 S. Lazizi
S. Lazizi R. Labrosse
R. Labrosse F. Graham
F. Graham
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Allergy , 26 August 2022
Sec. Food Allergy
Volume 3 - 2022 | https://doi.org/10.3389/falgy.2022.974250
This article is part of the Research Topic Pediatric Food Allergy: Novel Issues in Diagnosis and Management View all 4 articles
Peanut allergy is on the rise in industrialized countries, affecting 1%–4.5% of children and generally persisting into adulthood. It is associated with a risk of severe anaphylaxis and is one of the major causes of food allergy-induced deaths. Health-related quality of life is significantly impaired for patients and affected families due to food restrictions attributable to omnipresent precautionary allergen labeling, constant risk of potentially life-threatening reactions, and limitation of social activities. Oral immunotherapy (OIT) has emerged as a valid treatment option for patients with IgE-mediated peanut allergy, with randomized controlled trials and real-life studies showing a high rate of desensitization and a favorable safety profile, especially in young children. Ultimately, the decision to initiate peanut OIT relies on a multidisciplinary shared decision-making process, involving open, personalized and evidence-based discussions with patients and their caregivers.
Peanut allergy is on the rise in industrialized countries, affecting 1%–4.5% of children and generally persisting into adulthood (1–4). It is associated with a risk of severe anaphylaxis and is one of the major causes of food allergy-induced deaths (5). Health-related quality of life is significantly impaired for affected families (6) due to food restrictions attributable to omnipresent precautionary allergen labeling (PAL), constant risk of potentially life-threatening reactions, and limitation of social activities (7). Strict dietary avoidance and emergency treatment of accidental reactions with an epinephrine auto-injector is the current standard of care. Nonetheless, accidental reactions occur frequently with an annual incidence of 12%–14% (8, 9), leading many patients to seek alternative treatment options.
Oral immunotherapy (OIT) is increasingly recognized as a valid option for the treatment of IgE-mediated food allergy, with many studies focusing on peanut OIT. It involves daily ingestion of a food allergen with the goal of increasing allergen tolerance (10). OIT protocols usually consist of 3 steps: initial dose escalation, up-dosing or buildup phase and maintenance phase (11). The initial dose escalation determines the starting dose, which is followed by dose increases every 1–2 weeks over several months until a predefined maintenance dose is reached. This maintenance dose is then ingested every day for a prolonged period. This continuous exposure is expected to modulate the immune response against the allergen, resulting in a decreased production of IgE and increased production of neutralizing IgG4 antibodies (10).
In this review, clinical desensitization is defined as a state in which a patient can tolerate peanuts as long as regular ingestion occurs. Sustained unresponsiveness is defined as a state in which the patient who is desensitized can stop eating the food for a short period of time (generally 4–8 weeks but up to 6 months in some studies) and remains non-reactive when the food is reingested. Oral tolerance refers to permanent resolution of peanut allergy, a state where tolerance is maintained even after prolonged period of peanut avoidance (i.e., patient can eat peanuts at any given dose and time without regular ingestion). The purpose of this review is to examine data on peanut OIT efficacy and safety and to discuss evidence towards transitioning peanut OIT into clinical practice.
Several randomized controlled trials (RCTs), uncontrolled studies, and clinical practice retrospective chart reviews have demonstrated the efficacy of peanut OIT at inducing clinical desensitization to peanuts (Table 1). Generally, clinical desensitization rates vary between 60 and 80% in clinical trials, and 80%–90% in outpatient practice. PALISADE is the largest peanut OIT RCT (using a peanut-derived drug containing up to 300 mg of protein) and was conducted by Vickery et al. in 2018 (27). The primary endpoint was tolerance of 600 mg peanut protein on an exit double-blind, placebo-controlled food challenge (DBPCFC). Of 496 children aged 4–17 years old, 67.2% were able to tolerate the dose of 600 mg compared to 4% in the placebo group. ARTEMIS is another recent peanut OIT RCT using the same peanut-derived drug, in which 58% of 132 children aged 4–17 years old tolerated 1,000 mg of peanut protein on an exit DBPCFC after 3 month maintenance at 300 mg of peanut protein (34). Afinogenova et al. described the largest retrospective study of patients having undergone peanut OIT. A chart review of 783 patients aged 3.5–48.3 years old who underwent peanut OIT at the New England Food allergy treatment center showed a desensitization rate of 89% (33). All in all, studies point to a high desensitization rate with peanut oral immunotherapy in children, although more data is needed in adults (10). One important caveat is that desensitization may not be the most adequate efficacy endpoint, and reactions in the community may be a better surrogate marker of clinical efficacy (38, 39), which is an important point to be addressed in future studies.
