 Allart M. Venema
Allart M. Venema Marko M. Sahinovic
Marko M. Sahinovic Anthony R. Absalom
Anthony R. Absalom J. K. Götz Wietasch
J. K. Götz Wietasch- Department of Anesthesiology, University Medical Center Groningen, University of Groningen, Groningen, Netherlands
Objective: It is challenging for rescuers to perform cardiopulmonary resuscitation (CPR) onboard lifeboats, particularly during rough weather. A mechanical chest compression device (MCD) may provide better quality chest compressions. The aim of this study was to compare the quality of chest compressions performed by lifeboat-crewmembers with those of a MCD during rough-sea conditions.
Methods: Lifeboat-crewmembers were scheduled to provide compression-only CPR on a resuscitation-mannequin during two sets of five 6-min epochs on a lifeboat at sea in two different weather-conditions. Simultaneously a MCD was used for compression-only CPR on another mannequin onboard the lifeboat. On a third occasion compressions by MCD only were measured due to COVID-19 restrictions. The primary outcome variable was the quality of chest compression, evaluated using published variables and standards (mean compression depth and compression frequency, percentage correct compression depth, percentage of not leaning on the thorax, percentage of correct hand placement on the thorax, hands-off-time).
Results: Six male lifeboat-crewmembers (mean age 35 years) performed CPR during two different weather conditions. In weather-conditions one (wind ~6–7 Beaufort/wave-height: 100–150 cm) quality of manual compressions was significantly worse than mechanical compressions for mean compression depth (p < 0.05) and compression frequency (p < 0.05), percentage correct compression depth (p < 0.05), percentage of not leaning on the thorax (p < 0.05), and hands off time (p < 0.05). Crewmembers could only perform CPR for a limited time-period (sea-conditions/seasickness) and after one set of five epochs measurements were halted. In weather-condition two (wind ~9 Beaufort/wave-height ~200 cm) similar results were found during two epochs, after which measurements were halted (sea-conditions/seasickness). In weather-condition three (wind ~7 Beaufort/wave-height ~300–400 cm) MCD compressions were according to resuscitation-guidelines except for three epochs during which the MCD was displaced.
Conclusion: Crewmembers were only able to perform chest-compressions for a limited time because of the weather-conditions. The MCD was able to provide good quality chest compressions during all but three epochs during the study period. More research is needed to determine whether MCD-use in real-life circumstances improves outcome. Inclusion of data on use of a MCD on lifeboats should be considered in future revisions of the USFD and resuscitation guidelines.
Introduction
Research about resuscitation onboard (life) boats is scarce [1], but a few studies have been performed, and have found that the quality of cardiopulmonary resuscitation (CPR) onboard lifeboats is suboptimal [2–4]. Search and rescue (SAR) operations commonly occur during adverse weather conditions, and given the complexity of performing research in such conditions, it is not surprising that only very limited evidence is available to guide and improve CPR-performance. This clearly highlights the need for more scientific research to improve resucitation onboard lifeboats.
Current resucitation guidelines recommend considering the use of a MCD during terrestrial and air transport or in circumstances where high-quality manual chest compressions are not practical or may compromise rescuer safety [5]. It is also specifically recommended to use a MCD in hypothermic patients when transport time is long or on difficult terrain [6]. Although use of a MCD device on board a lifeboat may provide better CPR, at present no specific advice for their use onboard lifeboats are provided in current resuscitation guidelines [5, 6].
Until now, only two studies have investigated the use of MCDs on mannequins on a lifeboat but both involved calm conditions with low windspeeds—one on a calm sea and the other on a river (with and without the boat making s-turns)—and both showed an MCD device was able to provide satisfactory CPR [7, 8]. CPR on lifeboats is however often required during less favorable weather conditions, which may hamper CPR-performance by lifeboat-crewmembers [4]. Even with the best training imaginable, performing CPR while on rough seas is difficult, impractical, especially if the rescuers suffer from seasickness, and sometimes impossible. Under certain conditions it might also endanger the lives and safety of lifeboat-crewmembers if they are not able to adequately brace themselves from (sudden) boat movements.
Crewmembers of the Royal Netherlands Sea Rescue Institution (KNRM) are trained to perform CPR onboard while being supported by one or more fellow crewmembers to counter the motion of the lifeboat (Figure 1). This additional stability of the person performing CPR is thought to enhance the chances of optimal CPR-performance and prevention of injuries of crewmembers. However, despite the additional support, during bad weather conditions performing adequate CPR remains challenging and potentially compromises rescuer safety.

