
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 28 April 2022
Sec. Obstetrics and Gynecological Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.888281
This article is part of the Research Topic Changing Backgrounds and Groundbreaking Changes: Gynecological surgery in the third decade of the 21st century View all 11 articles
 Shoufeng Zhang1†
Shoufeng Zhang1† Zhiyong Dong2†
Zhiyong Dong2† Junling Liu2†
Junling Liu2† Zhenyue Qin1
Zhenyue Qin1 Huihui Wang1Mingyue Bao1Weiwei Wei2Ruxia Shi2
Huihui Wang1Mingyue Bao1Weiwei Wei2Ruxia Shi2 Jiming Chen2*Bairong Xia3*
Jiming Chen2*Bairong Xia3*
Study Objective: The aim was to investigate the outcome of vaginal delivery of full-term pregnancies in patients after transvaginal-natural orifice transluminal endoscopic surgery (vNOTES) treatment for gynecological disorders.
Design: A case series report.
Setting: A medical university hospital.
Patients: 12 cases of successful delivery after transvaginal-natural orifice transluminal endoscopic surgery.
Interventions: Long-term follow-up of patients with fertility needs after transvaginal-natural orifice transluminal endoscopic surgery.
Measurements and Main Results: From 2018 to 2021, 163 cases of gynecological diseases were treated by vNOTES. One hundred forty-seven patients were followed up, with a follow-up rate of 90.1%. The average follow-up time was 28 (15–47) months, including 66 cases with fertility requirements. Among these 66 patients, 12 patients successfully got pregnant and completed delivery, including 10 cases of vaginal delivery and 2 cases of cesarean section, with no adverse pregnancy outcomes associated with vNOTES arising.
Conclusion: Vaginal delivery of a full-term pregnancy after transvaginal-natural orifice transluminal endoscopic surgery appears to be safe and feasible and would not be one of the bases for elective cesarean delivery.
vNOTES is an emerging minimally invasive technique that enables surgical access to the peritoneal cavity through the vagina, a natural body orifice. In recent years, with the rapid development of minimally invasive gynecology and the concept of accelerated recovery surgery, combined with the unique advantages of scarless skin and fast recovery, vNOTES has made not only a splash in the field of gynecology (1) but also became an emerging surgical modality in general surgery (2, 3) and urology (4, 5).
Although the therapeutic efficacy and safety of vNOTES in the treatment of a variety of benign and malignant gynecological diseases have been demonstrated (6–8), there is still a lack of research on its long-term postoperative effects, such as the safety of vaginal delivery in full-term pregnancies and the impact on sexual life. In this study, we investigated the impact of vNOTES on vaginal delivery of full-term pregnancies after surgery in patients by retrospectively analyzing a case series.
This study retrospectively collected 163 patients with gynecological diseases treated by vNOTES in the Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University from 2018 to 2021. 147 patients were followed up, with a follow-up rate of 90.1%. The average follow-up time was 28 (15–47) months. Among the 66 patients with fertility requirements, 12 cases were successfully pregnant and completed delivery, including 10 cases of vaginal delivery and 2 cases of cesarean section. See Supplementary Appendix S1 and Appendix S2 for case data.
The patient requires vaginal cleansing one day before the procedure. Anterior vaginal vault approach: cervical forceps or Allis forceps the anterior cervical lip and pull downward, make a transverse incision slightly below the cervical portion of the bladder attachment, bluntly separate the vesicovaginal space, free the bulging bladder, separate the cervical ligament of the bladder and push the bladder upward to the retroperitoneum of the bladder and open the retroperitoneum of the bladder and uterus into the pelvis; posterior vaginal vault approach: cervical forceps or Allis forceps the rear cervical lip and pull upward to expose the posterior vaginal vault. A transverse incision of approximately 2–3 cm is made 1.5–2.0 cm below the cervix to separate the rectal space and enter the pelvis bluntly. The pneumoperitoneum was established by inserting a particular HangT Port (Beijing HangTian KaDi Technology R&D Institute, Beijing, China) vaginal access (Figure 1). A standard 10-mm rigid 30° laparoscope was used through 1 trocar, whereas 2 endoscopic instruments were used through the other two trocars (Figure 2); through the surgical platform, access to remove the lesion peritoneal and vaginal vault incisions were closed with a running Vicryl 2 suture. All procedures were performed by a chief surgeon with extensive experience in vNOTES surgery.
