
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Aging Neurosci. , 27 February 2025
Sec. Parkinson’s Disease and Aging-related Movement Disorders
Volume 17 - 2025 | https://doi.org/10.3389/fnagi.2025.1455432
This article is part of the Research Topic Function of Vestibular and Auditory Systems in Neurogenerative Disorders View all 6 articles
 Jônatas Augusto Cursiol1
Jônatas Augusto Cursiol1 Paulo Cezar Rocha dos Santos2,3
Paulo Cezar Rocha dos Santos2,3 Victor Spiandor Beretta4
Victor Spiandor Beretta4 Diego Orcioli-Silva5
Diego Orcioli-Silva5 Lucas Simieli1
Lucas Simieli1 Christian Schlenstedt6
Christian Schlenstedt6 Daniel Boari Coelho7
Daniel Boari Coelho7 Fabio Augusto Barbieri1*
Fabio Augusto Barbieri1*Introduction: This study investigated the influence of rhythmic auditory cues (RAC) on gait asymmetry (GA) during unobstructed and obstacle avoidance walking in people with Parkinson’s disease (PD) and neurologically healthy individuals.
Methods: Thirteen individuals with PD (70.33 ± 6.02 years) and 13 healthy controls (CG) (70.77 ± 7.56 years) participated in this study. They performed a total of five trials during unobstructed walking and 10 trials during obstacle walking under each auditory cue condition (without and with RAC). For obstacle walking, five trials were performed with each limb as leading during obstacle avoidance. First, the volunteers performed the trials without RAC. The trial order, unobstructed or obstacle walking, was randomly defined, and the cues (controlled by a metronome) were personalized according to participants’ cadence. The symmetric index of gait parameters was analyzed using 2 × 2 factorial analysis of variance (group and RAC as factors) separately for each gait type (unobstructed and obstructed walking).
Results: A group-by-auditory cue interaction for step velocity (p = 0.027) showed that the PD group exhibited 57.6% reduced asymmetry with RAC during unobstructed walking, with no significant effects observed for the CG. However, RAC had no effect on GA during obstacle avoidance walking in people with PD. Conversely, the CG exhibited 10.5% greater step length asymmetry, 7.1% greater step duration asymmetry, 7.0% greater step velocity asymmetry, and 10.6% greater double support duration asymmetry during obstacle avoidance with RAC (p < 0.001).
Conclusion: We conclude that RAC can reduce GA in people with PD during unobstructed walking, but appear to have no effect and negative effects on GA during obstacle walking in people with PD and neurologically healthy individuals, respectively.
Symmetric onset, which refers to the simultaneous or nearly equal appearance of motor symptoms on both sides of the body, is considered a “red flag” for the diagnosis of Parkinson’s disease (PD) (Postuma et al., 2015). Traditionally, motor symptoms on the initially affected side are more severe compared to the other side (Miller-Patterson et al., 2018). This disparity in motor symptom severity contributes to an asymmetric gait (Barbieri et al., 2017). During unobstructed walking, individuals with PD show increased stride time, swing time (Patoz et al., 2023) and step length asymmetry (Seuthe et al., 2024) compared to neurologically healthy controls. Asymmetry also manifests when crossing an obstacle with asymmetry patterns in the leading and trailing toe clearance (Orcioli-Silva et al., 2020). In fact, obstacle avoidance requires heightened sensorimotor integration, leading to reduced automatic control due to the absence of cognitive compensatory options (Vitório et al., 2023). This increases gait asymmetry compared to unobstructed walking in people with PD (Barbieri et al., 2018a). Although not entirely understood, the asymmetric neural dysfunction in the basal ganglia (Riederer and Sian-Hülsmann, 2012; Van der Hoorn et al., 2011) and the asymmetrical onset of motor symptoms, such as bradykinesia, rigidity and postural control (Peterson and Horak, 2016), may contribute to gait asymmetry in people with PD.
Pharmacological treatment is widely implemented to decrease PD signs and symptoms and also seems to be effective in reducing gait asymmetry (Barbieri et al., 2018a; Warmerdam et al., 2021; Wilson et al., 2020). Barbieri et al. (2018a) showed that antiparkinsonian medication reduced both stride length asymmetry and stride velocity asymmetry during obstacle circumvention in people with PD. However, prolonged use of dopaminergic medication may cause dependency, side effects (e.g., dyskinesia), and reduce the medication’s effectiveness (Olanow and Stocchi, 2018). The effect of medication tends to decrease throughout the years with the progression of the disease, leading to gait impairments such as reduced step length, decreased walking speed, and increased variability in stride time (Wilson et al., 2020). Additionally, Warmerdam et al. (2021) indicated that walking at higher speeds or avoiding obstacles may reduce the effectiveness of dopaminergic medication in people with PD. These conditions increase the complexity of motor control demands, potentially surpassing the compensatory effects of the medication. Hence, complementary interventions have been explored to decrease gait asymmetry, such as the use of additional externally driven stimuli.
Previous studies indicated that rhythmic auditory cues (RAC), defined as external rhythmic stimuli, such as metronome beats or music with a consistent tempo, are a complementary and effective intervention for counteracting PD-related gait impairments (Forte et al., 2021; Ghai et al., 2018; Rinaldi et al., 2019). RAC complement drug treatment for PD by using the constant beat of a metronome or music to improve balance and gait problems (Ginis et al., 2018; Pando-Naude et al., 2024), resulting in improvements in walking velocity and stride length (Belluscio et al., 2021; Minino et al., 2021). Additionally, Rinaldi et al. (2019) observed that RAC could increase muscle activation, potentially improving stability and aiding individuals with PD to safely cross obstacles. Particularly relevant, the use of RAC may minimize PD-related impairments in gait control, reflecting improved obstructed walking performance through greater propulsive braking impulses and shorter time to process obstacle characteristics (Rinaldi et al., 2019), thereby reducing the risk of falls.
From a neurological perspective, RAC’s effects on regulating gait are likely related to improvements in brainstem and cerebellum activations (Devlin et al., 2019), reducing deficits involved in automatic movement in the basal ganglia (Koshimori and Thaut, 2018), and providing phasic cues to the supplementary motor area (Woerd et al., 2017). Prior studies have employed diverse methodologies to apply RAC, such as metronome beats at individualized cadences (Devlin et al., 2019) or music with embedded rhythmic patterns (Koshimori and Thaut, 2018). These stimuli were typically synchronized with participants’ steps to enhance temporal gait parameters, with variations in time, to examine effects during both steady-state and obstacle-crossing scenarios. Our experimental design builds on these findings by specific justification, e.g., testing novel rhythmic patterns, focusing on obstacle negotiation, or exploring underrepresented gait metrics, allowing for a comprehensive evaluation of RAC’s effects on both obstructed and unobstructed walking. Brodie et al. (2015) found that symmetry-matched RAC compensated for unsteady gait in most people with PD without exacerbating gait asymmetry. However, the authors suggested that RAC may be particularly beneficial in cognitively demanding walking tasks, such as obstacle avoidance, which require precise motor coordination and significant attentional resources. Based on this evidence, we hypothesize that RAC will reduce gait asymmetry (e.g., decrease step length and velocity asymmetry) during obstacle avoidance walking, where its effects are more likely to manifest, but not during unobstructed walking, where motor demands are comparatively lower.
The purpose of this study is to investigate whether auditory cueing can reduce gait asymmetry during unobstructed walking and obstacle avoidance in people with PD. The novelty of this study lies in testing the effects of RAC on gait asymmetry during obstacle avoidance in people with PD and matched-control individuals. Understanding how people with PD interact with sensory information during walking is crucial in order to make clinical decision-making for personalized care and design assistive devices.
