, or if they knew they did not know asthma knowledge by choosing “I don't know” as an answer on both questionnaires (Figure 2B). A positive correlation was found between the pre-use “I don't know” scores in AKQ and the associated relative learning gains (r = 0.82; p < 0.001). This indicates that children who knew the less about asthma were honest from the beginning and they did not answer randomly.
Concerning DKQ, Figure 3A was ranked according to children results on the AKQ in order to visualize whether the high-ranking children from Figure 2A were also present in the high rankings of Figure 3A.
There was no correlation between the gain of knowledge on asthma and diabetes learning scores. This indicates that learning curves for asthma and for diabetes did not share relationships, as expected.
As also expected, results from DKQ scores were associated to a high random answer behaviors irrespective of assessment session conditions. Complementary analyses about “I don't know” answers in DKQ didn't show difference between the M0 (52.8%), M1 (52.1%), and M2 (46.4%) sessions, which supported the no learning-gain for the diabetes knowledge (Figure 3B).
Short-term effect of KidBreath (M0 vs. M1)
A two-way mixed ANOVA [2 (time: M0 vs. M1) x 2 (questionnaire: AKQ vs. DKQ)] only revealed questionnaire effect [F(1,13) = 59.21; p < 0.0001; η2 = 0.820] indicating that a majority of children showed better score on asthma (61.5%) than on diabetes (35.7%) questionnaire. Although the time effect as well as Time x Questionnaire effect didn't reach the significance (respectively, p > 0.08; p > 0.100), a time-related increase of AKQ score was observed on AKQ score [t(13) = 3.49; p = 0.004], but not for DKQ score (p > 0.600) (Figure 4A).
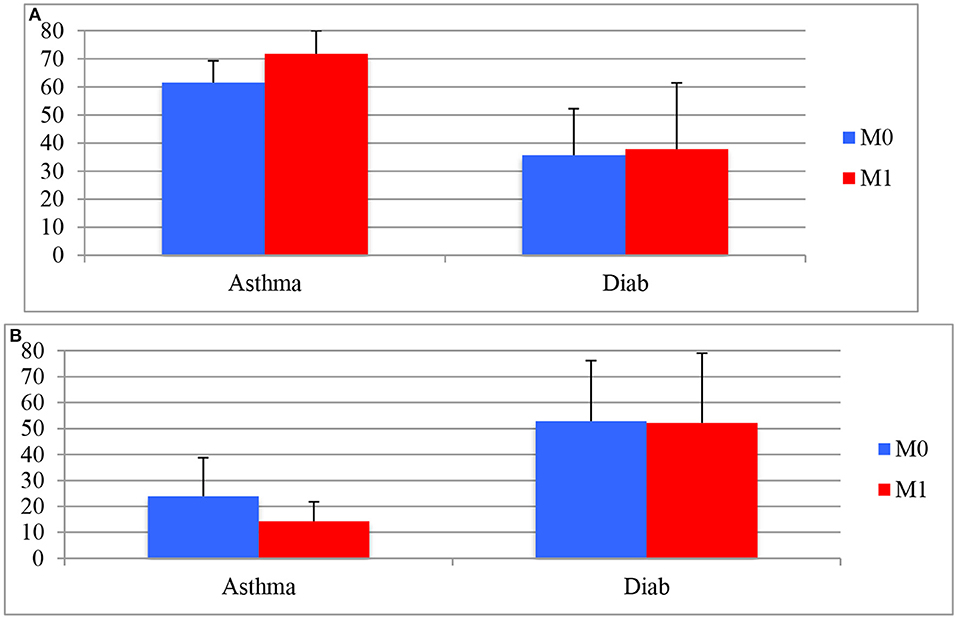
Figure 4. (A) Means and standard deviation for AKQ and DKQ score as a function of time (pre- vs. M1 post-use). (B) Means and standard deviation of children's “I don't know” answers for AKQ and DKQ as a function of time (pre- vs. M1 post-use).
According to “I don't know” answers in AKQ and DKQ (Figure 4B), a two-way mixed ANOVA [2 (time: M0 vs. M1) x 2 (questionnaire: AKQ vs. DKQ)] showed questionnaire effect [F(1,13) = 43.42; p < 0.0001; η2 = 0.770] and interaction effect [F(1,13) = 7.12; p < 0.02; η2 = 0.354], but no time effect was found (p > 0.100). Pairwise comparisons only revealed a significant time-related decrease of “I don't know” answers in AKQ (23.9 vs. 14.3%) [t(13) = 2.60; p < 0.03] (Figure 4B).
Overall results from mid-point assessment indicated both children enhanced their asthma knowledge after using KidBreath and they gained confidence in their answers.
Long-term effect of KidBreath (M0 vs. M2)
A two-way mixed ANOVA [2 (time: M0 vs. M2) x 2 (questionnaire: AKQ vs. DKQ)] showed over a 2-month period a significant questionnaire effect [F(1,13) = 62.20; p < 0.0001; η2 = 0.827], a time effect [F(1,13) = 9.24; p < 0.01; η2 = 0.416] and an interaction effect [F(1,13) = 4.39; p = 0.05; η2 = 0.253] (Figure 5A). Thus, all the children clearly exhibited greater performance over 2-month period for AKQ scores than in DKQ scores.
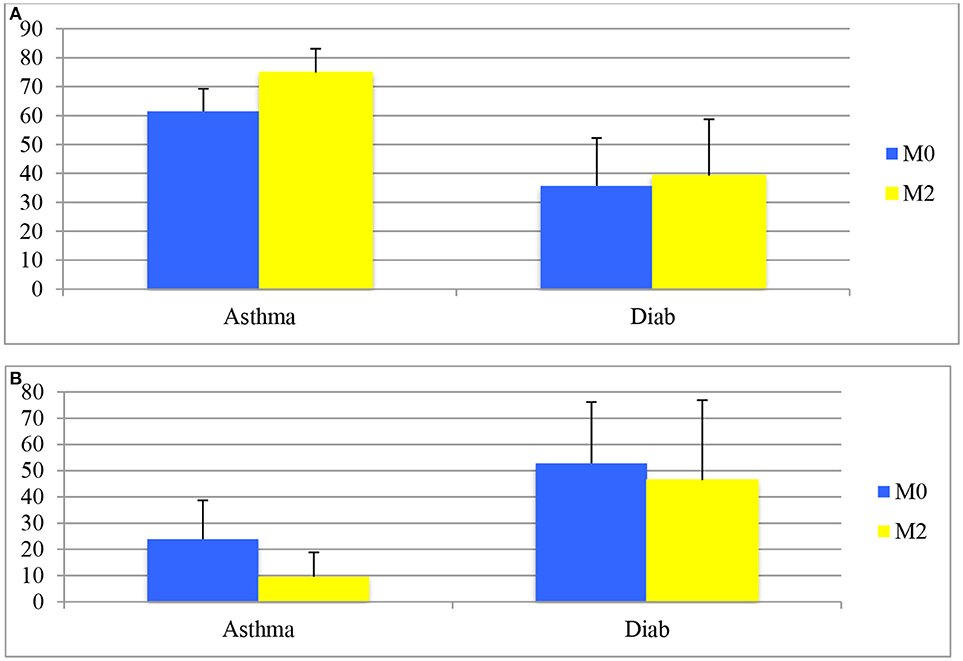
Figure 5. (A) Means and standard deviation of children's pre- and M2 post-use questionnaires (AKQ and DKQ). (B) Means and standard deviation of children's “I don't know” answers pre- and M2 post-use questionnaires (AKQ and DKQ).
To check if children answered in random way, a two-way mixed ANOVA [2 (time: M0 vs. M2) x 2 (questionnaire: AKQ vs. DKQ)] showed a questionnaire effect [F(1,13) = 29.40; p < 0.0001; η2 = 0.693] and time effect [F(1,13) = 7.48; p < 0.02; η2 = 0.365], but no interaction effect (p > 0.100) (Figure 5B). Pairwise comparisons revealed a significant decrease of “I don't know” answers in AKQ across the time conditions (23.9 vs. 9.6%) [t(13) = 3.82; p = 0.002] but not for DKQ scores (p > 0.200).
Overall results from end-point assessment indicated both children clearly increased their asthma knowledge after using KidBreath and they were more confident in their answers.
Pedagogical Efficiency
For motivation scores, a two-way mixed ANOVA [2 (time: M1 vs. M2) x 3 (motivation type: AM vs. EM vs. IM)] showed a significant motivation effect [F(2,26) = 27.35; p < 0.0001;η2 = 0.855] but neither time effect (p > 0.600) nor interaction effect (p > 0.300) were found. Pairwise comparisons revealed this effect was in the favor of the IM condition regardless the time period [M1: tIM vs. AM(13) = 5.25; p < 0.0001; tIM vs. EM(13) = 5.92; p < 0.0001; tEM vs. AM(13) = 2.98; p = 0.011; M2: tIMvs.AM(13) = 4.46; p = 0.001; tIMvs.EM(13) = 8.72; p < .0001], which revealed an intrinsic motivation was generated during KidBreath's use across the 2-month use (Table 2).
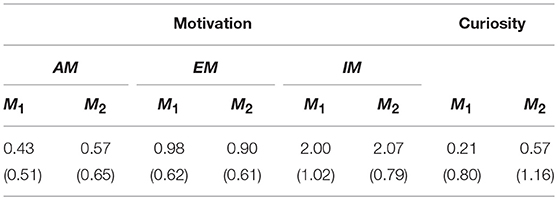
Table 2. Means (standard deviation) scores on Motivation and Curiosity measures (N = 14).
To complete pedagogical efficiency with the curiosity indicator scores, one-way repeated ANOVA [2 (time)] revealed a significant increase of questions asked from the mid-point to the end-point time session [F(1,13) = 4.45; p = 0.05; η2 = 0.255], revealing an increased interest in learning further with the serious game.
Relationship Between Pedagogical Efficacy and Efficiency Measures
In order to explore any possible association between learning gains across time, and the type of motivation elicited during play, we have examined the correlations between the different measures.
