 Francisco Javier Ortiz de Frutos1Carolina Cisneros2José Miguel Villacampa3Óscar Palomares4Ignacio Dávila5*
Francisco Javier Ortiz de Frutos1Carolina Cisneros2José Miguel Villacampa3Óscar Palomares4Ignacio Dávila5*
- 1Dermatology Department, University Hospital 12 de Octubre, Madrid, Spain
- 2Pneumology Department, La Princesa Hospital, Madrid, Spain
- 3ENT Department, Fundación Jiménez Díaz University Hospital, Madrid, Spain
- 4Department of Biochemistry and Molecular Biology, School of Chemistry, Complutense University of Madrid, Madrid, Spain
- 5Allergy Service, University Hospital of Salamanca, Red de Enfermedades Inflamatorias, ISCIII, Departamento de Ciencias Biomédicas y del Diagnóstico, Instituto de Investigación Biosanitaria de Salamanca, Salamanca, Spain
Objective: This study aimed to validate a 15-item screening questionnaire for the early detection of coexisting type 2 (T2) inflammatory diseases, such as asthma, atopic dermatitis, and chronic rhinosinusitis with nasal polyps (CRSwNP), among others.
Methods: The questionnaire, designed through expert consensus by a scientific committee, underwent Delphi methodology for validation. A multidisciplinary panel of 19 clinicians from different specialties reviewed the questionnaire for clinical relevance, while 39 patients from different regions of Spain evaluated its comprehensibility.
Results: The clinician panel reached a consensus on the relevance of 13 out of 15 items in the first round and agreed that a single positive response was sufficient to justify referral to the appropriate specialist. Two items were modified and validated in the second round. The patient panel unanimously agreed on the comprehensibility of the questionnaire in the first round. Linguistic variations were also ranked to ensure clarity across regions, further enhancing the validation of the tool.
Conclusion: This validated questionnaire offers a practical tool for early detection of T2 inflammatory diseases. Its simplicity and comprehensibility, confirmed by clinicians and patients, make it suitable for use in various healthcare settings, supporting timely specialist referrals and improved patient care. Future studies will evaluate its effectiveness in real-world clinical practice.
1 Introduction
Dysregulation of type 2 (T2) immune responses, a natural defense mechanism under normal circumstances, can lead to pathological inflammation and is implicated in the pathophysiology of various diseases, such as asthma, atopic dermatitis (AD), and chronic rhinosinusitis with nasal polyps (CRSwNP), among others (1, 2). This common endotype partly explains the frequent coexistence and similar pathophysiological features of these entities. Despite advances in understanding the mechanisms driving T2 inflammation, leading to the development of targeted therapeutic strategies, significant unmet needs persist (3). In this respect, inadequate interdisciplinary communication and the absence of effective detection tools can delay diagnosis, resulting in suboptimal patient care. In fact, patients themselves have emphasized the necessity for interdisciplinary collaboration in managing T2-mediated diseases (4).
In response to this need, we recently developed a short questionnaire based on the cardinal symptoms of T2-mediated inflammatory diseases, in order to promote the early detection of coexisting T2 pathologies (5). Briefly, a comprehensive literature review was performed and expert meetings were conducted to develop a 15-item questionnaire to identify the eight most prevalent T2 diseases: asthma, CRSwNP, allergic rhinitis, allergic conjunctivitis, IgE-mediated food allergy, AD, eosinophilic esophagitis (EoE), and nonsteroidal anti-inflammatory drug-exacerbated respiratory disease (N-ERD). The questionnaire was drafted using patient-friendly language that allows them to identify and describe their symptoms easily. This tool, designed for clinical practice in Spain, is intended to be implemented across all levels of care, from primary to specialized settings, in both public and private healthcare systems, to support the initial screening of patients for suspected coexisting T2 diseases.
The present study aims to validate this questionnaire's item construction and language choice.
2 Methods
2.1 Study design and panel formation
A schematic workflow of the study is shown in Figure 1. First, the language and construction of items from the initial questionnaire were reviewed by the scientific committee previously responsible for its development (5) to identify synonyms and alternative phrasings for each concept. Subsequently, the clinical relevance of the selected items and the proposal that one positive answer to any of the questionnaire items would be sufficient for specialist derivation were tested in a Delphi consultation conducted with a panel of physicians from each specialty. The previously identified linguistic variants were also assessed through a simple preference ranking. After the clinicians validated the questionnaire, a selection of patients from patient advocacy groups were invited to validate its ease of comprehension, also through a Delphi consultation. These consultation rounds were conducted through a survey implemented on the SurveyMonkey platform (https://www.surveymonkey.com/).