The analysis with G*Power software (version 3.1; University of Düsseldorf, Dusseldorf, Germany) showed that a sample size of at least 26 individuals (13 in each group) would be necessary to obtain a power of 80% probability to detect a difference of 20% between the two groups for the primary outcome with a type I error of 0.05, based on previously published data (Rinaldi et al., 2019). Hence, a total of 13 individuals with PD (PD group - seven females) and 13 neurologically healthy participants (CG) (eight females) matched by age, height, and body mass participated in this study. Participants with PD and neurologically healthy control participants were recruited from the local community and rehabilitation programs. All participants underwent an interview to collect demographic, sociocultural, and overall health information. An experienced neurologist evaluated and confirmed the diagnosis of PD specifically for this study using the London Brain Bank criteria (Hughes et al., 1992). This evaluation included a detailed clinical assessment and a comprehensive review of medical history to ensure diagnostic accuracy and participant eligibility. Neurologically healthy individuals were screened to ensure the absence of any neurological or motor impairments.
The inclusion criteria were: independent living in the community; ability to walk without the use of any aids; absence of uncontrolled diabetes, hypertension, cardio-respiratory diseases, balance, and vision disorders that may impair locomotion. In addition, for the PD group, the individuals were included in the study if they had a diagnosis of idiopathic PD, were taking their antiparkinsonian medication regularly and with a Hoehn & Yahr stage (H&Y) (Hoehn and Yahr, 1967) 3 or below. Participants with PD were evaluated in the ON-state of medication (1 h after taking their dopaminergic medication).
Initially, an experienced evaluator conducted an anamnesis to characterize both the PD and control groups, focusing particularly on the side where PD symptoms were present. After that, a clinical assessment using the motor section of the Unified Parkinson’s Disease Rating Scale (UPDRS) (Fahn and Elton, 1987; Goetz et al., 2003) and the H&Y scale was applied to determine the motor disease severity and the stage of disease of PD participants, respectively. In addition, cognitive condition screening in both groups was analyzed using the Mini-Mental State Examination (MMSE) (Brucki et al., 2003).
Footedness was assessed in the CG by asking all participants to kick a ball to hit a target. The limb that each individual preferred to kick the ball was considered as the preferred limb. For PD participants, motor UPDRS items 20–23 and 25–26 were used to assess appendicular asymmetry (Araújo-Silva et al., 2022). The most affected limb was determined by calculating the difference between the scores of the right and left limbs in the UPDRS items mentioned above. A positive value indicated the right limb as the most critically affected, whereas negative values indicated the left limb.
Participants performed four walking conditions: unobstructed gait without and with RAC, and obstacle avoidance without and with RAC. A total of five trials were performed in each auditory cue condition for unobstructed walking, and 10 trials were performed in each auditory cue condition for obstacle avoidance - five trials for each limb crossing the obstacle. First, participants performed a trial without RAC. The order of trial conditions was randomly assigned, comprising unobstructed trials, obstacle avoidance trials with the most affected/non-preferred limb, and obstacle avoidance trials with the least affected/preferred limb. The same sequence was maintained for the trials conducted with and without RAC.
Participants were instructed to walk at their self-selected pace with the instruction, “Please walk at your preferred speed, just like you would on the street,” to maintain uniformity across trials. Walking took place on a 10-m wooden pathway covered with a 3 mm thick black rubber carpet. During the obstacle avoidance trials, participants were instructed to avoid contact with a single obstacle (15 cm high, 80 cm wide, and 2 cm thick) placed midway at the 5-m mark. The starting point was adjusted to ensure participants completed at least two strides before encountering the obstacle, ensuring consistency in task complexity and conditions for all participants. The experimental design is demonstrated in Figure 1.
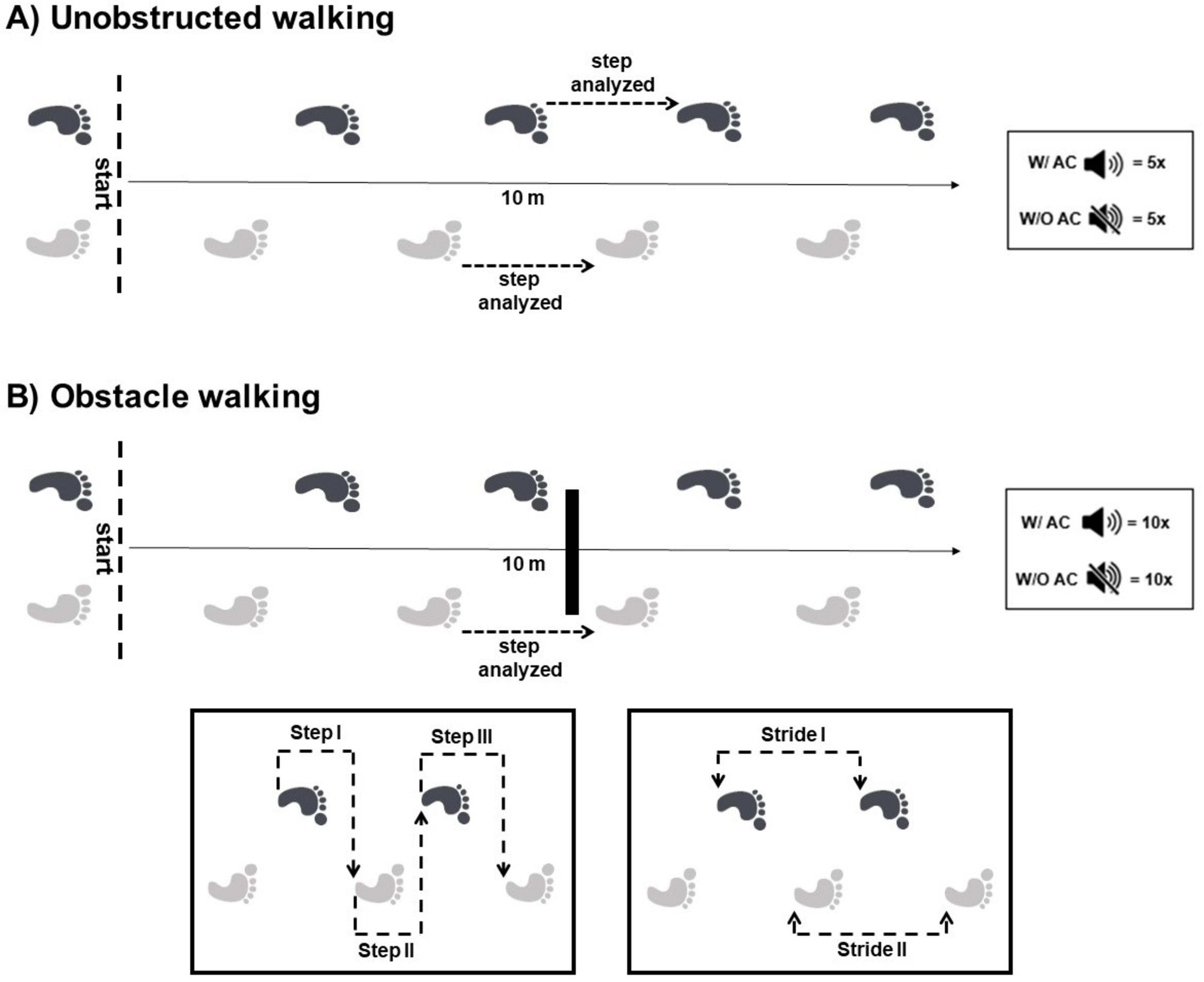
Figure 1. Representative illustration of the steps analyzed in unobstructed walking (A) and obstacle avoidance (B). Obstacle features: 15 cm height × 80 cm width × 2 cm thick. W/ AC, with auditory cue; W/O AC, without auditory cue. A total of five trials in each cue condition were performed in unobstructed walking and 10 trials, five for each limb crossing the obstacle in obstacle walking. The crossing step was analyzed when the leading limb crossed the obstacle.
