
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Allergy , 21 February 2023
Sec. Rhinology
Volume 4 - 2023 | https://doi.org/10.3389/falgy.2023.1052386
This article is part of the Research Topic Chronic Rhinosinusitis with Nasal Polyps: Patient Perspectives, Empowerment and Treatment View all 5 articles
 Vibeke Backer1*
Vibeke Backer1* Lars Olaf Cardell2,3
Lars Olaf Cardell2,3 Lauri Lehtimäki4,5
Lauri Lehtimäki4,5 Sanna Toppila-Salmi6
Sanna Toppila-Salmi6 Leif Bjermer7
Leif Bjermer7 Sietze Reitsma8
Sietze Reitsma8 Peter W. Hellings8,9,10Dan Weinfeld11Kasper Aanæs1Charlotte Suppli Ulrik12,13Gert-Jan Braunstahl14,15Bernt Bøgvald Aarli16,17Arild Danielsen18
Peter W. Hellings8,9,10Dan Weinfeld11Kasper Aanæs1Charlotte Suppli Ulrik12,13Gert-Jan Braunstahl14,15Bernt Bøgvald Aarli16,17Arild Danielsen18 Hannu Kankaanranta5,19,20
Hannu Kankaanranta5,19,20 Sverre Steinsvåg21
Sverre Steinsvåg21 Claus Bachert2,10,22
Claus Bachert2,10,22
Background: Chronic rhinosinusitis with nasal polyps (CRSwNP) and asthma frequently co-exist and share pathologic features. Taking a “global” treatment approach benefits diagnosis and treatment of both, but care is often siloed by specialty: joined-up clinics are uncommon. Our objectives were to explore expert opinion to give practical suggestions to identify adults needing global airways care; enhance cross-specialty working; and widen knowledge to support diagnosis and management, integrate with existing care pathways, and supplement existing guidelines.
Methods: Sixteen practicing physicians from northern Europe were invited for their national and/or international standing in treating asthma and/or chronic rhinosinusitis. Appreciative Inquiry techniques were used to guide their discussions.
Results: Key themes arising were screening and referral, collaboration on management, awareness and education, and research. Provided are screening criteria and suggestions for specialist referrals, and pointers for physicians to optimize their knowledge of global airways disease. Collaborative working is underscored, and practical suggestions are given for multidisciplinary teamworking within global airways clinics. Research gaps are identified.
Conclusion: This initiative provides practical suggestions for optimizing the care of adults with CRSwNP and asthma. Discussion of the role of allergy and drug exacerbations on these conditions, and care for patients with other global airways diseases were beyond scope; however, we expect some principles of our discussion will likely benefit patients with related conditions. The suggestions bridge asthma and CRSwNP management guidelines, envisioning interdisciplinary, global airway clinics relevant to various clinical settings. They highlight the value of joint screening for early recognition and referral of patients.
Chronic upper and lower airways diseases, such as chronic rhinosinusitis (CRS) and asthma, cause substantial morbidity and mortality. Asthma accounted for some 298 disability-adjusted life-years per 100,000 people worldwide in 2017 (1), and CRS substantially impairs quality of life and carries a high socioeconomic burden (2, 3).
CRS with nasal polyposis (CRSwNP) often coexists with asthma (4, 5): asthma affects 45–49% of patients with CRSwNP (6–9) [some estimates are higher, up to 65% (10, 11)], and CRS affects up to half of those with asthma (10, 12). Both diseases associate with other airway diseases including aspirin/non-steroidal anti-inflammatory drug-exacerbated respiratory disease (AERD/N-ERD) (13, 14), eosinophilic chronic otitis media (15), and allergic rhinitis (16). Indeed, the interlinked and complex nature of airway diseases warrants a holistic management approach (17–19).
CRS is classically divided into the phenotype with nasal polyps (CRSwNP) or without (CRSsNP), and can be further subdivided by immune pathophysiology (20). CRSwNP has a prevalence of around 2.5% in Europe but is more common among those with asthma (21); polyposis also correlates with asthma severity (22, 23). Around 80% of CRSwNP cases involve intense eosinophilic airway inflammation with high immunoglobulin (Ig)-E and interleukin (IL)-5 (24, 25). However, the clinical spectrum is complex: some patients exhibit no atopic features or IgEs specific for inhaled allergens (14, 26).
Increasing understanding of the shared pathophysiological features of these conditions, their frequent co-existence, and the anatomic continuity of the upper and lower airways, has led to the concept of “global” airways diseases (19, 27–27). Mechanisms for this interaction include not just local upregulation of cytokines and adhesion molecules at mucosal sites, but systemic pathways involving the bloodstream, bone marrow and mucosa-associated lymphoid tissue (28, 29). Despite differences between compartments, the importance of treating upper and lower airway conditions together is underscored by studies showing that treating one often improves the other, and that inadequate treatment of either may exacerbate the other (19, 30).
Despite compelling evidence of the benefits a global airways approach can bring to diagnosis, treatment, and adherence, it is not yet widespread within clinical practice (31, 32). Recently, when advising the European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA), European patients with long-term Type-2 airway inflammation urged better coordination between all physicians involved in treating Type-2 inflammation, whether in the upper or lower airways (33). For example, traditionally, ear, nose, and throat (ENT) physicians or rhinologists manage upper airways diseases, and pulmonologists manage lower airways diseases (33). While both specialties have specific tools and therapies to manage diseases within their area, cross-specialty collaboration and understanding, multi-disciplinary team (MDT) working, and knowledge-sharing with general practitioners (GPs), is often lacking (32, 34). This disjointed structure means current systems may hinder optimal care for patients with combined diseases (32, 34).