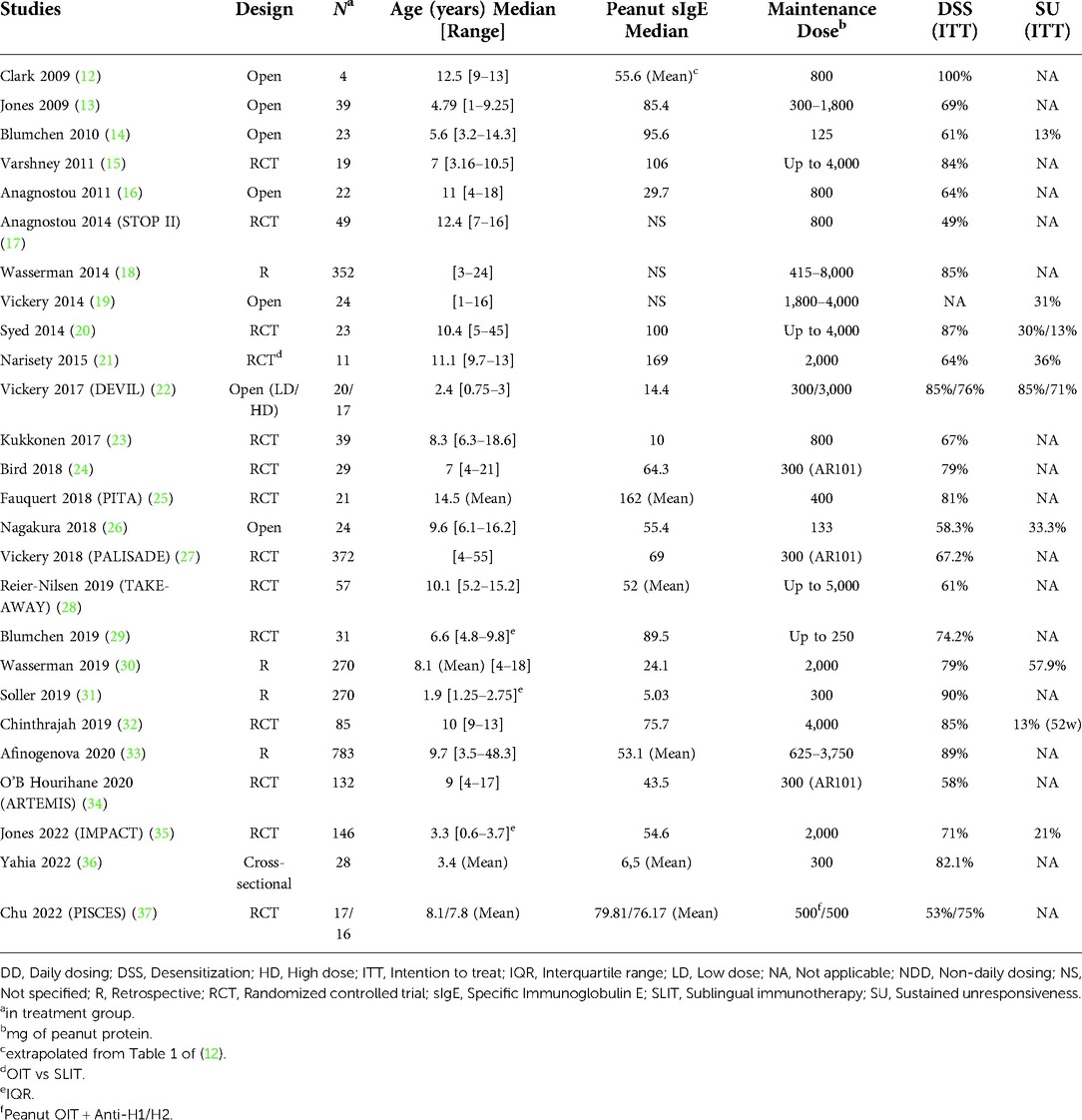
Table 1. Peanut OIT studies and efficacy outcomes.
The intention-to-treat desensitization rates presented above (Table 1) show that approximately 15%–20% of study participants fail to reach desensitization targets by the end of the study period. The reasons for this are numerous and include treatment discontinuation due to OIT-related side effects, non-compliance, relocation, or uncontrolled asthma among others.
Adverse reactions during OIT are reported in 50%–95% of patients (27, 40), depending on the severity of the peanut allergy. The most frequently reported symptoms are generally mild, and usually include itching of the mouth and throat and abdominal discomfort. Between 10% and 25% of patients experience severe allergic reactions requiring the injection of epinephrine when taking doses at home (18, 22, 33, 40). One study reports a rate of 9% of patients requiring at least one dose of epinephrine during physician supervised up-dosings (35).
Cofactors are external factors that can influence the reactivity threshold of patients undergoing peanut OIT and are sometimes implicated in allergic reactions at home to doses that were previously well tolerated. These include physical exertion, infections, extreme heat, poorly controlled asthma, alcohol consumption, use of non-steroidal anti-inflammatory drugs (e.g., ibuprofen), viral infections, sleep deprivation, as well as menstrual cycles (41). When beginning OIT, patients are given precise instructions to minimize the impact of these cofactors surrounding daily doses. For example, they are instructed to reduce their doses to half during viral illnesses, and to avoid exercise 1 h before and 2 h after their doses (42). These recommendations generally stay in effect even at the maintenance stage.
In addition to dose-related immediate reactions, eosinophilic esophagitis (EoE) has been associated with OIT in up to 2.7% of cases (43), although this seems to be a temporary effect that usually resolves upon discontinuation of treatment (44). This is distinct from spontaneous EoE, developing in the absence of OIT, which usually has a chronic clinical course. Interestingly, esophageal eosinophilia was seen during dose escalations in the majority of patients undergoing peanut OIT but resolved without treatment during maintenance phase (45). Other GI manifestations include eosinophilic esophagitis like oral immunotherapy related syndrome (ELORS), which manifests as delayed vomiting usually around 2–6 h after doses and is accompanied by peripheral eosinophilia (46, 47). Lastly, peanut aversion can develop in a substantial portion of patients and can limit treatment compliance, and lead to treatment failure in some cases (42, 48). Importance is placed on varying textures and food formats to improve palatability of OIT peanut doses (see Table 2 for peanut maintenance dose food equivalences), especially in children.
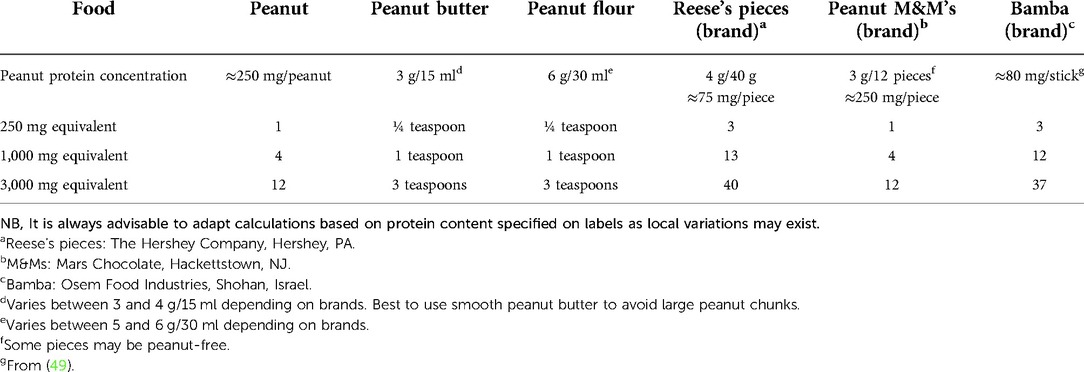
Table 2. Peanut maintenance dose examples with food equivalents.
