 Ramiro Soria1
Ramiro Soria1 Mónica Del Compare2
Mónica Del Compare2 Marisa Sallaberry3
Marisa Sallaberry3 Graciela Martín4
Graciela Martín4 Gustavo Aprigliano5
Gustavo Aprigliano5 Verónica Hermida6
Verónica Hermida6 Mabel Carosella7
Mabel Carosella7 Martín Gruenberg8
Martín Gruenberg8 Silvana Monsell8
Silvana Monsell8 Paula Micone9
Paula Micone9 Eugenia Maciero7
Eugenia Maciero7 Norberto Giglio7*
Norberto Giglio7*
- 1Sanatorio Infantil San Lucas, San Miguel de Tucumán, Tucumán, Argentina
- 2Consultorios Externos Sanatorio Mater Dei, Ciudad Autónoma de Buenos Aires, Argentina
- 3Pediatras de Uriburu, Ciudad Autónoma de Buenos Aires, Argentina
- 4Clínica del Niño y Consultorios de Especialistas, Corrientes, Argentina
- 5Consultorio Pediátrico Urquiza, Ciudad Autónoma de Buenos Aires, Argentina
- 6Consultorios Neuropediatría Barracas, Ciudad Autónoma de Buenos Aires, Argentina
- 7Grupo Pediátrico Belgrano R, Ciudad Autónoma de Buenos Aires, Argentina
- 8Consultorio Privado, Ciudad Autónoma de Buenos Aires, Argentina
- 9Servicio de Tocoginecología, Hospital Durand, Ciudad Autónoma de Buenos Aires, Argentina
Introduction: Cow's milk protein allergy (CMPA) is the most frequent food allergy in early childhood. For those infants requiring breastmilk substitutes, formulas with extensively hydrolyzed proteins (EHF), should be the treatment of choice. As there are limited data showing the progression of initial symptoms in infants newly diagnosed with CMPA who are treated with EHF with added synbiotics, the main objective of this study was to evaluate the resolution of symptoms in said infants after 4 weeks of treatment. As a secondary objective this study aimed to assess the impact of the treatment on the family's quality of life.
Materials and Methods: observational, longitudinal, prospective, and multicentric real-world evidence study. The intervention phase (EHF with synbiotics) lasted 28 days and was completed by 65 patients. Treating physicians registered child´s anthropometry, Infant Gastrointestinal Symptoms Questionnaire (IGSQ-13) and CoMiSS (Cow´s Milk Allergy Symptoms Score) both at baseline and after 28 days of treatment. During treatment, caregivers reported child´s regurgitation and stools, PO-SCORAD (Patient Oriented Scoring of Atopic Dermatitis) and FAQL-PB (Family Quality of Life—Parental Burden). Data were collected using Google Forms and analyzed through the STATA program.
Results: 95.4% of the patients showed an improvement or disappearance of the overall initial symptoms after 4 weeks of treatment. Gastrointestinal symptoms improved or disappeared in 92% of patients (p < 0.05) while dermatological symptoms improved or disappeared in 87.5% of patients (p < 0.05). The median CoMiSS at baseline was 9, with 21 patients exceeding the cut-off point of 12. After 4 weeks of treatment, the median dropped to 3, and no patient exceeded the 12-cut-off point (p = 0.000). At baseline, patients had a PO-SCORAD of 11.5 (interquartile range 1–23) that went to 1.0 (interquartile range 1–6) at day 28 (p = 0.000). The treatment diminished stool frequency (p < 0.05), improved stool consistency (p = 0.004) and decreased the frequency of regurgitation in infants with CMPA (p = 0.01). The percentage of patients who no longer had any episode of regurgitation increased from 11% to 31% on day 28 (p = 0.003). At baseline, 13% of patients cried more than 3 h per day, while at day 28 that percentage dropped to 3% (p = 0.03). An improvement in the infants' sleep pattern was also appreciated with the treatment. At study onset, 56% of the families reported feeling very overwhelmed, a percentage that dropped to 17% after 28 days of treatment (p < 0.05). The small percentage of families who did not feel overwhelmed at study onset (17%), grew to 43% on day 28 (p < 0.05).
Conclusions: The use of an EHF with synbiotics for the management of infants diagnosed with or suspected to have CMPA suggested a good safety profile, an adequate infant growth, and improvement of overall, gastrointestinal, and dermatological symptoms. It also suggested a lower daily frequency of regurgitations and stools, and an improvement in stool consistency, sleeping pattern, and quality of life of the infant and his family.
1. Introduction
Food allergies are a frequent consultation in pediatrics and one of the most frequent in early childhood is cow's milk protein allergy (CMPA) (1, 2). The diagnosis of CMPA tripled in the last decade, with a prevalence reported between 1.8 and 7.5% (1, 3, 4).
Breastfeeding is the most complete alternative for infants with CMPA to adequately grow and develop, with a milk protein elimination diet being the treatment of choice for the control of clinical manifestations (4). If the infant requires breastmilk substitutes, a hypoallergenic formula should be given. These can be formulas with extensively hydrolyzed proteins (EHF), or elemental formulas based on free amino acids (AAF). EHF are the first-line treatment for mild and moderate forms of CMPA (4).
As it has been shown that an alteration of the intestinal microbiota is involved in the development of CMPA (5–7), in recent years, this dietary management has gone from being passive (elimination diet to alleviate symptoms) to being proactive, using prebiotics, probiotics and synbiotics that can actively modulate the immunological system through the microbiota (8–10). It has recently been reported that the use of hypoallergenic formulas with specific synbiotics resulted in a sustained improvement in gut microbiota composition (11).
Finally, it is important to consider that, beyond its clinical symptoms, CMPA implies a much broader burden, ranging from a decrease in the quality of life of families and infants with this condition (12) to a significant economic burden on health systems (13).
For all the above reasons, the main objective of this study is to evaluate the progression of symptoms in infants diagnosed with or suspected to have CMPA after 4 weeks of treatment with an EHF with synbiotics. As secondary objectives, the study intends to evaluate the impact of treatment on the family's quality of life after 4 weeks of treatment and to describe the use of health resources up to one year of life.