The advent of biologic treatment for patients with asthma in some countries (35, 36), and—more recently—CRSwNP (37), spotlights the benefits of global airways management; however, questions remain around their optimal usage (38–40). In this project, ENT physicians/rhinologists and pulmonologists from northern Europe convened to develop practical recommendations for treating adults with severe asthma and CRSwNP as a global airways disease, to try to answer the outstanding questions. Although we focused only on this specific combination, we recognize that global airways disease is a large and multi-faceted topic, and many other types—including, for example, allergic and atopic presentations—are also deserving of similar study. Our suggestions supplement existing guidelines addressing either upper or lower airways diseases, or global airways diseases together (16, 32, 41–43). This work builds on earlier consensus: in 2021, EUFOREA agreed definitions and principles of managing severe CRSwNP with biologics (43). Our work builds on this foundation by exploring how to integrate these considerations with existing care pathways, and how to improve them with cross-specialty collaboration. We explored the following hypotheses:
1. Improving global airways knowledge among specialists will facilitate timely and adequate treatment.
2. Systematic upper and lower airways assessment increases the likelihood of discovering global airways disease.
3. Collaboration between upper and lower airways physicians will improve treatment, adherence, and disease control for patients with global airways disease.
Therefore, this project aimed to provide practical suggestions for identifying and assessing upper and lower airways disease; to suggest models of collaboration between ENT physicians/rhinologists, allergologists, and pulmonologists; and to optimize treatment for patients benefiting from a global airways approach.
The experts comprised 16 practicing physicians from Belgium, Denmark, Finland, The Netherlands, Norway, and Sweden. Each was selected for their experience in managing patients with asthma and/or CRS. Also considered was their involvement in scientific meetings, guidelines, and education, and publications records. Selection ensured a variety of care models, and equal numbers of pulmonologists and ENT physicians/rhinologists—including those also specialized in allergology—were represented.
The expert group was led by a Steering Committee of eight individuals with at least one member from each country, and co-chaired by one pulmonologist and one ENT physician. The Steering Committee guided the project's scope and provided clinical leadership.
To ensure the suggestions arising from the experts’ discussions were relevant to patients’ and primary care concerns, the all-expert meeting was joined by a practicing GP from Norway, and a patient from Finland with severe asthma and CRS.
For the purposes of this initiative, CRSwNP was defined as per the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020 guidelines (44).
This initiative was conducted between March and June 2021: its key steps are shown in Figure 1.
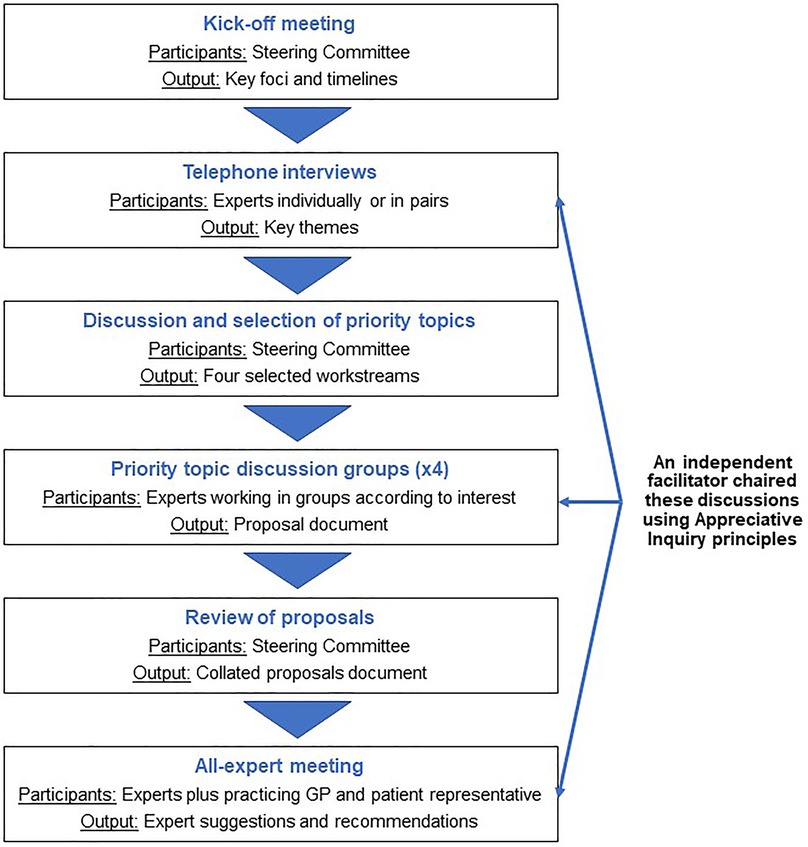
Figure 1. Schematic of the Appreciative Inquiry process used for this project.
The Steering Committee met virtually to define the project's foci and set its timelines and milestones. This was followed by 60-minute telephone interviews with the experts, either individually or in pairs of one ENT physician/rhinologist and one pulmonologist. To avoid biasing or leading the discussions, these interviews were conducted by an independent facilitator, alongside an observer. The facilitator and observer then analyzed transcripts and contemporaneous notes to identify the key themes arising.
Key themes were discussed at a Steering Committee meeting, and four priority topics among them were chosen for further exploration based on the findings. Experts were then assigned to one of four groups—one for each primary topic—according to their self-professed interests. Each group convened at least once to discuss their topic in the context of the initiative's aims, and to make suggestions. Each group submitted their proposals to the Steering Committee for review.
The Steering Committee used the proposals to shape an agenda for an all-expert virtual meeting. This included all participants, including the reference stakeholders. Its aims were to discuss the proposals among the wider group and to finalize the key recommendations.
Appreciative Inquiry is a multi-step process that encourages participants to consolidate existing successes, not focus on problems, making positive changes more likely. Given the existence of separate recommendations for the management of asthma and CRS, Appreciative Inquiry offered a positive way to explore and unite those further, as it is an enabling process of facilitation that helps participants address evidence and its context, and to use these insights to promote evidence-based practices in healthcare (45).
The key ideas identified following the interviews were analyzed and arranged into themes, discussed below.
Awareness among non-specialists of the global airways concept may be limited.