Figure 1. Lifeboat-crewmember demonstrating CPR with support by another crewmember (photograph by K. Knol-Bosscher).
The aim of our study was therefore to compare the quality of manual chest compressions by lifeboat crewmembers with that of mechanical chest compressions by a MCD on a lifeboat at sea during different bad weather conditions. Our hypothesis was that a MCD will provide better quality chest compressions. The results of this study may assist guidance and improvement of CPR performance on (life)boats. It may also provide information for future revisions of the Utstein Style for Drowning (USFD) and resuscitation guidelines, in which the use of an MCD onboard a lifeboat is currently not specifically included [5, 6, 9].
Methods
This was a prospective two arm parallel mannequin study. The local ethics committee of the University Medical Center Groningen waived the requirement for a full consideration of the study (METc-reference number 2019/620). The study was registered with the Netherlands Trial Register (NTR NL8222) according to ICMJE-requirements.
Participants
Active KNRM lifeboat-crewmembers who were 18 years old or older were invited to participate in this study. After a written and verbal explanation of the study, written consent was obtained. Exclusion criteria were: KNRM-members who are not part of a lifeboat-crew (office-members, inspectors, board, etc.) (possible) pregnancy and physical restraints [10].
All participants received their most recent CPR training 10 weeks prior to the study.
Equipment
We used a LUCAS™ 3 chest Compression System device (Jolife AB/Stryker, Lund, Sweden) for the Mechanical chest compressions.
Two resuscitation-mannequins with electronic data collection (full body Resusci Anne CPR-Mannequin with skill-reporter software; Laerdal Medical, Stavanger, Norway) were used for the simulations and measurement recording.
The measurements at sea were performed on an “all weather” KNRM-lifeboat (which can be deployed in all-weather circumstances) of the “Johannes Frederik” class (15.0 meter long, 5.4 meters wide) with self-righting capability, waterjet propulsion and a top speed of 32 knots (59 km/h) (Figure 2).

Figure 2. KNRM-lifeboat of the “Johannes Frederik” class.
Procedures
We performed baseline measurements with the MCD under controlled conditions on land, to establish its performance without interference of any movement or vibrations.
For our goal to perform study measurements during rough sea conditions, we had to wait for bad weather circumstances, and select suitable moments. On weekends when the crew were available, we retrieved information from several weather stations surrounding the area in which we planned to perform the measurements. There can however be marked local variations in wave height, as it is influenced by wind strength, water currents, tides, local differences in water depths and the presence of sandbanks. Consequently, in addition to the meteorological measurements for the three periods when we performed study measurements, we report the local wind and wave conditions that were estimated by the lifeboat coxswain, as he has extensive experience and expertise in this regard.
On February 22nd 2020, we performed study measurements during two different weather conditions in the morning and the afternoon.
During these sessions, pairs of lifeboat-crewmembers performed continuous chest compressions inside of the lifeboat on a mannequin while wearing their protective gear (waterproof survival-suit with integrated life vest) as described previously [10]. During each session we planned to ask crewmembers twice to provide CPR during 5 epochs of 6 min each, switching roles every 2 min (i.e., a total of 60 min of CPR spread over two periods). Simultaneously the MCD device was used to provide continuous chest compressions on another mannequin inside the same lifeboat, next to the other mannequin. During the measurements, the coxswain was asked to steer and control the lifeboat as he would do during real resuscitation circumstances: trying to go as fast as possible without jeopardizing safety of the crew and the victim and enabling optimal circumstances for adequate resuscitation. After each epoch the speed of the lifeboat was briefly reduced while an investigator electronically saved the measurement data and reset the computer for the next 6-min epoch.
Variables
The primary outcome variable was the quality of chest compression, evaluated using a set of published variables and standards [5, 10, 11]. The variables and standards used were: mean compression depth (goal 50–60 mm), mean compression frequency (goal 100–120/min), percentage compressions for which compression depth was correct (goal 100%), percentage of not leaning on the thorax after compressions (i.e., full thoracic recoil) (goal 100%), percentage time during which hand placement on the thorax was correct (goal 100%), hands off time (time of no-CPR in seconds) as short as possible [5, 10, 11]. These parameters were automatically recorded using Laerdal skill reporter software (Laerdal Medical, Stavanger, Norway). Additionally we report the overall QCPR score per epoch as provided by the skill-reporter software (Laerdal Medical, Stavanger, Norway).