For auditory cue trials, the cues were personalized for each individual according to the cadence determined by three unobstructed trials performed prior to the start of the experiment. During auditory cue trials, participants were instructed to walk normally, while stepping in time with the metronome beats, trying to synchronize each heel contact with the beat. Participants performed two trials to practice before starting. The trials were stopped and repeated if participants ceased to follow the cues during the experiment.
RAC were delivered using a metronome application on a smartphone, played through a speaker placed at a comfortable distance from the participants. The participants listened to the cues during the walking trials through the speaker, and the volume was adjusted individually to ensure that the cues were clearly audible but not overwhelming. The auditory cues were provided continuously throughout the walking task, starting at the beginning of the trial and stopping once the participant had completed the walking task. The tone of the metronome was consistent throughout, and the frequency was maintained at the specified beats per minute for each group.
The acquisition of kinematic gait parameters was accomplished using a GAITRite® system (CIR System, Clifton, NJ, USA) with a sample rate of 200 Hz. For unobstructed gait, one step from each side of the middle of the pathway was analyzed per trial. Steps were taken from the middle of the 10-m pathway, defined as the section between 2.5 and 7.5 m. This segment was selected to capture steady-state walking, minimizing the influence of acceleration and deceleration phases. The same length was used for all participants to ensure uniformity in the data collection process.
For obstacle avoidance, the crossing step taken by the leading limb during the avoidance maneuver was analyzed in each trial. Length, duration, width, velocity, limb swing duration (as a percentage of step duration), and double support duration (as a percentage of step duration) were calculated for each step.
To investigate the gait asymmetry, we considered the steps with the most and least affected limb (right or left according to UPDRS items) for PD participants as well as preferred and non-preferred limb (right or left according to footedness test) for the control group in each gait type. Although a recent study by Seuthe et al. (2024) suggests a potential mismatch between step length dominance and UPDRS-based dominance, our classification was solely used to ensure consistent averaging for the same leg across multiple trials.
Initially, the average of each gait parameter was calculated for the most and least affected limb in PD participants, and for the preferred and non-preferred limb in the control group. Next, the Symmetry Index (SI) (Herzog et al., 1989) was calculated for each participant based on gait conditions, where MA represents the most affected limb, P is the preferred limb, LA is the least affected limb, and NP is the non-preferred limb. A value of zero for an index indicates no difference between the sides. Since we were not interested in the side effect of asymmetry but in the effect of RAC, we adopted the absolute value of the SI for the statistical analysis. For obstacle avoidance, the average of each gait parameter of the crossing step with the most and least affected limb, or preferred and non-preferred limb, was used to calculate the SI.
Statistical analyses were performed using the JASP (version 0.18.3) for Windows. Normality and homogeneity were checked through the Shapiro-Wilk and Levene’s tests, respectively. To analyze cognitive status, a Student’s t-test for independent samples was employed to compare the PD group with the control group. Additionally, this test was conducted to evaluate potential differences in cadence between the groups under the RAC condition. To analyze the symmetric index of gait parameters, a 2 × 2 factorial analysis of variance (ANOVA) with independent measures was performed, considering the factors “Group” (PD group vs. CG) and “RAC” (with vs. without auditory stimulus). These analyses were conducted separately for unobstructed walking and obstacle-avoidance walking conditions. Post hoc analyses using Tukey’s tests were conducted to explore significant effects. Cohen’s d was used to report the effect size for the Student’s t-test comparing cognitive status between the PD group and the control group, while Eta squared (η2) was used to report effect sizes for the ANOVA results. Statistical significance for all analyses was set at p < 0.05, with effect sizes interpreted as Cohen’s d (>0.2 small effect; >0.5 medium effect; >0.8 large effect) or η2 as small (effect size > 0.01), moderate (effect size > 0.06), or large (effect size > 0.14) (Cohen, 1988).
The group characteristics and clinical variables are detailed in Table 1. Cognitive levels, measured by the Mini Mental State Examination, were comparable between the PD group and CG (t24 = 1.95; p = 0.059, d = 0.783). The average frequencies were 106.92 beats per minute for the PD group and 109.07 beats per minute for the CG.
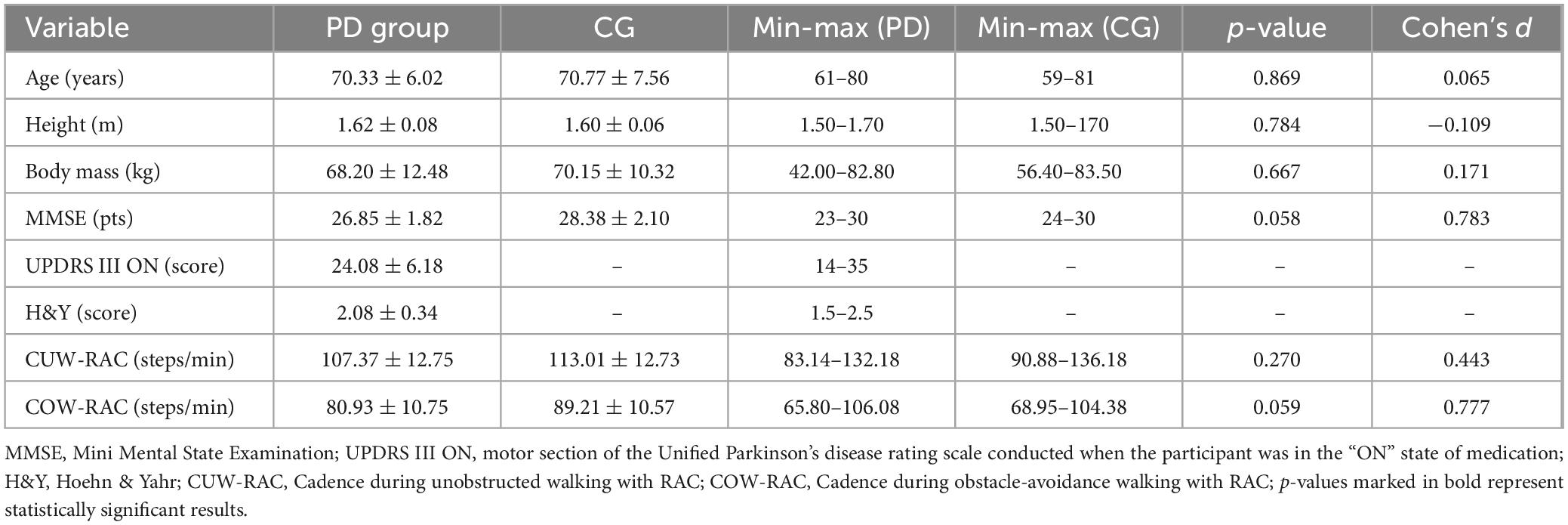
Table 1. Means and standard deviations of characteristics and clinical variables for individuals with PD and the control group.
Means and standard deviations of kinematic gait parameters under each condition (unobstructed vs. obstacle walking), by group (PD vs. CG), side (preferred vs. non-preferred), and cue presence (with vs. without RAC), are presented in Supplementary Tables 1–6. The ANOVAs revealed statistically significant differences in step length, duration, width, velocity, limb swing duration, and double support duration between PD and control groups across walking conditions and limb preferences.
Table 2 presents the symmetry index of the spatial-temporal parameters. The ANOVAs revealed a main effect of group for limb swing [F(1, 26) = 4.013; p = 0.007, η2 = 0.16] and double support duration [F(1, 26) = 7.728; p = 0.008, η2 = 0.14], demonstrating greater asymmetry (44.8% and 40.4% higher, respectively) in the PD group compared to the CG (Figure 2). Furthermore, a group-by-auditory cue interaction for step velocity [F(1, 26) = 5.193; p = 0.027, η2 = 0.10] showed that the PD group exhibited 57.6% reduced asymmetry with RAC, with no significant effects observed for the CG.