Although “global airways” is a familiar concept to our experts, they were unsure how widely accepted it is beyond specialist settings. They suggest that applying a global airways approach in practice would involve collaboration between ENT physicians/rhinologists and pulmonologists to diagnose and manage patients in a joined-up way: from referral through diagnosis and long-term management.
Care for those with moderate-to-severe asthma and CRSwNP is particularly siloed: adopting a “global airways” approach may greatly benefit such patients.
The experts agreed that patients with various respiratory conditions could benefit from borderless airway management, rather than divided care from upper and lower airway specialists working separately. The experts suggested that care is particularly siloed for those with moderate-to-severe asthma and CRSwNP, and so these patients could benefit greatly from joined-up care. Nevertheless, given the cumulative burden of combined symptoms and risk of disease progression, such approaches are likely to be beneficial even to those with milder forms of disease, and for those with other airway diseases such as allergic rhinitis, AERD/N-ERD, and asthma.
Patients are “lost in the system” because of a lack of common screening or referral approaches for patients with global airways conditions.
Global airways disease management is not yet established in most clinical practices, and timely diagnosis is challenging. The experts report patients often becoming “lost in the system”, which was corroborated by the patient stakeholder. A lack of clear inter-specialty collaboration means that patients can bounce around within primary care and among different specialists.
Diagnosis of comorbid asthma and CRSwNP needs improvement.
Effective screening for combined upper and lower airways disease is vital to enable systematic diagnostic workup and referral of patients who would benefit from a global approach. Enhancing screening in primary care and in non-specialist ENT/rhinology and pulmonology settings is crucial, especially since some patients with asthma and CRSwNP respond poorly to biologics in their upper or lower airway: for them particularly, a thorough, joined-up diagnosis is important.
Collaborative care models for patients with upper and lower respiratory diseases are heterogenous.
To manage patients with combined disease, many experts rely on intra-specialty referrals in non-synchronous clinics. Others use informal relationships, formal agreements, or run joint ENT/pulmonology clinics focusing on specific patients. These models are determined by local healthcare settings, inter-specialist and inter-organizational relationships, local “traditions”, and established business models.
Knowledge and culture are barriers to inter-specialty collaboration.
Differences in clinical approaches and working cultures exist between specialties. Traditionally, ENT physicians/rhinologists have had primary interests in surgical approaches, while pulmonologists were perceived as focusing on medical approaches. This has changed as the importance of combined approaches to treating CRSw/sNP has been realized. Furthermore, in general, neither ENT physicians/rhinologists nor pulmonologists have a detailed understanding of the other's specialty, and complementary (or shared) approaches to diagnosis and management are lacking.
Current guidelines provide only disjointed guidance for combined upper and lower airways disease.
Existing guidelines for upper and lower airways diseases do not provide detailed, joined-up plans for holistic diagnosis and inter-specialty management. Each specialty knew the guidelines relevant to their focus, but cross-specialty awareness and understanding was low.
The advent of biologics for CRSwNP is improving collaborative working.
Biologics are changing the management of CRSwNP, but ENT physicians/rhinologists cannot routinely (or at all) prescribe them, owing to lacking approval or reimbursement, or organizational difficulties. The experts report the advent of biologic treatment is increasing inter-specialty engagement, perhaps because ENT physicians/rhinologists increasingly rely on pulmonology colleagues to access biologics when direct prescribing is difficult. This shift has begun to facilitate more inter-referral, communication, collaboration and MDT working.
From the thematic report, the Steering Committee identified four topics for further exploration, discussed below.
All patients presenting with upper or lower respiratory symptoms in primary or secondary care should be screened for both asthma and CRS using the definitions and care pathways outlined in the Global Initiative for Asthma (GINA) (46), EPOS (21, 44), and EUFOREA (32, 43) guidelines, and according to the recommendations in Table 1.

Table 1. Screening for asthma and CRS.
Exact referral pathways vary among countries and clinical settings. For example, in some resource-rich countries, referrals to global airways clinics may come from allergy/immunology specialists. Therefore, the experts could not define one global pathway, although the integrated care pathway outlined in the EPOS 2020 guidelines (44) was commended. The following principles were agreed:
1. GPs, working with patients, must oversee referral and proactively integrate information between specialties, but this does not always happen in practice. Providing detailed referral letters (see Table 2)—in addition to standard medical and medication history—is desirable.
2. Specialists working in tertiary centers should collaborate, consulting together or referring patients to other specialties when appropriate. They should also proactively seek to train and educate their primary and secondary care colleagues, where appropriate, and support collaborative working.
3. Global airways clinics are recommended for complex cases. Referring directly from primary care (as well as secondary care) is appropriate.

Table 2. Clinical information to gather before referral.
Collaboration between clinical disciplines is critical to enhance interdisciplinary knowledge and training, accelerate diagnosis, simplify referrals, minimize clinic visits, and improve patient management. Similarly, collaboration between GPs and secondary care is necessary to guide investigations, treatment, and triggers for referral.
The ideal specialist care model for patients with severe CRSwNP and asthma is via a dedicated MDT—a global airways clinic—including, at a minimum, a rhinologist and an asthma specialist (or allergologist) working collaboratively. A rhinologist would support diagnosis and staging of CRS and recommend optimal treatment. Asthma or allergy specialists would support asthma or allergic rhinitis diagnosis and treatment, and may provide drug challenges when assessing for N-ERD. For example, specific cyclooxygenase-2 inhibitors, if highly selective, are usually well tolerated, although this is sparsely known outside specialist settings (13, 21): collaboration would help share this knowledge. An MDT may also include other specialties, including pathologists, dermatologists, and researchers. Specialist nurses could be employed as patients’ points of contact, helping them navigate their treatment, and educating them in device usage and medication adherence.
The global airways clinic ideally should reside within a tertiary care setting, where its role should be to make overarching treatment decisions regarding types of surgery (e.g., reboot, polypectomy), and prescribe biologics. Diagnostic tests and investigations, as well as ongoing management of any chosen treatments (e.g., administering recurrent injections), should be managed in local settings, with cross-referral with global airways clinics as needed.