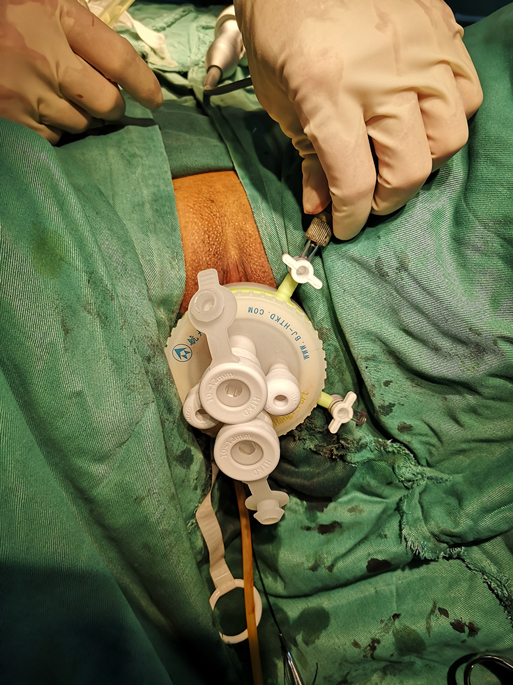
Figure 1. Establish vaginal access.
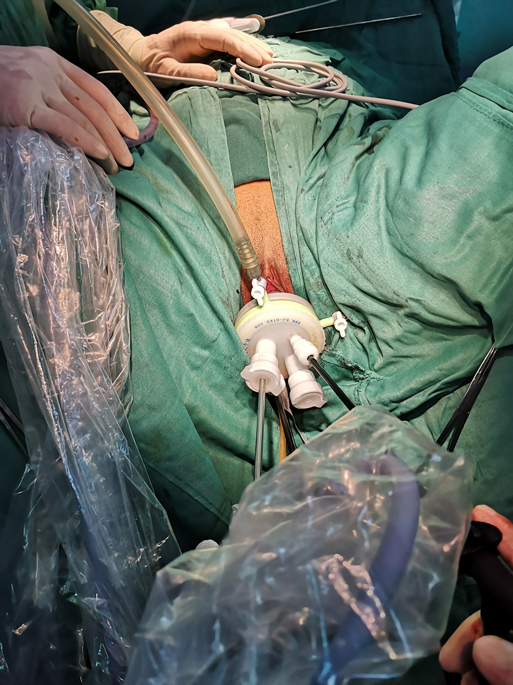
Figure 2. Schematic diagram of laparoscopic operation devices.
Baseline characteristics of patients included age, body mass index (BMI), obstetric history, and history of previous pelvic surgery. Surgical correlates included time of surgery, location of the surgical incision, surgical approach, postoperative pathological diagnosis, need for conversion to laparoscopy or cesarean, and surgical complications as indicated by Clavien-Dindo classification. All patients were followed up at one week, 1, 3, and 6 months postoperatively and annually postoperatively. Assessment of the healing of the surgical incision, non-healing or delayed healing of the incision, abnormal sensation of the incision (pain, itching), rupture or fluid flow from the incision, narrowing or shortening of the vagina, and adhesion of the vault are noted as poor healing of the incision. Detailed obstetric and delivery data were recorded for all patients, such as the gestational week of delivery, pregnancy and delivery complications, the time interval from the first day after vNOTES to the next delivery, perineal incision rate, and grading of perineal rupture. After delivery of the placenta and three days after delivery, the vaginal vault is exposed using a speculum or vaginal puller to check for tears or bleeding from the surgical scar. All data were tallied by one physician and examined by two others.
