
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Urol. , 28 February 2024
Sec. Pediatric, Adolescent and Developmental Urology
Volume 3 - 2023 | https://doi.org/10.3389/fruro.2023.1281081
This article is part of the Research Topic Insights in Pediatric, Adolescent, and Developmental Urology: Volume I View all 4 articles
 Bagdagul Aksu1,2*
Bagdagul Aksu1,2* Alberto Caldas Afonso3Ipek Akil4
Alberto Caldas Afonso3Ipek Akil4 Harika Alpay5
Harika Alpay5 Bahriye Atmis6,7Ozlem Aydog8Sevcan Bakkaloglu9
Bahriye Atmis6,7Ozlem Aydog8Sevcan Bakkaloglu9 Aysun Karabay Bayazıt7
Aysun Karabay Bayazıt7 Meral Torun Bayram10
Meral Torun Bayram10 Ilmay Bilge11Ipek Kaplan Bulut12Ayse Pinar Goksu Cetinkaya2
Ilmay Bilge11Ipek Kaplan Bulut12Ayse Pinar Goksu Cetinkaya2 Elif Comak13
Elif Comak13 Belde Kasap Demir14,15
Belde Kasap Demir14,15 Nida Dincel16Osman Donmez17
Nida Dincel16Osman Donmez17 Mehmet Akif Durmus18
Mehmet Akif Durmus18 Hasan Dursun19Ruhan Dusunsel20
Hasan Dursun19Ruhan Dusunsel20 Ali Duzova21Pelin Ertan4Asuman Gedikbasi22
Ali Duzova21Pelin Ertan4Asuman Gedikbasi22 Nilufer Goknar23Sercin Guven5Duygu Hacihamdioglu24
Nilufer Goknar23Sercin Guven5Duygu Hacihamdioglu24 Augustina Jankauskiene25Mukaddes Kalyoncu26
Augustina Jankauskiene25Mukaddes Kalyoncu26 Salih Kavukcu10Bahriye Uzun Kenan9Nuran Kucuk27Bahar Kural28
Salih Kavukcu10Bahriye Uzun Kenan9Nuran Kucuk27Bahar Kural28 Mieczysław Litwin29
Mieczysław Litwin29 Giovanni Montini30,31
Giovanni Montini30,31 William Morello30Lukasz Obrycki29Beyhan Omer32Ebru Misirli Ozdemir33Nese Ozkayin34Dusan Paripovic35Cemile Pehlivanoglu36Seha Saygili37Franz Schaefer38Susanne Schaefer38Ferah Sonmez39Yilmaz Tabel40Nesrin Tas21
William Morello30Lukasz Obrycki29Beyhan Omer32Ebru Misirli Ozdemir33Nese Ozkayin34Dusan Paripovic35Cemile Pehlivanoglu36Seha Saygili37Franz Schaefer38Susanne Schaefer38Ferah Sonmez39Yilmaz Tabel40Nesrin Tas21 Mehmet Tasdemir11,41
Mehmet Tasdemir11,41 Ana Teixeira3
Ana Teixeira3 Demet Tekcan8
Demet Tekcan8 Rezan Topaloglu21Sebahat Tulpar42Ozde Nisa Turkkan5Berfin Uysal43,44Metin Uysalol45Renata Vitkevic25Sevgi Yavuz46Sibel Yel20Tarik Yildirim47Zeynep Yuruk Yildirim2,1Nurdan Yildiz5
Rezan Topaloglu21Sebahat Tulpar42Ozde Nisa Turkkan5Berfin Uysal43,44Metin Uysalol45Renata Vitkevic25Sevgi Yavuz46Sibel Yel20Tarik Yildirim47Zeynep Yuruk Yildirim2,1Nurdan Yildiz5 Selcuk Yuksel48
Selcuk Yuksel48 Eray Yurtseven49Alev Yilmaz2,1
Eray Yurtseven49Alev Yilmaz2,1Background: Congenital anomalies of the kidney and urinary tract (CAKUT) are defined as structural malformations of the kidney and/or urinary tract. Heat shock proteins (HSPs) are expressed in the kidney in response to cellular changes, such as thermal, hemodynamic, osmotic, inflammatory, and mechanical stresses. This study aimed to assess uHSP70 levels during acute urinary tract infections (UTI) and non-infection periods in patients with CAKUT, and to evaluate whether uHSP70 is elevated in CAKUT subtypes.
