
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 01 September 2023
Sec. Heart Valve Disease
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1182530
This article is part of the Research Topic Biomarkers in Structural Cardiovascular Disease: Insights into Screening, Diagnosis and Prognosis View all 9 articles
 Pâmela Nogueira Cavalcante1
Pâmela Nogueira Cavalcante1 Gabriel Kanhouche1
Gabriel Kanhouche1 Vitor Emer Egypto Rosa1
Vitor Emer Egypto Rosa1 Carlos M. Campos1,2*
Carlos M. Campos1,2* Mariana Pezzute Lopes1
Mariana Pezzute Lopes1 Maria Antonieta Albanez A. de M. Lopes1
Maria Antonieta Albanez A. de M. Lopes1 Roney Orismar Sampaio1Fábio Sândoli de Brito Júnior1
Roney Orismar Sampaio1Fábio Sândoli de Brito Júnior1 Flavio Tarasoutchi1
Flavio Tarasoutchi1 Alexandre Antonio Cunha Abizaid1
Alexandre Antonio Cunha Abizaid1
B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-pro BNP) are cardiac biomarkers that are released in response to increased ventricular and atrial wall stress. Aortic stenosis (AS) leads to hemodynamic changes and left ventricular hypertrophy and may be associated with natriuretic peptide levels. Several studies have shown that increased natriuretic peptide levels are correlated with AS severity and can predict the need for intervention. It can be useful in risk stratification, monitoring follow-up, and predicting cardiovascular outcomes of patients with severe AS. This paper aims to summarize the evidence of the role of BNP and NT-pro BNP in AS, before and after intervention.
Biomarkers are measurable laboratory indicators that could be helpful in the diagnosis or in the therapeutic decision of certain diseases. Several biomarkers have been studied in aortic stenosis, but B-type natriuretic peptide (BNP) is currently the only biomarker that is supported by valvular heart disease guidelines recommendations (1). BNP is a cardiac hormone mediating natriuresis, diuresis, and vasodilation (2). It is released in response to increased ventricular and atrial wall stress (1–3). Elevated BNP levels may reflect ventricular hypertrophy and cardiac dysfunction (3). BNP is cleaved from its prohormone, pro-BNP, and the N-terminal fragment, N-terminal pro-BNP (NT-pro BNP), is also released into circulation. NT-pro BNP has a similar diagnosis and prognostic implication to BNP, however, the evidence is weaker in the context of aortic stenosis (AS) (4).
AS is the most prevalent valve heart disease in the general population aged over 65 years, mainly in developed countries (5). The pathological process that occurs in aortic stenosis leads to hemodynamic changes and left ventricular hypertrophy (2). During the systole, aortic stenosis increases the resistance to the work of the left ventricle (LV). As a result, LV adapts to increased afterload by myocardial remodeling, which allows for the restoration of wall tension. This mechanism is a physiological response to normalize wall stress and, thus, maintain contractile function (1, 2, 6). However, in the natural evolution, LV may decompensate, and cardiac output decreases (6). Ventricular hypertrophy is correlated to BNP levels (3). Chen et al. (7) suggested that the hypertrophic response and BNP expression were controlled by a common pathway, but the exact mechanisms behind the release of BNP and how they lead to LV remodeling are still uncertain (1, 6, 7).
The role of natriuretic peptides as cardiac biomarkers in congestive heart failure (HF), as well as the prognostic value in patients with HF, is well recognized (8). BNP levels are correlated to New York Heart Association (NYHA) symptom class and are predictors of cardiovascular outcomes in HF (8, 9). Additionally, they are useful for discerning between cardiac and non-cardiac dyspnea, except for patients with AS (10). Previous studies showed that BNP levels correlated with severe AS and its echocardiographic parameters of severity (11–13). Furthermore, the onset of symptoms may be correlated with enhanced BNP levels (12). The use of BNP as a method of risk stratification of patients with AS is also a great research interest area, especially in the timing of intervention (14).