Baseline characteristics were the demographics of the involved crewmembers. Secondary outcome variables were the opinions of crewmembers regarding how realistic the resuscitation scenario was compared with resuscitation of a human drowning victim on board a lifeboat.
Statistics
The measurements were checked by two investigators (AMV and MMS), and statistically analyzed using SPSS Statistics version 28 (IBM, New York, United States). The data distribution was analyzed with the Shapiro-Wilk test. Normally distributed data were summarized as mean (SD) per group and tested for statistical significance between groups using the student's t-test. Non-normally distributed data were summarized as median (IQR) per group and tested for statistical significance between groups using the Mann-Whitney U test.
Sample size calculation
A pragmatic sample size was chosen based on the number of crewmembers at the participating lifeboat station and feasibility considerations (discussed with KNRM representative and the local lifeboat coxswain) [10]. As a result, it was decided to perform a measurement session between two and four moments of bad weather conditions.
Since Seesink et al. demonstrated a median time of CPR of 32 min (interquartile range: 25–45 min) by KNRM lifeboat-crewmembers in real circumstances, a period of 30 min of CPR measurements per session was used in this study [2].
COVID-19 restrictions
The COVID-19 pandemic began shortly after we had conducted the first two sets of measurements. We had to put the study on hold because the social distancing regulations in place precluded the conduct of experiments, particularly within in the confined spaces of a lifeboat. As the COVID-19 pandemic was still ongoing almost 2 years later, we therefore eventually decided to perform only one additional measurement session at sea with only the MCD performing chest compressions and no simultaneous manual chest compressions (as described above) by crewmembers. These additional measurements (weather condition 3) were done during bad weather on January 30th, 2022.
Results
Six male KNRM lifeboat-crewmembers with a mean age of 34.8 years participated in the study (Table 1). In general, they considered the measurements and scenario to be realistic (Table 2).
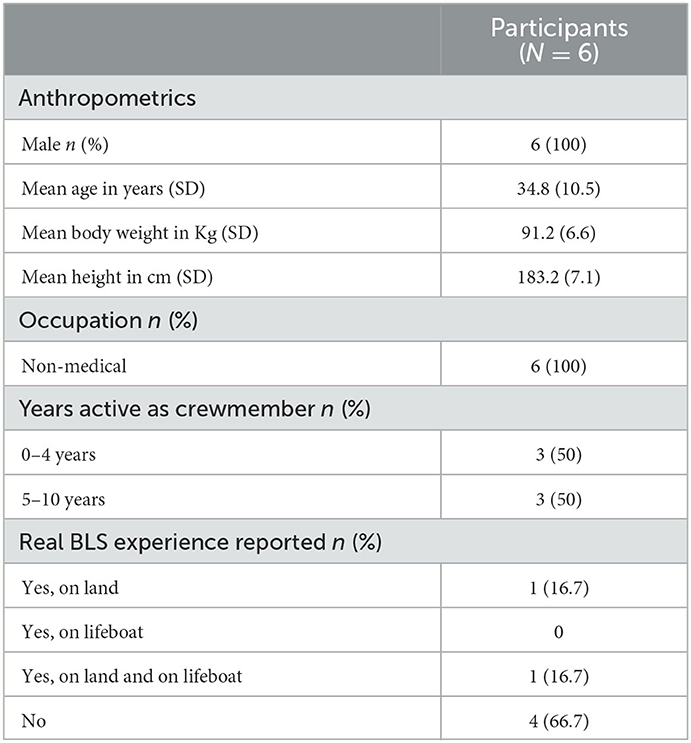
Table 1. Demographics.