2. Materials and methods
2.1. Study design
Observational, longitudinal, prospective, and multicenter real-world evidence (RWE) study. The intervention phase (single arm) lasted 28 days. To obtain data on the use of healthcare resources up to one year of life, an analysis of medical records (hospital visits, infections, medications used) was performed when the individuals reached one year of age. The study was conducted between June 2021 and December 2022 in 10 sites of 3 regions in Argentina. The approval of the Independent Ethics Committee for Trials in Clinical Pharmacology of the Foundation for Pharmacological and Drug Studies (FEFYM) “Luis María Zieher” was obtained. The study was conducted in accordance with Good Clinical Practices and the Declaration of Helsinki. The parents of all recruited patients signed a written informed consent.
2.2. Population
Infants with presumptive or confirmed diagnosis of CMPA, who had, as their first indication, an EHF for a minimum period of 28 days. The EHF used in this study was Nutrilon Pepti Syneo® (Nutricia, the Netherlands), a nutritionally complete food for specific medical purposes with hydrolyzed whey protein, long-chain fatty acids and synbiotics (GOSsc/FOSlc and Bifidobacterim breve M-16V), intended for the dietary management of CMPA in infants from birth, either as a sole source of nutrition or as a supplement to breastfeeding and/or complementary foods. The initial evaluation and subsequent follow-up of each participant was performed according to the usual practices for patients with suspected CMPA.
2.3. Inclusion and exclusion criteria
Patients with presumptive or confirmed diagnosis of CMPA who were less than or equal to 8 months of age, with parents already feeding their child with formula, were included. Infants who had already been previously fed hypoallergenic formulas, who suffered from severe CMPA thus requiring an AAF, or who had contraindications for consuming synbiotics (short bowel, parenteral nutrition, post pyloric feeding, central venous catheter and/or immunocompromised infants) were excluded. For follow-up at one year of life, all infants who had completed the 28 days of initial treatment were included. Children who subsequently required an AAF and those for whom data could not be extracted from medical records were excluded from this analysis.
2.4. Data collection and statistical analysis
For data collection, Infant Gastrointestinal Symptoms Questionnaire (IGSQ-13) (14) and Cow's Milk Allergy Symptoms Score (CoMiSS) (3) had to be completed by the treating physicians, while Patient Oriented Scoring Atopic Dermatitis (PO-SCORAD) (15) and Family Quality of Life—Parental Burden questionnaire (FAQL-PB) (16) had to be completed by the patient's families.
2.4.1. CoMiSS
The CoMiSS assesses 5 clinical domains (crying, regurgitation, stools, respiratory symptoms, and skin signs), with total scores ranging from 0 to 33 (3). A score of 5 is considered normal in healthy infants under 6 months of age (17).
2.4.2. IGSQ-13
The 13-item IGSQ index score assesses infants' GI-related signs and symptoms observed by parents over the previous week in 5 domains: stooling, spitting up/vomiting, flatulence, crying, and fussiness. Items were scored on a scale of 1–5, with higher values indicating greater GI distress. The total IGSQ score was calculated by summing item responses. Thus, the possible range in scores was 13–65, where a score of 13 indicated no GI distress at all and a score of 65 represented extreme GI distress (14). In addition, daily stool frequency and stool consistency (Brussels Infant and Toddler Stool Scale) were also recorded at the same time points (18).
2.4.3. PO-SCORAD
This tool rates severity (from none to extreme) of dryness, erythema, edema, oozing, scratches, skin thickening, as well as indicating sleep quality and crying frequency on visual analog scales (ranging from 0 [none] to 10 [unbearable]). The numeric value from the tool indicates a score ranging from 0 (no skin affected and no symptoms) to 103 (entire body affected and extreme symptoms) (15).
2.4.4. FAQL-PB
The FAQL-PB Scale is a 17-item instrument. It utilizes a 7-point Likert scale ranging from 1 (not troubled) to 7 (extremely troubled). Questions include issues concerning going on vacation, social activities and worries and anxieties over the previous week. The number circled for each question is summed to provide a total continuous score with a higher score indicating greater burden on the family. Scores can range from 17 to 119 (16).
2.4.5. Use of health resources
To obtain data on the use of health care resources up to one year of life, an analysis of medical records (hospital visits, infections, medication use) was performed when the individuals reached one year of age.
2.4.6. Statistical análisis
Data were collected using Google Forms and analyzed through the STATA program. The detail of the study design can be seen in Figure 1. Data were described as frequency and percentage, for categorical variables. For numerical variables, mean and standard deviations were used for normal distributions while median and interquartile interval were used for non-normal distributions. To assess the differences from baseline, comparisons were made using Wilcoxon signed rank test for continuous variables with nonparametric distribution and χ2 test for categorical variables. Statistically significant differences were considered to exist when the p-value was less than 0.05 (p < 0.05).
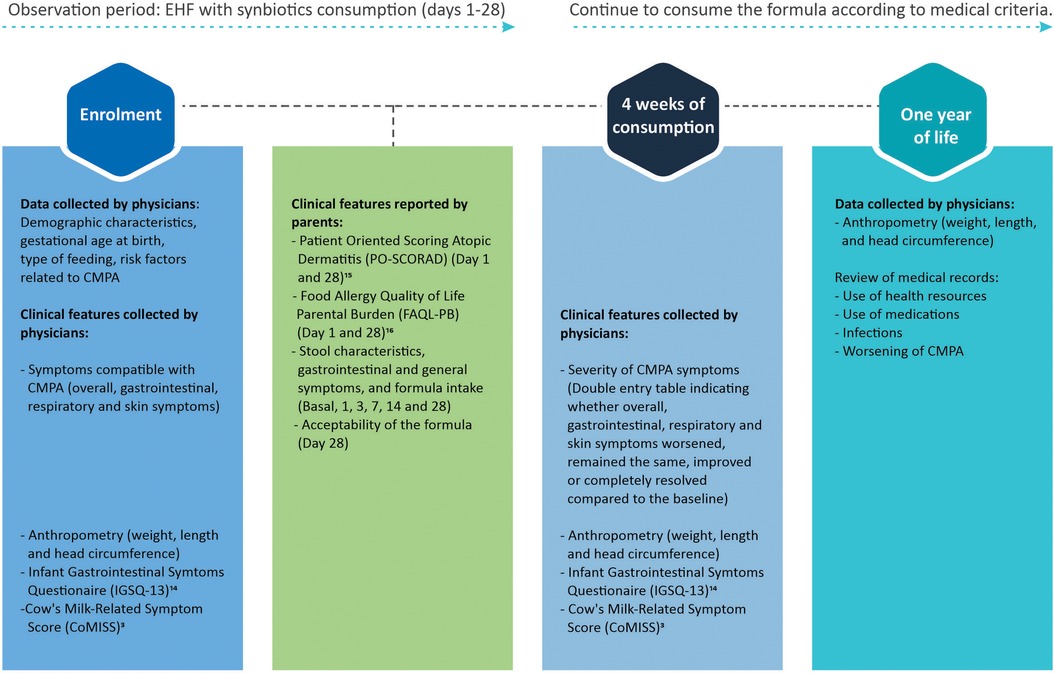
Figure 1. Study design.