Percentages, mean, and standard deviation were performed. Statistical analysis was carried out with IBM-Microsoft SPSS version 26.0.
During the study period, a total of 12 patients completed their pregnancies and delivered successfully, and the characteristics of all patients are shown in Table 1.
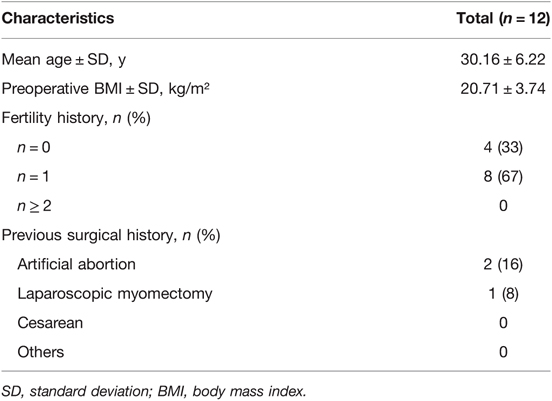
Table 1. Characteristics of 12 patients who delivered after vNOTES.
In this study, all 12 vNOTES patients had successful surgical completion. These included mature ovarian teratoma (n = 6), tubal ectopic pregnancy (n = 5), an ovarian cyst (n = 1); the mean operative time was 128.4 min and the longest operative time was 190 min; the operative incisions included anterior vaginal fornix incision (n = 6), posterior vaginal fornix incision (n = 6), and no additional vaginal wall injury due to surgical manipulation was observed in all patients; according to Clavien-Dindo classification, there were two postoperative complications, one postoperative incisional infection, which healed well after incisional dressing change (Grade 1 complication); one postoperative fever due to abdominal infection (Grade 2 complication), which improved after antibiotic treatment. The surgical incision healing was reviewed at 1 week, 1 month, 3 months, and 6 months after surgery. One of the 12 patients had poor surgical incision healing due to infection. After cleaning and dressing change, the incision healed well within one week after the operation, and the patient delivered successfully through vagina in the follow-up (See Table 2).
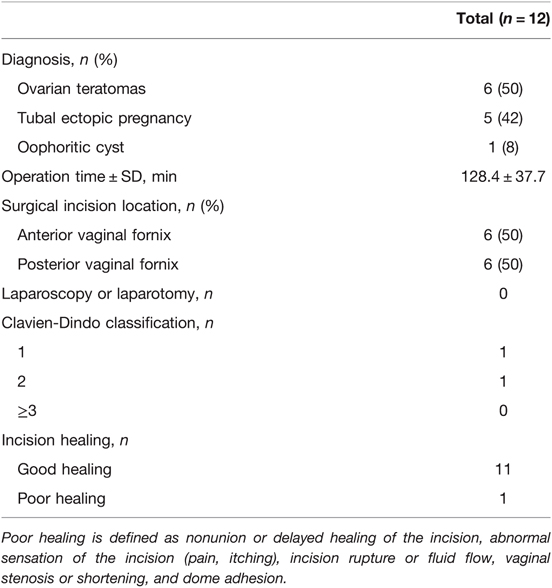
Table 2. Surgical data and postoperative review results of 12 patients.
