 Michael A. Golding1,2*
Michael A. Golding1,2* Cathérine Lemoine-Courcelles1,2
Cathérine Lemoine-Courcelles1,2 Elissa M. Abrams1,2,3Moshe Ben-Shoshan4Philippe Bégin5
Elissa M. Abrams1,2,3Moshe Ben-Shoshan4Philippe Bégin5 Edmond S. Chan3,6
Edmond S. Chan3,6 Derek K. Chu7,8,9Jennifer D. Gerdts10Beatrice Povolo10Harold Kim8,11Elinor Simons1,12
Derek K. Chu7,8,9Jennifer D. Gerdts10Beatrice Povolo10Harold Kim8,11Elinor Simons1,12 Julia Upton13
Julia Upton13 Jennifer L. P. Protudjer1,2,14,15,16
Jennifer L. P. Protudjer1,2,14,15,16- 1The Children's Hospital Research Institute of Manitoba, Winnipeg, MB, Canada
- 2Department of Pediatrics and Child Health, The University of Manitoba, Winnipeg, MB, Canada
- 3Division of Allergy and Immunology, Department of Pediatrics, University of British Columbia, Vancouver, BC, Canada
- 4Division of Pediatric Allergy and Clinical Immunology, Department of Pediatrics, McGill University Health Center, Montreal, QC, Canada
- 5Division of Clinical Immunology, Rheumatology, and Allergy, Department of Pediatrics, Sainte-Justine University Hospital Center, Montreal, QC, Canada
- 6BC Children's Hospital Research Institute, Vancouver, BC, Canada
- 7Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada
- 8Department of Medicine, McMaster University, Hamilton, ON, Canada
- 9The Research Institute of St. Joe's Hamilton, Hamilton, ON, Canada
- 10Food Allergy Canada, Toronto, ON, Canada
- 11Department of Medicine, Western University, London, ON, Canada
- 12Section of Allergy and Immunology, Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, MB, Canada
- 13Division of Immunology and Allergy, Department of Pediatrics, Hospital for Sick Children, University of Toronto, Toronto, ON, Canada
- 14George and Fay Yee Center for Healthcare Innovation, Winnipeg, MB, Canada
- 15Centre for Allergy Research, Karolinska Institutet, Stockholm, Sweden
- 16Department of Food and Human Nutritional Sciences, The University of Manitoba, Winnipeg, MB, Canada
Background: The COVID-19 pandemic has affected the supply, cost, and demand for certain foods, but it is not clear how these changes have affected food-allergic households.
Objective: To describe the changes in food-related costs that have followed COVID-19, as reported by higher- and lower-income households with a food-allergic member.
Methods: Between May 1-June 30, 2020, Canadian households, with at least one food-allergic member, completed an online survey on food shopping and preparation habits before and during the COVID-19 pandemic. The sample was divided into binary groups, either higher or lower than the sample median income. Data were analyzed using descriptive statistics and multiple regression.
Results: The sample was comprised of 102 participants (i.e., 51/ income group). The three most common food allergies amongst both groups were peanuts, tree nuts and milk. Since the start of the pandemic, both groups reported greater monthly direct grocery costs, although costs amongst the higher-income group were twice as high as the lower-income group ($212.86 vs. $98.89, respectively). Indirect food preparation costs were similarly elevated. Higher-income households with food procurement difficulties reported increased indirect shopping costs following the outbreak of COVID-19, whereas those without such difficulties reported decreased costs. Lower-income households with allergies to milk, wheat, or eggs (i.e., staple allergy) experienced a larger change in indirect food preparation costs following the outbreak of COVID-19 relative to those with other food allergies ($244.58 vs. –$20.28, respectively; p = 0.03).
Conclusion: Both higher and lower income households with food allergy reported greater direct food costs and indirect food preparation costs following the COVID-19. Households with staple allergy and those with difficulties finding their typical food items were particularly affected.
Introduction
For the estimated 7% of families whose children live with food allergy (1), avoidance of the food to which they are allergic is essential to prevent a potentially fatal reaction (2). Owing to the perpetual need for dietary vigilance, children with food allergy and their families report worse health-related quality of life (3, 4) and mental health (5–7) than families not managing this condition. Prior to the COVID-19 pandemic, such vigilance also had substantial costs, including direct costs, such as the excess cost of food, estimated at, $2,500 more per year, on average, compared to families without food allergy, as well as indirect costs, attributable to time and opportunity costs (8).