3. Results
The 28-day treatment with an EHF with synbiotics was completed by 65 patients. In 59 of them, data regarding the use of healthcare resources could be collected at one year of life. The recruitment flow can be seen in Figure 2.
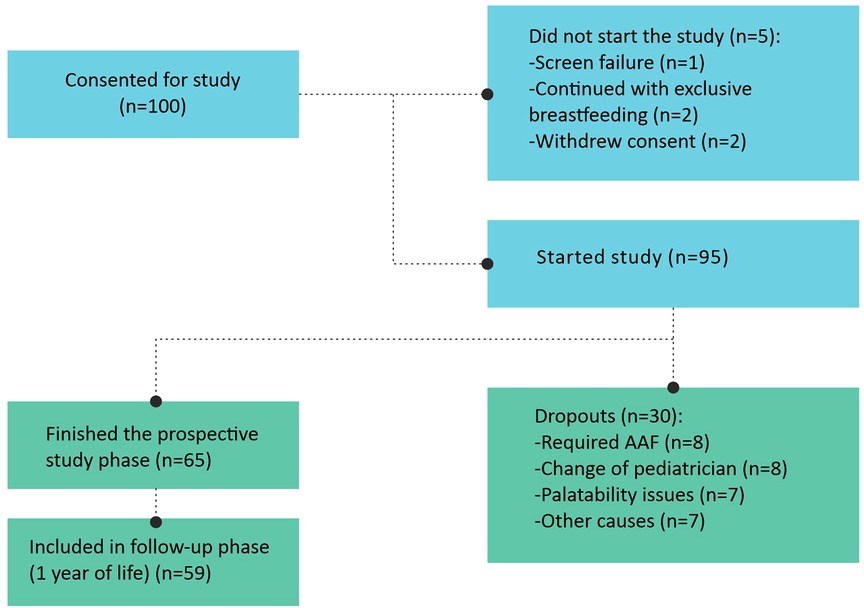
Figure 2. Recruitment flow.
Demographic characteristics of the population, route of delivery, type of feeding at study onset and family history of atopy are shown in Table 1.
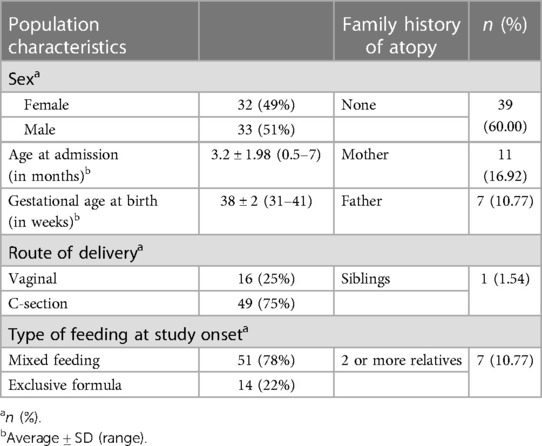
Table 1. On the left: demographic characteristics of the population, route of delivery and type of feeding at study onset. On the right: family history of atopy (n = 65).
3.1. Main outcome: clinical efficacy and symptoms resolution after 28 days of treatment with an EHF with synbiotics
At baseline, 96.8% of the infants presented gastrointestinal symptoms (60% along with dermatological symptoms, 16.9% with respiratory symptoms, 9.2% with both dermatological and respiratory symptoms, and 10.7% presenting exclusively gastrointestinal symptoms). The remaining 3.2% presented dermatological and respiratory symptoms.
The progression of these symptoms after 4 weeks of treatment with an EHF with synbiotics is shown in Table 2.
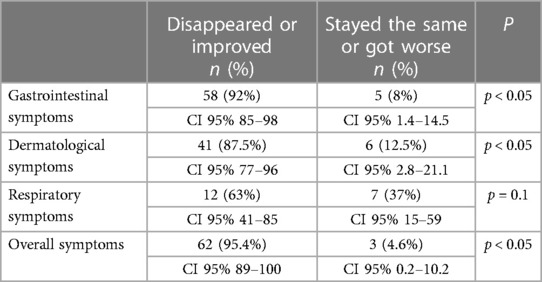
Table 2. Symptoms progression after 28 days of treatment with an EHF with synbiotics (n = 65).
At baseline, 21 patients showed a CoMiSS greater than or equal to 12. At the end of the treatment, no patient exceeded it. Figure 3A shows that the median CoMiSS at study onset was 9, decreasing significantly to 3 with treatment (p = 0.000).
