Abstract
Children with developmental disorders affecting learning and behaviour (DDALB) (e.g., attention, social communication, language, and learning disabilities, etc.) require individualized support across multiple environments to promote participation, quality of life, and developmental outcomes. Support to enhance participation is based largely on individual profiles of functioning (e.g., communication, cognitive, social skills, executive functioning, etc.), which are highly heterogeneous within medical diagnoses. Currently educators, clinicians, and parents encounter widespread difficulties in meeting children’s needs as there is lack of universal classification of functioning and disability for use in school environments. Objective: a practical tool for functional classification broadly applicable for children with DDALB could facilitate the collaboration, identification of points of entry of support, individual program planning, and reassessment in a transparent, equitable process based on functional need and context. We propose such a tool, the Functional Abilities Classification Tool (FACT) based on the concepts of the ICF (International Classification of Functioning, Disability and Health). FACT is intended to provide ability and participation classification that is complementary to medical diagnosis. For children presenting with difficulties, the proposed tool initially classifies participation over several environments. Then, functional abilities are classified and personal factors and environment are described. Points of entry for support are identified given an analysis of functional ability profile, personal factors, environmental features, and pattern of participation. Conclusion: case examples, use of the tool and implications for children, agencies, and the system are described.
Introduction
A universal classification system for children with developmental disorders affecting learning and behaviour (DDALB) currently does not exist in school systems, or anywhere (Sutherland et al., 2008; Rutter, 2011; Ysseldyke et al., 2017). The impact of this on service delivery (and presumably outcomes) for this large and heterogeneous group of students, their families, education systems, and society is substantial (Florian et al., 2006). DDALB are among the most prevalent presentations in child health and include communication, emotional–behavioural, cognitive, and learning problems (Horridge et al., 2016). These children may be labeled with diagnoses such as attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), learning disability (LD), oppositional defiant disorder (ODD), emotional and behavioural disorders, and others.
In the school environment, DDALB are associated with a developmental cascade of poor psychosocial outcomes for many children (Lansford et al., 2010; Dombrowski and Gischlar, 2014; Portilla et al., 2014). As the global child and adolescent mental health crisis mounts (Patel et al., 2007), it is clear that addressing child functioning and participation in the critical environment of school is of the utmost importance. This article describes the proposed tool, the Functional Abilities Classification Tool (FACT), that focuses on operationalizing the concept of functioning from the International Classification of Functioning, Disability, and Health (ICF) (World Health Organization, 2001, 2002) for use in the school environment for children with DDALB. This is meant to serve as a practical approach to identifying points of entry for supporting participation and optimizing development of skills.
Sorting, categorizing, and labeling is a necessary function of special education in order to decide which students require additional supports (Kauffman et al., 2017). Currently, the predominant method of achieving this utilizes categorical medical or psychological diagnoses [e.g., as found in the Diagnostic and Statistical Manual fifth edition (DSM) (American Psychiatric Association, 2013)]. Disability diagnoses are generally diagnosed by the medical model, even though we recognize that disability is not purely a medical condition, but rather the result of a complex relationship between an individual’s functioning and environment (Leonardi et al., 2006). Nonetheless, they continue to be diagnosed primarily based on symptoms and deficits in functioning in the child. The term developmental disability itself is vague, sometimes used to refer specifically to Intellectual Disability or as an umbrella term for all disabilities.
Classification solely by medical categorical diagnosis does not provide sufficient information to inform supports for individual students (Eze et al., 2013; Bolte et al., 2014). Medical or psychological diagnosis itself has been found to be a poor predictor of participation in individuals with DDALB compared with personal and environmental factors (Almqvist and Granlund, 2005; Anaby et al., 2014). The heterogeneity of functional abilities within and across standard DDALB categories such as ADHD, ASD, learning disorders, etc. is tremendous (Lee, 2011). For example, in a child with ASD, categorical diagnosis alone does not capture the variability of social communication ability (a core feature) nor for cognitive and executive functioning (non-core ASD features.) Furthermore, categorical diagnoses fail to capture the effect of multiple sub-diagnostic weakness, child–environment interactions, and problems without well-defined diagnostic categories (e.g., self-regulation impairments, the effects of early childhood trauma).
Although categorical diagnosis may serve as a broad starting point, supporting students demands us to understand abilities and needs using terminology that is understandable across disciplines and stakeholders. Furthermore, support for children with DDALB is not specific to medical or psychological diagnosis, but rather depends on the relationship of a child’s abilities to the features of the environment (e.g., demand on functional skills, physical features, attitudes, etc.) (Bates et al., 2006; Lillvist and Granlund, 2010; Garner, 2016; Foster-Cohen and Mirfin-Veitch, 2017). For example, the label of LD does not guide specific instructional practices for an individual student (Kauffman et al., 2017). As Ruppar et al. (2017) notes, “teams should resist assigning fulltime, one-to-one paraprofessionals based on disability labels, and instead carefully examine the specific areas in which the student requires extensive supports, and when natural supports can be leveraged.” However, no standard framework currently exists to act upon these concepts.
The field of disability has shifted its focus to a transactional, dimensional-based biopsychosocial approach, focusing on functioning and participation in individuals with disabilities (Rosenbaum et al., 2014). The advantages of dimensional profiles complementary to categorical diagnosis have been described (Hudziak et al., 2007). However, optimizing participation for children with DDALB remains widely problematic (Ysseldyke et al., 2017). We continue to encounter an inconsistent array of diagnostic and descriptive terminology. Without common language or framework, there is no starting point or process to move forward. Not surprisingly, communication and collaboration between community and school practitioners and parents is often challenged and care fragmented (Ritzema et al., 2014). It has been found that teachers generally do not feel that they have the knowledge or skills to plan inclusive environments for students with disabilities (Ruppar et al., 2017). As we will discuss in more detail, the potential of the biopsychosocial framework of ICF to address this problem has been extensively noted, although met with challenge to operationalize (Aljunieda and Frederickson, 2014).
“Behaviour”: A Sign, Not a Diagnosis
Behaviour requires specific mention because of its misunderstood nature and devastating consequences for many children with DDALB. The word behaviour is intended as neutral and objective; however, it often takes on the meaning of bad behaviour, even volitional or premeditated. Challenging behaviour is a frequent non-specific final common pathway of problematic child–environment interactions. Disruptive behaviour should not be considered a diagnosis, but rather a sign of an overwhelmed biopsychosocial system that may have multiple contributing (transactional) factors. Disruptive behaviour is, therefore, a symptom of a stressed system pointing to a problematic interaction of the individual and environment (Bates et al., 2006).
Children (humans) have a finite ability to control behaviour in the face of stress (i.e. self-regulation). This may be a relative developmental weakness compared to a child’s other abilities (or the general population). When the load of stress on a child’s system exceeds self-regulation ability the brain can automatically switch from a calm, alert mode to a fight-or-flight mode. Symptoms of this state may include aggression, anxiety, withdrawal, flight, and hyperactivity. Essentially involuntary behaviours in young children in a dysregulated state (e.g., a tantrum) can mislead caregivers to the level of intentionality in the child. This can lead to a vicious cycle (Turecki, 2000) of hostile caregiver affect, more stress, further overwhelmed self-regulation ability (Shanker, 2012; Portilla et al., 2014), and entrench maladaptive patterns of responses. Diagnoses centred only on the child such as ODD do not capture the complete picture and may further damage child–caregiver relationships by bolstering the belief that the child’s problem is willful (Walter et al., 2006).
Defining and classifying the population of school-age children with an emotional or behavioural disorder is a critical problem in education, particularly as it relates to special education services (Forness et al., 2012). This challenge is not surprising given that emotional and behavioural phenomena are dimensional variables, continuous between typical and atypical, and can be non-specific to multiple problems (e.g., adjustment difficulties to social stressors or academic failure). Self-regulation as a developmental ability can be challenging to assess. Disability in self-regulation is common and indistinguishable among many medical diagnoses (e.g., effect of antenatal alcohol, trauma, genetic conditions, ADHD, etc.) (Malone and Koren, 2012). Behaviour expectedly occurs in typically developing children. This needs to be distinguished from problems of clinical significance in the child–environment interaction. There is no standardized tool to directly measure self-regulation, but rather we depend heavily on the subjective collateral histories of parents, teachers, and others.
ICF as a Conceptual Framework for a FACT
The ICF aims to provide a standard language and framework for the description of health and health-related states (p. 3) (World Health Organization, 2001). The ICF is a biopsychosocial approach that defines disability as the result of the relationship between an individual’s health condition, personal factors, and environmental (external) factors (p. 17) (World Health Organization, 2001). For example, a child with language delay (i.e., function) has difficulty with activities such as playing with peers (i.e., participation, environment), tends to withdraw when frustrated (personal factor), losing opportunities (participation) for the developing brain (body structures) and falls further behind in social and language development (functions). ICF is meant to be used clinically for assessment, goal setting, treatment planning, monitoring, and outcome measurement (Kraus de Camargo, 2010; Lee, 2011; Bartlett et al., 2016), as well as for research, education, and social policy (p. 5) (World Health Organization, 2001). The International Classification of Functioning, Disability and Health Children and Youth Version (ICF-CY) is a classification derived from the ICF with expanded coverage to encompass data specific to children and adolescents (p. xi) (World Health Organization, 2007).
