 Vanessa Tomas
Vanessa Tomas- 1School of Rehabilitation Science, McMaster University, Hamilton, ON, Canada
- 2CanChild Centre for Childhood Disability Research, McMaster University, Hamilton, ON, Canada
Since the 1990s, educators have prioritized inclusion of students with disabilities in general educational settings. Concurrently, health-care professionals have recognized the need to support students’ academic functioning and participation at school. Despite this recognition, integration of health support services in schools remains a significant challenge and the extent to which students with special needs fully participate at school is often less than optimal. In this study, we suggest that combining health and education conceptual frameworks would advance the goal of inclusion by enhancing interprofessional communication and collaboration. The World Health Organization’s International Classification of Functioning, Disability and Health (ICF) is a health framework that focuses on functioning and participation via a lens of inclusivity, universality, and a holistic approach to health and disability. Similarly, Universal Design for Learning (UDL) is an educational framework for guiding the design of instructional materials, methods, and assessments to be inclusive and accessible for all. Both frameworks are well established in their respective fields, but they have yet to “cross the border” to influence each discipline’s practices. While researchers have alluded to the potential utilization of both frameworks in education settings, there is limited guidance on how these two frameworks may be combined in practice. In this study, we will compare the ICF and UDL frameworks, and provide insight into how utilization of both frameworks may enhance interprofessional collaboration and support inclusion in school settings.
Introduction
Inclusive education refers to “the creation of learning environments that maximize the potential for every young person in … diverse societies to receive a high-quality education alongside their peers in local schools that serve the whole community” (Porter and Towell, 2017). In Canada, although inclusive education is widely accepted as best practice, its implementation varies across the country (Towle, 2015). Indeed, while policy exists to support inclusive education in most jurisdictions in Canada, evidence suggests a gap between these directives and actual practices (Timmons and Wagner, 2009; Thompson et al., 2015). This gap has implications for Canadian children: data from Statistics Canada indicate that children with disabilities who attend inclusive schools are physically and emotionally healthier; participate in more physical and social activities; and require access to fewer health services than children with disabilities who are segregated for all or part of the school day (Timmons and Wagner, 2009). According to Thompson et al. (2015), insufficient human resources to support educators in the classroom appear to be a key barrier to successful implementation of inclusive education in Canada.
One means of addressing this human resource barrier is to enhance collaboration between educators and health-care professionals (HCPs). Educators’ knowledge of curriculum and instruction is complemented by HCPs’ knowledge of specific disabilities and how these may affect students’ functioning and participation (Campbell et al., 2016). Therefore, collaboration between HCPs and educators ostensibly would enhance educators’ knowledge of children with disabilities and support HCPs’ provision of educationally relevant services that are directly embedded in the classroom (Missiuna et al., 2012). Ultimately, this sharing of knowledge and skills between educators and HCPs should assist efforts to implement inclusive education. However, how to best support this collaboration across disciplines remains unknown.
In this study, we suggest that integrating the International Classification of Functioning, Disability and Health (ICF) and Universal Design for Learning (UDL), which are health and education frameworks, respectively, can support interprofessional sharing of knowledge and expertise beyond what either framework could achieve on its own. In particular, we believe these frameworks to be compatible due to a shared underlying philosophy of universality. That is, both frameworks are inclusive of all people and both recognize that human functioning exists along a continuum. To make this case, we will proceed systematically. First, we will introduce and describe each framework. Next, we will compare the two frameworks to demonstrate how they complement one another in their purpose and content. Finally, we will use a hypothetical case example to illustrate how these frameworks could be used interprofessionally to support inclusive education.
The International Classification of Functioning, Disability and Health (ICF)
The ICF was developed by the World Health Organization (WHO) in 2001 and is a framework that embraces concepts of universality in human health; that is, functioning and ability lie on a continuum and every person is expected to vary on these across the lifespan. The ICF merges concepts from the medical and social models of disability to create a “bio-psycho-social” model that acknowledges the multiple influences on health and functioning (World Health Organization, 2001, 2013).