The increase of reactivity threshold achieved by OIT leads to a reduction of accidental reactions to peanuts. Baumert et al. performed a quantitative assessment of risk reduction following OIT and found that increasing the baseline threshold from 100 mg or less to 300 mg of peanut protein post-OIT would reduce the risk of reacting to foods with precautionary allergen labeling by more than 95% (50). Further increasing the threshold to 1,000 mg would provide an additional risk reduction of 70-fold. This has also been suggested by a clinical trial where peanut OIT was found to reduce the number and severity of allergic reactions after accidental peanut consumption compared to placebo (51).
Open trials with peanut OIT have described a significant improvement in quality of life (QoL) in patients undergoing the treatment. Several studies have shown a statistically and clinically significant effect on the QoL with OIT using standardized questionnaires such as the Food Allergy Quality of Life Questionnaire (FAQLQ). More specifically, there was an improvement in emotional impact and a decrease in hypervigilance, social limitations, dietary restrictions and anxiety regarding diet (17, 52–56). QoL tends to improve significantly upon reaching the maintenance phase but may be preceded by a temporary detrimental effect on QoL during up-dosing (57).
While data has clearly demonstrated the effectiveness of peanut OIT in inducing desensitization in a large portion of patients, data concerning sustained unresponsiveness is limited and, although variable, rates are generally under 50% (Table 1). This depends on numerous factors including age, length of avoidance and duration of the maintenance phase. Blumchen et al. reported a sustained unresponsiveness rate of barely 13%, after a short treatment of 9 months, with a therapeutic target set at 500 mg of protein (approximately 2 peanuts) (14). Vickery et al, on the other hand, reported a 50% sustained unresponsiveness rate with a higher maintenance dose and longer protocol duration (median of 5-year treatment with a maintenance dose of 4,000 mg peanut protein) (19). Interestingly, Chinthrajah et al. performed up-dosings up to a maintenance dose of 4,000 mg of peanut protein for nearly 2 years and patients were then split in two groups for 52 weeks: discontinuation or dose lowering to 300 mg of peanut protein (32). Sustained unresponsiveness in the group discontinuing treatment gradually decreased throughout the study period reaching a low of 13% (8/60) after 52 weeks. This study highlights the fact that sustained unresponsiveness decreases with increasing duration of peanut avoidance (32).
Thus, patients beginning treatment should be warned that long-term (lifetime) ingestion of peanuts may be necessary to maintain desensitization. One important aspect to mention is that in patients presenting a return of clinical reactivity after a period of avoidance (failed sustained unresponsiveness), the threshold of reactivity to the allergen is generally still higher than before OIT.
Adjuvanted peanut OIT studies are ongoing with the objective to improve long-term sustained unresponsiveness and/or increase the safety profile of OIT (58). Examples of adjuvants currently being studied in peanut OIT trials include omalizumab (59), dupilumab (NCT03682770), abatacept (NCT04872218), prebiotics (ACTRN12617000914369) and probiotics. Tang et al. notably reported a very high sustained unresponsiveness rate of 82% with a peanut OIT protocol combined with probiotic Lactobacillus rhamnosus in children after a short 2-week discontinuation period (60). Unfortunately, the clinical trial did not include a probiotic-free OIT arm and the 2-week period was relatively short compared to other studies, which may have led to an overestimation of the sustained unresponsiveness rate. Indeed, a more recent phase 2b trial by the same group found a sustained unresponsiveness rate of 46% in the peanut probiotic group compared to 51% in the peanut OIT without probiotic group (not significantly different) (61). Future studies will hopefully provide a better understanding of the pathomechanisms associated with sustained unresponsiveness and tolerance in oral immunotherapy to help develop more effective adjuvants.
A recent meta-analysis showed that peanut OIT is associated with higher risk of anaphylactic reactions requiring epinephrine than avoidance (62). Anaphylaxis can occur both during escalation period and maintenance doses. It is important to note that these reactions occur in a controlled environment (at home) and are an expected potential side effect of treatment, discussed prior to obtaining informed consent from the patient, as opposed to accidental reactions in the community, which generally occur in unprepared social situations (63). OIT is expected to decrease long-term and accidental reactions (51, 63), which could justify having potential increased reactions during up-dosing and beginning of maintenance phase. Furthermore, studies that were excluded from PACE include real-life observational data which have shown a high safety profile for peanut OIT (22, 31). All in all, the risk of anaphylaxis during OIT should always be discussed before providing OIT, and patients should have a personalized action plan to guide them in the acute management of anaphylaxis.
Although longer-term quality of life seems to improve (see previous section), OIT comes with a lot of constraints, especially related to cofactor avoidance during treatment. This can lower the quality of life in certain patients (64). OIT is also time-consuming and requires frequent clinic visits, which can lead to absenteeism from work and school.
Thus, prior to initiation, OIT risks and benefits should be discussed with a focus on the patient and their family's objectives to allow shared decision-making (65).
A growing number of allergists in North America have started adopting OIT in private practice. In a survey, 13.8% of allergists said they had already incorporated OIT in their practice (66). In clinical practice, OIT has generally been effective with clinical desensitization rates of 80%–90% (18, 30, 31, 33). Wasserman et al. recently published clinical experience with 270 patients undergoing peanut OIT in private practice (30). Dose escalations were achieved in 79% of patients. Adverse effects included grade I–II reactions in 170 patients, and grade III–IV reactions in 91 patients, whereas 63/270 (23%) incurred anaphylactic reactions requiring epinephrine (Mueller grading system (67)). The largest private practice peanut OIT study by Afinogenova et al. involving 783 patients showed a desensitization rate of 89% with 10% of patients experiencing systemic reactions during buildup and 19% during maintenance (33). These data support the successful transition of peanut OIT into clinical practice, with data from private practice showing high efficacy with safety parameters comparable to research protocols.