The construct of participation in the ICF has been recognized as the ultimate health outcome (Adair et al., 2015), although it has not yet been firmly defined (Imms et al., 2016a). The ICF defines participation restriction as “problems an individual may experience in involvement in life situations” (p. 123) (World Health Organization, 2001). Imms et al. (2016a), describe participation in terms of attendance (i.e., physically being part of an activity) and involvement (i.e., quality of connectedness with an activity), as objective, observable aspects of participation. Optimizing positive participation is considered the most important treatment and outcome for most children (Imms et al., 2016b) and has been evaluated for use in individual child support planning, agency program development, and population research (Coster et al., 2013). There is an increasing realization that service delivery based on functioning and participation considerations (rather than diagnostic labels) is more appropriate in a system supporting individuals with disabilities (Benson and Oakland, 2011).
The use of objective measures of functioning and participation based on the concepts outlined in the ICF hold great promise to be developed into practical tools to inform supports in all children with disabilities (Wright, 2015). Functional classification systems are already standard in the field of cerebral palsy (i.e., Gross Motor Function Classification System and Manual Abilities Classification System) (Rosenbaum et al., 2014). Tools to measure functional abilities related to DDALB have been developed (Simeonsson et al., 1995; Bates et al., 2006; Greenspan and Wieder, 2008; Castro and Pinto, 2015); however, widespread practical implementation (e.g., in schools) continues to present a challenge. The exhaustiveness of the ICF itself limits applicability for this purpose (Berry and O’Connor, 2009). To address this, the development of ICF Core Sets aim to describe functioning of specific diagnostic populations, such as cerebral palsy or ASD (Stucki and Grimby, 2004; Bolte et al., 2014). In our opinion, this approach does not address the many difficulties involved in relying on categorical medical diagnosis in DDALB as described above. To our knowledge, this has not been attempted in a broad population such as children with DDALB, many of whom face a systems barrier of not having a unifying diagnosis that can qualify a child for services.
The School Function Assessment (SFA) (Davies et al., 2004) involves a standardized questionnaire completed by teachers and other school based staff that measures elementary students’ participation, skills, and supports in place. The SFA is meant to be used for screening, program planning, and reevaluation. Skill performance in activities in 21 different areas between two sections covering academic, social, and adaptive school-related activities is scored out of four (none, partial, inconsistent, and consistent performance) and each has multiple questions. Participation is rated in six settings on a six-point scale. Supports are measured in terms of both assistance and adaptations over 18 areas (West et al., 2014). The Participation and Environment Measure for Children and Youth (PEM-CY) (Coster et al., 2012) is a questionnaire-based tool (Coster et al., 2011) for a broad range of children with and without disability. PEM-CY includes questions on participation frequency (how often) and quality (how involved) on 0–7 and 1–5 point scales, respectively (Coster et al., 2013). The Child Participation Questionnaire entails parent report on intensity, independence level, and enjoyment of a child’s participation and parent satisfaction on scales of 1–5 or 1–6 (Rosenberg et al., 2010). The Child and Adolescent Scale of Participation (CASP) is a questionnaire-based tool that has been validated in a broad range of DDALB, including intellectual disability and acquired brain injury (Bedell, 2009). The Child and Adolescent Functional Assessment Scale involves a rater selection of severity from 165 behavioural descriptions (Bates, 2001).
In summary, standardized, validated tools have emerged to describe functioning and participation in children with disabilities based on the principles of ICF (2002). However, to our knowledge, there does not exist a comprehensive tool in widespread usage in schools that measures both abilities and participation in the population of children with DDALB. In this article, we discuss possible reasons for this and propose a novel ICF-based tool that includes classification of participation and function in children with DDALB with a focus on the school environment.
A Proposed FACT
In this section, we outline the use of the proposed FACT (see supplementary material). The FACT is a concept that is based on the biopsychosocial framework of the ICF and builds on other classifications, as mentioned above. No formal use or validation has been done with the FACT. The FACT uses a strength-based approached to classify abilities, participation to classify outcomes, and describes environment as a critical modifiable variable within which entry points of support are identified (Anaby et al., 2014) The authors constructed the FACT a priori informed by scientific literature as well as experience working with multidisciplinary teams in schools, hospitals, rehabilitation centres, and mental health facilities in the region of Southern ON, Canada, including the urban and rural catchment areas of over 1 million people.
In the authors’ observation, much time is spent in multidisciplinary meetings describing symptoms based in the child rather than broader child-context systems. Of particular note are many children with severe adaptive functioning problems but not meeting criteria for relatively well-resourced categories such as ASD or Intellectual Disability. In our observation, children with ability weaknesses in social-emotional and executive functioning development (usually without a unifying diagnostic label) are most likely to present challenges to program planning teams. There is often a palpable frustration at the table related to the distribution of resources (i.e., who gets what), straining parent–school relationships and often spilling into child–family interactions.
A traditional focus on symptoms (e.g., behaviour) in attempts to help struggling children is understandable, since medical diagnosis (upon which special education categories are heavily based) mostly relies on symptom clusters. However, as noted recent literature is clear that the usual diagnostic categories are of limited use in constructing individual plans of support. We propose a new tool to fill this gap that describes profiles of abilities (i.e., “what can this student do?” rather than “what does this child have?”) and centres on participation as the key variable for determining success. In the following sections, we outline the terminology and process of the proposed FACT. A core issue of the classification tool is simplifying categories enough to avoid obscuration in numbers or description (e.g., standard scores, many categories of function), but not be so vague as to have questionable meaning (e.g., mild, moderate, severe).
Objectives of the FACT
The main objectives of the FACT are to provide a snapshot of a child’s current situation in terms 1. participation across school contexts, 2. a comprehensive summary of the child’s abilities, 3. personal factors, and 4. the child’s environmental contexts in the school. This information is meant to be complementary to categorical medical or psychological diagnosis (e.g., ASD, LD, etc.). The FACT aims to outline a system for identification of needs and points of entry of support for individual students. We make the assumption that mismatches in functioning–environment interactions are central to participation restrictions and that environment or context is the primary point of entry for planning supports. Furthermore, The FACT is flexible in allowing individual needs (e.g., complexity of child presentation), local resources (e.g., funding for assessment), and available expertise determine the data required to complete the FACT. The FACT classifies an individual child’s functioning using a flexible summary of data from observation, standardized testing, history taking and clinical assessment.
The FACT is constructed for conciseness, ease of use, and broad applicability. A child’s profile of abilities and participation across core school contexts is highlighted in order to lead to points of entry for support. For instance, a finding of relative strength in visual cognitive abilities may suggest visual augmentative communication to address a participation restriction in an environment with heavy verbal demands. The FACT identifies core abilities that are common to the gamut of children with DDALB (with or without a medical diagnosis) using terminology that can be meaningful across stakeholders, including general education staff, school administrators, and parents. In the school setting in particular, we suspect that a common approach to classifying relevant data will result in more efficient, effective and satisfying experiences for all involved (for example, as a basis to structure a multidisciplinary meeting at school in support of a child with participation restrictions).
Terminology Used in the FACT
Functional Abilities
The construct of functional abilities proposed by the FACT draws from previously described activity, capability, performance, and capacity terminology that we review briefly. ICF-CY (World Health Organization, 2007) defines activity as the execution of a task and participation as involvement in a life situation (p. 129). ICF-CY defines performance as what a person does do in usual circumstances and capacity as what people can do at their best or according to standardized situations (p. 129). Capability has been defined as what a person can do in specific situations (Holsbeeke et al., 2009).
The FACT proposes the term functional abilities as a child’s expected use of skills in a typical environment without special support. In other words, a child’s functional ability level is an estimation of how much support a child would be expected to require in order to participate within typical limits. The proposed functional abilities construct in the FACT sets out to link classification of functioning to entry points of support. As has been noted, the ICF definitions do not clearly differentiate activity from participation and this issue has not been resolved (Whiteneck and Dijkers, 2009).
The FACT imagines each functional ability domain in terms of capacity (i.e., ideal or standardized conditions), however, recognizes that skills in children often cannot be tested in ideal, standardized conditions (e.g., due to multiple interacting areas of weakness), or are not readily directly testable (i.e., self-regulation, executive functioning, social skills). Certain functional ability domains are, therefore, more likely to be informed by capability assessment (i.e., observation in the naturalistic environment or by report), rather than direct capacity testing. The FACT classifies levels of functional abilities in a single snapshot that blends of capacity and capability assessment into the best estimate of what a child can do in each domain. This is primarily meant to allow determination of skills–environmental demand gaps that can be targeted as entry points for support.
Functional Ability Domains
Functional ability domains of the FACT include verbal communication, visual cognitive, social skills, executive functioning, self-regulation, and for school-aged children, literacy. The specific functional ability domains included in the FACT were informed through review of domains that are repeatedly identified in the literature as important to child functioning. The number of functional ability domains was determined as a balance of sufficient detail without an unwieldy number of domains. The paradigm was a vision of maximal usability at a multidisciplinary case conference at school. We note that specialists may necessarily see these domains and levels as a simplification. We believe that some degree of simplification is unavoidable in a tool that is practical and informative to all professional service providers (e.g., non-specialist physicians, teachers, therapists of varied disciplines), among whom it is imperative to use a common language.
Verbal Communication, Visual Cognitive, and Literacy
Verbal communication and visual cognitive as functional ability domains are self-evident. They are amenable to direct standardized testing in most children from late preschool equivalent levels of functioning. Verbal communication includes receptive language, expressive language, articulation, verbal knowledge, vocabulary, verbal reasoning, etc. Visual cognitive includes visual perceptual abilities, nonverbal fluid reasoning, etc. Literacy is the functional ability domain used when children are typically expected to participate in such activities and is defined as the ability to fluently read, understand, and express written language.