The ICF consists of two major components: functioning and disability (body structures and function, activities, and participation); and contextual factors (environmental and personal factors) (World Health Organization, 2001). Each of these components consists of multiple domains, which then encompass categories used for classification (World Health Organization, 2001, 2013). A notable advancement in the ICF relative to previous disability models is the incorporation of environmental factors, which acknowledges the impact an individual’s environment can have on their overall life experience (McPherson et al., 2015).
The ICF framework is a tool that can be used as a method of classification in various situations, including healthcare and education (World Health Organization, 2001). When using the ICF as a classification tool, each person is considered in context, specifically looking at the interaction between the individual’s health and level of functioning and the features of their environment (World Health Organization, 2002). Overall, the ICF provides a holistic and strengths-based model, which aims to highlight assets and skills of all individuals (Stewart and Rosenbaum, 2003).
Examples of Applying the ICF in Education
In educational settings, the focus of classification of children with disabilities is on skills and characteristics related to meeting academic demands as well as consideration of the school environment (Florian and McLaughlin, 2008). The ICF provides codes that classify specific functions related to school, such as attention, learning, and communication (Simeonsson, 2009). When analyzing the important domains for children with disabilities, it increases understanding of supports and services that are required (Florian and McLaughlin, 2008). However, having knowledge about children’s functional and academic capabilities is not enough to fully support students in the classroom. It is critical that educators and HCPs understand how to use knowledge gained from the ICF to create an inclusive and academically enriching classroom environment for students with special needs (Hellblom-Thibblin et al., 2013).
Two countries, Switzerland and Portugal, have applied the ICF in educational settings (Hollenweger, 2011; Sanches-Ferreira et al., 2013). In Switzerland, Hollenweger (2011) reported findings from a study in which the ICF was used to establish educational and developmental goals for students with disabilities, along with estimating their educational requirements and needs. Interestingly, Hollenweger (2011) noted that classroom participation was a goal set by many students and families, thereby suggesting a need for environmental interventions to support inclusion. In Portugal, Sanches-Ferreira and colleagues (2013) concluded that educators’ use of the ICF as a tool for determining students’ needs provided a holistic view of students’ functioning within the school setting. However, while all ICF domains were utilized, school personnel were least likely to incorporate environmental factors within their assessments. The authors noted the need for tools/frameworks that focus on environmental interventions and the need for collaboration among different professionals who have knowledge regarding educational environments (Sanches-Ferreira et al., 2013).
Universal Design for Learning
Universal Design for Learning (UDL) is a framework and set of guidelines developed in the 1990s by the Center for Applied Special Technology (2016). UDL emerged from the universal design movement in architecture, which found that planning physical structures and spaces to be accessible to a diverse range of users from the outset was more efficient and effective than retro-fitting individual structures (Rose and Strangman, 2007; Campbell et al., 2016). UDL takes this lesson from architecture and applies it to the educational curriculum. By accounting for student variability and learning differences throughout the initial stages of curriculum design, educators seek to reduce the need for individual student accommodations after-the-fact (Center for Applied Special Technology, 2016).
The UDL guidelines include three main principles: (1) providing multiple ways of representing the curriculum to students; (2) providing multiple ways for students to express what they know and have learned; and (3) providing multiple ways to engage students in the learning process (Meyer et al., 2014). Providing multiple means of representation is considered the “what” of learning. Utilizing different forms of methods and media for students to learn and perceive information is the foundation of this principle (Meyer et al., 2014). Providing multiple means of student action and expression, the second UDL principle, tackles the “how” of learning (Meyer et al., 2014). The educator needs to offer options to allow multiple ways for students to communicate information, including options for physical action and executive functions. Providing an assortment of options to engage students in the classroom, the third UDL principle, targets the “why” of learning (Meyer et al., 2014). This principle focuses on strategies to engage students in the classroom and supports excitement, motivation, and interest in a topic (Table 1).