Among the 66 patients with reproductive needs, 46(69.7%) cases were successfully pregnant, but 6 (13%) cases had an abortion, and 3(50%) cases were successfully pregnant after abortion. At present, there are 31(67.4%) patients during pregnancy. Twelve cases of pregnancy and delivery were successful, conception modes were classified as natural (n = 11), and assisted reproduction (n = 1), and all patients were examined during pregnancy according to the maternity program. Complications of pregnancy included gestational diabetes (n = 2), gestational obesity (n = 1), gestational hypothyroidism (n = 1), gestational mild anemia (n = 1), cord encirclement (n = 3), and premature rupture of membranes (n = 2). The 12 cases of successful delivery were vaginal delivery (n = 10) and cesarean delivery (n = 2). One cesarean delivery was due to a twin pregnancy, and the fetal position did not allow for vaginal delivery. The other was due to a previous history of obstructed labor. The patient refused the attempt of vaginal delivery. Ten vaginal deliveries were full-term pregnancies, singleton in the first position, normal deliveries (n = 8), obstructed deliveries (n = 2), and one obstructed delivery due to a previous history of obstructed labor. The other case was cervical edema during pregnancy, which was not significantly associated with the vNOTES procedure. No bleeding or tearing of the vNOTES surgical scar was detected after delivery of the placenta and on the third postpartum day. Six patients with perineal rupture were all with first-degree perineal rupture, which was not significantly associated with the vNOTES procedure. No bleeding or tearing of the vNOTES surgical scar was detected after delivery of the placenta and on the third postpartum day. The mean interval from the first postoperative day to the next delivery was approximately 21.8 months, with the shortest being 11.1 months. (See Table 3)
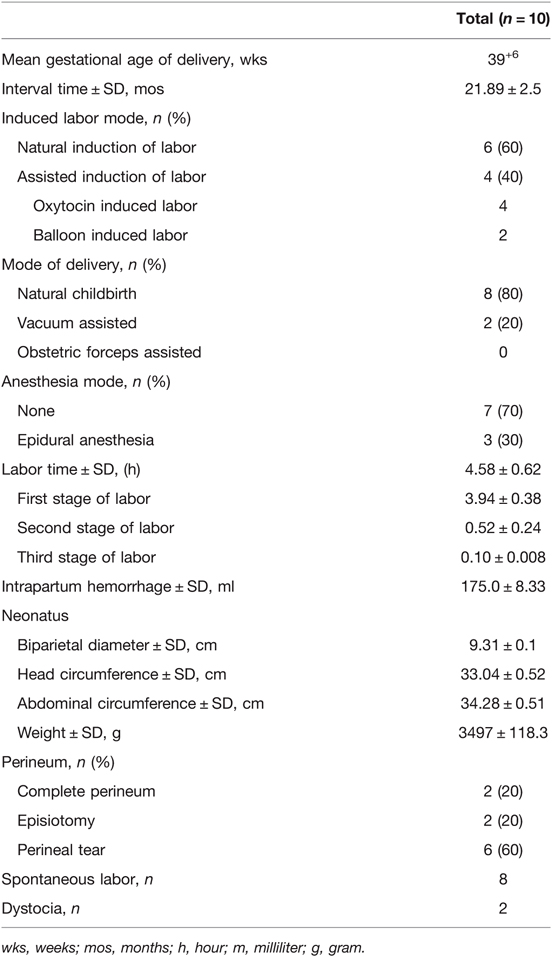
Table 3. Obstetric delivery outcomes of 10 patients undergoing vaginal delivery.
vNOTES is a minimally invasive surgical technique for treating disease after endoscopic access to the pelvic and abdominal cavity via the vagina, a natural cavity. It is the most used and developed surgical technique for trans-natural cavity surgery. vNOTES was widely used to treat benign gynecological diseases after Lee reported using vNOTES for tubal resection for tubal pregnancy in 2012 (9). In vNOTES, the intraoperative blood transfusion and hospital days are comparable to trans umbilical single-port laparoscopic surgery. Still, vNOTES has more advantages in postoperative pain relief, reduction of incisional fat liquefaction, and cosmetic results (6–8). In recent years, vNOTES has been gradually explored in gynecologic malignancies (10). Due to the significant advantage of no scar on the abdominal wall, vNOTES has been favored by many young women of reproductive age. In China’s open third-child policy, promoting fertility and reducing the cesarean section rate has been favored become a priority (11, 12). Therefore, we are concerned about the possible long-term effects of vNOTES on vaginal delivery in term pregnancies. It has been reported that full-term delivery can lead to rupture of the vaginal vault (13), but whether vNOTES will receive long-term benefits on vaginal delivery of full-term pregnancy and female sexual function has been less reported (14, 15).
