
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Allergy, 08 April 2024
Sec. Food Allergy
Volume 5 - 2024 | https://doi.org/10.3389/falgy.2024.1346843
This article is part of the Research TopicUnderstanding Eosinophilic EsophagitisView all 7 articles
 Luiza Salgado Nader1,2*
Luiza Salgado Nader1,2* Matias Epifanio1
Matias Epifanio1 Mariana Guimarães Coelho3
Mariana Guimarães Coelho3 Cintia Steinhaus1,2
Cintia Steinhaus1,2 Melina Melere1,2
Melina Melere1,2 Carolina Soares da Silva1,2Cristina Targa Ferreira1,2
Carolina Soares da Silva1,2Cristina Targa Ferreira1,2
Introduction: Eosinophilic esophagitis is a newly recognized entity, in which there is significant evidence available that clearly demonstrates the positive impact of PPIs on reducing esophageal eosinophilia in individuals across different age groups, including children, adolescents, and adults. Multiple mechanisms have been proposed to explain how this treatment effect occurs. In Brazil, there seems to be a lack of studies that have prospectively assessed the clinical and therapeutic response rate in pediatric patients with EoE. The objective of this study was to prospectively evaluate the clinical and therapeutic response of pediatric patients with EoE in a medical center located in southern Brazil, by investigating the effectiveness of PPI treatment.
Methods: This study is a clinical, prospective, open trial that took place in a pediatric hospital located in southern Brazil. The focus of the study was on patients diagnosed with Eosinophilic Esophagitis (EoE) who were given treatment using omeprazole/esomeprazole at a dosage of 1 mg.kg per dose, twice daily, for a period of 8–12 weeks. Following the treatment period, the patients underwent another endoscopy. Patients who exhibited 15 or less eosinophils in the biopsy conducted after the treatment were considered as responders.
Results: A total of 27 patients was evaluated (74.1% boys). The average age (± standard deviation) was 8 years (±4). Nineteen patients (70.3%) were considered as responders to PPI treatment: 6 patients—22.2%—exhibited a complete response (defined as having 5 or fewer eosinophil per high power field. Additionally, 13 patients—48.1%—demonstrated a partial response, characterized by eosinophil counts exceeding 5 but less than 15 eos/hpf. When comparing the responder and non-responder groups at presentation, a statistical difference was observed in the prevalence of food refusal as a presenting symptom. Food refusal was found to be more prevalent in the non-responder group (87.5% vs. 26.3%, P = 0.008). No differences were observed in terms of atopy history and endoscopic scores. Upon comparing the histological findings from the post-treatment endoscopy of the two groups, it was observed that PPI responders exhibited a greater tendency to decrease basal cell hyperplasia (P = 0.06) and intercellular edema (P = 0.08).
Conclusion: In this group of pediatric patients with EoE in Southern Brazil most patients showed a high prevalence of histological, endoscopic, and clinical response to PPI treatment. PPIs showed efficacy in Brazilian patients with EoE, most of whom would probably not be able to adequately undergo other treatments.
Clinical Trial Registration: https://ensaiosclinicos.gov.br/rg/RBR-2ntbth9, identifier (U1111-1301-1842).
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated disease with a type 2 inflammatory response. It is characterized by symptoms related to esophageal dysfunction and histologically by the presence of eosinophilic infiltrate in the esophagus, defined as having more than 15 eosinophils per high-power field (eos/hpf) on esophageal biopsy (1).
To establish a diagnosis of EoE, it is necessary to have symptoms indicating esophageal dysfunction and the presence of at least 15 eos/phf on esophageal biopsy. Additionally, it is necessary to rule out non-EoE disorders that could cause or contribute to esophageal eosinophilia (1).
Currently, the prevalence of the disease has been increasing worldwide (2, 3). In Brazil, this number varies from 10 to 50/100.000 people, based on adult and pediatric population (4). The incidence is constantly rising and is estimated to be 10/100.000 cases per year in the country (5). This increase is probably due to a real increase in the disease and, also, due to the result of a greater awareness of it (3).
However, there is no current treatment approved in Brazil that directly disrupts disease pathogenesis.