Methods: Among patients with CAKUT, 89 patients with UTI (CAKUT-A), 111 without UTI (CAKUT-B), and 74 healthy children were included in the study. uHSP70 levels were measured using enzyme-linked immunosorbent assay (ELISA).
Results: uHSP70 level was significantly higher in the CAKUT-A group than in the CAKUT-B and healthy control groups (p < 0.0001). Moreover, the level of uHSP70 was significantly higher in the CAKUT-B group than in the control group (p < 0.0001), but was not different between the CAKUT subtypes (p > 0.05).
Conclusion: Urine HSP70 can also be used to predict UTI in patients with CAKUT. Moreover, uHSP70 levels were higher in children with CAKUT during the non-infectious period than in healthy controls. This suggests that children with CAKUT are at risk of chronic non-infectious damage.
Congenital anomalies of the kidney and urinary tract (CAKUT) include structural malformations of the kidney and/or the urinary system (1). CAKUT occurs due to disruption of nephrogenesis under the influence of genetic or environmental factors and usually presents as urinary tract dilation on antenatal ultrasound. It has been reported that CAKUT occurs in 1/500 live birth neonates and accounts for 20-30% of all anomalies in the prenatal period (1).
Urinary tract infection (UTI) is a common clinical finding in patients with CAKUT. The UTILISE (Urinary Tract Infection and Levels of heat shock protein 70 In children as a Sensitive marker for Excluding other infections) study showed that urine Heat Shock Protein 70 (uHSP70) is elevated during acute UTI and decreases after antibiotic treatment (2). HSPs are expressed in the kidneys in response to cellular changes, such as thermal, hemodynamic, osmotic, inflammatory, and mechanical stress (3). HSPs increase cell protection and help maintain homeostasis; these stress responses induce HSP production (4). Few studies have investigated the relationship between HSP70 and CAKUT, and most of them address HSP70 in obstructive nephropathy (5, 6). To the best of our knowledge, no study has evaluated uHSP70 expression in other subtypes of CAKUT, such as renal agenesis, multicystic dysplastic kidney, hypo-dysplastic kidney, and/or atrophic kidney. We aimed to assess uHSP70 levels during acute UTI and non-infection periods in patients with CAKUT, and to evaluate whether uHSP70 was elevated in CAKUT subtypes.
This study was planned as a part of UTILISE study, a prospective multicenter and multinational study (2). The UTILISE study had a group of patients with proven UTI (n=191); among them, we included those with CAKUT in the CAKUT-A group (n=89). The algorithm used for patient selection is shown in Figure 1. Patients in this group had symptoms suggestive of UTI and were evaluated using routine physical examination, urinalysis, and urine culture at the time of admission. The sampling method for urine culture was determined by the physician according to the UTI protocol of the participating center. The inclusion criteria for the UTI group were a combination of the following three features: (a) symptoms suggestive of UTI such as fever, dysuria, or abdominal pain; (b) presence of any of positive findings in urinalysis for UTI, such as pyuria, leukocyte esterase positivity or nitrite test; and (c) significant bacterial growth in the urine culture (7). Pyuria is defined as the presence of >5 WBCs per high-power field at the microscopic analysis after centrifugation of the urine (7). Bacterial growth in urine culture was defined as significant if there was growth of ≥ 105 colony forming units (cfu)/mL of a single uropathogen for samples obtained via collecting bag and mid-stream urine, and ≥104 cfu/mL by catheterization (8, 9). All children in the UTI group were treated according to the UTI protocols of the participating centers.