Despite this, the relative importance of BNP and its utility as a cardiac biomarker in aortic stenosis is currently under discussion. This paper aims to summarize the evidence of the role of BNP and NT pro-BNP in aortic stenosis, before and after interventions, highlighting a comprehensive analysis of their diagnostic and prognostic significance, which thus sets this paper apart from other reviews in the field. Boolean searches on PubMed, Medline, and Google Scholar included terms related to BNP or NT-pro BNP with terms for aortic stenosis and aortic valve replacement. The data analysis focused on randomized controlled trials, meta-analyses, and cohort studies conducted between 1995 and 2023. A total of 60 papers were reviewed excluding review articles and others less relevant to the topic.
The first studies published correlating BNP levels to severe AS demonstrated that increased natriuretic peptide levels are correlated with the mean pressure gradient, peak velocity, peak transaortic gradient pressure, aortic valve area, and functional status (NYHA symptom class) (11–13). Qi et al. (11) described that higher natriuretic peptide values may result not only from LV hypertrophy but also increased left atrial pressure caused by LV diastolic dysfunction. A stronger association was found between natriuretic peptides and LV mass index, aortic valvular area index, and mean aortic valve gradient. After multivariate analysis, only BNP remained as a predictor of these echocardiographic parameters (11).
In 2004, Weber et al. (12) found a positive correlation of NT-pro BNP levels to the mean transaortic pressure gradient, linked to the severity of AS and NYHA class, and that NT-pro BNP levels can serve as a recommendation for aortic valve replacement (AVR). AUC for NT-pro BNP to discriminate the need for intervention was 0.73. Their results were in agreement with the data published previously (12, 15, 16). Most of these studies excluded patients with reduced LV ejection fraction and valve disease concomitant with AS, which might cause elevated natriuretic peptide levels (15, 16).
Other studies have identified a progressive increase in BNP and NT-pro BNP values with decreasing aortic valve area but included a large increase in patients with LVEF <50%, which may emphasize the association between natriuretic peptide levels and cardiac function (11, 17).
These findings suggest that BNP is related to AS severity and could be useful to monitor asymptomatic patients (14).
The onset of symptoms is a critical point in the natural history of AS and is a hallmark for the recommendation of AVR. In some patients, the development of symptoms related to severe AS, such as exertional dyspnea, is unclear, non-specific, and often difficult to be evaluated clinically (12).
The use of BNP as a biomarker reflecting early decompensation in asymptomatic patients had been demonstrated previously in several studies (12–16). Gerber et al. (12) identified a strong association between NYHA class and natriuretic peptide plasma levels. It was higher in patients with NYHA class II than in those with class I symptoms, emphasizing that BNP could be used to distinguish between early-onset symptoms and normal effort tolerance. In contrast, they did not find a correlation between syncope or angina with enhanced natriuretic peptide levels, which suggests that these symptoms may have different pathophysiology in AS (12). These findings were corroborated by Lim et al. (18), who observed that BNP serum level >66 pg/ml detected symptomatic patients with increased NYHA functional class with a sensitivity, specificity, and accuracy of 84%, 82%, and 84%, respectively (18).
The optimal timing of intervention in asymptomatic patients with severe AS remains a challenge in clinical decision-making, and monitoring BNP levels may be helpful in this context. However, measurements of BNP do not substitute clinical and echocardiographic evaluation of these patients.
In asymptomatic patients, the relationship between classical parameters of AS severity, in cases of normal flow and high gradient, with elevated natriuretic peptide levels and poor prognosis is well established. In contrast, the association of biomarkers and prognosis for other AS categories remains unexplored. Results from a cohort study with specific subgroups of AS showed that patients with normal flow and low gradient who had lower BNP levels exhibited the best prognosis. While patients with true low flow and low gradient who had higher BNP levels displayed the worse outcome, with more LV remodeling and increased global LV afterload, similar to those patients with normal flow and high gradient (19). Results from the TOPAS study corroborated these findings, demonstrating that, in patients with classical low flow-low gradient AS (CLFLG-AS), BNP and NT-proBNP were powerful independent predictors of all-cause mortality. Furthermore, high levels of natriuretic peptides could accurately identify high-risk patients that could have survival benefits from early intervention. In addition, it was the first study to reveal that the prognostic value from NT-proBNP appears superior to that of BNP for this specific group of CLFLG-AS patients (20).
