 J. J. Ley-Tomas
J. J. Ley-Tomas A. M. Xicotencatl-Tellez†,§
A. M. Xicotencatl-Tellez†,§ M. L. García-Cruz
M. L. García-Cruz M. A. Jiménez-Chobillon
M. A. Jiménez-Chobillon- IAPA ’s Clinic, Department of Otorhinolaryngology–Head and Neck Surgery, Instituto Nacional de Enfermedades Respiratorias, Ismael Cosío Villegas, Ciudad de México, México
It has been estimated that Nonsteroidal Anti-inflammatory drug (NSAID) Exacerbated Respiratory Disease (N-ERD) previously named as Aspirin Exacerbated Respiratory Disease (A-ERD) affects around 1.4 million persons in the United States. Its prevalence in asthmatic patients has widely been underestimated, as a considerable number of patients would need an aspirin provocation test to confirm the diagnosis. N-ERD physiopathology is somehow complex, but basically involves an imbalance in the arachidonic acid metabolite pathway. The syndrome is characterized by the presence of asthma, chronic rhinosinusitis with nasal polyposis (CRSwNP) and NSAID and aspirin intolerance. Despite maximal and comprehensive medical treatment, the disease tends to be severe, with difficult to treat asthma and highly aggressive and recurrent ethmoidal polyposis. Recently, monoclonal antibodies aimed at reducing type 2 inflammation have demonstrated very promising results on disease control. The goal of this review is to provide the most recent published advances and evidence on physiopathology, diagnostic protocols and therapeutic strategies of N-ERD.
1 Introduction
Aspirin hypersensitivity reactions were first reported in medical literature more than a century ago (1), but it was not until 1922 that the classical triad of asthma, chronic rhinosinusitis with nasal polyposis (CRSwNP) and aspirin intolerance was first described by Widal et al. (2). More than forty years later, in 1968, Samter and Beer fully described the clinical syndrome characterized by CRSwNP, asthma and hypersensitivity to aspirin and cyclooxygenase-1 (COX-1) inhibitors (2, 3). This syndrome has also been named Aspirin Exacerbated Respiratory Disease (A-ERD), and more recently NSAID Exacerbated Respiratory Disease (N-ERD).
N-ERD physiopathology remains somewhat occult, an idiopathic dysfunction of arachidonic acid metabolism causes an imbalance in the synthesis of eicosanoids and prostaglandins (PG) that finally results in a non-allergic hypersensitivity reaction (4).
The objective of this review is to summarize the most recent scientific evidence on the physiopathology, natural history, diagnosis, and therapeutic options of N-ERD.
2 Epidemiology
Worldwide, there is very limited epidemiologic information, studies from the United States report that around 1.4 million people in that country suffer from N-ERD, a 1.9% in a European multicenter study, 1.2% in Finland and 1.3% in Sweden, and a limited number of studies population-based in Poland, Australia (5). Some of the reasons that could explain the absence of this type of studies are that the relationships between dyspnea, asthma and rhinitis induced by NSAIDs in N-ERD and the sub phenotypes of N-ERD are incomplete, in addition to the lack of knowledge of the presentation of symptoms, for example, patients with asthma and aspirin intolerance who do not present with sinonasal polyposis, during medical evaluation, the possibility of N-ERD is often ruled out without proper follow-up. The impact on public health lies in sub-optical medical and surgical treatments, substantially increasing spending on the care of these patients.
The disease affects around 9.7% of patients with CRSwNP, 7.2% of patients with asthma and 14.9% of patients with severe asthma (6).
Clinical manifestations tend to appear between the third and fourth decade of life, with a moderate predominance for the female gender.
One metanalysis published in 2015 concludes that N-ERD is diagnosed in 5.5% to 12.4% of asthmatic patients, but this prevalence increases to 21% when aspirin provocation tests are performed. This would indicate that, globally, N-ERD can affect up to one in five of all asthmatic patients (7).
Reported risk factors for the disease include positive family history of N-ERD, diagnosis of CRSwNP and/or asthma, and, according to some authors, the existence of an atopic status (8).
3 Physiopathology
In the pathogenesis of N-ERD, it has been proposed that several environmental factors, such as viruses and allergens impact on the respiratory epithelium, inducing local release of alarmins, IL-33, IL-25 and Thymic Stromal Lymphopoietin (TSLP), that will direct T-helper cell differentiation towards a TH2 response (9, 10). Under alarmin stimulation, both type 2 innate lymphoid cells (ILC2) and mast cells amplify this TH2 response (11, 12). Particularly in N-ERD patients, PGD2 released by mast cells, combines with IL-33 in a synergistic mechanism that will further increase PGD2 concentrations. Indeed, higher expression of IL-33 and TSLP has been found in nasal polyps of patients with N-ERD than in aspirin tolerant patients (13–15).
One of the main biologic characteristics of N-ERD is an imbalance of arachidonic acid metabolism, with a preponderance of 5 Lipoxygenase (5 LOX) pathway and an overall reduced activity of cyclooxygenase 1 (COX-1) (Figure 1). Further reduction of COX-1 is triggered by NSAID or aspirin intake, and arachidonic acid is then predominantly metabolized through 5-LOX, obtaining 5-Hydroperoxyeicosatetraenoic acid (5HPETE) and Leukotriene A4 (LTA4). There also exists a paradoxical synthesis of prostaglandin D2 (PGD2) because of mast cell and eosinophil activation through thromboxane receptors. Activated PGD2 receptors further stimulate TH2 cells recruitment (16, 17).
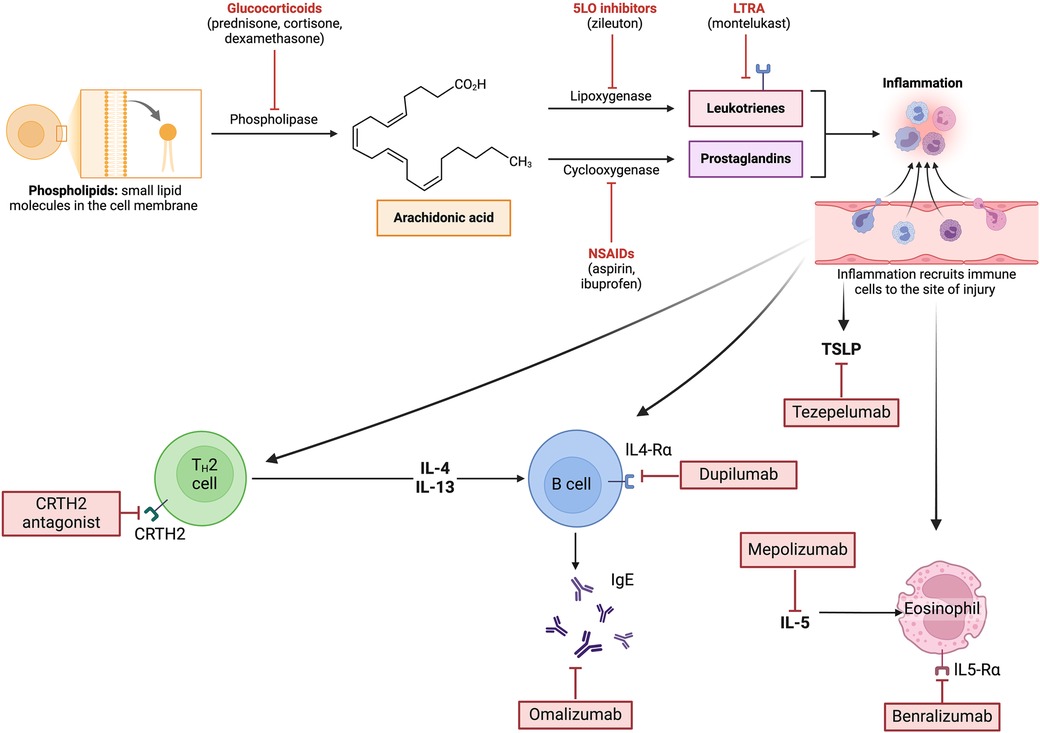
Figure 1. Some common medications and their role in arachidonic acid metabolism. In N-ERD, there is a preponderance of 5-LOX pathway and reduced activity of COX-1 with an overproduction of proinflammatory eicosanoids. Created with BioRender.com.
Leukotriene C4 synthase is significantly overexpressed in eosinophils and mast cells within respiratory tissue of N-ERD patients. Also, cysteinyl-Leukotriene concentrations are four times higher in this group of patients, when compared to aspirin-tolerant asthmatic patients (18, 19).
Thus, a hallmark of N-ERD physiopathology is a complex dysregulation of arachidonic acid metabolic pathways, with an overproduction of proinflammatory eicosanoids (LTC4, cysteinyl-leukotrienes and PGD2) and a deficient release and expression of anti-inflammatory mediators such as cyclooxygenase-2, PGE2, PGE2-receptor and lipoxins (20).
Chronic eosinophilic inflammation is also a paramount feature of N-ERD, with an overexpression of T2 cytokines; IL-4, IL-5, IL-13 GM-CSF, RANTES and eotaxin. Increased concentrations of IL-5 directly enhance eosinophil survival. N-ERD is also associated with increased production of IL-6, IL-13, MCP-3, CCL7, CCL5, TLR 9, and overexpression of endothelial adhesion molecules such as VCAM1, ICAM1 and E-Selectin through the inhibition of NF-KB and IKB. Some potential triggers of this inflammatory profile have been identified in N-ERD patients, were chronic viral infections and TLR3 alterations are mentioned (21–23).
There is recent evidence that patients with N-ERD present a heterogeneous set of dysregulated inflammatory cytokines, both type 2, innate lymphoid cells and IL-6 related cytokines which are elevated in the respiratory tract, oncostatin M and IL-6 overproduction are produced locally in nasal polyps and probably cause epithelial barrier disruption. Blockade of IL-4Ra, although apparently targeting T2 inflammation, also decreases innate inflammatory mediators and epithelial dysregulation (24).
Studies report a higher gene expression of GATA3, IL-4, IL-5, IL17 in patients with N-ERD, which indicates a more severe form of inflammation. The gene expression of IL-17 in the N-ERD group may suggest the coexistence of TH3 and TH2 inflammation with a predominance of Th2 inflammation (25) (Table 1).
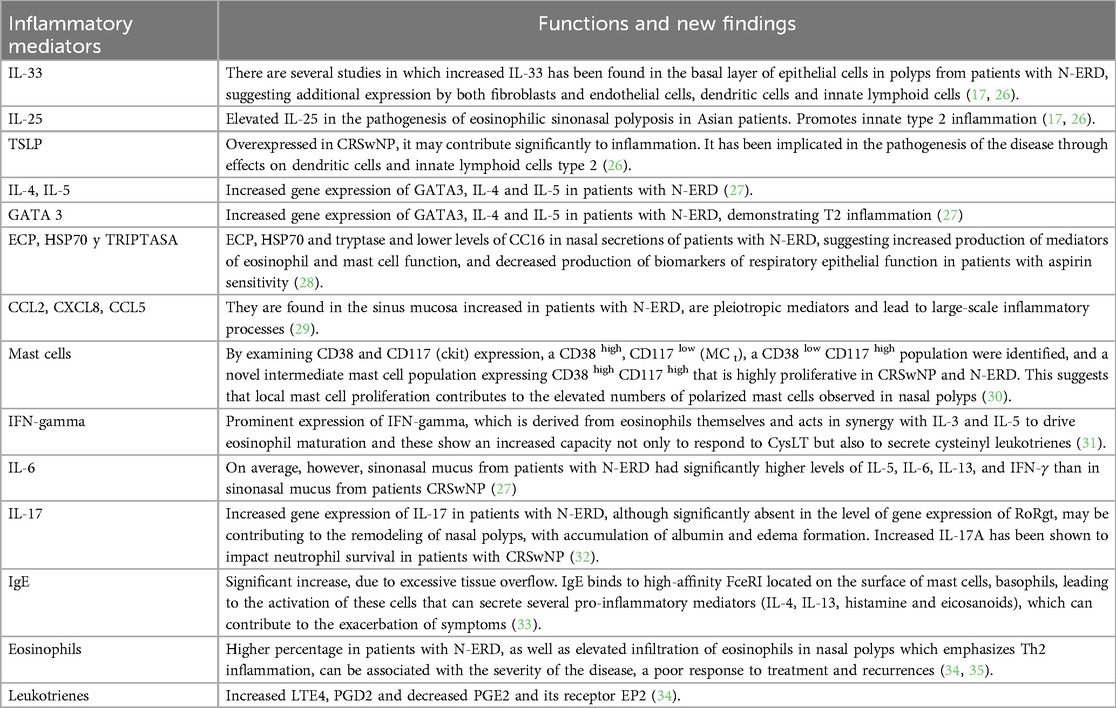
Table 1. The role of main inflammatory mediators involved in N-ERD.