Executive Functioning, Self-Regulation, and Social Skills
Social, emotional and behavioural competencies are crucial for success in the classroom (Andrews et al., 2001; Rosenberg, 2015) and are interrelated (Kilgus et al., 2017; Ysseldyke et al., 2017). Supports in these domains may be required for some students to make the age appropriate academic skill gains of which they are capable (Ysseldyke et al., 2017). There are many examples of literature and methods available to aid school personnel in supporting student executive functioning (Dawson and Guare, 2003), self-regulation (Shanker, 2012; Woodward et al., 2017), and social skills (Reid et al., 2007; Frankel and Whitham, 2011).
However, these domains are harder to define and less amenable to direct measurement (i.e., as opposed to IQ scores), as Foster-Cohen and Mirfin-Veitch (
2017) noted that:
“Removing barriers to learning that come not from the challenges of the curriculum itself (although these may also exist), but from socio-emotional and organizational issues that limit access to the curriculum should be of the utmost importance if we are to promote the capabilities of young children in school.”
The FACT defines social skills as the ability to interact successfully with others (Vaz et al., 2015), including the social developmental milestones of play (e.g., independent, parallel, interactive, functional, symbolic, imaginary), understanding and use of humor, sarcasm, non-literal language, body language, facial expressions, gestures, and culturally appropriate social conventions such as greeting, sharing, and the to-and-fro of social interactions.
Executive functioning is the ability to plan, organize, and persist with tasks; and focus, shift and inhibit attention according to demands. Executive functioning is expected to come into play particularly with novel, multistep tasks, working in groups and in busy environments with a high level of extraneous stimuli. Executive functioning has been found to be an important contributor to children’s participation (Rosenberg, 2015).
Self-regulation has been described as the ability to volitionally plan and modulate behaviour for adaptive purposes (Montroy et al., 2016). Self-regulation is also depicted in physiologic terms as the stress regulation system (i.e., hypothalamic–pituitary–adrenal axis, limbic system–cortex, etc.) (Zeman et al., 2006). Emotional stress dysregulation is associated with the fight-or-flight response, which can manifest as internalizing or externalizing problem behaviour. Self-regulation as a functional ability in the FACT is defined as the ability to maintain emotional–behavioural regulation in the face of environmental stressors such as unpredictability, lack of control, failure, hostility, boredom, being told “no,” sensory input, etc. (Zeman et al., 2006; Shanker, 2012).
Functional Ability Levels
The proposed FACT identifies four levels for each functional ability domain. The level of classification is based on the expected use of skills to confer a described level of participation in a typical environment. Level 1 describes a functional ability that allows a child to participate to a reasonable extent in a typical environment without any special support. Level 2 describes a functional ability that allows participation intermittently or with partial involvement in a typical environment, without any special support. Intermittent or low intensity supports are expected at Level 2 to attain participation within typical limits. Level 3 describes a functional ability level that allows participation a minority of time and with partial involvement. Continuous (or near continuous) and/or high intensity supports are expected at functional ability Level 3 to attain participation within typical limits. Level 4 describes a functional ability that even with continuous, intensive support would not result in meaningful participation in the intended activities, and would, therefore, require significant modification of the task or environment.
Distinguishing between Functional Ability Levels
Level 2 is distinguished from Level 1 by the expected need for any special support beyond what would typically be required to allow a child’s reasonable participation. Level 3 is distinguished from Level 2 by the expected intensity and frequency of the support needed to bring participation into typical limits in a typical environment. For example, literacy Level 2 may require extra time and intermittent cueing of words, whereas Level 3 requires significant ongoing adaptions, accommodation, and modifications, such as the use of text to speech technology or augmentation of text with graphics to learn material in a typical environment. Level 3 is distinguished from Level 4 in that intensive and or continuous support allows the child to participate in the intended typical peer activity, whereas children at Level 4 require a significant modification of environment or task, often in addition to intensive support.
There is significant debate regarding the meaning of full access to the general curriculum for students with disabilities (Ruppar et al., 2017). A child with Level 4 functional ability, according to the FACT by definition means that full participation is not attained in typical environments for the purpose of that functional ability domain. This does not mean that a child with a Level 4 classification in one or more domains would be automatically expected not to be able to participate in some typical peer environments with supports. However, a child with Level 4 classifications in functional ability domains would generally not be expected to achieve participation in many typical activity contexts that depend on the functional abilities in question. For example, a 10-year-old child with severe to profound Intellectual Disability would not be expected to be able to participate fully in most developmentally typical school activities due to functioning impairments in all domains, even with unlimited supports in place. It is clear that children with abilities so discrepant from typical students necessitate alternative environment or highly modified activities for a significant part of an academic curriculum. Not all such special education teaching can be provided in general education classrooms (Kauffman et al., 2017). There is a danger here that a level 4 functional ability will be used as a pretext to inappropriately exclude a child from an environment when supportive measures could achieve successful integration. In such as case, the child’s functional ability would by definition be level 3, not level 4. The authors contend that this should not occur when the FACT is used properly.
Consideration of Standardized Testing Results in Functional Abilities Classification
The FACT does not set strict standardized testing score cutoffs for levels of classification, but rather encourages special educators and clinicians to apply the best judgment to available assessment results. As noted by Kauffman (Kauffman et al., 2017), “special education should involve the most objective and helpful criteria possible for sorting, categorizing, and labeling, but it is extremely unlikely that anyone will ever find a means of eliminating all subjectivity from these necessary processes any more than the subjectivity that exists in psychological and psychiatric evaluations can be eliminated.” Thus, the FACT proposes functional ability levels based on an amalgam of objective information and professional judgment considering history, observation, and standardized assessment. As a general guideline in terms of standardized assessment, functional ability classification levels may often correspond to the following approximate percentiles: less than 1st percentile to 10th percentile for Level 4; 5th to 15th percentile for Level 3; 10th to 25th percentile for Level 2; 20th to 25th percentile and above for Level 1. It should be emphasized that the FACT considers standardized testing as a valuable component of assessment. However, we acknowledge limitations in direct testing, including variable resources available for testing, evolution of child abilities over time, measurement error, child–environment interactions, difficulties in the direct testing of certain abilities (e.g., self-regulation, executive functioning), etc. (Bagnato, 2007; Simeonsson, 2007). This prompts us to emphasize overall impression of a child’s functional abilities given available information while interpreting available testing results.
Consideration of Age Norms in Functional Abilities by Age and Domain (Developmental Milestones)
As mentioned, functional ability classification may include standardized testing, informal testing, naturalistic observation, and history taking (preferably from multiple collaterals). In general, a developmental milestone inventory itself is limited by several factors. Skills often appear gradually rather than in discrete stages. There is significant variation in timing that would be considered within normal limits. It is difficult to separate domains of functional abilities, since many observable life situations require multiple skills. For example, a child may have the verbal communication ability to understand a set of instructions; however, executive functioning may limit ability to remember and organize the steps. Furthermore, executive functioning and self-regulation are considered closely related constructs (Montroy et al., 2016).
Nonetheless, clinicians generally have a working understanding of skills as they occur typically across chronological ages from clinical experience and utilize the many developmental trajectory references available in the literature (Dosman et al., 2012; Kliegman et al., 2016; Scharf et al., 2016). The need for a comprehensive assessment in addition to milestone history taking is clear.
Environment
The ICF defines environment as factors that make up the physical, social and attitudinal environment in which people live and conduct their lives (p. 10). Environment shares a transactional relationship with a child’s functioning and participation (Coster et al., 2012). The school environment includes the physical classroom layout (e.g., seating arrangement, facilities, space for play, entrance and corridors that are used for transitions), the primary location of instruction or placement (e.g., inclusive or specialized classroom) (Ruppar et al., 2017), the teacher (e.g., way of speaking, interacting, organizing, and providing instruction and feedback), schedule of specific activities, content of work, peer behaviour, general attitudes and any special supports the child receives, peer supports, adaptations, accommodations, modifications, and material supports (e.g., technology, visual supports). The social environment including peers and teachers can have a significant impact on social and academic participation for students with disabilities (Tsai and Cheney, 2012; Cameron and Cook, 2013; White, 2016; Ruppar et al., 2017). The sensory environment may be described as all the visual, auditory and tactile elements in the classroom and school (Kuhaneck and Kelleher, 2015).
Students with disabilities have been found to interact less with the school environment, including the teacher, other students, and classroom activities (McIntosh et al., 1993; Selanikyo et al., 2017). Interactions between children with DDALB and their environments at school are complex and not fully understood (Sutherland et al., 2008; Vaz et al., 2015). Children with disabilities tend to engage cooperatively less at school than children without disabilities (Hestenes and Carroll, 2000) and can elicit reactions from the school environment. For example, it has been found that children with mild disabilities of learning and behaviour (including working memory, motor planning, auditory processing, self-regulation, and attention) are more often rejected by teachers than children with severe disabilities (Cameron and Cook, 2013).
Successful supports in the classroom environment may allow students with DDALB to develop skills and increase a sense of self-efficacy, promoting increasing participation in a positive cycle (Almqvist and Granlund, 2005). There are multitudes of possible supportive measures targeting participation for children with disabilities in school, although the evidence base is still emerging (Adair et al., 2015). Social environments at school such as recess and play can be supported to enhance interactions for children with problems in social skills (Fantuzzo et al., 1996; Harper et al., 2008). Specific environmental supports can have variable effects on individual students’ participation. For example, as Giangreco (2010) notes, the support of a one-to-one educational assistant can have negative impacts, such as dependency, stigmatization, and decreased interaction with peers and the teacher. Instructional practices can also be variably effective depending on students’ skill levels at the time of delivery (McDonald Connor et al., 2004).