First, a significant correlation was found between AMM0−M1 scores and learning gainsM0−M1 (r = −0.62; p < 0.02), which indicates that the children who learned the most from software use at mid-point were those who were the less amotivated.
Second, the EMM1−M2 scores was negatively correlated with both the learning gain M0−M2 (r = −0.53; p = 0.05), and learning gains M1−M2 (r = −0.62; p < 0.02), revealing that the children who learned the most from software use in long-term were those who were the less extrinsically motivated, especially for reward expectation.
KidBreath Adherence and Therapeutic Effects
For child engagement measures (Table 3), pairwise comparisons revealed a significant decrease across long-term study, and more specifically from the mid-point to the end-point time session. This lost engagement indicated a dropout behavior from the second mid-point of the study. Similar results were observed for parents' reports. These observations pinpointed their honesty relative to the KidBreath experience.
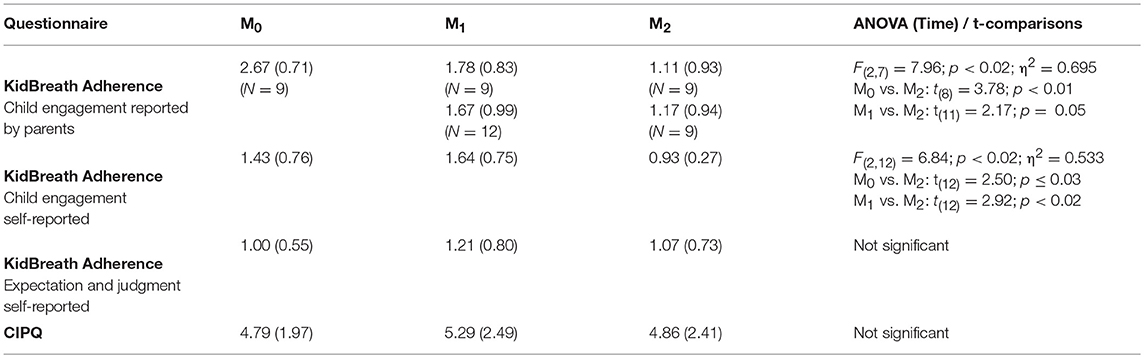
Table 3. Means (standard deviation) scores on therapeutic adherence measures (N = 14).
Also, time effect didn't reach the significance for KidBreath-related expectation and judgment score as well as for IPQ scores.
To complete quantitative measures, qualitative data were transcribed during user tests interviews in the 3 sessions (Table 4).
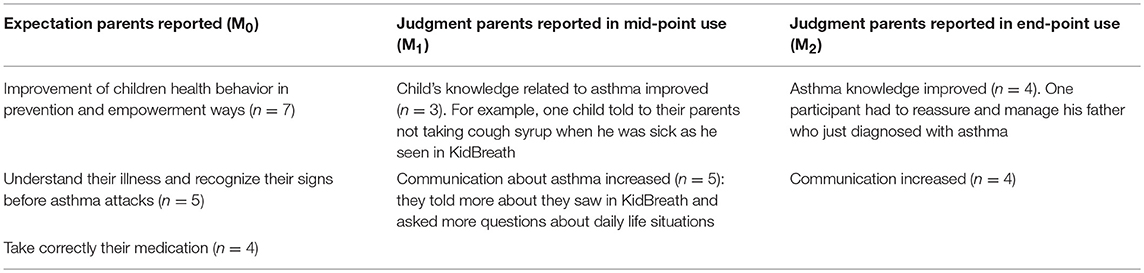
Table 4. Most frequent expectations reported by parents during interviews in pre-use, and judgment about system utility in mid-point and end-point sessions.
Discussion
The main results from study 1 are now discussed in terms of pedagogical efficacy, pedagogical efficiency, KidBreath adherence, and therapeutic effect.
Regarding short-term and long-term pedagogical efficacy, 79% of the children showed a significant improvement in learning gains on asthma knowledge score after post-using of KidBreath. For these children, results show a better general knowledge about asthma, and a significantly higher learning gain for asthma than for diabetes—the other chronic illness questionnaire used as control condition. Similar results were found in our previous study with non-asthma children (82%) (Delmas et al., 2018).
The significant decrease of “I don't know” answers across assessment sessions comforted the fact that both children learnt more after using KidBreath and that they did not answer it randomly. Pedagogical efficacy was also supported by the negative correlation between learning gains and asthma general knowledge—scores calculated from the answers to the AKQ pre-use questionnaire. This points out that the tool's use benefitted more to children who initially knew less about the illness. This is reinforced by the negative correlation found between learning gains and children expectation in adherence measurement (r = −0.61; p = 0.02), where the tool's use benefitted more for children who not only initially knew less about the illness, but also expected the less about the system to help them for better managing asthma. To check if children didn't answer in a random way, the positive correlation with the answer “I don't know” in AKQ pre-use and the associated relative learning gains showed the tool's use benefitted more to children who were the most aware about their lack of the knowledge asthma-related, i.e., who knew it is in their interest to use KidBreath.
The achieved performance on AKQ at mid- and end-points were similar (M1 = 71.7%; M2 = 74.8%) revealing that the asthma-related knowledge was maintained across sessions. Indeed, although young patients completed different questions, the correction component explained most of the time via similar information “blocks” essential to understand for better managing asthma. Hence, children often learned similar information, as up-to-date knowledge, which can explain why the AKQ scores were maintained over time. Although learning activities were imposed in predefined sequences defined by the research team, these near and far results showed KidBreath use triggered strong pedagogical efficacy for learning asthma.
Concerning pedagogical efficiency, a focus was made on identifying which type of motivation (AM, EM, or IM) such a learning tool could generate. This information is essential to guaranty a continued use of the tool in the short to medium term. Mostly used in education (Vallerand et al., 1997), it is rarely used in the development of TEL devices (Cordova and Lepper, 1996), and no mention of its use was made in current serious games. After 1 month-use, a strong intrinsic motivation was scored compared with the others, which matches with our expectations in the previous study (Delmas et al., 2018). Furthermore, the intrinsic motivation stayed constant over the 2-month period and significantly higher than the extrinsic motivation and amotivation. The “ceiling” effect recorded in the end-point for asthma-related knowledge and for intrinsic motivation was found in similar studies carried out on serious games (Brown et al., 1997; Rikkers-Mutsaerts et al., 2012). Indeed, the first month matches with the “discovery” step, where all activities bring enjoyment because of the novelty aspect, but this effect was attenuated in long-term use. This tendency is supported in children playing with a serious game. In an interesting way, the curiosity indicator revealed a significant increase of asthma-related questions asked between the mid- and the end-point assessment time, suggesting some interest in learning further with the serious game.
Concerning therapeutic effect, there is no effect in short or long-term on illness perception. Among the possible explanation ways, two main ones can be advanced. First, a 2-months intervention is not long enough for a deep change in disease perceptions. It is well-known that illness beliefs are resilient and only long-term interventions are able to durably change disease representations of person (Chan et al., 2007; Bindels et al., 2008; Rikkers-Mutsaerts et al., 2012). Second, the age of some children could explain this absence of effect. Indeed, 6 children were born in 2006 (11 years) and 2007 (10 years), which matches the pre-teens period and all the major issues arising for coping, with a strong denial of the disease (de Benedictis and Bush, 2007).
A similar result to the therapeutic effect was found for judgment system efficacy in disease self-management (KidBreath adherence questionnaire). To support the denial hypothesis for coping explained above, most of the children were recruited in the health education association and by pediatrician who worked in this structure, so children initially had some knowledge units. Moreover, this study was composed of children with mild-asthma, so they didn't need to apply information learnt in daily-life situations. Probably, the impact of KidBreath on asthma self-management could be increased in children with severe asthma. Therefore, initial asthma knowledge exhibited by children could be a critical factor for the KidBreath adherence, and then its impact.
The significant decrease of the children cooperation in KidBreath use reported by the parents or themselves between M1 and M2 sessions showed a progressive disinterest with time. Once again, initial asthma knowledge in children could be a critical factor for KidBreath use on the long term. Moreover, real-life situations such as family constraints, hospitalizations and parent's implication could also increase KidBreath dropout. For example, participants told us a lack of time for weekly playing KidBreath due to extra-curricular activities, holidays and the homework. However, verbatim also indicated an improvement of child—parent communication on asthma, which is the first step for better managing asthma (Lieberman, 2001). It could be interesting to study the disease-management benefits from the addition of a learning component for parents in KidBreath.
Overall results lead us to develop personalization features into the learning process provided by KidBreath as a way of its improvement. As we noted several times, the variety of children's prior knowledge on asthma could be a key factor for adhering to KidBreath activities, and then supply an actual benefit. Each learner has an initial set of knowledge and skills, and their own learning rate. ITSs were created in the TEL community with optimized learning algorithms offering beneficial personalized learning experiences to students. The study 2 proposed to explore such an improvement of KidBreath.
Study 2: Exploring ITS for Augmenting KidBreath
Related Work
The current advances of learning and teaching technologies have the potential to improve education accessibility and personalization (Dunlosky et al., 2013; Roediger, 2013). ITS have been proposed for these goals, and as a way to provide useful objective metrics on learning (Anderson et al., 1995). One of the most important goals of an ITS is to provide feedback tailored to the learner unique need.
Recently, ITS were implemented in health context such as training medical students in Integrated Management of the Childhood Illness (ICMI) strategy (Muñoz et al., 2010), and for medical problem-based learning in the area of head injury diagnosis (Suebnukarn and Haddawy, 2004); for population gist comprehension of topics relevant to decisions about BRCA (BReast CAncer genes) testing (Wolfe et al., 2015).
One of the main aspects of ITS is to be able to identify the current level of students and how to address particular difficulties in the student learning process. The goal is to be able to choose online the activity that better addresses the challenges being encountered by each particular student. Even two students with the same knowledge will require different activities to progress further due to their previous experience, cognitive skills or preferences. This is a difficult challenge because as ITSs are encountering the students for the first time, it is difficult to know what is the impact of each activity on their progress. There are several approaches to automatically choose exercises based on the current knowledge level of students. We are here particularly interested in optimization methods that rely on minimal prior assumptions about the students or the knowledge domain.
