
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Cardiovasc. Med. , 17 April 2023
Sec. General Cardiovascular Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fcvm.2023.1135848
This article is part of the Research Topic Contemporary Causes of Acute Myocarditis and Pericarditis: Diagnosis by advanced imaging techniques and therapeutic strategies View all 12 articles
 Luca Valore1*
Luca Valore1* Till Junker1Eva Heilmann2Christine S. Zuern3,4Matthias Streif5
Till Junker1Eva Heilmann2Christine S. Zuern3,4Matthias Streif5 Beatrice Drexler1Christian Arranto1Jörg P. Halter1,4
Beatrice Drexler1Christian Arranto1Jörg P. Halter1,4 Christoph T. Berger6,7
Christoph T. Berger6,7
Introduction: Vaccine-induced myocarditis is a rare complication of messenger RNA (mRNA) COVID-19 vaccines.
Case presentation: We report a case of acute myopericarditis in a recipient of allogeneic hematopoietic cells following the first dose of the mRNA-1273 vaccine and the successful administration of a second and third dose while on prophylactic treatment with colchicine to successfully complete the vaccination.
Conclusion: Treatment and prevention of mRNA-vaccine-induced myopericarditis represent a clinical challenge. The use of colchicine is feasible and safe to potentially reduce the risk of this rare but severe complication and allows re-exposure to an mRNA vaccine.
Vaccine-induced myocarditis is a rare complication of messenger RNA (mRNA) vaccines against SARS-CoV-2. There are no reliable data about this adverse event in patients who received allogeneic hematopoietic cell transplantation (HCT). We report a case about a severe clinical course of mRNA-vaccine-induced myopericarditis, its challenging diagnostic process and plausible pathological background, the therapeutical use of colchicine in the acute phase of the disease, and also as a successful prophylaxis by re-exposure to mRNA vaccine against SARS-CoV-2.
A 70-year-old patient presented to the emergency department complaining of severe back pain radiating to the chest and dyspnea occurring within 12 h following the first dose of the mRNA-1273 vaccine (Spikevax, Moderna). Twenty months earlier, the patient underwent allogeneic hematopoietic cell transplantation for primary myelofibrosis. At the time of presentation, he was in complete remission without signs of active graft versus host disease (GvHD) or infectious disease. Current medication included bisoprolol, ursodeoxycholic acid, budesonide, esomeprazole, insulin, valaciclovir, co-trimoxazole, and gabapentin.
On admission, he was hemodynamically stable (blood pressure 136/79 mmHg, heart rate 79 bpm), afebrile, and adequately oxygenated (oxygen saturation 99% in ambient air). Besides arterial hypertension, no other cardiovascular risk factors were present. An electrocardiogram (ECG) showed concave ST-elevation and PQ-segment depression in several ECG leads and not related to a single coronary artery (Figure 1A). Initial laboratory tests indicated a mildly elevated high sensitivity Troponin T of 53 ng/L (reference <14 ng/L), and an N-terminal prohormone of brain natriuretic peptide (NTproBNP) of 655 ng/L (reference <124 ng/L). The remaining laboratory values are summarized in Table 1.