The COVID-19 pandemic has caused significant changes in how individuals acquire, prepare and consume food. During the early months of the pandemic, supply chains, weakened by travel restrictions, physical distancing requirements, and workplace outbreaks, struggled to keep up with shifting dietary patterns. As a result, consumers reported difficulties finding many grocery items during the initial Spring 2020 wave of COVID-19 (9–11). Since that time, acute food shortages have become less of a concern, but consumers continue to be impacted by higher food prices (12–14). Although reductions in the availability of food and increased food prices likely affect all families, households with a food-allergic member(s) may bare a disproportionate burden given the restricted nature of their diet (15). Moreover, it is possible that the food-related changes that have followed COVID-19 may impact higher and lower income families differently, given their unique needs and financial resources. As such, the current study aimed to describe the changes in food-related costs that have followed COVID-19, as reported by higher and lower income households with a food-allergic member. We also investigated whether certain food allergy or household-level characteristics were predictive of cost changes. We hypothesized that food allergy-related household costs in the early months of the pandemic were higher than those prior to the pandemic.
Methods
Participants were recruited from May 1st to June 30th 2020 through Food Allergy Canada, the national patient organization for those living with food allergy, and through social media. Canadians over the age of 18 years who self-reported a physician-diagnosed food allergy or who were living with someone with a physician-diagnosed food allergy were eligible to participate. Participants were excluded if they had an unclear diagnosis of food allergy, or reported any other chronic disease including, but not limited to celiac disease, diabetes or malignancies. The survey was posted online on food allergy social media pages, and was promoted by Food Allergy Canada, the largest food allergy patient organization in Canada. Participants were asked to complete an online, modified version of the Food Allergy Economic Questionnaire (FA-EcoQ), a validated, self-report measure designed to assess the direct (i.e., out of pocket) and indirect (i.e., loss of time or wages) costs of food allergy (16). Based on the information collected via the FA-EcoQ, the following cost variables (all reported in CAD) were derived:
Change in direct grocery costs: Monthly out-of-pocket grocery expenses during COVID-19 minus monthly out-of-pocket grocery costs prior to the pandemic.
Change in indirect costs: Described in detail elsewhere, (8) indirect costs were calculated by multiplying the number of hours devoted to food preparation and food shopping by the average hourly wage for non-unionized employees in Canada in the year 2020 ($26.27) (17). The time of unemployed respondents was valued at the average hourly minimum wage in Canada ($13.07). Indirect costs were calculated for the period prior to the pandemic and subtracted from pandemic costs to yield a change in food preparation costs variable and a change in food shopping costs variable.
Each of the cost variables were found to have missing data (amounts ranged from 3–16%); therefore, multiple imputation was used to create and analyze 70 datasets. Following imputation, participants were stratified into higher and lower income groups based on whether their monthly income fell above or below the sample median ($5,830 CAD) in order to better understand cost changes across income groups. The sample median was used for stratification not only because the income distribution was positively skewed, but also because it was comparable to the Canadian median ($4,642) (18) and provided two equal income groups. Means ± SDs were used to describe changes in food-related costs during COVID-19. Linear regression was used to identify factors associated with changes in food-related costs after adjusting for covariates. Data were analyzed using Stata Version 16.0 (College Station, TX). All participants provided their informed consent (University of Manitoba Health Research Ethics Board: HS22066).
Results
Participant demographics
In total, 102 patients participants were recruited, corresponding to 51 per income group (Table 1). In both groups, participants were predominantly female (>90%), approximately half reported 3–4 household members, and most managed one food allergy (higher income: 74%; lower income: 86%). The three most common food allergies amongst both groups were peanuts, tree nuts and milk. With consideration to EAI prescription, 90% of higher income families reported a prescription, compared to 71% of lower income families.