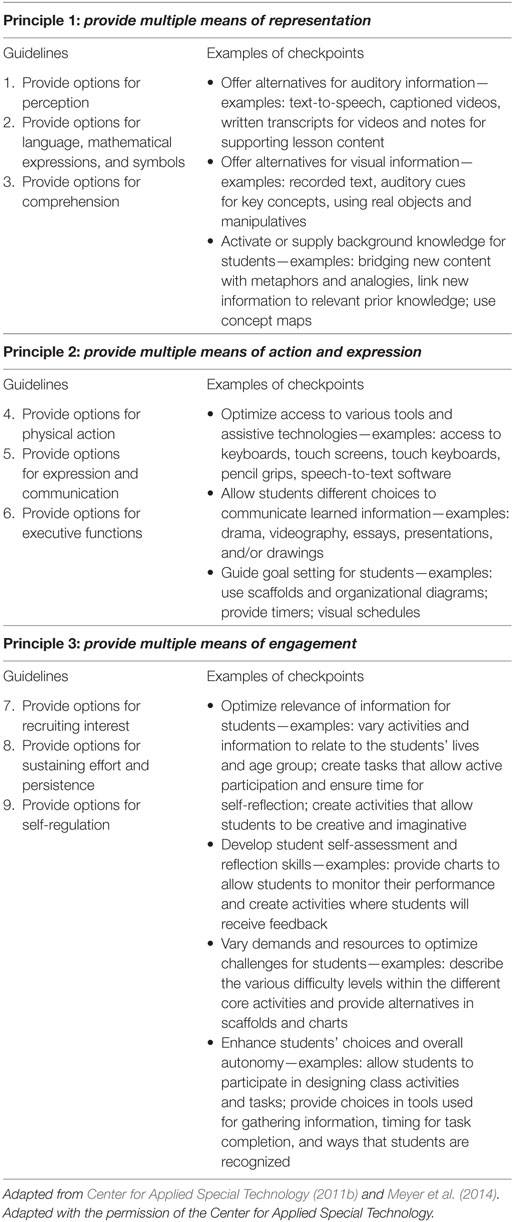
Table 1. The Universal Design for Learning principles, guidelines, and checkpoint examples.
As shown in Table 1, each UDL principle is further defined by three guidelines and several checkpoints that identify various strategies that can be used to execute the UDL principles (Center for Applied Special Technology, 2011a). The guidelines offer general strategies that can be used to enact each of the principles with the checkpoints providing specific suggestions for implementation. When the three principles are implemented in tandem, the UDL framework supports educators in cultivating students who are knowledgeable, resourceful, goal-directed, and motivated learners (Meyer et al., 2014). Importantly, UDL puts the emphasis on creating dynamic and flexible learning environments that “fit” the student, rather than assuming the student must change to “fit” a standard or static environment (Meyer et al., 2014).
Examples of Applying UDL in Education
Universal Design for Learning is a promising framework that provides options and strategies to enhance inclusivity for students, including those with special needs. In a study conducted by Dymond and colleagues (2006), the authors described how UDL was utilized to redesign a science curriculum. Laptops and computers with internet access, interactive software, and group projects were some components added to the curriculum to permit enactment of the UDL guidelines (Dymond et al., 2006). Following these modifications, the authors reported an increase in student engagement and participation through measurement of increased social skills, class attendance, and overall enjoyment (Dymond et al., 2006).
Inclusivity of students also was enhanced in a study by Marino (2009), who studied the impact of an online scientific-inquiry program called Alien Rescue on students with reading difficulties. Alien Rescue incorporates evidence-based cognitive tools, such as databases and interactive tutorials that reduce processing and memory load for learners. Both low-ability readers and proficient readers gained an increase in their posttest scores after usage of Alien Rescue (Marino, 2009). Students of varying levels were able to utilize this UDL-based program, helping to enhance learning and inclusivity.