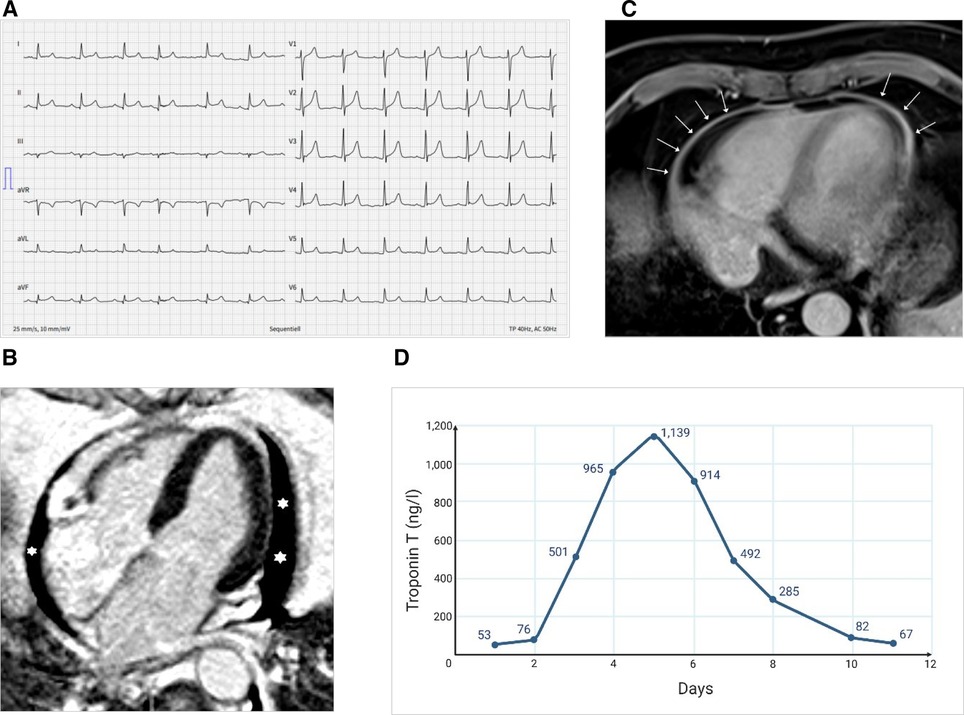
Figure 1. Electrocardiographic and imaging findings at admission and course of high-sensitive troponin T. (A) ECG showing diffuse concave ST-elevation (II, aVF, V3-6) and PQ-depression (II, aVF). (B) MRI showing pericardial effusion (asterisks) in the four-chamber view (late enhancement PSIR). (C) MRI showing pericardial enhancement (arrows) (axial T1 DIXON Water only, which is a fat-saturated, non-ECG-triggered). (D) Longitudinal evolution of the high-sensitive troponin T levels during the hospitalization (MRI done on day 3; i.e., troponin 501 ng/L).
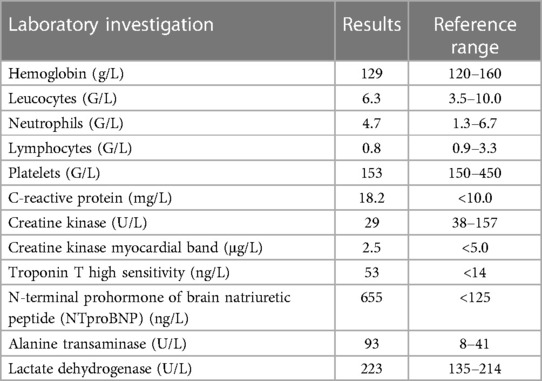
Table 1. Laboratory values at admission.
Aortic dissection, pulmonary embolism, and type 1 myocardial infarction were ruled out by computed tomography scan and coronary angiography, respectively. A single-vessel coronary artery disease with a non-critical right coronary artery stenosis was identified that was not assumed to be responsible for the acute symptoms. Bedside echocardiography showed a hemodynamically insignificant pericardial effusion with preserved left systolic and right heart function bedside echocardiography. A cardiac magnetic resonance imaging (MRI) performed 2 days after symptom onset confirmed pericardial effusion and showed a circumferential pericardial contrast enhancement compatible with pericarditis; the myocardium showed no late gadolinium enhancement and no edema (Figures 1B,C). However, based on the dynamical rise of troponin levels (peak 1,139 ng/L on day 5), a substantial myocardial injury was present. Combined with the ECG changes and cardiac imaging findings and after ruling out alternative causes, acute mRNA vaccine-related probable myopericarditis was diagnosed. No infections or other medical problems in the weeks prior to the presentation could be identified in the patient's history. A nasopharyngeal swab for respiratory viruses, an autoimmune serology panel, and serological tests for enterovirus and adenovirus antibodies were repeatedly negative. A nasal swab and a negative anti-SARS-CoV-2-Nucleoprotein-IgG/M excluded an acute or previous infection with SARS-CoV-2.