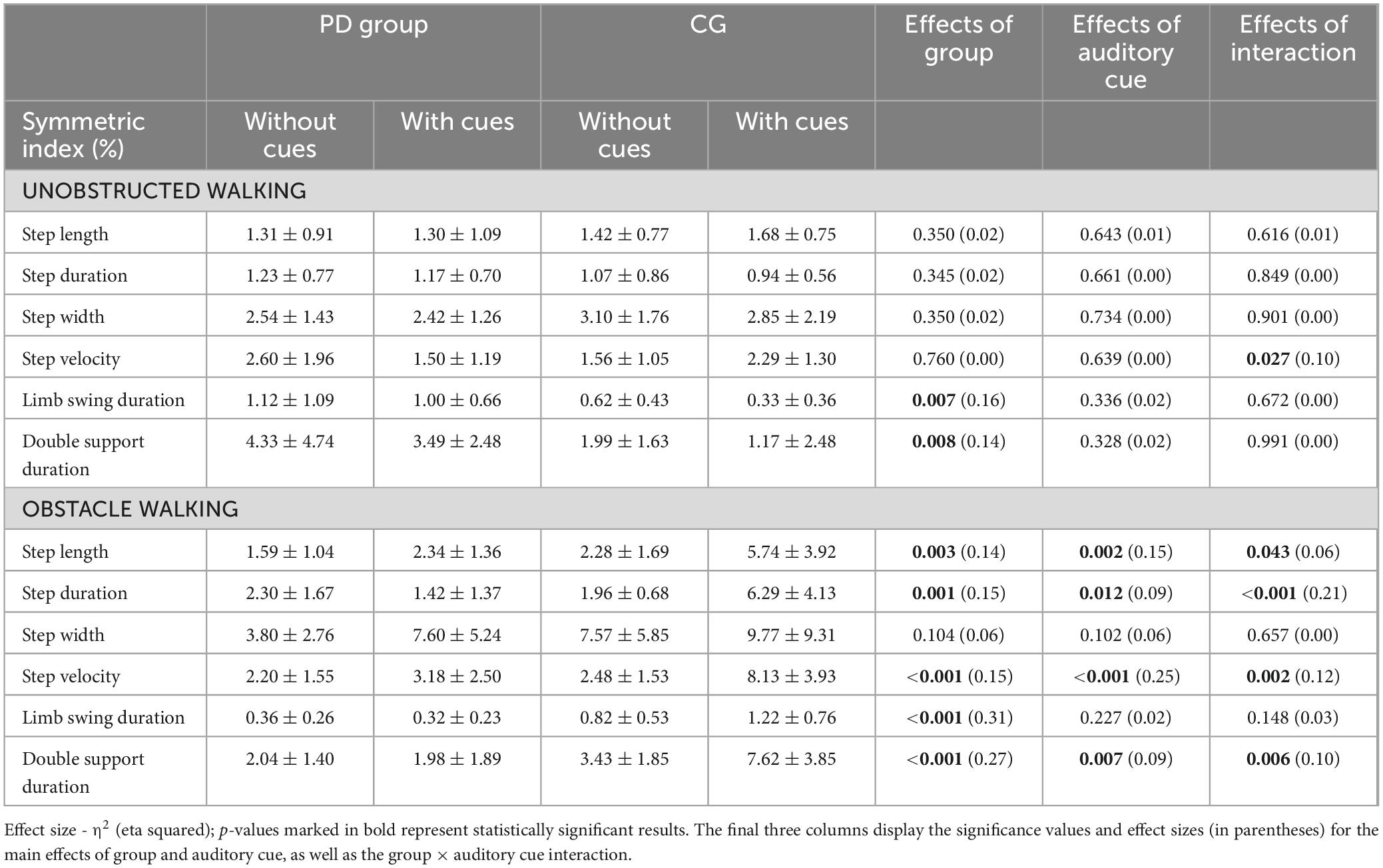
Table 2. The means and standard deviations of the symmetric index (%) of walking parameters in the PD group (PD group) and control group (CG) are presented for unobstructed and obstacle avoidance walking, both without and with auditory cues.
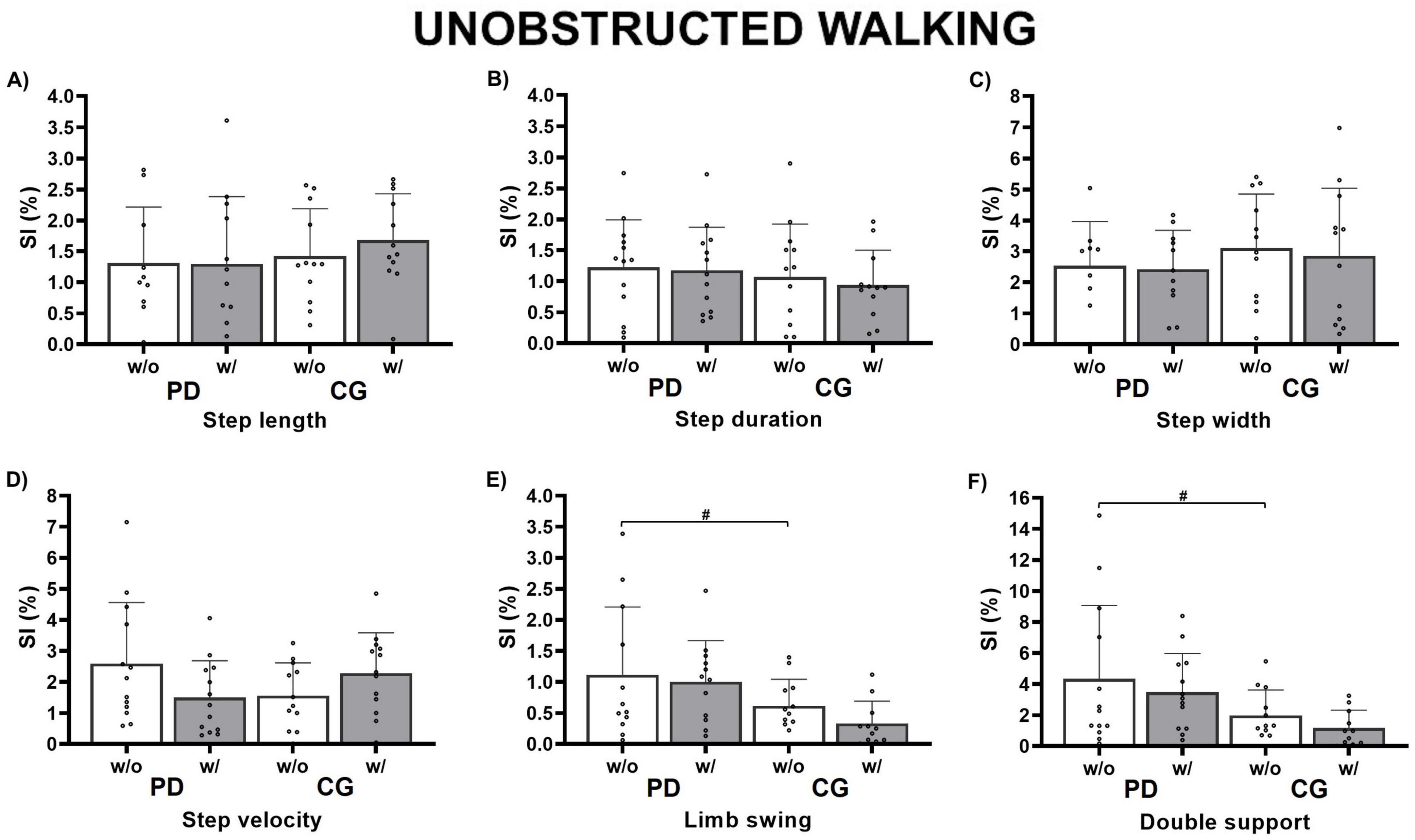
Figure 2. Bar graphs showing the results of the Group × RAC interaction for the unobstructed walking condition. Circles represent individual values. #Indicates significant differences identified in post-hoc comparisons between the groups (PD vs. CG) without auditory cues. SI (%), symmetry index; w/o, without auditory cue (white); w/, with auditory cue (gray); PD, Parkinson’s disease group; CG, control group. Panel (A) Step length; (B) Step duration; (C) Step Width; (D) Step velocity; (E) Limb swing; (F) Double support.