The location of the incision depends mainly on the location of the lesion. Although the vNOTES approach of the posterior vaginal fornix is enough to complete the surgical treatment of most diseases in general surgery, urology, and gynecological surgery, due to the natural barrier of the uterus, the posterior vaginal fornix approach is still a difficult challenge for the lesions of the anterior wall of the uterus and the front of the pelvic cavity, and the incision of the anterior vaginal fornix can well solve this difficulty. For examples, anterior wall myomas and cesarean scar pregnancies are suitable for the anterior vaginal vault approach. In contrast, most adnexal diseases, posterior uterine wall myomas (16), and pelvic lymph node dissection (17) are more suitable for posterior vaginal vault incisions. Simultaneously, the posterior vault is more extensible, and the surgical specimen is easier to obtain intact than the anterior vault. In our study, we found that in many patients, especially those with endometriosis, the incidence of posterior pelvic adhesions is higher than that in the front of the pelvic cavity. Posterior vaginal fornix adhesions or the closure of the uterine rectum depression often led to the failure of the establishment of posterior vaginal fornix approach in vNOTES surgery and the conversion to laparoscopic surgery or rectal injury. In this study, ten vaginal deliveries included anterior vaginal vault incisions (n = 5) and posterior vaginal vault incisions (n = 5), and none of them had surgical scar tears during delivery. The current research data show that the anterior vaginal fornix incision and the posterior vaginal fornix incision have no relevant impact on the vaginal delivery of full-term pregnancy. With further follow-up, we will obtain more data to confirm this view. Vaginal preparation 1 day before surgery can effectively reduce the number of bacteria in the vagina and reduce the risk of intraoperative infection (18), and surgical incision healing is unlikely to result in abnormal incision sensation (pain, itching), incision rupture, or fluid flow, or vault adhesions that could affect the patient’s sexual life and ability to give birth. In addition, the surgical operation may damage the vaginal wall, or the suture may cause vaginal narrowing or shortening, which may affect the patient’s sexual function after surgery and thus reduce the probability of natural conception. At present, there are few research reports in this field (14).
The vNOTES produce an old surgical scar between the anterior and posterior vault of the cervix, which lacks extensibility relative to healthy tissue and may become a factor that delays the progress of labor or causes scar tearing during vaginal delivery—becoming an indication for the choice of cesarean delivery? In this study, 10 patients delivered vaginally were full-term pregnancies, and 2 were delivered by cesarean section, with a mean cesarean section rate of 16.6%, which is lower than the cesarean section rate of 39.2% in the region; the mean neonatal weight was 3,497 g, and the maximum neonatal weight was 4,220 g. No slow progression of labor or tearing of the scar was observed during delivery, which may suggest that vNOTES surgery does not full-term affect the way full-term pregnancy is delivered vaginally. The shortest postoperative interval between the patient’s surgery and full-term delivery was 11.1 months, with a mean time of 21.8 months. It may still be a topic for discussion about how long it takes after vNOTES to qualify for transvaginal delivery.
Younger patient age is a distinctive feature of the vNOTES surgery population with high estrogen production and estrogen’s ability to increase collagen deposition, increase wound strength, and promote healing of the vaginal vault surgical incision; low estrogen may increase inflammation production, prolong healing time, and affect wound healing relative to older age groups (19–21), and for those older than 45 years of age advanced maternal age, the safety of vaginal delivery after vNOTES for full-term pregnancies was not explored.
The retrospective case report of the small sample is an essential limitation of this study and there was no systematic sexual function assessment for all patients with fertility requirements after vNOTES.
In this retrospective case series, all women who successfully conceived and delivered did not have adverse birth outcomes significantly associated with vNOTES; based on our data, vNOTES appears to be safe and feasible for vaginal delivery after a full-term pregnancy, does not become a basis for elective cesarean delivery, and has important implications for the promotion of vNOTES. Multicenter, randomized controlled studies are needed to confirm the long-term benefits of vNOTES for vaginal delivery and sexuality.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
SZ: Conception and Design of Study. ZD: Data Collection. JL: Data Analysis and Interpretation. ZQ, RS, JC, BX: Responsible Surgeon or Imager. HW: Statistical Analysis. MB: Manuscript Preparation. WW: Patient Recruitment. All authors contributed to the article and approved the submitted version.