Moreover, the prognostic value of natriuretic peptides combined with high-sensitivity troponin T (hs-TnT) could be enhanced in LFLG-AS patients who had either preserved or reduced LV ejection fraction. Elevations of both BNP and hs-TnT were associated with a significantly higher risk of cardiovascular mortality in this group (21). Furthermore, higher levels of BNP and hs-TNI combined were also associated with progressive worsening of imaging parameters of LV remodeling and fibrosis by cardiac magnetic resonance (CMR) and poor outcomes in CLFLG-AS patients (22).
Studies correlating natriuretic peptides and biomarkers, such as troponin or imaging modalities, e.g., LV global longitudinal strain (LV-GLS), can provide synergistic risk stratification, independent of symptoms, risk factors, and other severe echo parameters in critical patients with AS. After aortic valve replacement, reversal of LV remodeling with regression of myocardial hypertrophy was observed, leading to an improvement in LV-GLS and decreased NT-pro BNP levels. However, more prospective studies are needed before natriuretic peptides can be used routinely to determine valve intervention timing (23, 24).
Mixed aortic valve disease (MAVD) is defined as an association between AS and aortic regurgitation (AR). In patients with moderate-to-severe MAVD, high BNP levels were correlated with worse LV-GLS, higher LV-mass index, elevated left atrial volume index, and higher prevalence of moderate or greater tricuspid regurgitation, which are significantly associated with critical clinical outcomes. Previous studies demonstrated worse outcomes in patients with moderate MAVD when compared to those with either moderate AS or AR alone (25).
The prognostic value of natriuretic peptides was demonstrated by several authors (26–31). Bergler-Klein et al. (26) showed that preoperative NT pro-BNP independently predicted the risk of death and postoperative outcomes. Symptom free-survival at the 12-month event rate was 31% vs. 92%, with NT pro-BNP <80 pmol/L vs. ≥80 pmol/L, respectively (p < 0.001) (26). In addition, Lim et al. (18) identified that in both symptomatic and asymptomatic patients, higher BNP was a strong independent predictor for cardiovascular death and may be helpful for risk stratification in AS (18).
Pedrazzini et al. (31) showed a comparison between logistic EuroSCORE and BNP in predicting in-hospital and late postoperative mortality in patients with severe AS undergoing AVR. BNP, but not logistic EuroSCORE, was shown to be an independent predictor of mortality. BNP levels >312 pg/ml could discriminate survivors from non-survivors with a C statistic of 0.80 and 0.75 for the perioperative and overall mortality, respectively (31).
The relationship between AS and sudden death is well-recognized (16). Previous studies suggested that adaptative LV hypertrophy leads to the development of myocardial fibrosis and it may be associated with an increased risk of cardiac events and mortality in AS (32, 33). Furthermore, BNP levels are associated with LV hypertrophy, which could explain the correlation between higher BNP and cardiac mortality (33).
The plasma level of pre-procedure BNP has also been linked with the left ventricle mass index after surgical AVR in early and late evaluation, and this is closely related to unfavorable outcomes and worsening of symptoms in the post-procedure follow-up (34). The study by Iwahashi et al. (34) showed that elevated BNP levels preoperatively were associated with NYHA >I in the late evaluation of post-surgical AVR follow-up, and BNP> 312 pg/ml had a lower event-free survival rate compared to patients who had BNP ≤ 312 pg/ml (34).
Importantly, Clavel et al. (16) showed in a prospective observational study a prognostic value for the BNP activation, defined as the ratio between the measured BNP, and maximal normal BNP value specific to age and sex in patients with severe AS. Elevated BNP clinical activation was associated with higher mortality, independently of baseline characteristics, emphasizing the role of BNP as a strong predictor of mortality. The level of BNP activation was also correlated to mortality in asymptomatic patients, with an adjusted HR of 7.38 when the BNP ratio ≥ 3 (16).
Thus, ESC/EACTS and AHA/ACC guidelines recommend intervention in patients with asymptomatic AS and BNP levels >3 × normal, as a class IIB recommendation (16, 18, 26, 35–37).
Recent evidence in studies on transcatheter AVR (TAVR) showed superiority in primary outcomes compared to conventional surgical AVR in most scenarios (38). In fact, the technical evolutions of TAVR operators and devices favor the improvement of results with this strategy, thus becoming a very reproducible possibility for the treatment of elderly patients with aortic stenosis, including intermediate and low-risk patients (38).