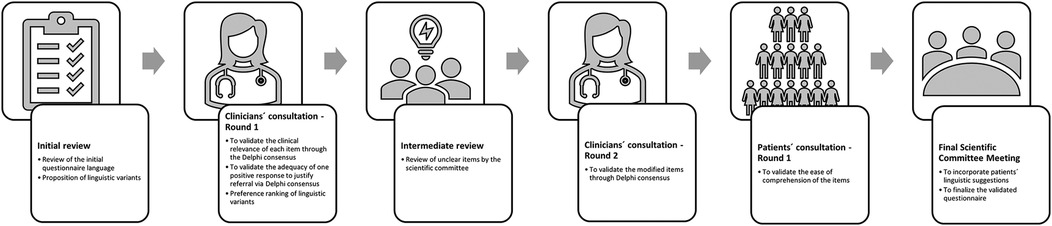
Figure 1. Workflow of the validation process.
The scientific committee members recommended three to seven experts from each relevant specialty to form the panel of physicians, dispersed geographically across the entire national Spanish territory. Those who accepted the invitation to participate formed a multidisciplinary panel of 19 clinicians. The panel included four otolaryngologists, three dermatologists, four pulmonologists, six allergists, and two immunologists. A modified questionnaire was developed on the basis of on the survey results from this panel. The revised questionnaire underwent a Delphi consultation process with a panel of 39 patients from patient associations diagnosed with at least one T2-related pathology. Five associations were contacted by phone to explain the study and invite participation. Subsequently, an email was sent with further details, requesting that each one selected at least five patients (adults with moderate to severe conditions). The Delphi methodology was outlined, highlighting the need for committed participants due to the potential for two questionnaire rounds. A follow-up email containing the link to the questionnaire was then provided. The associations were tasked with overseeing the selected participants, ensuring that only those who completed the first round would be eligible to respond to a second round, if necessary.
2.2 Delphi process and consensus criteria
The Delphi process involved iterative rounds of feedback and consensus from the multidisciplinary panels of experts and patients to ensure the questionnaire's relevance, clarity, and practical utility and to validate and refine the tool effectively. Based on the “BIOMED Concerted Action on Appropriateness” definitions for different panel sizes, the criteria for disagreement and agreement were established for a panel size of 19 and 39 clinicians and patients, respectively (6).
The Rand/UCLA appropriateness method was used for consensus analysis within the panels (6). Each item of the questionnaire was classified as “Appropriate”, “Uncertain”, or “Inappropriate”, based on the median score of the panel and the degree of agreement among panelists. Thus, items were categorized as “Appropriate”, if the median score ranged from 7–9, “Uncertain”, if the median score ranged from 4–6 or any median in disagreement, and “Inappropriate”, if the median score ranged from 1–3. The criteria for the degree of agreement were as follows: “Disagreement” if the median fell at one extreme (ranges 1–3 or 7–9) and the number of ratings at the opposite extreme was greater than or equal to one-third of the panel size or if the median fell in the range 4–6 and the number of ratings at one of the extremes was greater than or equal to one-third of the panel size. “Agreement” was established when the number of ratings outside the range containing the median was less than one-third of the panel size. A “Neutral” classification was used when neither agreement nor disagreement was achieved.
2.3 Evaluation metrics and data analysis
The clinicians' evaluation encompassed several aspects. Sociodemographic variables, including age, gender, region, hospital level, specialty, and years of experience were recorded. Clinicians then assessed the relevance of questionnaire items and if one positive response was sufficient for referral. Panelists also provided a ranking of linguistic variants of technical terms to ensure clarity for patient understanding.
Patients evaluated the comprehensibility of the questionnaire from their perspective and provided sociodemographic and clinical data. Patients were also given the opportunity to provide comments on each item of the questionnaire, so that they could express any doubts they had about the questions or offer suggestions regarding the clarity and ease of understanding.