The patient was admitted to the hospital for telemetric monitoring and treatment with a non-steroidal anti-inflammatory drug (NSAID) as well as colchicine 0.5 mg every 12 h without systemic steroids was started.
After 13 days, he was discharged (Figure 1D). After 2 months, colchicine was stopped, followed by symptom recurrence after 2 weeks. Troponin was negative then, but C-reactive protein was 16 mg/L (reference <10 mg/L). Echocardiography and a computed tomography scan indicated increased pericardial effusion; thus, a second episode of isolated pericarditis was diagnosed. Therapy with NSAIDs and colchicine was reintroduced and could finally be tapered after 6 weeks without relapse.
Due to the non-availability of alternative (non-mRNA) vaccines in Switzerland at that time and due to the high individual risk for severe COVID in this patient, we discussed a re-exposure with a second dose of an mRNA vaccine to complete the immunization. In order to prevent the re-occurrence of myopericarditis, we initiated a prophylactic therapy with colchicine 0.5 mg every 12 h, starting a week before the second dose. The rationale for using an inflammasome-inhibiting drug as prophylaxis was based on the data suggesting inflammasome-induced inflammation in the pathogenesis of mRNA vaccine-associated myocarditis (1), and data indicating a reduced risk of (inflammasome mediated) mRNA vaccine induced gout flares on colchicine treatment (2). Because the symptoms developed exceptionally rapidly after the first dose, we opted to monitor the patient in the hospital for 72 h. He received the second dose of mRNA-1273 in September 2021, 5 months after the first dose. No symptoms, arrhythmias, or ECG changes occurred. Colchicine was discontinued 4 weeks after the second dose. The clinical course was uneventful. SARS-CoV-2-S-IgG/M antibody levels 5 weeks after second vaccination were >2,500 U/mL. Subsequently, the patient could successfully complete the vaccination course with a third dose of mRNA-1273, again under colchicine prophylaxis for 4 weeks and without evidence of myopericarditis. Figure 2 shows the timeline of the clinical milestones of the patient.
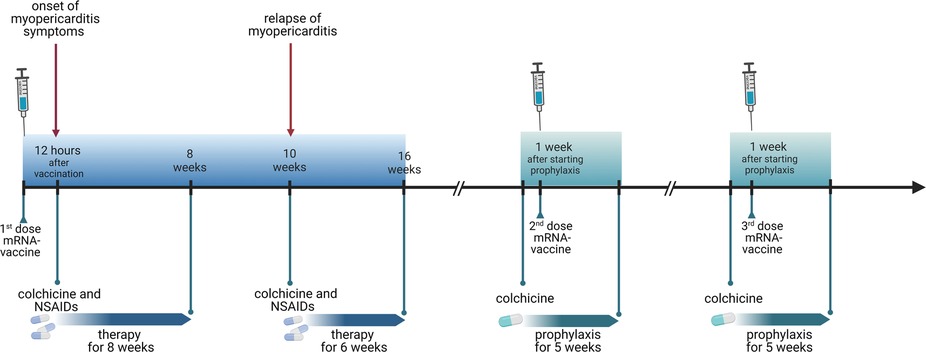
Figure 2. Timeline of clinical course (figure created with biorender.com).
We present a case of myopericarditis in temporal association with a first dose of an mRNA COVID vaccine. The patient had classical pericarditis and a substantial dynamic troponin elevation. The troponin level was elevated before an uneventful diagnostic angiography without intervention was performed. The cardiac MRI 2 days following the angiography showed no evidence of ischemia or alternative causes of the troponin elevation. Based on the case definitions for vaccine-associated myocarditis by the Brighton Collaboration, the case fulfilled the criteria for “probable myocarditis” in addition to pericarditis (3).