One option already explored is the use of a partial-observable Markov decision process (POMDP) (Rafferty et al., 2011). PODMPs offer an appealing theoretical framework that guarantees an optimal long-term solution for a planning problem. However, in general, as the computational complexity is high, it is practically impossible to find an exact solution to the problem. Some approximate solutions in the domain of ITS have considered the use of aggregations of states instead of tracking the full knowledge components. Another drawback is that POMDPs require a precise student model for which the policy is optimized. If the real student encountered deviates from this model, then the optimality properties are lost.
As noted, before optimizing the sequence of exercises it is important to have some knowledge about the impact of a given exercise in the learning of the KCs, and also to be able to track what each student already masters. A large part of ITS research has been on the modeling aspects of the cognitive and student models. A seminal work on this topic was the Knowledge Tracing framework (Corbett and Anderson, 1994) which builds a detailed cognitive model of the student, of its learning processes by considering a set of independent KCs, the probability of learning them and the probability of correct or wrong answer in exercises that relies on those KCs. More recent methods extend this framework to a Bayesian probabilistic approach (Villano, 1992; Chang et al., 2006) improving the performance and understanding of those methods. Recent methods have started to consider how to learn such models, and variants of it, allowing to simultaneously discover the relation between activities and KC (e.g., Cen et al., 2006; Baker et al., 2008; González-Brenes and Mostow, 2012; González-Brenes et al., 2014).
A more recent approach is to use the Multi-Arm Bandit (MAB) framework (Auer et al., 2002) to manage pedagogical activities (Clement et al., 2015). MABs have the advantage of being extremely computationally efficient and rely on very weak student models. The main drawback is that there is no long-term planning of the best sequence of activities relying on an exploration-exploitation tradeoff to find the best path. Aware of such problem, authors of one such algorithm considered that standard MAB needs to be complemented with a weakly specified knowledge/activity graph to provide a long-term view on the optimization (Clement et al., 2015).
In this work, they developed and tested a set of experiment in simulation to tailor hyperparameters of the algorithm implemented, named ZPDES (Zone of Proximal Development and Empirical Success) and with 400 students to see the impact in a real controlled environment. They showed their method was efficient to personalize and adapt pedagogical content depending of the student progression. Indeed, the students were able to do more different activities and reached them faster with the algorithms than with a predefined sequence defined by a pedagogical expert. As this ITS has been successful, its integration into KidBreath is appeared as a relevant improvement way for providing an automatized personalization.
To test the ITS-augmented KidBreath, it was experimented on similar population (asthma children aged from 8 to 12) and with similar assessment procedure (pedagogical efficacy, efficiency, KidBreath adherence and therapeutic effect) than in study 1.
Material (Details in the Supplementary Material, Appendix 2)
To manage activities, ZPDES combines three things. It uses a hierarchical structure of multiple layers of MABs to explore an activity graph. An activate/deactivate mechanism is present to manage the Zone of Proximal Development explore by the MAB for activities presenting multiple difficulty levels. And an evaluation of the learning progress is used to exploit the activities presenting the best learning interest for the user.
Figure 6 shows the formal description of ZPDES in the algorithm 1 and also how ZPDES works for KidBreath on the diagram. There are three layers in the MAB hierarchy for KidBreath: Theme—Theme's level—Type. The Zone of Proximal Development is represented with yellow outline grouping the active activities.
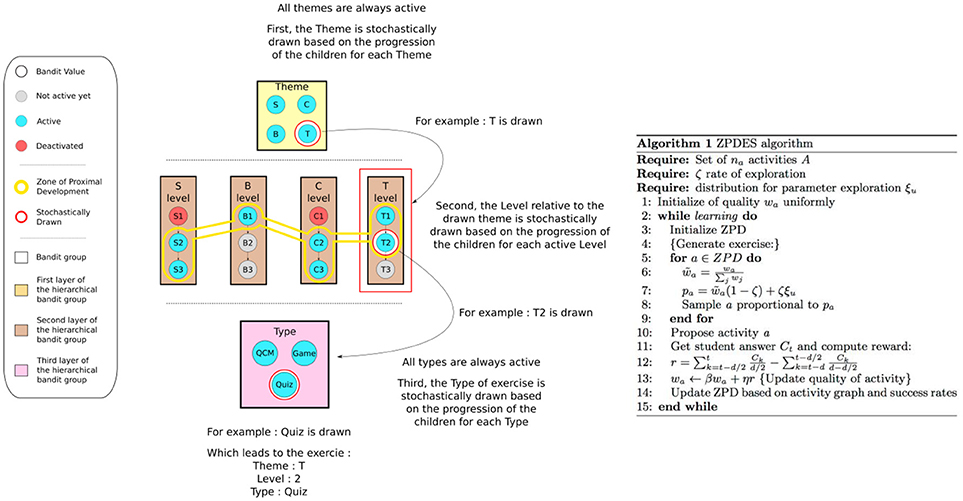
Figure 6. ZPDES exploration of a KidBreath activity graph.
First, the main MAB draws the theme for the next exercise proportionally to the learning progress the student has for each theme. All the Themes are always active, there is no difficulty relation between them and they are all interesting from the start. Each Theme's interest evolves for each children depending of his learning progress for each Theme. For example, in the figure, the Theme T is drawn.
Second, the difficulty Level relative to the theme previously picked is then drawn by active activities. Here, only Level 1 and 2 are active for the theme T. The Level will be stochastically drawn depending of the current learning progress of the children for each Level. In the example, the Level 2 for the Theme T is drawn.
Third, the Type of activity is drawn. As for the Theme, all the Types are always active, there is no difficulty relation between them and all the types are interesting from the start to the end. Also depending of the student learning progress for each Type, each Type's interest will evolve. In this example, the Type Quiz is drawn which leads to the exercise: Theme T; Level 2; Type Quiz.
The ZPDES algorithm was implemented in the “My journey” unit of KidBreath. Therefore, the improved KidBreath version is unchanged except for this learning unit. Precisely, in “My journey,” the framework within a learning activity didn't change, but the only difference was in the display sequence of learning activities in “My journey,” which take into account answers provided by children in quiz, MCQ or games to go to the next activity, thanks to the integration of ZPDES algorithm. As in the previous study, the child could switch to other units, but if they wanted to return to play in “My journey,” the learning activity in progress was also displayed and they had to complete it to go to the next one.
Method
The method used was very close to the one used for the study 1. So, next sections document differences between the two studies rather than similarities.
Participants
Table 5, below, summarizes participants' characteristics, inclusion and exclusion criteria, and ethics procedures comparatively to study 1.

Table 5. Summary of participant recruitment procedure.
Procedure, Measures, and Statistics
Procedure, measures and statistics were similar to those of study 1 (in section Procedure and Measurement).
Due to exploring purposes, only the experiment duration is different because it was stopped over 1-month period.
Regarding measurement, log interaction measures were added to probe the total gaming duration and the learning paths for each participant in the “Riddles” subunit according to children's identification of connection, dates and times of when they began and ended each activity. As already evoked in the design section each activity could be identified by its theme and level of difficulty.
Results
Pedagogical Efficacy
Individual scores across time
In Figure 7A, learning gains gathered in post session (i.e., over 1-month period—M1–) are ranked from lowest to highest. A negative correlation was found between the pre-use AKQ scores and the associated relative learning gains (r = −0.754; p < 0.0001). Once again, children who knew the least about asthma before using KidBreath benefited the most in terms of asthma-related knowledge gained.
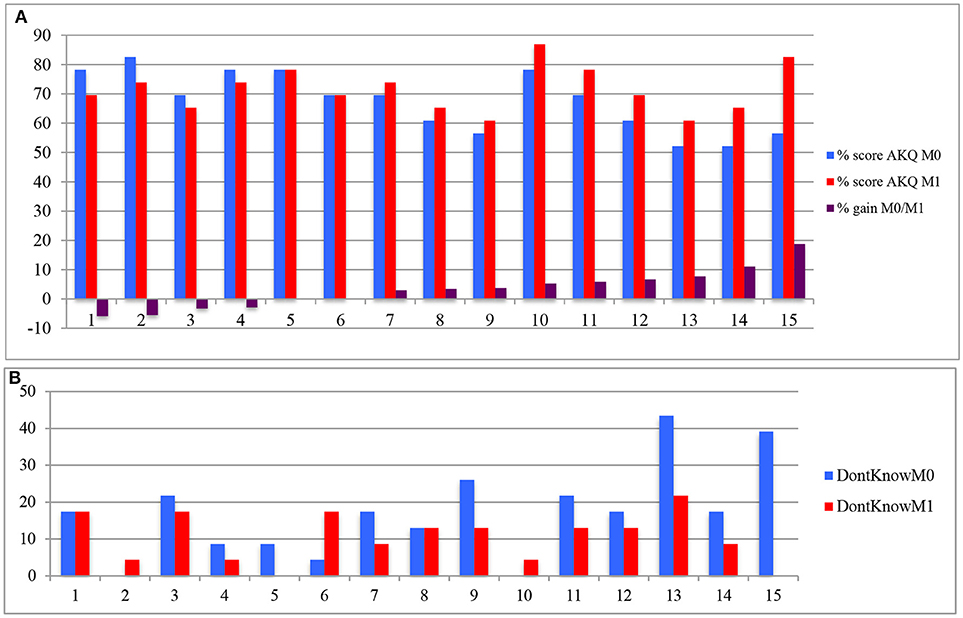
Figure 7. (A) Child's performance (percentage) for AKQ in M0 (pre-use), M1 (mid-point assessment), and relative learning gains. (B) Child's performance (percentage) for I don't know” answers in AKQ for M0 (pre-use) and M1 (mid-point assessment).
A positive correlation was found between the pre-use “I don't know” scores in AKQ (Figure 7B) and the associated relative learning gains (r = 0.607; p = 0.016). Once again, children who knew the least about asthma were honest from the beginning, they did not answer randomly, and it was people who benefited the most in terms of asthma-related knowledge gained.