3 Results
The panel of clinicians consisted of 19 specialists whose sociodemographic characteristics are shown in Table 1. In the first Delphi round, consensus was reached on two aspects: the clinical relevance of each questionnaire item (n = 15) for referral to another specialist and the sufficiency of a single positive response to justify referral. Two questionnaire items failed to reach a consensus regarding their clinical relevance and were returned to the scientific committee for modification. Item number 1 was deemed “uncertain” (most of the panel doubted the appropriateness of the statement's wording) and reached “disagreement” (most of the panel was unsure about the relevance of this item for referral to the corresponding specialist). Item number 13 was considered “appropriate” in terms of the statement's correctness but “neutral” (there was no agreement within the panel regarding the relevance of this item for referral). These two items were then modified and resubmitted to the clinician's panel in Delphi round 2. They were then considered appropriate and achieved consensus. Additionally, different linguistic options were explored for every item, and the most preferred option for each item was incorporated into the new version of the questionnaire (Supplementary Table S3).

Table 1. Demographic characteristics of the panel of clinicians.
The patient sample comprised 39 individuals who provided demographic and clinical data (Table 2). They were presented with the questionnaire version that had been validated by clinician consensus and featured the top-ranked language variants. Consensus was achieved on the ease of comprehension of the questionnaire items. The scientific committee examined the patients' comments from the first round and used them to make slight linguistic adjustments to specific terms. However, these changes were not deemed sufficiently significant to warrant another round of consultation, given that the comprehensibility of all items had already been agreed upon in the first round. This process led to the final validated version of the questionnaire (Supplementary Tables S1, S2). A summary of the results from the three rounds of the Delphi process is shown in Table 3.
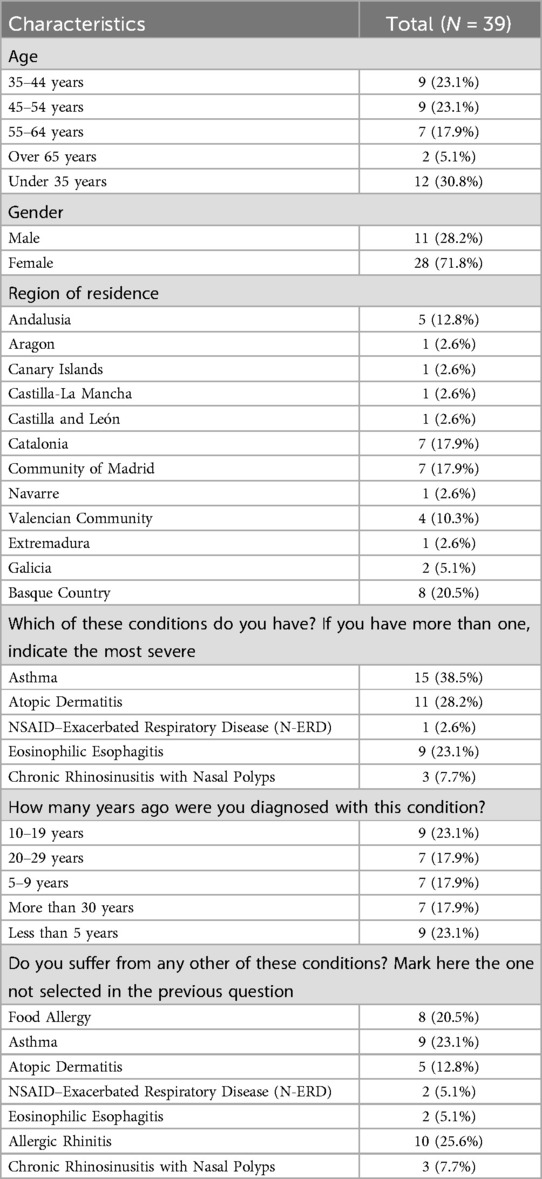
Table 2. Demographic and clinical characteristics of the panel of patients.

Table 3. Summary of the results from the three rounds of the Delphi process.
4 Discussion
This study aimed to validate a previously developed screening tool to identify and facilitate early referral for T2 inflammation-related diseases (5), addressing critical gaps in interdisciplinary communication and early detection. Although the appropriate referral of patients has been primarily reported as a major challenge in the case of asthma (7), this issue seems equally relevant to other pathologies driven by T2 inflammation. In fact, in the specific case of patients with difficult-to-control asthma, identifying and effectively treating asthma comorbidities, including other T2-driven conditions such as chronic sinusitis with nasal polyps, may improve asthma control and reduce exacerbations (8). Furthermore, identifying comorbid T2 inflammatory conditions may help guide the optimal selection of biologic therapies (8).