The environment section of the FACT is descriptive. The process of recording the environmental features is not strictly defined because specific practices are expected to vary widely (i.e., across schools and education professionals) due to the complexity of child–environment interactions at school. The FACT review of environment includes a child’s schedule of activities, physical locations and a detailed account of supports in place including specific communication, tools and other actions used by teachers and paraprofessionals to support the individual student. As the principal entry point of support, we cannot overemphasize the need to obtain a detailed account of child’s environment with an eye to opportunities for supportive changes such as teacher interactions, peer support, adaptations, accommodations, etc. (Poulou, 2014; Schulte-Korne, 2016).
Personal Factors
According to the ICF, personal factors are “contextual factors that relate to the individual such as age, gender, social status, life experiences, and so on” (p. 214) However, personal factors is not classified in the ICF and its purpose in general is controversial (Simeonsson et al., 2014). Nonetheless, personal factors have been recognized as important to optimizing functioning and participation (Rosenbaum and Gorter, 2012). For example, a child’s individual preferences can interact dramatically with their ability levels, such as in self-regulation and executive functioning (Baum and Olenchak, 2002). There has been debate regarding the concept of standard classification of personal factors for improving assessment and service planning (Geyh et al., 2011; Leonardi et al., 2016).
The personal factors section of the FACT is descriptive given the state of the literature (Kraus de Camargo, 2016), particularly with respect to its application in education (Geyh et al., 2011). The FACT uses a definition of personal factors that includes personal preferences, interests, as well as family and cultural information. Additional psychosocial factors, including availability of supportive parents, family composition and functioning, and economic resources, obviously can have implications for individual students’ plans of support at school (Greenham et al., 2015). For example, foster care placement is a risk factor for challenges across academic, social, and behavioural domains (Palmieri and La Salle, 2017).
The FACT additionally includes personality or temperament traits in personal factors, noting that ICF-CY categorizes “dispositions and intra-personal functions” (p. 48), including adaptability, responsivity, activity, predictability, persistence, and approachability (p. 48), and “temperament and personality functions” (p. 49) in the body function section. We argue that for purposes of the FACT, temperament and personality are best used as descriptors regardless of ability level. For instance, a student may have a negative “responsivity” (p. 125) or low “extraversion” (p. 126), despite typically developed social skills and adequate social participation. Such personality or temperament traits can help inform supports. For example, transitions between activities can be made more gradual for students with low adaptability, or academic activities more appealing by incorporating personal interests of the child. Additionally, students’ personality has been found to be associated with relationships with teachers and academic progress (Zee et al., 2013). Incorporating knowledge of students’ positive relationships with individual teachers may be helpful for support planning. Of note, the ICF-CY remarks that “the taxonomic properties of these codes and their relationship need to be developed through research” (p. 46).
Participation
ICF defines participation as “involvement in life situations” (p. 123) and participation restrictions as “problems an individual may experience in involvement in life situations” (p. 123). As discussed, validated tools such as PEM-CY and CASP operationalize participation into a strength-based (Rashid and Ostermann, 2009) classification approach. The FACT draws on this work in proposing a four-level participation measure to be used in each school context or environment. These environment domains include individual skill-based work (reading, writing, math), project (or multistep task), student-directed group work, teacher-directed group instruction (e.g., circle time, question and answer), unstructured group activity (e.g., lunch), unstructured group physical activity (e.g., recess), and structured group activity (e.g., physical education). The environments were chosen as self-evident situational archetypes in which children are expected to participate in school. Implicit in the environmental domains are demands for different combinations of functional abilities (e.g., language skills in teacher led instruction; verbal, executive functioning, self-regulation and social skills in group work, etc.) that may provide clues to points of entry for support.
The participation classification in the FACT is meant to be completed by teachers or other educational staff who are familiar with the child across school activities. Although subjective participation measures (i.e., child report) have been discussed in the literature (Whiteneck and Dijkers, 2009), the FACT uses only proxy measures (i.e., teacher report) because of age and practical data collection considerations. Participation is expected to fluctuate over time (and hopefully improve with supportive measures put in place as a result of the process).
The FACT assumes that participation will vary across environments as a function of a student’s functional abilities, personal factors and the unique components of the child’s environments. A student’s participation profile is expected to yield important clues about functional abilities that do not meet contextual demands and, therefore, what type of additional support may be helpful. For example, consistent difficulties in unstructured group situations is suggestive of self-regulation, executive functioning or social skills support requirements for cueing or modelling skills, or increasing the structure or supervision of the activity.
Participation Levels
The FACT classifies participation in four levels (similar to the CASP) (Bedell, 2009). We emphasize level of participation as the child’s actual involvement regardless of presumed ability level (i.e., does or does not regardless of can or cannot). Level 1 indicates adequate participation; Level 2 indicates participation most of the time with gaps in attendance and/or involvement; Level 3 indicates a minority of time participating and consistently lower level of involvement than expected; Level 4 indicates the child is essentially not meaningfully participating in expected activities (all the time or most of the time).
Distinguishing between Participation Levels
Level 2 is distinguished from Level 1 by the frequency and/or degree of involvement of participation. Level 3 is distinguished from Level 2 in that the frequency and involvement of participation is significantly lower than expected. Level 4 is distinguished from Level 3 in that participation is obviously different in involvement compared to typical peers, and very infrequent or non-existent.
Proposed Process of Using the FACT
Classification of Participation
The initial step of the FACT is to classify levels of participation across environments in children who present with difficulties in participation, for example, manifesting as challenging behaviour. Participation classification is completed by educators who know the child well (e.g., teacher) for individual work tasks (e.g., reading, writing, math), multistep tasks, teacher-led instruction, group work with peers, structured group physical activities (e.g., physical education, gym), unstructured group physical activities (e.g., recess), and unstructured time in groups (e.g., lunch).
Classification of Functional Abilities
Once participation has been classified, the FACT classifies functional abilities. As discussed, FACT identifies domains of functional abilities as communication (i.e., verbal, language), visual cognitive (i.e., nonverbal cognitive), social skills, executive functioning, self-regulation (i.e., emotional stress regulation), and for school-aged children, literacy.
Clinicians and/or special educators complete the functional abilities classification in domains pertinent to their practical areas of expertise. The functional ability domains may be completed using a transdisciplinary approach, in which individuals combine their expertise (Ruppar et al., 2017). For an individual child, there may exist sufficient documentation of recent assessments and observations such that no additional direct assessment of functional abilities is required at the time of functional abilities classification. For example, a special education teacher may review recent reports from psychology, speech language pathology, occupational therapy, as well as questionnaire information from parents and teachers to arrive at functional ability levels. Alternatively, a child may have had very little or no formal assessment and require significant additional direct assessment. Gaps in information regarding specific functional abilities should prompt targeted assessment until sufficient data are obtained to confidently inform levels of classification. The degree of complexity of an individual child’s functioning should direct the required extent of assessment required to complete the FACT. Data gathering, therefore, will depend on the individual child as well as special educators’ or clinicians’ practice, and may include a variable array of direct assessment, including observation, clinical assessment, and standardized (e.g., psychometric) testing.
Identification of Points of Entry for Support and Goal Setting
Participation classification across contexts is compared to functional abilities classification, personal factors, and description of a student’s current program (i.e., environment). This is expected to yield insights regarding possible points of entry for support to improve participation (Rosenbaum and Gorter, 2012). Individual support planning in education based on participation has emerging support (Adair et al., 2015) and has been carried out successfully in community settings (Khetani et al., 2014). The FACT encourages a collaborative process between teachers and clinicians, a strategy found to be effective in promoting participation among students with disabilities (Selanikyo et al., 2017). Points of entry emerging from the FACT may be used to inform a child’s formal individual education plan as well as the gritty details of a child’s daily routine, such as the specific wording used to communicate with a child, precise location of strategic seating, or individual child chosen as a peer supporter.
The FACT displays functional ability and participation classification levels in a concise graphical and textual format along with personal factors and environment description to facilitate the analysis. For example, a child noted to have difficulty with inattention may have low participation in the teacher-led instruction environmental domain. Functional ability weaknesses in verbal communication and executive functioning in combination with participation restrictions in a busy classroom environment may be suggestive of specific supports, such as communication accommodations or strategic seating. Furthermore, strengths in functional ability areas may be utilized (e.g., visual augmentative communication for individuals with strong visual cognitive ability).
Participation Reassessment
Once supportive interventions and goals are in place, intermittent reassessment of participation over time can measure success and inform the evolving individual plan. Participation levels should be seen as a reflection of adequacy of supports. Frequently, the symptoms of inadequate participation reflect stress, such as withdrawal, non-compliance, acting out, poor engagement, or poor productivity. A child’s functional abilities profile should not be considered static, since children’s functional abilities may develop at different rates over time and across individuals. Improved functional ability classification may be a goal for some children with conditions generally responsive to interventions, such as in literacy. For all children, optimizing participation in all contexts is the central goal. Participation should be re-classified on a regular basis for children at risk to evaluate the effects of supports put in place and at any time concerning symptoms or features arise.
Illustrative Fictional Cases
Below, we present two fictional cases to illustrate the process of using the proposed FACT. These histories are not from actual individuals, but rather created on the basis of common clinical presentations.