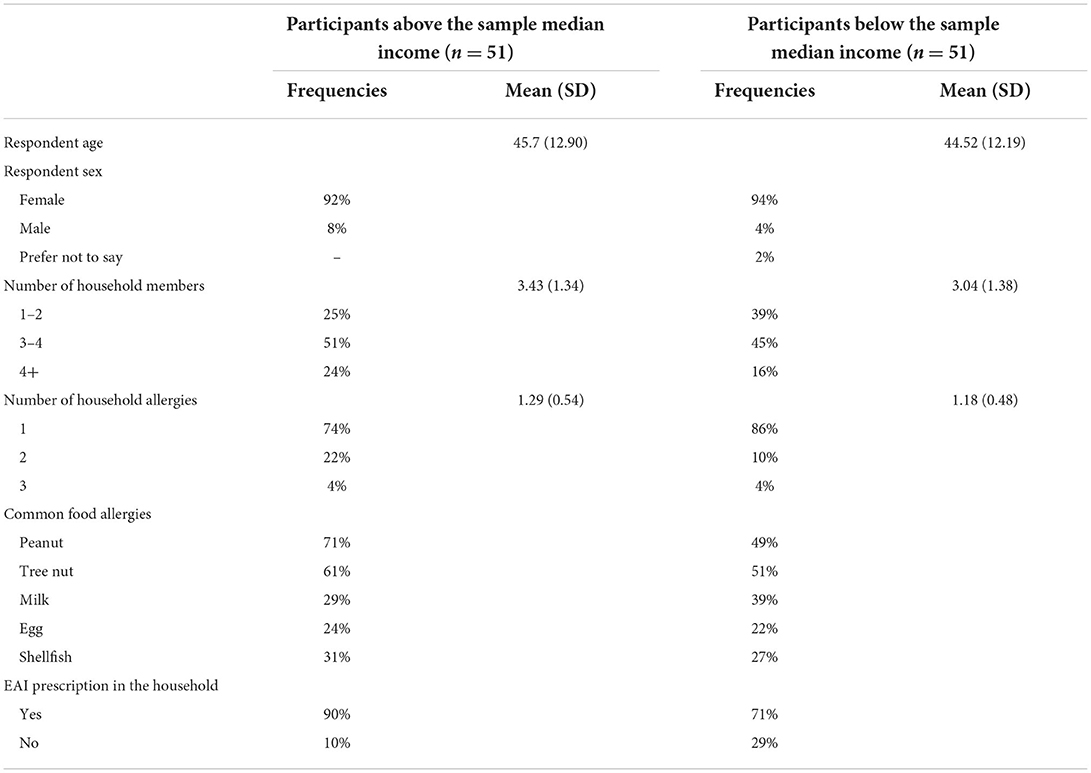
Table 1. Participant characteristics.
Cost comparisons between income groups
In the early months of the COVID-19 pandemic, both higher income and lower income groups reported that they spent more directly on groceries ($212.86 ±335.53 and $98.89 ± 285.56, respectively, per month) and indirectly on food preparation ($272.60 ± 360.36 and $130.23 ± 291.11, respectively) following the outbreak of COVID-19. In contrast, participants in both income groups reported decreased indirect shopping costs (–$14.80 ± 149.23 and; –$19.07 ± 142.44, respectively, per month), on average, over the same period.
Predictors of monthly direct costs
Despite reporting higher total direct costs of $212 per month, on average, neither the type, number of household food allergies, severity of food allergy, nor the unavailability of typical foods, were predictive of greater costs amongst the higher income group (Table 2). A similar pattern was identified amongst lower the income group, except for the unavailability of typical foods, which was associated with, excess costs of $164.30 per month, on average (b=196.25; 95%CI 22.33 – 370.16). By comparison, participants in the lower income group with access to their typical foods reported spending less on food following the outbreak of the pandemic (i.e., -$31.94).