Natriuretic peptide values were also evaluated in patients submitted to TAVR and were related to prognosis (39, 40). High levels of pre-procedure BNP negatively influenced short and midterm outcomes. In addition, high BNP levels were associated with atrial fibrillation, kidney injury, lower ejection fraction, higher transaortic gradient, and smaller valve area (40). Nevertheless, high levels of BNP were found to be an independent factor for overall mortality (39). A sub-analysis of the PARTNER 2 study showed that there is a J-association of BNP and all-cause mortality in 2 years (7). Both very low and high values of this marker were associated with increased mortality. Ventricular hypertrophy in response to AS was associated with increased mortality, and elevated BNP levels were correlated with the degree of hypertrophy (7, 40). On the other hand, low BNP levels represent an inadequate ventricular response to elevated afterload of AS. The absence of hypertrophy increases LV wall stress, leading to irreversible damage to the left ventricle, such as stiffening and fibrosis, and thus increasing mortality. The patients with low BNP also presented increased troponin, which may infer myocardial injury (40). Thus, earlier intervention in aortic stenosis in this profile of patients could possibly avoid irreversible myocardial damage (7). Irreversible myocardial remodeling was observed in patients with elevated basal BNP who maintained elevated BNP levels at the 2-year follow-up. In general, after the procedure, BNP levels rise, except in patients whose levels are already high, and decrease in the majority of patients in 6- to 12-month follow-up (40). Approximately 40% of patients will persist with elevated natriuretic peptides despite TAVR, suggesting that other factors, beside the high afterload pressure, may be involved (41).
Post-TAVR BNP value also has clinical and prognostic correlation. BNP values after discharge were analyzed in patients included in the OCEAN-TAVI multicenter registry in order to evaluate prognosis and correlations with the patient profile and procedure (42). The cutoff point for increased mortality at 2 years was BNP >202 pg/ml. This profile of patients had more comorbidities, with higher age, lower mean LVEF, higher surgical risk scores, and a smaller effective aortic orifice area. In addition to mortality, more hospitalization for heart failure was also observed in patients with high BNP levels (43). Furthermore, a Portuguese study showed that 1-month post-procedure NT-pro BNP higher than 2,500 pg/ml was an independent risk factor for 1-year mortality. On the other hand, baseline NT-pro BNP did not predict outcomes (44). Previously, the prognostic value of NT-pro BNP was demonstrated by Lopes-Otero et al., who emphasized NT pro-BNP as a predictor of short and long-term outcomes after TAVR (45).
Figure 1 summarizes the major utilities and main correlations of natriuretic peptides (BNP and NT-proBNP) with different clinical aspects of AS.
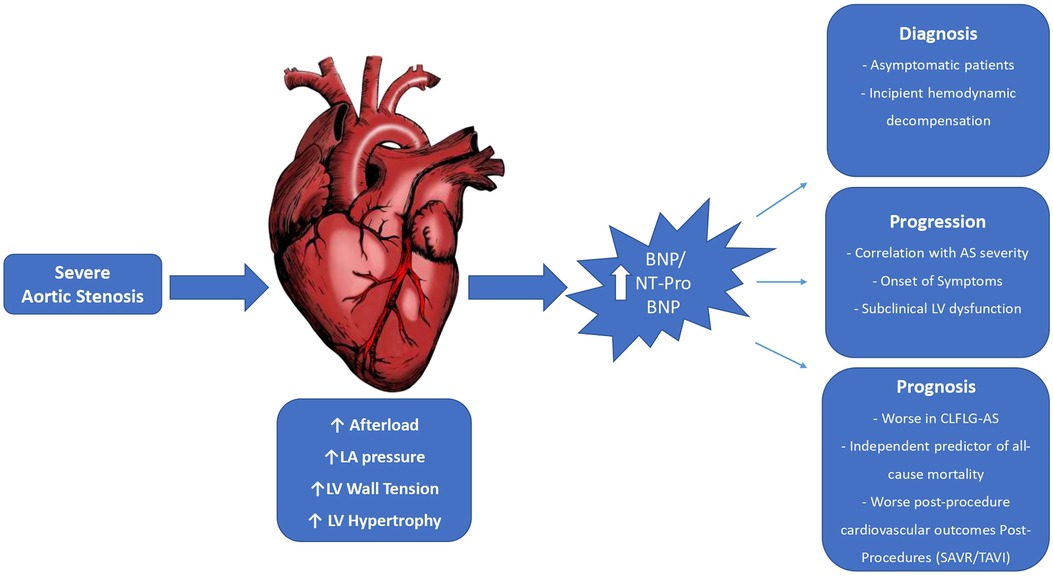
Figure 1. B-type natriuretic peptide and N-terminal Pro B-type natriuretic peptide in severe aortic stenosis. AS, aortic stenosis; BNP, B-type natriuretic peptide; CLFLG-AS, classical low-flow low-gradient aortic stenosis; LA, left atrium; LV, left ventricular; NT-ProBNP, N-terminal pro-B-type natriuretic peptide; SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement.