Pericarditis following mRNA COVID vaccinations has been reported, although actual incidence rates have not yet been established (4, 5), likely due to a mix between isolated myocarditis and myopericarditis (5). In a case series, Ochs et al. reported five cases of isolated pericarditis occurring within 7 days following COVID vaccination (6). In contrast to our case, these subjects had normal, or borderline elevated, troponin levels. Vaccine-induced myocarditis emerged as a rare but serious adverse event following immunization with mRNA—vaccines against SARS-CoV-2 during the postmarketing surveillance (7, 8). While no cases occurred in the pivotal phase III studies trials (8, 9), epidemiological data estimated the incidence of SARS-CoV-2 vaccine-associated myocarditis between 0.3 and 5.5 per 100 per 100,000 vaccinated persons (7, 10–16). Data from different studies are summarized in Table 2. Most frequently, mRNA vaccine-induced myocarditis occurred in young male (<40 years of age) 1–5 days after the second dose of an mRNA vaccine with higher incidence following mRNA-1273 than BNT162b. The clinical course was mostly mild with only a few patients requiring steroids or intensive care treatment while the majority responded well to NSAIDs (14). So far, no further risk factors for the onset of vaccine-induced myocarditis could be identified.
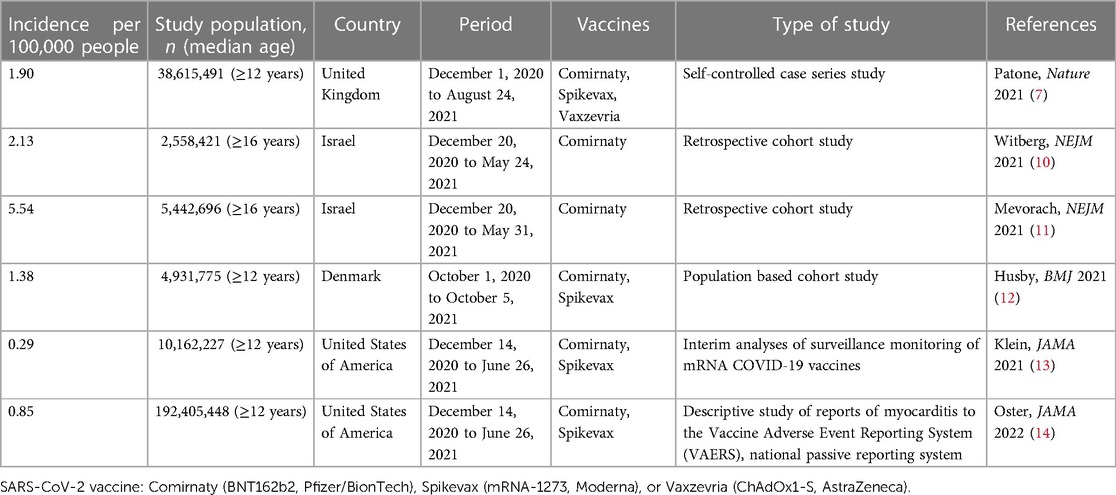
Table 2. Reported incidence of myocarditis among general population after at least one dose of after SARS-CoV-2 vaccine.
To the best of our knowledge, this is the first case report on mRNA vaccine-induced myopericarditis in a patient who underwent allogeneic HCT. This case shows various specific peculiarities. Our patient was already 70 years old, and the symptoms developed about 12 h after vaccination. Although young men seem to be at the highest risk and the median time to symptom onset is 2–3 days, in real life, the age range of persons affected by mRNA vaccine-associated myocarditis is much broader, and a considerable number of individuals become symptomatic within the first 24 h (14, 17).