Selecting the right patients for OIT is crucial for treatment success. Factors associated with increased side effects of therapy include older age, high baseline specific IgE (sIgE), history of severe anaphylaxis, although these are not absolute contraindications to initiating therapy after risk-benefit discussion. However, one might refer these more challenging cases to tertiary specialized centers, whereas milder allergies could be treated in outpatient settings. Absolute contraindications for OIT initiation include uncontrolled asthma and pregnancy (10). Relative contraindications include active EoE, severe active atopic dermatitis, and relative contraindications to epinephrine (e.g., active heart disease); decision to initiate OIT in such situations should be based on clinical judgment and shared decision-making. In addition, patients who are unable to comprehend desensitization protocols, unmitigated language barriers, non-collaborative family dynamics, lack of commitment from patients or caregivers and non-adherence to protocol also constitute contraindications to peanut OIT (10).
Data from the literature shows higher desensitization and sustained unresponsiveness rates as well as less frequent severe adverse events in toddlers when compared to older children, possibly due to greater immune plasticity (22, 31, 35). The DEVIL study showed that a maintenance dose of 300 mg or 3,000 mg is safe and effective in preschool children, achieving desensitization rates of 85% and 76% respectively (22). Sustained unresponsiveness after 4 weeks of avoidance was very high at 85% for the low dose and 71% for the high dose.
In a multicentric Canadian study, Soller et al. examined real-world safety of peanut OIT in 270 preschoolers who achieved a 90% desensitization rate (31). Grade I-II reactions occurred in 67.4% of participants, grade III-IV occurred in 0.4% of participants and epinephrine was required in only 4.1% of patients (World Allergy Organization Subcutaneous Immunotherapy Reaction Grading System (68)). A recent RCT by Jones et al. studying peanut OIT in children under 4 years old showed that 71% of 96 children achieved desensitization whereas only 21% achieved sustained unresponsiveness (Intention-to-treat) after 6 months of avoidance, which is a longer avoidance period than in most protocols (usually 4–8 weeks) (35). Nevertheless, younger patients had significantly higher rates of remission with 71% of children under 2 years of age achieving sustained unresponsiveness. Overall, remission was associated with younger age and lower baseline peanut-specific IgE (35). Thus, future peanut OIT resources may need to be invested in younger children to maximize positive long-term outcomes.
A major obstacle to widespread implementation of OIT is the lack of standardized product and the tedious process of preparing precise peanut doses. Pre-weighted doses of peanut powder such as PB2 peanut flour have been used in different clinical trials. Generally, these doses are weighed using a microbalance and individual doses are delivered to the patient in powder forms (e.g., in plastic cups). Doses are ingested daily by patients by mixing powders with soft foods such as apple sauce. Although effective, this process is time consuming and requires appropriate resources. Another option is to prepare a peanut suspension in simple syrup using peanut flour (50 mg/ml of peanut protein) (10). This was shown to add a gain in efficiency of 2,340% when compared to weighing powders (69) and may be an option to facilitate implementation of OIT in clinical practice. Once the patient reaches higher doses, switching powders or suspensions to readily accessible prepackaged foods or whole peanuts may be an easier option and less resource-intensive (see Table 2 for maintenance dose equivalences).
In the United States, the FDA recently approved Palforzia (AR101), a standardized good manufacturing practice (GMP) manufactured peanut powder derived from roasted peanut flour and premeasured in capsules with different dosages. The product is intended to simplify the preparation steps of peanut doses and provides a precise dose of peanut to the consumer undergoing OIT. Unfortunately, Palforzia costs $9,840 USD per year ($820 per month) and this high cost (100 times more than market-available peanut powder) could negatively affect widespread consumer access to this treatment. The product likely has no efficacy or safety advantage compared to shelf-bought peanut products, considering that slight peanut dose variations have not been shown to increase risk of dose-related reactions (70).
Another challenge in routine implementation of peanut OIT is the lack of a standardized protocols. This is partly because OIT should be personalized, and one cannot use a one-size-fits-all approach (10). As with all foods, peanut OIT involves an initial dose escalation, followed by up-dosing and maintenance phases (71). An initial dose escalation typically involves a fixed series of very low doses to identify the most sensitive patients (e.g., 0.1–6 mg of protein (22)); the patient then continues daily ingestion of the highest tolerated dose or the final dose if no reaction occurs. Peanut up-dosings are generally performed every 1 to 2 weeks in research protocols, although up-dosings can occur at longer intervals (up to 3 months (71)) depending on OIT provider resources and availabilities. After achieving the maintenance dose, the patient pursues daily dose ingestion (See Table 2 for peanut food equivalents for maintenance dose) and is generally re-assessed every 6–12 months, with discussion of adverse reactions and treatment compliance since last follow-up. Reduction in maintenance dosing frequency may sometimes be an option to counter long-term dosing fatigue (e.g., every other day, 3 times per week, or weekday dosing with weekends off), although there is a lack of data for optimal guidance. This is sometimes based on a successful high threshold OFC in clinical practice. In some situations, patients can be challenged for sustained unresponsiveness after a certain period of time has elapsed, based on clinical and immunological factors (e.g., fall in specific IgE levels, negativation of skin prick test) (30). More in-depth information about different protocols and maintenance doses can be found elsewhere in the literature and is beyond the scope of this review (10, 49, 71, 72).
Another challenge of implementing peanut OIT in clinical practice is the reorganization of infrastructure. All physicians administering peanut OIT should be able to recognize and treat OIT-related symptoms and have access to the appropriate infrastructure and equipment to treat anaphylactic reactions. This includes a space to receive the patients, a designated room to prepare doses, an emergency treatment space and access to a service corridor to transport patients in case of reaction (10, 49). Moreover, the ability to safely and efficiently provide food challenges is an essential part of an OIT practice and not all allergists offer them because of perceived barriers such as time, space, staffing, and proximity to a hospital (73).
Before initiating OIT, patients should have a personalized action plan to guide them in the management of adverse effects. Families should be equipped with an algorithm providing guidance for situations such as missed doses or illness (49). They should also be able to contact a professional to whom they can address questions and concerns during treatment. Some physicians offer 24/7 on call availability to their OIT patients (74), which can require significant personal commitment and time investment, especially in OIT practices with a large number of patients. Another more practical option is to offer OIT-related assistance only during work hours; outside of those hours, patients are instructed to follow their emergency care plan in case of dose-related reactions, which includes treating themselves with epinephrine and calling 911 in case of anaphylaxis (patients are always instructed to contact the clinic in case of anaphylactic reactions to their doses).