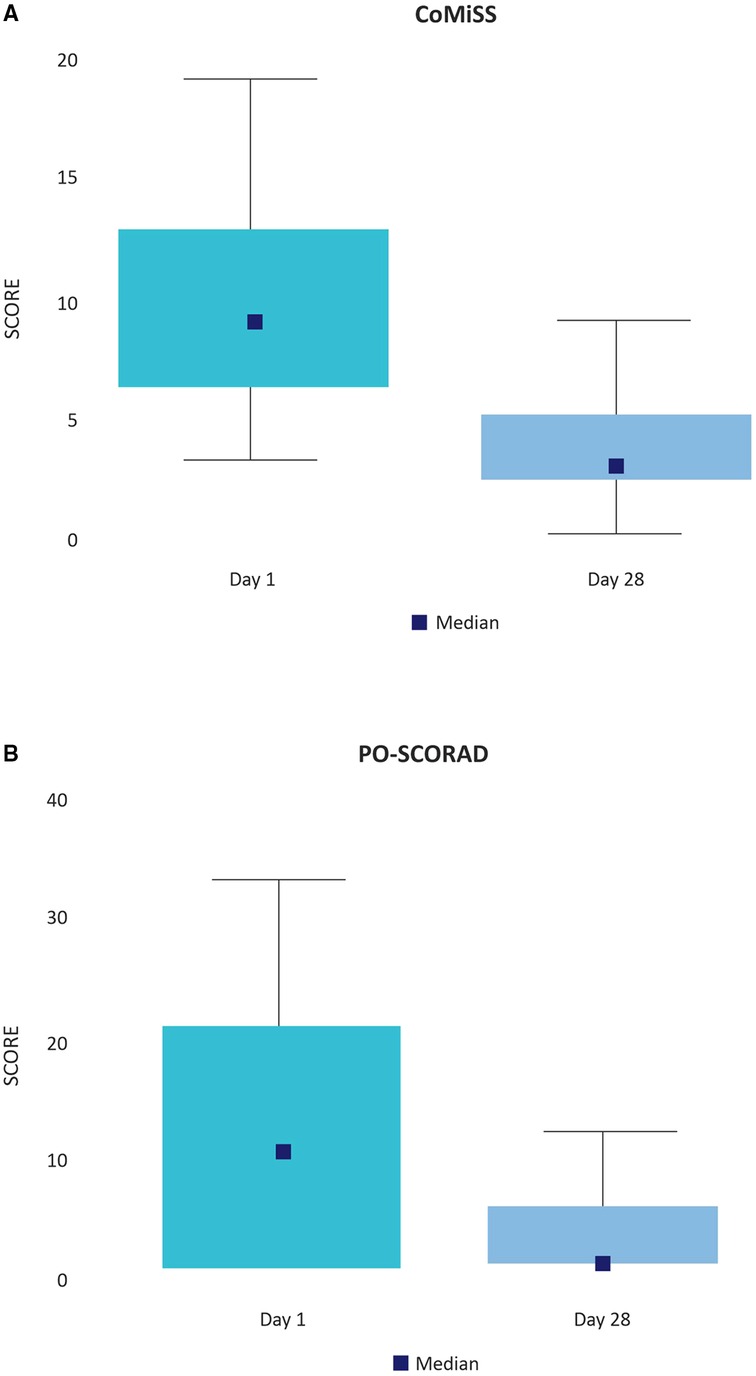
Figure 3. (A) CoMiSS (days 1 and 28). Data collected by physicians. (B) PO-SCORAD (days 1 and 28). Data collected by caregivers.
Patients included in the study had mild eczema, judging by a median PO-SCORAD at baseline of 11.5 (Interquartile range 1–23). With the treatment the median PO-SCORAD dropped to 1.0 (Interquartile range 1–6) on day 28 (p = 0.000) (Figure 3B).
3.2. Secondary outcome: the infant's and the family's life quality
Figure 4 shows the changes in infants' stools and regurgitation with treatment, as well as the impact of these modifications on the quality of life of their caregivers. The percentage of infants with more than 5 daily stools decreased throughout treatment between day 1 and day 28 (p < 0.05) (Figure 4A). Regarding consistency, 28% of parents reported watery stools on day 1, decreasing to 10% on day 28 (p = 0.004) (Figure 4B).
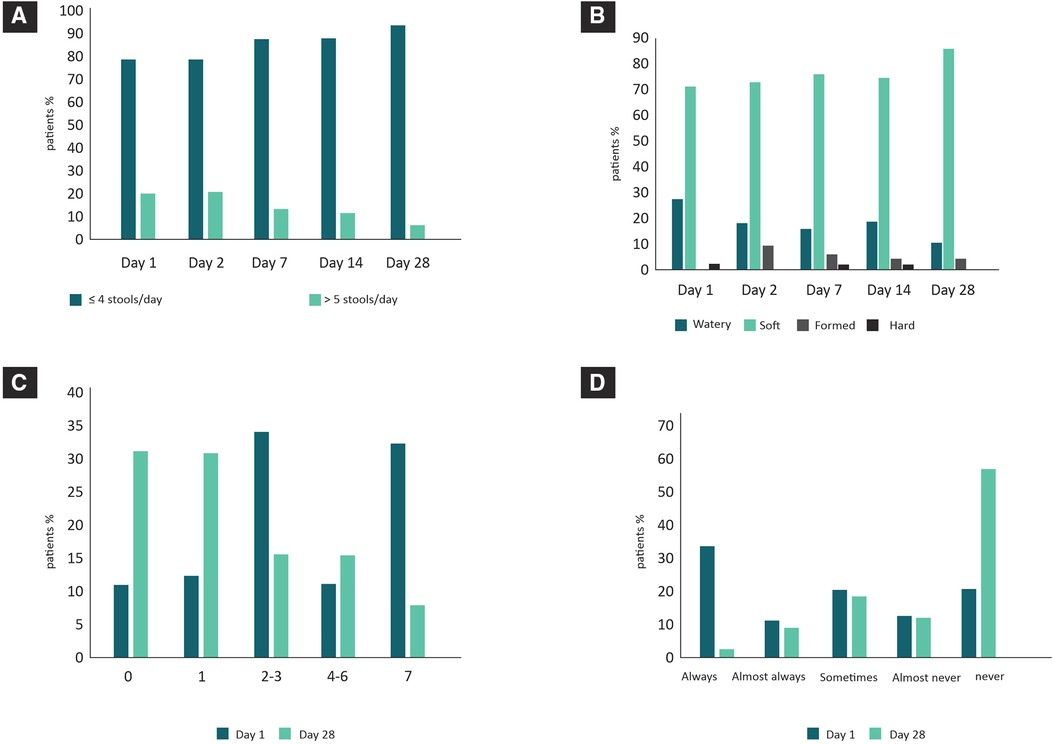
Figure 4. Changes in infants' stools and regurgitation with treatment (data collected by caregivers). (A) Stool frequency during treatment. (B) Stool consistency during treatment. (C) Number of daily regurgitations (days 1 and 28). (D) Frequency of infants' discomfort that was attributed to regurgitation by their caregivers (days 1 and 28).