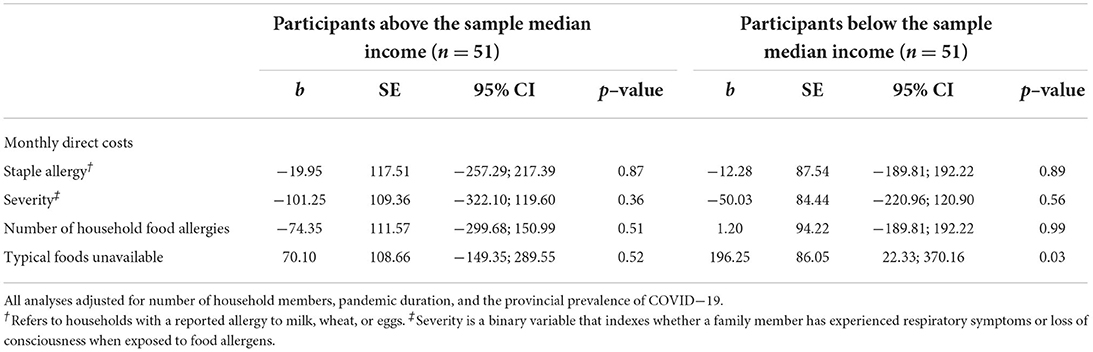
Table 2. Predictors of monthly direct grocery costs among higher and lower income households with food allergy.
Predictors of monthly indirect costs
Both income groups reported decreased indirect shopping costs, but increased food preparation costs in the early months of the pandemic. Amongst each income group, consideration to different types of indirect costs yielded differences (Table 3). With consideration to monthly indirect food preparation costs, no significant differences were found for higher income families, whereas lower income families with an allergy to milk, wheat, or eggs (i.e., staple allergy) experienced a larger change in indirect food preparation costs relative to those with other food allergies ($244.58 vs. –$20.28, respectively; b = 224.30; 95%CI 43.60–405.01, p = 0.03). Lower income families with severe disease reported a smaller change in indirect preparation costs relative those with less severe disease, albeit it did not reach statistical significance ($48.63 vs. $215.09, b = −166.46; 95%CI −334.53 – 1.61; p = 0.06). With consideration to monthly indirect shopping costs, higher income families who had difficulties finding their typical grocery items reported an increase in indirect shopping costs while those without such difficulties reported spending less time shopping ($34.09 vs. –$69.80, respectively; b = 103.89; 95CI 5.47–202.31). No such differences were identified amongst the lower income group.
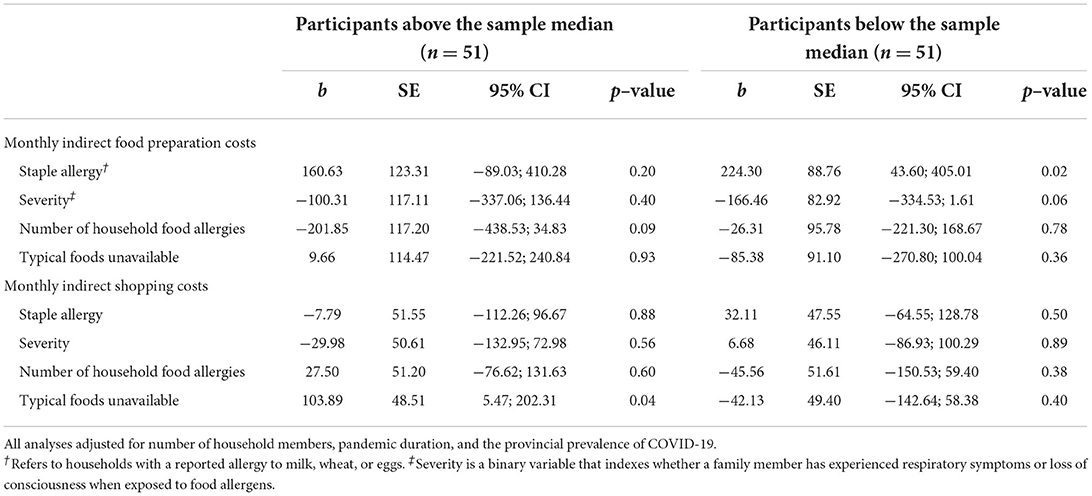
Table 3. Predictors of monthly indirect food preparation and shopping costs among higher and lower income households with food allergy.