The precise operations of global airways clinics will vary because of local and national health service considerations and structures. However, the experts agree that, as a minimum, a global airways clinic must have the facilities and experience to perform nose and sinus surgeries, and the capacity to apply and monitor biologics use. Physicians should involve policymakers, insurance companies, patients’ boards, and local communities to organize their global airways clinic to best meet local needs.
Such structures have been implemented in The Netherlands, where collaboration between global and local clinics has underpinned their success. This global/local approach builds and concentrates in-depth knowledge in specialist centers, facilitates data collection for registries, educates clinicians working outside specialist settings, and can be more convenient for patients. Global airways clinics also exist in some Danish hospitals, in which nasal polyps and lung function are assessed together. This approach increases staffing and associated costs, but its key advantage is that different specialists collaborate to evaluate patients once, then diagnose and treat individually. Nurses follow up regularly with patients.
Table 3 describes the experts’ specific advice for healthcare settings considering establishing a global airways clinic.
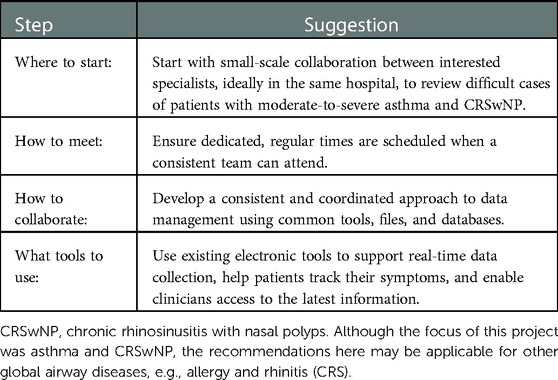
Table 3. Practical advice for establishing a global airways clinic.
Improving diagnosis, referral, and treatment depends on raising awareness of global airways, as well as ensuring patients, GPs, and specialists can confidently recognize and treat upper and lower airways symptoms. Recognition of the key differentiating symptoms of combined severe asthma and CRSwNP (Figure 2) is vital, as is awareness of guideline-recommended treatment paradigms (Table 4).

Figure 2. Key differentiating symptoms of combined severe asthma and chronic rhinosinusitis with nasal polyps. Additional symptoms associated with other airways conditions may also be present including for allergic rhinitis: runny nose, itchy nose, eyes and ears, sneezy, nasal discharge, seasonal variation; for chronic rhinosinusitis: loss of smell, nasal closure/obstruction, facial headache, nasal discharge; and additionally for asthma: chest tightness, night time symptoms, exercise-induced symptoms.
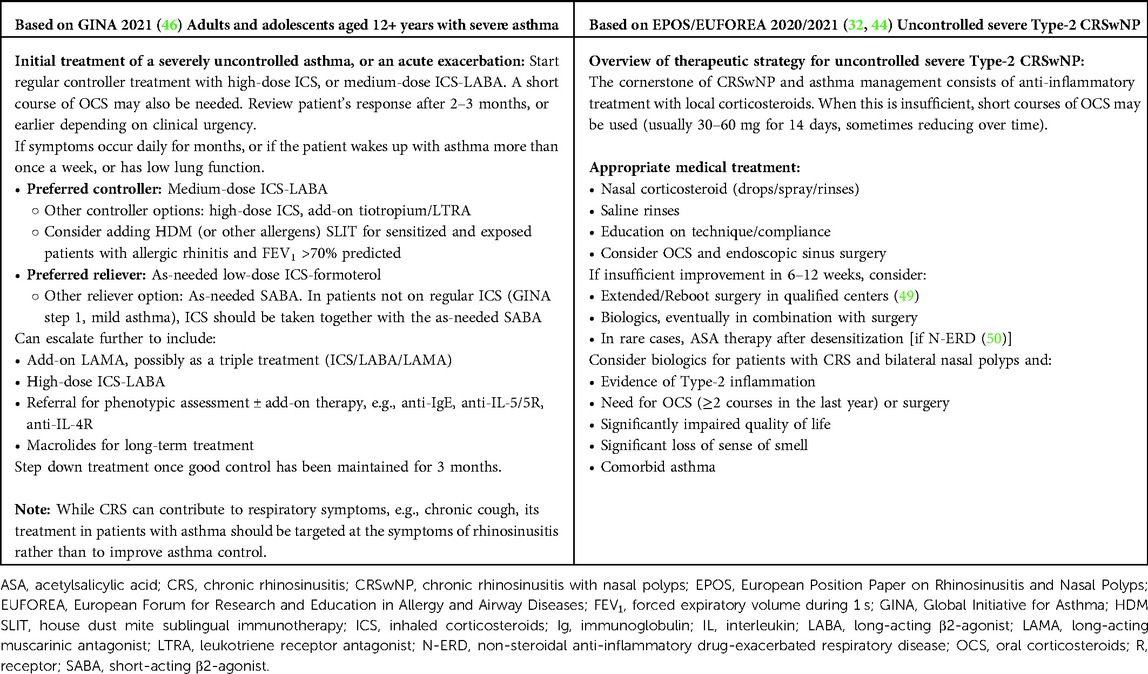
Table 4. Overview of the treatment paradigms for moderate-to-severe asthma and CRSwNP.
Cross-specialty education would accelerate patients’ identification and referral, and prevent patients from becoming “lost in the system” without holistic care from any provider. Education should be tailored to each audience. Respiratory nurses’ roles could be expanded to help educate primary care practitioners, who should themselves focus on screening for comorbid diseases, investigations helpful for secondary care, and referrals. In secondary care, education should be delivered jointly for involved specialties to develop a common understanding of global airways disease and its management.
Collaborative care of patients with global airways disease is advocated in guidelines, and anecdotal examples demonstrate its value, but further consolidating research is needed. Evaluation tools to stage and characterize patients with combined disease are desirable, and could be used to guide their management. The experts identified five topics deserving of priority research:
1. If a composite tool existed to aid screening and referral to secondary or tertiary care, which symptoms should, and could, it measure?
