
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Allergy, 20 March 2024
Sec. Rhinology
Volume 5 - 2024 | https://doi.org/10.3389/falgy.2024.1372919
This article is part of the Research Topic2022 in Review: RhinologyView all 8 articles
 T. Teeling1
T. Teeling1 C. Djouder1H. Laurens1
C. Djouder1H. Laurens1 J. H. Preyra1C. M. E. Shire1
J. H. Preyra1C. M. E. Shire1 E. Van Staeyen2
E. Van Staeyen2 D. M. Conti2,3
D. M. Conti2,3 G. K. Scadding4,5P. W. Hellings6,7,8*
G. K. Scadding4,5P. W. Hellings6,7,8*
Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) is a chronic inflammatory disease of the nose and paranasal sinus cavities that significantly affects well-being and social function, particularly in young adults and middle-aged populations. CRSwNP is a common health condition in the Western world, with an estimated prevalence of 3%. Despite worldwide evidence-based treatment guidelines such as the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020 and the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) chronic rhinosinusitis (CRS) pocket guide, a significant number of patients remain undiagnosed and/or uncontrolled with repeated oral corticosteroids (OCS) treatments and/or (multiple) endoscopic sinus surgeries (ESS).
Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) is a chronic inflammatory disease of the nose and paranasal sinus cavities that significantly affects well-being and social function, particularly in young adults and middle-aged populations (1). CRSwNP is a common health condition in the Western world, with an estimated prevalence of 3% (1–3). Despite worldwide evidence-based treatment guidelines such as the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020 (4) and the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) chronic rhinosinusitis (CRS) pocket guide (5), a significant number of patients remain undiagnosed and/or uncontrolled with repeated oral corticosteroids (OCS) treatments and/or (multiple) endoscopic sinus surgeries (ESS).
Patients with CRSwNP exhibit sinonasal symptoms like nasal obstruction, smell dysfunction with anosmia in a significant proportion, persistent nasal discharge, and/or facial pain (1). Apart from sinonasal symptoms, CRSwNP is associated with an increased risk of asthma, otitis media, depression and social dysfunction (6). Similarly important is the extensively studied association between CRSwNP and sleep disturbance, which is linked to cardiovascular and cerebrovascular disease and reduced quality of life for both the patient and their partner (7–9). The impact of CRSwNP on quality of life (QoL) has been observed to be equivalent to other chronic conditions such as chronic obstructive pulmonary disease (COPD), congestive heart failure, and diabetes (10, 11). Yet in comparison to asthma, respiratory allergies and atopic dermatitis (12–14), few global patient initiatives have been undertaken to bring the physical and psychosocial burden of disease of CRSwNP to the attention of health policymakers, the general public, or physicians. Although it is commonly acknowledged that upper and lower airway diseases are linked to inflammation in the airways (15), few global initiatives have been undertaken to emphasise the patient perspective and the impact of diseases in both the upper and lower airways (16–18).
The substantial burden of CRSwNP on both the patient as well as the society warrant the implementation of improved treatment options and the reorganisation of existing care pathways (19, 20). The substantial financial burden associated with CRSwNP arises from expenditures associated with healthcare use, absenteeism from work and school, and decreased job productivity (21, 22).
During the EUFOREA's first annual Global Chronic Rhinosinusitis with Nasal Polyps Awareness Day on April 20, 2022 in the European Parliament in Brussels (Figure 1A) a moderator and a panel consisting of global experts in CRSwNP and patient representatives from EUFOREA's patient advisory board (PAB) took part in an informal debate on the burden of CRSwNP (Figure 1B) on the nature of the complex names “CRSwNP” or “Chronic Rhinosinusitis with Nasal Polyps’ for patients, for health policy makers and for physicians. Discussions among members of EUFOREA's patient advisory board revealed the challenges faced by patients with CRSwNP as they not only navigate conversations with family, friends and peers about the burden of their disease and its associated comorbidities, but also as they seek out reliable information about their disease online to play an active and empowered role in as they discuss treatment options with their healthcare team. The difficult and inconsistent naming used for CRSwNP by patients and healthcare professionals alike not only exacerbates patients” reported perception of a lack of resources about their disease, but also hinders patients’ involvement in shared decision making with their healthcare team.