In the build-up phase, patients are generally monitored for 1 h after up-dosings (49), but the timeframe can vary depending on the clinical practice and increased surveillance could be necessary in higher-risk patients (e.g. patient with previous delayed reaction to up-dosing). In addition, physicians should be aware of the possibility of EoE and inquire about suggestive symptoms during follow-ups.
A multidisciplinary approach can be implemented to relieve the burden of certain tasks from OIT providers (10, 49). For instance, nurses can be an essential point of contact with patients and answer questions regarding doses and treatment of allergic reactions. They can additionally coordinate care with treating physicians. Dieticians can provide important information for food equivalents once maintenance dose is attained. Psychologists may be beneficial in patients with anxiety or stress related to their food allergy. Patient and food allergy support groups can provide an important outlet for discussing information that may not be readily available.
With the advent of personalized medicine, OIT represents a novel therapeutic modality for IgE-mediated peanut allergy, wherein the status quo has been avoidance. A patient-centered discussion before initiating OIT might entail multiple visits to ensure adequate comprehension of benefits as well as limitations of this therapy. Although transition to clinical practice has already begun in many centers, obstacles to wider implementation include substantial infrastructure and human resource requirements. Further data is needed to better establish long-term outcomes such as sustained unresponsiveness. Younger patients (preschool children) seem to have more favorable long-term outcomes and should increasingly be prioritized for this form of treatment. Ultimately, the decision to initiate peanut OIT relies on a multidisciplinary shared decision-making process, involving open, personalized, and evidence-based discussions with patients and their caregivers.
SL contributed to the redaction of manuscript, and approval of final manuscript.
RL contributed to the redaction of manuscript, and approval of final manuscript.
FG contributed to the preparation of manuscript, redaction of manuscript, and approval of final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Savage J, Sicherer S, Wood R. The natural history of food allergy. J Allergy Clin Immunol Pract. (2016) 4(2):196–203; quiz 4. doi: 10.1016/j.jaip.2015.11.024
2. Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics. (2011) 128(1):e9–e17. doi: 10.1542/peds.2011-0204
3. Sicherer SH, Munoz-Furlong A, Burks AW, Sampson HA. Prevalence of peanut and tree nut allergy in the US determined by a random digit dial telephone survey. J Allergy Clin Immunol. (1999) 103(4):559–62. doi: 10.1016/S0091-6749(99)70224-1
4. Sicherer SH, Munoz-Furlong A, Godbold JH, Sampson HA. US Prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J Allergy Clin Immunol. (2010) 125(6):1322–6. doi: 10.1016/j.jaci.2010.03.029
5. Bock SA, Munoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. (2001) 107(1):191–3. doi: 10.1067/mai.2001.112031
6. King RM, Knibb RC, Hourihane JO. Impact of peanut allergy on quality of life, stress and anxiety in the family. Allergy. (2009) 64(3):461–8. doi: 10.1111/j.1398-9995.2008.01843.x
7. Stensgaard A, Bindslev-Jensen C, Nielsen D, Munch M, DunnGalvin A. Quality of life in childhood, adolescence and adult food allergy: patient and parent perspectives. Clin Exp Allergy. (2017) 47(4):530–9. doi: 10.1111/cea.12849
8. Cherkaoui S, Ben-Shoshan M, Alizadehfar R, Asai Y, Chan E, Cheuk S, et al. Accidental exposures to peanut in a large cohort of Canadian children with peanut allergy. Clin Transl Allergy. (2015) 5:16. doi: 10.1186/s13601-015-0055-x
9. Yu JW, Kagan R, Verreault N, Nicolas N, Joseph L, St Pierre Y, et al. Accidental ingestions in children with peanut allergy. J Allergy Clin Immunol. (2006) 118(2):466–72. doi: 10.1016/j.jaci.2006.04.024
10. Begin P, Chan ES, Kim H, Wagner M, Cellier MS, Favron-Godbout C, et al. CSACI Guidelines for the ethical, evidence-based and patient-oriented clinical practice of oral immunotherapy in IgE-mediated food allergy. Allergy Asthma Clin Immunol. (2020) 16:20. doi: 10.1186/s13223-020-0413-7
11. Pajno GB, Fernandez-Rivas M, Arasi S, Roberts G, Akdis CA, Alvaro-Lozano M, et al. EAACI Guidelines on allergen immunotherapy: IgE-mediated food allergy. Allergy. (2018) 73(4):799–815. doi: 10.1111/all.13319
12. Clark AT, Islam S, King Y, Deighton J, Anagnostou K, Ewan PW. Successful oral tolerance induction in severe peanut allergy. Allergy. (2009) 64(8):1218–20. doi: 10.1111/j.1398-9995.2009.01982.x
13. Jones SM, Pons L, Roberts JL, Scurlock AM, Perry TT, Kulis M, et al. Clinical efficacy and immune regulation with peanut oral immunotherapy. J Allergy Clin Immunol. (2009) 124(2):292–300, e1–97. doi: 10.1016/j.jaci.2009.05.022
14. Blumchen K, Ulbricht H, Staden U, Dobberstein K, Beschorner J, de Oliveira LC, et al. Oral peanut immunotherapy in children with peanut anaphylaxis. J Allergy Clin Immunol. (2010) 126(1):83–91.e1. doi: 10.1016/j.jaci.2010.04.030