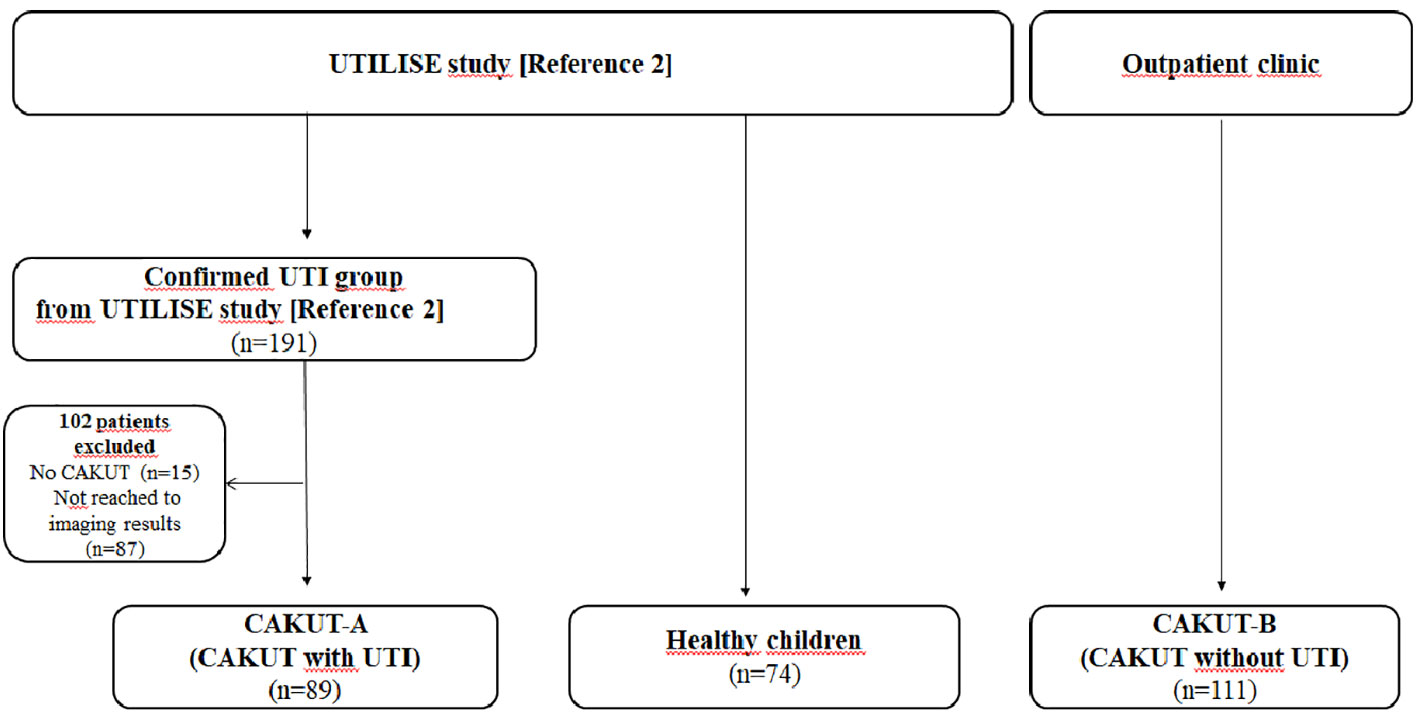
Figure 1 Algorithm for patient selection.
In this study, we included another group of patients with CAKUT, but without UTI (CAKUT-B). The CAKUT-B group consisted of 111 patients recruited from the pediatric nephrology outpatient clinics of the Istanbul Medical Faculty, Umraniye Training and Research Hospital, and Bursa Dortcelik Hospital during the same timeframe as that of the UTILISE study. These patients had no complaints, no leukocyte esterase and/or nitrite positivity on urinalysis, or bacterial growth in urine culture.