Comparing the ICF and UDL Frameworks
To the best of our knowledge, few authors have explicitly explored the relationship between the ICF and UDL. Therefore, we endeavored to identify similarities and differences between these frameworks by examining their general applications within literature, and the overall goals and components of each framework. Specifically, the first and second authors (Vanessa Tomas and Andrea Cross) contributed expertise on UDL and the ICF, respectively. Both authors examined seminal literature on their respective topics of expertise (World Health Organization, 2001, 2013; Meyer et al., 2014; Center for Applied Special Technology, 2016). Vanessa Tomas and Andrea Cross then engaged in a series of meetings to discuss the various components of each framework as well as to compare each framework’s principles, components, and general applications. This iterative process culminated in the identification of four areas of similarity and four areas of difference.
Similarities
First, as noted previously, both the ICF and the UDL frameworks embrace the concept of universality in human functioning, meaning each acknowledges that human diversity is the norm rather than the exception (Campbell and Skarakis-Doyle, 2007). Second, both frameworks highlight the importance of the environment as a factor that can influence human functioning, either positively or negatively, depending on how that environment is configured. Third, the ICF and UDL both view successful participation as a goal that is more important than “fixing” the individual so that he or she conforms to some preconceived status as “normal” (Campbell and Skarakis-Doyle, 2007; Rosenbaum and Gorter, 2012). That is, both frameworks aim to enhance inclusivity by emphasizing the importance of the “fit” between the environment and the child. Finally, both frameworks use positive and neutral wording, along with focusing on an individual’s strengths.
Differences
Although the frameworks have multiple similarities, there also are key differences. First, each framework has its origins in different fields, ICF in health and UDL in education; thus, each uses terminology that is tailored for health professionals and educators, respectively. Second, while the ICF highlights how an individual’s health condition interacts with a given environment, the UDL framework emphasizes creating environments that are flexible for many individuals irrespective of the reason for their diverse abilities. Third, while the ICF considers functioning in many different environments, the UDL framework focuses specifically on the school and classroom environment. Fourth, while the ICF is a bio-psycho-social model that considers health and functioning to reflect the combination of medical and social models of disability (i.e., the person and the environment can contribute to functioning and disability), UDL places itself firmly in the social model (i.e., the environment is the limiting factor rather than the individual).
Are the ICF and UDL Complementary Frameworks?
Having examined the similarities and differences in the ICF and UDL frameworks, it is fair that one might question their joint use. Are the similarities more powerful than the differences, or vice versa? It is our contention that the differences between these two frameworks can work in their favor, with one complementing the other so that together they form a “bridge” between health and education.
To date, there remains a lack of literature evaluating the use of both frameworks in educational settings. In 2007, Campbell and Skarakis-Doyle explored how the ICF framework could be used to identify common features across categories of developmental disorders in school-age children. Through the lens of the ICF, the authors suggested how school-based health services could be configured to support children who have different diagnostic labels but similar academic needs. Of note, they suggested that the UDL framework could point to specific environmental interventions that would apply across disorder types and could be implemented collaboratively by HCPs and educators. Moreover, by implementing UDL, educators and HCPs also would enhance curricular accessibility for all children within the classroom. Campbell and Skarakis-Doyle (2007) concluded that by using the ICF and UDL in tandem, HCPs and educators not only would have a means of holistically describing the needs of individual children with learning needs, but they also would have access to concrete strategies for embedding services in the classroom.
Case Study Example: Exploring How the ICF and UDL Frameworks Jointly Support Inclusion
To illustrate how the ICF and UDL could be used synergistically to enhance inclusion, we will present and discuss a hypothetical case study.