Standard treatments for EoE include proton pump inhibitors (PPIs), food elimination diets, swallowed topical corticosteroids and esophageal dilations in case of stenosing disease (6). Recent studies show a histological response rate of 1 food elimination diet and 6 food elimination diets of 34% and 40%, respectively (7, 8). Topical steroids had a histological response rate of 59% (7). Nevertheless, these therapies have limitations, and, in clinical practice, food elimination diets have the issue of lower quality of life because of the dietary restrictions and there are concerns about using topical preparations, especially in young children who are using other topical preparations for co-morbid atopic conditions (9).
The use of PPI monotherapy may demonstrate clinical benefits for certain patients. PPIs have a potential to be an effective, primary therapeutic option. Due to their longstanding safety profile and easy administration, patients may choose to initiate treatment with PPIs prior to considering corticosteroids or exclusion diets (10).
The exact mechanism by which PPIs reduce eosinophilia in EoE is still a matter of debate. The proposed mechanisms are gastric acid suppression, which leads to a restoration of esophageal barrier function, and anti-inflammatory effects unrelated to gastric acid suppression. The antisecretory mechanism hypothesis is that the integrity of the esophageal epithelium would be compromised by exposure to gastric acid, leading to the entry of antigens and the activation of an immune response. The hypotheses of anti-inflammatory mechanisms are: (1) PPIs inhibit the migration of inflammatory cells to the esophageal epithelium, blocking the expression of cell surface adhesion molecules; (2) PPIs block STAT6-mediated eotaxin-3 expression, reducing the recruitment of eosinophils to the esophageal epithelium; (3) PPIs can stimulate the aryl hydrocarbon receptor, which normalizes the expression of genes involved in barrier function through inhibition of the IL-4/IL-13- STAT6 pathway; (4) PPIs can inhibit H+-K+-ATPase, which plays a role in eotaxin-3 expression, blocking eosinophil recruitment (11, 12).
We consider the present study relevant and important in clinical practice for populations with difficulties and social disparities, making it difficult to follow diets, and in countries where there are no approved corticosteroids. PPIs become a more inclusive option, as they are less expensive and more feasible being an applicable treatment for this population.
PPIs, despite having a non-optimal response, can help the group of less severe patients, especially children, as these patients will go through different stages in their development. Due to the absence of an approved formulation of swallowed topical corticosteroids in Brazil, the safety profile and convenient administration of PPIs make them an attractive and preferred initial treatment option (10, 13).
In general there is a lack of studies that have prospectively evaluated the clinical and therapeutic response rate in pediatric patients with EoE. This is the first Brazilian study that prospectively evaluates the response to PPIs in pediatric patients with EoE. According to the 2018 AGREE EoE guideline, published studies on the effectiveness of PPIs in treating EoE in children have variable results, probably due to the different doses used and duration of treatment, in addition to different environmental and phenotypic characteristics (1).
The objective of this study was to prospectively evaluate the clinical and therapeutic response of pediatric patients with EoE in a medical center located in southern Brazil, by investigating the effectiveness of PPI treatment. The secondary objective of this study is to assess the associations between demographic factors, clinical characteristics, endoscopic findings and histological features with the response to PPIs.
This study is a clinical, prospective, open trial carried out in a Pediatric Hospital located in southern Brazil, from May 2021 to May 2023. Children ranging from 1 month to 18 years of age who were referred to the pediatric endoscopy unit were included. Patients were included when they met the diagnostic criteria for EoE (presenting at least one symptom indicating esophageal dysfunction and the presence of at least 15 eos/hpf on esophageal biopsy) and absence of gastric and duodenal eosinophilia. Four to six biopsies were randomly obtained from the distal and middle esophagus. In order to rule out gastritis and eosinophilic gastroenteritis, biopsy specimens were also collected from the antrum and the duodenum.
Biopsy specimens were stained with hematoxylin and eosin, always analyzed by the same pathologist (M.G.C).
Patients received treatment with either omeprazole or esomeprazole magnesium at a dosage of 1 mg.kg per dose, max dose 40 mg twice a day, for a period of 8–12 weeks. Following the treatment period, the patients underwent another endoscopy. A questionnaire was given to patients to assess symptoms after the first and follow-up endoscopy.
Patients who had 15 or fewer eosinophils in the biopsy obtained after the PPI treatment were considered as responders. A complete response was considered as having 5 or less eos/hpf in all esophageal biopsies taken during the follow-up endoscopy. A partial response was considered to be one with a value of more than 5 and less than 15 eos/hpf. And a nonresponse to PPI therapy was determined by the presence of 15 or more eos/hpf in any of the esophageal biopsies obtained during the follow-up endoscopy.