Figure 4C shows that on day 1, 43% of patients had 4 or more daily regurgitations. After 28 days of treatment, this percentage dropped to 22% (p = 0.01). Within this group, the percentage of patients who had more than 7 regurgitations per day changed from 32% at baseline to only 7% on day 28 (p = 0.0003). The percentage of patients who no longer had any episodes increased from 11% (day 1) to 31% on day 28 (p = 0.003).
Consistent with the above data, 34% of parents reported that their children “were always uncomfortable due to regurgitation” at the beginning of treatment, a percentage that dropped to 2% on day 28 (p = 0.000). On the other hand, only 20% reported not being uncomfortable on day 1, while 58% reported that they never felt uncomfortable on day 28 (p = 0.000) (Figure 4D).
Other relevant aspects for the quality of life of infants and their caregivers are those related to sleeping and crying. At baseline, 13% of patients cried more than 3 h per day, while on day 28 that percentage dropped to 3% (p = 0.03). Children who, according to their parents, did not cry due to irritability changed from 31% at baseline to 49% on day 28 (p = 0.03). Likewise, an improvement in the infants' sleeping pattern was appreciated with the treatment (not shown).
Table 3 shows the impact on the family's quality of life that represents an infant with CMPA and how it improves significantly with treatment. At study onset, 56% of the families reported feeling very overwhelmed, a percentage that dropped to 17% after 28 days of treatment (P < 0.05). The small percentage of families that did not feel overwhelmed at study onset (17%) grew to 43% on day 28 (p < 0.05).
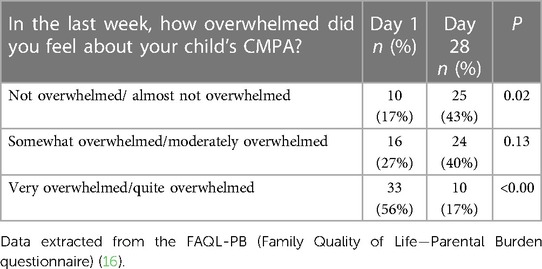
Table 3. Impact of CMPA and its treatment with an EHF with synbiotics in the patient's family quality of life (n = 59).
The median FAQL-PB score at baseline was 49 (Interquartile range 27–64), dropping to 30 (Interquartile range 18–54) with the treatment on day 28 (p = 0.02).
3.3. Secondary outcome: use of healthcare resources up to one year of life
More than half of the infants (52%) did not require any consultation to the emergency service until one year of life, while only 6 infants (10.17%) required more than 5 consultations. Of these, 2 patients had to be hospitalized for reasons unrelated to their CMPA.
42.3% of the infants did not require pharmacological medication during follow-up. Only 12% (7 patients) required additional drug treatment for their allergic symptoms, 34% used analgesics and/or antipyretics, and 24% required antibiotics.
Less than half of the infants (n = 29; 49%) presented at least one infectious condition: 2 presented gastrointestinal infections, 18 presented respiratory infections, 3 a combination of both, and 6 patients presented other infections.
3.4. Other relevant aspects
When establishing a nutritional treatment for CMPA it is also important to demonstrate an appropriate infant growth and to ensure a proper compliance with the treatment.
All the subjects included in this study presented anthropometric measures (height, weight, and head circumference) within the WHO growth chart percentiles for their sex and age. The average anthropometric measures can be seen in Supplementary Table S1.
Considering some issues of daily family management that contribute to treatment compliance, 98.5% of the caregivers found it easy to prepare the formula, and the acceptance by the infants was 69%. According to the appreciation of the caregivers, 66% of the infants seemed to enjoy it (not shown).
4. Discussion
4.1. Demographic characteristics, family history of atopy, type of delivery and feeding
The mean age of patients who entered the study with a diagnosis or suspicion of CMPA agrees with international (10) and local (19) reports. It is known that food allergy is a complex immune disorder caused by specific genetic variants in combination with environmental and nutritional exposures (20). In this context, both the high rate of C-section and the low rate of exclusive breastfeeding appreciated in our sample have been shown to interfere with the homeostasis of the intestinal microbiota and to be determinants of dysbiosis (21, 22), which is considered one of the main responsible for the increasing incidence of allergic disorders (23–25). The family history of atopy present in the recruited infants is also a risk factor associated with CMPA. It is known that the existence of a history of atopy in a sibling increases the risk of allergic disease by 25%–30%, in one parent increases it by 20%–40% and in both parents by 40%–60% (26, 27).
4.2. Main outcome: clinical efficacy and symptoms resolution after 28 days of treatment with an EHF with synbiotics
More than 95% of the infants showed complete improvement or resolution of CMPA symptoms with treatment, confirming the previously reported efficacy of the formula (10). Although 92% of the gastrointestinal symptoms and 87.5% of the dermatological symptoms evolved favorably, only 63% of the respiratory symptoms showed this positive outcome. From an epidemiological point of view, as the study was conducted during autumn and winter, an increase in respiratory symptoms not associated with CMPA but with seasonal viruses may have been appreciated. This is partially confirmed by the results of nasopharyngeal swabs that showed the presence of respiratory syncytial virus in some infants.
The treatment efficacy is also evidenced by the improvement of both the CoMiSS (captured by treating physicians) and the PO-SCORAD (captured by caregivers). Previous reports have shown similar results in infants with CMPA receiving an EHF with GOS, FOS and Bifidobacterium breve M-16V (10, 28, 29).
A multicenter, double-blind, placebo-controlled study, in which 90 exclusively formula-fed infants with atopic dermatitis were randomly assigned to receive an EHF with or without synbiotics for 12 weeks, showed that both treatments improved atopic dermatitis, as assessed by the SCORAD index. Although no significant differences were observed between the consumption of an EHF with or without synbiotics in the subgroup of patients with non-IgE-mediated atopic dermatitis, the differences were significant in favor of the consumption of EHF with synbiotics in the subgroup of patients with IgE-mediated atopic dermatitis (28).
On the other hand, it has also been reported that the treatment with EHF with synbiotics enhanced the management of infants with non-IgE-mediated CMPA who were already established on EHF without synbiotics, showing a significant improvement in atopic dermatitis in those patients with severe baseline symptoms (PO-SCORAD reduction from 34.7 to 18.2) (10).