Various factors can lead to misinterpretation, either overestimating or underestimating BNP value. For instance, renal dysfunction, advanced age, female sex, atrial fibrillation, inflammation, hyperthyroidism, and the use of sacubitril/valsartan can cause an overestimation of BNP levels. On the other hand, certain factors including obesity, the immediate period following acute coronary syndrome onset, and the presence of pericardial effusion can result in an underestimation of BNP levels (46). Thus, in patients with AS associated with such conditions, we must assess natriuretic peptides with caution.
BNP is a prognostic marker in asymptomatic patients with severe AS, and values above the 3 × normal level may help indicate intervention (16, 18, 26, 35–37). BNP and NT-pro BNP also show promise for detecting symptoms onset and AS severity, but further studies are needed to validate their use in this context. Post-procedure BNP also appears to be a predictor of worse outcomes. BNP and NT-proBNP combined with other biomarkers or imaging modalities could enhance diagnostic accuracy and provide a comprehensive assessment of cardiac function and structure, especially in asymptomatic AS patients, thus guiding therapeutic management. However, more prospective studies are necessary to determine a cutoff value and whether changes in the levels of natriuretic peptides could be used appropriately to decide the best valve intervention timing.
PC, VR, and CC conceived of the presented idea. PC, GK, and VR developed and performed the literature review. VR and CC supervised the findings of this work. All author contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Redfors B, Furer A, Lindman BR, Burkhoff D, Marquis-Gravel G, Francese DP, et al. Biomarkers in aortic stenosis: a systematic review. Structural Heart. (2017) 1(1–2):18–30. doi: 10.1080/24748706.2017.1329959
2. White M, Baral R, Ryding A, Tsampasian V, Ravindrarajah T, Garg P, et al. Biomarkers associated with mortality in aortic stenosis: a systematic review and meta-analysis. Med Sci (Basel). (2021) 9(2):29. doi: 10.3390/medsci9020029
3. Yamamoto K, Burnett JC Jr, Jougasaki M, Nishimura RA, Bailey KR, Saito Y, et al. Superiority of brain natriuretic peptide as a hormonal marker of ventricular systolic and diastolic dysfunction and ventricular hypertrophy. Hypertension. (1996) 28(6):988–94. doi: 10.1161/01.HYP.28.6.988
4. Bottaro G, Zappulla P, Deste W, Famà F, Agnello F, Trovato D, et al. Severe aortic valve stenosis: symptoms, biochemical markers, and global longitudinal strain. J Cardiovasc Echogr. (2020) 30(3):154. doi: 10.4103/jcecho.jcecho_13_20
5. Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart disease and stroke statistics—2022 update: a report from the American heart association. Circulation. (2022) 145(8):e153–639.35078371
6. Hein S, Arnon E, Kostin S, Schönburg M, Elsässer A, Polyakova V, et al. Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation. (2003) 107(7):984–91. doi: 10.1161/01.CIR.0000051865.66123.B7
7. Chen S, Redfors B, O’Neill BP, Clavel M-A, Pibarot P, Elmariah S, et al. Low and elevated B-type natriuretic peptide levels are associated with increased mortality in patients with preserved ejection fraction undergoing transcatheter aortic valve replacement: an analysis of the PARTNER II trial and registry. Eur Heart J. (2020) 41(8):958–69. doi: 10.1093/eurheartj/ehz892
8. Tsutamoto T, Wada A, Maeda K, Hisanaga T, Maeda Y, Fukai D, et al. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: prognostic role of plasma brain natriuretic peptide concentration in patients with chronic symptomatic left ventricular dysfunction. Circulation. (1997) 96(2):509–16. doi: 10.1161/01.CIR.96.2.509