The validation process results highlight the potential of this tool to prevent missing any coexisting T2 diseases and avoid delays in evaluation by the corresponding specialist, thereby improving patient care and outcomes. The Delphi technique is well-suited to the study's objective, as it has allowed many individuals from diverse locations and areas of expertise to participate anonymously, thus preventing the domination of the consensus process by one or a few experts (9). In this case, the role of the Delphi method is further enhanced by the collaborative strategy between clinicians and patients. In fact, including expert patients in the validation process is a crucial aspect of this study, as this approach has proven effective in other contexts (10, 11). The consensus achieved for most questionnaire items in the first Delphi round with clinicians in terms of comprehensibility and clinical relevance highlights the robustness of the questionnaire in identifying key indicators of T2 inflammatory diseases that warrant further evaluation.
Furthermore, affirming that a single positive response was sufficient to justify referral to a specialist is a significant advantage for this questionnaire. The only two items that initially failed to reach consensus were Question 1 (related to cough as a cardinal asthma symptom) and Question 13 (related to dysphagia in eosinophilic esophagitis). This was probably because the questions did not provide sufficient details and, as such, were unclear. However, after the scientific committee made consistent modifications regarding more specific signs, their duration, time of day or situation, and/or intensity, a consensus was achieved for these two items in the subsequent round. The ease of comprehension and the significance of patient input in refining the questionnaire after only one round, in which consensus was achieved for all items with a median score of 9, are remarkable. Moreover, the fact that the questionnaire's comprehensibility was evaluated by patients from different regions of Spain, each with distinct linguistic characteristics, further reinforces the validation results. Despite the relatively limited sample, the sociodemographic and clinical variables of the overall T2 population were adequately represented, except for patients over 65 years old who, as expected, were underrepresented.
Other authors have highlighted the need for improved diagnostic tools and multidisciplinary approaches to managing T2 inflammation-related diseases (12). A recent survey sponsored by the patient-driven T2i Network Project identified the common drivers and challenges related to the quality of life of patients with T2 inflammatory diseases from the patient's perspective (13). Senna et al. emphasized how a multidisciplinary team can serve as a central point for patient management, improving outcomes, reducing costs, and ensuring the most appropriate therapeutic decisions (14).
This validated questionnaire might therefore potentially help to overcome these unmet needs. It can be integrated into various healthcare settings, particularly primary care, although the questionnaire is designed to be adaptable across different healthcare levels, from primary care to specialized clinical settings, both in the public and private sectors. By providing a structured approach to symptom identification, this tool can enhance communication among specialists and primary care providers, ensuring that patients with suspected Type 2 inflammatory diseases are referred to the appropriate specialists without unnecessary delays. For example, in clinical practice, this questionnaire could be used as a screening tool in primary care consultations, facilitating early referral to specialized units. Moreover, in a hospital setting, its use by multidisciplinary teams would allow for systematic case identification and better coordination between different specialties, such as dermatology, ORL, or asthma units. This would ultimately lead to more personalized treatment strategies, particularly in selecting biological therapies tailored to individual patient profiles. A possible implementation model could involve its integration into the electronic medical record, with automated alerts for referrals when certain risk thresholds are met.
Despite its strengths, this study has limitations. The Delphi process itself may have introduced potential biases, for example, by including patient representatives from patient associations. These members may likely present with more severe forms of the disease and are usually more familiar with its clinical characteristics. This could skew the results, as the questionnaire is intended for early-stage diagnosis. However, it is worth noting that these patients may have severe forms of their primary diagnosed condition but not necessarily of the associated comorbidities. It is also worth considering whether the consensus decision to refer patients based on a single positive response could present a limitation. Even though this criterion simplifies decision-making, there is some uncertainty about whether it might lead to either unnecessary referrals or insufficient sensitivity to variations in disease severity, and further investigation is warranted. Another limitation concerns the unclear minimum age at which the questionnaire is valid. The current panel consisted of adult patients (over 18 years) who answered for themselves, and the questionnaire has not been validated with caregivers of pediatric patients. While it is reasonable to assume that caregivers will comprehend the items as adult patients did, specific symptoms may be more easily recognized in young children by caregivers, while others might be more challenging, especially in non-verbal pediatric patients. Nonetheless, the ability to implement the questionnaire in most patients would represent a significant advancement. Overall, these limitations should be considered when interpreting the findings, as they may affect their generalizability. The selection of experts and patients within the Delphi method may introduce biases, and the study's single-country scope, along with the exclusion of pediatric populations, may limit its applicability to broader, international, and younger patient groups. Therefore, although this method provides expert consensus on the development of the questionnaire, the external validity of our findings may be limited, as the composition of the panel may not fully represent the clinical variability in different healthcare settings.