15. Varshney P, Jones SM, Scurlock AM, Perry TT, Kemper A, Steele P, et al. A randomized controlled study of peanut oral immunotherapy: clinical desensitization and modulation of the allergic response. J Allergy Clin Immunol. (2011) 127(3):654–60. doi: 10.1016/j.jaci.2010.12.1111
16. Anagnostou K, Clark A, King Y, Islam S, Deighton J, Ewan P. Efficacy and safety of high-dose peanut oral immunotherapy with factors predicting outcome. Clin Exp Allergy. (2011) 41(9):1273–81. doi: 10.1111/j.1365-2222.2011.03699.x
17. Anagnostou K, Islam S, King Y, Foley L, Pasea L, Bond S, et al. Assessing the efficacy of oral immunotherapy for the desensitisation of peanut allergy in children (STOP II): a phase 2 randomised controlled trial. Lancet. (2014) 383(9925):1297–304. doi: 10.1016/S0140-6736(13)62301-6
18. Wasserman RL, Factor JM, Baker JW, Mansfield LE, Katz Y, Hague AR, et al. Oral immunotherapy for peanut allergy: multipractice experience with epinephrine-treated reactions. J Allergy Clin Immunol Pract. (2014) 2(1):91–6. doi: 10.1016/j.jaip.2013.10.001
19. Vickery BP, Scurlock AM, Kulis M, Steele PH, Kamilaris J, Berglund JP, et al. Sustained unresponsiveness to peanut in subjects who have completed peanut oral immunotherapy. J Allergy Clin Immunol. (2014) 133(2):468–75. doi: 10.1016/j.jaci.2013.11.007
20. Syed A, Garcia MA, Lyu SC, Bucayu R, Kohli A, Ishida S, et al. Peanut oral immunotherapy results in increased antigen-induced regulatory T-cell function and hypomethylation of forkhead box protein 3 (FOXP3). J Allergy Clin Immunol. (2014) 133(2):500–10. doi: 10.1016/j.jaci.2013.12.1037
21. Narisety SD, Frischmeyer-Guerrerio PA, Keet CA, Gorelik M, Schroeder J, Hamilton RG, et al. A randomized, double-blind, placebo-controlled pilot study of sublingual versus oral immunotherapy for the treatment of peanut allergy. J Allergy Clin Immunol. (2015) 135(5):1275–82, e1–6. doi: 10.1016/j.jaci.2014.11.005
22. Vickery BP, Berglund JP, Burk CM, Fine JP, Kim EH, Kim JI, et al. Early oral immunotherapy in peanut-allergic preschool children is safe and highly effective. J Allergy Clin Immunol. (2017) 139(1):173–81.e8. doi: 10.1016/j.jaci.2016.05.027
23. Kukkonen AK, Uotila R, Malmberg LP, Pelkonen AS, Makela MJ. Double-blind placebo-controlled challenge showed that peanut oral immunotherapy was effective for severe allergy without negative effects on airway inflammation. Acta Paediatr. (2017) 106(2):274–81. doi: 10.1111/apa.13668
24. Bird JA, Spergel JM, Jones SM, Rachid R, Assa'ad AH, Wang J, et al. Efficacy and safety of AR101 in oral immunotherapy for peanut allergy: results of ARC001, a randomized, double-blind, placebo-controlled phase 2 clinical trial. J Allergy Clin Immunol Pract. (2018) 6(2):476–85.e3. doi: 10.1016/j.jaip.2017.09.016
25. Fauquert JL, Michaud E, Pereira B, Bernard L, Gourdon-Dubois N, Rouzaire PO, et al. Peanut gastrointestinal delivery oral immunotherapy in adolescents: results of the build-up phase of a randomized, double-blind, placebo-controlled trial (PITA study). Clin Exp Allergy. (2018) 48(7):862–74. doi: 10.1111/cea.13148
26. Nagakura KI, Yanagida N, Sato S, Nishino M, Asaumi T, Ogura K, et al. Low-dose oral immunotherapy for children with anaphylactic peanut allergy in Japan. Pediatr Allergy Immunol. (2018) 29(5):512–8. doi: 10.1111/pai.12898
27. Investigators PGoC, Vickery BP, Vereda A, Casale TB, Beyer K, du Toit G, et al. AR101 Oral immunotherapy for peanut allergy. N Engl J Med. (2018) 379(21):1991–2001. doi: 10.1056/NEJMoa1812856
28. Reier-Nilsen T, Michelsen MM, Lodrup Carlsen KC, Carlsen KH, Mowinckel P, Nygaard UC, et al. Feasibility of desensitizing children highly allergic to peanut by high-dose oral immunotherapy. Allergy. (2019) 74(2):337–48. doi: 10.1111/all.13604
29. Blumchen K, Trendelenburg V, Ahrens F, Gruebl A, Hamelmann E, Hansen G, et al. Efficacy, safety, and quality of life in a multicenter, randomized, placebo-controlled trial of low-dose peanut oral immunotherapy in children with peanut allergy. J Allergy Clin Immunol Pract. (2019) 7(2):479–91.e10. doi: 10.1016/j.jaip.2018.10.048
30. Wasserman RL, Hague AR, Pence DM, Sugerman RW, Silvers SK, Rolen JG, et al. Real-world experience with peanut oral immunotherapy: lessons learned from 270 patients. J Allergy Clin Immunol Pract. (2019) 7(2):418–26.e4. doi: 10.1016/j.jaip.2018.05.023
31. Soller L, Abrams EM, Carr S, Kapur S, Rex GA, Leo S, et al. First real-world safety analysis of preschool peanut oral immunotherapy. J Allergy Clin Immunol Pract. (2019) 7(8):2759–67.e5. doi: 10.1016/j.jaip.2019.04.010
32. Chinthrajah RS, Purington N, Andorf S, Long A, O’Laughlin KL, Lyu SC, et al. Sustained outcomes in oral immunotherapy for peanut allergy (POISED study): a large, randomised, double-blind, placebo-controlled, phase 2 study. Lancet. (2019) 394(10207):1437–49. doi: 10.1016/S0140-6736(19)31793-3
33. Afinogenova Y, Rubin TN, Patel SD, Powell RL, Gilo JM, Denno MN, et al. Community private practice clinical experience with peanut oral immunotherapy. J Allergy Clin Immunol Pract. (2020) 8(8):2727–35. doi: 10.1016/j.jaip.2020.03.016
34. Hourihane JOB, Beyer K, Abbas A, Fernández-Rivas M, Turner PJ, Blumchen K, et al. Efficacy and safety of oral immunotherapy with AR101 in European children with a peanut allergy (ARTEMIS): a multicentre, double-blind, randomised, placebo-controlled phase 3 trial. Lancet Child Adolesc Health. (2020) 4(10):728–39. doi: 10.1016/S2352-4642(20)30234-0