The pathogenesis of myopericarditis associated with mRNA vaccination is not entirely understood but may involve a dysregulation of several immunological pathways, including mRNA-induced innate immune stimulation via Toll-like receptors, hypersensitivity reaction against vaccine components, molecular mimicry between cardiac self-antigen and the spike protein of SARS-CoV-2, or hormone-dependent alteration of inflammatory pathways (testosterone vs. estrogen) (7, 18–20). Recently, autoantibodies against the interleukin-1 receptor antagonist (IL-1RA) were found in histologically proven myocarditis cases after SARS-CoV-2 vaccination (21). Given the early onset of symptoms after a single dose of the mRNA and in the absence of a previous SARS-CoV-2 infection, it is unlikely that vaccine-induced adaptive immune mechanisms were involved in our case. Previously, an in-depth immunological analysis of a case of mRNA vaccine-associated myocarditis revealed a dysregulation of the innate immune system underlying the pathogenesis of myocarditis (19). The clinical response of our patient to colchicine, an inhibitor of the innate immunity, is well matching this hypothesis. Notably, the transplanted immune system could have interfered with those mechanisms contributing to this side effect presentation. Because this patient underwent allogeneic HCT, we also considered a flare of GvHD in differential diagnosis. Pericarditis as a sign of chronic GvHD is rare, usually manifests as part of a polyserositis and/or other signs of GvHD. Because systemic immunosuppression has already been stopped 7 months prior to the event of myopericarditis and no other clinical signs of GvHD occurred, we consider a GvHD flare highly unlikely.
Our patient presented with a severe clinical course requiring longer in-hospital management because of prolonged precordial pain and delayed troponin normalization. Colchicine is a standard of care for patients with pericarditis (22–25). While less frequently used for the treatment of myopericarditis, a recent study indicated better outcome of myopericarditis if treated with colchicine (26). Based on (i) the observation that the inflammasome pathway, that is targeted by colchicine (Figure 3), is involved in the pathogenesis of mRNA vaccine-associated myocarditis (1), and (ii) the reported reduced risk of gout flares in association with mRNA vaccinations in patients treated with colchicine (2), we speculated that colchicine may reduce the risk for symptom reoccurrence upon re-exposure to an mRNA vaccine. Indeed, colchicine seemed to be effective for both acute treatment and prophylaxis, allowing a safe re-exposure to the mRNA vaccine and thereby the completion of the immunization resulting in an adequate SARS-CoV-2-S-antibody response. Whether colchicine reduces the risk for mRNA vaccine-associated pericarditis and myocarditis should be assessed in larger patient cohorts.
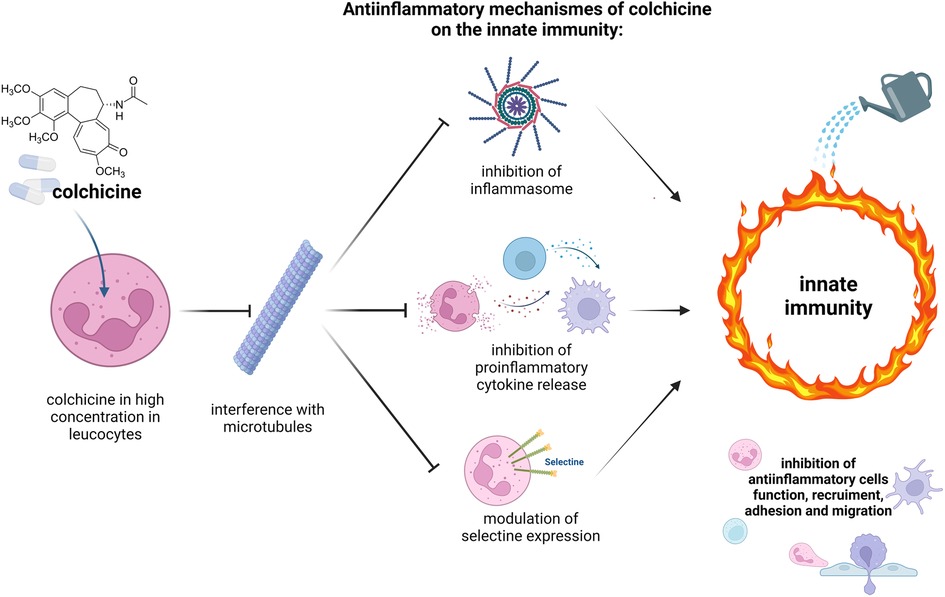
Figure 3. Mechanisms of action of colchicine on the innate immunity. High cytoplasmic concentration of colchicine especially in neutrophils are reached because of physiological reduced expression of transport P-glycoprotein (P-gp), which usually excretes drugs out of the cells. Colchicine inhibits assembly and attachment of microtubules. Consequently, several mechanisms of anti-inflammatory cell of the innate immunity are inhibited: inflammasome, a cytosolic multiprotein oligomers complex, which should activate an inflammatory cascade; release of proinflammatory cytokines (such as IL-1-β and IL-18) are downregulated; the expression E- and L-selectine on neutrophil surface, which promote the adhesion and the migration of those cells, are inhibited. This complex and sophisticated model results into inhibition of anti-inflammatory cells functions, recruitment, and motility of the innate immunity (22, 23, 25) (figure created with biorender.com).