The presence of obstacles significantly increased the asymmetry scores for both PD and control groups (Figure 3). A main effect of group was found for step length [F(1, 26) = 9.93; p = 0.003, η2 = 0.14], step duration [F(1, 26) = 11.75; p = 0.001, η2 = 0.15], step velocity [F(1, 26) = 13.68; p < 0.001, η2 = 0.15], limb swing duration [F(1, 26) = 5.575; p < 0.001, η2 = 0.31], and double support duration [F(1, 26) = 23.06; p < 0.001, η2 = 0.27], indicating that the CG exhibited significantly greater asymmetry compared to the PD group (step length: 59%, step duration: 47%, step velocity: 56%, limb swing duration: 12%, and double support duration: 23% higher, respectively).
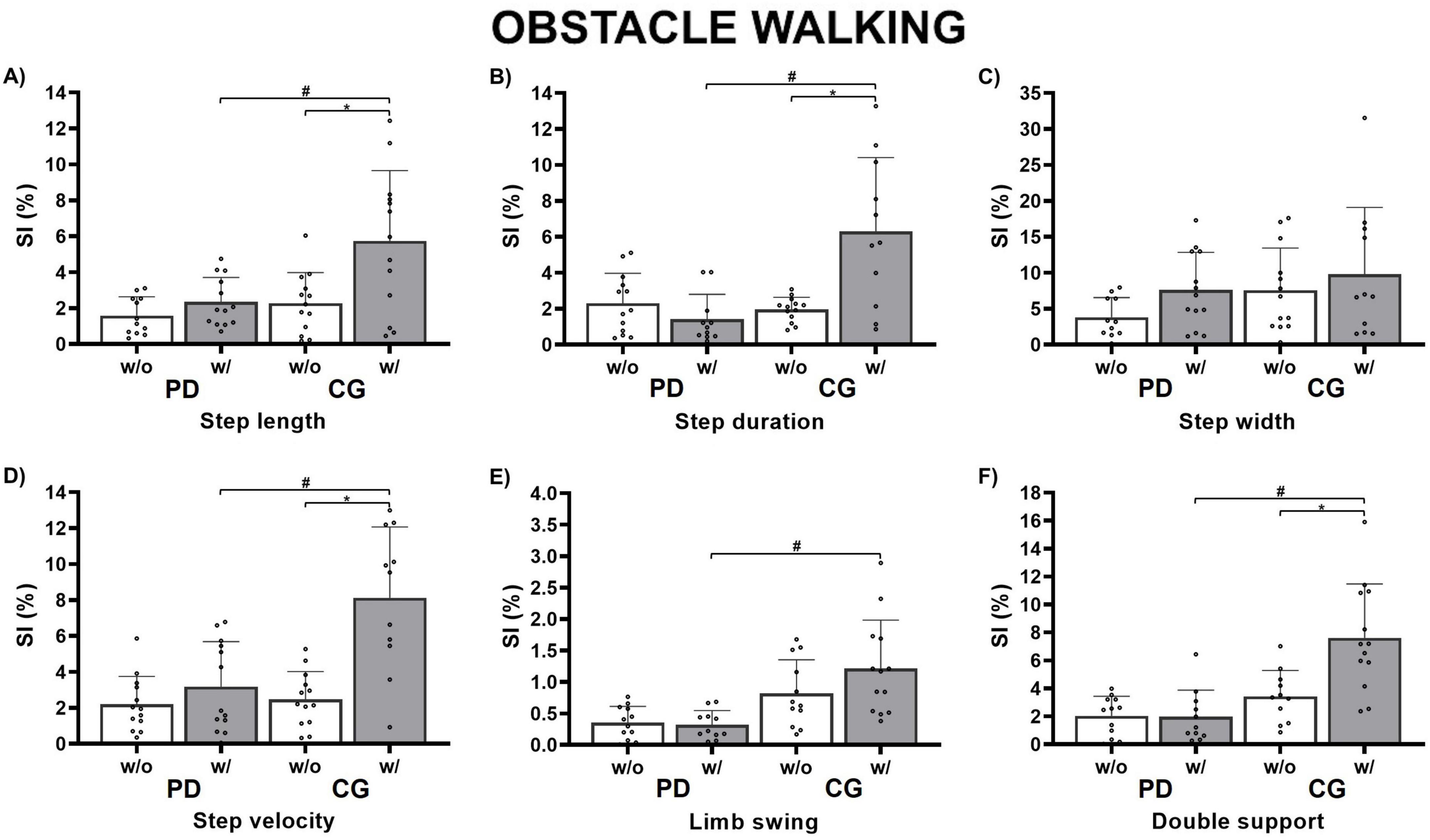
Figure 3. Bar graphs showing the results of the Group × RAC interaction for the obstacle avoidance walking condition. Circles represent individual values. #Indicates significant differences identified in post-hoc comparisons between the groups (PD vs. CG) with auditory cues. *Denotes the main effect of the auditory cue within the group. SI (%), symmetry index; w/o, without auditory cue (white); w/, with auditory cue (gray); PD, Parkinson’s disease group; CG, control group. Panel (A) Step length; (B) Step duration; (C) Step Width; (D) Step velocity; (E) Limb swing; (F) Double support.
A main effect of auditory cue was found for step length [F(1, 26) = 10.54; p = 0.002, η2 = 0.15], step duration [F(1, 26) = 6.852; p = 0.012, η2 = 0.09], step velocity [F(1, 26) = 21.94; p < 0.001, η2 = 0.25], and double support duration [F(1, 26) = 8.004; p = 0.007, η2 = 0.09, moderate], indicating that the CG showed more asymmetry with RAC compared to without RAC (step length: 10.5%, step duration: 6.9%, step velocity: 21.9%, and double support duration: 8.0% higher, respectively).
ANOVAs revealed a group-by-auditory cue interaction for step length [F(1, 26) = 4.325; p = 0.043, η2 = 0.06], step duration [F(1, 26) = 15.58; p < 0.001, η2 = 0.21], step velocity [F(1, 26) = 10.93; p = 0.002, η2 = 0.12], and double support duration [F(1, 26) = 8.468; p = 0.006, η2 = 0.10]. During the condition with RAC, the CG showed 10.9% greater step length asymmetry, 6.9% greater step duration asymmetry, 21.9% greater step velocity asymmetry, and 8.5% greater double support duration asymmetry than the PD group (p < 0.001). Furthermore, the CG exhibited 10.5% greater step length asymmetry, 7.1% greater step duration asymmetry, 7.0% greater step velocity asymmetry, and 10.6% greater double support duration asymmetry during obstacle avoidance with RAC compared to without RAC (p < 0.001), with no significant effects observed for the PD group.
We investigated whether rhythmic auditory cues reduce gait asymmetry during unobstructed and obstacle avoidance walking in people with PD and neurologically healthy individuals. Interestingly, our hypothesis was only partially supported. Although RAC decreased step velocity asymmetry during unobstructed walking in people with PD, they had no effect on gait asymmetry during obstacle avoidance walking. Additionally, one unexpected finding was that RAC during obstacle avoidance increased asymmetry in step length, duration, velocity, and double support duration in neurologically healthy individuals. Our results extend the current literature, suggesting that RAC represent an effective strategy to reduce gait asymmetry in people with PD during unobstructed walking, without affecting gait asymmetry during obstacle avoidance. These findings may have significant implications for planning gait interventions in people with PD.