4.3. Secondary outcome: the infant's and the family's quality of life
Parents or caregivers of infants with food allergies reported a lower quality of life, due to the social and emotional impact they suffer, and referred high levels of anxiety and stress (30). In our study, parents reported an improvement in their quality of life after 28 days of receiving an EHF with synbiotics. This is in line with was previously reported by Hubbard et al., who also showed a significant reduction in the FAQL-PB score between baseline (mean 30.9) and after 4 weeks of treatment with an EHF with synbiotics (mean 22.6) (10).
Non-IgE-mediated CMPA can present a wide range of gastrointestinal manifestations, including vomiting, regurgitation, or diarrhea (31). Although a randomized clinical trial comparing the consumption of an EHF with and without synbiotics showed that stool consistency was significantly softer in the group that consumed the formula with synbiotics without finding significant differences in relation to stool frequency (28), our results showed that a 28-day treatment with an EHF with synbiotics significantly improved stool consistency but also decreased the number of daily regurgitations and stools. These results were in accordance with the perception of caregivers, who reported that the discomfort that these symptoms generated before treatment decreased substantially after treatment, indicating a substantial improvement in both infants and caregivers' quality of life. For the correct interpretation of these results, it is important to consider two aspects: time and feeding. On the one hand, at least partially, the improvement of these symptoms could have occurred just over time and could not be completely attributed to the treatment. On the other hand, both the frequency and consistency of stools also depended on whether the patient is being breastfed or not. In the present study, we were unable to carry out a subgroup analysis to specify whether the decrease in the frequency and consistency of stools is seen differentially in those infants of mothers who feed their children with breast milk and formula or exclusively with formula.
Other aspects that substantially modified the infant's and the family's quality of life were the sleeping pattern and the crying attributed to irritability. There is a close relationship between food allergy and sleep disorders; an association that has increased in recent times (32). Our data indicated an improvement in the sleeping pattern of infants with CMPA after treatment, reflected both in the increase of those patients who reached what caregivers consider a normal pattern and in the lower percentage of patients with nocturnal awakenings.
Regarding inconsolable paroxysmal crying, it can often be a sign of an underlying medical condition and it may be the first manifestation of a food allergy (33). In our study, the positive evolution of CMPA symptoms led to a significant improvement in the irritability of infants, which was reflected in the decrease in the number of hours of crying after treatment and in the decrease in the crying perceived by parents as related to irritability.
4.4. Secondary outcome: use of healthcare resources up to one year of life
Given that the EHF evaluated in the present study has as a distinctive characteristic the addition of synbiotics with potential modulating effect on the immune system (7), and since the management of an infant with CMPA represents a significant burden for the health system in terms of the use of health resources and medical consultations (10), our study evaluated the patient's medical records at one year of life to describe the number of hospital visits, infections and medication used.
In a recent study, hospital visits and prescriptions of medications were collected from hospital medical records and caregivers, during the 6-months before, and 6-months after EHF with synbiotics treatment initiation. In said study, significant reductions in the mean number of overall hospital visits required by infants were observed in the 6 months after the treatment with EHF with synbiotics. The authors also showed a significant decrease in prescriptions for gastrointestinal conditions (46.2% vs. 7.7% before and after EHF with synbiotics, respectively) (10) which impresses to be in line with our report where only 6.9% of the patients suffered from gastrointestinal infections up to one year of life. Taking these results into account, the low use of healthcare resources observed in our study could also be due to an improvement in the species balance of the intestinal microbiota of patients who received synbiotics which has been previously described (10). It is worth noting that this is only a hypothesis as our study, being a RWE study and not a randomized controlled trial, lacks a control group.
Despite this important limitation, the data obtained in our study together with contributions such as those of Hubbard et al. (10) can help to understand the role of synbiotics in the management of CMPA through changes in the composition of their intestinal microbiota that bring it closer to that of a healthy child.
4.5. Preparation and acceptance of an EHF with synbiotics
Although the study had some palatability-related dropouts, a high percentage of infants entering the study protocol appeared to enjoy consuming the formula, as reported by their caregivers. This better palatability of the EHF used in this study may be since it contains whey proteins and lactose, which would result in better palatability than formulas with casein and without lactose (34).
Both an easy preparation and acceptance of an EHF by infants have been reported in the present study and are essential to achieve a good adherence to treatment (35).
4.6. Strengths and weaknesses of the present study
The main strength of the study was to be one of the first reports to evaluate the progression of CMPA symptoms treated with an EHF with synbiotics, in a real world setting with a significant sample.
One of the limitations of this study was the relatively high dropout rate, mainly for three reasons: change of treating physician, palatability, or AAF requirement. In relation to palatability, it is important to consider that, since one of the exclusion criteria for the study was having previously consumed hypoallergenic formulas, all the children who entered the protocol had been exclusively breastfed or consuming infant formulas, both more palatable options than an EHF. On the other hand, since those patients who required the consumption of AAF were excluded from the analysis (selective dropout), the results of the study may be slightly affected by attrition bias. Another limitation of the study is that the initial diagnosis of CMPA was based on the clinical judgment of the treating physician, without necessarily being confirmed by a diagnostic oral food challenge. Finally, other weaknesses of the study are that, as being a RWE study, lacks a control group and that its results cannot be extrapolated to other types of synbiotic combinations, as the results are specific for the GOS/FOS and Bifidobacterium breve M-16V combination.
5. Conclusions
In this study, the use of an EHF with synbiotics for the management of infants diagnosed with or suspected to have CMPA suggested a good safety profile, an adequate infant growth, and improvement of overall, gastrointestinal, and dermatological symptoms. It also suggested a lower daily frequency of regurgitations and stools, and an improvement in stool consistency, sleeping pattern, and the infant's and the family's quality of life.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Independent Ethics Committee for Trials in Clinical Pharmacology of the Foundation for Pharmacological and Drug Studies (FEFYM) “Luis María Zieher”. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
ME: Methodology, Project administration, Software, Supervision, Writing – review & editing. GN: Conceptualization, Investigation, Resources, Writing – original draft, Writing – review & editing. SR: Investigation, Validation, Writing – review & editing. DCM: Investigation, Validation, Writing – review & editing. SM: Investigation, Validation, Writing – review & editing. MG: Investigation, Validation, Writing – review & editing. MG: Investigation, Validation, Writing – review & editing. AG: Investigation, Validation, Writing – review & editing. HV: Investigation, Validation, Writing – review & editing. CM: Investigation, Validation, Writing – review & editing. GM: Investigation, Validation, Writing – review & editing. MS: Investigation, Validation, Writing – review & editing. MP: Formal analysis, Methodology, Writing, review and editing.