Data on vaccine-re-exposure in patients experiencing a myopericarditis after a previous single dose of vaccination are scare (27). Due to the high individual risk for severe COVID and the ongoing pandemic situation, we decided to re-expose the patient to a second dose with the same vaccine (mRNA-1273 Spikevax; Moderna) but under colchicine prophylaxis. At that time only, mRNA vaccines (mRNA-1273 and BNT162b) were available in Switzerland; therefore, no switching to another class of vaccine was possible. At the time of the second vaccination, no data were available about the differences in the rate of myopericarditis among mRNA vaccines.
This report has some limitations: first, it is a single-case report of an immunocompromised patient after allogeneic HCT, thus precluding generally valid conclusions of our observations. Second, the presentation differed from published cases of mRNA vaccine-induced myocarditis by the absence of typical myocarditis findings, such as late gadolinium enhancement and edema, in the cardiac MRI. However, given the high troponin indicating myocardial injury and the extensive work-up to exclude alternative causes, probable myopericarditis could be diagnosed, according to the proposed case definition of the Brighton Collaboration (3). In line with this, the patient had chest pain over several days, and the troponin levels showed an increase to a peak 5 days following vaccination. Third, we cannot exclude that second dose was well-tolerated independent of colchicine prophylaxis. Finally, we only assessed humoral immunogenicity after the second dose and therefore cannot comment on whether colchicine may have affected the adaptive T-cell response to the vaccination in this patient. However, colchicine is generally not considered to interfere with adaptive immunity (Figure 3).
Our observation suggests that, following careful individual risk–benefit assessment, re-exposition can be safe under prophylaxis with colchicine inducing sufficient immunization thus reinforcing our conviction to continue a uniform and widespread vaccination campaign to protect our fragile patient population.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
All authors have contributed substantially to this work. LV and EH collected clinical data on the case; CZ performed the echocardiography; MS performed the MRI; LV reviewed the literature; and LV, JH, and CB wrote the draft of the manuscript. All authors contributed to the article and approved the submitted version.
The authors wish to thank the patient and the whole hospital staff, who has been taking care of him.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online https://www.frontiersin.org/articles/10.3389/fcvm.2023.1135848/full#supplementary-material.
ECG, electrocardiogram; GvHD, graft versus host disease; HCT, hematopoietic stem cell transplantation; MRI, magnetic resonance imaging; mRNA, messenger RNA; NTproBNP, N-terminal prohormone of brain natriuretic peptide; NSAID, non-steroidal anti-inflammatory drug; P-gp, transport protein p-glycoprotein.