9. Berger R, Huelsman M, Strecker K, Bojic A, Moser P, Stanek B, et al. B-type natriuretic peptide predicts sudden death in patients with chronic heart failure. Circulation. (2002) 105(20):2392–7. doi: 10.1161/01.CIR.0000016642.15031.34
10. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. (2002) 347(3):161–7. doi: 10.1056/NEJMoa020233
11. Qi W, Mathisen P, Kjekshus J, Simonsen S, Bjørnerheim R, Endresen K, et al. Natriuretic peptides in patients with aortic stenosis. Am Heart J. (2001) 142(4):725–32. doi: 10.1067/mhj.2001.117131
12. Gerber IL, Stewart RA, Legget ME, West TM, French RL, Sutton TM, et al. Increased plasma natriuretic peptide levels reflect symptom onset in aortic stenosis. Circulation. (2003) 107(14):1884–90. doi: 10.1161/01.CIR.0000060533.79248.0C
13. Weber M, Arnold R, Rau M, Brandt R, Berkovitsch A, Mitrovic V, et al. Relation of N-terminal pro–B-type natriuretic peptide to severity of valvular aortic stenosis. Am J Cardiol. (2004) 94(6):740–5. doi: 10.1016/j.amjcard.2004.05.055
14. Jaiswal V, Khan N, Jaiswal A, Dagar M, Joshi A, Huang H, et al. Early surgery vs conservative management among asymptomatic aortic stenosis: a systematic review and meta-analysis. IJC Heart & Vasc. (2022) 43:101125. doi: 10.1016/j.ijcha.2022.101125
15. Capoulade R, Magne J, Dulgheru R, Hachicha Z, Dumesnil JG, O'Connor K, et al. Prognostic value of plasma B-type natriuretic peptide levels after exercise in patients with severe asymptomatic aortic stenosis. Heart. (2014) 100(20):1606–12. doi: 10.1136/heartjnl-2014-305729
16. Clavel M-A, Malouf J, Michelena HI, Suri RM, Jaffe AS, Mahoney DW, et al. B-type natriuretic peptide clinical activation in aortic stenosis: impact on long-term survival. J Am Coll Cardiol. (2014) 63(19):2016–25. doi: 10.1016/j.jacc.2014.02.581
17. Ikeda T, Matsuda K, Itoh H, Shirakami G, Miyamoto Y, Yoshimasa T, et al. Plasma levels of brain and atrial natriuretic peptides elevate in proportion to left ventricular end-systolic wall stress in patients with aortic stenosis. Am Heart J. (1997) 133(3):307–14. doi: 10.1016/S0002-8703(97)70225-4
18. Lim P, Monin JL, Monchi M, Garot J, Pasquet A, Hittinger L, et al. Predictors of outcome in patients with severe aortic stenosis and normal left ventricular function: role of B-type natriuretic peptide. Eur Heart J. (2004) 25(22):2048–53. doi: 10.1016/j.ehj.2004.09.033
19. Lancellotti P, Magne J, Donal E, Davin L, O'Connor K, Rosca M, et al. Clinical outcome in asymptomatic severe aortic stenosis: insights from the new proposed aortic stenosis grading classification. J Am Coll Cardiol. (2012) 59(3):235–43. doi: 10.1016/j.jacc.2011.08.072
20. Annabi MS, Zhang B, Bergler-Klein J, Dahou A, Burwash IG, Guzzetti E, et al. Usefulness of the B-type natriuretic peptides in low ejection fraction, low-flow, low-gradient aortic stenosis results from the TOPAS multicenter prospective cohort study. Structural Heart. (2021) 5(3):319–27. doi: 10.1080/24748706.2021.1900630
21. Dahou A, Clavel MA, Capoulade R, O'Connor K, Ribeiro HB, Côté N, et al. B-Type natriuretic peptide and high-sensitivity cardiac troponin for risk stratification in low-flow, low-gradient aortic stenosis: a substudy of the TOPAS study. JACC Cardiovasc Imaging. (2018) 11(7):939–47. doi: 10.1016/j.jcmg.2017.06.018
22. Lopes MAAADM, Campos CM, Rosa VEE, Sampaio RO, Morais TC, de Brito Júnior FS, et al. Multimodality imaging methods and systemic biomarkers in classical low-flow low-gradient aortic stenosis: key findings for risk stratification. Front Cardiovasc Med. (2023) 10:1149613. doi: 10.3389/fcvm.2023.1149613