2. Would early intervention in patients with combined upper and lower airways disease reduce their total inflammatory burden? Would this reduce their future risk of deterioration and/or systemic consequences (e.g., increased total disease burden including comorbid conditions)? How cost-effective is this approach?
3. What measurable impact does collaborative management have on patients? What evidence already exists? Which endpoints should we measure to assess its impact?
4. What is the impact of treating a patient’s asthma on their nasal polyposis, and vice versa? More evidence is needed for individual treatments and disease phenotypes.
5. What is the role of endotyping and/or phenotyping in diagnosing and managing combined airways disease?
This project gathered specialists in managing patients with some of the most intractable upper and lower respiratory diseases. This group considered how to practically implement global airways screening, assessment, diagnosis, and management across disciplines and clinical settings to enhance patients’ care.
The experts suggest screening criteria for asthma and CRS, suggesting what to do if either is suspected, what information to gather, and when to refer to specialist care. They underscore the importance of collaborative working between all physicians involved in these patients’ care, primarily via a dedicated MDT working in a global airways clinic, ideally in a tertiary setting. The experts advise how to establish such a clinic within existing frameworks. The experts give care providers ways to optimize their awareness of symptoms and guideline-recommended treatment paradigms. Lastly, the experts identify research questions to optimize the care of patients with global airways disease in future.
We focused on patients with moderate-to-severe asthma and moderate-to-severe CRSwNP, for whom treatment paradigms are changing given the advent of biologic therapies, and for whom existing care is particularly siloed (51). Biologics now offer the possibility of combining medical and surgical solutions (32, 43, 44), and although this shift is encouraging, the absence of multi-disciplinary working is evident (43). However, we recognize that asthma and CRSwNP is just one of many manifestations of global airways disease that could benefit from better joined-up working, and hope that our principles will have broader application to other indications.
The suggestions arising from this initiative supplement, but do not replace, guidelines for asthma (41, 42, 46) and CRS (21, 44), by augmenting them with practical advice for clinicians wishing to collaborate and implement global airways approaches in their practice.
The difficulties arising from managing respiratory tract conditions as distinct—often siloed—specialties were a recurring theme in this initiative, and this echoes concerns repeatedly raised by patients in a recent EUFOREA study (52). Vital to the success of our initiative was to build on separate established traditions and best practices in the management of upper and lower airways diseases. Using Appreciative Inquiry, we explored how existing successes could be broadened and united. In healthcare, Appreciative Inquiry helps people consider evidence, its context and its application (45). Appreciative Inquiries typically involve large groups working face-to-face over several days; however, coronavirus restrictions necessitated a virtual approach. This may have slowed the project's momentum, but nevertheless enabled deep discussion and reflection.
Our vision for collaborative care of patients with moderate-to-severe global airways disease has three parts: dedicated teams of specialists collaboratively manage the most severely affected patients in global airways clinics; GPs and non-specialists understand global airways disease and can quickly screen and appropriately refer patients; and informed patients can identify their symptoms as global airways disease, advocate for themselves, and self-manage their own care. The gold standard recommended here is a multi-disciplinary approach, but we accept this may be difficult to achieve in all health settings, although digital solutions may make this more accessible in future.
The wider adoption of telemedicine during the COVID-19 pandemic, especially in secondary care (53), may now enable the use of virtual multi-disciplinary consultations. This could aid initial patient assessment and support appropriate referral to tertiary settings, potentially streamlining the process and expanding patient access especially in areas where health resources are limited.
At the time of our initiative, no composite screening tools for assessing upper and lower respiratory tract signs had been developed. In the absence of such a tool, we highlighted the concurrent use of existing screening approaches for asthma and CRS as a pragmatic alternative, building on those already validated and available. However, success would depend on clinicians having a greater understanding of global airways disease and its impact on referral pathways. While not available at the time our initiative was done, the STARR-15 tool now offers the first global airways questionnaire to be used when examining patients with upper and lower airways symptoms, such as allergic rhinitis, CRS and asthma (54). While pending validation, we hope that this and future tools may help improve the diagnosis of patients with global airways diseases, which is among our key recommendations.
Integrated care is common when treating patients with comorbid conditions. For example, Allergic Rhinitis and its Impact on Asthma (ARIA) advocates this approach for managing allergic rhinitis and asthma as one disease (41), and this is desired by patients with various global airways diseases (51, 52). Again, these pathways need to be identified locally and supported by targeted education for clinicians in primary care and non-specialist settings.
Shared decision-making and patient empowerment are essential (43). We advocate for a more symptoms-based approach to recognizing global airways disease, and suggest focusing on the symptoms most indicative of Type-2 disease.
This project's limitations mainly relate to the breadth of expert and non-expert involvement. A small number of experts were involved, albeit selected for their understanding of their countries’ health systems. Most were ENT/rhinology consultants or pulmonologists (with some specializing in asthma and allergology), and most work in university or tertiary care settings. Although representative of the specialists encountering the most severe cases, we recognize we may have overlooked the nuanced viewpoints from other disciplines (such as pathology or pharmacy). In addition, ENT physicians/rhinologists and pulmonologists working outside specialist settings were not included. Overall, expert selection ensured the group was weighted for experts familiar with the patients in question, and with experience implementing collaborative practices.
Patients and primary care practitioners were under-represented in our expert group, and no specialist nurses were involved: in retrospect, we recognize the group would have benefited from earlier and more extensive input from these stakeholders. However, the consensus underscores the need to engage these groups locally, to build and embed referral practices, and to improve communication and symptom recognition.
The recommendations herein are based on clinical practice in northern European countries, while considering their heterogeneity. We suggest they may therefore have wider relevance to similar high-income health settings. We hope these first steps to collaborative clinical practice will be developed further, perhaps by a collaborative working group spanning the organizations focused on global airways disease. In parallel, further evidence is needed to understand the value of different treatment models, as is a validated, composite tool to identify patients with combined disease burden. We suggest that, in future, such topics may lend themselves well to more formalized consensus recommendations using Delphi or similar methods.