The CAKUT-A and CAKUT-B groups comprised patients with renal parenchymal malformations, migration anomalies, and collecting system anomalies. Renal parenchymal malformations include renal agenesis, hypoplasia/dysplasia, and multicystic dysplastic kidney disease. Ectopic and horseshoe kidneys are migratory anomalies. Collecting system anomalies include nonobstructive dilation (NOD) or ureteropelvic junction obstruction (UPJO), ureterovesical junction obstruction (UVJO), megaureter, ureter duplex, ectopic ureter, double collector system, vesicoureteral reflux (VUR), ureterocele, and posterior urethral valve. The imaging and laboratory results of patients in groups A and B were obtained from patient files.
The healthy control group from the UTILISE study (2) was enrolled in this study and consisted of 74 children with no acute and/or chronic diseases or urinary tract abnormalities. In the CAKUT-B and control groups, urine samples were collected midstream and/or in collection bags.
The ethical committee of Istanbul University, Istanbul Faculty of Medicine, approved the study for Turkish centers (2017/752). Ethical approval was obtained from the local Ethics Committees of all other participating countries.
Pre-treatment samples were obtained from the UTI group before the initiation of antibiotic treatment. In the other groups, urine samples were collected once at the time of admission. Random urine samples were obtained and stored at -80°C. Samples from participating centers were sent to the laboratory of the Istanbul University Istanbul Faculty of Medicine on dry ice. Urine samples that were stored at -80°C were brought to room temperature before the analysis. uHSP70 levels were measured using enzyme-linked immunosorbent assay (ELISA) using a HSP70 ELISA Kit (Cat no: KTE62748) purchased from Abbkine (Abbkine, Inc., China), following the manufacturer’s instructions. The levels of HSP70 were expressed as ng/mL. The detection and quantification limits were set to < 0.05 ng/ml for HSP70. The intra-assay coefficient of variation (CV) for HSP70 were 7.9% and 8.6%.
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). Data for continuous variables are presented as percentages or medians and interquartile ranges (IQR). The normality of the parameter distribution was tested using the Kolmogorov-Smirnov test. Non-parametric tests (Mann-Whitney U test or Kruskal-Wallis test in cases of more than two groups) were used for between-group comparisons. The Mann-Whitney U test was used to test the significance of pairwise differences, with Bonferroni correction applied to adjust for multiple comparisons. When investigating changes in uHSP70 levels between groups, age effects were adjusted using analysis of covariance (ANCOVA). For all statistical analyses p < 0.05 was considered statistically significant.
Totally 89 CAKUT patients with UTI (CAKUT-A), 111 CAKUT patients without UTI (CAKUT-B), and 74 healthy children were included in this study. Sex distribution was comparable in all groups (p=0.071). Patients in the CAKUT-A group were younger than those in the other groups (p < 0.0001) (Table 1). uHSP70 median level was not different between the children with estimated glomerular filtration rate (eGFR) ≥90 and <90 mL/min/1.73m2 (p>0.05).

Table 1 Demographic data of the study and control groups and uHSP70 levels.
uHSP70 levels were significantly higher in the CAKUT-A group than in the CAKUT-B and healthy control groups (p < 0.0001) (Table 1). When the effect of age was adjusted using covariance analysis, uHSP70 levels were higher in the CAKUT-A group than in the other two groups (p < 0.0001). Furthermore, uHSP70 expression in the CAKUT-B group was significantly lower than that in the CAKUT-A group (p < 0.0001), whereas it was significantly higher than that in the control groups (p < 0.0001) (Table 1; Figure 2).