Another important inflammatory factor of CRSwNP in N-ERD, is the presence of tissular Staphylococcus aureus in around 87% of patients. This microorganism produces Staphylococcus aureus enterotoxin (SAE) that acts as a superantigen, triggering local allergic reactions within the ethmoid. High concentrations of specific IgE against SAE have been identified within nasal polyp tissue. These can activate TH2 cells and enhance the release of T2 cytokines and induce a strong eosinophilic response that plays an important role in the severity of both nasal polyposis and bronchial asthma (36–41) (Figure 2).
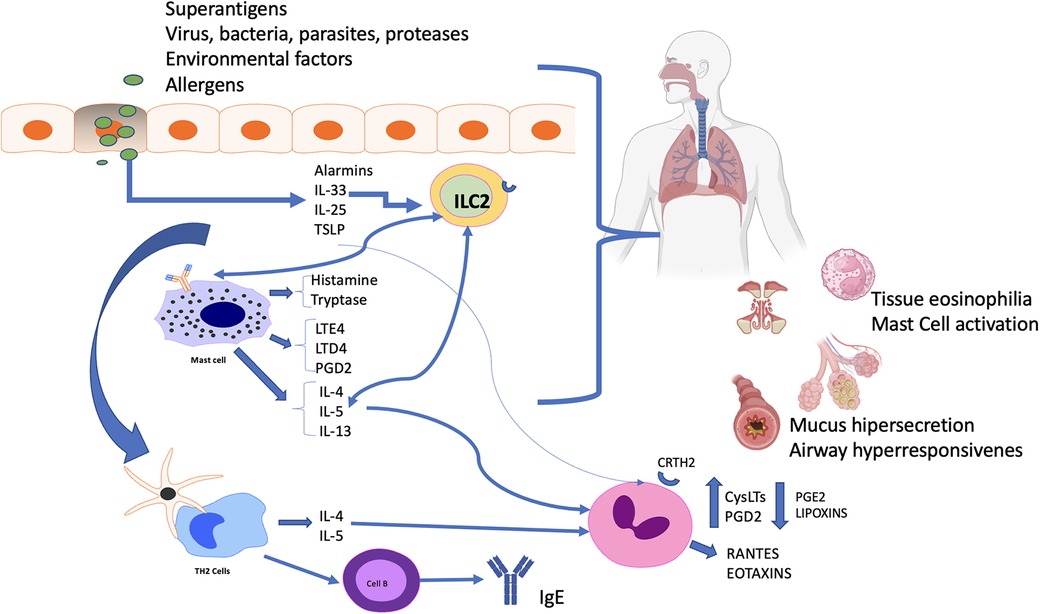
Figure 2. Summary of physiopathology. Allergens, superantigens, viral infection, and environmental factors are all capable of initiating epithelial injury and release of alarmins, interleukin-33, thymic stromal lymphopoietin (TSLP), and interleukin-25. These upstream cytokines have multiple effects focusing on type 2 inflammatory responses. Type 2 innate lymphoid cells (ILC2) and mast cells in N-ERD both amplify the responses, leading to eosinophilia. The combination of inflammatory mediators and cytokines, including IL-4, IL-13, and IL-31, directly affects epithelial cells, stimulating mucus overproduction, edema, and bronchoconstriction. cysLTs, Cysteinyl leukotrienes; ILC2, group 2 innate lymphoid cell; TSLP, Thymic Stromal Lymphopoietin; PGD2, prostaglandin D2; PGE2, Prostaglandin E2; LTE4, Leukotriene E4; LTD4, Leukotriene D4, CRTH2; Prostaglandin D2 receptor 2.
In a study made by Steinke et al, was the elevated expression of IFN-γ in N-ERD, consistent with recognition that this cytokine can be expressed by eosinophils. IFN-γ can block IgE class and it is possible that this co-expression of IFN-γ might contribute to the absence of allergy. Eosinophil-derived IFN-γ synergizes with IL-3 and IL-5 to drive maturation of eosinophils and these eosinophils display an upregulated capacity to not only respond to CysLTs but also to secrete cysteinyl leukotrienes (31).
4 Environmental and genetic factors
Among environmental pollutants, tobacco smoke is well recognized as one of them. In a case-control study conducted by Chang et al, a significant association (OR, 3.46; 95% CI, 2.22–5.39) was found between childhood environmental tobacco smoke (ETS) exposure and N-ERD. If a patient was exposed to ETS during both childhood and adulthood, results showed an OR of 5.09 for developing N-ERD (95% CI, 2.75–9.43) (42). Cigarette smoke stimulates COX-2 expression in airway epithelia, the development of N-ERD would be suppressed by elevated PGE 2 levels in smokers, and smoking cessation might increase susceptibility to N-ERD. The results of a case-control study by Hayashi et al. in 2018 demonstrate that N-ERD was positively associated with smoking cessation between 1 and 4 years before disease onset (43). Tobacco smoke, secondhand smoke and occupational exposure led to increased odds for the development of N-ERD (5).
An identification of polymorphisms in LT-related genes in affected patients suggested a role for genetic variation in the development of N-ERD, this have been implicated in genes encoding enzymes synthesizing eicosanoids from arachidonic acid, related to antigen presentation and inflammation, encoding receptors for cysteinyl leukotrienes and encoding receptors that affect airway sensitivity, mucous production, lung function (44).
Epigenetics is the study of reversible molecular mechanisms that modify gene activity and expression without altering the DNA base-pair nucleotide structure, these changes are a consequence of the impact of the host environment. The influence of epigenetic changes in promoters has been shown to dramatically alter gene expression, which results in reduction in expression of PGE2 receptor 2, PGE 2 resistance, and enhanced eosinophil infiltration into respiratory tissue (45). Characteristic methylation patterns affecting 337 genes have been demonstrated, a recent study showed that there was overexpression of miR-125b in patients with eosinophilic polyposis, which plays an important role as a regulator of innate immunity through miR-125b-EIF4E binding protein 1 in the IFN pathway for mucosal eosinophilia in these patients (46).
In healthy subjects, the normal sinonasal mucosa acts as an immune mechanical barrier against pathogens. Viruses like rhinovirus and coronavirus (the most implicated in CRS) may alter host gene expression, additionally, may lead to alteration of the normal sinonasal microbiome, increased susceptibility to bacterial adherence and inhibit ciliary function leading to altered patterns of immune response and pathogenic changes in levels of cytokines/chemokines which could lead to a cascade of events causing inflammation of the upper airway (47).
5 Clinical presentation
N-ERD clinical symptoms usually start in the upper airway, with rhinorrhea, nasal obstruction, post-nasal drip, and smell impairment. Asthma symptoms tend to appear around two years later, usually, sinonasal polyposis is diagnosed last and around 15% of N-ERD patients present with no previous reactions to NSAIDs or aspirin and will need a provocation test to confirm the diagnosis. Hypersensitivity reactions to NSAIDs tend to appear around four years after the first upper airway symptoms (48); these include sudden nasal obstruction, watery rhinorrhea, cough, wheezing, respiratory distress and even fatal or near fatal asthmatic reactions (49).
One prospective cohort study reported by Dages et al. classified 240 patients in four groups according to the first symptom of presentation. The first group included 119 patients (50% of all patients) who presented with asthma as the first clinical manifestation. 72% of these were women, were significantly younger than patients from other groups (25 years, SE 1.3, P < .001) and presented with higher body mass indexes BMI [OR = 1.3 [95% confidence interval (CI): 1.06–1.7, P = .02]. The second group included 70 patients (29%) who presented with sinonasal polyposis as a first clinical manifestation. Of these, 70% were female and they tended to present NSAIDs intolerance at a later age (OR = 1.03, 95% CI: 1.01–1.06, P = .009). The third group included 39 patients (16%) who presented a NSAID-intolerance reaction as a first clinical manifestation. In this group male predominance was significant (OR = 3.3, 95% CI: 1.5–7.4, P = .004), and there was also significantly higher exposure to air pollution (OR = 4.4, 95% CI: 1.6–11.9, P = .003). The fourth group included 12 patients (5%) who presented the full triad since the beginning of the disease. 83% of these patients were female (50). This study suggests that the differences in initial clinical manifestations of N-ERD could be associated with several patient-specific risk factors that need to be studied to better categorize patient profile and enhance disease control.
A review manuscript published by Kowalski concludes that N-ERD can have very heterogeneous clinical presentations (sub-phenotypes) and possible variations in pathophysiologic mechanisms (sub-endotypes) (49). Studies from Poland and South Korea describe several clinical sub-phenotypes in terms of asthma control and severity, extension and severity of sinonasal affection, presence or absence of atopic status and of chronic urticaria. Significant differences in serum IgE, blood eosinophil count and urinary cysteinyl-leukotrienes were found between these different sub-phenotypes, thus suggesting the existence of real sub-genotypes of the disease. Understanding the clinical diversity of the disease and of its pathophysiological processes could help us better define the existing sub-phenotypes and sub-genotypes, and thus allow us to personalize treatments and improve therapeutic outcomes (49, 51).
6 Diagnosis and prognosis
The first step in establishing N-ERD diagnosis is an exhaustive clinical history, followed by a comprehensive physical exploration, nasal endoscopy and complementary studies such as pulmonary function testing and aspirin provocation tests.
A positive history of multiple hypersensitivity reactions, classically occurring within the first one or two hours after NSAIDs or aspirin intake, manifesting with respiratory symptoms in an adult asthmatic patient who also suffers from CRSwNP is the classical criterion for N-ERD diagnosis. Nevertheless, relying solely on these positive findings in clinical history can lead to underdiagnosis of the disease, as clinical features are not always so straightforward. Not unfrequently, an aspirin provocation test (either oral, intranasal or bronchial) is needed to confirm the diagnosis, also, one study showed that 16% of patients who reported aspirin intolerance presented negative oral provocation tests (52). Thus, an aspirin provocation test can be considered the gold standard in the diagnosis of N-ERD, as it allows to confirm or exclude ASA-hypersensitivity in patients who present with unclear history.
There are four types of aspirin provocation test: oral, intranasal, bronchial or intravenous (1).
Oral challenge is most frequently employed, as it mimics the classic exposure to medication, however, it is very time-consuming, and potential systemic reactions can prove very severe. The most positive oral provocation tests (90%–98%) include naso-ocular reaction, and 35%–90% of cases bronchial reaction, gastrointestinal, cutaneous, and laryngeal symptoms appear in 23%, 10%, and 8% of cases, respectively (35). EAACI group recommends oral challenge, starting with an initial dose of 20–40 mg of aspirin, then increasing the dose every two hours, if no reaction is seen three hours after delivering 325 mg of aspirin, the test is considered negative (7). To be considered as candidates for an oral aspirin provocation test, patients must present with a stable clinical condition and with a minimal FEV1 of 70% of the predicted value. Lower FEV1 values are a contraindication for the test (7).
Bronchial testing is also considered to be safe and fast, and a major disadvantage is that a negative result must be followed by an oral challenge test to obtain definitive diagnosis. The contraindications are basically those of spirometry itself. Oral provocation testing has been compared with bronchial provocation testing in 3 studies, both methods have the same specificity (93%), although oral provocation is more sensitive (89% vs. 77%) (53–55).