In conclusion, this initiative gives practical suggestions for better identifying patients who would benefit from a global airways approach, enhancing referral pathways and promoting collaborative cross-specialty working and education. We have specifically focused on patients with CRSwNP and comorbid severe asthma, although these principles will likely benefit patients with more wide-ranging, difficult-to-treat, or even less-severe indications that nevertheless need better recognition. We hope this initiative stimulates reflection, prompts cross-functional discussion, and renews focus on improving the care of patients with global airways disease.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
VB, LOC were co-chairs leading the initiative and together with the steering committee of LL, ST-S, LB, SR, PH, CB substantially contributed to the conception and design of the work; DW, KA, CU, G-JB, BA, AD, HK, SS contributed to workstream development supporting collection and interpretation of information. All authors contributed to the drafting, review, and revision of the manuscript and agree the submission.
This study received funding from Sanofi. The funder participated in early discussions with the Chairs on the relevance and potential design of the project, but was not involved in the collection, analysis, or interpretation of data, the writing of this article, or the decision to submit it for publication. All authors declare no other competing interests.
Medical writing support was provided by Alice Kirk, funded by Sanofi. Janice Steed and Keena McKillen were Appreciative Inquiry facilitators supported by Sheila Tang, Sanofi. The authors thank Eivind Kamøy and the patient from Finland who participated as part of a stakeholder reference group.
LOC has received institutional grants and/or personal fees from Orion Pharma, Sanofi, GlaxoSmithKline and ALK-Abello. LL has received honoraria for educational activities, lectures or advisory boards from ALK, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mundipharma, Novartis, Orion, Sanofi, and Teva. ST-S has received personal fees from ALK-Abello, Mylan Laboratories, Biomedical Systems, Roche Products, Sanofi Pharma, and Novartis Investments for consultancy, and a grant from GlaxoSmithKline. LB has during the last 3 years received honoraria for educational activities, lectures, or advisory boards from ALK, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Sanofi, and Teva. SR has received honoraria for educational activities, lectures, advisory boards, and research grants from Novartis, Sanofi, and GlaxoSmithKline. DW has received renumeration for advisory boards with Teva and AstraZeneca. KA has received honoraria for educational activities and advisory boards from Sanofi. CU has received honoraria for educational activities, lectures, and advisory boards from AstraZeneca, GlaxoSmithKline, Sanofi, Mundipharma, Teva, Boehringer Ingelheim, Novartis, Orion Pharma, Actelion, ALK-Abello, and Sandoz. BA has received honoraria for educational activities and advisory boards from GlaxoSmithKline, AstraZeneca, Novartis, Sanofi-Aventis, Boehringer Ingelheim, and Chiesi outside the submitted work. HK has received personal fees and non-financial support from AstraZeneca, personal fees from Chiesi Pharma AB, personal fees from Boehringer Ingelheim, personal fees from MSD, personal fees from Novartis, personal fees and non-financial support from Orion Pharma, personal fees from Sanofi Genzyme, and personal fees from GlaxoSmithKline, outside the submitted work. CB has received honoraria as principal investigator of the study, consultant and advisory from Sanofi and Novartis, advisory boards from GlaxoSmithKline and as principal investigator from AstraZeneca. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Soriano JB, Kendrick PJ, Paulson KR, Gupta V, Abrams EM, Adedoyin RA, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. (2020) 8(6):585–96. doi: 10.1016/S2213-2600(20)30105-3
2. Chen S, Zhou A, Emmanuel B, Thomas K, Guiang H. Systematic literature review of the epidemiology and clinical burden of chronic rhinosinusitis with nasal polyposis. Curr Med Res Opin. (2020) 36(11):1897–911. doi: 10.1080/03007995.2020.1815682
3. Lourijsen ES, Fokkens WJ, Reitsma S. Direct and indirect costs of adult patients with chronic rhinosinusitis with nasal polyps. Rhinology. (2020) 58(3):213–7. doi: 10.4193/Rhin19.468
4. Delemarre T, Holtappels G, De Ruyck N, Zhang N, Nauwynck H, Bachert C, et al. Type 2 inflammation in chronic rhinosinusitis without nasal polyps: another relevant endotype. J Allergy Clin Immunol. (2020) 146(2):337–43.e6. doi: 10.1016/j.jaci.2020.04.040
5. Bachert C, Zhang N, Holtappels G, De Lobel L, van Cauwenberge P, Liu S, et al. Presence of IL-5 protein and IgE antibodies to staphylococcal enterotoxins in nasal polyps is associated with comorbid asthma. J Allergy Clin Immunol. (2010) 126(5):962–8. doi: 10.1016/j.jaci.2010.07.007
6. Khan A, Vandeplas G, Huynh TMT, Joish VN, Mannent L, Tomassen P, et al. The global allergy and asthma European network (GALEN) rhinosinusitis cohort: a large European cross-sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology. (2019) 57(1):32–42. doi: 10.4193/Rhin17.255
7. Philpott CM, Erskine S, Hopkins C, Kumar N, Anari S, Kara N, et al. Prevalence of asthma, aspirin sensitivity and allergy in chronic rhinosinusitis: data from the UK national chronic rhinosinusitis epidemiology study. Respir Res. (2018) 19(1):129. doi: 10.1186/s12931-018-0823-y