Children who had previously or recently (up to 1 month before the endoscopy) received treatment with corticosteroids, an elimination diet or PPIs were excluded from the study. In addition, those diagnosed with gastric or duodenal eosinophilia or fungal, viral or caustic esophagitis were also excluded.
Endoscopic findings were described based on the EoE Endoscopic Reference Score (EREFS) established by Hirano et al. (14).
The description of qualitative variables was done by expressing them as absolute (N) and relative frequencies (%). When the distributions of quantitative variables were significantly close to normality, they were described using the mean and standard deviation.
The normality of the data was assessed using the Sapiro-Wilk test. Fisher's exact test, on the other hand, was used to test the relationship among qualitative (categorical) variables. The McNemar test was applied for the paired analysis of qualitative variables.
The student's T Test for independent samples was employed to test quantitative variables with a normal distribution. A level of statistical significance was considered when p ≤ 0.05. The analysis was carried out using the Python programming language in the Google Collab environment. As support, some calculations were performed in SPSS version 23 for Mac (IBM).
Both the patients and their parents consented to take part in the study, which was approved by the ethics committee (number 44070821.9.0000.5683) and the Research Committee of the Hospital da Criança Santo Antônio (HCSA), which belongs to the Irmandade Santa Casa de Misericórdia de Porto Alegre (ISCMPA). A Brazilian clinical trial registry was obtained (number RBR-2nbth9).
In this study, a sample of 27 patients, ranging from 1 month to 18 years, was diagnosed with EoE and all of them received PPI as first choice treatment.
19 patients (70.3%) were considered as responders to PPI. 6 patients (22.2%) had a complete response, and 13 (48.1%) had partial response (Figures 1, 2).
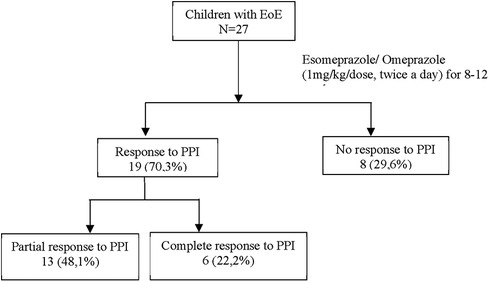
Figure 1. Patient flow. EoE, Eosinophilic Esophagitis; mg, milligram; kg, kilogram; PPI, proton-pump inhibitor.
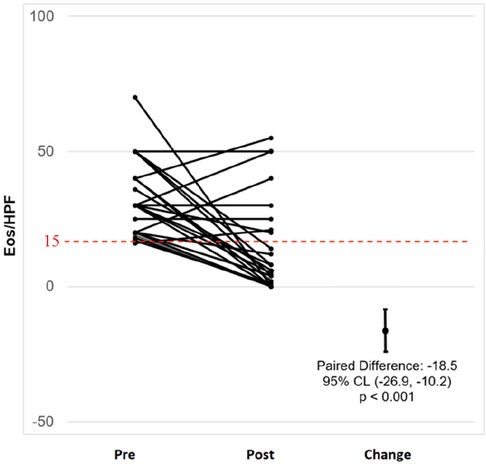
Figure 2. Paired graph with the number of eos/HPF of all individual patients before and after PPI treatment.
Table 1 summarizes the demographic and clinical features of all the responders and non-responders PPI groups.
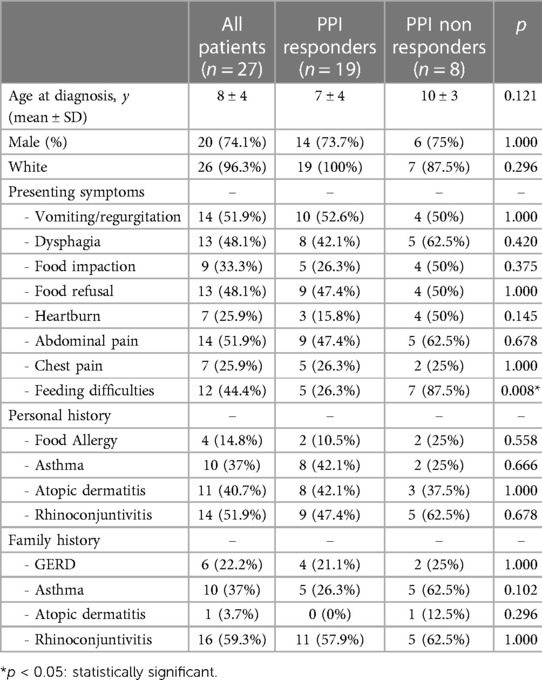
Table 1. Demographic and clinical features of patients with EoE.