Intranasal provocation testing with lysine-aspirin is mostly recommended in patients with predominant sinonasal symptoms and is also considered a sound alternative in patients with any contraindication for oral or bronchial testing. Intranasal challenge is very safe and allows to identify a subgroup of patients who present sole intranasal reactions, but it also tends to be less sensitive than oral or bronchial challenges (7). A main limitation of this diagnostic method results from its low sensitivity, therefore, a history that is suggestive of N-ERD and a negative result in a nasal provocation still require confirmatory oral provocation. This aspirin provocation test is contraindicated in massive nasal polyposis, perforated septum, autoimmune diseases, immunodeficiency and concomitant respiratory infection (56).
Intravenous provocation testing is used exclusively in Japan, for the risk of severe adverse reaction, the IV aspirin provocation test has not been used often in clinical practice, and the safety and efficacy of this convenient method has not been assessed (57).
Characterization of the inflammatory endotype of CRSwNP is also important in N-ERD patients. The biomarkers can be obtained from peripheral blood, nasal secretions, nasal polyp tissue and even exhaled air. Peripheral blood biomarkers are easier to obtain, requiring less experience, cost and time than a nasal biopsy. However, peripheral blood biomarkers often have a poor correlation with the local sinonasal inflammatory phenomena that characterize CRSwNP (58).
Classically, CRSwNP presents as an eosinophilic disease, while CRSsNP tends to be non-eosinophilic. Classification of a rich eosinophilic milieu is established histologically through tissue microscopy. According to Kountakis et al. (59), a polyp is considered eosinophilic when 5 or more eosinophils per high-power field are found, whereas for Solear et al, a minimum of 10 eosinophils per high-power field are required (60).
Several studies have demonstrated that patients with eosinophilic CRSwNP present with higher recurrence rates, worse symptomatic and radiologic scores and higher prevalence of asthma (61, 62). Other studies correlate tissue eosinophilia and concentrations of eosinophilic cationic protein (ECP) with the severity of the disease (63).
In N-ERD, asthma is generally severe and has a T2 eosinophilic inflammatory profile and some patients present with persistent bronchospasm, rapid decrease in lung function and severe inflammation of the whole lower airway. A better understanding of the bronchial epithelial damage in N-ERD is needed to better preserve lung function on the long term (64).
Nowadays, there is no available in vitro test for the diagnosis of N-ERD. Urinary Leukotriene E4 (uLTE4) remains the most reliable biomarker, with higher concentrations found in N-ERD patients when compared to controls. Also, levels of uLTE4 rise significantly after aspirin or NSAIDs intake, nevertheless, this biomarker should not replace an aspirin provocation test and is not recommended for the routine diagnosis of N-ERD (29).
Imaging studies are required only when surgical treatment of CRSwNP is considered. One study demonstrated more severe ethmoidal and frontal sinuses involvement, and less maxillary sinus affection in patients with N-ERD when compared to aspirin tolerant patients with CRSwNP (65).
7 Treatment
There are several therapeutic options when treating N-ERD. Corticosteroids, either inhaled, intranasal or systemic, remain the cornerstone for the initial treatment; endoscopic sinus surgery is widely used in the management of CRSwNP; Aspirin desensitization remains an alternative for selected cases, and recently, monoclonal antibodies have demonstrated an important efficacy.
7.1 Treatment of chronic rhinosinusitis
7.1.1 Medical treatment
Intranasal corticosteroids remain the gold standard of treatment of CRSwNP, and their use is linked with a decrease in inflammatory cells and proteins within the sinonasal mucosa, significantly reducing nasal symptoms such as obstruction, congestion, rhinorrhea, postnasal discharge and hyposmia. In a double blinded randomized controlled trial in N-ERD patients, Mastalerz et al. demonstrated that after a single week of intranasal fluticasone use, nasal peak inspiratory flow improved and there was a significant reduction of nasal symptomatic scores when compared to placebo (66).
The International Consensus Statement on Allergy and Rhinology recommends that nasal lavages or irrigations should be used as a first adjuvant therapeutic option for improving symptoms of CRS (66). Budesonide or other corticosteroids have been added (off label) to isotonic saline solution irrigations resulting in clinical benefit, Steinke et al., in a pilot study in subjects with eosinophilic CRS who had not responded to conventional medical therapy, were treated with budesonide nasal lavage for ≥3 months and seem to improve both olfactory function and polyp size on endoscopy and CT scan (67). However, it should be noted that this common practice is not approved by the FDA and reported results are difficult to compare because of the heterogeneity within the studies in terms of irrigation technique, type of corticosteroid, volume and dilution of the solution, rendering a metanalysis almost impossible to perform (68).
In N-ERD patients, CRSwNP and asthma tend to be quite aggressive. Systemic corticosteroids, mostly taken orally and in short courses, rapidly improve symptoms in both the upper and lower airway, but are accompanied by a wide array of endocrine, muscular, skeletal and ocular adverse effects that should limit their use as much as possible (1).
Antileukotrienes cause an important decrease in the effect and production of Cys-LTs (69). Montelukast, a direct antagonist of cys-LT1 receptor, is the most widely used agent and has been shown to improve asthma symptoms, peak expiratory flow and FEV-1 in patients with N-ERD (1). Zileuton inhibits 5-lipooxygenase, downregulating further release of Cys-LTs. Antileukotrienes help in reducing the severity and frequency of asthmatic reactions and are useful in the control of lower airway symptoms during a provocation test, nevertheless, their use during an intranasal L-aspirin provocation test can lead to false negative results (70).
7.1.2 Surgical treatment
As previously stated, N-ERD patients tend to present with severe and diffuse forms of sinonasal polyposis that are frequently unresponsive to medical treatment and present with high recurrence rates thus requiring surgical treatment. Endoscopic sinus surgery (ESS) with maximal mucosa preservation aims to restore drainage and ventilation of the sinonasal cavities, while creating a common cavity that allows an optimal penetration of topical intranasal corticosteroids, thus enhancing inflammation control at the epithelial level (1) (Figure 3).
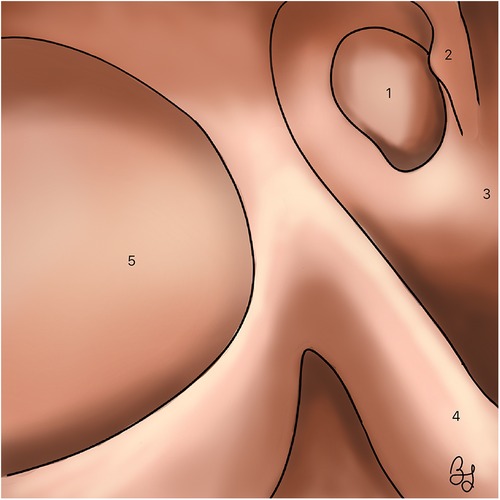
Figure 3. Right nasal cavity. A wide maxillary antrostomy and a sphenoidotomy are illustrated, obtaining a common cavity. (1) Sphenoid sinus. (2) Superior turbinate. (3) Septum. (4) Middle turbinate. (5) Maxillary sinus.
There is still a lot of controversy on the recommended extent of surgery for CRSwNP in N-ERD. Some authors are in favor of a “Full house ESS”, consisting of an elective complete spheno-ethmoidectomy with comprehensive dissection of the frontal recess cells (Draf II A), instead of just addressing the affected sinus cavities (71). However, one study showed that even with this “full house” technique, polyp recurrence rate is of about 58% and the need of revision surgery varies between 2 and 26.2% (72). Indeed, there is a subgroup of patients that present with highly aggressive and recurrent disease that will systematically fail to any mucosal sparing surgical treatment. Therefore, more extended and radical surgical treatments, such as nasalization, Draf III extended frontal surgery and “reboot” surgery have been proposed (73).
Nasalization consists of a radical ethmoidectomy with the systematic resection of all ethmoidal bony partitions and mucosa, followed by a comprehensive frontal recess dissection, a wide maxillary and sphenoid sinusotomy and middle turbinate resection (1) (Figure 4). In a prospective study on patients with diffuse sinonasal polyposis, Jankowski et al. demonstrated that nasalization had a significantly lower recurrence rate (22.7%) than classical ESS (58.3%) (74).

Figure 4. Sagittal section illustrating the classical nasalization technique. (1) Ethmoid bulla. (2) Basal lamella of the middle turbinate. (3) Superior turbinate. (4) Sphenoid sinus. (5) Maxillary sinus (6) Uncinate process. (7) Agger nasi. (8) Frontal recess. (9) Frontal Nasal Beak. (10) Inferior turbinate.
However, classic nasalization technique can lead to late complications such as mucoceles, nasofrontal tract stenosis or ethmoidal cavity collapse. Jiménez-Chobillon et al. proposed some modifications of the technique; the preservation of the middle turbinate and its suture fixation to the nasal septum, obtaining similar functional results with a lower complication rate (75). “Reboot” surgery was proposed by Alsharif et al. for extremely severe and recurrent polypoid disease. In this “rescue” technique, the mucosa of all the sinus cavities is eradicated as much as possible. This technique has shown further decrease of the recurrence rate at 30 months after surgery when compared with mucosal sparing techniques (76).
In a recent pilot study, Moreno-Luna et al. proposed the use of a free mucosal, harvested from the floor of the nasal fossa and adhered to the roof of the ethmoidal cavity after the full resection of the mucosa. This free mucosal flap seems to improve healing, nasal function and recurrence rates (77, 78).
Diffuse polyposis and aspirin sensitivity are both independent risk factors for failure of frontal sinus surgery (79) (Figure 5). Bassiouni et al. demonstrated in a prospective study on N-ERD patients with severe polyposis that Draf III surgery (bilateral extended frontal sinusotomy with superior septectomy) was superior to Draf IIa in terms of recurrence rate (11 Vs. 55%) (80). Naidoo et al. also demonstrated that addressing frontal sinus polypoid disease with a Draf III technique enhanced the penetration of topical steroid irrigations, favoring local inflammation control and sinus ventilation (81). Noller et al. propose that Draf III surgery should be the preferred technique in cases of severe and diffuse sinonasal polyposis such as in N-ERD patients and other diseases like cystic fibrosis and primary mucociliary dyskinesia (82).

Figure 5. Frontal sinus surgery. (1) Draft I: anterior ethmoidectomy (2) Draft IIa: Opening of frontal sinus between lamina papyracea and middle turbinate (3) Draft IIb: Opening of frontal sinus between lamina papyracea and nasal septum (4) Draft III: removal of the frontal sinus floor and septectomy.
7.2 Aspirin desensitization
Desensitization to aspirin is another therapeutic strategy that has been used in N-ERD patients to develop drug tolerance under strict medical supervision. It has been shown to reduce polyp recurrence after ESS, increase time interval between surgeries, reduce the need for systemic corticosteroids, and improve sense of smell and quality of life (83). Several protocols have been described, with varying aspirin amounts, delivery methods, times of intake and increasing doses. Classically, desensitization is attained when a final maximal dose of 325 mg of aspirin is reached.
In a retrospective study on 32 N-ERD patients who underwent ESS and subsequent aspirin desensitization, significant improvement in SNOT-22 scores were noted and only 3 patients (9.4%) required revision surgery after 30 months of follow-up (84).
In a prospective study, Sharan et al. found that ESS could improve the effectiveness of aspirin desensitization in N-ERD, even in patients who previously failed this kind of therapy. This study suggests that ESS can bring patients to a phenotype that is more receptive to desensitization, mostly when preoperative elevated serum levels of IgE are present (85).
Despite its efficacy, treatment withdrawal rate is high because of the frequent adverse effects such as gastrointestinal disorders, bleeding and respiratory symptoms.
7.3 Biotherapy
Monoclonal antibodies that target type 2 inflammatory cytokines such as IL-4, IL-5 and IL-13 have gained popularity in the treatment of complex respiratory diseases. The European Position paper on Rhinosinusitis and Nasal Polyps (EPOS), in collaboration with the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) have proposed guidelines for the proper indications and use of biologics in the treatment of CRSwNP (86) (Figure 6).