Concerning DKQ, Figure 8A was ranked according to children results on the AKQ questionnaire in order to visualize whether the high-ranking children from Figure 7A are also present in the high rankings of Figure 9A.
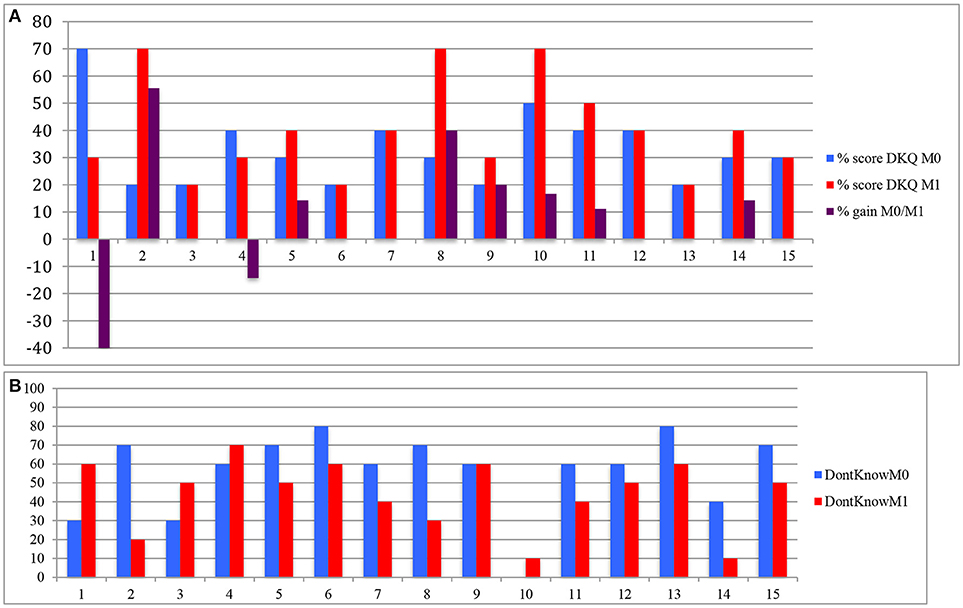
Figure 8. (A) Child's performance (percentage) for I don't know” answers in DKQ in M0 (pre-use), M1 (mid-point assessment), and relative learning gains. (B) Child's performance (percentage) for I don't know” answers in AKQ for M0 (pre-use) and M1 (mid-point assessment).
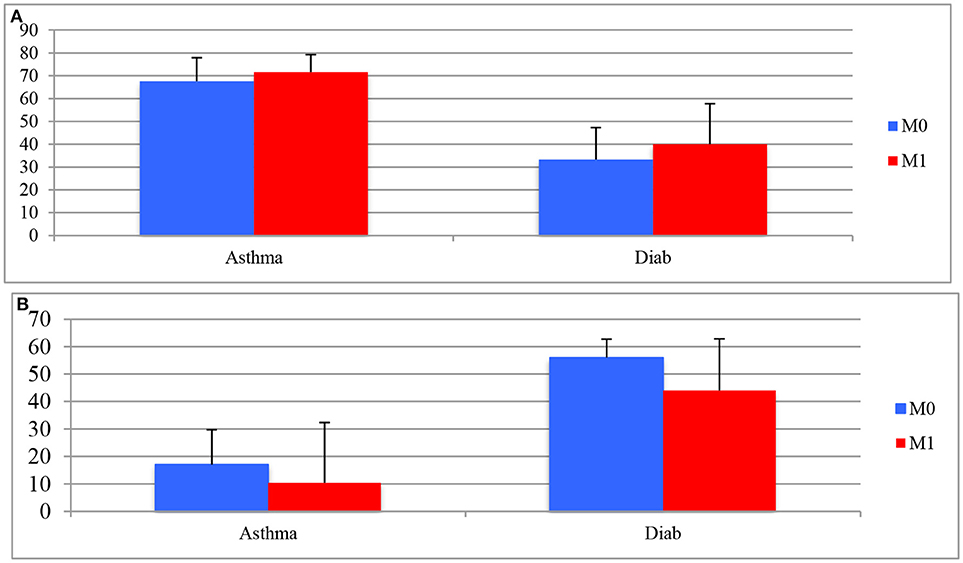
Figure 9. (A) Means and standard deviation for AKQ and DKQ score as a function of time (pre- vs. M1 post-use). (B) Means and standard deviation of children's “I don't know” answers for AKQ and DKQ as a function of time (pre- vs. M1 post-use).
As for study 1, there was no correlation between the gain of knowledge on asthma and diabetes learning scores. This indicates that children who learnt about asthma didn't learn about diabetes. As their general knowledge about one illness or the other ought to have been of similar level, results from DKQ scores were associated to random answers (Figure 8B).
Short-term effect of ITS-based KidBreath (M0 vs. M1)
A two-way mixed ANOVA [2 (time) x 2 (questionnaire)] replicated a significant questionnaire effect [F(1,14) = 155.43; p < 0.0001; η2 = 0.917] and the absence of both pre-post effect (p = 0.092) and interaction effect (p = 0.653) (Figure 9A). Pairwise comparisons didn't reach the significance (p > 0.09). Therefore, all the children exhibited greater performance for AKQ scores than for DKQ scores and, they performed in post-evaluation (M1) as well as in pre-evaluation.
According to “I don't know” answers in AKQ and DKQ (Figure 9B), a two-way mixed ANOVA [2 (time) x 2 (questionnaire-“I don't know”)] showed questionnaire effect [F(1,14) = 78.04; p < 0.0001; η2 = 0.848] and pre-post effect [F(1,14) = 7.73; p < 0.02; η2 = 0.356], but no interaction effect was found (p = 0.412). Pairwise comparisons revealed a significant decrease of “I don't know” answers in AKQ between the two sessions (17.1 vs. 10.4%) [t(14) = 2.12; p = 0.05]. Similar trend was found with “I don't know” answers in DKQ [t(14) = 2.10; p = 0.05]. This indicates both children learned more after 1 month using KidBreath and they were more confident in their answers regardless of the type of disease knowledge questionnaires.
Pedagogical Efficiency
Concerning motivation scores, a one-way repeated ANOVA [3 (motivation type)] again showed a significant motivation effect [F(2,13) = 8.21; p < 0.01; η2 = 0.558]. Pairwise comparisons revealed that this effect was in favor of the IM condition in short-term [tIMvs.AM(14) = 3.98; p = 0.001; tIMvs.EM(14) = 4.04; p = 0.001; tEMvs.AM(14) = 2.92; p = 0.01), which revealed that an intrinsic motivation was generated during KidBreath's use (Table 6).
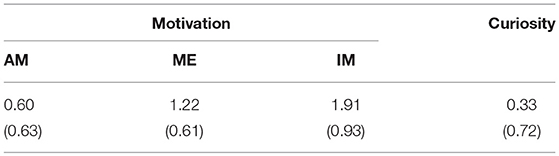
Table 6. Means (standard deviation) scores on Motivation, and Curiosity at M1.
The curiosity indicator showed one third of the children asked information about asthma, revealing some interest in learning further with the serious game.
Relationship Between Pedagogical Efficacy and Efficiency Measures
A significant correlation was found between AKQ post-use score and the intrinsic motivation mean score (r = 0.74; p < 0.01), which indicates that the most intrinsically motivated children were those who knew the most about asthma knowledge after using KidBreath over a 1-month period.
More specifically, the IM—feelings subscale score was positively correlated with AKQ post-use score (r = 0.80; p < 0.0001), which is the most internalized motivation in the Motivation questionnaire—where children do the activity for the feeling (provided itself). It reveals that children who knew the most about asthma knowledge were those who were intrinsically motivated for the pleasure of playing with KidBreath.
KidBreath Adherence and Therapeutic Effect
A one-way repeated ANOVA [2 (time)] is done for CIPQ scores and showed no significant effect (p = 0.363) (albeit a slight decrease after 1-month use) (Table 7).
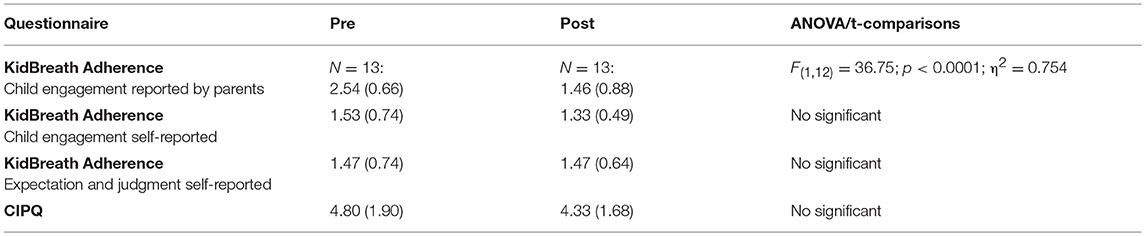
Table 7. Means (standard deviation) scores on scores therapeutic adherence-related (N = 15).
A one-way repeated ANOVA [2 (time)] on child engagement reported by parents score showed a decrease, revealing children neglected the tool use progressively, according to parents' point of view. This trend was also significant by adding questionnaire which be mailed in mid-point study over 1-month period (i.e., after 2 weeks) [n = 11; F(2,9) = 13.34; p < 0.01;η2 = 0.748].
The same analysis failed to show significant difference about child engagement self-reported, even if there is also a decrease (p > 0.200).
Finally, concerning the system expectation about therapeutic adherence and judgment over 1 month-period, results were the same in pre- and post-conditions. This trend showed KidBreath fulfilled the expectations after using it 1 month.
Qualitative data were transcribed during user tests interviews in the 2 sessions (Table 8).