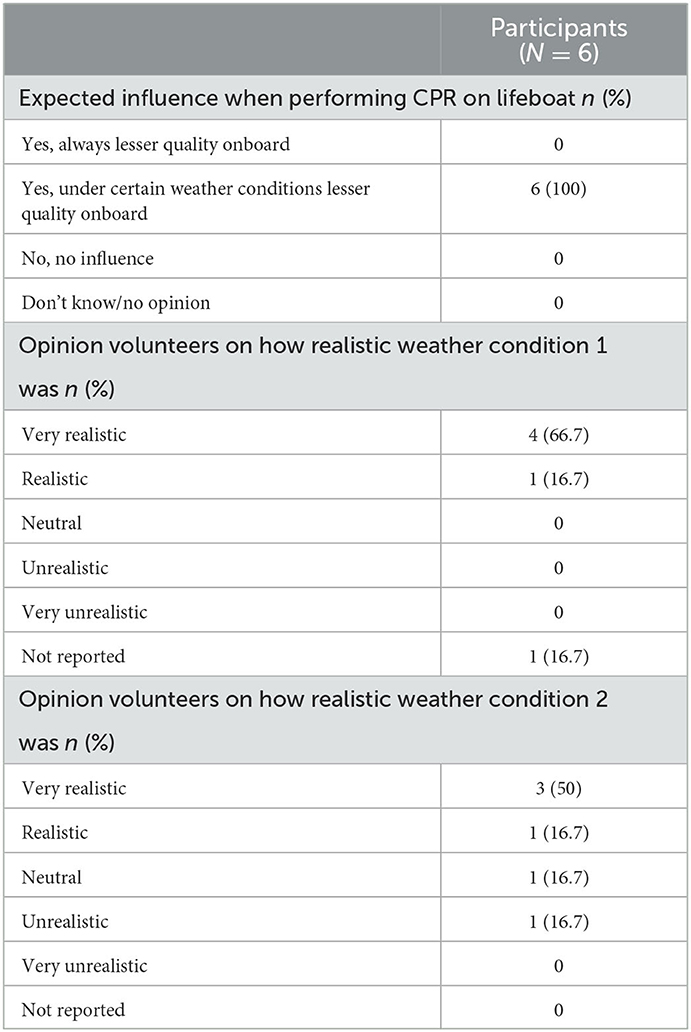
Table 2. Opinion rescuers on realism of study conditions.
The weather conditions are described in order of severity (Table 3). During weather conditions one and two crew members were not always able to perform manual compressions for the planned 2-min period due to the bad weather circumstances. When a crewmember was unable to continue, a change-over to another crewmember was done ahead of schedule.
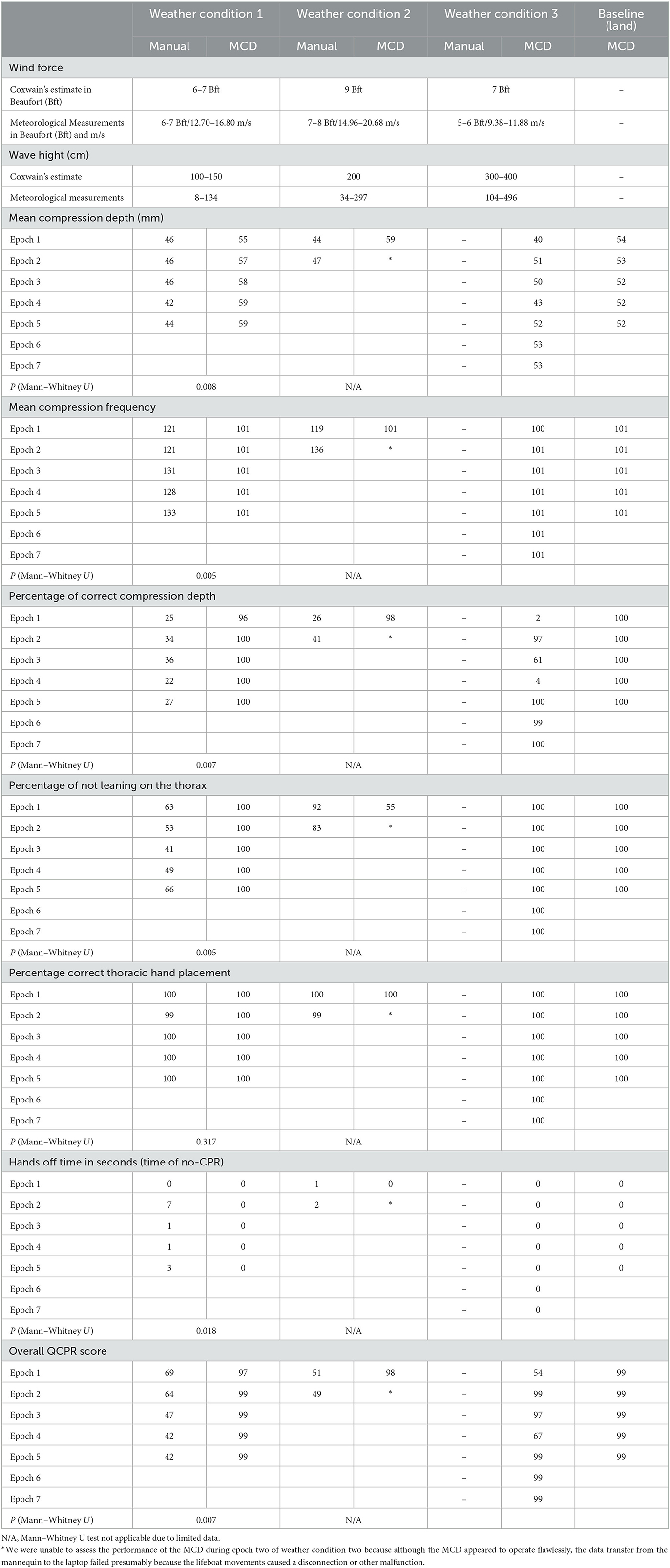
Table 3. Results of manual and mechanical chest compressions (MCD) with weather conditions in order of severity.