35. Jones SM, Kim EH, Nadeau KC, Nowak-Wegrzyn A, Wood RA, Sampson HA, et al. Efficacy and safety of oral immunotherapy in children aged 1–3 years with peanut allergy (the Immune Tolerance Network IMPACT trial): a randomised placebo-controlled study. Lancet. (2022) 399(10322):359–71. doi: 10.1016/S0140-6736(21)02390-4
36. Yahia SH, Machnes-Maayan D, Frizinsky S, Maoz-Segal R, Offenganden I, Kenett RS, et al. Oral immunotherapy for children with a high threshold peanut allergy. Ann Allergy Asthma Immunol. (2022) doi: 10.1016/j.anai.2022.05.001. [Epub ahead of print]
37. Chu DK, Freitag T, Marrin A, Walker TD, Avilla E, Freitag A, et al. Peanut oral immunotherapy with or without H1- and H2- antihistamine premedication for peanut allergy (PISCES): a placebo-controlled randomized clinical trial. J Allergy Clin Immunol Pract. (2022) doi: 10.1016/j.jaip.2022.05.015. [Epub ahead of print]
38. Tice JA, Guzauskas GF, Hansen RN, Herron-Smith S, Segel C, Walsh JME, et al. The effectiveness and value of oral immunotherapy and viaskin peanut for peanut allergy A summary from the institute for clinical and economic review’s California technology assessment forum. J Manag Care Spec Pharm. (2020) 26(5):620–3. doi: 10.18553/jmcp.2020.26.5.620
39. Plaut M, Sawyer RT, Fenton MJ. Summary of the 2008 national institute of allergy and infectious diseases-US food and drug administration workshop on food allergy clinical trial design. J Allergy Clin Immunol. (2009) 124(4):671–8.e1. doi: 10.1016/j.jaci.2009.05.027
40. Braun C, Caubet JC. Food oral immunotherapy is superior to food avoidance-CON. Ann Allergy Asthma Immunol. (2019) 122(6):569–71. doi: 10.1016/j.anai.2019.02.006
41. Dua S, Ruiz-Garcia M, Bond S, Durham SR, Kimber I, Mills C, et al. Effect of sleep deprivation and exercise on reaction threshold in adults with peanut allergy: a randomized controlled study. J Allergy Clin Immunol. (2019) 144(6):1584–94.e2. doi: 10.1016/j.jaci.2019.06.038
42. Anagnostou A. A practical, stepwise approach to peanut oral immunotherapy in clinical practice: benefits and risks. J Asthma Allergy. (2021) 14:277–85. doi: 10.2147/JAA.S290915
43. Lucendo AJ, Arias A, Tenias JM. Relation between eosinophilic esophagitis and oral immunotherapy for food allergy: a systematic review with meta-analysis. Ann Allergy Asthma Immunol. (2014) 113(6):624–9. doi: 10.1016/j.anai.2014.08.004
44. Goldberg MR, Elizur A, Nachshon L, Appel MY, Levy MB, Golobov K, et al. Oral immunotherapy-induced gastrointestinal symptoms and peripheral blood eosinophil responses. J Allergy Clin Immunol. (2017) 139(4):1388–90.e4. doi: 10.1016/j.jaci.2016.09.053
45. Wright BL, Fernandez-Becker NQ, Kambham N, Purington N, Cao S, Tupa D, et al. Gastrointestinal eosinophil responses in a longitudinal, randomized trial of peanut oral immunotherapy. Clin Gastroenterol Hepatol. (2020) 19(6):1151–9.e14. doi: 10.1016/j.cgh.2020.05.019
46. Silvers SK, Hague AR, Pence DM, Herbert MA, Sugerman RW, Wasserman RL. Eosinophilic esophagitis like oral immunotherapy related syndrome (ELORS). (2017) 139(2):AB258. doi: 10.1016/j.jaci.2017.12.820
47. Goldberg MR, Nachshon L, Levy MB, Elizur A, Katz Y. Risk factors and treatment outcomes for oral immunotherapy-induced gastrointestinal symptoms and eosinophilic responses (OITIGER). J Allergy Clin Immunol Pract. (2020) 8(1):125–31. doi: 10.1016/j.jaip.2019.07.034
48. Nachshon L, Goldberg MR, Katz Y, Levy MB, Elizur A. Long-term outcome of peanut oral immunotherapy-real-life experience. Pediatr Allergy Immunol. (2018) 29(5):519–26. doi: 10.1111/pai.12914
49. Abrams EM, Erdle SC, Cameron SB, Soller L, Chan ES. How to incorporate oral immunotherapy into your clinical practice. Curr Allergy Asthma Rep. (2021) 21(4):30. doi: 10.1007/s11882-021-01009-8
50. Baumert JL, Taylor SL, Koppelman SJ. Quantitative assessment of the safety benefits associated with increasing clinical peanut thresholds through immunotherapy. J Allergy Clin Immunol Pract. (2018) 6(2):457–65.e4. doi: 10.1016/j.jaip.2017.05.006
51. Trendelenburg V, Blumchen K, Bellach J, Ahrens F, Gruebl A, Hamelmann E, et al. Peanut oral immunotherapy protects patients from accidental allergic reactions to peanut. J Allergy Clin Immunol Pract. (2020) 8(7):2437–41.e3. doi: 10.1016/j.jaip.2020.03.043
52. Blackman AC, Staggers KA, Kronisch L, Davis CM, Anagnostou A. Quality of life improves significantly after real-world oral immunotherapy for children with peanut allergy. Ann Allergy Asthma Immunol. (2020) 125(2):196–201.e1. doi: 10.1016/j.anai.2020.03.028
53. Factor JM, Mendelson L, Lee J, Nouman G, Lester MR. Effect of oral immunotherapy to peanut on food-specific quality of life. Ann Allergy Asthma Immunol. (2012) 109(5):348–52.e2. doi: 10.1016/j.anai.2012.08.015
54. Carraro S, Frigo AC, Perin M, Stefani S, Cardarelli C, Bozzetto S, et al. Impact of oral immunotherapy on quality of life in children with cow milk allergy: a pilot study. Int J Immunopathol Pharmacol. (2012) 25(3):793–8. doi: 10.1177/039463201202500329
55. Otani IM, Begin P, Kearney C, Dominguez TL, Mehrotra A, Bacal LR, et al. Multiple-allergen oral immunotherapy improves quality of life in caregivers of food-allergic pediatric subjects. Allergy Asthma Clin Immunol. (2014) 10(1):25. doi: 10.1186/1710-1492-10-25