Regarding clinical outcomes, most of the patients (26 children and 96%) reported symptom improvement with PPI treatment after follow-up endoscopy (Table 2). Symptoms were similar in both responders and non-responders to PPIs. Feeding difficulty as an initial symptom was a statistically significant feature in the responder group (n = 7/8) (p = 0.008).
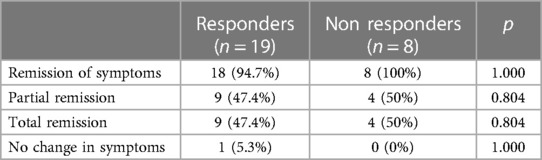
Table 2. Clinical outcome with EoE patients after PPI treatment.
Before the second endoscopy all patients were questioned about adherence to treatment and 100% of them reported having adhered to treatment with PPIs.
Pre- and post- treatment endoscopic and histological features are summarized in Table 3. Regarding pre- and post-treatment histological findings, the peak esophageal eosinophil count dropped significantly from the PPI responder group. Furthermore, we observed that the reduction in esophageal eosinophil counts was correlated with an improvement in other histological markers, such as basal cell hyperplasia (p = 0.003), edema (p = 0.008) in the PPI responder group (Table 3). The non-responder group had a persistence of basal cell hyperplasia and it could be a marker of failure of treatment response (p < 0.001) (Table 4).

Table 3. Endoscopic and histologic features.
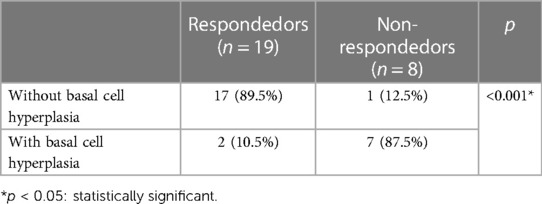
Table 4. Basal cell hyperplasia in the second endoscopy and treatment response.
Twenty-four patients (47%) had complete remission and 11 (21.6%) had a partial response. The same authors published a cross-sectional multicenter study in 2023, which analyzed the response to PPIs of 387 EoE patients, based on the analysis of the RENESE registry. In this group, 51.4% of patients presented a histological response, 36.9% being a complete response (15). Gómez-Torrijos et al. (16), in a 34 children prospective study in 2018, found a histological response of 26.5%. Lucendo et al. (17), in a systematic review in 2016, which included 188 children, showed a histological response of 54% and a clinical response of 65%, although heterogeneity was high (18).
In this group of pediatric patients with EoE in Southern Brazil, there was a high response rate to PPI treatment. Considering the 4 pediatric prospective studies in the literature (Table 5), our results are similar to Gutiérrez et al. (2) in 2016. The different responses in different locations may reflect variations in severity, doses administered or genetic, phenotype and/or environmental factors.
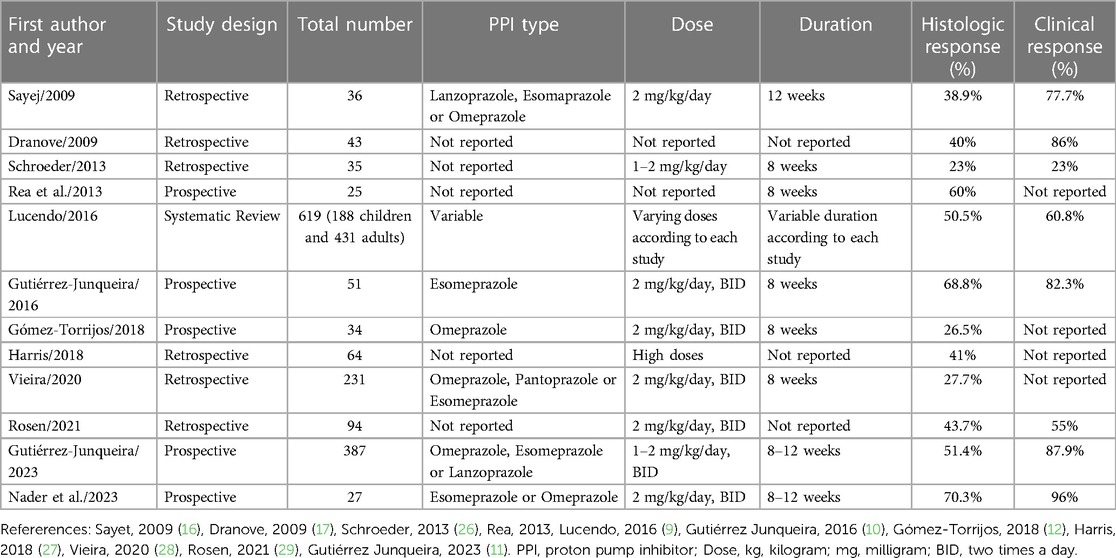
Table 5. PPI efficacy in children: histologic remission (<15 eos/hpf). Studies published in children.