Daniel is an 8-year-old boy who is always disheveled—shirt untucked and shoes untied. He is clumsy and has been described as “having two left feet.” At school, Daniel has trouble keeping his belongings and school work organized. He has trouble with printing and often falls behind in his written work. Daniel lives at home with his mother and father, who are both very supportive. He has a dog who he walks every day and loves to spend time with. Daniel also likes to watch basketball on television, and often attends basketball games with his father. Daniel’s teacher is very supportive in helping with his studies, as she notices he is quite bright and just does not seem to be achieving his academic potential. Daniel’s parents and the school staff are working together to identify his needs at school, initiate any referrals needed, and develop an individual education plan. Daniel’s teacher wants to be sure that she can successfully support him in the classroom.
Consistent with the literature (e.g., Hollenweger, 2011), the ICF can be used as a classification tool to identify Daniel’s needs and strengths at school, as well as other environments. The ICF also can be used to determine goals for Daniel and educational requirements. Figure 1 provides an example of how the ICF framework can be used to understand Daniel’s strengths, needs, goals, and support in collaborative educational planning.
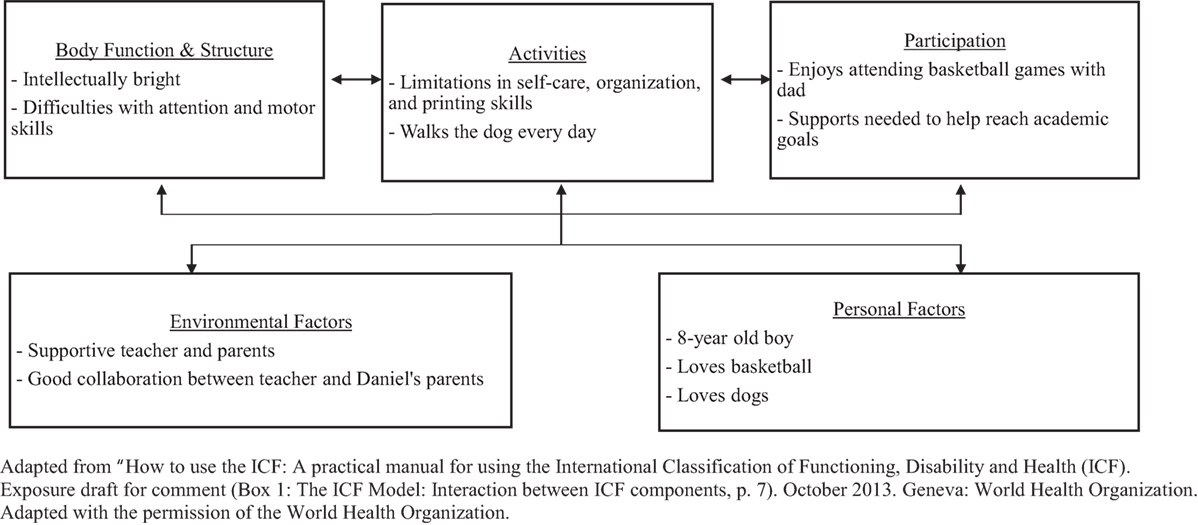
Figure 1. Classification of Daniel’s case study using the ICF framework. Adapted from World Health Organization (2013) (Box 1: the ICF model: interaction between ICF components, p. 7). Adapted with the permission of the World Health Organization.
To complement use of the ICF to describe Daniel, the UDL framework can suggest classroom supports that the educator and HCP could implement together to ensure that Daniel is successful at school. For example, Daniel’s interest in basketball (a Personal Factor) could be leveraged by designing assignments that allowed him (and other students) to draw on topics that were personally motivating, thereby providing options for engagement that may increase focus and attention (UDL Principle 3). Specifically, Table 1 indicates that UDL Guideline 7 recommends the provision of options for recruiting student interest by seeking opportunities to enhance the personal relevance and value of learning to students. Thus, a Personal Factor in the ICF can be translated into a tangible change in a learning activity within the classroom environment.