Discussion
During the COVID-19 pandemic, families managing food allergy reported higher direct and indirect food costs. However, important differences were noted by income strata. Higher income households reported increases in direct grocery costs twice as high as lower income households. Moreover, higher income households with difficulty procuring their typical foods reported increased indirect shopping costs, whereas trouble obtaining one's typical foods was associated with increased direct food costs for those in the lower income strata. Lastly, lower income households with allergies to staple foods reported increased food preparation costs.
At the time data were collected (between May-June 2020), grocery store visits across Canada were largely limited to one visit or less per week, and while food access was not reported to be problematic amongst the general population, there was a notable lack of availability of canned or frozen fruits and vegetables, and grain products (19). One possible explanation for the increased direct grocery costs among lower income food-allergic families with food procurement difficulties is that these families are obliged to buy more expensive alternatives when faced with product shortages. Unfortunately, for lower income families, the need to purchase more expensive products may cause financial strain, particularly in the current climate of financial uncertainty. In contrast, higher income food-allergic families appear not to experience a significant increase in direct costs in response to product shortages as it is likely that their typical items are already higher-priced. These greater increases in costs amongst higher income families may also reflect differences in baseline (pre-COVID) costs of food, a phenomenon that we previously reported (8).
Higher income families with food procurement difficulties did report greater indirect shopping costs following the outbreak of COVID-19, while lower income families did not. While it is difficult to know what accounts for this discrepancy, it is possible that it reflects the fact that lower wage workers are less likely to be afforded the opportunity to work remotely (20). Consequently, they may be reluctant to devote more time to shopping due to a lack of free-time or a desire to limit their exposure to COVID-19.
Findings from the current study also revealed a greater COVID-19 change in indirect food preparation costs among lower income families with an allergy to milk, wheat, or eggs. Given the ubiquity of these ingredients, it stands to reason that families with staple allergies would be more likely to rely on pre-packaged allergen-friendly products to meet their dietary needs. However, faced with higher grocery prices, lower income families with staple allergies may have shifted their consumption away from these convenient, but often expensive products, toward those requiring more preparation.
While the current study provides preliminary evidence of how the pandemic has affected the food-related costs of higher and lower income food-allergic households, its retrospective nature means that the pre-pandemic cost estimates could have been affected by recall bias. As participants were recruited online, confirmatory allergy testing was not possible. However, online recruitment was initiated on food allergy social media pages and email lists, and thus likely reached the intended audiences. The modest sample size means the study was, unfortunately, underpowered to detect small effect sizes. Given the small sample size and the exploratory nature of the research we decided not to control for family-wise error. However, failing to control for family-wise error does increase the risk of type 1 error. In light of these limitations, future research should utilize more objective measures of food costs and larger samples in order to better understand how the COVID-19 pandemic has affected households with food allergy. Such research is important to ensure that households with food allergy are not unduly affected by future supply chain disruptions, nor unexpected changes in demand. Prior to the COVID-19 pandemic, Canadian households managing food allergy were burdened with excess costs of approximately $200 per month, compared to households not managing food allergy (8). Owing to projected increases in food prices in 2022 (21), a continued focus on the impact of increasing food prices amongst those with medical dietary restrictions, such as food allergy, is warranted. Referrals to food allergy dietitians may be appropriate for families with the financial ability, either through household finances or insurance, to absorb these fees. Additional information, such as food substitutions and low-cost recipes, ought to be offered to families at the time of diagnosis. Finally, allergists are encouraged to be familiar with any food banks in their area that support families with allergy. While the prevalence of food insecurity amongst Canadian families generally has increased since the start of the COVID-19 (22), with the highest prevalence (19–22%) noted amongst households with children (22), families with food allergy are likely to be disproportionately affected, owing to higher food costs and fewer products from which to choose owing to medical dietary restrictions.
In conclusion, both higher and lower income households with food allergy reported greater direct food costs and indirect food preparation costs following the outbreak of COVID-19. Households with staple allergy and those with difficulties finding their typical food items were particularly affected.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by University of Manitoba Health Research Ethics Board: HS22066. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MG performed the statistical analysis and wrote the first draft of the manuscript. CL-C led the French translation of the survey instrument and contributed to the study design. EA, JG, and ES contributed to the study design, provided constructive comments on the manuscript, and including interpretation of the data. MB-S, PB, EC, DC, BP, HK, and JU provided constructive comments on the manuscript and including interpretation of the data. JP led the study design, secured funding for this work, contributed to the statistical analysis, and writing of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Funding for this project was provided by the Canadian Institutes of Health Research through their Early Career Investigator in Maternal, Reproductive, Child and Youth Health Operating Grant, awarded to JP. JP's New Investigator Grant, jointly provided by the Manitoba Medical Services Foundation and the Children's Hospital Research Institute of Manitoba, also helped to support the current study. These funding bodies had no influence on the study design, data collection, analysis and interpretation, or manuscript writing.