Acknowledgments
We acknowledge Paula Mizrahi, our dedicated Center Coordinator, for her invaluable contribution to our research endeavors and her empathetic care for the study participants.
Conflict of interest
Unrestricted grant was provided by Nutricia Bago to support this research study. It is important to note that Nutricia Bago had no involvement or influence in the study design, data collection, analysis, interpretation, or the decision to publish the findings. We declare no conflicting interests that could compromise the integrity, objectivity, or impartiality of the study.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/falgy.2023.1265083/full#supplementary-material
References
1. Høst A. Frequency of cow’s milk allergy in childhood. Ann Allergy Asthma Immunol. (2002) 89(6):33–7. doi: 10.1016/S1081-1206(10)62120-5
2. Zepeda-Ortega B, Goh A, Xepapadaki P, Sprikkelman A, Nicolaou N, Hernandez REH, et al. Strategies and future opportunities for the prevention, diagnosis, and management of cow milk allergy. Front Immunol. (2021) 12. doi: 10.3389/fimmu.2021.608372
3. Vandenplas Y, Dupont C, Eigenmann P, Host A, Kuitunen M, Ribes-Koninckx C, et al. A workshop report on the development of the cow’s milk-related symptom score awareness tool for young children. Acta Paediatr. (2015) 104(4):334–9. doi: 10.1111/apa.12902
4. Toca MC, Morais MB, Vázquez-Frias R, Becker-Cuevas DJ, Boggio-Marzet CG, Delgado-Carbajal L, et al. Consensus on the diagnosis and treatment of cow’s milk protein allergy of the Latin American society for pediatric gastroenterology, hepatology and nutrition. Rev Gastroenterol Mex (Engl Ed). (2022) 87(2):235–50. doi: 10.1016/j.rgmxen.2022.01.002
5. Gholizadeh P, Mahallei M, Pormohammad A, Varshochi M, Ganbarov K, Zeinalzadeh E, et al. Microbial balance in the intestinal microbiota and its association with diabetes, obesity and allergic disease. Microb Pathog. (2019) 127:48–55. doi: 10.1016/j.micpath.2018.11.031
6. Mennini M, Reddel S, Del Chierico F, Gardini S, Quagliariello A, Vernocchi P, et al. Gut Microbiota profile in children with IgE-mediated cow’s milk allergy and cow’s milk sensitization and probiotic intestinal persistence evaluation. Int J Mol Sci. (2021) 22(4):1649. doi: 10.3390/ijms22041649
7. Cukrowska B, Bierła JB, Zakrzewska M, Klukowski M, Maciorkowska E. The relationship between the infant gut Microbiota and allergy. The role of Bifidobacterium breve and prebiotic oligosaccharides in the activation of anti-allergic mechanisms in early life. Nutrients. (2020) 12(4):946. doi: 10.3390/nu12040946
8. D’Auria E, Salvatore S, Pozzi E, Mantegazza C, Sartorio MUA, Pensabene L, et al. Cow’s milk allergy: immunomodulation by dietary intervention. Nutrients. (2019) 11(6):1399. doi: 10.3390/nu11061399
9. Kukkonen K, Savilahti E, Haahtela T, Juntunen-Backman K, Korpela R, Poussa T, et al. Long-term safety and impact on infection rates of postnatal probiotic and prebiotic (synbiotic) treatment: randomized, double-blind, placebo-controlled trial. Pediatrics. (2008) 122(1):8–12. doi: 10.1542/peds.2007-1192
10. Hubbard GP, Atwal K, Graham L, Narayanan S, Cooke L, Casewell C, et al. Synbiotic containing extensively hydrolyzed formula improves gastrointestinal and atopic symptom severity, growth, caregiver quality of life, and hospital-related healthcare use in infants with cow’s milk allergy. Immun Inflamm Dis. (2022) 10(6). doi: 10.1002/iid3.636
11. Fox AT, Wopereis H, Van Ampting MTJ, Oude Nijhuis MM, Butt AM, Peroni DG, et al. A specific synbiotic-containing amino acid-based formula in dietary management of cow’s milk allergy: a randomized controlled trial. Clin Transl Allergy. (2019) 9(1). doi: 10.1186/s13601-019-0241-3
12. Valentine AZ, Knibb RC. Exploring quality of life in families of children living with and without a severe food allergy. Appetite. (2011) 57(2):467–74. doi: 10.1016/j.appet.2011.06.007
13. Berktas M, Kirbiyik F, Aribal E, Aksit A, Altintas DU. Treatment options for cow’s milk protein allergy: a modeling analysis. Clinicoecon Outcomes Res. (2020) 12:307–15. doi: 10.2147/CEOR.S242021
14. Riley AW, Trabulsi J, Yao M, Bevans KB, DeRusso PA. Validation of a parent report questionnaire. Clin Pediatr (Phila). (2015) 54(12):1167–74. doi: 10.1177/0009922815574075
15. Stalder JF, Barbarot S, Wollenberg A, Holm EA, De Raeve L, Seidenari S, et al. Patient-oriented SCORAD (PO-SCORAD): a new self-assessment scale in atopic dermatitis validated in Europe. Allergy. (2011) 66(8):1114–21. doi: 10.1111/j.1398-9995.2011.02577.x
16. Knibb RC, Stalker C. Validation of the food allergy quality of life—parental burden questionnaire in the UK. Qual Life Res. (2013) 22(7):1841–9. doi: 10.1007/s11136-012-0295-3
17. Vandenplas Y, Salvatore S, Ribes-Koninckx C, Carvajal E, Szajewska H, Huysentruyt K. The cow milk symptom score (CoMiSSTM) in presumed healthy infants. PLoS One. (2018) 13(7):e0200603. doi: 10.1371/journal.pone.0200603