RAC significantly improved gait asymmetry in people with PD during unobstructed walking, notably reducing step velocity asymmetry (η2 = 0.10, moderate). Our findings are in line with previous research and highlight the effectiveness of RAC in improving gait in people with PD. RAC, utilized through a metronome or via music, have been recommended for reducing gait impairments in people with PD (Forte et al., 2021; Ghai et al., 2018; Rinaldi et al., 2019), potentially enhancing balance (Pando-Naude et al., 2024), walking speed, and stride length (Belluscio et al., 2021; Minino et al., 2021) by increasing muscle activation (Rinaldi et al., 2019) during unobstructed walking. The key neurophysiological mechanism behind this effectiveness is that external cues can redirect neural circuits from those that are more affected to those that are not, leading to a shift from habitual to goal-directed (Redgrave et al., 2010). RAC, in particular, perform an executive role in facilitating attention focus on gait and a stabilizing role in reducing variability while improving spatiotemporal gait parameters (Ginis et al., 2018). Moreover, RAC can also reduce gait asymmetry in individuals with PD by enhancing external timing, motor planning, and sensory integration (Ghai et al., 2018). Previous theories suggest that RAC may act as an external generator, optimizing motor execution by recalibrating predictions based on sensory consequences (Harrison and Earhart, 2023; Izawa et al., 2012).
Using RAC can be a beneficial strategy for dealing with the asymmetric neural neurodegeneration seen in PD. It induces functional asymmetry between hemispheres, with a relative reduction of neural excitability in the most affected hemisphere and an apparent increase in the least affected one (Claassen et al., 2016; Riederer and Sian-Hülsmann, 2012), as well as reduced transcallosal sensorimotor structural connectivity (Fling et al., 2018). In a previous study of our group, we showed that people with PD presented asymmetric cortical activity behavior during gait initiation, with no asymmetry in anticipatory postural adjustments (Faria et al., 2023). We interpreted that higher asymmetry in cortical activity was an adaptive mechanism to improve motor behavior (specifically, gait initiation), as damaged areas of the most affected hemisphere are substituted by residual networks within both hemispheres (Berenguer-Rocha et al., 2020; Brain et al., 2020; Knights et al., 2021; Peterson and Fling, 2018). Therefore, in the current study, we suggest that RAC can also have a positive impact on brain activity, functionally remapping from degenerated areas onto homologous areas within the hemisphere experiencing less degeneration (Berenguer-Rocha et al., 2020). Additionally, RAC are likely to enhance the activity of the brainstem and cerebellum (Devlin et al., 2019), mitigating deficits related to automatic movement control in the basal ganglia (Koshimori and Thaut, 2018), providing temporal cues to the supplementary motor area (Woerd et al., 2017), and consequently reducing gait asymmetry.
The effect on step velocity is intriguing as it encompasses both the spatial and temporal aspects of gait. Gait velocity is determined by the ratio of step length to step duration. Thus, one may argue that a reduction in step velocity asymmetry can indicate a decrease in either step length asymmetry, step duration asymmetry, or both. While step velocity asymmetry tends to worsen with age to compensate for the reduction in step length (Forte et al., 2021), our study demonstrates that RAC can be effective in promoting gait symmetry in people with PD during unobstructed walking. These findings offer novel insights for gait interventions in people with PD.
RAC did not affect obstacle avoidance during walking in people with PD. Therefore, it seems that RAC do not interfere with gait asymmetry during obstacle avoidance in people with PD. Obstacle avoidance represents a challenging task that is likely to increase gait asymmetry in both people with PD and neurologically healthy individuals (Barbieri et al., 2018b). Although previous studies have shown that RAC during obstacle avoidance walking benefit both people with PD and neurologically healthy individuals to safely overcome obstacles due to better positioning of the feet on the ground, stability and ability to maintain synchronization with RAC (Rinaldi et al., 2019), our findings indicated that they do not appear to have an effect on gait asymmetry.
One possible explanation is that due to the increase in difficulty, complexity, motor cortex activity and cognitive resources required during obstacle avoidance (Ambike et al., 2021), PD participants probably prioritized the motor task and ignored the external cues, increasing the attention control to perform obstacle avoidance. A possible additional explanation may be related to the weight of sensory information attributed to vision. According to Faria et al. (2023), obstacles up to 15 cm high, such as the one used in our study, act as a visual cue during the gait of people with PD. In this case, visual information is utilized to track the characteristics of the obstacle in order to make adjustments to safely prevent it (Santos et al., 2010). Furthermore, Föcker et al. (2022) elucidated that the visual signal can make it difficult to integrate an auditory cue. Therefore, due to the risk and importance of spatial variables when negotiating with an obstacle to avoid tripping, visual information may have had more relevance/weight compared to auditory information. However, our findings should not be interpreted negatively. On the contrary, these results may serve as helpful indicators for implementing the RAC approach in gait intervention, considering that RAC do not interfere with gait asymmetry and promote other benefits in gait during obstacle avoidance in people with PD.
An intriguing finding of this study is that, for certain gait parameters such as step velocity and step length the PD group exhibited lower asymmetry values than the control group during obstacle avoidance walking, particularly in the absence of RAC. One possible explanation for this observation is that individuals with PD are more accustomed to managing motor deficits and may inherently adopt compensatory mechanisms to maintain balance and motor control, even without external cues. One important aspect here is that our sample is composed of adults over 65 years old, which may be minimally affected by the aging process in motor and non-motor variables. It may suggest that the gait pattern is disrupted during obstacle avoidance in older adults, likely increasing gait variability (Baker et al., 2008; Harrison and Earhart, 2023). Harrison and Earhart (2023), in a recent systematic review, found similar findings for gait variability during rhythmic RAC: from 11 papers with neurologically healthy older adults, 10 papers found no or negative (higher) effects on gait variability. The authors suggest that for healthy older adults with minimal gait impairment, RAC may disrupt the normal gait pattern, potentially relating to increased attentional or cognitive demands in order to synchronize gait to an outside source.
The increase in gait asymmetry in the CG can be explained by the fact that it is more challenging for older adults to synchronize their gait with a rhythm as it is an action that can lead to dual-task interference that slows gait and shortens steps (Roberts et al., 2021). Very likely, RAC during obstacle avoidance increase the robustness of the task, which may interfere with well-learned movement patterns in people without basal ganglia deficits and perturb the functioning of internal mechanisms (Brodie et al., 2015). Nevertheless, the study’s major limitation was the lack of specificity in determining the metronome pace for obstacle walking, potentially causing discrepancies between unobstructed and obstacle situations. This may have interfered with the obstacle walking results. Future studies should confirm auditory cue frequency separately for each condition. It is possible that the CG walked faster during unobstructed walking, which may have been too fast to maintain during obstacle avoidance, leading to increased asymmetry. The CG might have adjusted their gait rhythm during obstacle avoidance, possibly changing the rhythm only on the non-preferred side, contributing to gait asymmetry.
Other limitations of our study should be mentioned. First, participants were restricted to those with mild to moderate PD. As demonstrated by Lirani-Silva et al. (2019), the benefits of RAC increase as diseases progress. Future research could include people with more severe PD (H&Y ≥ 3), who experience freezing of gait with and without medication, and those with greater gait asymmetry. Furthermore, gait parameters did not demonstrate any significant changes in the auditory cue condition. Although we observed significant changes in certain gait parameters, such as step velocity asymmetry during unobstructed walking in the PD group, other parameters like step length and step duration did not demonstrate significant changes in response to RAC. This suggests that RAC may not uniformly affect all gait parameters and highlights the complexity of gait modulation in different walking conditions. Even though a single session of auditory cue administration may improve gait asymmetry in people with PD (Belluscio et al., 2021), familiarization and longer administration of auditory cue training could be necessary to observe significant improvements in spatiotemporal gait parameters in PD.