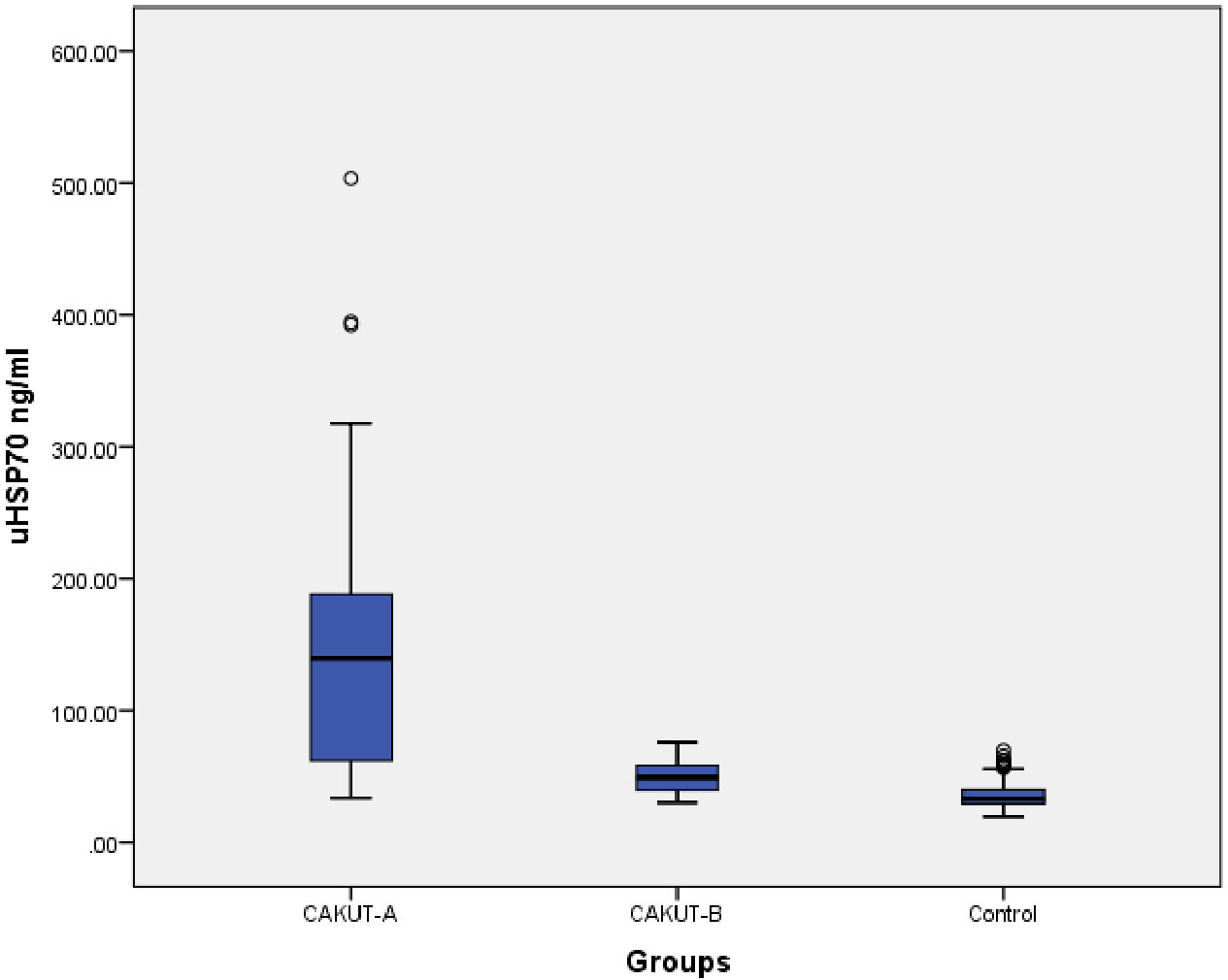
Figure 2 Comparison of the urine HSP70 levels between CAKUT-A, CAKUT-B, and Control groups.
The CAKUT subtypes are listed in Table 2. In the CAKUT-A group, collecting system anomalies occurred in 91% (n=81) of the patients, of whom 55% were diagnosed with VUR. In this group, nonobstructive dilation was the second most frequent disease, with a ratio of 30%. Moreover, some patients with VUR in the CAKUT-A group were also diagnosed with UVJO (n=2), UPJO (n=1) and ureterocele (n=1).