Thus, several future actions are necessary to continue this line of research. First, further large-scale validation of this screening tool in larger, more diverse populations must confirm its applicability across different healthcare settings. Future studies should focus on prospective validation in real-world clinical practice, assessing its performance in various demographic and clinical contexts and its impact on referral accuracy and patient outcomes. Translating and validating the questionnaire across various languages and cultural contexts will be crucial for global use. Continuous refinement based on real-world application and feedback will further improve its accuracy and relevance. Additionally, ongoing education and clinician training will be essential to maximize the questionnaire's effectiveness. Finally, integrating the tool into electronic health records could greatly enhance accessibility and ease of use, paving the way for its broader implementation in clinical practice.
5 Conclusions
This screening questionnaire provides a simple and practical tool for the early detection of coexisting T2 inflammatory diseases, enhancing comprehensive and personalized patient care by increasing multidisciplinary efforts and accelerating diagnosis. The next phase will involve evaluating the questionnaire's effectiveness in real-world clinical settings to determine its practical utility.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of Hospital 12 de Octubre (Madrid, Spain). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because no interventional human studies were conducted, the study involved patient data collection through a survey which was anonymous and did not collect any identifiable participant information.
Author contributions
FO: Conceptualization, Formal analysis, Validation, Writing – review & editing. CC: Conceptualization, Formal analysis, Validation, Writing – review & editing. JV: Conceptualization, Formal analysis, Validation, Writing – review & editing. ÓP: Conceptualization, Formal analysis, Validation, Writing – review & editing. ID: Conceptualization, Formal analysis, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Methodological support and writing were provided by Laura Hidalgo, Ph.D., and Maria Giovanna Ferrario, Ph.D. (Medical Science Consulting, Valencia, Spain), funded by Sanofi.
Acknowledgments
We thank Dr. Laura Hidalgo and Dr. Maria Giovanna Ferrario (Medical Science Consulting, Valencia) for their methodological, review literature and medical writing support. We gratefully acknowledge the Asociación Española de Esofagitis Eosinofílica (AEDESEO), Asociación Española de Poliposis Nasal (AEPONA), Asociación Sevilla Respira, Asociación para el Apoyo a Personas Afectadas por el Asma de Euskadi (ASMABI), and Asociación de Afectados por la Dermatitis Atópica (AADA) for their invaluable assistance in managing the creation and monitoring of the patient panel for this validation study.
Conflict of interest
OP has received fees for lectures or participation in advisory boards from AstraZeneca, Diater, GSK, Pfizer, Immunotek SL, Novartis, Regeneron, and Sanofi Genzyme. OP has received research grants from Immunotek SL, Novartis SL, AstraZeneca, MINECO, MICINNIN, and CAM. CC states that she has received financial support in the past three years from AstraZeneca, Chiesi, Novartis, Sanofi, Mundifarma, GSK, Menarini, Pfizer, Gebro Pharma, and TEVA for advisory services, articles, research studies, attending congresses or training courses. FO has received honoraria for serving on advisory boards from Novartis, Astellas, Uriach, Sanofi, GSK, Pfizer, Abbvie, Lilly, and Leo; for participation in lectures from Leo, BDF, Astellas, Novartis, MSD, and Sanofi; for participation in clinical trials from Astellas, Novartis, Bayer, Sanofi, Leo, Lilly, Pfizer, and Abbvie; and has received grants for congresses from Isdin, Menarini, Astellas, Novartis, MSD, Sanofi, Leti, Leo, and Abbvie. JV has received honoraria for serving on advisory boards from AstraZeneca, GlaxoSmithKline, and Sanofi and for participation in lectures from Cinfa, GlaxoSmithKline, Sanofi, and Viatris. In the past three years, ID has received payment for lectures, including serving on speaker's bureaus from Allergy Therapeutics, AstraZeneca, Chiesi, Diater, GSK, Leti, Novartis, Sanofi; for a consultancy from Allergy Therapeutics, ALK-Abello, AstraZeneca, GSK, Merck, MSD, Novartis, Sanofi; and grants from Thermofisher Diagnostics, ISCIII, and Junta de Castilla y León.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/falgy.2025.1543504/full#supplementary-material