This work was supported by grants from the maternal and child health research project of Jiangsu Province (F202138), the Scientific Research Support Program for Postdoctoral of Jiangsu Province(2019K064), and the Scientific Research Support Program for “333 Project” of Jiangsu Province (BRA2019161). JC disclosed the source of funding for this study.
The institutional review board (IRB) of The Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University exempted the study. It was a retrospective case series with anonymous data and written informed consent.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/article/10.3389/fsurg.2022.888281/full#supplementary-material.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lee CL, Wu KY, Su H, Ueng SH, Yen CF. Transvaginal natural-orifice transluminal endoscopic surgery (NOTES) in adnexal procedures. J Minim Invasive Gynecol. (2012) 19(4):509–13. doi: 10.1016/j.jmig.2012.02.005
2. Zhou H, Zhang J, Wang Q, Hu Z. Transvaginal natural orifice transluminal endoscopic surgery cholecystectomy: is it the best route? Ann Surg. (2010) 251(3):578–9; author reply 579–80. doi: 10.1097/SLA.0b013e3181d0d3e3
3. Benhidjeb T, Kosmas IP, Hachem F, Mynbaev O, Stark M, Benhidjeb I. Laparoscopic cholecystectomy versus transvaginal natural orifice transluminal endoscopic surgery cholecystectomy: results of a prospective comparative single-center study. Gastrointest Endosc. (2018) 87(2):509–16. doi: 10.1016/j.gie.2017.09.039
4. Xue Y, Zou X, Zhang G. Transvaginal natural orifice transluminal endoscopic nephrectomy in a series of 63 cases: stepwise transition from hybrid to pure NOTES. Eur Urol. (2015) 68(2):302–10. doi: 10.1016/j.eururo.2015.03.033
5. Porpiglia F, Fiori C, Morra I, Scarpa RM. Transvaginal natural orifice transluminal endoscopic surgery-assisted minilaparoscopic nephrectomy: a step towards scarless surgery. Eur Urol. (2011) 60(4):862–6. doi: 10.1016/j.eururo.2010.09.038
6. Kaya C, Alay I, Cengiz H, Baghaki S, Aslan O, Ekin M, et al. Conventional laparoscopy or vaginally assisted natural orifice transluminal endoscopic surgery for adnexal pathologies: a paired sample cross-sectional study. J Invest Surg. (2021) 34(11):1185–90. doi: 10.1080/08941939.2020.1789246
7. Yassa M, Kaya C, Kalafat E, Tekin AB, Karakas S, Mutlu MA, et al. The comparison of transvaginal natural orifice transluminal endoscopic surgery and conventional laparoscopy in opportunistic bilateral salpingectomy for permanent female sterilization. J Minim Invasive Gynecol. (2022) 29(2):257–64.e1. doi: 10.1016/j.jmig.2021.08.009
8. Karakaş S, Kaya C, Yildiz Ş, Alay İ, Durmuş U, Aydiner İE, et al. Comparison of vNOTES technique with conventional laparoscopy in gynecological emergency cases. Minim Invasive Ther Allied Technol. (2022) 24:1–7. doi: 10.1080/13645706.2021.2025111
9. Li CB, Hua KQ. Transvaginal natural orifice transluminal endoscopic surgery (vNOTES) in gynecologic surgeries: a systematic review. Asian J Surg. (2020) 43(1):44–51. doi: 10.1016/j.asjsur.2019.07.014
10. Wang Y, Deng L, Tang S, Dou Y, Yao Y, Li Y, et al. vNOTES hysterectomy with sentinel lymph node mapping for endometrial cancer: description of technique and perioperative outcomes. J Minim Invasive Gynecol. (2021) 28(6):1254–61. doi: 10.1016/j.jmig.2021.01.022: S1553-4650(21)00055-8.