Case 1: “Graydon”
“Graydon” Case Description
Graydon is a 6-year-old boy in grade 1 with behavioural difficulties who was apprehended by Child Protection Services at age 3 for neglect. There was suspected, but not confirmed, alcohol or other drug exposures prenatally. He has had multiple foster home placements. His activity level at school is frequently very high. His language and reading skills are described as “weak, but other kids are worse.” Episodes of aggression have led to multiple classroom “evacuations.” He takes medication (methylphenidate and risperidone). He enjoys peer interactions and sometimes has positive to-and-fro conversation and play, but frequently requires direct support for sharing and turn taking. Free play often results in agitation and aggression, especially at recess. Speech language pathology assessment noted “mild language delay” with standardized testing at age 4 at 12th percentile in receptive and expressive language with normal articulation. Occupational therapy assessment at age 5 noted 45th percentile in visual spatial standardized testing, difficulties with executive functioning, and normal fine motor skills. A pediatrician diagnosed ADHD, ODD, and reading delay. A Fetal Alcohol Spectrum Disorder assessment program did not find an FASD diagnosis.
“Graydon”: Potential Points of Entry for Support
Analysis of Graydon’s profile (Figures 1 and 2) yielded a trend toward difficulties in environments tapping multiple skills, including communication, planning, and spontaneous social interactions. Specific supportive measures included trauma informed self-regulation strategies for teachers (modelling affect control and self-talk, strategic seating and support transitioning between activities) and increased structure and supervision in spontaneous social environments (e.g., recess and lunch). Executive functioning and communication supports (e.g., visual schedule, repeating, chunking) were planned for novel tasks.
Figure 1
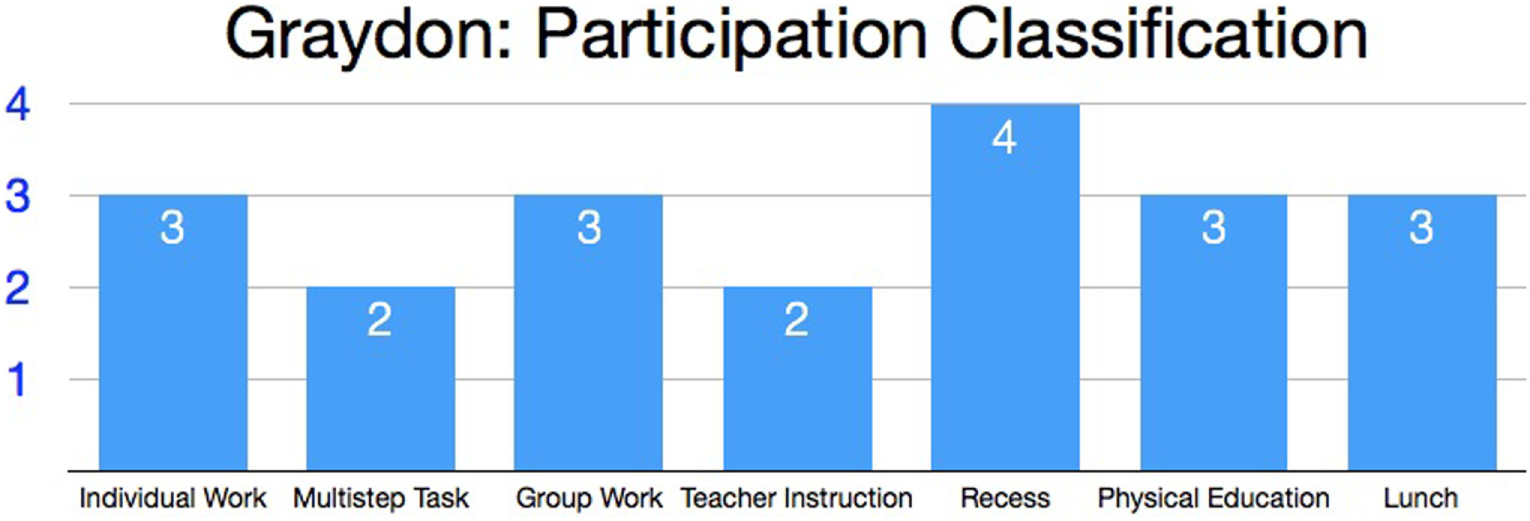
“Graydon”: classification of participation levels for activities in the school environment.
Figure 2
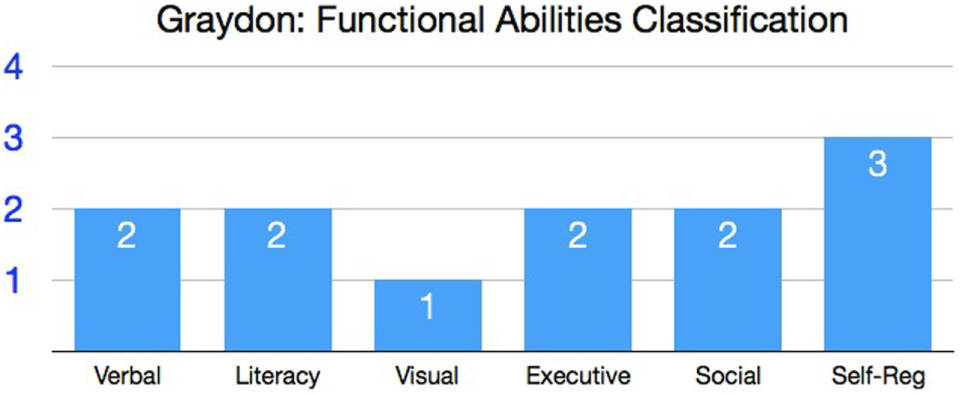
“Graydon”: classification of functional ability levels.
Case 2: “Grace”
“Grace” Case Description
Grace is a 12-year-old girl in grade 7 diagnosed with “high functioning” ASD. Parents report that she can talk at length about topics of interest, such as dance and animals, but has struggled with peer interactions and increasing social isolation. She requires considerable support to learn new tasks, but functions adequately in routine activities of daily living. Her semantic vocabulary is well beyond most peers; however, she has no friends, does not engage in group work or unstructured recreation (e.g., recess), and is usually found by herself. She has done well in primary grade academics with support, and her reading, reading comprehension, and some math skills are at or above grade level. However, she has struggled with poor productivity with tasks requiring multiple steps (e.g., reports, projects), working with abstract concepts (e.g., identifying themes in a story), or fine motor output (e.g., copious writing, crafts). She tends to “shut down” or wander away when frustrated or disengaged, leading to concern for safety among school staff. She often appears distant; when asked, she says, “I didn’t know what to do.” Psychoeducational assessment noted verbal and visual cognitive abilities in the “high average” range, and “low average” information processing and working memory.
“Grace”: Potential Points of Entry for Support
Information was provided to school staff regarding social pragmatic and executive functioning deficits (Figures 3 and 4). Specific supports based on these difficulties included frequent check-ins regarding comprehension, explanations of non-literal language and scaffolding of novel, multi-steps tasks. Group work and peer social interaction direct instruction was planned by a child and youth worker, including modelling/cueing during lunch, recess or and extracurricular activities.
Figure 3
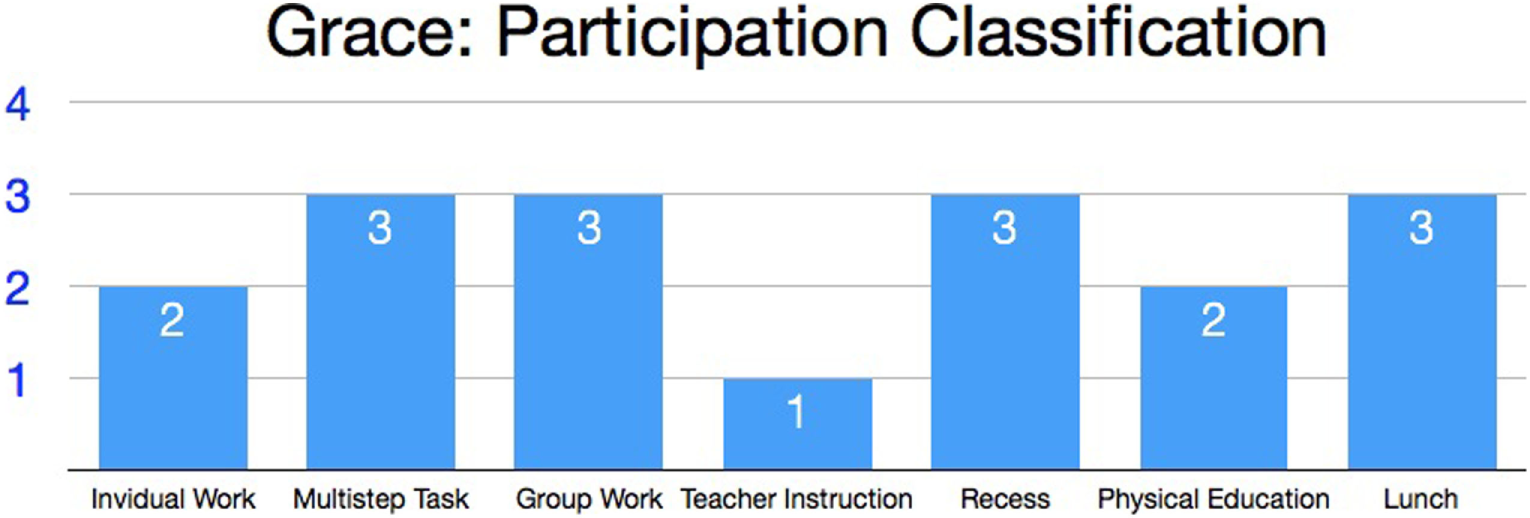
“Grace”: classification of participation levels for activities in the school environment.