23. Goodman A, Kusunose K, Popovic ZB, Parikh R, Barr T, Sabik JF, et al. Synergistic utility of brain natriuretic peptide and left ventricular strain in patients with significant aortic stenosis. J Am Heart Assoc. (2016) 5(1):e002561. doi: 10.1161/JAHA.115.002561
24. Poulsen SH, Søgaard P, Nielsen-Kudsk JE, Egeblad H. Recovery of left ventricular systolic longitudinal strain after valve replacement in aortic stenosis and relation to natriuretic peptides. J Am Soc Echocardiogr. (2007) 20(7):877–84. doi: 10.1016/j.echo.2006.11.020
25. Onishi H, Naganuma T, Izumo M, Ouchi T, Yuki H, Mitomo S, et al. Prognostic relevance of B-type natriuretic peptide in patients with moderate mixed aortic valve disease. ESC Heart Fail. (2022) 9(4):2474–83. doi: 10.1002/ehf2.13946
26. Bergler-Klein J, Klaar U, Heger M, Rosenhek R, Mundigler G, Gabriel H, et al. Natriuretic peptides predict symptom-free survival and postoperative outcome in severe aortic stenosis. Circulation. (2004) 109(19):2302–8. doi: 10.1161/01.CIR.0000126825.50903.18
27. Feuchtner GM, Muller S, Grander W, Alber HF, Bartel T, Friedrich GJ, et al. Aortic valve calcification as quantified with multislice computed tomography predicts short-term clinical outcome in patients with asymptomatic aortic stenosis. J Heart Valve Dis. (2006) 15(4):494.16901041
28. Dichtl W, Alber HF, Feuchtner GM, Hintringer F, Reinthaler M, Bartel T, et al. Prognosis and risk factors in patients with asymptomatic aortic stenosis and their modulation by atorvastatin (20 mg). Am J Cardiol. (2008) 102(6):743–8. doi: 10.1016/j.amjcard.2008.04.060
29. Antonini-Canterin F, Popescu BA, Popescu AC, Beladan CC, Korcova R, Piazza R, et al. Heart failure in patients with aortic stenosis: clinical and prognostic significance of carbohydrate antigen 125 and brain natriuretic peptide measurement. Int J Cardiol. (2008) 128(3):406–12. doi: 10.1016/j.ijcard.2007.05.039
30. Katz M, Tarasoutchi F, Pesaro A, Lopes RD, Spina GS, Vieira M, et al. Natriuretic peptides and long-term mortality in patients with severe aortic stenosis. J Heart Valve Dis. (2012) 21(3):331–6.22808834
31. Pedrazzini GB, Masson S, Latini R, Klersy C, Rossi MG, Pasotti E, et al. Comparison of brain natriuretic peptide plasma levels versus logistic EuroSCORE in predicting in-hospital and late postoperative mortality in patients undergoing aortic valve replacement for symptomatic aortic stenosis. Am J Cardiol. (2008) 102(6):749–54. doi: 10.1016/j.amjcard.2008.04.055
32. Cioffi G, Faggiano P, Vizzardi E, Tarantini L, Cramariuc D, Gerdts E, et al. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart. (2011) 97(4):301–7. doi: 10.1136/hrt.2010.192997
33. Capoulade R, Clavel M-A, Le Ven F, Dahou A, Thebault C, Tastet L, et al. Impact of left ventricular remodelling patterns on outcomes in patients with aortic stenosis. Eur Heart J Cardiovasc Imaging. (2017) 18(12):1378–87. doi: 10.1093/ehjci/jew288
34. Iwahashi N, Nakatani S, Umemura S, Kimura K, Kitakaze M. Usefulness of plasma B-type natriuretic peptide in the assessment of disease severity and prediction of outcome after aortic valve replacement in patients with severe aortic stenosis. J Am Soc Echocardiogr. (2011) 24(9):984–91. doi: 10.1016/j.echo.2011.03.012
35. Clavel M-A, Pibarot P, Messika-Zeitoun D, Capoulade R, Malouf J, Aggarwal SR, et al. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis: results of an international registry study. J Am Coll Cardiol. (2014) 64(12):1202–13. doi: 10.1016/j.jacc.2014.05.066
36. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS). Eur Heart J. (2022) 43(7):561–632. doi: 10.1093/eurheartj/ehab395
37. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP III, Gentile F, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. (2021) 77(4):450–500. doi: 10.1016/j.jacc.2020.11.035
38. Siontis GC, Overtchouk P, Cahill TJ, Modine T, Prendergast B, Praz F, et al. Transcatheter aortic valve implantation vs. Surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. (2019) 40(38):3143–53. doi: 10.1093/eurheartj/ehz275
39. Abramowitz Y, Chakravarty T, Jilaihawi H, Lee C, Cox J, Sharma RP, et al. Impact of preprocedural B-type natriuretic peptide levels on the outcomes after transcatheter aortic valve implantation. Am J Cardiol. (2015) 116(12):1904–9. doi: 10.1016/j.amjcard.2015.09.031
40. Lehtola H, Piuhola J, Niemelä M, Tauriainen T, Junttila J, Mäkikallio T, et al. B-type natriuretic peptide ability to predict mortality after transcatheter aortic valve replacement. J Cardiovasc Med. (2022) 23(1):e18. doi: 10.2459/JCM.0000000000001230
41. Rubattu S, Volpe M. BNP Level and post-transcatheter aortic valve replacement outcome: an intriguing J-shaped relationship. Eur Heart J. (2020) 41(8):970–2. doi: 10.1093/eurheartj/ehz922
42. Ribeiro HB, Urena M, Le Ven F, Nombela-Franco L, Allende R, Clavel M-A, et al. Long-term prognostic value and serial changes of plasma N-terminal prohormone B-type natriuretic peptide in patients undergoing transcatheter aortic valve implantation. Am J Cardiol. (2014) 113(5):851–9. doi: 10.1016/j.amjcard.2013.11.038
43. Mizutani K, Hara M, Iwata S, Murakami T, Shibata T, Yoshiyama M, et al. Elevation of B-type natriuretic peptide at discharge is associated with 2-year mortality after transcatheter aortic valve replacement in patients with severe aortic stenosis: insights from a multicenter prospective OCEAN-TAVI (optimized transcatheter valvular intervention–transcatheter aortic valve implantation) registry. J Am Heart Assoc. (2017) 6(7):e006112. doi: 10.1161/JAHA.117.006112
44. Vale NC, Teles RC, Madeira S, Brito J, Almeida MS, Nolasco T, et al. Post-procedural N-terminal pro-brain natriuretic peptide predicts one-year mortality after transcatheter aortic valve implantation. Rev Port Cardiol. (2018) 37(1):67–73. doi: 10.1016/j.repc.2017.06.016
45. López-Otero D, Trillo-Nouche R, Gude F, Cid-Álvarez B, Ocaranza-Sanchez R, Álvarez MS, et al. Pro B-type natriuretic peptide plasma value: a new criterion for the prediction of short-and long-term outcomes after transcatheter aortic valve implantation. Int J Cardiol. (2013) 168(2):1264–8. doi: 10.1016/j.ijcard.2012.11.116
Keywords: biomarkers, natriuretic peptides, B-type natriuretic peptide, aortic stenosis, aortic valve replacement
Citation: Cavalcante PN, Kanhouche G, Rosa VEE, Campos CM, Lopes MP, Lopes MAAAdM, Sampaio RO, Brito Júnior FSd, Tarasoutchi F and Abizaid AAC (2023) B-type natriuretic peptide and N-terminal Pro-B-type natriuretic peptide in severe aortic stenosis: a comprehensive literature review. Front. Cardiovasc. Med. 10:1182530. doi: 10.3389/fcvm.2023.1182530
Received: 8 March 2023; Accepted: 11 August 2023;
Published: 1 September 2023.
Edited by:
Guoping Li, Harvard Medical School, United StatesReviewed by:
Michail Spanos, Harvard Medical School, United States© 2023 Cavalcante, Kanhouche, Rosa, Campos, Lopes, Lopes, Sampaio, Brito Júnior, Tarasoutchi and Abizaid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos M. Campos Y2FybG9zYWNhbXBvczFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.