Expanding our understanding of the long-term prognosis for patients with EoE who respond to PPI is crucial (13). These aspects have been investigated in a few pediatric and adult studies. According to two prospective studies, a majority of EoE patients who exhibit a positive response to initial high-dose PPI therapy tend to sustain this response even when the dosage is subsequently reduced (16, 19). Gutierrez-Junquera et al. demonstrated in a pediatric population up to 70% clinical and histological remission in 1 year of follow-up with half the initial dose (1 mg/kg/day).
Histologically, the improvement of basal cell hyperplasia after PPI treatment in responding patients may be an important finding, as there is some evidence that shows the persistence of this histological finding as a predictor of poor response to treatment (20, 21). Clinical improvement was observed in 94.1% of the children treated with PPIs, regardless of whether they achieved histological remission of eosinophils, as also observed in other pediatric studies (2, 15, 22, 23). Gutierréz et al. (2) showed 82.3% clinical improvement despite histological improvement. This study emphasizes that clinical improvement may not reflect a histological improvement, highlighting the importance of performing a endoscopy with esophageal biopsies to assess the response to PPI treatment.
A group of 630 patients, 76 of whom were children, showed a reduction in initial symptoms in 71%. The only statistically significant relationship was between PPIs non-responders and eating difficulties (p = 0.018) (24).
Our findings are similar to other pediatric (2) and adult studies that also found no relationship between clinical and endoscopic factors that could predict response to PPIs (25–28).
It is important to consider the limitations and strengths of this study. The biggest limitation of this study was the number of patients, as it was carried out during the COVID-19 pandemic. Other limitations to consider are the rarity of the disease and the even rarer patients who were not treated. Many patients were already receiving some form of OES treatment when the first endoscopy was performed and could not be included in the study.
The strength of this study is that it was a prospective study of new cases of OES in pediatric patients who had not undergone any type of treatment. In addition, the biopsy samples were analyzed by the same experienced pathologist and the same microscope that could have the same lighting configuration, object magnification levels, ocular lens system and image quality.
In conclusion, in this group of pediatric patients with OES in southern Brazil, the majority of patients has a high prevalence of histological, endoscopic and clinical response to treatment with PPIs.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Hospital Santa Casa de Porto Alegre (Ethic Committee number 44070821.9.0000.5683). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
LN: Writing – original draft, Writing – review & editing. ME: Supervision, Writing – review & editing. MC: Data curation, Formal Analysis, Writing – review & editing. CS: Project administration, Writing – review & editing. MM: Investigation, Writing – review & editing. Cd: Data curation, Writing – review & editing. CF: Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dellon ES, Liacouras CA, Molina-Infante JA, Furuta GT, Spergel JM, Zevit N, et al. Updated international consensus diagnostic criteria for eosinophilic esophagitis: proceedings of the AGREE conference. Gastroenterology. (2018) 155:1022–33.