18. Huysentruyt K, Koppen I, Benninga M, Cattaert T, Cheng J, De Geyter C, et al. The Brussels infant and toddler stool scale: a study on interobserver reliability. J Pediatr Gastroenterol Nutr. (2019) 68(2):207–13. doi: 10.1097/MPG.0000000000002153
19. Mehaudy R. Prevalence of cow’s milk protein allergy among children in a university community hospital. Arch Argent Pediatr. (2018) 116(3):219–23. doi: 10.5546/aap.2018.eng.219
20. Sampath V, Abrams EM, Adlou B, Akdis C, Akdis M, Brough HA, et al. Food allergy across the globe. J Allergy Clin Immunol. (2021) 148(6):1347–64. doi: 10.1016/j.jaci.2021.10.018
21. Vandenplas Y, Carnielli VP, Ksiazyk J, Luna MS, Migacheva N, Mosselmans JM, et al. Factors affecting early-life intestinal microbiota development. Nutrition. (2020) 78. doi: 10.1016/j.nut.2020.110812
22. Halken S, Muraro A, de Silva D, Khaleva E, Angier E, Arasi S, et al. EAACI guideline: preventing the development of food allergy in infants and young children (2020 update). Pediatr Allergy Immunol. (2021) 32(5):843–58. doi: 10.1111/pai.13496
23. Milani C, Duranti S, Bottacini F, Casey E, Turroni F, Mahony J, et al. The first microbial colonizers of the human gut: composition, activities, and health implications of the infant gut Microbiota. Microbiol Mol Biol Rev. (2017) 81(4). doi: 10.1128/MMBR.00036-17
24. Han P, Gu JQ, Li LS, Wang XY, Wang HT, Wang Y, et al. The association between intestinal bacteria and allergic diseases-cause or consequence? Front Cell Infect Microbiol. (2021) 11. doi: 10.3389/fcimb.2021.650893
25. Vandenplas Y, Brough HA, Fiocchi A, Miqdady M, Munasir Z, Salvatore S, et al. Current guidelines and future strategies for the management of cow's milk allergy. J Asthma Allergy. (2021) 14:1243–56. doi: 10.2147/JAA.S276992
26. Jaime BE, Martín JJD, Baviera LCB, Monzón AC, Hernández AH, Burriel JIG, et al. Non-IgE-mediated cow’s milk allergy: consensus document of the spanish society of paediatric gastroenterology, hepatology, and nutrition (SEGHNP), the spanish association of paediatric primary care (AEPAP), the spanish society of extra-hospital paediatrics and primary health care (SEPEAP), and the spanish society of paediatric clinicaL immunology, allergy, and asthma (SEICAP). An Pediatr (Engl Ed). (2019) 90(3):193.e1–193.e11. doi: 10.1016/j.anpedi.2018.11.007
27. Cordero RC, Prado SF, Bravo JP. Update on management of cow’s milk protein allergy: available milk formulas and other juices. Rev Chil Pediatr. (2018) 89(3):310–7. doi: 10.4067/S0370-41061997000300001
28. Van Der Aa LB, Heymans HS, Van Aalderen WM, Sillevis Smitt JH, Knol J, Ben Amor K, et al. Effect of a new synbiotic mixture on atopic dermatitis in infants: a randomized-controlled trial. Clin Exp Allergy. (2010) 40(5):795–804. doi: 10.1111/j.1365-2222.2010.03465.x
29. Salminen S, Stahl B, Vinderola G, Szajewska H. Infant formula supplemented with biotics: current knowledge and future perspectives. Nutrients. (2020) 12(7):1–20. doi: 10.3390/nu12071952
30. Walkner M, Warren C, Gupta RS. Quality of life in food allergy patients and their families. Pediatr Clin North Am. (2015) 62(6):1453–61. doi: 10.1016/j.pcl.2015.07.003
31. Salvatore S, Agosti M, Baldassarre ME, D’auria E, Pensabene L, Nosetti L, et al. Cow’s milk allergy or gastroesophageal reflux disease-can we solve the dilemma in infants? Nutrients. (2021) 13(2):1–17. doi: 10.3390/nu13020297
32. Filiz S, Keleş Ş, Akbulut UE, Işık A, Kara MZ. Sleep disturbances and affecting factors in young children with food allergy and their mothers. Allergol Immunopathol (Madr). (2020) 48(2):158–64. doi: 10.1016/j.aller.2019.06.014
33. Gordon M, Biagioli E, Sorrenti M, Lingua C, Moja L, Banks SSC, et al. Dietary modifications for infantile colic. Cochrane Database Syst Rev. (2018) 10(10). doi: 10.1002/14651858.CD011029.pub2
34. Maslin K, Fox AT, Chambault M, Meyer R. Palatability of hypoallergenic formulas for cow’s milk allergy and healthcare professional recommendation. Pediatr Allergy Immunol. (2018) 29(8):857–62. doi: 10.1111/pai.12979
Keywords: cow's milk allergy, cow’s milk protein allergy, food allergy, extensively hydrolyzed formula, synbiotics
Citation: Soria R, Del Compare M, Sallaberry M, Martín G, Aprigliano G, Hermida V, Carosella M, Gruenberg M, Monsell S, Micone P, Maciero E and Giglio N (2023) Efficacy of an extensively hydrolyzed formula with the addition of synbiotics in infants with cow's milk protein allergy: a real-world evidence study. Front. Allergy 4:1265083. doi: 10.3389/falgy.2023.1265083
Received: 21 July 2023; Accepted: 11 September 2023;
Published: 9 October 2023.
Edited by:
Edoardo Muratore, University of Bologna, ItalyReviewed by:
Arianna Dondi, IRCCS Azienda Ospedaliero-Universitaria di Bologna, ItalyClaudio Alberto Salvador Parisi, Italian Hospital of Buenos Aires, Argentina
Jorge Martinez, Hospital Fernández, Argentina
© 2023 Soria, Del Compare, Sallaberry, Martín, Aprigliano, Hermida, Carosella, Gruenberg, Monsell, Micone, Maciero, Giglio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Norberto Giglio bmdpZ2xpb0BidWVub3NhaXJlcy5nb2IuYXI=