We conclude that even though RAC demonstrate a beneficial effect on gait asymmetry during unobstructed walking in people with PD, their impact on gait asymmetry during obstacle avoidance is negligible in this population. Interestingly, in neurologically healthy older adults, RAC during obstacle avoidance may disrupt rhythmicity and contribute to increased gait asymmetry. These conclusions suggest that while RAC can enhance gait symmetry in certain conditions, their efficacy and potential disturbances vary across different walking contexts and neurological statuses.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the research ethics committee of the São Paulo State University at Rio Claro - Brazil (#0227/2013). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JC: Data curation, Writing – original draft, Writing – review and editing. PS: Conceptualization, Methodology, Writing – review and editing. VB: Conceptualization, Methodology, Writing – review and editing. DO-S: Conceptualization, Methodology, Writing – review and editing. LS: Conceptualization, Methodology, Writing – review and editing. CS: Supervision, Writing – original draft, Writing – review and editing. DC: Supervision, Writing – original draft, Writing – review and editing. FB: Conceptualization, Data curation, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants #22/02971-2 and #12/24040-9 from São Paulo Research Foundation (FAPESP), #88881.800232/2022-01 from CAPES/Alexander von Humboldt Foundation, and IDOR/Pioneer Science Initiative (www.pioneerscience.org). This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior in Brasil (CAPES) - Finance Code 001 and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). The funders played no role in the design, data collection, analysis and interpretation of data, or the writing process of this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2025.1455432/full#supplementary-material
Ambike, S., Penedo, T., Kulkarni, A., Balistieri, F. S., and Barbieri, F. A. (2021). Step length synergy while crossing obstacles is weaker in patients with Parkinson’s disease. Gait Posture 84, 340–345. doi: 10.1016/j.gaitpost.2021.01.002
Araújo-Silva, F., Santinelli, F. B., Felipe, L., Imaizumi, I., Silveira, A. P. B., Vieira, H. P., et al. (2022). Temporal dynamics of cortical activity and postural control in response to the first levodopa dose of the day in people with Parkinson’s disease. Brain Res. 1775, 1–11. doi: 10.1016/j.brainres.2021.147727
Baker, K., Rochester, L., and Nieuwboer, A. (2008). The effect of cues on gait variability - Reducing the attentional cost of walking in people with Parkinson’s disease. Parkinsonism Relat. Disord. 14, 314–320. doi: 10.1016/j.parkreldis.2007.09.008
Barbieri, F. A., Fiorelli, C. M., Penedo, T., Paula, P. H. A., Simieli, L., Moretto, G. F., et al. (2017). “Parkinson’s disease and gait asymmetry,” in Locomotion and Posture in Older Adults: The Role of Aging and Movement Disorders, eds F. A. Barbieri and R. Vitório (Berlin: Springer), 161–175. doi: 10.1007/978-3-319-48980-3_10
Barbieri, F. A., Polastri, P. F., Gobbi, L. T. B., Simieli, L., Pereira, V. I. A., Baptista, A. M., et al. (2018a). Obstacle circumvention and eye coordination during walking to least and most affected side in people with Parkinson’s disease. Behav. Brain Res. 346, 105–114. doi: 10.1016/j.bbr.2017.11.032
Barbieri, F. A., Simieli, L., Orcioli-Silva, D., Baptista, A. M., Borkowske Pestana, M., Spiandor Beretta, V., et al. (2018b). Obstacle avoidance increases asymmetry of crossing step in individuals with Parkinson’s disease and neurologically healthy individuals. J. Motor Behav. 50, 17–25. doi: 10.1080/00222895.2016.1271303
Belluscio, V., Iosa, M., Vannozzi, G., Paravati, S., and Peppe, A. (2021). Auditory cue based on the golden ratio can improve gait patterns in people with Parkinson’ s disease. Sensors 21, 1–12. doi: 10.3390/s21030911
Berenguer-Rocha, M., Baltar, A., Rocha, S., Shirahige, L., Brito, R., Monte-silva, K., et al. (2020). Interhemispheric asymmetry of the motor cortex excitability in stroke: Relationship with sensory-motor impairment and injury chronicity. Neurol. Sci. 41, 2591–2598. doi: 10.1007/s10072-020-04350-4
Brain, A., Hill, C., Gemmert, A. W. A., Van, Fang, Q., Hou, L., et al. (2020). Asymmetry in the aging brain: A narrative review of cortical activation patterns and implications for motor function. Laterality 25, 413–429. doi: 10.1080/1357650X.2019.1707219
Brodie, M. A. D., Dean, R. T., Beijer, T. R., Canning, C. G., Smith, S. T., Menant, J. C., et al. (2015). Symmetry matched auditory cues improve gait steadiness in most people with Parkinson’s disease but not in healthy older people. J. Parkinson’s Dis. 5, 105–116. doi: 10.3233/JPD-140430
Brucki, S. M. D., Nitrini, R., Caramelli, P., Bertolucci, P. H. F., and Okamoto, I. H. (2003). Suggestions for utilization of the mini-mental state examination in Brazil. Arquivos Neuro-Psiquiatria 61, 777–781. doi: 10.1590/S0004-282X2003000500014
Claassen, D. O., McDonell, K. E., Donahue, M., Rawal, S., Wylie, S. A., Neimat, J. S., et al. (2016). Cortical asymmetry in Parkinson’s disease: Early susceptibility of the left hemisphere. Brain Behav. 6:e00573. doi: 10.1002/brb3.573
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences. Mahwah, NJ: Lawrence Erlbaum.
Devlin, K., Alshaikh, J. T., and Pantelyat, A. (2019). Music therapy and music-based interventions for movement disorders. Curr. Neurol. Neurosci. Rep. 19, 1–13.
Fahn, S., and Elton, R. (1987). “UPDRS program members. Unified parkinsons disease rating scale,” in Recent Developments in Parkinsons Disease, 2nd Edn, eds F. S. C. Marsden, M. Goldstein, and D. Calne (London: Macmillan Healthcare Information), 153–163.
Faria, M. H., Simieli, L., Rietdyk, S., Penedo, T., Santinelli, F. B., and Barbieri, F. A. (2023). (A)symmetry during gait initiation in people with Parkinson’s disease: A motor and cortical activity exploratory study. Front. Aging Neurosci. 15:1142540. doi: 10.3389/fnagi.2023.1142540
Fling, B. W., Curtze, C., and Horak, F. B. (2018). Gait asymmetry in people with Parkinson’s disease is linked to reduced integrity of callosal sensorimotor regions. Front. Neurol. 9:215. doi: 10.3389/fneur.2018.00215
Föcker, J., Atkins, P., Vantzos, F.-C., Wilhelm, M., and Schenk, T. (2022). Exploring the effectiveness of auditory, visual, and audio-visual sensory cues in a multiple object tracking environment. Attent. Percept. Psychophys. 84, 1611–1624. doi: 10.3758/s13414-022-02492-5
Forte, R., Tocci, N., and De Vito, G. (2021). The impact of exercise intervention with rhythmic auditory stimulation to improve gait and mobility in parkinson disease: An umbrella review. Brain Sci. 11:685. doi: 10.3390/brainsci11060685
Ghai, S., Ghai, I., Schmitz, G., and Effenberg, A. O. (2018). Effect of rhythmic auditory cueing on parkinsonian gait: A systematic review and meta-analysis. Sci. Rep. 8:506. doi: 10.1038/s41598-017-16232-5
Ginis, P., Nackaerts, E., Nieuwboer, A., and Heremans, E. (2018). Cueing for people with Parkinson’s disease with freezing of gait: A narrative review of the state-of-the-art and novel perspectives. Ann. Phys. Rehabil. Med. 61, 407–413. doi: 10.1016/j.rehab.2017.08.002
Goetz, C. G., Poewe, W., Rascol, O., Sampaio, C., Stebbins, G. T., Fahn, S., et al. (2003). The unified Parkinson’s disease rating scale (UPDRS): Status and recommendations. Movement Disord. 18, 738–750.