1. Won T, Gilotra NA, Wood MK, Hughes DM, Talor MV, Lovell J, et al. Increased interleukin 18-dependent immune responses are associated with myopericarditis after COVID-19 mRNA vaccination. Front Immunol. (2022) 13:851620. doi: 10.3389/fimmu.2022.851620
2. Lu J, He Y, Terkeltaub R, Sun M, Ran Z, Xu X, et al. Colchicine prophylaxis is associated with fewer gout flares after COVID-19 vaccination. Ann Rheum Dis. (2022) 81(8):1189–93. doi: 10.1136/annrheumdis-2022-222199
3. Sexson Tejtel SK, Munoz FM, Al-Ammouri I, Savorgnan F, Guggilla RK, Khuri-Bulos N, et al. Myocarditis and pericarditis: case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. (2022) 40(10):1499–511. doi: 10.1016/j.vaccine.2021.11.074
4. Gao J, Feng L, Li Y, Lowe S, Guo Z, Bentley R, et al. A systematic review and meta-analysis of the association between SARS-CoV-2 vaccination and myocarditis or pericarditis. Am J Prev Med. (2023) 64(2):275–84. doi: 10.1016/j.amepre.2022.09.002
5. Buchan SA, Seo CY, Johnson C, Alley S, Kwong JC, Nasreen S, et al. Epidemiology of myocarditis and pericarditis following mRNA vaccination by vaccine product, schedule, and interdose interval among adolescents and adults in Ontario, Canada. JAMA Netw Open. (2022) 5(6):e2218505. doi: 10.1001/jamanetworkopen.2022.18505
6. Ochs MM, Haass M, Hagstotz S, Giusca S, Korosoglou G. Case report: case series of isolated acute pericarditis after SARS-CoV-2 vaccinations. Front Cardiovasc Med. (2022) 9:990108. doi: 10.3389/fcvm.2022.990108
7. Patone M, Mei XW, Handunnetthi L, Dixon S, Zaccardi F, Shankar-Hari M, et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med. (2022) 28(2):410–22. doi: 10.1038/s41591-021-01630-0
8. Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. (2021) 384(5):403–16. doi: 10.1056/NEJMoa2035389
9. Thomas SJ, Moreira ED Jr, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine through 6 months. N Engl J Med. (2021) 385(19):1761–73. doi: 10.1056/NEJMoa2110345
10. Witberg G, Barda N, Hoss S, Richter I, Wiessman M, Aviv Y, et al. Myocarditis after COVID-19 vaccination in a large health care organization. N Engl J Med. (2021) 385(23):2132–9. doi: 10.1056/NEJMoa2110737
11. Mevorach D, Anis E, Cedar N, Bromberg M, Haas EJ, Nadir E, et al. Myocarditis after BNT162b2 mRNA vaccine against COVID-19 in Israel. N Engl J Med. (2021) 385(23):2140–9. doi: 10.1056/NEJMoa2109730
12. Husby A, Hansen JV, Fosbol E, Thiesson EM, Madsen M, Thomsen RW, et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study. Br Med J. (2021) 375:e068665. doi: 10.1136/bmj-2021-068665
13. Klein NP, Lewis N, Goddard K, Fireman B, Zerbo O, Hanson KE, et al. Surveillance for adverse events after COVID-19 mRNA vaccination. J Am Med Assoc. (2021) 326(14):1390–9. doi: 10.1001/jama.2021.15072
14. Oster ME, Shay DK, Su JR, Gee J, Creech CB, Broder KR, et al. Myocarditis cases reported after mRNA-based COVID-19 vaccination in the US from December 2020 to August 2021. J Am Med Assoc. (2022) 327(4):331–40. doi: 10.1001/jama.2021.24110
15. Gargano JW, Wallace M, Hadler SC, Langley G, Su JR, Oster ME, et al. Use of mRNA COVID-19 vaccine after reports of myocarditis among vaccine recipients: update from the advisory committee on immunization practices—United States, June 2021. Morb Mortal Wkly Rep. (2021) 70(27):977–82. doi: 10.15585/mmwr.mm7027e2
16. Barda N, Dagan N, Ben-Shlomo Y, Kepten E, Waxman J, Ohana R, et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N Engl J Med. (2021) 385(12):1078–90. doi: 10.1056/NEJMoa2110475