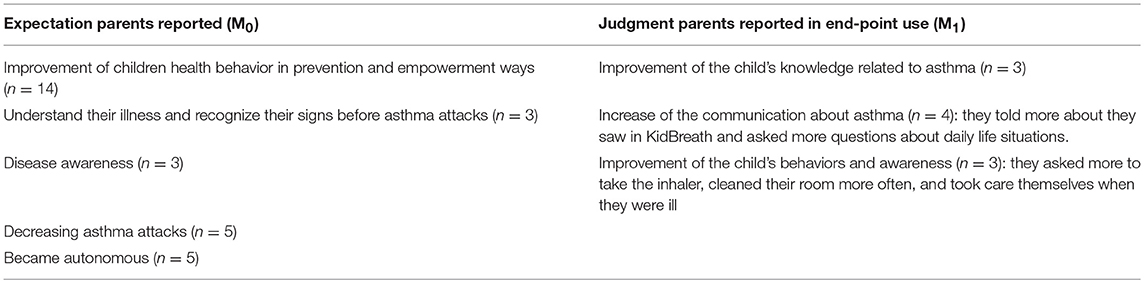
Table 8. Most frequent expectations reported by parents during interviews in pre-use, and judgment about system utility in mid-point and end-point sessions.
Sequence-Exploring KidBreath
Regarding the total time spent to play KidBreath, children fulfilled less learning activities than those in study 1. Indeed, significant differences in log time recorded were found [(mstudy1 = 3312” vs. mstudy2 = 1424”); (t(29) = 3.267; p < 0.05)].
Regarding KidBreath exploration strategies, the learning paths of children were analyzed using Circos (Krzywinski et al., 2009). This software allows, when informed by KidBreath's session logs, to visualize interface transitions (when users change activity within KidBreath) and to produce a graphical output summarizing the different behaviors observed in the form of curved red et blue lines (see Figure 10). One transition begins on the yellow part of an activity label and ends on the brown part of another activity label. Each line's thickness corresponds to the number of children who selected this transition in their learning strategy. Time is also represented on the graphical output, with pale colors matching the most recent activities. This visual display was used to follow children's “journey” while playing on KidBreath.
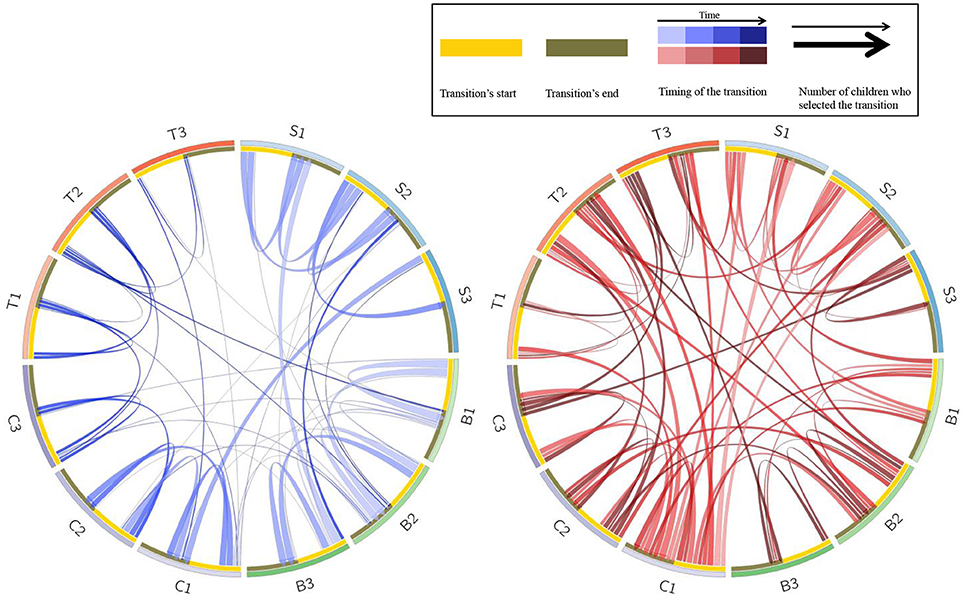
Figure 10. Circos graphical output of activity transitions with the predefined sequence presented in study 1 (left/blue: n = 14) and with ZPDES algorithm (right/red: n = 15).
As previously explained, learning activities were coded according to their theme [My Body (B), My Warnings (S), My Tips (C), and My Medicine (T)] and level of difficulty (from 1: easy to 3: hard). Activity B1 therefore corresponds here to the level 1 biomedical activity within the “My Body” sub-units.
In the blue Circos, learning paths (by each participant) in the study 1 were plotted. Due to predefined sequence condition—defined by the research team—, they were very homogenous. Indeed, linear transitions between first B1 B2B3 (curved lines lighter), then S1S2S3, C1C2C3 and T1T2T3 (darker) were noticeable. The internal transitions matched with the game component, which was carried out after quiz and MCQ activities (and few games in the end-point study). Therefore, the circos mirrors the linear pedagogical strategy by asthma subdomain knowledge (Biomedicine, Symptom, General knowledge, and Treatment).
B2B3 (curved lines lighter), then S1S2S3, C1C2C3 and T1T2T3 (darker) were noticeable. The internal transitions matched with the game component, which was carried out after quiz and MCQ activities (and few games in the end-point study). Therefore, the circos mirrors the linear pedagogical strategy by asthma subdomain knowledge (Biomedicine, Symptom, General knowledge, and Treatment).
In the red Circos, explorations were personalized for each participant because ZPDES algorithm proposed the next activity according to the children's progress for each activity, and thus learning paths were more diversified compared to the predefined sequence defined by the research team and visualized in blue circos. Indeed, there are more transitions between each theme for the same level (e.g., B1S1C1T1). Children whose knowledge improved significantly over time predominantly completed first the lower level of activities (lighter for B1, S1, C1, T1) then they achieved moderate and difficult levels (darker), even if few did activities in T1, B3, and S3, which indicates the children's progress was reduced (too easy for the first, too hard for the second last). In an interesting way, the C1 activities were the most achieved because the learning progress was faster in this set than others. In the same vein, many contents were included in this part (i.e., first level of General knowledge) because during Participatory Design steps, children reported they wanted to learn the most possible things about daily life tips related to asthma. This data personalization illustrated the learning progression toward getting the easy activities done first, just as they are taught to do in school.
In summary, ZPDES algorithm implemented in KidBreath highlighted the learning personalization in activities asthma-related, first with sequences determined by level of difficulty within a sub-domain of asthma knowledge and secondly with sequences driven by individual interests for a given subdomain of asthma knowledge.
Discussion
After the pedagogical assessment of KidBreath with a predefined sequence version defined by the research team, we focused on the added value of an ITS using MAB method for therapeutic education of asthma children in real-world environment.
Regarding pedagogical efficacy, 75% of the children showed a significant improvement in learning gains on asthma post-use of the improved KidBreath. For these children, results showed a better general knowledge about asthma, with a significantly higher learning gain for asthma than for diabetes. In addition, a significant decrease of “I don't know” answers in pre-post revealed that both children learnt more after 1 month using KidBreath and they were more certain of their answers. Once again, correlations found between learning gains, correct and “I don't know” answers in AKQ pre-use points the tool's use out benefitted more to children who initially knew less about the illness and who had the most awareness about their lack of the knowledge asthma-related, i.e., who knew it is in their interest to use KidBreath. Finally, the positive correlation found between learning gains and children cooperation post-use (r = 0.55; p < 0.04) supported this view, where the tool's use benefitted more the children who are the most implicated in the experiment (Rikkers-Mutsaerts et al., 2012).
Regarding pedagogical efficiency, after 1 month-use, a strong intrinsic motivation was scored compared with study 1. Here, when considering children with high learning-gain, a strong intrinsic motivation—especially for feelings enjoy-related provided—was associated to the use of KidBreath and corresponding post-use AKQ scores. In light of the correlation results, efficacy in KidBreath seems more linked to intrinsic than extrinsic motivation. This high intrinsic motivation can be related to ZPDES algorithm from which the learning paths (Circos visualization) were first determined by level of difficulty within a sub-domain of asthma knowledge and secondly driven by the children progress. In addition, under ZPDES condition, children fulfilled less learning activities than those in study 1, but they expressed similar level of pedagogical efficacy (roughly 70% of correct answers in AKQ). Similarly, a reduction of 50% of learning time for achieving the same learning performance in the ZPDES condition compared to study 1 (pre-defined learning condition). In other words, with the ZPDES condition, asthma children performed as well as those without ZPDES condition, but with a diminished time and a decreased content extent. This highlighted the asset of personalized learning sequences over linear predefined sequence.
Therefore, some results related to pedagogical efficiency could be supportive to the added value of ZPDES although we failed to show an improvement of pedagogical efficacy measures.
Similarly, although non-significant, the ZPDES-related slight decrease in illness perception scores can be noticed as well as the parent's verbatim, which indicated an improvement in disease knowledge and child-parent communication. These positive verbatim from parents are reported only after a 1-month period of intervention. The parents expressed an increased illness awareness of their child as well as improved health-related behaviors. Interestingly, the improved behaviors were those exhibited in the KidBreath videos (e.g., taking more carefully the medication, avoiding triggers of asthma attacks), which reinforced the need to integrate videos in the ITS. Indeed, videos were reported as the most appreciated channel to learn about asthma, while learning optimization algorithm was implemented only in riddles section. In all the cases, this fitted with finding on the child's coping with a chronic disease where the wish to know the most possible things is stressed (Miller, 1987; Chateaux and Spitz, 2006, 2007).
Last, but not least, interviews carried out over 1-month use revealed some dropout behaviors because children were complaining KidBreath ran learning redundancies. This fitted the significant decrease of the child engagement in the study reported by parents. Although this is in line with the literature (Vallerand et al., 1997; Rikkers-Mutsaerts et al., 2012), this “ceiling effect” was not induced by the ZPDES algorithm, which was functional, but by its implementation itself. Indeed, our ITS offered learning activities as quiz, MCQ and games, personalized depending on the answer. Concerning quiz, children had to enter the correct answers using the keyboard, but major spelling mistakes were not taken into account, and the system recorded the corresponding answers as wrong, even if it was correct but misspelled. For MCQ, children had to tick all the expected answers, not only one of them: consequently, major answers were considered as wrong. For these reasons, ZPDES exploration was not expanded because the threshold was never achieved and the success rate was poor. Consequently, activities were not deactivated and algorithm submitted the same set of learning activities. To summarize, learning redundancies by ZPDES were irrelevantly inflated. This problem of ZPDES operationalization into KidBreath can be easily fixed with an appropriate scoring of children inputs. Such a corrected operationalization of ZPDES will be stringently matching with the zone of proximal development of each child, and then will probably yield an increased pedagogical efficacy.