Harrison, E. C., and Earhart, G. M. (2023). The effect of auditory cues on gait variability in people with Parkinson’s disease and older adults: A systematic review. Neurodegenerative Dis. Manag. 13, 113–128. doi: 10.2217/nmt-2021-0050
Herzog, W., Nigg, B. M., Read, L. J., and Olsson, E. (1989). Asymmetries in ground reaction force patterns in normal human gait. Med. Sci. Sports Exerc. 21, 110–114.
Hoehn, M. M., and Yahr, M. D. (1967). Parkinsonism: Onset, progression, and mortality. Neurology 17, 427–442. doi: 10.1212/WNL.17.5.427
Hughes, A. J., Daniel, S. E., Kilford, L., and Lees, A. J. (1992). Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 55, 181–184. doi: 10.1136/jnnp.55.3.181
Izawa, J., Criscimagna-Hemminger, S. E., and Shadmehr, R. (2012). Cerebellar contributions to reach adaptation and learning sensory consequences of action. J. Neurosci. 32, 4230–4239. doi: 10.1523/JNEUROSCI.6353-11.2012
Knights, E., Morcom, A. M., and Henson, R. N. (2021). Does hemispheric asymmetry reduction in older adults in motor cortex reflect compensation? J. Neurosci. 41, 9361–9373. doi: 10.1523/JNEUROSCI.1111-21.2021
Koshimori, Y., and Thaut, M. H. (2018). Future perspectives on neural mechanisms underlying rhythm and music based neurorehabilitation in Parkinson’s disease. Ageing Res. Rev. 47, 133–139. doi: 10.1016/j.arr.2018.07.001
Lirani-Silva, E., Lord, S., Moat, D., Rochester, L., and Morris, R. (2019). Auditory cueing for gait impairment in persons with Parkinson disease: A pilot study of changes in response with disease progression. J. Neurol. Phys. Therapy 43, 50–55. doi: 10.1097/NPT.0000000000000250
Miller-Patterson, C., Buesa, R., McLaughlin, N., Jones, R., Akbar, U., and Friedman, J. H. (2018). Motor asymmetry over time in Parkinson’s disease. J. Neurol. Sci. 393, 14–17. doi: 10.1016/j.jns.2018.08.001
Minino, R., Lopez, E. T., Sorrentino, P., Rucco, R., Lardone, A., Pesoli, M., et al. (2021). The effects of different frequencies of rhythmic acoustic stimulation on gait stability in healthy elderly individuals: A pilot study. Sci. Rep. 11:19530. doi: 10.1038/s41598-021-98953-2
Olanow, C. W., and Stocchi, F. (2018). Levodopa: A new look at an old friend. Movement Disord. 33, 859–866. doi: 10.1002/mds.27216
Orcioli-Silva, D., Barbieri, F. A., dos Santos, P. C. R., Beretta, V. S., Simieli, L., Vitorio, R., et al. (2020). Double obstacles increase gait asymmetry during obstacle crossing in people with Parkinson’s disease and healthy older adults: A pilot study. Sci. Rep. 10:2272. doi: 10.1038/s41598-020-59266-y
Pando-Naude, V., Jespersen, K. V., Johnsen, E., and Vuust, P. (2024). Rhythmic auditory stimulation for motor rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2:CD015759. doi: 10.1002/14651858.CD015759
Patoz, A., Malatesta, D., and Burtscher, J. (2023). Isolating the speed factor is crucial in gait analysis for Parkinson’s disease. Front. Neurosci. 17:1119390. doi: 10.3389/fnins.2023.1119390
Peterson, D. S., and Fling, B. W. (2018). How changes in brain activity and connectivity are associated with motor performance in people with MS. NeuroImage Clin. 17, 153–162. doi: 10.1016/j.nicl.2017.09.019
Peterson, D. S., and Horak, F. B. (2016). Neural control of walking in people with parkinsonism. Physiology 31, 95–107. doi: 10.1152/physiol.00034.2015
Postuma, R. B., Berg, D., Stern, M., Poewe, W., Olanow, C. W., Oertel, W., et al. (2015). MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 30, 1591–1601. doi: 10.1002/mds.26424
Redgrave, P., Rodriguez, M., Smith, Y., and Rodriguez-oroz, M. C. (2010). Goal-directed and habitual control in the basal ganglia: Implications for Parkinson’s disease. Nat. Rev. Neurosci. 11, 760–772. doi: 10.1038/nrn2915.Goal-directed
Riederer, P., and Sian-Hülsmann, J. (2012). The significance of neuronal lateralisation in Parkinson’s disease. J. Neural Transmission 119, 953–962. doi: 10.1007/s00702-012-0775-1
Rinaldi, N. M., Pereira, M. P., Formaggio, P. M., Morais, L. C., and Gobbi, L. T. B. (2019). Auditory cues assist patients with Parkinson’s disease (on and off L-dopa) during obstacle crossing. Rev. Brasileira Educação Física Esporte 33, 333–343. doi: 10.11606/issn.1981-4690.v33i3p333-343
Roberts, B. S., Ready, E. A., and Grahn, J. A. (2021). Musical enjoyment does not enhance walking speed in healthy adults during music-based auditory cueing. Gait Posture 89, 132–138. doi: 10.1016/j.gaitpost.2021.04.008
Santos, L. C., Moraes, R., and Patla, A. E. (2010). Visual feedforward control in human locomotion during avoidance of obstacles that change size. Motor Control 14, 424–439. doi: 10.1123/mcj.14.4.424
Seuthe, J., Hermanns, H., Hulzinga, F., D’Cruz, N., Deuschl, G., Ginis, P., et al. (2024). Gait asymmetry and symptom laterality in Parkinson’s disease: Two of a kind? J. Neurol. 271, 4373–4382. doi: 10.1007/s00415-024-12379-0
Van der Hoorn, A., Bartels, A. L., Leenders, K. L., and de Jong, B. M. (2011). Handedness and dominant side of symptoms in Parkinson’s disease. Parkinson. Relat. Disord. 17, 58–60. doi: 10.1016/j.parkreldis.2010.10.002
Vitório, R., Lirani-Silva, E., Orcioli-Silva, D., Beretta, V. S., and Gobbi, A. S. O. T. B. (2023). Electrocortical dynamics of usual walking and the planning to step over obstacles in Parkinson’s disease. Sensors 23, 1–13. doi: 10.3390/s23104866
Warmerdam, E., Romijnders, R., Hansen, C., Elshehabi, M., Zimmermann, M., Metzger, F. G., et al. (2021). Arm swing responsiveness to dopaminergic medication in Parkinson’s disease depends on task complexity. Npj Parkinson’s Dis. 7:89. doi: 10.1038/s41531-021-00235-1
Wilson, J., Alcock, L., Yarnall, A. J., Lord, S., Lawson, R. A., Morris, R., et al. (2020). Gait progression over 6 years in Parkinson’s disease: Effects of age, medication, and pathology. Front. Aging Neurosci. 12:577435. doi: 10.3389/fnagi.2020.577435
Keywords: walking, rhythmic auditory cueing, rehabilitation, symmetry, neurodegenerative disease, movement disorders
Citation: Cursiol JA, dos Santos PCR, Beretta VS, Orcioli-Silva D, Simieli L, Schlenstedt C, Coelho DB and Barbieri FA (2025) Rhythmic auditory cues improve gait asymmetry during unobstructed walking in people with Parkinson’s disease but have no effect on obstacle avoidance - AsymmGait-Parkinson study. Front. Aging Neurosci. 17:1455432. doi: 10.3389/fnagi.2025.1455432
Received: 26 June 2024; Accepted: 31 January 2025;
Published: 27 February 2025.
Edited by:
Tatyana Yakusheva, Washington University in St. Louis, United StatesReviewed by:
Kyoung Shin Park, Emory University, United StatesCopyright © 2025 Cursiol, dos Santos, Beretta, Orcioli-Silva, Simieli, Schlenstedt, Coelho and Barbieri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabio Augusto Barbieri, ZmFiaW8uYmFyYmllcmlAdW5lc3AuYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.