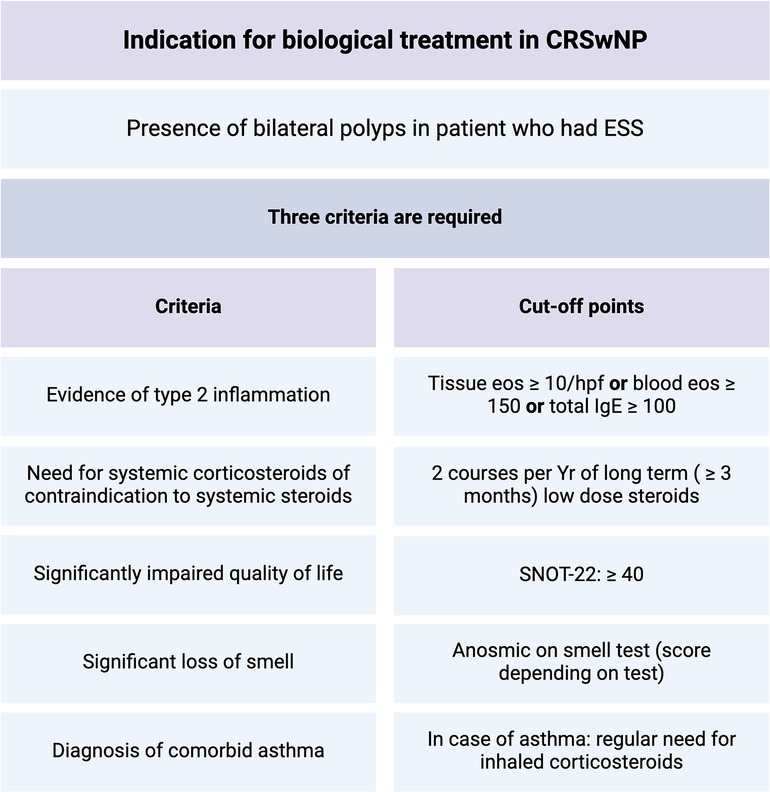
Figure 6. Indications for biologic agents use in CRSwNP, adapted from EPOS/EUFOREA, 2023.
7.3.1 Anti-IgE
Omalizumab is a monoclonal antibody that selectively binds to free circulating IgE and reduces the expression of IgE receptors in mast cells, basophils and dendritic cells, thus interfering with their activation. Its efficacy has been demonstrated in patients with severe asthma and other allergic diseases. In N-ERD several eosinophilic inflammatory mechanisms may be involved, thus, clinical effects of omalizumab can be quite heterogenous when compared with other forms of severe eosinophilic asthma. In a prospective cohort study, Hiyashi et al. reported a reduction of urinary LTE4 (76.2%; P < 0.001) and of PGD2M (89.0%; P = 0.002) after omalizumab use (87). Clinical parameters such as the number of asthmatic exacerbations, emergency department visits, systemic corticosteroids use and sinonasal and asthma symptoms scores also improved (88).
In POLYP 1 and POLYP 2 studies, omalizumab was compared to placebo in 265 patients with CRSwNP (57% with aspirin-tolerant asthma, 27% with N-ERD). 67% of patients had previous ESS. Patients who were treated with omalizumab presented a significant improvement in SNOT-22, Nasal Polyp Score and Asthma Quality of Life Questionnaire (AQLQ) (89). In a recent retrospective study by Förster-Ruhrmann et al, patients with N-ERD (confirmed by aspirin provocation test) who were treated with omalizumab presented significant clinical improvement in VAS, endoscopic staging, ACT and FEV1 during 9 months of follow up (90).
7.3.2 Anti-IL-5
Nowadays, three commercially available biologics that inhibit IL-5 have been used in N-ERD patients. Mepolizumab and Reslizumab directly target IL-5, thus reducing both the production and survival of eosinophils. Benralizumab is a biologic agent that targets IL-5 receptor 5Rα which is expressed in eosinophils, thus inducing eosinophil destruction (91).
Mepolizumab was first designed to treat severe eosinophilic asthma. However, in a randomized double blinded study by Gevaert et al, patients with CRSwNP were treated monthly with 750 mg of IV Mepolizumab and presented a significant reduction in polyp size. Five out of twenty of these patients presented N-ERD (79). In a similar study on 105 CRSwNP patients with clear indications for sinus surgery, Bachert et al. treated 54 subjects with 750 mg of IV Mepolizumab Vs. 51 placebo controls, every 4 weeks for six months. At week 25, only five patients (10%) who had received mepolizumab still needed surgery Vs. 16 patients (30%) in the placebo group (P = 0.006) (92). However, it should be noticed that neither of these two studies specifically assessed N-ERD patients.
In a retrospective study, Tuttle et al. studied the effects of 100 mg monthly subcutaneous injections of Mepolizumab in N-ERD patients and reported that after three or more injections, there was a significant symptomatic improvement in both the upper and lower airway (93). Indeed, prospective, double blinded clinical trials are needed to support these data on N-ERD patients.
Benralizumab has been widely used in patients with severe eosinophilic asthma, and some studies report improvement of accompanying sinonasal symptoms. However, studies that specifically assess the efficacy of this drug on N-ERD patients are needed (94, 95).
7.3.3 Anti-IL4Rα
Dupilumab is a monoclonal antibody that binds to the alpha subunit of IL-4 receptor which is also shared with IL-13, thus blocking both cytokines that are essential in T2 inflammation. In a study by Laidlaw et al. on N-ERD patients, both olfactory function (UPSIT score) and sinonasal related quality of life (SNOT-22) significantly improved after Dupilumab use (96). In two studies analyzing the cost of treatment for CRSwNP, Scangas et al. and Parasher et al. demonstrated that ESS is still a more cost-effective treatment than Dupilumab (97, 98). Thus, it is important to better define the phenotype and endotype of patients that will really benefit from a biologic treatment.
7.3.4 Anti-TSLP
Tezepelumab is a recently developed monoclonal antibody that binds specifically to TSLP, blocking its action on its heterodimeric receptor. In the phase III study NAVIGATOR, Tezepelumab therapy was able to reduce asthmatic reactions and SNOT-22 score, improve lung function and normalize biomarker levels such as blood eosinophil count, FeNO, serum IgE, IL-5 and IL-13, when compared to placebo (99). In a meta-analysis published in 2023, looking at 10 randomized controlled trials, tezepelumab and dupilumab were associated with greater improvements in exacerbation rates and lung function than benralizumab or mepolizumab in subjects with eosinophilic asthma (100).
Despite the great utility and proven benefits of monoclonal antibodies, they can have serious adverse effects that are worth knowing, which is why Fernandez-del-Campo et al. made an analysis of adverse drug reactions (ADRs) reported in the Database of the Spanish Pharmacovigilance System (101) (Figure 7).
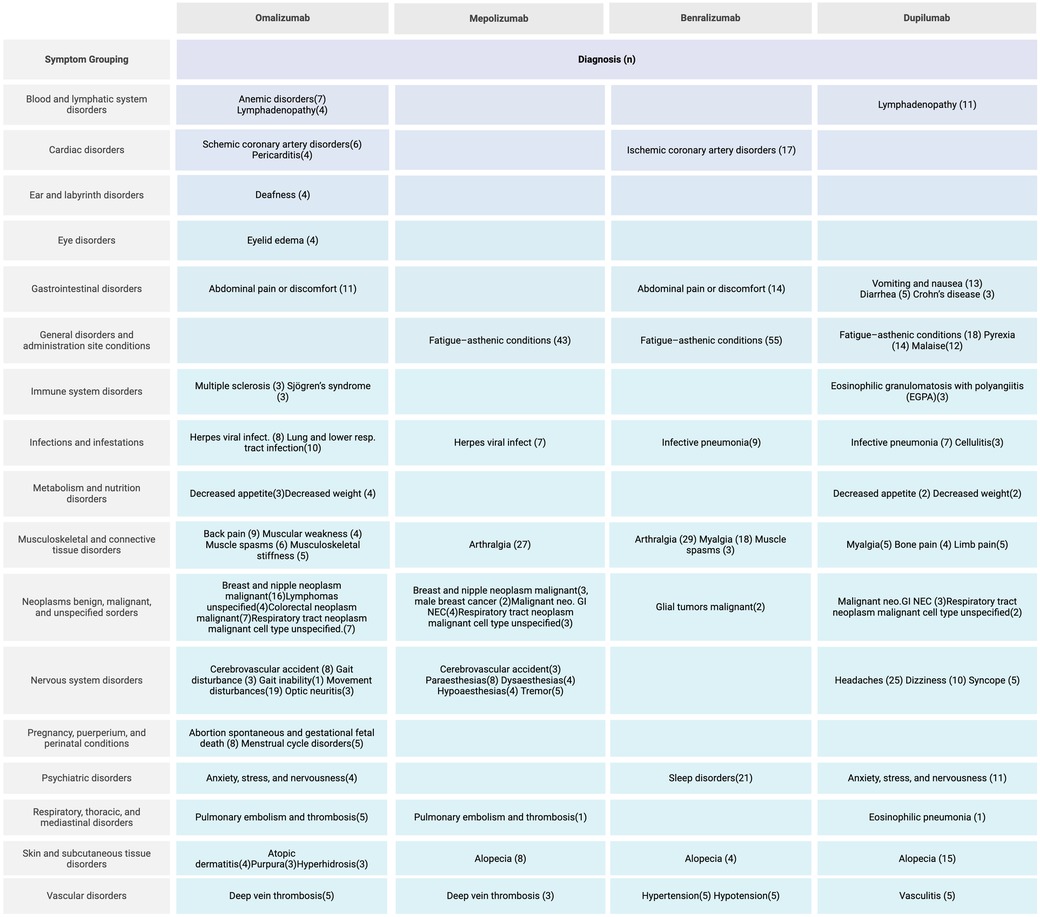
Figure 7. Adverse reactions of biological drug, adapted from Fernandez-del-Campo, et al.
7.3.5 ASA and biotherapies
In a meta-analysis by Oykhman et al. of over 3,400 patients with CRSwNP in 29 randomized trials evaluating 9 treatment options, including ASA-D, both biologics, and ATAD, improved health-related quality of life, sinus symptoms, oral corticosteroid use, and nasal polyp size were demonstrated, with dupilumab and omalizumab demonstrating improvement in most categories evaluated (102).
In those with severe CRSwNP and eosinophilic asthma, systemic therapy is likely to significantly benefit both conditions, but the absolute benefits and cost-effectiveness are less clear. Therefore, treatment should be a decision between patients, healthcare providers, and policy makers for optimal management of CRSwNP considering benefits, costs, and adverse effects.
7.4 Other treatments
7.4.1 Diet
Changes in nutritional habits and lifestyle can have a major impact in several chronic diseases such as diabetes or systemic hypertension. In N-ERD patients, a low salicylate diet enriched with omega-3 supplements could help in reducing the overall inflammatory status.
In a systematic review, Wood et al. were able to establish the average of daily salicylate intake in the diet of Scottish population, making it possible to define what is a high or low salicylate diet (103). However, it is difficult to apply this information to other populations because of the diversity of food and types of food processing in each country. In a multicenter prospective study, Sommer et al. evaluated the effects of a normal vs. a low salicylate diet in N-ERD patients, reporting a significant improvement in SNOT-22, Nasal Sinus Symptom Scale (NSSS) and Asthma Control Questionnaire (ACQ-7) scores in the low-salicylate diet group (104). In a prospective, randomized and two arms study, Sowerby et al. compared a high and low salicylate diet in N-ERD patients and reported that low salicylate diet group had a significant improvement in SNOT-22 scores. However, other measured parameters such as urinary salicylates and LTE4 did not reach statistical significance (105).
Due to the importance of fatty acids in the metabolic pathways of arachidonic acid, Schneider et al. studied the effects of a rich omega-3 (more than 3 g/day) and low omega-6 (less than 4 g/d) diet in N-ERD patients. They found that this diet produced a significant reduction in uLTE4 and SNOT-22 scores. However, no improvement was noted in FEV1 and FVC (106).