11. Lumbiganon P, Laopaiboon M, Gülmezoglu AM; World Health Organization Global Survey on Maternal and Perinatal Health Research Group. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007-08. Lancet. (2010) 375(9713):490–9. doi: 10.1016/S0140-6736(09)61870-5
12. Liang J, Mu Y, Li X. Relaxation of the one child policy and trends in caesarean section rates and birth outcomes in China between 2012 and 2016: observational study of nearly seven million health facility births. BMJ. (2018) 360:k817. doi: 10.1136/bmj.k817
13. Resnick L, Muller HW. Colporrhexis; with a report of a case of spontaneous primary rupture of the posterior vaginal vault during labour. S Afr Med J. (1955) 29(35):818–21. PMID: 13256025
14. Bulian DR, Trump L, Knuth J, Cerasani N, Heiss MM. Long-term results of transvaginal/transumbilical versus classical laparoscopic cholecystectomy–an analysis of 88 patients. Langenbecks Arch Surg. (2013) 398(4):571–9. doi: 10.1007/s00423-013-1071-8
15. Thomaidis P, Weltermann NJ, Seefeldt CS, Richards DC, Sauerwald A, Heiss MM, et al. Transvaginal Hybrid-NOTES procedures-do they have a negative impact on pregnancy and delivery? Langenbecks Arch Surg. (2021) 406(6):2045–52. doi: 10.1007/s00423-021-02105-z
16. Baekelandt J. Transvaginal natural-orifice transluminal endoscopic surgery: a new approach to myomectomy. Fertil Steril. (2018) 109(1):179. doi: 10.1016/j.fertnstert.2017.09.009
17. Lee C-L, Wu K-Y, Tsao F-Y, Huang C-Y, Han C-M, Yen C-F, et al. Natural orifice transvaginal endoscopic surgery for endometrial cancer. Gynecol Minim Invasive Ther. (2014) 3(3):89–92. doi: 10.1016/j.gmit.2014.08.004
18. Box GN, Bessler M, Clayman RV. Transvaginal access: current experience and potential implications for urologic applications. J Endourol. (2009) 23(5):753–7. doi: 10.1089/end.2009.0150
19. Abramov Y, Golden B, Sullivan M, Goldberg RP, Sand PK. Vaginal incisional wound healing in a rabbit menopause model: a histologic analysis. Int Urogynecol J. (2012) 23(12):1763–9. doi: 10.1007/s00192-012-1793-0
20. Calvin M, Dyson M, Rymer J, Young SR. The effects of ovarian hormone deficiency on wound contraction in a rat model. Br J Obstet Gynaecol. (1998) 105:223–7. doi: 10.1111/j.1471-0528.1998.tb10057.x
Keywords: transvaginal-natural orifice transluminal endoscopic surgery, Minimally invasive gynecology techniques, transvaginal delivery, full-term pregnancy, Childbirth ability
Citation: Zhang S, Dong Z, Liu J, Qin Z, Wang H, Bao M, Wei W, Shi R, Chen J and Xia B (2022) Safety and Feasibility of Vaginal Delivery in Full-Term Pregnancy After Transvaginal-Natural Orifice Transluminal Endoscopic Surgery: A Case Series. Front. Surg. 9:888281. doi: 10.3389/fsurg.2022.888281
Received: 2 March 2022; Accepted: 12 April 2022;
Published: 28 April 2022.
Edited by:
Rafał Watrowski, University of Freiburg, GermanyReviewed by:
Dirk Rolf Bulian, Witten/Herdecke University, Witten, GermanyCopyright © 2022 Zhang, Dong, liu, Qin, Wang, Bao, Wei, Shi, Chen and Xia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiming Chen Y2ptaW5nQDEyNi5jb20= Bairong Xia eGlhYmFpcm9uZ0B1c3RjLmVkdS5jbg==
†These authors have contributed equally to this work
Speciality section: This article was submitted to Obstetrics and Gynecological Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.