Overall, the results from study 2 were mitigated regarding ZPDES benefits for asthma children, although positive results are obtained for several pedagogical efficiency measures (intrinsic motivation, time duration of learning, the extent of explored contents).
Conclusion
For the first time, our study proposed an attempt in the therapeutic learning domain to create a health-related serious game tailored and personalized to foster health education and disease self-management for children with a chronic illness.
In study 1, the pedagogical assessment of KidBreath, deployed with the target population, indicated near and far learning benefits (pedagogical efficacy) associated with high pedagogical efficiency (intrinsic motivation and elicited curiosity), and an increase in disease self-management although disinterest reported because of the linear-predefined sequence—defined by the research team—, highlighting the need to personalize learning activities.
In study 2, personalized learning by implementing an ITS into KidBreath yielded at mid-point study a boosted pedagogical efficiency in terms of intrinsic motivation, learning duration, and explored extent of contents, but without an increase in pedagogical efficacy (no change of level of asthma knowledge elicited by KidBreath).
Regarding therapeutic adherence measures, for both studies, no deterioration was recorded which is relatively positive considering the use in non-controlled environment. It could be noted that a close eye on parent's and child's verbatim suggested a qualitative improvement of therapeutic adherence in terms of parent-child communication as well as disease awareness and healthy behaviors.
Learnt Lessons From Its Implementation
First, one third of the children were recruited after participating to therapeutic education workshops—as a consequence pre-existing knowledge on asthma. This can be critical as the inter-individual variability is the core of research challenge of automatized learning personalization. We could imagine the ZPDES impact can benefited more to a population without any knowledge or health education.
Second, children suffered from mid-asthma, so they didn't always need to apply information learnt in daily life situations. It could be interesting to analyze KidBreath and the ZPDES impact in children with severe asthma whom intrinsic motivation and/or initial asthma-related knowledge would be high.
Third, the incomplete operationalization of ZPDES algorithm into KidBreath led to repeated learning activities that disregarded the actual knowledge level about asthma. Consequently children reported that the set of activities was the same and they were frustrated because their answers were considered wrong all the time. In future work the system implementation has to be improved, especially all spelling mistakes have to be taken into account. During design steps, the research team did not expect children to make many entry errors, and this human factor could have been avoided with more pilot testing. It will be also interesting to integrate a complementary module that gives the possibility of choosing the activities proposed by ZPDES, because most of children complained that they could not choose activities.
Four, our study is based on Clement's works in math tutoring system (Clement et al., 2014a) who showed strong positive results in personalization and adaptation of pedagogical activities because many pilot studies with a sufficient sample size have been carried out to tailor parameters to learning model (Clement et al., 2014a,b, 2015, 2016). In our context with a clinical population, the opportunities of pilot studies for adjusting the operationalization of ZPDES were not possible, and then, the present study was the first pilot study with ITS-augmented KidBreath.
Five, in a related way, the ZPDES algorithm has been only developed on Quiz, MCQ and Game modules while most of participants have expressed their learning preference for video media. Probably, the ZPDES effects would increase on preferred learning support of the targeted population.
Consequently, it will be interesting to carry out other similar studies than ours with the same algorithm but with an adjustment of hyper-parameters integrated in student model. These hyper-parameters would be related to the target population with for example learning parameters such as the initial asthma-related knowledge, the asthma severity, and media preference for learning.
Limitations
First, the sample of participants was small (n = 14 in study 1; n = 15 in study 2). Nevertheless, in similar studies of health serious games evaluations, none of them took place at home but rather within a hospital, following a very controlled procedure with a larger number of participants, but restricting the tool's uses and spontaneous patients' behaviors. We focused on the potential impact of the tool's use in a non-controlled environment, which is the most representative of ecological issues.
Second, in a related way, due to real-life setting of studies, many external family constraints have been challenging (e.g., lack of time with extra-curricular activities, holidays etc.). To keep participants involved, it could be interesting to study the monitoring effect of learning progress by the adding in KidBreath of a module for children, their parents and their practitioner for self- and hetero-monitoring purposes.
Third, the age of most children recruited was late (half of them were aged from 10 to 13 years). Consequently, the user interface was not appropriate for them (childish world) and it matches all the major issues arising for coping, with a strong denial of the disease with this pre-teens period (de Benedictis and Bush, 2007). Yet, most of them exhibited continued efforts in participating to the experiments.
Fourth, ZPDES was developed for learning activities related quiz, MCQ and games, but not for videos. Videos were not taken into account because watch time had to be considered vs. answers (for other materials) as input needed for ZPDES functioning. The integration of videos into ZPDES parameters could be implemented in the next version thanks to interactive videos requiring child answers.
Five, only ZPDES was tested as ITS added into KidBreath. Further studies could investigate the impact of other learning optimization algorithms and variants of ZPDES implemented in KidBreath via comparative studies, as Clement et al.'s did (Miller, 1987; González-Brenes and Mostow, 2012).
To conclude, these pilot studies supported the viability of our participatory design-based methodology to enhance serious game design for health education according to both the content and the personalization display (ITS), even if improvements have to be added (ZPDES operationalization, hyper-parameter implementation, new module learning monitoring…). The expected success was not fully achieved for ZPDES value but some results were encouraging such as gains in time for learning and in the number of contents for achieving a given learning level. The lesson learned discussed above are future lines of research to explore ITS, via ZPDES algorithm, as an opened door for designing and evaluating serious games dedicated to therapeutic education in children with chronic disease.
Ethics Statement
This study was carried out in accordance with the recommendations of INRIA's ethics comity for experimental studies on humans (ethical comittee internal to the research center), the Operational Committee for the Evaluation of Legal and Ethical Risks with written informed consent from all subjects and their parents (or guardians). All subjects and their parents (or guardians) gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Operational Committee for the Evaluation of Legal and Ethical Risks.
Author Contributions
AD, BC, P-YO, and HS contributed conception and design of the study. AD organized the database, performed the statistical analysis and wrote the first draft of the manuscript. AD and BC wrote sections of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank Catherine Argillier, CEO of ItWell Company, which permitted to implement KidBreath application. We would like to thank Dr. Marc Sapène, president of CETBA association, which allowed its patients and physicians network to carry out the two user studies. Obviously, we would like to thank all the 31 patient families who participated of the two user studies.
This work forms part of a thesis project which is sponsored by ItWell Company, Inria Research Institute and French Ministry of Higher Education and Research.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2018.00099/full#supplementary-material
Footnotes
1. ^http://www.who.int/respiratory/asthma/en/
2. ^Similarly to traditional Literacy and Numercacy, Health Literacy is defined by a set of skills and knowledge units to be acquired before one can develop a healthy behavior toward health and illness. ≪ Health Literacy has been defined as the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health. ≫ (http://www.who.int/healthpromotion/conferences/7gchp/track2/en/).
3. ^Comité Opérationnel d'Evaluation des Risques Légaux et Ethiques.
4. ^Commission Nationale de l'Informatique et des Libertés.
5. ^Direction des Services Départementaux de l'Education Nationale.
6. ^Operational Committee for the Evaluation of Legal and Ethical Risks (ethical comittee internal to the research center).
7. ^Commission Nationale de l'Informatique et des Libertés (National Commission of Computing and Freedoms).
8. ^Services Départementaux de l'Education Nationale.
9. ^From the web site: https://www.quizz.biz/quizz-948885.html
References
Al-Motlaq, M., and Sellick, K. (2011). Development and validation of an asthma knowledge test for children 8-10 years of age: child asthma knowledge test. Child Care Health Dev. 37, 123–128. doi: 10.1111/j.1365-2214.2010.01133.x
ANAES (2002). Education Thérapeutique de l'Enfant Asthmatique. Serv Recomm Réf Prof [Internet]. [cité 21 mars 2017]. Available online at: http://splf.fr/wp-content/uploads/2014/08/6recoeduc_asthma_enfan_argumentaire2002.pdf
Anderson, J. R., Corbett, A. T., Koedinger, K. R., and Pelletier, R. (1995). Cognitive tutors: lessons learned. J. Learn. Sci. 4, 167–207. doi: 10.1207/s15327809jls0402_2
Auer, P., Cesa-Bianchi, N., Freund, Y., and Schapire, R. E. (2002). The nonstochastic multiarmed bandit problem. SIAM J. Comput. 32, 48–77. doi: 10.1137/S0097539701398375
Baker, R. S., Corbett, A. T., and Aleven, V. (2008). “More Accurate student modeling through contextual estimation of slip and guess probabilities in Bayesian knowledge tracing,” in Intelligent Tutoring Systems [Internet], eds B. P. Woolf, E. Aïmeur, R. Nkambou, and S. Lajoie (Berlin; Heidelberg: Springer), 406–415. [cité 8 juin 2018]. Available online at: http://link.springer.com/10.1007/978-3-540-69132-7_44
Bangor, A., Kortum, P. T., and Miller, J. T. (2008). An empirical evaluation of the system usability scale. Int. J. Hum. Comput. Interact. 24, 574–594. doi: 10.1080/10447310802205776
Bastien, J. M. C., and Scapin, D. L. (1993). Ergonomic Criteria for the Evaluation of Human-Computer Interfaces. Report No.: 156.
Bauman, L. J., Wright, E., Leickly, F. E., Crain, E., Kruszon-Moran, D., Wade, S. L., et al. (2002). Relationship of adherence to pediatric asthma morbidity among inner-city children. Pediatrics 110:e6. doi: 10.1542/peds.110.1.e6
Beale, I. L., Kato, P. M., Marin-Bowling, V. M., Guthrie, N., and Cole, S. W. (2007). Improvement in cancer-related knowledge following use of a psychoeducational video game for adolescents and young adults with cancer. J. Adolesc. Health 41, 263-270. doi: 10.1016/j.jadohealth.2007.04.006
Beaudouin-Lafon, M., and Mackay, W. E. (2003). Prototyping tools and techniques. Hum. Comput. Interact. Dev. Process. 122–142.