2. Gutiérrez-Junquera C, Fernández-Fernández S, Cilleruelo ML, Rayo A, Echeverría L, Quevedo S, et al. High prevalence of response to proton-pump inhibitor treatment in children with esophageal eosinophilia. J Pediatr Gastroenterol Nutr. (2016) 62(5):704–10. doi: 10.1097/MPG.0000000000001019
3. Ferreira CT, Vieira MC, Furuta GT, de Barros FCLF, Chehade M. Eosinophilic esophagitis—where are we today? J Pediatr (Rio J). (2019) 95(3):275–81. doi: 10.1016/j.jpedp.2018.06.021
4. Queiros MC, Bandeira LA, de Souza AEF, de Paiva SF, Alcântara VS, Mouro MF, et al. A prevalência da esofagite eosinofílica no Brasil—uma revisão da literatura. Braz J Dev. (2023) 9(05):16867–76. doi: 10.34117/bjdv9n5-157
5. Greuter T, Hirano I, Dellon ES. Emerging therapies for eosinophilic esophagitis. J Allergy Clin Immunol. (2020) 145(1):38–45. doi: 10.1016/j.jaci.2019.10.027
6. Lee CJ, Dellon ES. Real-world efficacy of dupilumab in severe, treatment-refractory, and fibrostenotic patients with eosinophilic esophagitis. Clin Gastroenterol Hepatol. (2024) 22(2):252–8. doi: 10.1016/j.cgh.2023.08.015
7. Oliva S, Dias JA, Rea F, Malamisura M, Espinheira MC, Papadopoulou A, et al. Characterization of eosinophilic esophagitis from the European pediatric eosinophilic esophagitis registry (pEEr) of ESPGHAN. J Pediatr Gastroenterol Nutr. (2022) 75(3):325–33. doi: 10.1097/MPG.0000000000003530
8. Kliewer KL, Gonsalves N, Dellon ES, Katzka DA, Abonia JP, Aceves SS, et al. One Food versus Six Food Elimination Diet Therapy for Treatment of Eosinophilic Esophagitis: A 1 Multicenter Randomized Clinical Trial 2 (2023).
9. Hsu S, Wood C, Pan Z, Rahat H, Zeitler P, Fleischer D, et al. Adrenal insufficiency in pediatric eosinophilic esophagitis patients treated with swallowed topical steroids. Pediatr Allergy Immunol Pulmonol. (2017) 30(3):135–40. doi: 10.1089/ped.2017.0779
10. Hirano I, Chan ES, Rank MA, Sharaf RN, Stollman NH, Stukus DR, et al. AGA institute and the joint task force on allergy-immunology practice parameters clinical guidelines for the management of eosinophilic esophagitis. Gastroenterology. (2020) 158(6):1776–86. doi: 10.1053/j.gastro.2020.02.038
11. Franciosi JP, Mougey EB, Dellon ES, Gutierrez-Junquera C, Fernandez-Fernandez S, Venkatesh RD, et al. Proton pump inhibitor therapy for eosinophilic esophagitis: history, mechanisms, efficacy, and future directions. J Asthma Allergy. (2022) 15:281–302. doi: 10.2147/JAA.S274524
12. Gutiérrez-Junquera C, Fernández-Fernández S, Cilleruelo ML, Rayo A, Román E. The role of proton pump inhibitors in the management of pediatric eosinophilic esophagitis. Front Pediatr. (2018) 6(May):1–7. doi: 10.3389/fped.2018.00119
13. Hirano I, Furuta GT. Approaches and challenges to management of pediatric and adult patients with eosinophilic esophagitis. Gastroenterology. (2020) 158:840–51. doi: 10.1053/j.gastro.2019.09.052
14. Hirano I, Moy N, Heckman MG, Thomas CS, Gonsalves N, Achem SR. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: validation of a novel classification and grading system. Gut. (2013) 62(4):489–95. doi: 10.1136/gutjnl-2011-301817
15. Gutiérrez-Junquera C, Fernández-Fernández S, Domínguez-Ortega G, Vila Miravet V, García-Puig R, La Orden-Izquierdo E, et al. Proton pump inhibitor therapy in pediatric eosinophilic esophagitis: predictive factors and long-term step-down efficacy. J Pediatr Gastroenterol Nutr. (2023) 76(2):191–8. doi: 10.1097/MPG.0000000000003660
16. Gómez Torrijos E, Donado Palencia P, Sanchez Miranda MP, Moreno Lozano L, Extremera Ortega AM, Borja Segade JM, et al. Eosinophilic esophagitis: treatment with different doses of omeprazole in children under 16 years. J Investig Allergol Clin Immunol. (2018) 28:191–2. doi: 10.18176/jiaci.0230
17. Arias A, Pérez-Martínez I, Tenías JM, Lucendo AJ. Systematic review with meta-analysis: the incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment Pharmacol Ther. (2016) 43(1):3–15. doi: 10.1111/apt.13441
18. Rea F, Caldaro T, Tambucci R, Romeo EF, Caloisi C, Torroni F, et al. Eosinophilic esophagitis: is it also a surgical disease? J Pediatr Surg. (2013) 48(2):304–8. doi: 10.1016/j.jpedsurg.2012.11.006
19. Gutiérrez-Junquera C, Fernández-Fernández S, Cilleruelo ML, Rayo A, Echeverría L, Borrell B, et al. Long-term treatment with proton pump inhibitors is effective in children with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2018;67(2):210–6. doi: 10.1097/MPG.0000000000001952
20. Whelan KA, Godwin BC, Wilkins B, Elci OU, Benitez A, DeMarshall M, et al. Persistent basal cell hyperplasia is associated with clinical and endoscopic findings in patients with histologically inactive eosinophilic esophagitis. Clin Gastroenterol Hepatol. (2020) 18(7):1475–1482.1. doi: 10.1016/j.cgh.2019.08.055
21. Thakk KP, Philpott H, Lafata S, Fowler M, Keene S, Iuga A, et al. Effect of proton pump inhibitor treatment in “PPI non-responsive patients with eosinophilic esophagitis. J Gastrointestin Liver Dis. (2023) 32(1):15–22. doi: 10.15403/jgld-4746
22. Sayej WN, Patel R, Baker RD, Tron E, Baker SS. Treatment With High-Dose Proton Pump Inhibitors Helps Distinguish Eosinophilic Esophagitis From Noneosinophilic Esophagitis (2009).