Another example relates to Daniel’s difficulties with motor skills as identified in the ICF as an impairment in Body Function and Structure. Specifically, Daniel struggles with printing, thereby not completing his work in a timely fashion (an Activity Limitation). By providing options for action and expression (UDL Principle 2), such as making keyboards available in the classroom, Daniel would have an alternative way to express his knowledge when handwriting is not the goal of learning activity. As shown in Table 1, this strategy would become evident through utilization of UDL Guideline 4: provide options for physical action, specifically the guideline’s checkpoint of optimizing access to tools and assistive technologies. In this way, the UDL framework suggests an environmental change that can enhance Daniel’s ability to meet his academic goals (an aspect of Participation).
The teacher could enhance Daniel’s organizational skills (an Activity Limitation) by providing visual and written reminders about where to store and when to use different class materials; such strategies provide multiple options for representing information (UDL Principle 1) and could be used with all students. Daniel’s organizational skills also could be targeted through application of UDL Guideline 6: provide options for executive functions, specifically the checkpoint involving guiding appropriate goal setting. Table 1 suggests that this could be accomplished by providing Daniel and all students with visual schedules and organizational diagrams to help increase organizational skills.
In summary, Daniel’s needs in multiple ICF domains can be addressed through the environmental interventions suggested in the UDL framework. Increasing relevance and interest of course content may help Daniel tackle learning activities that require attention and sustained effort. Providing access to various tools and assistive technologies (i.e., keyboard) as well as strategies to enhance organizational skills will ensure that learning activities can be more easily achieved by Daniel. Ultimately, these environmental adaptations would positively impact Daniel’s ability to function and participate successfully at school. Thus, while the ICF indicates “what” may need to be targeted by HCPs and educators, UDL provides the “how” by identifying options for environmental interventions and strategies.
Discussion
In considering the example of Daniel, it will no doubt have occurred to the reader that each student will have individualized needs and requirements in the classroom. Thus, how does one reconcile the balance between the needs of one child, such as Daniel, with the needs of the other children in the classroom? The ICF is intended to identify the needs of individual children, while UDL strategies are designed to benefit all, thereby enhancing overall inclusivity within the classroom. Utilization of both frameworks by educators and HCPs could provide different perspectives, enhance knowledge, and increase interprofessional collaboration. HCPs have greater knowledge regarding the ICF and can provide their expertise in classification within the various domains. Educators have greater knowledge regarding UDL and will have knowledge and opinions on different options and strategies. However, through using the frameworks together, we suggest that educators will gain knowledge about the ICF, and HCPs will learn how to utilize UDL strategies. Through collaboration between the professions, the best possible strategies could be determined to increase learning and inclusivity for all students, including students with health and special education needs.
Although we have articulated a conceptually driven position for joint use of the ICF and UDL frameworks in education settings, we fully acknowledge that empirical studies are needed to validate the hypothesized benefits that we have described. However, we also take the position that empirical work is stronger when a strong logical and theoretical foundation is established first. The purpose of this perspective article is to provide that foundation. Certainly, in our own province of Ontario, major initiatives are underway to enhance the integration of health services within school, home, and community (Ontario Ministry of Children and Youth Services, 2016). Moreover, such initiatives are not unique to Canada (e.g., Law et al., 2013; Hutton et al., 2016). Thus, we anticipate that there will be increasing opportunities for the research community to investigate our ideas and determine if they are supported by the evidence.
Summary and Conclusion
The ICF is a holistic framework that serves as a starting point in providing a universal language that promotes communication and collaboration between HCPs and educators to assess students’ needs and describe childhood disability (Allan et al., 2006; Sanches-Ferreira et al., 2013). The ICF provides classification of student needs that relate specifically to functions related to schooling (Simeonsson, 2009). There is a priority for research to identify environmental interventions that can then be utilized to benefit student functioning and performance after classification with the ICF (Florian and McLaughlin, 2008). UDL provides a potential solution for providing environmental support and interventions that may not be specified in the ICF.