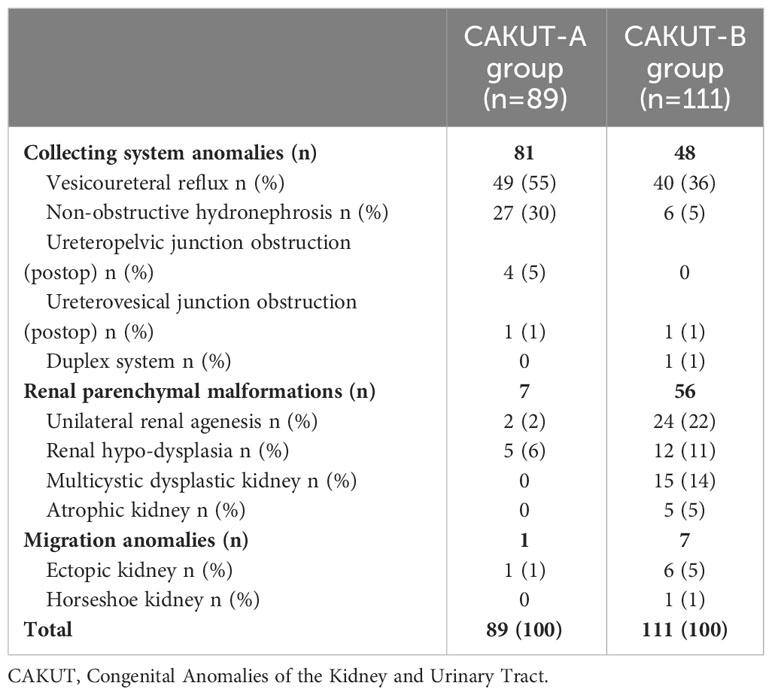
Table 2 Identification of CAKUT subtypes.
When we compared CAKUT-A patients with VUR and without VUR, uHSP70 median levels were not different between these two groups (139.1 ng/mL and 142.9 ng/mL, respectively; p=0.830) (Figure 3).
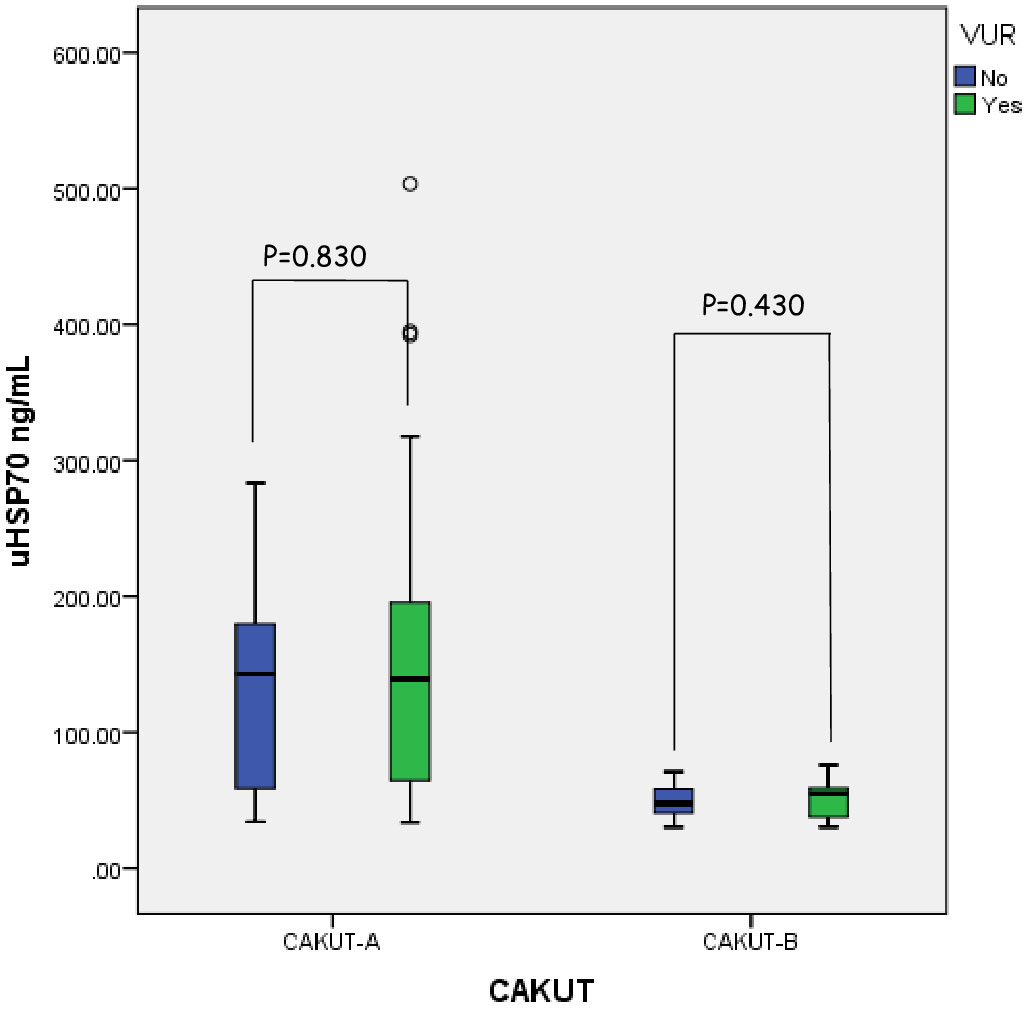
Figure 3 Comparison of the urine HSP70 levels between the patients with VUR in CAKUT-A and CAKUT-B.
Renal parenchymal malformations and collecting system anomalies constituted 52% and 43% of the CAKUT-B group, respectively. In this group, seven patients with VUR had additional anomalies [posterior urethral valve (n=3), duplex system (n=3), and meningomyelocele (n=1)]. When we analyzed the subgroups of CAKUT-B, there was no difference in median HSP70 levels between collecting system anomalies and renal parenchymal malformations (49.9 ng/mL vs. 49.0 ng/mL; p=0.940). Collecting system anomalies and renal parenchymal malformations in the CAKUT-B group were compared separately with the control group. Median uHSP70 levels were higher in patients with collecting system anomalies (49.9 ng/mL vs. 32.8 ng/mL; p < 0.0001) and renal parenchymal disorders (49.0 ng/mL vs. 32.8 ng/mL; p < 0.0001) compared to controls. Median uHSP70 levels did not differ between patients with and without VUR in the CAKUT-B group (55.3 ng/mL vs. 47.5 ng/mL; p=0.434). A comparison of the uHSP70 levels between patients with and without VUR in the CAKUT-A and CAKUT-B groups was shown in Figure 3.