23. Dranove JE, Horn DS, Davis MA, Kernek KM, Gupta SK. Predictors of response to proton pump inhibitor therapy among children with significant esophageal eosinophilia. J Pediatr. (2009) 154(1):96–100. doi: 10.1016/j.jpeds.2008.07.042
24. Laserna-Mendieta EJ, Casabona S, Guagnozzi D, Savarino E, Perelló A, Guardiola-Arévalo A, et al. Efficacy of proton pump inhibitor therapy for eosinophilic oesophagitis in 630 patients: results from the EoE connect registry. Aliment Pharmacol Ther. (2020) 52(5):798–807. doi: 10.1111/apt.15957
25. Molina-Infante J, Ferrando-Lamana L, Ripoll C, Hernandez-Alonso M, Mateos JM, Fernandez-Bermejo M, et al. Esophageal eosinophilic infiltration responds to proton pump inhibition in most adults. Clin Gastroenterol Hepatol. (2011) 9(2):110–7. doi: 10.1016/j.cgh.2010.09.019
26. Dellon ES, Speck O, Woodward K, Gebhart JH, Madanick RD, Levinson S, et al. Clinical and endoscopic characteristics do not reliably differentiate PPI-responsive esophageal eosinophilia and eosinophilic esophagitis in patients undergoing upper endoscopy: a prospective cohort study. Am J Gastroenterol. (2013) 108(12):1854–60. doi: 10.1038/ajg.2013.363
27. Moawad FJ, Schoepfer AM, Safroneeva E, Ally MR, Chen YJ, Maydonovitch CL, et al. Eosinophilic oesophagitis and proton pump inhibitor-responsive oesophageal eosinophilia have similar clinical, endoscopic and histological findings. Aliment Pharmacol Ther. (2014) 39(6):603–8. doi: 10.1111/apt.12636
28. Warners MJ, Van Rhijn BD, Curvers WL, Smout AJPM, Bredenoord AJ. PPI-responsive esophageal eosinophilia cannot be distinguished from eosinophilic esophagitis by endoscopic signs. Eur J Gastroenterol Hepatol. (2015) 27(5):506–11. doi: 10.1097/MEG.0000000000000331
Keywords: proton-pump inhibitor responsive esophageal eosinophilia, eosinophilic esophagitis, children, proton-pump inhibitor, histological remission
Citation: Nader LS, Epifanio M, Coelho MG, Steinhaus C, Melere M, da Silva CS and Ferreira CT (2024) High prevalence of response to PPI treatment in children and adolescents with eosinophilic esophagitis in southern Brazil. Front. Allergy 5:1346843. doi: 10.3389/falgy.2024.1346843
Received: 30 November 2023; Accepted: 21 March 2024;
Published: 8 April 2024.
Edited by:
Amanda Muir, Children’s Hospital of Philadelphia, United StatesReviewed by:
Nurit P. Azouz, Cincinnati Children’s Hospital Medical Center, United States© 2024 Nader, Epifanio, Coelho, Steinhaus, Melere, da Silva and Ferreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luiza Salgado Nader bHVpemFzbmFkZXJAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.