Alcohol intolerance has also been reported in N-ERD patients, mostly characterized by respiratory symptoms after intake. In a study on 50 patients, Cardet et al. described a 75% prevalence of alcohol induced upper respiratory symptoms such as rhinorrhea and nasal congestion in N-ERD patients. These symptoms were also present in 33% of aspirin tolerant asthmatic patients, 30% of other chronic rhinosinusitis (CRS) patients and even 14% of healthy controls. When analyzing lower airway symptoms secondary to alcohol intake, wheezing and dyspnea were present in up to 51% of N-ERD patients, and in 20% of aspirin tolerant asthmatic patients. No CRS patient or healthy controls presented lower airway affection after drinking alcohol (107).
Mechanisms of alcohol induced airway symptoms are not fully understood. Candelo et al. describe that phenols such as resveratrol found in beer and red wine can induce COX-1 inhibition, thus leading to the same pharmacologic effects than aspirin or NSAIDs (108). In a prospective cohort study, Glicksman et al. found that aspirin desensitization can improve tolerance to alcohol intake (109). Also, Mustafa et al. describe that 70% of N-ERD patients develop alcohol tolerance after initiating Dupilumab therapy (110).
7.4.2 New treatments
The cellular effector CRTH2 + has been reported to be involved in PGD2 mediated inflammation, in asthma, expression of the prostaglandin D 2 receptor 2 (DP 2 receptor) is increased in the bronchial submucosa and DP 2 receptor stimulation by prostaglandin D 2 mediates the activation and migration of Th2 cells, ILC2, basophils, and eosinophils, and stimulates type 2 cytokine release from these cells, as well as the migration of airway smooth muscle cells (111), the findings implicate the prostaglandin D2—DP 2 axis in the pathogenesis of asthma. On the other side, DP 2 expression is algo associated with CRS, including nasal polyps formation (112), so the pathophysiology of CRSwNP and asthma are similar in terms of the involvement of the DP 2 receptor pathway. A newly designed agents such as feviviprant are targeted against this molecule. In LUSTER-1 and LUSTER-2 studies, feviviprant was compared to placebo in subjects with severe asthma with modest reductions in exacerbations rates were observed in both studies with the 450 mg dose of fevipiprant (113). In THUNDER study this monoclonal antibody was compared to placebo in subjects with CRSwNP and concomitant asthma measured by improvement in nasal polyp score (primary end point), nasal congestion score, SNOT-22, and UPSIT score with no clinical effect and the main limitation of this study were that only 1 patient had a diagnosis of N-ERD (114).
Feviviprant may have a role in the treatment of N-ERD, where it is thought that the role of DP2 receptor pathway be more important supported by the fact that N-ERD subjects have elevated levels of urinary PGD2 metabolites compared to aspirin-tolerant asthma subjects, furthermore, suppression of PGD2 in N-ERD subjects by high-dose aspirin therapy is understood to be one of the mechanisms of benefit of high-dose aspirin therapy in N-ERD (115, 116).
Finally, the inflammatory role of platelets through the activation of thromboxane receptors has been investigated in N-ERD. Ifetroban, a thromboxane receptor antagonist would attenuate the severity of sinonasal, and respiratory symptoms induced during aspirin challenges in patients with N-ERD by blocking platelet activation, reducing cysLT generation, and reducing aspirin-induced bronchoconstriction. A trial conducted in 2024, ifetroban was compared to placebo in subjects with N-ERD where worsening of aspirin-induced reactions was observed with possible ablation of the low-level protective PGE2 effect (117, 118).
7.5 Effectiveness and cost-effectiveness
Worldwide, many health systems, especially public ones, are under high demand and often have limited budgets to provide the necessary services. As already mentioned, there are different treatment modalities for N-ERD, of which monoclonal antibodies are currently the most expensive therapeutic measures, so it is important to assess their cost-effectiveness and efficacy against other forms of treatment to promote the sustainability of health care.
Some cost-effectiveness studies on CRSwNP suggest that FEES, including revision surgery, is more cost-effective than dupilumab, however these analyses do not consider other factors such as the number of prior surgeries, nasal polyp scores, initial SNOT-22 scores, and the proportion of patients with concomitant asthma, so the true cost-benefit of monoclonal antibodies in N-ERD is still unknown (Table 2).
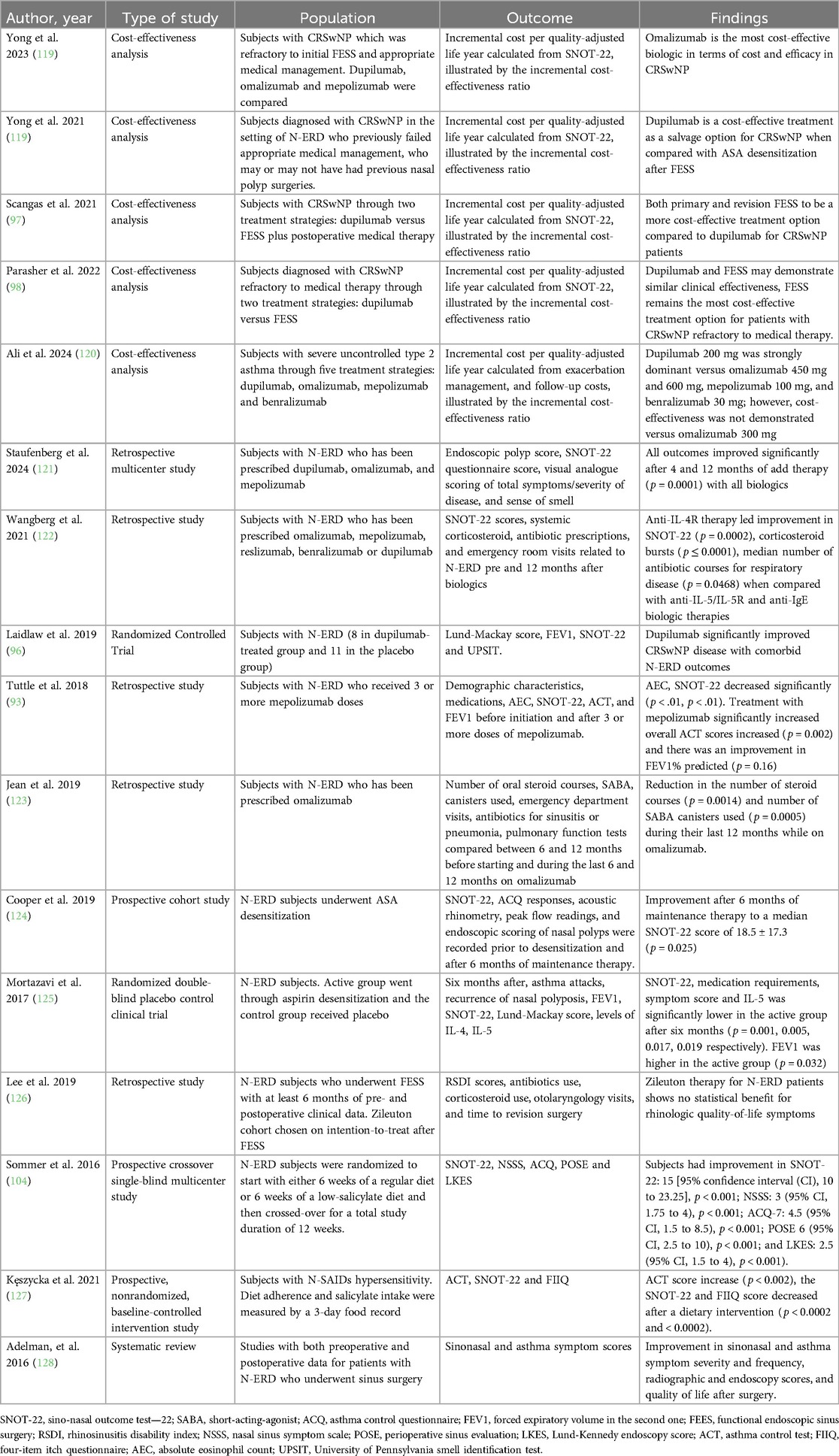
Table 2. Summary of studies on effectiveness and cost-effectiveness of different treatment options.
8 Conclusions
N-ERD is a very complex and heterogenous disease that requires a multidisciplinary approach, involving pneumologists, allergists, ENT-surgeons among other medical specialties to attain optimal results in terms of control and quality of life. When comprehensive medical treatment fails, surgery is indicated, and although conservative surgeries are intended as they present fewer complications, now a days, ethmoidal radical surgical techniques are recommended for the control of CRSwNP in N-ERD.
In recent years, a better understanding of the mechanisms involved in T2 inflammation has allowed the development of several more targeted therapies, such as monoclonal antibodies targeting T2 inflammation cytokines, which offer a new paradigm in treatment and still need to be investigated to obtain their true long-term efficacy. The genetics and epigenetics of N-ERD need to continue to be studied to obtain more personalized and targeted therapies, therefore, more effective in the future.
Author contributions
JL-T: Investigation, Resources, Writing – original draft, Writing – review & editing. AX-T: Resources, Writing – original draft. MG-C: Data curation, Investigation, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. MJ-C: Supervision, Validation, Writing – review & editing, Data curation, Investigation, Project administration, Resources.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors acknowledge Berenice Lazcano-Velasco MD for her valuable support with the anatomical illustration of paranasal sinuses.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Li K, Lee A, Abuzeid W. Aspirin exacerbated respiratory disease: epidemiology, pathophysiology, and management. Med Sci. (2019) 7(3):45. doi: 10.3390/medsci7030045
2. Widal F, Abrami P, Lermoyez J. First complete description of the aspirin idiosyncrasy-asthma-nasal polyposis syndrome (plus urticaria)–1922 (with a note on aspirin desensitization). by F. Widal, P. Abrami, J. Lermoyez. J Asthma Off J Assoc Care Asthma. (1987) 24(5):297–300.