Figure 1. (A) Group picture of debate at the first annual Global Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) awareness day 2022. (B) EUFOREA Innovation Forum debate on the need for a lay language term to improve patient-provider communications.
The definition of CRSwNP was proposed at the first EPOS expert committee meeting in Amsterdam in 2001. This term encompasses multiple facets of the disease, including its inflammatory nature, the involvement of the nasal and paranasal sinus cavities, as well as the presence of bilateral sino-nasal polyps found either during nasal endoscopy or on CT scans. The name CRSwNP also allows the phenotypic distinction of CRSwNP from those patients without the presence of nasal polyps, defined as CRSsNP with “s” standing for “sin” or without. In addition, the term CRSwNP also avoids confusion with a condition called “adenoid hypertrophy”, which is often referred to as “nasal polyps” in lay language. Since the release of the first EPOS consensus document, experts worldwide have adopted the term CRSwNP in all guidelines and publications given the best coverage of the disease with phenotypic definition of the presence of nasal polyps.
In spite of all benefits and accuracy of the name CRSwNP, the introduction of a lay language term for CRSwNP is considered useful by patients in the light of the following considerations:
- CRSwNP is barely pronounceable by patients and even more so by non-native English-speaking patients and even physicians, hence leading to several uncomfortable situations where patients can neither express nor discuss their disease with physicians and peers as the name is too complex, and
- CRSwNP is still not a well-known disease entity beyond the ear, nose and throat (ENT) specialist community, and
- CRSwNP does not cover the complexity of the disease with most severe patients having co-morbidities like middle ear problems, lower airways disease (including asthma), aspirin intolerance and/or allergies, and
- CRSwNP disease often requires a multispeciality approach for reaching optimal disease control.
This exercise in patient advocacy has been done in the past and the literature shows how terminology has been divided when naming diseases. As a result, there are terms used by the medical community and others used by the patient community that refer to the same disease or event and are equally accepted. Examples included in Table 1:
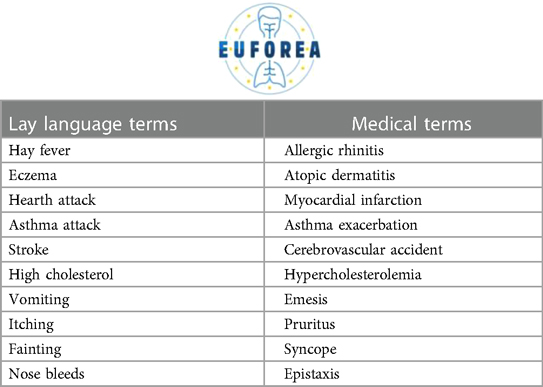
Table 1. Examples of lay language terms vs. medical terms.
Following the PAB meeting of EUFOREA in September 2022, European patients suffering from long-standing severe CRSwNP expressed the suggestion to implement a new lay language term for CRSwNP (16–18), with the ambition to find a consensus amongst patients on how to properly name their condition in a simple, comprehensive and appealing way for all stakeholders. The following names for CRSwNP were discussed during two virtual meetings with a panel of over 50 European patients as well as over 30 experts affiliated with the EUFOREA expert panel teams in 2022 and 2023: Nasal Polyp Syndrome (NPS), Sinus Disease, Type 2 Inflammation Disease, Nasal Polyps, NP, Chronic Nasal Inflammation, or Stuffy/Blocked Nose Syndrome. After 2 rounds of discussions with patients and exploration with expert colleagues, in which some of the names were dropped and others proposed, the majority of patients have opted for the name Nasal Polyp Syndrome (Figure 2). This name was also approved by experts involved in the recent EUFOREA new pocket guide and treatment algorithm for chronic rhinosinusitis (Figure 3).
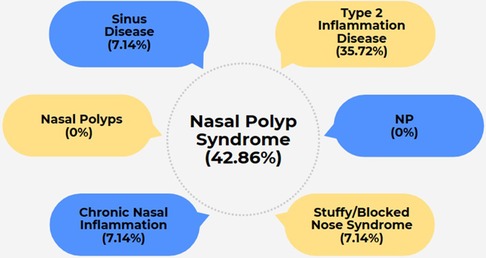
Figure 2. Lay language terms proposed by the EUFOREA patient advisory board along with poll results for preferred term.