Figure 4
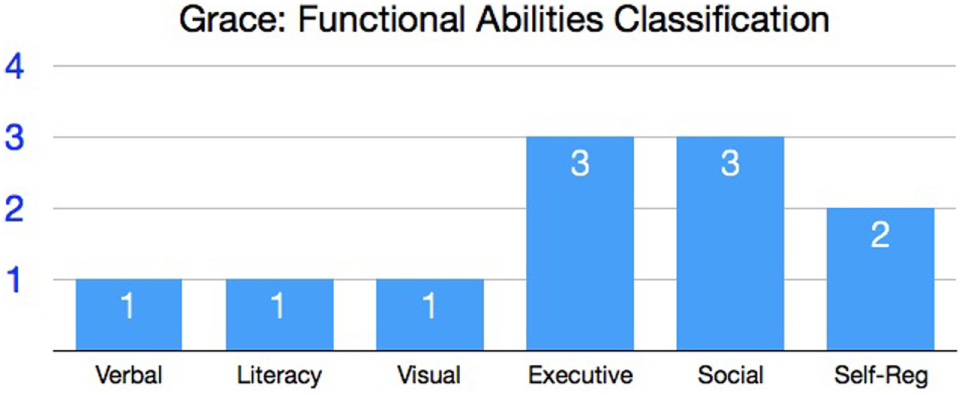
“Grace”: classification of functional ability levels.
Conclusion
The
status quofor many children with DDALB and their families involves a daunting challenge in navigating service systems to obtain appropriate supports for participation across environments. Resource allocation for special needs currently still relies heavily on categorical medical diagnoses, as per Tomlinson (
2012):
“In the current global recession governments find it easier to focus on individual deficiencies … rather than more costly strategies of reorganizing educational institutions to support all young people in their preparation for adulthood.”
Within this system are multiple disciplines of professionals that use variable assessment tools and distinct terminologies to describe function and disability. The lack of consistent terminology contributes to communication gaps, service delays, inefficiencies, disparities, redundancies, and poorly timed and placed interventions. Meanwhile, significant resources are spent dealing with the fallout of suboptimal participation (e.g., support needed for “behaviour” in the classroom) and stress (e.g., meetings between frustrated parents and service providers). The system is clogged with confusing arrays of “alphabet” (Baum and Olenchak, 2002) diagnoses (e.g., ADHD, LD, ODD, ASD, etc.), children with functional impairments without a diagnosis, and shifting eligibility criteria for programs that present a quagmire of barriers for children, families, and teachers.
There is an urgent need to implement functional measures to guide implementation of supports (McDowell and O’Keeffe, 2012). It is critical to provide timely support for participation utilizing readily available assessments without waiting for a gold standard test that may never happen in a quest for a diagnosis for which the child may not qualify anyway. The utility of categorizing developmental disorders simultaneously with medical diagnosis and functional abilities classification (i.e., dimensional measures) has been identified repeatedly (Carrey and Gregson, 2008).
This concept article has provided a review of the rationale for the routine classification of functional abilities and participation for children with DDALB. We have described a proposed tool for this purpose, FACT, aiming to strike the balance of comprehensiveness and succinctness to be of practical value to children and care providers across disciplines and agencies (i.e., education, developmental, medical, mental health, etc.). We propose the widespread use of such a tool that will provide parents, teachers, and clinicians with a functional abilities profile to identify points of entry for supports and as a basis for effective communication.
Shifting the assessment paradigm to emphasize functional abilities and participation will lead to a more child and family-centred model of timely, just enough assessment to define goals and inform plans, and away from system-centred exhaustive qualification assessments and cutoff criteria. We hypothesize that utilizing a flexible collaboration of capable, accessible special educators and clinicians to arrive at actionable conclusions in a systematic fashion will result in more and better support, leading to better outcomes for children and families. Furthermore, we predict that clear, common terminology and graphic presentation will facilitate efficient multidisciplinary meetings, seamless transfer of information across agencies, and reduce the need for redundant assessments and the opportunity cost of idiosyncratic care pathways. Dispensing resources based on functional need is expected to reduce angst among stakeholders, allowing the refocus of time, energy, and resources to those we support.
Limitations and Future Work
The proposed FACT includes a substantial amount of subjectivity in its assessment of functional ability levels, including incorporation of historical and observational data, transdisciplinary approach, and avoidance of strict standardized testing materials and cutoffs. We do not prescribe a method of assessment due to individual child needs (e.g., complexity of disability, testability) and case by case availability of historical data and local assessment methods and resources. The determination of a typical environment is also subjective. An exhaustive definition of environment, however, is not currently available. Furthermore, environmental demands across cultural and educational contexts may place different demands on functional abilities and may require a more fluid definition.
We argue that subjective and flexible methodologies are already rampant wherever there are children with problems at school, but without highly individualized programs based on extensive standardized testing. We have shown that domains of child functioning that are core to educational and life success, including self-regulation, executive functioning, and social skills, are not readily assessed by objective (i.e., capacity) measures. Furthermore, resource-limited realities dictate the need for a more flexible, practical, and responsive system. It would behoove us to build on capacity that already exists on a more grass roots level through scientific research instead of clinging to the illusion of a degree of standardized, objective categorization processes that is unsustainable in equitable public systems and outdated in light of biopsychosocial approaches. Readily quantifiable variables may in fact be something that is more appealing from administrative (gatekeeping) and political points of view rather than it is actually valuable from a child and proximal educational environment perspective.
The FACT is a proposed tool that requires validation study. There is much scientific work to draw from in previously validated instruments based on the ICF, for example among the tools mentioned above (Bedell, 2009; Rosenberg et al., 2010; Bolte et al., 2014; Khetani, 2015). Other questions include determining inter-rater reliability of functional ability and participation levels, and the possibility of incorporating more systematic measures of environmental and personal factors. Possible system-wide cost savings and effects on stakeholder satisfaction require evaluation. Above all, determining effects on participation outcomes is required. A detailed discussion of potential validation studies of the FACT is beyond the scope of the current article. The authors encourage other research groups to this end.
Statements
Author contributions
BK reviewed literature and composed the majority of this article. OK reviewed literature, composed parts of the article, and provided discussion and reviews/edits.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary material
The Supplementary Material for this article can be found online at http://www.frontiersin.org/articles/10.3389/feduc.2018.00002/full#supplementary-material.
References
1
Adair B. Ullenhag A. Keen D. Granlund M. Imms C. (2015). The effect of interventions aimed at improving participation outcomes for children with disabilities: a systematic review. Dev. Med. Child Neurol.57, 1093–1104.10.1111/dmcn.12809
2
Aljunieda M. Frederickson N. (2014). Utility of the International Classification of Functioning, Disability and Health (ICF) for educational psychologists’ work. Educ. Psychol. Pract.30, 380–392.10.1080/02667363.2014.949627
3
Almqvist L. Granlund M. (2005). Participation in school environment of children and youth with disabilities: a person-oriented approach. Scand. J. Psychol.46, 305–314.10.1111/j.1467-9450.2005.00460.x
4
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Arlington, VA: American Psychiatric Association.
5
Anaby D. Law M. Coster W. Bedell G. Khetani M. Avery L. et al (2014). The mediating role of the environment in explaining participation of children and youth with and without disabilities across home, school, and community. Arch. Phys. Med. Rehabil.95, 908–917.10.1016/j.apmr.2014.01.005
6
Andrews J. J. W. Saklofske D. H. Janzen H. L. (2001). Handbook of Psychoeducational Assessment. San Diego: Academic Press.
7
Bagnato S. J. (2007). How Can Authentic Assessment Prevent the Mismeasure of Young Children? Authentic Assessment for Early Childhood Intervention – Best Practices. New York: T. G. Press, 17–39.
8
Bartlett D. J. Galuppi B. Palisano R. J. McCoy S. W. (2016). Consensus classifications of gross motor, manual ability, and communication function classification systems between therapists and parents of children with cerebral palsy. Dev. Med. Child Neurol.58, 98–99.10.1111/dmcn.12933
9
Bates M. P. (2001). The Child and Adolescent Functional Assessment Scale (CAFAS): review and current status. Clin. Child Fam. Psychol. Rev.4, 63–84.10.1023/A:1009528727345
10
Bates M. P. Furlong M. J. Green J. G. (2006). Are CAFAS subscales and item weights valid? A preliminary investigation of the Child and Adolescent Functional Assessment Scale. Adm. Policy Ment. Health33, 682–695.10.1007/s10488-006-0052-4
11
Baum S. M. Olenchak F. R. (2002). The alphabet children: GT, ADHD, and more. Exceptionality10, 77–91.10.1207/S15327035EX1002_3
12
Bedell G. (2009). Further validation of the Child and Adolescent Scale of Participation (CASP). Dev. Neurorehabil.12, 342–351.10.3109/17518420903087277
13
Benson N. Oakland T. (2011). International classification of functioning, disability, and health: implications for school psychologists. Can. J. Sch. Psychol.26, 3–17.10.1177/0829573510396982
14
Berry D. O’Connor E. (2009). Behavioral risk, teacher–child relationships, and social skill development across middle childhood: a child-by-environment analysis of change. J. Appl. Dev. Psychol.31, 1–14.10.1016/j.appdev.2009.05.001
15
Bolte S. de Schipper E. Robison J. E. Wong V. C. Selb M. Singhal N. et al (2014). Classification of functioning and impairment: the development of ICF core sets for autism spectrum disorder. Autism Res.7, 167–172.10.1002/aur.1335
16
Cameron D. L. Cook B. G. (2013). General education teachers’ goals and expectations for their included students with mild and severe disabilities. Educ. Train. Autism Dev. Disabil.48, 18–30.
17
Carrey N. Gregson J. (2008). A context for classification in child psychiatry. J. Can. Acad. Child Adolesc. Psychiatry17, 50–57.