3. Samter M, Beers RF. Intolerance to aspirin. Clinical studies and consideration of its pathogenesis. Ann Intern Med. (1968) 68(5):975–83. doi: 10.7326/0003-4819-68-5-975
4. Kim SD, Cho KS. Samter’s triad: state of the art. Clin Exp Otorhinolaryngol. (2018) 11(2):71–80. doi: 10.21053/ceo.2017.01606
5. Andersén H, Ilmarinen P, Honkamäki J, Tuomisto LE, Hisinger-Mölkänen H, Backman H, et al. NSAID-exacerbated respiratory disease: a population study. ERJ Open Res. (2022) 8(1):00462–2021. doi: 10.1183/23120541.00462-2021
6. Rajan JP, Wineinger NE, Stevenson DD, White AA. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: a meta-analysis of the literature. J Allergy Clin Immunol. (2015) 135(3):676–681.e1. doi: 10.1016/j.jaci.2014.08.020
7. Morales DR, Guthrie B, Lipworth BJ, Jackson C, Donnan PT, Santiago VH. NSAID-exacerbated respiratory disease: a meta-analysis evaluating prevalence, mean provocative dose of aspirin and increased asthma morbidity. Allergy. (2015) 70(7):828–35. doi: 10.1111/all.12629
8. Stevens WW, Peters AT, Hirsch AG, Nordberg CM, Schwartz BS, Mercer DG, et al. Clinical characteristics of patients with chronic rhinosinusitis with nasal polyps, asthma, and aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. (2017) 5(4):1061–1070.e3. doi: 10.1016/j.jaip.2016.12.027
9. Pan D, Buchheit KM, Samuchiwal SK, Liu T, Cirka H, Raff H, et al. COX-1 mediates IL-33-induced extracellular signal-regulated kinase activation in mast cells: implications for aspirin sensitivity. J Allergy Clin Immunol. (2019) 143(3):1047–1057.e8. doi: 10.1016/j.jaci.2018.06.033
10. Lee JU, Chang HS, Lee HJ, Bae DJ, Son JH, Park JS, et al. Association of interleukin-25 levels with development of aspirin induced respiratory diseases. Respir Med. (2017) 123:71–8. doi: 10.1016/j.rmed.2016.11.020
11. Buchheit KM, Cahill KN, Katz HR, Murphy KC, Feng C, Lee-Sarwar K, et al. Thymic stromal lymphopoietin controls prostaglandin D2 generation in patients with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2016) 137(5):1566–1576.e5. doi: 10.1016/j.jaci.2015.10.020
12. Cavagnero K, Doherty TA. Cytokine and lipid mediator regulation of group 2 innate lymphoid cells (ILC2s) in human allergic airway disease. J Cytokine Biol. (2017) 2(2):116. doi: 10.4172/2576-3881.1000116s
13. Nagata Y, Maruoka S, Gon Y, Mizumura K, Kishi H, Nomura Y, et al. Expression of IL-25, IL-33, and thymic stromal lymphopoietin in nasal polyp gland duct epithelium in patients with chronic rhinosinusitis. Am J Rhinol Allergy. (2019) 33(4):378–87. doi: 10.1177/1945892419835333
14. Pelaia C, Pelaia G, Maglio A, Tinello C, Gallelli L, Lombardo N, et al. Pathobiology of type 2 inflammation in asthma and nasal polyposis. J Clin Med. (2023) 12(10):3371. doi: 10.3390/jcm12103371
15. Badrani JH, Cavagnero K, Eastman JJ, Kim AS, Strohm A, Yan C, et al. Lower serum 15-HETE level predicts nasal ILC2 accumulation during COX-1 inhibition in AERD. J Allergy Clin Immunol. (2023) 152(5):1330–1335.e1. doi: 10.1016/j.jaci.2023.06.028
16. Cavagnero KJ, Doherty TA. Lipid-mediated innate lymphoid cell recruitment and activation in aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. (2021) 126(2):135–42. doi: 10.1016/j.anai.2020.09.011
17. Liu T, Kanaoka Y, Barrett NA, Feng C, Garofalo D, Lai J, et al. Aspirin-Exacerbated respiratory disease involves a cysteinyl leukotriene-driven IL-33-mediated mast cell activation pathway. J Immunol Baltim Md 1950. (2015) 195(8):3537–45. doi: 10.4049/jimmunol.1500905
18. Liu T, Barrett NA, Kanaoka Y, Yoshimoto E, Garofalo D, Cirka H, et al. Type 2 cysteinyl leukotriene receptors drive IL-33-dependent type 2 immunopathology and aspirin sensitivity. J Immunol Baltim Md 1950. (2018) 200(3):915–27. doi: 10.4049/jimmunol.1700603
19. Garcia Cruz ML, Jimenez-Chobillon MA, Teran LM. Rhinosinusitis and aspirin-exacerbated respiratory disease. J Allergy. (2012) 2012:273752. doi: 10.1155/2012/273752
20. Badrani JH, Doherty TA. Cellular interactions in aspirin-exacerbated respiratory disease. Curr Opin Allergy Clin Immunol. (2021) 21(1):65–70. doi: 10.1097/ACI.0000000000000712
21. Gervais FG, Cruz RP, Chateauneuf A, Gale S, Sawyer N, Nantel F, et al. Selective modulation of chemokinesis, degranulation, and apoptosis in eosinophils through the PGD2 receptors CRTH2 and DP. J Allergy Clin Immunol. (2001) 108(6):982–8. doi: 10.1067/mai.2001.119919
22. Steinke JW, Payne SC, Borish L. Eosinophils and mast cells in aspirin-exacerbated respiratory disease. Immunol Allergy Clin North Am. (2016) 36(4):719–34. doi: 10.1016/j.iac.2016.06.008
23. Palikhe NS, Kim SH, Kim JH, Losol P, Ye YM, Park HS. Role of toll-like receptor 3 variants in aspirin-exacerbated respiratory disease. Allergy Asthma Immunol Res. (2011) 3(2):123–7. doi: 10.4168/aair.2011.3.2.123
24. Chen CC, Buchheit KM, Lee PY, Brodeur KE, Sohail A, Cho L, et al. IL-4Rα signaling promotes barrier-altering oncostatin M and IL-6 production in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2024) 154(2):458–467.e3. doi: 10.1016/j.jaci.2024.04.020
25. Nazari J, Shahba F, Jafariaghdam N, Mohebbi S, Arshi S, Bemanian MH, et al. Immune endotyping and gene expression profile of patients with chronic rhinosinusitis with nasal polyps in the aspirin-exacerbated respiratory disease (AERD) and the non-AERD subgroups. Allergy Asthma Clin Immunol. (2024) 20(1):14. Published 2024 February 15. doi: 10.1186/s13223-024-00876-w
26. Ogasawara N, Klingler AI, Tan BK, Poposki JA, Hulse KE, Stevens WW, et al. Epithelial activators of type 2 inflammation: elevation of thymic stromal lymphopoietin, but not IL-25 or IL-33, in chronic rhinosinusitis with nasal polyps in Chicago, Illinois. Allergy. (2018) 73(11):2251–4. doi: 10.1111/all.13552
27. Scott WC, Cahill KN, Milne GL, Li P, Sheng Q, Huang LC, et al. Inflammatory heterogeneity in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2021) 147(4):1318–1328.e5. doi: 10.1016/j.jaci.2020.11.001
28. Perić A, Gaćeša D, Cvetković G, Vojvodić D. Inflammatory mediators in nasal secretions of patients with nasal polyposis with and without aspirin sensitivity. Immun Inflamm Dis. (2023) 11(2):e791. doi: 10.1002/iid3.791
29. Chiang S, Yu SE, Athni TS, Bergmark RW, Maxfield AZ, Roditi RE, et al. Not just snot: local inflammatory profiles in patients with aspirin-exacerbated respiratory disease differ from patients with aspirin-tolerant chronic rhinosinusitis. Int Forum Allergy Rhinol. (2024) 14(1):110–3. doi: 10.1002/alr.23216
30. Stevens WW, Cahill KN. Mechanistic and clinical updates in AERD: 2021–2022. J Allergy Clin Immunol. (2023) 151(6):1448–56. doi: 10.1016/j.jaci.2023.03.015
31. Steinke JW, Liu L, Huyett P, Negri J, Payne SC, Borish L. Prominent role of IFN-γ in patients with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2013) 132(4):856–65.e1-3. doi: 10.1016/j.jaci.2013.05.008
32. Derycke L, Zhang N, Holtappels G, Dutré T, Bachert C. IL-17A as a regulator of neutrophil survival in nasal polyp disease of patients with and without cystic fibrosis. J Cyst Fibros. (2012) 11(3):193–200. doi: 10.1016/j.jcf.2011.11.007
33. Kariyawasam HH, James LK. Chronic rhinosinusitis with nasal polyps: targeting IgE with anti-IgE omalizumab therapy. Drug Des Devel Ther. (2020) 14:5483–94. Published 2020 December 10. doi: 10.2147/DDDT.S226575
34. Stevens WW, Ocampo CJ, Berdnikovs S, Sakashita M, Mahdavinia M, Suh L, et al. Cytokines in chronic rhinosinusitis. Role in eosinophilia and aspirin-exacerbated respiratory disease. Am J Respir Crit Care Med. (2015) 192(6):682–94. doi: 10.1164/rccm.201412-2278OC
35. Hao J, Pang YT, Wang DY. Diffuse mucosal inflammation in nasal polyps and adjacent middle turbinate. Otolaryngol Head Neck Surg. (2006) 134(2):267–75. doi: 10.1016/j.otohns.2005.09.026
36. Corriveau MN, Zhang N, Holtappels G, Van Roy N, Bachert C. Detection of Staphylococcus aureus in nasal tissue with peptide nucleic acid-fluorescence in situ hybridization. Am J Rhinol Allergy. (2009) 23(5):461–5. doi: 10.2500/ajra.2009.23.3367
37. Bachert C, Zhang N, Holtappels G, De Lobel L, van Cauwenberge P, Liu S, et al. Presence of IL-5 protein and IgE antibodies to staphylococcal enterotoxins in nasal polyps is associated with comorbid asthma. J Allergy Clin Immunol. (2010) 126(5):962–8, 968.e1-6. doi: 10.1016/j.jaci.2010.07.007
38. Van Zele T, Gevaert P, Watelet JB, Claeys G, Holtappels G, Claeys C, et al. Staphylococcus aureus colonization and IgE antibody formation to enterotoxins is increased in nasal polyposis. J Allergy Clin Immunol. (2004) 114(4):981–3. doi: 10.1016/j.jaci.2004.07.013
39. Muluk NB, Altın F, Cingi C. Role of superantigens in allergic inflammation: their relationship to allergic rhinitis, chronic rhinosinusitis, asthma, and atopic dermatitis. Am J Rhinol Allergy. (2018) 32(6):502–17. doi: 10.1177/1945892418801083
40. Shaghayegh G, Cooksley C, Bouras G, Panchatcharam BS, Feizi S, Javadian S, et al. S. aureus biofilm properties correlate with immune B cell subset frequencies and severity of chronic rhinosinusitis. Clin Immunol Orlando Fla. (2024) 263:110221. doi: 10.1016/j.clim.2024.110221
41. Milovanović J, Božić DD, Pavlović B, Jotić A, Brkić S, Ćirković I. Biofilm-producing Bacteria and quality of life after endoscopic sinus surgery in patients with chronic rhinosinusitis with nasal polyposis. Am J Rhinol Allergy. (2024) 38(3):159–68. doi: 10.1177/19458924241236233
42. Chang JE, Ding D, Martin-Lazaro J, White A, Stevenson DD. Smoking, environmental tobacco smoke, and aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol. (2012) 108(1):14–9. doi: 10.1016/j.anai.2011.09.022
43. Hayashi H, Fukutomi Y, Mitsui C, Nakatani E, Watai K, Kamide Y, et al. Smoking cessation as a possible risk factor for the development of aspirin-exacerbated respiratory disease in smokers. J Allergy Clin Immunol Pract. (2018) 6(1):116–125.e3. doi: 10.1016/j.jaip.2017.04.035
44. Dahlin A, Weiss ST. Genetic and epigenetic components of aspirin-exacerbated respiratory disease. Immunol Allergy Clin North Am. (2016) 36(4):765–89. doi: 10.1016/j.iac.2016.06.010
45. Brar T, Marks L, Lal D. Insights into the epigenetics of chronic rhinosinusitis with and without nasal polyps: a systematic review. Front Allergy. (2023) 4:1165271. doi: 10.3389/falgy.2023.1165271
46. Cheong HS, Park SM, Kim MO, Park JS, Lee JY, Byun JY, et al. Genome-wide methylation profile of nasal polyps: relation to aspirin hypersensitivity in asthmatics. Allergy. (2011) 66(5):637–44. doi: 10.1111/j.1398-9995.2010.02514.x