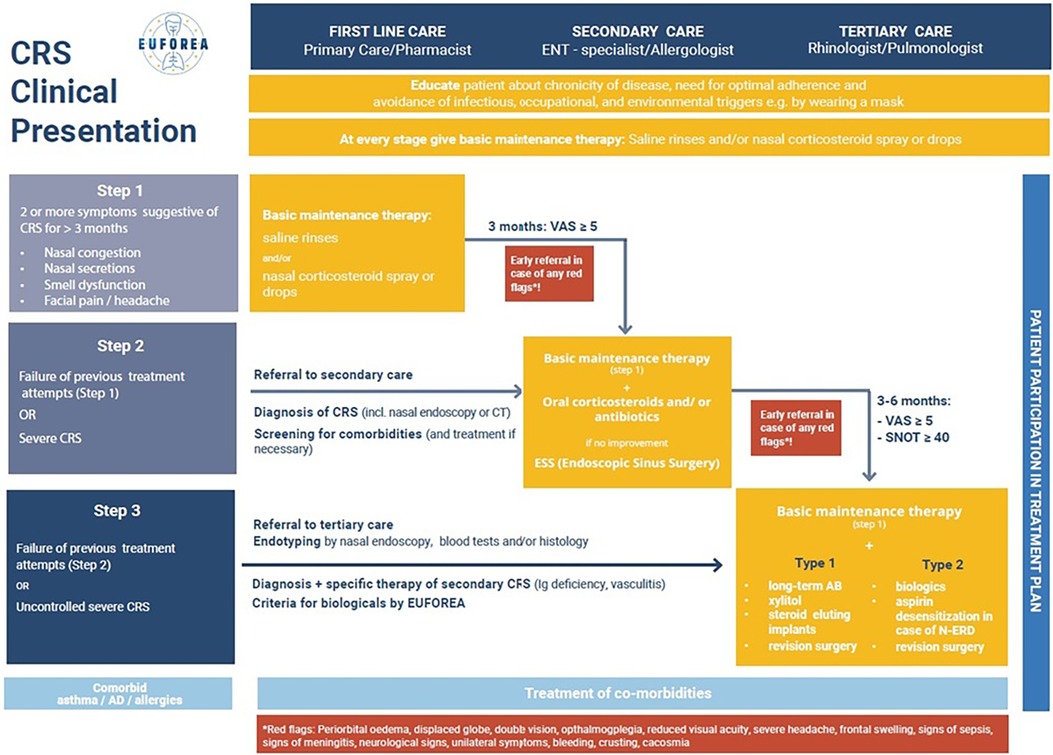
Figure 3. EUFOREA chronic rhinosinusitis treatment algorithm.
The newly proposed name “Nasal Polyp Syndrome” by EUFOREA is endorsed by the CRS expert panel of EUFOREA and the EUFOREA patient advisory board members as it carries the following advantages:
- Simplicity in pronunciation
- Simplicity in communication about the disease with the patient, with physicians and with health policy makers
- Shorter name than CRSwNP, both in full as well as in abbreviated form
- Covering the burden of disease, with “syndrome” referring to a more than just localised inflammatory or mechanical obstruction of the sinonasal cavities by nasal polyps
- Syndrome implicitly refers to a severe and chronic condition, with/without comorbidities and challenges to achieve disease control
- Syndrome implicitly refers to the need for a multispeciality approach in a substantial portion of patients where multispeciality collaboration is warranted.
In case the ENT community would adopt the term Nasal Polyp Syndrome in the future, the patients of the PAB of EUFOREA are convinced that this might represent a step towards better recognition of the disease by the healthcare community and society as a whole.