18
Castro S. Pinto A. (2015). Matrix for assessment of activities and participation: measuring functioning beyond diagnosis in young children with disabilities. Dev. Neurorehabil.18, 177–189.10.3109/17518423.2013.806963
19
Coster W. Bedell G. Law M. Khetani M. A. Teplicky R. Liljenquist K. et al (2011). Psychometric evaluation of the participation and environment measure for children and youth. Dev. Med. Child Neurol.53, 1030–1037.10.1111/j.1469-8749.2011.04094.x
20
Coster W. Law M. Bedell G. Khetani M. A. Anaby D. Teplicky R. et al (2013). The Participation and Environment Measure for Children and Youth (PEM-CY): An Innovative Measure for Home, School and Community. Available from: https://www.canchild.ca/en/resources/228-the-participation-and-environment-measure-for-children-and-youth-pem-cy-an-innovative-measure-for-home-school-and-community
21
Coster W. Law M. Bedell G. Khetani M. A. Cousins M. Teplicky R. (2012). Development of the participation and environment measure for children and youth: conceptual basis. Disabil. Rehabil.34, 238–246.10.3109/09638288.2011.603017
22
Davies P. L. Soon P. L. Young M. Clausen-Yamaki A. (2004). Validity and reliability of the school function assessment in elementary school students with disabilities. Phys. Occup. Ther. Pediatr.24, 23–43.10.1300/J006v24n03_03
23
Dawson P. Guare R. (2003). Executive Skills in Children and Adolescents: A Practical Guide to Assessment and Intervention. New York: Guilford Publications.
24
Dombrowski S. C. Gischlar K. L. (2014). Ethical and empirical considerations in the identification of learning disabilities. J. Appl. Sch. Psychol.30, 68–82.10.1080/15377903.2013.869786
25
Dosman C. Andrews D. Goulden K. (2012). Evidence-based milestone ages as a framework for developmental surveillance. Paediatr. Child Health17, 561–568.10.1093/pch/17.10.561
26
Eze N. Ofo E. Jiang D. O’Connor A. F. (2013). Systematic review of cochlear implantation in children with developmental disability. Otol. Neurotol.34, 1385–1393.10.1097/MAO.0b013e3182a004b3
27
Fantuzzo J. Sutton-Smith B. Atkins M. Meyers R. Stevenson H. Coolahan K. et al (1996). Community-based resilient peer treatment of withdrawn maltreated preschool children. J. Consult. Clin. Psychol.64, 1377–1386.10.1037/0022-006X.64.6.1377
28
Florian L. Hollenweger J. Wedell K. Terzi L. Holland A. (2006). Cross-cultural perspectives on the classification of children with disabilities: part I. Issues in the classification of children with disabilities. J. Spec. Educ.1, 36–45.10.1177/00224669060400010401
29
Forness S. R. Freeman S. F. N. Paparella T. Kauffman J. M. Walker H. M. (2012). Special education implications of point and cumulative prevalence for children with emotional or behavioral disorders. J. Emot. Behav. Disord.20, 1–14.10.1177/1063426611401624
30
Foster-Cohen S. Mirfin-Veitch B. (2017). Evidence for the effectiveness of visual supports in helping children with disabilities access the mainstream primary school curriculum. J. Res. Spec. Educ. Needs17, 79–86.10.1111/1471-3802.12105
31
Frankel F. Whitham C. (2011). Parent-assisted group treatment for friendship problems of children with autism spectrum disorders. Brain Res.1380, 240–245.10.1016/j.brainres.2010.09.047
32
Garner A. S. (2016). Thinking developmentally: the next evolution in models of health. J. Dev. Behav. Pediatr.37, 579–584.10.1097/DBP.0000000000000326
33
Geyh S. Peter C. Muller R. Bickenbach J. E. Kostanjsek N. Ustun B. T. et al (2011). The personal factors of the international classification of functioning, disability and health in the literature – a systematic review and content analysis. Disabil. Rehabil.33, 1089–1102.10.3109/09638288.2010.523104
34
Giangreco M. F. (2010). One-to-one paraprofessionals for students with disabilities in inclusive classrooms: is conventional wisdom wrong?Intellect. Dev. Disabil.48, 1–13.10.1352/1934-9556-48.1.1
35
Greenham M. Hearps S. Gomes A. Rinehart N. Gonzalez L. Gordon A. et al (2015). Environmental contributions to social and mental health outcomes following pediatric stroke. Dev. Neuropsychol.40, 348–362.10.1080/87565641.2015.1095191
36
Greenspan S. I. Wieder S. (2008). The interdisciplinary council on developmental and learning disorders diagnostic manual for infants and young children – an overview. J. Can. Acad. Child Adolesc. Psychiatry17, 76–89.
37
Harper C. B. Symon J. B. Frea W. D. (2008). Recess is time-in: using peers to improve social skills of children with autism. J. Autism Dev. Disord.38, 815–826.10.1007/s10803-007-0449-2
38
Hestenes L. L. Carroll D. E. (2000). The play interactions of young children with and without disabilities: individual and environmental influences. Early Child. Res. Q.15, 229–246.10.1016/S0885-2006(00)00052-1
39
Holsbeeke L. Ketelaar M. Schoemaker M. M. Gorter J. W. (2009). Capacity, capability, and performance: different constructs or three of a kind?Arch. Phys. Med. Rehabil.90, 849–855.10.1016/j.apmr.2008.11.015
40
Horridge K. A. McGarry K. Williams J. Whitlingum G. British Academy of Childhood Disability . (2016). Prospective pilots of routine data capture by paediatricians in clinics and validation of the Disabilities Complexity Scale. Dev. Med. Child Neurol.58, 581–588.10.1111/dmcn.13101
41
Hudziak J. J. Achenbach T. M. Althoff R. R. Pine D. S. (2007). A dimensional approach to developmental psychopathology. Int. J. Methods Psychiatr. Res.16(Suppl. 1), S16–S23.10.1002/mpr.217
42
Imms C. Adair B. Keen D. Ullenhag A. Rosenbaum P. Granlund M. (2016a). ‘Participation’: a systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev. Med. Child Neurol.58, 29–38.10.1111/dmcn.12932
43
Imms C. Granlund M. Wilson P. H. Steenbergen B. Rosenbaum P. Gordon A. M. (2016b). Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev. Med. Child Neurol.59, 16–25.10.1111/dmcn.13237
44
Kauffman J. M. Anastasiou D. Maag J. W. (2017). Special education at the crossroad: an identity crisis and the need for a scientific reconstruction. Exceptionality25, 139–155.10.1080/09362835.2016.1238380
45
Khetani M. A. (2015). Validation of environmental content in the young children’s participation and environment measure. Arch. Phys. Med. Rehabil.96, 317–322.10.1016/j.apmr.2014.11.016
46
Khetani M. A. Cliff A. B. Schelly C. Daunhauer L. Anaby D. (2014). Decisional support algorithm for collaborative care planning using the participation and environment measure for children and youth (PEM-CY): a mixed methods study. Phys. Occup. Ther. Pediatr.35, 231–252.
47
Kilgus S. P. Bowman N. A. Christ T. J. Taylor C. N. (2017). Predicting academics via behavior within an elementary sample: an evaluation of the social, academic, and emotional behavior risk screener (SAEBRS). Psychol. Sch.54, 246–260.10.1002/pits.21995
48
Kliegman R. M. Stanton B. St. Geme J. Schor N. F. (2016). Nelson Textbook of Pediatrics. Philadelphia: Elsevier.
49
Kraus de Camargo O. (2010). The international classification of functioning, disability and health (ICF): an ideal framework for developmental-behavioral pediatrics. AAP Sect. Dev. Behav. Pediatr. Newsl. Spring20, 11–13.
50
Kraus de Camargo O. (2016). Personal Factors and Participation – How Should Professionals Proceed? Available from: https://medium.com/@DevPeds/personal-factors-and-participation-7372ad74ac06#.n5j91e1eb
51
Kuhaneck H. M. Kelleher J. (2015). Development of the classroom sensory environment assessment (CSEA). Am. J. Occup. Ther.69, 1–9.10.5014/ajot.2015.019430
52
Lansford J. E. Malone P. S. Dodge K. A. Pettit G. S. Bates J. E. (2010). Developmental cascades of peer rejection, social information processing biases, and aggression during middle childhood. Dev. Psychopathol.22, 593–602.10.1017/S0954579410000301
53
Lee A. M. (2011). Using the ICF-CY to organise characteristics of children’s functioning. Disabil. Rehabil.33, 605–616.10.3109/09638288.2010.505993
54
Leonardi M. Bickenbach J. Ustun T. B. Kostanjsek N. Chatterji S. Consortium M. (2006). The definition of disability: what is in a name?Lancet368, 1219–1221.10.1016/S0140-6736(06)69498-1
55
Leonardi M. C. R. Sykes R. C. Madden H. ten Napel J. Hollenweger S. Snyman R. H. et al (2016). Do we really need to open a classification box on personal factors in ICF?Disabil Rehabil.38, 1327–1328.10.3109/09638288.2015.1089604
56
Lillvist A. Granlund M. (2010). Preschool children in need of special support: prevalence of traditional disability categories and functional difficulties. Acta Paediatr.99, 131–134.10.1111/j.1651-2227.2009.01494.x
57
Malone M. Koren G. (2012). Alcohol-induced behavioural problems in fetal alcohol spectrum disorders versus confounding behavioural problems. J. Popul. Ther. Clin. Pharmacol.19, e32–e40.