56. Reier-Nilsen T, Carlsen KCL, Michelsen MM, Drottning S, Carlsen KH, Zhang C, et al. Parent and child perception of quality of life in a randomized controlled peanut oral immunotherapy trial. Pediatr Allergy Immunol. (2019) 30(6):638–45. doi: 10.1111/pai.13066
57. Epstein-Rigbi N, Goldberg MR, Levy MB, Nachshon L, Elizur A. Quality of life of food-allergic patients before, during, and after oral immunotherapy. J Allergy Clin Immunol Pract. (2019) 7(2):429–36.e2. doi: 10.1016/j.jaip.2018.06.016
58. Johnson-Weaver BT, Staats HF, Burks AW, Kulis MD. Adjuvanted immunotherapy approaches for peanut allergy. Front Immunol. (2018) 9:2156. doi: 10.3389/fimmu.2018.02156
59. Brandstrom J, Vetander M, Sundqvist AC, Lilja G, Johansson SGO, Melen E, et al. Individually dosed omalizumab facilitates peanut oral immunotherapy in peanut allergic adolescents. Clin Exp Allergy. (2019) 49(10):1328–41. doi: 10.1111/cea.13469
60. Tang ML, Ponsonby AL, Orsini F, Tey D, Robinson M, Su EL, et al. Administration of a probiotic with peanut oral immunotherapy: a randomized trial. J Allergy Clin Immunol. (2015) 135(3):737–44.e8. doi: 10.1016/j.jaci.2014.11.034
61. Loke P, Orsini F, Lozinsky AC, Gold M, O'Sullivan MD, Quinn P, et al. Probiotic peanut oral immunotherapy versus oral immunotherapy and placebo in children with peanut allergy in Australia (PPOIT-003): a multicentre, randomised, phase 2b trial. Lancet Child Adolesc Health. (2022) 6(3):171–84. doi: 10.1016/S2352-4642(22)00006-2
62. Chu DK, Wood RA, French S, Fiocchi A, Jordana M, Waserman S, et al. Oral immunotherapy for peanut allergy (PACE): a systematic review and meta-analysis of efficacy and safety. Lancet. (2019) 393(10187):2222–32. doi: 10.1016/S0140-6736(19)30420-9
63. Eiwegger T, Anagnostou K, Arasi S, Begin P, Ben-Shoshan M, Beyer K, et al. Conflicting verdicts on peanut oral immunotherapy from the institute for clinical and economic review and US food and drug administration advisory committee: where do we go from here? J Allergy Clin Immunol. (2020) 145(4):1153–6. doi: 10.1016/j.jaci.2019.10.021
64. Rigbi NE, Goldberg MR, Levy MB, Nachshon L, Golobov K, Elizur A. Changes in patient quality of life during oral immunotherapy for food allergy. Allergy. (2017) 72(12):1883–90. doi: 10.1111/all.13211
65. Graham F, Mack DP, Begin P. Practical challenges in oral immunotherapy resolved through patient-centered care. Allergy Asthma Clin Immunol. (2021) 17(1):31. doi: 10.1186/s13223-021-00533-6
66. Greenhawt MJ, Vickery BP. Allergist-reported trends in the practice of food allergen oral immunotherapy. J Allergy Clin Immunol Pract. (2015) 3(1):33–8. doi: 10.1016/j.jaip.2014.06.023
67. Mueller HL. Diagnosis and treatment of insect sensitivity. J Asthma Res. (1966) 3(4):331–3. doi: 10.3109/02770906609106941
68. Cox L, Larenas-Linnemann D, Lockey RF, Passalacqua G. Speaking the same language: the world allergy organization subcutaneous immunotherapy systemic reaction grading system. J Allergy Clin Immunol. (2010) 125(3):569–74, 74 e1–74 e7. doi: 10.1016/j.jaci.2009.10.060
69. Leroux H, Langlois A, Bastien V, Samaan K, Barrios JL, Paradis L, et al. Proceedings of the Canadian society of allergy and clinical immunology annual scientific meeting 2019: efficiency of peanut suspension with simple syrup compared to individual pre-weighted flour doses for oral immunotherapy. Allergy Asthma Clin Immunol. (2020) 16(1):47.
70. Anvari S, Tran D, Nguyen A, Devaraj S, Davis CM. Peanut oral immunotherapy dose variations do not result in allergic reactions. Pediatr Allergy Immunol. (2018) 29(2):218–20. doi: 10.1111/pai.12837
71. Graham F. Variations in protocol development during OIT. J Food Allergy. (2022) 4(2):86–97. doi: 10.2500/jfa.2022.4.220002
72. Waserman RL. Long term oral immunotherapy management and assessment of success. J Food Allergy. (2022) 4(2):102–5. doi: 10.2500/jfa.2022.4.220015
73. Greiwe J, Oppenheimer J, Bird JA, Fleischer DM, Pongracic JA, Greenhawt M. AAAAI work group report: trends in oral food challenge practices among allergists in the United States. J Allergy Clin Immunol Pract. (2020) 8(10):3348–55. doi: 10.1016/j.jaip.2020.07.035
Keywords: oral immunotherapy (OIT), peanut allergy, food allergy, desensitization, sustained unresponsiveness, clinical tolerance induction, shared decision making
Citation: Lazizi S, Labrosse R and Graham F (2022) Transitioning peanut oral immunotherapy to clinical practice. Front. Allergy 3:974250. doi: 10.3389/falgy.2022.974250
Received: 21 June 2022; Accepted: 5 August 2022;
Published: 26 August 2022.
Edited by:
Paula Cabrera Freitag, Gregorio Marañón Hospital, SpainReviewed by:
Justin Greiwe, Bernstein Allergy Group, Inc., United States© 2022 Lazizi, Labrosse and Graham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: François Graham ZnJhbmNvaXMuZ3JhaGFtQHVtb250cmVhbC5jYQ==
Specialty Section: This article was submitted to Food Allergy, a section of the journal Frontiers in Allergy
Abbreviations DBPCFC, Double-blind placebo-controlled food challenge; GMP, Good manufacturing practice; OFC, Oral food challenge; OIT, Oral immunotherapy; sIgE, Specific immunoglobulin E; SPT, Skin-prick test.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.