8. Promsopa C, Kansara S, Citardi MJ, Fakhri S, Porter P, Luong A. Prevalence of confirmed asthma varies in chronic rhinosinusitis subtypes. Int Forum Allergy Rhinol. (2016) 6(4):373–7. doi: 10.1002/alr.21674
9. Stevens WW, Peters AT, Hirsch AG, Nordberg CM, Schwartz BS, Mercer DG, et al. Clinical characteristics of patients with chronic rhinosinusitis with nasal polyps, asthma, and aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. (2017) 5(4):1061–70.e3. doi: 10.1016/j.jaip.2016.12.027
10. Benjamin MR, Stevens WW, Li N, Bose S, Grammer LC, Kern RC, et al. Clinical characteristics of patients with chronic rhinosinusitis without nasal polyps in an academic setting. J Allergy Clin Immunol Pract. (2019) 7(3):1010–6. doi: 10.1016/j.jaip.2018.10.014
11. Håkansson K, Bachert C, Konge L, Thomsen SF, Pedersen AE, Poulsen SS, et al. Airway inflammation in chronic rhinosinusitis with nasal polyps and asthma: the united airways concept further supported. PLoS One. (2015) 10(7):e0127228. doi: 10.1371/journal.pone.0127228
12. Jarvis D, Newson R, Lotvall J, Hastan D, Tomassen P, Keil T, et al. Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy. (2012) 67(1):91–8. doi: 10.1111/j.1398-9995.2011.02709.x
13. White AA, Stevenson DD. Aspirin-exacerbated respiratory disease. N Engl J Med. (2018) 379(11):1060–70. doi: 10.1056/NEJMra1712125
14. Cahill KN, Boyce JA. Aspirin-exacerbated respiratory disease: mediators and mechanisms of a clinical disease. J Allergy Clin Immunol. (2017) 139(3):764–6. doi: 10.1016/j.jaci.2016.09.025
15. Daval M, Picard H, Bequignon E, Bedbeder P, Coste A, Ayache D, et al. Chronic otitis media with effusion in chronic sinusitis with polyps. Ear Nose Throat J. (2018) 97(8):E13–e8. doi: 10.1177/014556131809700803
16. Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. (2017) 140(4):950–8. doi: 10.1016/j.jaci.2017.03.050
17. Guan W-J, Tran T, Wang D-Y. Intra/extracellular dynamics of the respiratory system and global airway disease. Front Cell Dev Biol. (2020) 8:523. doi: 10.3389/fcell.2020.00523
18. Hellings PW, Prokopakis EP. Global airway disease beyond allergy. Curr Allergy Asthma Rep. (2010) 10(2):143–9. doi: 10.1007/s11882-010-0107-1
19. Giavina-Bianchi P, Aun MV, Takejima P, Kalil J, Agondi RC. United airway disease: current perspectives. J Asthma Allergy. (2016) 9:93–100. doi: 10.2147/JAA.S81541
20. Porsbjerg C, Ulrik C, Skjold T, Backer V, Laerum B, Lehman S, et al. Nordic consensus statement on the systematic assessment and management of possible severe asthma in adults. Eur Clin Respir J. (2018) 5(1):1440868. doi: 10.1080/20018525.2018.1440868
21. Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. (2020) 58(S29):1–464. doi: 10.4193/Rhin20.600
22. Ceylan E, Gencer M, San I. Nasal polyps and the severity of asthma. Respirology. (2007) 12(2):272–6. doi: 10.1111/j.1440-1843.2006.00964.x
23. Pearlman AN, Chandra RK, Chang D, Conley DB, Tripathi-Peters A, Grammer LC, et al. Relationships between severity of chronic rhinosinusitis and nasal polyposis, asthma, and atopy. Am J Rhinol Allergy. (2009) 23(2):145–8. doi: 10.2500/ajra.2009.23.3284
24. Tomassen P, Vandeplas G, Van Zele T, Cardell LO, Arebro J, Olze H, et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J Allergy Clin Immunol. (2016) 137(5):1449–56.e4. doi: 10.1016/j.jaci.2015.12.1324
25. Bachert C, Zhang N. Medical algorithm: diagnosis and treatment of chronic rhinosinusitis. Allergy. (2020) 75(1):240–2. doi: 10.1111/all.13823
26. Jackson DJ, Busby J, Pfeffer PE, Menzies-Gow A, Brown T, Gore R, et al. Characterisation of patients with severe asthma in the UK severe asthma registry in the biologic era. Thorax. (2021) 76(3):220–7. doi: 10.1136/thoraxjnl-2020-215168
27. Vlaminck S, Acke F, Scadding GK, Lambrecht BN, Gevaert P. Pathophysiological and clinical aspects of chronic rhinosinusitis: current concepts. Front Allergy. (2021) 2:741788. doi: 10.3389/falgy.2021.741788
28. Braunstahl GJ. United airways concept: what does it teach us about systemic inflammation in airways disease? Proc Am Thorac Soc. (2009) 6(8):652–4. doi: 10.1513/pats.200906-052DP
29. Braunstahl GJ. The unified immune system: respiratory tract-nasobronchial interaction mechanisms in allergic airway disease. J Allergy Clin Immunol. (2005) 115(1):142–8. doi: 10.1016/j.jaci.2004.10.041
30. Kanda A, Kobayashi Y, Asako M, Tomoda K, Kawauchi H, Iwai H. Regulation of interaction between the upper and lower airways in united airway disease. Med Sci. (2019) 7(2):27. doi: 10.3390/medsci7020027
31. Tiotiu A, Novakova P, Baiardini I, Bikov A, Chong-Neto H, de-Sousa JC, et al. Manifesto on united airways diseases (UAD): an interasma (global asthma association–GAA) document. J Asthma. (2021) 59(4):639–54. doi: 10.1080/02770903.2021.1879130
32. Fokkens WJ, Lund V, Bachert C, Mullol J, Bjermer L, Bousquet J, et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy. (2019) 74(12):2312–9. doi: 10.1111/all.13875
33. Claeys N, Teeling MT, Legrand P, Poppe M, Verschueren P, De Prins L, et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front Allergy. (2021) 2(61):761388. doi: 10.3389/falgy.2021.761388
34. Vennik J, Eyles C, Thomas M, Hopkins C, Little P, Blackshaw H, et al. Chronic rhinosinusitis: a qualitative study of patient views and experiences of current management in primary and secondary care. BMJ Open. (2019) 9(4):e022644. doi: 10.1136/bmjopen-2018-022644