Conflict of interest
PB reports personal fees from Novartis, Pfizer, Sanofi, ALK and Aralez, as well as grants from DBV technologies, Regeneron and Sanofi outside the submitted work. EC has received research support from DBV Technologies and has been a member of advisory boards for Pfizer, Pediapharm, Leo Pharma, Kaleo, DBV, AllerGenis, Sanofi Genzyme, Bausch Health, and Avir Pharma. HK has served on the following speakers' bureau and/or advisory boards: AstraZeneca, Aralez, Bausch Health, CSL Behring, GSK, Kaleo, Novartis, Pediapharm, Pfizer, Sanofi, Shire, and Takeda. JU reports research support/grants from Novartis, Regeneron, ALK, DBV, CIHR, and fees from AstraZeneca, Pfizer, ALK Abello, Bausch Health, Kaleo, Food Allergy Canada, all outside the submitted work. JP sits on the steering committee for Canada's National Food Allergy Action Plan and is Section Head, Allied Health, Canadian Society of Allergy and Clinical Immunology.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Clarke AE, Elliott SJ, St Pierre Y, Soller L, La Vieille S, Ben-Shoshan M. Temporal trends in prevalence of food allergy in Canada. J Allergy Clin Immunl Pract. (2020) 8:1428–30.e5. doi: 10.1016/j.jaip.2019.10.021
2. Sicherer SH, Sampson HA. Food allergy: a review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol. (2018) 141:41–58. doi: 10.1016/j.jaci.2017.11.003
3. de Blok BMJ, Dubois AEK. Vlieg-Boerstra BJ, Oude Elberink JNG, Raat H, DunnGalvin A, Hourihane JO'B, Duiverman EJ. Health-related quality of life of food allergic patients: comparison with the general population and other diseases. Allergy. (2010) 65:238–44. doi: 10.1111/j.1398-9995.2009.02121.x
4. Protudjer JLP, Jansson S-A, Östblom E, Heibert Arnlind M, Bengtsson U, Dahlén S-E, et al. Health-related quality of life in children with objectively diagnosed staple food allergy assessed with a disease-specific questionnaire. Acta Paediatr. (2015) 104:1047–54. doi: 10.1111/apa.13044
5. King RM, Knibb RC, Hourihane JO'B. Impact of peanut allergy on quality of life, stress and anxiety in the family. Allergy. (2009) 64:461–8. doi: 10.1111/j.1398-9995.2008.01843.x
6. Lau G-YL, Patel N, Umasunthar T, Gore C, Warner JO, Hanna H, et al. Anxiety and stress in mothers of food-allergic children. Pediatr Allergy Immunol. (2014) 25:236–42. doi: 10.1111/pai.12203
7. Protudjer JLP, Golding MA, Salisbury MR, Abrams EM. Roos LE. High anxiety and health-related quality of life in families with children with food allergy during coronavirus disease 2019. Ann Allergy Asthma Immunol. (2021) 126:83–8. doi: 10.1016/j.anai.2020.09.010
8. Golding MA, Simons E, Abrams EM, Gerdts J, Protudjer JLP. The excess costs of childhood food allergy on Canadian families: a cross-sectional study. Allergy Asthma Clin Immunol. (2021) 17:28. doi: 10.1186/s13223-021-00530-9