47. Kumar N, Brar T, Kita H, Marks LA, Miglani A, Marino MJ, et al. Viruses in chronic rhinosinusitis: a systematic review. Front Allergy. (2023) 4:1237068. doi: 10.3389/falgy.2023.1237068
48. Szczeklik A, Nizankowska E, Duplaga M. Natural history of aspirin-induced asthma. AIANE investigators. European network on aspirin-induced asthma. Eur Respir J. (2000) 16(3):432–6. doi: 10.1034/j.1399-3003.2000.016003432.x
49. Kowalski ML, Agache I, Bavbek S, Bakirtas A, Blanca M, Bochenek G, et al. Diagnosis and management of NSAID -exacerbated respiratory disease (N- ERD)—a EAACI position paper. Allergy. (2019) 74(1):28–39. doi: 10.1111/all.13599
50. Dages KN, Sofola-James O, Sehanobish E, Regula P, Chen CC, Chiarella SE, et al. Sex, ethnicity, body mass index, and environmental exposures associated with NSAID-exacerbated respiratory disease symptom sequence. J Allergy Clin Immunol Pract. (2023) 11(12):3662–3669.e2. doi: 10.1016/j.jaip.2023.07.035
51. Kowalski ML. Heterogeneity of NSAID-exacerbated respiratory disease: has the time come for subphenotyping? Curr Opin Pulm Med. (2019) 25(1):64–70. doi: 10.1097/MCP.0000000000000530
52. Dursun AB, Woessner KA, Simon RA, Karasoy D, Stevenson DD. Predicting outcomes of oral aspirin challenges in patients with asthma, nasal polyps, and chronic sinusitis. Ann Allergy Asthma Immunol. (2008) 100(5):420–5. doi: 10.1016/S1081-1206(10)60465-6
53. Nizankowska E, Bestyńska-Krypel A, Cmiel A, Szczeklik A. Oral and bronchial provocation tests with aspirin for diagnosis of aspirin-induced asthma. Eur Respir J. (2000) 15(5):863–9. doi: 10.1034/j.1399-3003.2000.15e09.x
54. Dahlén B, Zetterström O. Comparison of bronchial and per oral provocation with aspirin in aspirin-sensitive asthmatics. Eur Respir J. (1990) 3(5):527–34. doi: 10.1183/09031936.93.03050527
55. Barranco P, Bobolea I, Larco JI, Prior N, López-Serrano MC, Quirce S. Diagnosis of aspirin-induced asthma combining the bronchial and the oral challenge tests: a pilot study. J Investig Allergol Clin Immunol. (2009) 19(6):446–52.20128418
56. Izquierdo-Domínguez A, Bobolea I, Doña I, Campo P, Segura C, Ortega N, et al. Statement of the spanish society of allergology and clinical immunology on provocation tests with aspirin/nonsteroidal anti-inflammatory drugs. J Investig Allergol Clin Immunol. (2020) 30(1):1–13. doi: 10.18176/jiaci.0449
57. Seong GM, Lee J, Kim C. Intravenous aspirin challenge as a diagnosis of nonsteroidal anti-inflammatory drugs hypersensitivity. Asian Pac J Allergy Immunol. (2020) 38(2):124–8. doi: 10.12932/AP-151018-0416
58. Workman AD, Kohanski MA, Cohen NA. Biomarkers in chronic rhinosinusitis with nasal polyps. Immunol Allergy Clin North Am. (2018) 38(4):679–92. doi: 10.1016/j.iac.2018.06.006
59. Kountakis SE, Arango P, Bradley D, Wade ZK, Borish L. Molecular and cellular staging for the severity of chronic rhinosinusitis. Laryngoscope. (2004) 114(11):1895–905. doi: 10.1097/01.mlg.0000147917.43615.c0
60. Soler ZM, Sauer D, Mace J, Smith TL. Impact of mucosal eosinophilia and nasal polyposis on quality-of-life outcomes after sinus surgery. Otolaryngol Head Neck Surg. (2010) 142(1):64–71. doi: 10.1016/j.otohns.2009.10.005
61. Snidvongs K, Lam M, Sacks R, Earls P, Kalish L, Phillips PS, et al. Structured histopathology profiling of chronic rhinosinusitis in routine practice. Int Forum Allergy Rhinol. (2012) 2(5):376–85. doi: 10.1002/alr.21032
62. Soler ZM, Sauer DA, Mace JC, Smith TL. Ethmoid histopathology does not predict olfactory outcomes after endoscopic sinus surgery. Am J Rhinol Allergy. (2010) 24(4):281–5. doi: 10.2500/ajra.2010.24.3477
63. Bachert C, Claeys SE, Tomassen P, van Zele T, Zhang N. Rhinosinusitis and asthma: a link for asthma severity. Curr Allergy Asthma Rep. (2010) 10(3):194–201. doi: 10.1007/s11882-010-0096-0
64. Lee Y, Kim C, Lee E, Lee HY, Woo SD, You SC, et al. Long-term clinical outcomes of aspirin-exacerbated respiratory disease: real-world data from an adult asthma cohort. Clin Exp Allergy. (2023) 53(9):941–50. doi: 10.1111/cea.14362
65. Kim MB, Lim GC, Park JA, Kim YS, Kim JH, Kang JW. Computed tomography findings in patients with samter’s triad: an observational study. Open Med. (2019) 14(1):241–6. doi: 10.1515/med-2019-0018
66. Mastalerz L, Milewski M, Duplaga M, Nizankowska E, Szczeklik A. Intranasal fluticasone propionate for chronic eosinophilic rhinitis in patients with aspirin-induced asthma. Allergy. (1997) 52(9):895–900. doi: 10.1111/j.1398-9995.1997.tb01248.x
67. Orlandi RR, Kingdom TT, Smith TL, Bleier B, DeConde A, Luong AU, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. (2021) 11(3):213–739. doi: 10.1002/alr.22741
68. Steinke JW, Payne SC, Tessier ME, Borish LO, Han JK, Borish LC. Pilot study of budesonide inhalant suspension irrigations for chronic eosinophilic sinusitis. J Allergy Clin Immunol. (2009) 124(6):1352–4.e7. doi: 10.1016/j.jaci.2009.09.018
69. Bernstein JA, White AA, Han JK, Lang DM, Elkayam D, Baroody FM. Review of evidence supporting the use of nasal corticosteroid irrigation for chronic rhinosinusitis. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. (2023) 130(1):46–57. doi: 10.1016/j.anai.2022.09.008
70. Dahlén SE, Malmström K, Nizankowska E, Dahlén B, Kuna P, Kowalski M, et al. Improvement of aspirin-intolerant asthma by montelukast, a leukotriene antagonist: a randomized, double-blind, placebo-controlled trial. Am J Respir Crit Care Med. (2002) 165(1):9–14. doi: 10.1164/ajrccm.165.1.2010080
71. Ceballos Cantu JC, Alobid I, Mullol J. Current evaluation and management of patients with chronic rhinosinusitis and nasal polyps. Expert Rev Clin Immunol. (2022) 18(12):1253–63. doi: 10.1080/1744666X.2022.2128767
72. Conti DM, Correa EJ, Scadding GK. Is endoscopic sinus surgery sufficient to modify the evolution of adult AERD? Aspirin desensitization as a maintenance factor: systematic review. Front Allergy. (2023) 4:1250178. doi: 10.3389/falgy.2023.1250178
73. Eloy JA, Marchiano E, Vázquez A. Extended endoscopic and open Sinus surgery for refractory chronic rhinosinusitis. Otolaryngol Clin North Am. (2017) 50(1):165–82. doi: 10.1016/j.otc.2016.08.013
74. Jankowski R, Pigret D, Decroocq F, Blum A, Gillet P. Comparison of radical (nasalisation) and functional ethmoidectomy in patients with severe sinonasal polyposis. A retrospective study. Rev Laryngol - Otol - Rhinol. (2006) 127(3):131–40.
75. Jiménez-Chobillon MA, Martínez-Castillo FA, Valdés-Hernández E, Cristerna-Sánchez L. Refinement of the nasalisation technique for nasal polyposis. Eur Ann Otorhinolaryngol Head Neck Dis. (2016) 133(4):237–41. doi: 10.1016/j.anorl.2015.08.043
76. Alsharif S, Jonstam K, Van Zele T, Gevaert P, Holtappels G, Bachert C. Endoscopic Sinus surgery for type-2 CRS wNP: an endotype-based retrospective study. Laryngoscope. (2019) 129(6):1286–92. doi: 10.1002/lary.27815
77. Moreno-Luna R, Gonzalez-Garcia J, Maza-Solano JM, Molina-Fernandez E, Pinheiro-Neto CD, Del Cuvillo Bernal A, et al. Free nasal floor mucosal grafting after endoscopic total ethmoidectomy for severe nasal polyposis: a pilot study. Rhinology. (2019) 57(3):219–24. doi: 10.4193/Rhin18.178
78. Moreno-Luna R, Martin-Jimenez DI, Callejon-Leblic MA, Gonzalez-Garcia J, Maza-Solano JM, Porras-Gonzalez C, et al. Usefulness of bilateral mucoplasty plus reboot surgery in severe type-2 chronic rhinosinusitis with nasal polyps. Rhinology. (2022) 60(5):368–76. doi: 10.4193/Rhin22.131
79. Abuzeid WM, Mace JC, Costa ML, Rudmik L, Soler ZM, Kim GS, et al. Outcomes of chronic frontal sinusitis treated with ethmoidectomy: a prospective study. Int Forum Allergy Rhinol. (2016) 6(6):597–604. doi: 10.1002/alr.21726
80. Bassiouni A, Wormald PJ. Role of frontal sinus surgery in nasal polyp recurrence. Laryngoscope. (2013) 123(1):36–41. doi: 10.1002/lary.23610
81. Naidoo Y, Bassiouni A, Keen M, Wormald PJ. Long-term outcomes for the endoscopic modified lothrop/draf III procedure: a 10-year review. Laryngoscope. (2014) 124(1):43–9. doi: 10.1002/lary.24258
82. Noller M, Fischer JL, Gudis DA, Riley CA. The draf III procedure: a review of indications and techniques. World J Otorhinolaryngol - Head Neck Surg. (2022) 8(1):1–7. doi: 10.1002/wjo2.6
83. Buchheit KM, Laidlaw TM. Update on the management of aspirin-exacerbated respiratory disease. Allergy Asthma Immunol Res. (2016) 8(4):298–304. doi: 10.4168/aair.2016.8.4.298
84. Adappa ND, Ranasinghe VJ, Trope M, Brooks SG, Glicksman JT, Parasher AK, et al. Outcomes after complete endoscopic sinus surgery and aspirin desensitization in aspirin-exacerbated respiratory disease. Int Forum Allergy Rhinol. (2018) 8(1):49–53. doi: 10.1002/alr.22036
85. Shah SJ, Abuzeid WM, Ponduri A, Pelletier T, Ren Z, Keskin T, et al. Endoscopic sinus surgery improves aspirin treatment response in aspirin-exacerbated respiratory disease patients. Int Forum Allergy Rhinol. (2019) 9(12):1401–8. doi: 10.1002/alr.22418
86. Fokkens WJ, Viskens AS, Backer V, Conti D, De Corso E, Gevaert P, et al. EPOS/EUFOREA update on indication and evaluation of biologics in chronic rhinosinusitis with nasal polyps 2023. Rhinology. (2023) 61(3):194–202. doi: 10.4193/Rhin22.489
87. Hayashi H, Mitsui C, Nakatani E, Fukutomi Y, Kajiwara K, Watai K, et al. Omalizumab reduces cysteinyl leukotriene and 9α,11β-prostaglandin F2 overproduction in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2016) 137(5):1585–1587.e4. doi: 10.1016/j.jaci.2015.09.034
88. Gevaert P, Omachi TA, Corren J, Mullol J, Han J, Lee SE, et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J Allergy Clin Immunol. (2020) 146(3):595–605. doi: 10.1016/j.jaci.2020.05.032
89. Forster-Ruhrmann U, Stergioudi D, Pierchalla G, Fluhr JW, Bergmann KC, Olze H. Omalizumab in patients with NSAIDs-exacerbated respiratory disease. Rhinology. (2020) 0(0):0–0. doi: 10.4193/Rhin19.318
90. Xu X, Reitsma S, Wang DY, Fokkens WJ. Updates in biologic therapy for chronic rhinosinusitis with nasal polyps and NSAID -exacerbated respiratory disease. Allergy. (2022) 77(12):3593–605. doi: 10.1111/all.15507
91. Gevaert P, Van Bruaene N, Cattaert T, Van Steen K, Van Zele T, Acke F, et al. Mepolizumab, a humanized anti-IL-5 mAb, as a treatment option for severe nasal polyposis. J Allergy Clin Immunol. (2011) 128(5):989–995.e1-8. doi: 10.1016/j.jaci.2011.07.056
92. Bachert C, Sousa AR, Lund VJ, Scadding GK, Gevaert P, Nasser S, et al. Reduced need for surgery in severe nasal polyposis with mepolizumab: randomized trial. J Allergy Clin Immunol. (2017) 140(4):1024–1031.e14. doi: 10.1016/j.jaci.2017.05.044