Bindels, P. J., Grol, M. H., Ponsioen, B. P., Salomé, P. L., Wiersma, T., and Goudswaard, A. N. (2008). Summary of the practice guideline'Asthma in children'(second revision) from the Dutch College of General Practitioners. Ned. Tijdschr. Geneeskd. 152, 550–555.
Brown, S. J., Lieberman, D. A., Gemeny, B. A., Fan, Y. C., Wilson, D. M., and Pasta, D. J. (1997). Educational video game for juvenile diabetes: results of a controlled trial. Med. Inform. 22, 77–89. doi: 10.3109/14639239709089835
Cen, H., Koedinger, K., and Junker, B. (2006). “Learning factors analysis – A general method for cognitive model evaluation and improvement,” in Intelligent Tutoring Systems [Internet], eds M. Ikeda, K. D. Ashley, and T.-W. Chan (Berlin; Heidelberg: Springer), 164-175. [cité 8 juin 2018]. Available online at: http://link.springer.com/10.1007/11774303_17
Chan, D. S., Callahan, C. W., Hatch-Pigott, V. B., Lawless, A., Proffitt, H. L., Manning, N. E., et al. (2007). Internet-based home monitoring and education of children with asthma is comparable to ideal office-based care: results of a 1-year asthma in-home monitoring trial. Pediatrics 119, 569-578. doi: 10.1542/peds.2006-1884
Chang, K., Beck, J., Mostow, J., and Corbett, A. (2006). “A Bayes net toolkit for student modeling in intelligent tutoring systems,” in Intelligent Tutoring Systems [Internet], eds M. Ikeda, K. D. Ashley, and T.-W. Chan (Berlin; Heidelberg: Springer), 104–113. [cité 8 juin 2018]. Available online at: http://link.springer.com/10.1007/11774303_11
Charles, T., Quinn, D., Weatherall, M., Aldington, S., Beasley, R., and Holt, S. (2007). An audiovisual reminder function improves adherence with inhaled corticosteroid therapy in asthma. J. Allergy Clin. Immunol. 119, 811-816. doi: 10.1016/j.jaci.2006.11.700
Chateaux, V., and Spitz, E. (2006). Perception de la maladie et adhérence thérapeutique chez des enfants asthmatiques. Pract. Psychol. 12, 1–16. doi: 10.1016/j.prps.2006.01.001
Chateaux, V., and Spitz, E. (2007). Perception de la maladie chez des enfants asthmatiques et leurs parents. Enfance 59, 161. doi: 10.3917/enf.592.0161
Clement, B., Oudeyer, P.-Y., and Lopes, M. (2016). “A comparison of automatic teaching strategies for heterogeneous student populations,” in EDM 16-9th International Conference on Educational Data Mining (Raleigh, NC).
Clement, B., Oudeyer, P.-Y., Roy, D., and Lopes, M. (2014a). “Online optimization of teaching sequences with multi-armed bandits,” in Educational Data Mining 2014 (London).
Clement, B., Roy, D., Oudeyer, P.-Y., and Lopes, M. (2014b). “Developmental learning for intelligent tutoring systems,” in Development and Learning and Epigenetic Robotics (ICDL-Epirob), 2014 Joint IEEE International Conferences on (IEEE) (Sydney, NSW), 426–433.
Clement, B., Roy, D., Oudeyer, P.-Y., and Lopes, M. (2015). Multi-armed bandits for intelligent tutoring systems. J Educ. Data Mining 7, 20-48.
Corbett, A. T., and Anderson, J. R. (1994). Knowledge tracing: Modeling the acquisition of procedural knowledge. User Model. User Adapt. Interact. 4, 253-278.
Cordova, D. I., and Lepper, M. R. (1996). Intrinsic motivation and the process of learning: beneficial effects of contextualization, personalization, and choice. J. Educ. Psychol. 88:715.
de Benedictis, D., and Bush, A. (2007). The Challenge of asthma in adolescence. Pediatr. Pulmonol. 42, 683–692. doi: 10.1002/ppul.20650
Deci, E. L., and Ryan, R. M. (1985). The general causality orientations scale: self-determination in personality. J Res Pers. 19, 109–134.
Delmas, A., Oudeyer, P.-Y., and Sauzéon, H. (2018). Participatory Design of a serious game to foster children Health Education.
Desrochers, A., Comeau, G., Jardaneh, N., and Green-Demers, I. (2006). L'élaboration d'une échelle pour mesurer la motivation chez les jeunes élèves en piano. Rech. Éduc. Music 24, 13–33.
Deterding, S., Dixon, D., Khaled, R., and Nacke, L. (2011). “From game design elements to gamefulness: defining gamification,” in Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments (ACM) (Tampere), 9–15.
Dunlosky, J., Rawson, K. A., Marsh, E. J., Nathan, M. J., and Willingham, D. T. (2013). Improving students' learning with effective learning techniques: promising directions from cognitive and educational psychology. Psychol. Sci. Public Interest 14, 4–58. doi: 10.1177/1529100612453266
Folkman, S. (1984). Personal control and stress and coping processes: A theoretical analysis. J. Pers. Soc. Psychol. 46, 839. doi: 10.1037/0022-3514.46.4.839
Gibson, P. G., Coughlan, J., Wilson, A. J., Abramson, M., Bauman, A., Hensley, M. J., et al. (2002). Self-management education and regular practitioner review for adults with asthma. Cochrane Library. 84. doi: 10.1002/14651858.CD001117
Glickman, C. L., and Dixon, J. K. (2002). Teaching intermediate algebra using reform computer assisted instruction. Int. J. Technol. Math. Educ. 9:75.
González-Brenes, J., Huang, Y., and Brusilovsky, P. (2014). “General features in knowledge tracing to model multiple subskills, temporal item response theory, and expert knowledge,” in The 7th International Conference on Educational Data Mining (University of Pittsburgh), 84–91
González-Brenes, J., and Mostow, J. (2012). “Dynamic cognitive tracing: towards unified discovery of student and cognitive models,” in Proceedings of the Fifth International Conference on Educational Data Mining (EDM), 8.
Gordon, G., Breazeal, C., and Engel, S. (2015). “Can children catch curiosity from a social robot?” in Proceedings of the Tenth Annual ACM/IEEE International Conference on Human-Robot Interaction [Internet] (ACM), 91–98. [cité 9 mars 2017]. Available online at: http://dl.acm.org/citation.cfm?id=2696469
Guevara, J. P., Wolf, F. M., Grum, C. M., and Clark, N. M. (2003). Effects of educational interventions for self management of asthma in children and adolescents: systematic review and meta-analysis. BMJ 326, 1308–1309. doi: 10.1136/bmj.326.7402.1308
Gustafsson, P. M., Watson, L., Davis, K. J., and Rabe, K. F. (2006). Poor asthma control in children: evidence from epidemiological surveys and implications for clinical practice. Int. J. Clin. Pract. 60, 321–334. doi: 10.1111/j.1368-5031.2006.00798.x
Hamari, J., Koivisto, J., and Sarsa, H. (2014). Does Gamification Work? – A Literature Review of Empirical Studies on Gamification (IEEE), 3025-3034. [cité 13 nov 2017]. Available online at: http://ieeexplore.ieee.org/document/6758978/
Harris, P. L. (2012). Trusting What You're Told: How Children Learn From Others. Cambridge: Harvard University Press.
Hirsh-Pasek, K., Zosh, J. M., Golinkoff, R. M., Gray, J. H., Robb, M. B., and Kaufman, J. (2015). Putting education in “educational” apps: lessons from the science of learning. Psychol. Sci. Public Interest 16, 3–34. doi: 10.1177/1529100615569721
Hoffman, H. G., Patterson, D. R., Seibel, E., Soltani, M., Jewett-Leahy, L., and Sharar, S. R. (2008). Virtual reality pain control during burn wound debridement in the hydrotank. Clin. J. Pain 24, 299–304. doi: 10.1097/AJP.0b013e318164d2cc
Huertas, C., and Juárez-Ramírez, R. (2013). Developing an intelligent tutoring system for vehicle dynamics. Procedia Soc. Behav. Sci. 106, 838–847. doi: 10.1016/j.sbspro.2013.12.096
Jan, R.-L., Wang, J.-Y., Huang, M.-C., Tseng, S.-M., Su, H.-J., and Liu, L.-F. (2007). An internet-based interactive telemonitoring system for improving childhood asthma outcomes in Taiwan. Telemed. E Health 13, 257–268. doi: 10.1089/tmj.2006.0053
Kaloti-Hallak, F., Armoni, M., and Ben-Ari, M. (2015). Students' Attitudes and Motivation During Robotics Activities. ACM Press, 102-110. [cité 14 nov 2017]. Available online at: http://dl.acm.org/citation.cfm?doid=2818314.2818317
Kam, M., Agarwal, A., Kumar, A., Lal, S., Mathur, A., Tewari, A., et al. (2008). “Designing e-learning games for rural children in India: a format for balancing learning with fun,” in Proceedings of the 7th ACM Conference on Designing Interactive Systems (ACM) (Cape Town), 58–67.
Kapp, K. M. (2012). The Gamification of Learning and Instruction: Game-Based Methods and Strategies for Training and Education. San Francisco, CA: John Wiley & Sons.
Kato, P. M., Cole, S. W., Bradlyn, A. S., and Pollock, B. H. (2008). A video game improves behavioral outcomes in adolescents and young adults with cancer: a randomized trial. Pediatrics 122, 305–317. doi: 10.1542/peds.2007-3134
Kharrazi, H., Watters, C., and Oore, S. (2008). Improving behavioral stages in children by adaptive applications. J. Inf. Technol. Healthc. 6, 322–326.
Koedinger, K. R., Anderson, J. R., Hadley, W. H., and Mark, M. A. (1997). Intelligent tutoring goes to school in the big city. Int. J. Artif. Intell. Edu. 8, 30–43.