35. Busse WW. Anti-immunoglobulin E (omalizumab) therapy in allergic asthma. Am J Respir Crit Care Med. (2001) 164(8 Pt 2):S12–7. doi: 10.1164/ajrccm.164.supplement_1.2103026
36. Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. (2018) 378(26):2486–96. doi: 10.1056/NEJMoa1804092
37. Patel GB, Peters AT. The role of biologics in chronic rhinosinusitis with nasal polyps. Ear Nose Throat J. (2021) 100(1):44–7. doi: 10.1177/0145561320964653
38. Bachert C, Zhang N, Cavaliere C, Weiping W, Gevaert E, Krysko O. Biologics for chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. (2020) 145(3):725–39. doi: 10.1016/j.jaci.2020.01.020
39. Hellings P, Verhoeven E, Fokkens W. State-of-the-art overview on biological treatment for CRSwNP. Rhinology. (2021) 59(2):151–63. doi: 10.4193/Rhin20.570
40. van der Lans RJL, Fokkens WJ, Adriaensen GFJPM, Hoven RD, Drubbel JJ, Reitsma S. Real-life observational cohort verifies high efficacy of dupilumab for chronic rhinosinusitis with nasal polyps. Allergy. (2021) 77(2):670–4. doi: 10.1111/all.15134
41. Bousquet JJ, Schünemann HJ, Togias A, Erhola M, Hellings PW, Zuberbier T, et al. Next-generation ARIA care pathways for rhinitis and asthma: a model for multimorbid chronic diseases. Clin Transl Allergy. (2019) 9:44. doi: 10.1186/s13601-019-0279-2
42. Bousquet J, Schünemann HJ, Togias A, Bachert C, Erhola M, Hellings PW, et al. Next-generation allergic rhinitis and its impact on asthma (aria) guidelines for allergic rhinitis based on grading of recommendations assessment, development and evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. (2020) 145(1):70–80.e3. doi: 10.1016/j.jaci.2019.06.049
43. Bachert C, Han JK, Wagenmann M, Hosemann W, Lee SE, Backer V, et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: definitions and management. J Allergy Clin Immunol. (2021) 147(1):29–36. doi: 10.1016/j.jaci.2020.11.013
44. Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. Executive summary of EPOS 2020 including integrated care pathways. Rhinology. (2020) 58(2):82–111. doi: 10.4193/Rhin20.601
45. Kavanagh T, Stevens B, Seers K, Sidani S, Watt-Watson J. Process evaluation of appreciative inquiry to translate pain management evidence into pediatric nursing practice. Implement Sci. (2010) 5(1):90. doi: 10.1186/1748-5908-5-90
46. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention (2021).
47. Usmani OS, Han MK, Kaminsky DA, Hogg J, Hjoberg J, Patel N, et al. Seven pillars of small airways disease in asthma and COPD–supporting opportunities for novel therapies. Chest. (2021) 160(1):114–34. doi: 10.1016/j.chest.2021.03.047
48. Diamant Z, Vijverberg S, Alving K, Bakirtas A, Bjermer L, Custovic A, et al. Toward clinically applicable biomarkers for asthma: an EAACI position paper. Allergy. (2019) 74(10):1835–51. doi: 10.1111/all.13806
49. Alsharif S, Jonstam K, van Zele T, Gevaert P, Holtappels G, Bachert C. Endoscopic sinus surgery for type-2 CRS wNP: an endotype-based retrospective study. Laryngoscope. (2019) 129(6):1286–92. doi: 10.1002/lary.27815
50. Stevens WW, Jerschow E, Baptist AP, Borish L, Bosso JV, Buchheit KM, et al. The role of aspirin desensitization followed by oral aspirin therapy in managing patients with aspirin-exacerbated respiratory disease: a work group report from the rhinitis, rhinosinusitis and ocular allergy committee of the American academy of allergy, asthma & immunology. J Allergy Clin Immunol. (2021) 147(3):827–44. doi: 10.1016/j.jaci.2020.10.043
51. Claeys N, Teeling MT, Legrand P, Poppe M, Verschueren P, De Prins L, et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front Allergy. (2021) 2(61):761388. doi: 10.3389/falgy.2021.761388
52. De Prins L, Raap U, Mueller T, Schmid-Grendelmeier P, Haase CH, Backer V, et al. White paper on European patient needs and suggestions on chronic type 2 inflammation of airways and skin by EUFOREA. Front Allergy. (2022) 3:889221. doi: 10.3389/falgy.2022.889221
53. Pinnock H, Murphie P, Vogiatzis I, Poberezhets V. Telemedicine and virtual respiratory care in the era of COVID-19. ERJ Open Res. (2022) 8:00111. doi: 10.1183/23120541.00111-2022
Keywords: asthma, nasal polyps, respiratory hypersensitivity, rhinitis, sinusitis, chronic rhinosinusitis with nasal polyps (CRSwNP), global airways disease, interdisciplinary care
Citation: Backer V, Cardell LO, Lehtimäki L, Toppila-Salmi S, Bjermer L, Reitsma S, Hellings PW, Weinfeld D, Aanæs K, Ulrik CS, Braunstahl G, Aarli BB, Danielsen A, Kankaanranta H, Steinsvåg S and Bachert C (2023) Multidisciplinary approaches to identifying and managing global airways disease: Expert recommendations based on qualitative discussions. Front. Allergy 4:1052386. doi: 10.3389/falgy.2023.1052386
Received: 23 September 2022; Accepted: 17 January 2023;
Published: 21 February 2023.
Edited by:
Laurent Eckert, Sanofi, FranceReviewed by:
Hideyuki Kawauchi, Shimane University, Japan© 2023 Backer, Cardell, Lehtimäki, Toppila-Salmi, Bjermer, Reitsma, Hellings, Weinfeld, Aanæs, Ulrik, Braunstahl, Aarli, Danielsen, Kankaanranta, Steinsvåg and Bachert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vibeke Backer YmFja2VyQGRhZGxuZXQuZGs=
Specialty Section: This article was submitted to Rhinology, a section of the journal Frontiers in Allergy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.