9. Canadian Consumers Adapt to COVID-19: A Look at Canadian Grocery Sales up to April 11 (Statistics Canada) (2020).
10. Bogart N. 'Nobody was ready': Retail Council of Canada urges consumers to stop panicking as grocers stripped bare. CTV News. Available online at: https://www.ctvnews.ca/health/coronavirus/nobody-was-ready-retail-council-of-canada-urges-consumers-to-stop-panicking-as-grocers-stripped-bare-1.4851901
11. Kishchuk O. Food Fight: Hoarding, Stockpiling and Panic Buying. Abacus Data. (2020). Available online at: https://abacusdata.ca/food-fight-hoarding-stockpiling-panicbuying/
12. OECD. Food Supply Chains and COVID-19: Impacts and Policy Lessons. OECD Policy Responses to COVID-19. (2020): 11. Available online at: https://www.oecd.org/coronavirus/policy-responses/food-supply-chains-and-covid-19-impacts-and-policy-lessons-71b57aea/
13. Statistics Canada. Consumer Price Index - Food. 18-10-0004-03. Available online at: https://doi.org/10.25318/1810000401-eng https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1810000403
14. Aslam S. Coronavirus pandemic drives food prices up in Canada, expert says. CityNews. 06/030/2020. https://winnipeg.citynews.ca/2020/06/30/coronavirus-food-prices-up-experts/
15. Guillaume JD, Jagai JS, Makelarski JA, Abramsohn EM, Lindau ST, et al. COVID-19-related food insecurity among households with dietary restrictions: a national survey. J Allergy Clin Immunol. (2021) 9:3323–30. doi: 10.1016/j.jaip.2021.06.015
16. Fox M, Voordouw J, Mugford M, Cornelisse J, Antonides G, Frewer L. Social and economic costs of food allergies in europe: development of a questionnaire to measure costs and health utility. Health Serv Res. (2009) 44:1662–78. doi: 10.1111/j.1475-6773.2009.00993.x
17. Statistics Canada. Data From: Table 14-10-0134-01 Average Weekly Earnings, Average Hourly Wage Rate and Average Usual Weekly Hours by Union Status, Annual, Ottawa. (2020).
18. Statistics Canada. Data From: Table 11-10-0190-01 Market Income, Government Transfers, Total Income, Income Tax and After-Tax Income by Economic Family Type, Ottawa (2022).
19. Nielsen DE, Labonté K, Karamanoglu I, Han HY, Tavanaei M, Duhamel P-G, et al. Longitudinal patterns of food procurement over the course of the COVID-19 pandemic: findings from a Canadian online household survey. Front Public Health. (2022). https://doi.org/10.3389/fpubh.2021.752204 doi: 10.3389/fpubh.2021.752204
20. Cetrulo A, Guarascio D, Virgillito ME. The privilege of working from home at the time of social distancing. Intereconomics. (2020) 55:142–7. doi: 10.1007/s10272-020-0891-3
21. Charlebois S, Gerhardt A, Taylor S, Kane M, Keselj V, Fitting E, et al. Canada's Food Price Report. 12th Edition (2022). Available online at: https://cdn.dal.ca/content/dam/dalhousie/pdf/sites/agri-food/Food%20Price%20Report%20-%20EN%202022.pdf (accessed March 29, 2022).
Keywords: food allergy, cost of illness, COVID-19, food-related costs, socio-economic status pandemic-related changes in allergy-friendly food purchasing 2
Citation: Golding MA, Lemoine-Courcelles C, Abrams EM, Ben-Shoshan M, Bégin P, Chan ES, Chu DK, Gerdts JD, Povolo B, Kim H, Simons E, Upton J and Protudjer JLP (2022) Changes in food-related costs during the COVID-19 pandemic among families managing food allergy. Front. Allergy 3:915014. doi: 10.3389/falgy.2022.915014
Received: 10 April 2022; Accepted: 27 June 2022;
Published: 15 July 2022.
Edited by:
William J. Sheehan, Children's National Hospital, United StatesReviewed by:
Maureen Egan Bauer, Children's Hospital Colorado, United StatesJarmila Celakovska, Charles University, Czechia
Ashley Ramos, Children's National Hospital, United States
Copyright © 2022 Golding, Lemoine-Courcelles, Abrams, Ben-Shoshan, Bégin, Chan, Chu, Gerdts, Povolo, Kim, Simons, Upton and Protudjer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael A. Golding, TWljaGFlbC5Hb2xkaW5nQHVtYW5pdG9iYS5jYQ==