58
McDonald Connor C. Morrison F. J. Katch L. E. (2004). Beyond the reading wars: exploring the effect of child-instruction interactions on growth in early reading. Sci. Stud. Read.8, 305–336.10.1207/s1532799xssr0804_1
59
McDowell M. O’Keeffe M. (2012). Public services for children with special needs: discrimination by diagnosis?J. Paediatr. Child Health48, 2–5.10.1111/j.1440-1754.2011.02394.x
60
McIntosh R. Vaughn S. Schumm J. S. Haager D. Lee O. (1993). Observations of students with learning disabilities in general education classrooms. Except. Child.60, 249–261.10.1177/001440299406000306
61
Montroy J. J. Bowles R. P. Skibbe L. E. McClelland M. M. Morrison F. J. (2016). The development of self-regulation across early childhood. Dev. Psychol.52, 1744–1762.10.1037/dev0000159
62
Palmieri L. E. La Salle T. P. (2017). Supporting students in foster care. Psychol. Sch.54, 117–126.10.1002/pits.21990
63
Patel V. Flisher A. J. Hetrick S. McGorry P. (2007). Mental health of young people: a global public-health challenge. Lancet369, 1302–1313.10.1016/S0140-6736(07)60368-7
64
Portilla X. A. Ballard P. J. Adler N. E. Boyce W. T. Obradovic J. (2014). An integrative view of school functioning: transactions between self-regulation, school engagement, and teacher-child relationship quality. Child Dev.85, 1915–1931.10.1111/cdev.12259
65
Poulou M. (2014). The effects on students’ emotional and behavioural difficulties of teacher–student interactions, students’ social skills and classroom context. Br. Educ. Res. J.40, 986–1004.10.1002/berj.3131
66
Rashid T. Ostermann R. F. (2009). Strength-based assessment in clinical practice. J. Clin. Psychol.65, 488–498.10.1002/jclp.20595
67
Reid M. J. Webster-Stratton C. Hammond M. (2007). Enhancing a classroom social competence and problem-solving curriculum by offering parent training to families of moderate- to high-risk elementary school children. J. Clin. Child Adolesc. Psychol.36, 605–620.10.1080/15374410701662741
68
Ritzema A. M. Sladeczek I. E. Ghosh S. Karagiannakis A. Manay-Quian N. (2014). Improving outcomes for children with developmental disabilities through enhanced communication and collaboration between school psychologists and physicians. Can. J. Sch. Psychol.29, 317–337.10.1177/0829573514536529
69
Rosenbaum P. Eliasson A. C. Hidecker M. J. Palisano R. J. (2014). Classification in childhood disability: focusing on function in the 21st century. J. Child Neurol.29, 1036–1045.10.1177/0883073814533008
70
Rosenbaum P. Gorter J. W. (2012). The ‘F-words’ in childhood disability: I swear this is how we should think!Child Care Health Dev.38, 457–463.10.1111/j.1365-2214.2011.01338.x
71
Rosenberg L. (2015). The associations between executive functions’ capacities, performance process skills, and dimensions of participation in activities of daily life among children of elementary school age. Appl. Neuropsychol. Child4, 148–156.10.1080/21622965.2013.821652
72
Rosenberg L. Jarus T. Bart O. (2010). Development and initial validation of the children participation questionnaire (CPQ). Disabil. Rehabil.32, 1633–1644.10.3109/09638281003611086
73
Ruppar A. L. Allcock H. Gonsier-Gerdin J. (2017). Ecological factors affecting access to general education content and contexts for students with significant disabilities. Remedial Spec. Educ.38, 53–63.10.1177/0741932516646856
74
Rutter M. (2011). Research review: child psychiatric diagnosis and classification: concepts, findings, challenges and potential. J. Child Psychol. Psychiatry52, 647–660.10.1111/j.1469-7610.2011.02367.x
75
Scharf R. J. Scharf G. J. Stroustrup A. (2016). Developmental milestones. Pediatr. Rev.37, 25–37.10.1542/pir.2014-0103
76
Schulte-Korne G. (2016). Mental health problems in a school setting in children and adolescents. Dtsch. Arztebl. Int.113, 183–190.10.3238/arztebl.2016.0183
77
Selanikyo E. Yalon-Chamovitz S. Weintraub N. (2017). Enhancing classroom participation of students with intellectual and developmental disabilities. Can. J. Occup. Ther.84, 76–86.10.1177/0008417416661346
78
Shanker S. (2012). Calm, Alert and Learning: Classroom Strategies for Self-Regulation. Toronto: Pearson Education.
79
Simeonsson R. Bailey D. Smith T. Buysse V. (1995). Children with disabilities: functional assessment by teachers. J. Dev. Phys. Disabil.7, 267–284.10.1007/BF02578431
80
Simeonsson R. J. (2007). Foreword Authentic Assessment for Early Childhood Intervention – Best Practices. New York, NY, USA: The Guilford Press, 9–11.
81
Simeonsson R. J. Lollar D. Bjorck-Akesson E. Granlund M. Brown S. C. Zhuoying Q. et al (2014). ICF and ICF-CY lessons learned: Pandora’s box of personal factors. Disabil. Rehabil.36, 2187–2194.10.3109/09638288.2014.892638
82
Stucki G. Grimby G. (2004). Applying the ICF in medicine. J. Rehabil. Med.44(Suppl.), 5–6.10.1080/16501960410022300
83
Sutherland K. S. Lewis-Palmer T. Stichter J. Morgan P. L. (2008). Examining the influence of teacher behavior and classroom context on the behavioral and academic outcomes for students with emotional or behavioral disorders. J. Spec. Educ.41, 223–233.10.1177/0022466907310372
84
Tomlinson S. (2012). The irresistible rise of the SEN industry. Oxford Rev. Educ.38, 267–286.10.1080/03054985.2012.692055
85
Tsai S. Cheney D. (2012). The impact of the adult–child relationship on school adjustment for children at risk of serious behavior problems. J. Emotional Behav. Disord.20, 105–114.10.1177/1063426611418974
86
Turecki S. (2000). The Difficult Child. New York: Bantam.
87
Vaz S. Cordier R. Falkmer M. Ciccarelli M. Parsons R. McAuliffe T. et al (2015). Should schools expect poor physical and mental health, social adjustment, and participation outcomes in students with disability?PLoS ONE10:e0126630.10.1371/journal.pone.0126630
88
Walter H. J. Gouze K. Lim K. G. (2006). Teachers’ beliefs about mental health needs in inner city elementary schools. J. Am. Acad. Child Adolesc. Psychiatry45, 61–68.10.1097/01.chi.0000187243.17824.6c
89
West S. Dunford C. Mayston M. J. Forsyth R. (2014). The school function assessment: identifying levels of participation and demonstrating progress for pupils with acquired brain injuries in a residential rehabilitation setting. Child Care Health Dev.40, 689–697.10.1111/cch.12089
90
White K. M. (2016). My teacher helps me: assessing teacher-child relationships from the child’s perspective. J. Res. Child. Educ.30, 29–41.10.1080/02568543.2015.1105333
91
Whiteneck G. Dijkers M. P. (2009). Difficult to measure constructs: conceptual and methodological issues concerning participation and environmental factors. Arch. Phys. Med. Rehabil.90(11 Suppl.), S22–S35.10.1016/j.apmr.2009.06.009
92
Woodward L. J. Lu Z. Morris A. R. Healey D. M. (2017). Preschool self regulation predicts later mental health and educational achievement in very preterm and typically developing children. Clin. Neuropsychol.31, 404–422.10.1080/13854046.2016.1251614
93
World Health Organization. (2001). International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization.
94
World Health Organization. (2002). Towards a Common Language for Functioning, Disability and Health ICF. Geneva: World Health Organization.
95
World Health Organization. (2007). International Classification of Functioning, Disability, and Health – Children and Youth. Geneva: World Health Organization.
96
Wright F. V. (2015). What needs to happen before an international classification of function, disability and health core set is ready for clinical use?Dev. Med. Child Neurol.57, 112–113.10.1111/dmcn.12566
97
Ysseldyke J. Scerra C. Stickney E. Beckler A. Dituri J. E. Llis K. (2017). Academic growth expectations for students with emotional and behavior disorders. Psychol. Sch.54, 792–807.10.1002/pits.22030
98
Zee M. Koomenineke H. M. Y. Van der Veen I. (2013). Student–teacher relationship quality and academic adjustment in upper elementary school: the role of student personality. J. Sch. Psychol.51, 517–533.10.1016/j.jsp.2013.05.003
99
Zeman J. Cassano M. Perry-Parrish C. Stegall S. (2006). Emotion regulation in children and adolescents. J. Dev. Behav. Pediatr.27, 155–168.10.1097/00004703-200604000-00014
Summary
Keywords
participation, functional abilities, child development, child disability, international classification of functioning, functional abilities classification tool
Citation
Klein B and Kraus de Camargo O (2018) A Proposed Functional Abilities Classification Tool for Developmental Disorders Affecting Learning and Behaviour. Front. Educ. 3:2. doi: 10.3389/feduc.2018.00002
Received
13 September 2017
Accepted
05 January 2018
Published
07 February 2018
Volume
3 - 2018
Edited by
Brahm Norwich, University of Exeter, United Kingdom
Reviewed by
Gregor Ross Maxwell, University of Tromsø, Norway; Mats Granlund, Jönköping University, Sweden
Updates
Copyright
© 2018 Klein and Kraus de Camargo.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benjamin Klein, benjamin.klein@medportal.ca
Specialty section: This article was submitted to Special Educational Needs, a section of the journal Frontiers in Education
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.