93. Tuttle KL, Buchheit KM, Laidlaw TM, Cahill KN. A retrospective analysis of mepolizumab in subjects with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. (2018) 6(3):1045–7. doi: 10.1016/j.jaip.2018.01.038
94. Lombardo N, Pelaia C, Ciriolo M, Della Corte M, Piazzetta G, Lobello N, et al. Real-life effects of benralizumab on allergic chronic rhinosinusitis and nasal polyposis associated with severe asthma. Int J Immunopathol Pharmacol. (2020) 34:2058738420950851. doi: 10.1177/2058738420950851
95. Maspero J, Harrison T, Werkström V, Wu Y, Gopalan G, Zangrilli J. Clinical efficacy of benralizumab in patients with severe, uncontrolled eosinophilic asthma and nasal polyposis: pooled analysis of the SIROCCO and CALIMA trials. J Allergy Clin Immunol. (2018) 141(2):AB12. doi: 10.1016/j.jaci.2017.12.038
96. Laidlaw TM, Mullol J, Fan C, Zhang D, Amin N, Khan A, et al. Dupilumab improves nasal polyp burden and asthma control in patients with CRSwNP and AERD. J Allergy Clin Immunol Pract. (2019) 7(7):2462–2465.e1. doi: 10.1016/j.jaip.2019.03.044
97. Scangas GA, Wu AW, Ting JY, Metson R, Walgama E, Shrime MG, et al. Cost utility analysis of dupilumab versus endoscopic Sinus surgery for chronic rhinosinusitis with nasal polyps. Laryngoscope. (2021) 131(1):E26–33. doi: 10.1002/lary.28648
98. Parasher AK, Gliksman M, Segarra D, Lin T, Rudmik L, Quast T. Economic evaluation of dupilumab versus endoscopic sinus surgery for the treatment of chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. (2022) 12(6):813–20. doi: 10.1002/alr.22936
99. Corren J, Parnes JR, Wang L, Mo M, Roseti SL, Griffiths JM, et al. Tezepelumab in adults with uncontrolled asthma. N Engl J Med. (2017) 377(10):936–46. doi: 10.1056/NEJMoa1704064
100. Nopsopon T, Lassiter G, Chen ML, Alexander GC, Keet C, Hong H, et al. Comparative efficacy of tezepelumab to mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: a Bayesian network meta-analysis. J Allergy Clin Immunol. (2023) 151(3):747–55. doi: 10.1016/j.jaci.2022.11.021
101. Boada-Fernández-Del-Campo C, García-Sánchez-Colomer M, Fernández-Quintana E, Poza-Guedes P, Rolingson-Landaeta JL, Sánchez-Machín I, et al. Real-World safety profile of biologic drugs for severe uncontrolled asthma: a descriptive analysis from the spanish pharmacovigilance database. J Clin Med. (2024) 13(14):4192. doi: 10.3390/jcm13144192
102. Oykhman P, Paramo FA, Bousquet J, Kennedy DW, Brignardello-Petersen R, Chu DK. Comparative efficacy and safety of monoclonal antibodies and aspirin desensitization for chronic rhinosinusitis with nasal polyposis: a systematic review and network meta-analysis. J Allergy Clin Immunol. (2022) 149(4):1286–95. doi: 10.1016/j.jaci.2021.09.009
103. Wood A, Baxter G, Thies F, Kyle J, Duthie G. A systematic review of salicylates in foods: estimated daily intake of a Scottish population. Mol Nutr Food Res. (2011) 55(Suppl 1):S7–14. doi: 10.1002/mnfr.201000408
104. Sommer DD, Rotenberg BW, Sowerby LJ, Lee JM, Janjua A, Witterick IJ, et al. A novel treatment adjunct for aspirin exacerbated respiratory disease: the low-salicylate diet: a multicenter randomized control crossover trial. Int Forum Allergy Rhinol. (2016) 4:385–91. doi: 10.1002/alr.21678
105. Sowerby LJ, Patel KB, Schmerk C, Rotenberg BW, Rocha T, Sommer DD. Effect of low salicylate diet on clinical and inflammatory markers in patients with aspirin exacerbated respiratory disease—a randomized crossover trial. J Otolaryngol - Head Neck Surg J Oto-Rhino-Laryngol Chir Cervico-Faciale. (2021) 50(1):27. doi: 10.1186/s40463-021-00502-4
106. Schneider TR, Johns CB, Palumbo ML, Murphy KC, Cahill KN, Laidlaw TM. Dietary fatty acid modification for the treatment of aspirin-exacerbated respiratory disease: a prospective pilot trial. J Allergy Clin Immunol Pract. (2018) 6(3):825–31. doi: 10.1016/j.jaip.2017.10.011
107. Cardet JC, White AA, Barrett NA, Feldweg AM, Wickner PG, Savage J, et al. Alcohol-induced respiratory symptoms are common in patients with aspirin exacerbated respiratory disease. J Allergy Clin Immunol Pract. (2014) 2(2):208–13. doi: 10.1016/j.jaip.2013.12.003
108. Candelo E, McCalla M, Valderrama OA, Avila-Castano K, Chelf C, Olomu O, et al. Relationship between alcohol intolerance and aspirin-exacerbated respiratory disease (AERD): systematic review. Otolaryngol–Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg. (2023) 169(1):12–20. doi: 10.1002/ohn.248
109. Glicksman JT, Parasher AK, Doghramji L, Brauer D, Waldram J, Walters K, et al. Alcohol-induced respiratory symptoms improve after aspirin desensitization in patients with aspirin-exacerbated respiratory disease. Int Forum Allergy Rhinol. (2018) 8(10):1093–7. doi: 10.1002/alr.22168
110. Mustafa SS, Vadamalai K, Scott B, Ramsey A. Dupilumab as add-on therapy for chronic rhinosinusitis with nasal polyposis in aspirin exacerbated respiratory disease. Am J Rhinol Allergy. (2021) 35(3):399–407. doi: 10.1177/1945892420961969
111. Brightling CE, Brusselle G, Altman P. The impact of the prostaglandin D2 receptor 2 and its downstream effects on the pathophysiology of asthma. Allergy. (2020) 75(4):761–8. doi: 10.1111/all.14001
112. Yamamoto M, Okano M, Fujiwara T, Kariya S, Higaki T, Nagatsuka H, et al. Expression and characterization of PGD2 receptors in chronic rhinosinusitis: modulation of DP and CRTH2 by PGD2. Int Arch Allergy Immunol. (2009) 148(2):127–36. doi: 10.1159/000155743
113. Brightling CE, Gaga M, Inoue H, Li J, Maspero J, Wenzel S, et al. Effectiveness of fevipiprant in reducing exacerbations in patients with severe asthma (LUSTER-1 and LUSTER-2): two phase 3 randomised controlled trials. Lancet Respir Med. (2021) 9(1):43–56. doi: 10.1016/S2213-2600(20)30412-4
114. Gevaert P, Bachert C, Maspero JF, Cuevas M, Steele D, Acharya S, et al. Phase 3b randomized controlled trial of fevipiprant in patients with nasal polyposis with asthma (THUNDER). J Allergy Clin Immunol. (2022) 149(5):1675–1682.e3. doi: 10.1016/j.jaci.2021.12.759
115. Cahill KN, Bensko JC, Boyce JA, Laidlaw TM. Prostaglandin D₂: a dominant mediator of aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2015) 135(1):245–52. doi: 10.1016/j.jaci.2014.07.031
116. Cahill KN. Immunologic effects of aspirin desensitization and high-dose aspirin therapy in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2021) 148(2):344–7. doi: 10.1016/j.jaci.2021.06.009
117. Laidlaw TM, Buchheit KM, Cahill KN, Hacker J, Cho L, Cui J, et al. Trial of thromboxane receptor inhibition with ifetroban: tP receptors regulate eicosanoid homeostasis in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. (2023) 152(3):700–710.e3. doi: 10.1016/j.jaci.2023.03.030
118. Laidlaw TM, Levy JM. NSAID-ERD Syndrome: the new hope from prevention, early diagnosis, and new therapeutic targets. Curr Allergy Asthma Rep. (2020) 20(4):10. doi: 10.1007/s11882-020-00905-9
119. Yong M, Kirubalingam K, Desrosiers MY, Kilty SJ, Thamboo A. Cost-effectiveness analysis of biologics for the treatment of chronic rhinosinusitis with nasal polyps in Canada. Allergy Asthma Clin Immunol. (2023) 19(1):90. Published 2023 October 14. doi: 10.1186/s13223-023-00823-1
120. Ali A, García E, Torres-Duque CA, Rey D, Botero L, Saenz S, et al. Cost-effectiveness analysis of dupilumab versus omalizumab, mepolizumab, and benralizumab added to the standard of care in adults with severe asthma in Colombia. Expert Rev Pharmacoecon Outcomes Res. (2024) 24(3):361–74. doi: 10.1080/14737167.2023.2282668
121. Staufenberg AR, Frankenberger HK, Förster-Ruhrmann U, Spahn FC, Klimek L, Fruth K, et al. Biologikatherapie bei schwer erkrankten patienten mit „NSAID-exacerbated respiratory disease“ und stattgehabter ASS-Desaktivierung: Ergebnisse einer multizentrischen Studie [biologic therapy in patients with severe NSAID-exacerbated respiratory disease and previous aspirin desensitization: results of a multicentric study]. HNO. (2024) 72(7):473–83. doi: 10.1007/s00106-024-01433-y
122. Wangberg H, Spierling Bagsic SR, Osuna L, White AA. Appraisal of the real-world effectiveness of biologic therapies in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. (2022) 10(2):478–484.e3. doi: 10.1016/j.jaip.2021.09.030
123. Jean T, Eng V, Sheikh J, Kaplan MS, Goldberg B, Jau Yang S, et al. Effect of omalizumab on outcomes in patients with aspirin-exacerbated respiratory disease. Allergy Asthma Proc. (2019) 40(5):316–20. doi: 10.2500/aap.2019.40.4241
124. Cooper T, Greig SR, Zhang H, Seemann R, Wright ED, Vliagoftis H, et al. Objective and subjective sinonasal and pulmonary outcomes in aspirin desensitization therapy: a prospective cohort study. Auris Nasus Larynx. (2019) 46(4):526–32. doi: 10.1016/j.anl.2018.12.002
125. Mortazavi N, Esmaeilzadeh H, Abbasinazari M, Babaie D, Alyasin S, Nabavizadeh H, et al. Clinical and immunological efficacy of aspirin desensitization in nasal polyp patients with aspirin-exacerbated respiratory disease. Iran J Pharm Res. (2017) 16(4):1639–47.29552073
126. Lee SE, Farquhar DR, Adams KN, Masood MM, Senior BA, Thorp BD, et al. Effect of zileuton treatment on sinonasal quality of life in patients with aspirin-exacerbated respiratory disease. Am J Rhinol Allergy. (2019) 33(6):791–5. doi: 10.1177/1945892419873211
127. Kęszycka PK, Lange E, Gajewska D. Effectiveness of personalized low salicylate diet in the management of salicylates hypersensitive patients: interventional study. Nutrients. (2021) 13(3):991. Published 2021 March 19. doi: 10.3390/nu13030991
Keywords: aspirin exacerbated respiratory disease, AERD, N-ERD, Samter's triad, chronic rhinosinusitis, nasal polyposis
Citation: Ley-Tomas JJ, Xicotencatl-Tellez AM, García-Cruz ML and Jiménez-Chobillon MA (2024) Nonsteroidal antiinflammatory drug-exacerbated respiratory disease: molecular mechanism, management and treatment. Front. Allergy 5:1462985. doi: 10.3389/falgy.2024.1462985
Received: 11 July 2024; Accepted: 7 November 2024;
Published: 27 November 2024.
Edited by:
Jessica Dal Col, University of Salerno, ItalyReviewed by:
Mona Al-Ahmad, Kuwait University, KuwaitJoshua L. Kennedy, University of Arkansas for Medical Sciences, United States
Copyright: © 2024 Ley-Tomas, Xicotencatl-Tellez, García-Cruz and Jiménez-Chobillon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. A. Jiménez-Chobillon, YWxqaWNob0BnbWFpbC5jb20=
†These authors share first authorship
‡These authors share senior authorship
§ORCID:
J. J. Ley-Tomas
orcid.org/0009-0003-3476-1588
A. M. Xicotencatl-Tellez
orcid.org/0009-0007-5070-2157
M. L. García-Cruz
orcid.org/0000-0002-5656-5196
M. A. Jiménez-Chobillon
orcid.org/0000-0001-6995-9453