Baseline measurements
Baseline measurements of CPR performance by the MCD indoors on land are summarized in Table 3. All results of the performance parameter measurements were within the pre-specified targets of the primary research parameters and were consistent throughout all epochs.
Weather condition 1
The conditions at sea (with wind force ~6–7 Beaufort and wave height ~100–150 cm) hampered measurements. The quality of manual compressions was significantly worse than mechanical compressions for the overall resuscitation quality score (Q-CPR, range 42–69 vs. 97–99, p < 0.05) as well as for mean compression depth (range 42–46 vs. 55–59 mm, p < 0.05), compression frequency (range 121–133 vs. 101–101/min, p < 0.05), percentage correct compression depth (range 22–36 vs. 96–100%, p < 0.05), percentage of not leaning on the thorax (range 41–66 vs. 100–100%, p < 0.05), and hands off time (range 0–7 vs. 0–0 s, p < 0.05) (Table 3).
For CPR performed by crewmembers, hand placement and hands-off time were adequate. However, compressions were too shallow and too fast, and crewmembers leaned on the thorax too much resulting in diminished quality of CPR.
For the MCD, the compressions were all within the pre-specified targets of the primary research parameters, with the exception of epoch 1 when the depth of compressions was within the pre-specified range in 96% of compressions.
The participants were able to perform only the first set of five epochs of CPR. A decision was made to not to perform a second set of measurements because some of the crewmembers and researchers experienced seasickness which hindered their abilities to perform CPR.
Weather condition 2
The conditions at sea (with wind force ~9 Beaufort and wave height ~200 cm) caused the lifeboat to move in multiple axes despite the coxswain's efforts to keep the lifeboat as stable as possible.
The quality of manual compressions was worse than mechanical compressions for the overall resuscitation quality score (Q-CPR, range 49–51 vs. 98) as well as for mean compression depth (range 44–47 vs. 59 mm), compression frequency (range 119–136 vs. 101/min), and the percentage correct compression depth (range 26–41 vs. 98%) (Table 3).
We were unable to perform more than two epochs of CPR because the conditions caused seasickness among several of the researchers and crew. The compressions by crewmembers were too shallow and too fast (similarly to weather condition one). The percentage of not leaning on the thorax were higher than in weather condition one.
The MCD compressions during epoch one all were within the pre-specified targets, except for the percentage of not leaning on the thorax despite a visually correct placement of the MCD. We were unable to assess the performance of the MCD during epoch two because although the MCD appeared to operate flawlessly, the data transfer from the mannequin to the laptop failed presumably because the lifeboat movements caused a disconnection or other malfunction.
Weather condition 3
The conditions at sea (wind force was ~7 Beaufort and the wave height was ~300–400 cm) were more severe than during the first two conditions. Measurements were only made with the MCD.
The overall resuscitation quality score of the MCD ranged from 54 to 99, the mean compression depth ranged from 40 to 53 mm, the mean compression frequency ranged from 100 to 101/min, the percentage correct compression depth ranged from 2 to 100%, the percentage of not leaning on the thorax was 100%, and hands off time was 0 s (Table 3). The mechanical compressions were within the pre-specified targets during epochs two and five. In epoch one the mean compression depth was too shallow from the beginning, possibly caused by inadequate positioning of the suction cup due to the movements of the lifeboat. After ~4 min the MCD displaced in a cranial direction. In epoch three the compression depth was adequate at the beginning but after 3.10 min started becoming too shallow, without displacement of the MCD being observed. Epoch four started with insufficiently deep compressions and displacement in the cranial direction was observed during the epoch.