With respect to interprofessional collaboration, HCPs possess knowledge of the ICF while educators are familiar with UDL. If both frameworks are utilized in tandem, educators would become more familiar with classification using the ICF and HCPs would become more familiar with environmental strategies available through UDL. Each profession could contribute to determining student requirements and services that would provide an enriching and optimal learning environment for all. Ultimately, we suggest that joint use of the ICF framework to identify areas of student need and the UDL framework to develop inclusive strategies will facilitate “bridging” health care and education in support of the greater goal to create schools where all children belong.
Author Contributions
With respect to individual contributions, VT, a master’s of Rehabilitation Science candidate at McMaster University, developed and wrote the main content of this manuscript. AC, a doctoral candidate in McMaster University’s School of Rehabilitation Science, cowrote and edited parts of the initial paper, and assisted in editing and enhancing the final manuscript. WC provided guidance on the overall content and organization and structure of the paper; assisted with the editing process throughout; and wrote components of the final manuscript. All the authors have consented to the order of authorship and agree to submission of the manuscript in its current form.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Allan, C., Campbell, W. N., Guptill, C. A., Stephenson, F. F., and Campbell, K. E. (2006). A conceptual model for interprofessional education: the international classification of functioning, disability and health (ICF). J. Interprof. Care 20, 235–245. doi: 10.1080/13561820600718139
Campbell, W., Selkirk, E., and Gaines, R. (2016). Speech-language pathologists’ role in inclusive education: a survey of clinicians’ perceptions of universal design for learning. Can. J. Speech Lang. Pathol. Audiol. 40, 121–132.
Campbell, W., and Skarakis-Doyle, E. (2007). School-aged children with SLI: the ICF as a framework for collaborative service delivery. J. Commun. Disord. 40, 513–535. doi:10.1016/j.jcomdis.2007.01.001
Center for Applied Special Technology. (2011a). Universal Design for Learning Guidelines Version 2.0. Wakefield, MA: Center for Applied Special Technology.
Center for Applied Special Technology. (2011b). UDL Guidelines 2.0 – Organizer with Links to Examples. Available at: https://sites.google.com/site/udlguidelinesexamples/home
Center for Applied Special Technology. (2016). About UDL. Available at: http://www.cast.org
Dymond, S. K., Renzaglia, A., Rosenstein, A., Chun, E. J., Banks, R. A., Niswander, V., et al. (2006). Using participatory action research approach to create a universally designed inclusive high school science course: a case study. Res. Pract. Pers. Severe Disabil. 31, 293–308. doi:10.1177/154079690603100403
Florian, L., and McLaughlin, M. J. (2008). Disability Classification in Education: Issues and Perspectives. Thousand Oaks, CA: Corwin Press.
Hellblom-Thibblin, T., Klang, N., and Aman, K. (2013). Biopsychosocial model and the ICF-CY in in-service training: general educators’ reflections. Int. J. Dev. Disabil. 58, 12–19. doi:10.1179/2047387711Y.0000000003
Hollenweger, J. (2011). Development of an ICF-based eligibility procedure for education in Switzerland. BMC Public Health 11:S7. doi:10.1186/1471-2458-11-S4-S7
Hutton, E., Tuppeny, S., and Hasselbusch, A. (2016). Making a case for universal and targeted children’s occupational therapy in the United Kingdom. Br. J. Occup. Ther. 79, 450–453. doi:10.1177/0308022615618218
Law, J., Reilly, S., and Snow, P. C. (2013). Child speech, language and communication need re-examined in a public health context: a new direction for the speech and language therapy profession. Int. J. Lang. Commun. Disord. 48, 486–496. doi:10.1111/1460-6984.12027
Marino, M. T. (2009). Understanding how adolescents with reading difficulties utilize technology-based tools. Exceptionality 17, 88–102. doi:10.1080/09362830902805848
McPherson, K., Gibson, B., and Leplege, A. (2015). Rethinking Rehabilitation: Theory and Practice. Boca Raton, FL: Taylor & Francis.
Meyer, A., Rose, D. H., and Gordon, D. (2014). Universal Design for Learning: Theory and Practice. Wakefield, MA: CAST Professional Publishing.