References
1. Henry EK, Inclan-Rico JM, Siracusa MC. Type 2 cytokine responses: regulating immunity to helminth parasites and allergic inflammation. Curr Pharmacol Rep. (2017) 3(6):346–59. doi: 10.1007/s40495-017-0114-1
2. McCormick JP, Lee JT. Insights into the implications of coexisting type 2 inflammatory diseases. J Inflamm Res. (2021) 14:4259–66. doi: 10.2147/jir.S311640
3. Hassoun D, Malard O, Barbarot S, Magnan A, Colas L. Type 2 immunity-driven diseases: towards a multidisciplinary approach. Clin Exp Allergy. (2021) 51(12):1538–52. doi: 10.1111/cea.14029
4. De Prins L, Raap U, Mueller T, Schmid-Grendelmeier P, Haase CH, Backer V, et al. White paper on European patient needs and suggestions on chronic type 2 inflammation of airways and skin by euforea. Front Allergy. (2022) 3:889221. doi: 10.3389/falgy.2022.889221
5. Palomares O, Cisneros C, Ortiz de Frutos FJ, Villacampa JM, Dávila I. Multidisciplinary management of type 2 inflammation diseases using a screening tool. Front Allergy. (2024) 5:1427279. doi: 10.3389/falgy.2024.1427279
6. Fitch K, Bernstein SJ, Aguilar MD, Burnand B, LaCalle JR, Lazaro P, et al. The Rand/Ucla Appropriateness Method User’s Manual. Santa Monica, CA: RAND Corporation (2001).
7. Pavord I, Bahmer T, Braido F, Cosío BG, Humbert M, Idzko M, et al. Severe T2-high asthma in the biologics era: european experts’ opinion. Eur Respir Rev. (2019) 28(152):190054. doi: 10.1183/16000617.0054-2019
8. Gaffin JM, Castro M, Bacharier LB, Fuhlbrigge AL. The role of comorbidities in difficult-to-control asthma in adults and children. J Allergy Clin Immunol Pract. (2022) 10(2):397–408. doi: 10.1016/j.jaip.2021.11.016
9. Powell C. The delphi technique: myths and realities. J Adv Nurs. (2003) 41(4):376–82. doi: 10.1046/j.1365-2648.2003.02537.x
10. Bull C, Crilly J, Latimer S, Gillespie BM. Establishing the content validity of a new emergency department patient-reported experience measure (ed Prem): a Delphi study. BMC Emerg Med. (2022) 22(1):65. doi: 10.1186/s12873-022-00617-5
11. Engler K, Vicente S, Mate KKV, Lessard D, Ahmed S, Lebouché B. Content validation of a new measure of patient-reported barriers to antiretroviral therapy adherence, the I-score: results from a Delphi study. J Patient Rep Outcomes. (2022) 6(1):28. doi: 10.1186/s41687-022-00435-0
12. Kolkhir P, Akdis CA, Akdis M, Bachert C, Bieber T, Canonica GW, et al. Type 2 chronic inflammatory diseases: targets, therapies and unmet needs. Nat Rev Drug Discov. (2023) 22(9):743–67. doi: 10.1038/s41573-023-00750-1
13. Gómez de la Fuente E, Alobid I, Ojanguren I, Rodríguez-Vázquez V, Pais B, Reyes V, et al. Addressing the unmet needs in patients with type 2 inflammatory diseases: when quality of life can make a difference. Front Allergy. (2023) 4:1296894. doi: 10.3389/falgy.2023.1296894
Keywords: T2 inflammation, management, multidisciplinary, screening, questionnaire
Citation: Ortiz de Frutos FJ, Cisneros C, Villacampa JM, Palomares Ó and Dávila I (2025) Development and validation of a Delphi consensus-based questionnaire for the multidisciplinary management of type 2 inflammation-related diseases. Front. Allergy 6:1543504. doi: 10.3389/falgy.2025.1543504
Received: 11 December 2024; Accepted: 17 March 2025;
Published: 3 April 2025.
Edited by:
Olga Lourenço, University of Beira Interior, PortugalReviewed by:
Ayse Fusun Kalpaklioglu, Kırıkkale University, TürkiyeNorma De Paula Motta Rubini, Rio de Janeiro State Federal University, Brazil
Copyright: © 2025 Ortiz de Frutos, Cisneros, Villacampa, Palomares and Dávila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ignacio Dávila, idg@usal.es