Due to the cranial displacement of the MCD in epochs one and four, we made an ad hoc decision to perform additional measurements during two extra epochs of 6 min. In both extra epochs there was no displacement of the MCD. The mechanical compressions during both extra epochs were within the pre-specified targets.
Discussion
The results of our study demonstrate that although crewmembers were able to perform chest compressions for a limited timespan during bad weather conditions, the MCD provided a better quality of chest compressions for a longer timespan on the resuscitation-mannequins during bad weather conditions. To our knowledge, this is the first study that has compared the quality of chest compressions with a MCD, with those of human rescuers, on a lifeboat at sea during bad weather conditions.
Two earlier studies demonstrated that CPR by a MCD was possible onboard a lifeboat which suggests that a MCD might be a good alternative to manual CPR [7, 8]. The results of our study, confirms their findings and provides evidence of adequate CPR performance by a MCD under more severe conditions than in the previous studies.
In a previous study, we evaluated the influence of the protective gear worn by KNRM crewmembers, on the quality of CPR performed on the same mannequins on land [10]. When comparing the results of that study with the current one, the performance of manual chest compressions in both studies was comparable. This indicates that even under bad weather conditions, lifeboat-crewmembers are able to perform chest compressions onboard a lifeboat with quality comparable to that on land. However, the results in this current study also demonstrate that they can only do so for a limited timespan during bad weather conditions, if at all.
In weather condition three lifeboat movements caused the MCD to move in a cranial direction in epochs one and four. We did not correct the position of the MCD during the epochs in which displacement occurred, because we did not want to interfere with the measurements. This led to suboptimal performance of the MCD during these epochs. After correction of its position before the start of the subsequent epochs, the MCD device again performed according to the pre-specified targets. Although correct (re)positioning the MCD can be somewhat challenging during bad weather conditions (movements), it does not take long to do and is still easier than performing manual chest compressions during these circumstances. However, previous studies have demonstrated that MCD misplacement can cause injuries to victims [12–15]. This suggests that both fixation methods of a MCD as well as the risk of injuries to victims when an MCD is used on a lifeboat need further exploration. Other potential drawbacks of a MCD such as time investment for training and maintaining operating skills, cost effectiveness, maintenance, need to be considered as well.
Even with additional efforts to enhance CPR performance by lifeboat-crews in general, mechanical chest compressions might still be superior during bad weather conditions. This is supported by the fact that the MCD was able to continue mechanical compressions during all sessions, even when conditions were worse (weather condition three) than those sessions in which manual compressions were performed (weather conditions one and two). This indicates that it might be prudent to consider MCD use onboard certain types of lifeboats. A MCD may be a good or even superior alternative during bad weather conditions with regards to both the quality of chest compressions and safety for lifeboat-crews, especially in even worse weather conditions then in our study. In addition, CPR results may be different when performed onboard a different size or type of lifeboat that might be affected differently by the weather conditions in which our study was performed. The potential benefit of a MCD might be more profound on smaller lifeboats, because they are more susceptible to bad weather conditions than the lifeboat used in our study was and have less space in which CPR can be performed. However, to test these hypotheses and to determine possible effects of mechanical chest compression on patient outcome, additional studies during bad weather in real circumstances and with more than one MCD must be performed first.
The mechanical chest compressions in general provided better quality of chest compressions for a longer timespan compared to manual compressions in this simulation study during bad weather conditions. Therefore, adding parameters on the use of a MCD during CPR for drowning victims rescued by lifeboat-crews should be considered in a future revision of the USFD, so it can be systematically studied in more detail in relation to outcome [9]. More research in this field may guide future resuscitation guidelines, as current evidence on drowning resuscitation is limited, especially regarding resuscitation on (life)boats [1].
Of course, transporting a victim back to shore is not the only event during SAR operations. First rescuing or evacuating a victim, for example from another ship, may have to be performed as well during resuscitation efforts. Exploring if and how a MCD can be of use during these circumstances, should also be studied in the future.
Limitations
This study has some limitations. First, it was a simulation study. However, this is one of the first and necessary steps in gaining more insights in the performance of CPR onboard lifeboats as safe as possible and obtaining leads for quality improvement. The weather circumstances during our study were however similar to those described in a study of resuscitations of humans by KNRM lifeboat-crewmembers and the results of manual compressions in our study were comparable to a previous mannequin study we performed [2, 10]. In addition, the participants generally considered the measurements and scenario to be realistic. Therefore, we expect our study data to be representative of real life circumstances. However, this has to be confirmed by future studies.