Missiuna, C. A., Pollock, N. A., Levac, D. E., Campbell, W. N., Whalen, S. D., Bennett, S. M., et al. (2012). Partnering for change: an innovative school-based occupational therapy service delivery model for children with developmental coordination disorder. Can. J. Occup. Ther. 79, 41–50. doi:10.2182/cjot.2012.79.1.6
Ontario Ministry of Children and Youth Services. (2016). Program Guidelines for the Integrated Delivery of Rehabilitation Services: Ontario’s Special Needs Strategy for Children and Youth. Available at: http://www.dsao.ca/wp-content/uploads/2016/07/Program-Guidelines-for-Integrated-Delivery-of-Rehabilitation-Services.pdf
Porter, G. I., and Towell, D. (2017). Advancing Inclusive Education: Keys to Transformational Change in Public Education Systems. Available at: http://inclusiveeducation.ca/2017/04/21/advancing-inclusive-education/
Rose, D., and Strangman, R. (2007). Universal design for learning: meeting the challenge of individual learning differences through a neurocognitive perspective. Univ. Access Info. Soc. 5, 381–391. doi:10.1007/s10209-006-0062-8
Rosenbaum, P., and Gorter, J. W. (2012). The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev. 38, 457–463. doi:10.1111/j.1365-2214.2011.01338.x
Sanches-Ferreira, M., Simeonsson, R. J., Silveira-Maia, M., Alves, S., Tavares, A., and Pinheiro, S. (2013). Portugal’s special education law: implementing the international classification of functioning, disability and health in policy and practice. Disabil. Rehabil. 35, 868–873. doi:10.3109/09638288.2012.708816
Simeonsson, R. J. (2009). ICF-CY: a universal tool for documentation of disability. J. Policy Pract. Intellect. Disabil. 6, 70–72. doi:10.1111/j.1741-1130.2009.00215.x
Stewart, D., and Rosenbaum, P. (2003). The International Classification of Functioning, Disability and Health (ICF): A Global Model to Guide Clinical Thinking and Practice in Childhood Disability. CanChild Keeping Current. Available at: http://canchild.ca
Thompson, S. A., Lyons, W., and Timmons, V. (2015). Inclusive education policy: what the leadership of Canadian teacher associations has to say about it. Int. J. Inclusive Educ. 19, 121–140. doi:10.1080/13603116.2014.908964
Timmons, V., and Wagner, M. (2009). Inclusive education knowledge exchange initiative: an analysis of the Statistics Canada participation and activity limitation survey. Can. Counc. Learn. Available at: http://en.copian.ca/library/research/ccl/inclusive_edu_know/inclusive_edu_know.pdf
Towle, H. (2015). Disability and inclusion in Canadian education: policy, procedure, and practice. Can. Centre Policy Altern. Available at: https://www.policyalternatives.ca/publications/reports/disability-and-inclusion-canadian-education
World Health Organization. (2001). International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization.
World Health Organization. (2002). Towards a Common Language for Functioning, Disability and Health. Geneva: World Health Organization.
Keywords: Universal Design for Learning, the International Classification of Functioning Disability and Health, universality, accessibility, inclusive education, conceptual framework
Citation: Tomas V, Cross A and Campbell WN (2018) Building Bridges Between Education and Health Care in Canada: How the ICF and Universal Design for Learning Frameworks Mutually Support Inclusion of Children With Special Needs in School Settings. Front. Educ. 3:18. doi: 10.3389/feduc.2018.00018
Received: 12 January 2018; Accepted: 01 March 2018;
Published: 19 March 2018
Edited by:
Brahm Norwich, University of Exeter, United KingdomReviewed by:
Tracey Colville, City of Edinburgh Council, United KingdomTaryn Moir, North Ayrshire Council, United Kingdom
Copyright: © 2018 Tomas, Cross and Campbell. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenonah N. Campbell, Y2FtcGJlbHdAbWNtYXN0ZXIuY2E=