17. Truong DT, Dionne A, Muniz JC, McHugh KE, Portman MA, Lambert LM, et al. Clinically suspected myocarditis temporally related to COVID-19 vaccination in adolescents and young adults: suspected myocarditis after COVID-19 vaccination. Circulation. (2022) 145(5):345–56. doi: 10.1161/CIRCULATIONAHA.121.056583
18. Heymans S, Cooper LT. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nat Rev Cardiol. (2022) 19(2):75–7. doi: 10.1038/s41569-021-00662-w
19. Bozkurt B, Kamat I, Hotez PJ. Myocarditis with COVID-19 mRNA vaccines. Circulation. (2021) 144(6):471–84. doi: 10.1161/CIRCULATIONAHA.121.056135
20. Hirsiger JR, Tzankov A, Alborelli I, Recher M, Daikeler T, Parmentier S, et al. Case report: mRNA vaccination-mediated STAT3 overactivation with agranulocytosis and clonal T-LGL expansion. Front Immunol. (2023) 14:1087502. doi: 10.3389/fimmu.2023.1087502
21. Thurner L, Kessel C, Fadle N, Regitz E, Seidel F, Kindermann I, et al. IL-1RA antibodies in myocarditis after SARS-CoV-2 vaccination. N Engl J Med. (2022) 387(16):1524–7. doi: 10.1056/NEJMc2205667
22. Leung YY, Yao Hui LL, Kraus VB. Colchicine—update on mechanisms of action and therapeutic uses. Semin Arthritis Rheum. (2015) 45(3):341–50. doi: 10.1016/j.semarthrit.2015.06.013
23. Casanova P, Artola RT, Mihos CG, Pineda AM, Santana O. The cardiovascular effects of colchicine: a comprehensive review. Cardiol Rev. (2015) 23(6):317–22. doi: 10.1097/CRD.0000000000000056
24. Sawalha K, Abozenah M, Kadado AJ, Battisha A, Al-Akchar M, Salerno C, et al. Systematic review of COVID-19 related myocarditis: insights on management and outcome. Cardiovasc Revasc Med. (2021) 23:107–13. doi: 10.1016/j.carrev.2020.08.028
25. Imazio M, Nidorf M. Colchicine and the heart. Eur Heart J. (2021) 42(28):2745–60. doi: 10.1093/eurheartj/ehab221
26. Behbahani-Nejad O, Mikolich B, Morgenstern D, Mikolich JR. Myocarditis response to colchicine therapy based on cardiac MRI diagnostic criteria. J Am Coll Cardiol. (2021) 77(18_Supplement_1):1432. doi: 10.1016/S0735-1097(21)02790-X
27. Banholzer S, Helbling A, Haschke M. Successful re-exposure to COVID-19 mRNA vaccination at a reduced dosage in a patient with clinically suspected pericarditis/myocarditis after a first dose of COVID-19 vaccine. In: Swissmedic, editor. Bern: Swissmedic, Swiss Agency for Therapeutic Products. Swissmedic Vigilance News (2022), p. 10–13.
Keywords: mRNA vaccine, myocarditis, colchicine, allogeneic stem cells transplantation, COVID-19, mRNA-1273
Citation: Valore L, Junker T, Heilmann E, Zuern CS, Streif M, Drexler B, Arranto C, Halter JP and Berger CT (2023) Case report: mRNA-1273 COVID-19 vaccine-associated myopericarditis: Successful treatment and re-exposure with colchicine. Front. Cardiovasc. Med. 10:1135848. doi: 10.3389/fcvm.2023.1135848
Received: 22 January 2023; Accepted: 27 March 2023;
Published: 17 April 2023.
Edited by:
Grigorios Korosoglou, GRN Klinik Weinheim, GermanyReviewed by:
Marco Ochs, Angiologie und internistische Intensivmedizin, Germany© 2023 Valore, Junker, Heilmann, Zuern, Streif, Drexler, Arranto, Halter and Berger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Valore bHVjYS52YWxvcmVAdXNiLmNo
Specialty Section: This article was submitted to General Cardiovascular Medicine, a section of the journal Frontiers in Cardiovascular Medicine
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.