Krzywinski, M., Schein, J., Birol, I., Connors, J., Gascoyne, R., Horsman, D., et al. (2009). Circos: An information aesthetic for comparative genomics. Genome Res. 19, 1639–1645. doi: 10.1101/gr.092759.109
Leventhal, H., Nerenz, D. R., and Steele, D. J. (1984). “Illness representations and coping with health threats,” in Handbook of Psychology and Health, eds A. Baum, S. E. Taylor, and J. E. Singer (Mahwah, NJ: Lawrence Erlbaum), 219-252.
Lieberman, D. A. (1997). “Interactive video games for health promotion: Effects on knowledge, self-efficacy, social support, and health,” in Health Promotion and Interactive Technology: Theoretical Applications and Future Directions, eds. R. L. Street, W. R. Gold, and T. R. Manning (New-York, NY; London: Routledge), 103–120.
Lieberman, D. A. (2001). Management of chronic pediatric diseases with interactive heath games: theory and research findings. J. Ambulatory Care Manage. 24, 26–38. doi: 10.1097/00004479-200101000-00004
Mackay, W. E. (2003). Educating multi-disciplinary design teams. Proc. Tales Disappearing Comput. 105–118.
Malone, T. W. (1980). “What makes things fun to learn? Heuristics for designing instructional computer games,” in: Proceedings of the 3rd ACM SIGSMALL Symposium and the first SIGPC Symposium on Small Systems (Palo Alto, CA: ACM), 162–169.
Malone, T. W., and Lepper, M. R. (1987). Making learning fun: a taxonomy of intrinsic motivations for learning. Aptit. Learn. Instr (Palo Alto, CA). 3, 223–253.
Melonio, A., and Gennari, R. (2012). Co-design with Children: the State of the Art [Internet]. Technical report, KRDB Research Centre Technical Report. [cité 2 févr 2017]. Available online at: http://www.academia.edu/download/41395015/KRDB13-1.pdf
Miller, S. M. (1987). Monitoring and blunting: validation of a questionnaire to assess styles of information seeking under threat. J. Pers. Soc. Psychol. 52, 345. doi: 10.1037/0022-3514.52.2.345
Mitic, W., Ben Abdelaziz, F., and Madi, H. (2012). Health Education: Theoretical Concepts, Effective Strategies and Core Competencies. Cairo: World Health Organization, Regional Office for the Eastern Mediterranean, 79.
Morris, L. S., and Schulz, R. M. (1992). Patient compliance—an overview. J. Clin. Pharm. Ther. 17, 283–295.
Muller, M. J., and Kuhn, S. (1993). Participatory design. Commun. ACM 36, 24–28. doi: 10.1145/153571.255960
Muñoz, D. C., Ortiz, A., González, C., López, D. M., and Blobel, B. (2010). Effective e-learning for health professional and medical students: the experience with SIAS-Intelligent Tutoring System. Stud. Health Technol. Inform. 156, 89–102s. doi: 10.3233/978-1-60750-565-5-89
Naimi, D. R., Freedman, T. G., Ginsburg, K. R., Bogen, D., Rand, C. S., and Apter, A. J. (2009). Adolescents and asthma: why bother with our meds? J. Allergy Clin. Immunol. 123, 1335–1341. doi: 10.1016/j.jaci.2009.02.022
National Institutes of Health (1997). Guidelines for the Diagnosis and Management of Asthma. Expert panel report.
Newell, A. F., and Gregor, P. (2000). “User sensitive inclusive design – in search of a new paradigm,” in Proceedings on the 2000 Conference of Universal Usability (CUU - ACM) (New York, NY), 39–44. doi: 10.1145/355460.355470
Nguyen, L., Raherison, C., Bozonnat, M.-C., Lheureux, M., Nocent, C., Tunon-de-Lara, J.-M., et al. (2003). Validation d'un questionnaire de connaissances sur l'asthme. Rev. Mal. Respir. 20, 871–880.
Nkambou, R., Mizoguchi, R., and Bourdeau, J. (2010). Advances in Intelligent Tutoring Systems, Vol. 308. Berlin: Springer Science & Business Media.
Nutbeam, D. (2008). The evolving concept of health literacy. Soc. Sci. Med. 67, 2072–2078. doi: 10.1016/j.socscimed.2008.09.050
Rabe, K. F., Adachi, M., Lai, C. K., Soriano, J. B., Vermeire, P. A., Weiss, K. B., et al. (2004). Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J. Allergy Clin. Immunol. 114, 40–47. doi: 10.1016/j.jaci.2004.04.042
Rafferty, A. N., Brunskill, E., Griffiths, T. L., and Shafto, P. (2011). “Faster teaching by POMDP planning,” in Artificial Intelligence in Education [Internet]. Eds G. Biswas, S. Bull, J. Kay, and A. Mitrovic (Berlin; Heidelberg: Springer), 280–287 [cité 8 juin 2018]. Available online at: http://link.springer.com/10.1007/978-3-642-21869-9_37
Rikkers-Mutsaerts, E. R., Winters, A. E., Bakker, M. J., van Stel, H. F., van der Meer, V., de Jongste, J. C., et al. (2012). Internet-based self-management compared with usual care in adolescents with asthma: a randomized controlled trial. Pediatr. Pulmonol. 47, 1170–1179. doi: 10.1002/ppul.22575
Roediger, H. L. (2013). Applying cognitive psychology to education: translational educational science. Psychol. Sci. Public Interest 14, 1–3. doi: 10.1177/1529100612454415
Sanders, E. (2002). “From user-centered to participatory design approaches,” in Design and the Social Sciences: Making Connections [Internet]. CRC Press, 1–8. [cité 2 févr 2017]. Available online at: http://www.crcnetbase.com/doi/pdf/10.1201/9780203301302.ch1
Sharar, S. R., Carrougher, G. J., Nakamura, D., Hoffman, H. G., Blough, D. K., and Patterson, D. R. (2007). Factors influencing the efficacy of virtual reality distraction analgesia during postburn physical therapy: preliminary results from 3 ongoing studies. Arch. Phys. Med. Rehabil. 88, S43–S49. doi: 10.1016/j.apmr.2007.09.004
Shegog, R., Bartholomew, L. K., Parcel, G. S., Sockrider, M. M., Mâsse, L., and Abramson, S. L. (2001). Impact of a computer-assisted education program on factors related to asthma self-management behavior. J. Am. Med. Inform. Assoc. 8, 49–61. doi: 10.1136/jamia.2001.0080049
Suebnukarn, S., and Haddawy, P. (2004). “A collaborative intelligent tutoring system for medical problem-based learning,” in Proceedings of the 9th International Conference on Intelligent User Interfaces (Funchal: ACM), 14–21.
Touré-Tillery, M., and Fishbach, A. (2014). How to measure motivation: a guide for the experimental social psychologist: how to measure motivation. Soc. Pers. Psychol. Compass 18, 328–341. doi: 10.1111/spc3.12110
Vallerand, R. J., Blais, M. R., Brière, N. M., and Pelletier, L. G. (1989). Construction et validation de l'échelle de motivation en éducation (EME). Can. J. Behav. Sci. Can. Sci. Comport. 21, 323.
Vallerand, R. J., Fortier, M. S., and Guay, F. (1997). Self-determination and persistence in a real-life setting: toward a motivational model of high school dropout. J. Pers. Soc. Psychol. 72:1161. doi: 10.1037/0022-3514.72.5.1161
Vallerand, R. J., Pelletier, L. G., Blais, M. R., Brière, N. M., Senecal, C., and Vallières, E. F. (1992). The Academic Motivation Scale: a measure of intrinsic, extrinsic, and amotivation in education. Educ. Psychol. Meas. 52, 1003-1017. doi: 10.1177/0013164492052004025
Villano, M. (1992). Probabilistic Student Models: Bayesian Belief Networks and Knowledge Space Theory. Berlin; Heidelberg: Springer, 491–498.
Weinman, J., Petrie, K. J., Moss-Morris, R., and Horne, R. (1996). The illness perception questionnaire: a new method for assessing the cognitive representation of illness. Psychol. Health 11, 431–445. doi: 10.1080/08870449608400270
Weinman, J., Petrie, K. J., Sharpe, N., and Walker, S. (2000). Causal attributions in patients and spouses following first-time myocardial infarction and subsequent lifestyle changes. Br. J. Health Psychol. 5, 263–273. doi: 10.1348/135910700168900
Whyte, E. M., Smyth, J. M., and Scherf, K. S. (2015). Designing serious game interventions for individuals with autism. J. Autism Dev. Disord. 45, 3820–3831. doi: 10.1007/s10803-014-2333-1
Wolfe, C. R., Reyna, V. F., Widmer, C. L., Cedillos, E. M., Fisher, C. R., Brust-Renck, P. G., et al. (2015). Efficacy of a web-based intelligent tutoring system for communicating genetic risk of breast cancer: a fuzzy-trace theory approach. Med. Decis. Making 35, 46–59. doi: 10.1177/0272989X14535983
Keywords: health education, serious game, asthma, Intelligent Tutoring System (ITS), intrinisic motivation, therapeutic education
Citation: Delmas A, Clement B, Oudeyer P-Y and Sauzéon H (2018) Fostering Health Education With a Serious Game in Children With Asthma: Pilot Studies for Assessing Learning Efficacy and Automatized Learning Personalization. Front. Educ. 3:99. doi: 10.3389/feduc.2018.00099
Received: 19 July 2018; Accepted: 25 October 2018;
Published: 14 November 2018.
Edited by:
Tom Crick, Swansea University, United KingdomReviewed by:
Krista Mincey, Xavier University of Louisiana, United StatesSankalp Das, Baptist Health South Florida, United States
Copyright © 2018 Delmas, Clement, Oudeyer and Sauzéon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandra Delmas, YWxleGFuZHJhLmRlbG1hc0BpbnJpYS5mcg==
Helène Sauzéon, aGVsZW5lLnNhdXplb25AaW5yaWEuZnI=