 Xueyao Yang1†Jinfan Tian1†Lijun Zhang2Wei Dong3Hongzhi Mi3Jianan Li1Jiahui Li1Ye Han4Huijuan Zuo5Jing An6Yi He4*Xiantao Song1*
Xueyao Yang1†Jinfan Tian1†Lijun Zhang2Wei Dong3Hongzhi Mi3Jianan Li1Jiahui Li1Ye Han4Huijuan Zuo5Jing An6Yi He4*Xiantao Song1*- 1Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China
- 2Department of Radiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China
- 3Department of Nuclear Medicine, Beijing Anzhen Hospital, Capital Medical University, Beijing, China
- 4Department of Radiology, Beijing Friendship Hospital, Capital Medical University, Beijing, China
- 5Department of Community Health Research, Beijing Institute of Heart, Lung and Blood Vessel Disease, Beijing Anzhen Hospital, Capital Medical University, Beijing, China
- 6Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
A Corrigendum on
Myocardial Viability, Functional Status, and Collaterals of Patients With Chronically Occluded Coronary Arteries
by Yang, X., Tian, J., Zhang, L., Dong, W., Mi, H., Li, J., Li, J., Han, Y, Zuo, H., An, J., He, Y., and Song, X. (2021). Front. Cardiovasc. Med. 8:754826. doi: 10.3389/fcvm.2021.754826
In the Abstract section of original article, there was an error. There is a typo in the “Conclusion” of the abstract of this paper, where “Myocardial infarction detected by CMR is widespread among patients with CMO” should be changed to “Myocardial infarction detected by CMR is widespread among patients with CTO.”
In the original article, there were some mistakes in Table 1 as published. The total number of patients who had hypertension should be 115 (59%) instead of 125 (64%). The mean ± standard deviation of LVEF (%) of all patients, patients with no scar in CTO territory and patients with scar in CTO territory should be 53.3 ± 14.9, 58.3 ± 12.7, 50.7 ± 15.2, respectively. The mean ± standard deviation of LVEDV (mL) of all patients, patients with no scar in CTO territory and patients with scar in CTO territory should be 107.1 ± 44.8, 90.0 ± 32.4, and 115.9 ± 47.8, respectively. The mean ± standard deviation of LVESV (mL) of all patients, patients with no scar in CTO territory and patients with scar in CTO territory should be 53.3 ± 37.8, 38.7 ± 20.1, and 61.1 ± 42.4, respectively. The corrected Table 1 appears below.
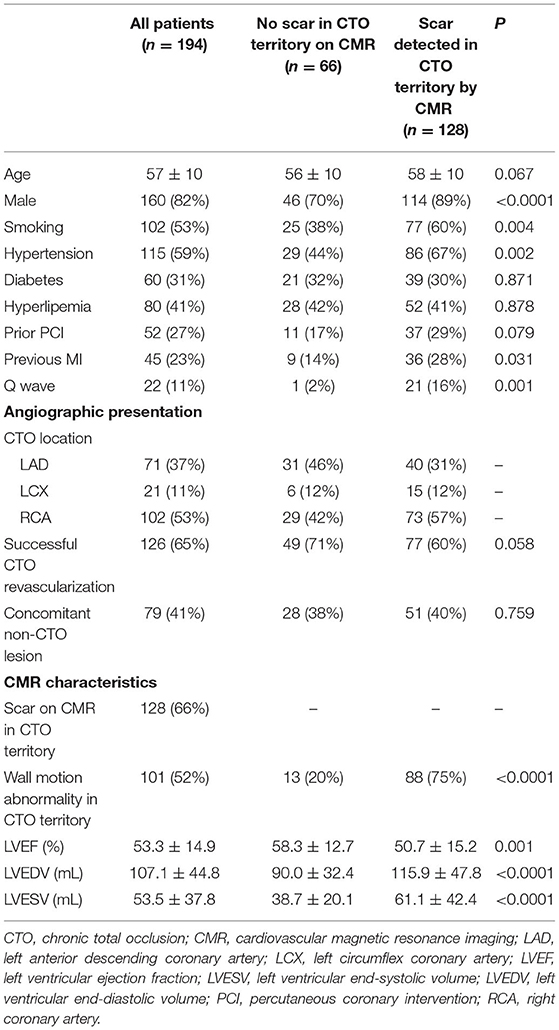
Table 1. Baseline characteristics.
The authors apologize for this error and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: chronic total occlusion, myocardial viability, coronary artery disease, cardiovascular magnetic resonance, cardiac function
Citation: Yang X, Tian J, Zhang L, Dong W, Mi H, Li J, Li J, Han Y, Zuo H, An J, He Y and Song X (2022) Corrigendum: Myocardial Viability, Functional Status, and Collaterals of Patients With Chronically Occluded Coronary Arteries. Front. Cardiovasc. Med. 9:877972. doi: 10.3389/fcvm.2022.877972
Received: 17 February 2022; Accepted: 18 February 2022;
Published: 18 March 2022.
Approved by:
Frontiers Editorial Office, Frontiers Media SA, SwitzerlandCopyright © 2022 Yang, Tian, Zhang, Dong, Mi, Li, Li, Han, Zuo, An, He and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiantao Song, songxiantao0929@qq.com; Yi He, heyi139@sina.com
†These authors have contributed equally to this work