From the patient's perspective, the need for a lay language name for Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) is evident. A lay name that acknowledges the multifaceted impact on patients can foster greater empathy and understanding from healthcare providers, family, and society. By adopting a more patient-centred and inclusive name, we can encourage a more compassionate approach to patient care and support, thereby strengthening the doctor-patient relationship and enhancing treatment adherence which is crucial to ensure better communication and patient understanding.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
TT: Writing – review & editing, Writing – original draft, Validation, Supervision, Methodology, Investigation, Formal Analysis, Conceptualization. CD: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Formal Analysis, Conceptualization. HL: Visualization, Writing – review & editing, Formal Analysis, Conceptualization. JP: Writing – review & editing, Writing – original draft, Supervision, Investigation, Formal Analysis, Conceptualization. CS: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Conceptualization. EVS: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Formal Analysis, Conceptualization. DC: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Formal Analysis, Conceptualization. GS: Writing – review & editing, Writing – original draft, Visualization, Formal Analysis, Conceptualization. PH: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Data curation, Conceptualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
DMC: Serves as academic manager at the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) and as review editor at Frontiers in Allergy, rhinology section. GKS: Honoraria for articles, speaker and advisory boards: ALK, Bayer, GlaxoSmithKline, Haleon, Noucor, Sanofi-Regeneron, and Viatris. Chair of BSACI rhinitis guidelines, Scientific Chief Editor, Rhinology Section of Frontiers in Allergy, Board member and AR lead for EUFOREA, and Chair/member Data Monitoring Committees on SLIT for ALK. MM: Honoraria for speaker and advisory boards: Sanofi, Glenmark, P&G, Immunotek, Cipla, Thermo-Scientific, Lancet laboratories. EUFOREA expert panel member. PWH: Is recipient of consultancy/lecture fees or unrestricted research grants from Sanofi/Regeneron, Novartis, GSK, Medtronic and Viatris.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European Position paper on rhinosinusitis and nasal polyps. Rhinology. (2020) 58:1–464. doi: 10.4193/Rhin20.601
2. Chen S, Zhou A, Emmanuel B, Thomas K, Guiang H. Systematic literature review of the epidemiology and clinical burden of chronic rhinosinusitis with nasal polyposis. Curr Med Res Opin. (2020) 36:1897–911. doi: 10.1080/03007995.2020.1815682
3. Sedaghat AR, Kuan EC, Scadding GK. Epidemiology of chronic rhinosinusitis: prevalence and risk factors. J Allergy Clin Immunol Pract. (2022) 10(6):1395–403. doi: 10.1016/j.jaip.2022.01.016
4. Calus L, Van Bruaene N, Bosteels C, Dejonckheere S, Van Zele T, Holtappels G, et al. Twelve-year follow-up study after endoscopic sinus surgery in patients with chronic rhinosinusitis with nasal polyposis. Clin Transl Allergy. (2019) 9:30. doi: 10.1186/s13601-019-0269-4
5. Hellings PW, Fokkens WJ, Orlandi R, Adriaensen GF, Alobid I, Baroody FM, et al. The EUFOREA pocket guide for chronic rhinosinusitis. Rhinology. (2023) 61(1):85–9. doi: 10.4193/Rhin22.344
6. Schlosser RJ, Gage SE, Kohli P, Soler ZM. Burden of illness: a systematic review of depression in chronic rhinosinusitis. Am J Rhinol Allergy. (2016) 30:250–6. doi: 10.2500/ajra.2016.30.4343
7. Alt JA, Smith TL. Chronic rhinosinusitis and sleep: a contemporary review. Int Forum Allergy Rhinol. (2013) 3(11):941–9. doi: 10.1002/alr.21217
8. Mahdavinia M, Schleimer RP, Keshavarzian A. Sleep disruption in chronic rhinosinusitis. Expert Rev Anti Infect Ther. (2017) 15(5):457–65. doi: 10.1080/14787210.2017.1294063