In weather conditions one and two, we were unable to complete all the scheduled measurements because of seasickness of some of the crew and researchers caused by the steep waves and the inability to focus on the horizon in the closed lifeboat. This highlights the difficulties of performing real-life studies like ours and is probably one of the reasons that there is a paucity of literature on this subject. To our knowledge, the incidence of seasickness of lifeboat crewmembers is unknown and would be an interesting subject to investigate in future studies, especially regarding its effects on CPR-performance. Although no study participants performed chest compressions during session three, we expect that had they done so, the results would have been similar to those in condition two.
The COVID-19 pandemic hindered the data collection for this study and might have influenced the results, as fewer sessions with manual chest compressions than planned could be performed. Hence, we only measured mechanical compressions during weather condition three. However, because of the clear differences between manual and mechanical chest compressions, we do not expect a significant influence.
Finally, in this study, we only focused on chest compressions. Providing adequate ventilations might be challenging during bad weather circumstances at sea. However, adequate ventilations are of course of great importance as well during CPR, especially for drowning victims, and this should be incorporated in future studies [16].
Conclusion
In this simulation study on manual vs. mechanical chest compressions onboard a lifeboat at sea during bad weather conditions, crewmembers were able to perform chest compressions for a limited timespan during bad weather conditions. The MCD provided a better quality of chest compressions for a longer timespan on the resuscitation-mannequins during bad weather conditions. More research to investigate the use of a MCD in real life circumstances is needed to determine effects on outcome. A MCD seems to be a promising and in some circumstances potentially safer CPR alternative onboard lifeboats which may enrich the current resuscitation guidelines. Including data on performance of mechanical chest compressions on lifeboats should be considered in future revisions of the USFD and resuscitation guidelines.
Data availability statement
The datasets presented in this article are not readily available because the data will not be available to other researchers as no approval has been obtained from the participants to share their data. Requests to access the datasets should be directed to YS5tLnZlbmVtYUB1bWNnLm5s.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AV, AA, and JW were involved in the conception and design of the study. AV was involved in the data collection. AV, AA, JW, and MS were involved in the analysis and interpretation of the data. All authors have been involved in drafting the manuscript or revising it critically for important intellectual content. All authors have given final approval of the version to be published.
Acknowledgments
We would like to thank E. Knol for his valuable assistance in the setup of this study, his willingness and efforts to coordinate and enabling the measurements at sea and reviewing the manuscript. We would also like to thank the other KNRM lifeboat-crew members who were willing to participate in this study, T. van der Linden of the KNRM for his support of this study, H. W. Roetert and J. Wicke for their assistance in collecting the data and J. Bierens for reviewing the manuscript as medical advisor of the KNRM. We would like to thank Laerdal Medical and its representatives for their willingness to loan the resuscitation mannequins and software for the study. We would like to thank Jolife AB/Stryker and its representatives for their willingness to provide the LUCAS™ 3 Chest Compression System device as a loan during the study.
Conflict of interest
AV reports non-financial support from Laerdal Medical (loan of the resuscitation mannequins with corresponding software), who were not involved in the conduct and reporting of this study, and non-financial support by Jolife AB/Stryker (loan of a LUCAS™ 3 Chest Compression System device during the study), who were not involved in the conduct and reporting of this study. AV is a volunteer at a KNRM lifeboat station. AA reports reimbursement for consultancy work and/or sponsor-initiated phase 1 studies performed for Philips, Ever Pharma, PAION, and Rigel Inc. All payments were to institution and none were relevant to the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bierens J, Abelairas-Gomez C, Barcala Furelos R, Beerman S, Claesson A, Dunne C, et al. Resuscitation and emergency care in drowning: a scoping review. Resuscitation. (2021) 162:205–17. doi: 10.1016/j.resuscitation.2021.01.033