9. Xiang B, Hu M, Yu H, Zhang Y, Wang Q, Xue F. Highlighting the importance of healthy sleep patterns in the risk of adult asthma under the combined effects of genetic susceptibility: a large-scale prospective cohort study of 455 405 participants. BMJ Open Respir Res. (2023) 10(1):e001535. doi: 10.1136/bmjresp-2022-001535
10. Van Agthoven M, Fokkens WJ, van de Merwe JP, Marijke van Bolhuis E, Uylde Groot CA, Busschbach JJ. Quality of life of patients with refractory chronic rhinosinusitis: effects of filgrastim treatment. Am J Rhinol. (2001) 15:231–7. doi: 10.1177/194589240101500403
11. Wensing M, Vingerhoets E, Grol R. Functional status, health problems, age and comorbidity in primary care patients. Qual Life Res. (2001) 10:141–8. doi: 10.1023/A:1016705615207
12. Menzies-Gow A, Canonica GW, Winders TA, de Sousa J C, Upham JW, Fink-Wagner AH. A charter to improve patient care in severe asthma. Adv Ther. (2018) 35:1485–96. doi: 10.1007/s12325-018-0777-y
13. Boguniewicz M, Alexis AF, Beck LA, Block J, Eichenfield LF, Fonacier L, et al. Expert perspectives on management of moderate-to-severe atopic dermatitis: a multidisciplinary consensus addressing current and emerging therapies. J Allergy Clin Immunol Pract. (2017) 5:1519–31. doi: 10.1016/j.jaip.2017.08.005
14. Cvetkovski B, Kritikos V, Yan K, Bosnic-Anticevich S. Tell me about your hay fever: a qualitative investigation of allergic rhinitis management from the perspective of the patient. NPJ Prim Care Respir Med. (2018) 28:3. doi: 10.1038/s41533-018-0071-0
15. Hellings PW, Prokopakis EP. Global airway disease beyond allergy. Curr Allergy Asthma Rep. (2010) 10:143–9. doi: 10.1007/s11882-010-0107-1
16. De Prins L, Raap U, Mueller T, Schmid-Grendelmeier P, Haase CH, Backer V, et al. White paper on European patient needs and suggestions on chronic type 2 inflammation of airways and skin by EUFOREA. Front Allergy. (2022) 3:889221. doi: 10.3389/falgy.2022.889221
17. Claeys N, Teeling MT, Legrand P, Poppe M, Verschueren P, De Prins L, et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front Allergy. (2021) 2:761388. doi: 10.3389/falgy.2021.761388
18. Pugin B, Deneyer L, Bachert C, Alobid I, Alobid I, Bousquet J, De Carlo G, et al. Patient advisory board for chronic rhinosinusitis—a EUFOREA initiative. Rhinology. (2019) 57(5):331–5. doi: 10.4193/Rhin19.012
19. Hellings PW. SWOT Analysis of chronic rhinosinusitis care anno 2022. J Allergy Clin Immunol Pract. (2022) 10(6):1468–71. doi: 10.1016/j.jaip.2022.01.039
20. Hellings PW. From prevention to optimal treatment in chronic rhinosinusitis. Rhinology. (2018) 56(4):305–6. doi: 10.4193/Rhin.18.404
21. Lourijsen ES, Fokkens WJ, Reitsma S. Direct and indirect costs of adult patients with chronic rhinosinusitis with nasal polyps. Rhinology. (2020) 58:213–7. doi: 10.4193/RHINOL/20.092
Keywords: EUFOREA, CRSwNP, Nasal Polyp Syndrome, global CRSwNP awareness day, patient-provider communications, lay language, patient advisory board
Citation: Teeling T, Djouder C, Laurens H, Preyra JH, Shire CME, Van Staeyen E, Conti DM, Scadding GK and Hellings PW (2024) Nasal polyp syndrome: a patient-centred term for CRSwNP by EUFOREA. Front. Allergy 5:1372919. doi: 10.3389/falgy.2024.1372919
Received: 18 January 2024; Accepted: 5 March 2024;
Published: 20 March 2024.
Edited by:
Giancarlo Ottaviano, University of Padua, ItalyReviewed by:
Alfonso Luca Pendolino, University College London, United Kingdom© 2024 Teeling, Djouder, Laurens, Preyra, Shire, Van Staeyen, Conti, Scadding and Hellings. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: P. W. Hellings cGV0ZXIuaGVsbGluZ3NAZXVmb3JlYS5ldQ==
Abbreviations COPD, Chronic Obstructive Pulmonary Disease; CRS, Chronic Rhinosinusitis; CRSsNP, Chronic Rhinosinusitis without Nasal Polyps; CRSwNP, Chronic Rhinosinusitis with Nasal Polyps; ENT, Ear, Nose and Throat; EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps; ERS, European Respiratory Society; ESS, Endoscopic Sinus Surgery; EUFOREA, European Forum for Research and Education in Allergy and Airway Diseases; NPS, Nasal Polyp Syndrome; OCS, Oral Corticosteroids; PAB, Patient Advisory Board.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.