2. Seesink J, Nieuwenburg SAV, van der Linden T, Bierens J. Circumstances, outcome and quality of cardiopulmonary resuscitation by lifeboat crews. Resuscitation. (2019) 142:104–10. doi: 10.1016/j.resuscitation.2019.07.012
3. Barcala-Furelos R, Abelairas-Gomez C, Palacios-Aguilar J, Rey E, Costas-Veiga J, Lopez-Garcia S, et al. Can surf-lifeguards perform a quality cardiopulmonary resuscitation sailing on a lifeboat? A quasi-experimental study. Emerg Med J. (2017) 34:370–5. doi: 10.1136/emermed-2016-205952
4. Tipton M, David G, Eglin C, Golden F. Basic life support on small boats at sea. Resuscitation. (2007) 75:332–7. doi: 10.1016/j.resuscitation.2007.04.027
5. Soar J, Bottiger BW, Carli P, Couper K, Deakin CD, Djarv T, et al. European resuscitation council guidelines 2021: adult advanced life support. Resuscitation. (2021) 161:115–51. doi: 10.1016/j.resuscitation.2021.02.010
6. Lott C, Truhlar A, Alfonzo A, Barelli A, Gonzalez-Salvado V, Hinkelbein J, et al. European resuscitation council guidelines 2021: cardiac arrest in special circumstances. Resuscitation. (2021) 161:152–219. doi: 10.1016/j.resuscitation.2021.02.011
7. Kazan C, Gupta P, Steeneken N, Kim YS, Cook S, Wogau I. The performance of manual versus mechanical cardiopulmonary resuscitation during a simulated rescue boat transport in cardiac arrest. Air Med J. (2021) 40:50–3. doi: 10.1016/j.amj.2020.10.007
8. Manoukian MAC, Tancredi DJ, Linvill MT, Wynia EH, Beaver B, Rose JS, et al. Manual versus mechanical delivery of high-quality cardiopulmonary resuscitation on a river-based fire rescue boat. Prehosp Disaster Med. (2022) 37:630–7. doi: 10.1017/S1049023X22001042
9. Idris AH, Bierens J, Perkins GD, Wenzel V, Nadkarni V, Morley P, et al. 2015 revised Utstein-style recommended guidelines for uniform reporting of data from drowning-related resuscitation: an ILCOR advisory statement. Resuscitation. (2017) 118:147–58. doi: 10.1016/j.resuscitation.2017.05.028
10. Venema AM, Sahinovic MM, Ramaker A, van de Riet YN, Absalom AR, Wietasch JKG. Performance of basic life support by lifeboat crewmembers while wearing a survival suit and life vest: a randomized controlled trial. Front Public Health. (2021) 9:666553. doi: 10.3389/fpubh.2021.666553
11. Olasveengen TM, Semeraro F, Ristagno G, Castren M, Handley A, Kuzovlev A, et al. European resuscitation council guidelines 2021: basic life support. Resuscitation. (2021) 161:98–114. doi: 10.1016/j.resuscitation.2021.02.009
12. Khan SU, Lone AN, Talluri S, Khan MZ, Khan MU, Kaluski E. Efficacy and safety of mechanical versus manual compression in cardiac arrest - a Bayesian network meta-analysis. Resuscitation. (2018) 130:182–8. doi: 10.1016/j.resuscitation.2018.05.005
13. Koster RW, Beenen LF, van der Boom EB, Spijkerboer AM, Tepaske R, van der Wal AC, et al. Safety of mechanical chest compression devices AutoPulse and LUCAS in cardiac arrest: a randomized clinical trial for non-inferiority. Eur Heart J. (2017) 38:3006–13. doi: 10.1093/eurheartj/ehx318
14. Gao Y, Sun T, Yuan D, Liang H, Wan Y, Yuan B, et al. Safety of mechanical and manual chest compressions in cardiac arrest patients: a systematic review and meta-analysis. Resuscitation. (2021) 169:124–35. doi: 10.1016/j.resuscitation.2021.10.028
15. Karasek J, Blankova A, Doubkova A, Pitasova T, Nahalka D, Bartes T, et al. The comparison of cardiopulmonary resuscitation-related trauma: mechanical versus manual chest compressions. Forensic Sci Int. (2021) 323:110812. doi: 10.1016/j.forsciint.2021.110812
Keywords: mechanical chest compressions, BLS, CPR, drowning, Utstein, lifeboat, rescue
Citation: Venema AM, Sahinovic MM, Absalom AR and Wietasch JKG (2023) Surviving the storm: manual vs. mechanical chest compressions onboard a lifeboat during bad weather conditions. Front. Disaster Emerg. Med. 1:1200857. doi: 10.3389/femer.2023.1200857
Received: 05 April 2023; Accepted: 02 May 2023;
Published: 09 June 2023.
Edited by:
Christoph Schriefl, Medical University of Vienna, AustriaReviewed by:
Roberto Barcala-Furelos, University of Vigo, SpainChristoph Testori, Medical University of Vienna, Austria
Copyright © 2023 Venema, Sahinovic, Absalom and Wietasch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Allart M. Venema, YS5tLnZlbmVtYUB1bWNnLm5s