In our previous UTILISE study, we evaluated children with UTI and found increased uHSP70 levels during infection (2). The presence of CAKUT is one of the most important risk factors for developing UTI (10). Our results in current study showed that uHSP70 level was significantly higher in both CAKUT-A and CAKUT-B groups than in the control group. In addition, the uHSP70 levels were significantly higher in the CAKUT-A group than in the CAKUT-B group. It was expected that uHSP70 is at its highest level during the UTI period, as the UTILISE study clearly demonstrated that uHSP70 is a reliable biomarker for predicting UTI. Further, uHSP70 is significantly higher during infection in patients with CAKUT, suggesting that uHSP70 levels could be used to predict UTI in patients with CAKUT. Interestingly, the level of uHSP70 in the non-infectious period was higher than that in the controls but much lower than that in the infectious period. We believe that the increased uHSP70 levels in the CAKUT-B group may be due to ongoing oxidative stress during the chronic process in patients with CAKUT. CAKUT is a chronic disease that meets the definition of chronic kidney disease (CKD) with evidence of kidney damage for 3 months or more as demonstrated by the presence of structural kidney disorders and by imaging methods (11). Many studies have shown that oxidative stress is increased in children with CKD (12, 13). In addition, it should be kept in mind that previous UTI attacks may contribute to this situation. We have earlier reported that uHSP70 was slightly elevated in patients with kidney-related chronic diseases, such as CKD, IgA nephropathy, and diabetic nephropathy (14, 15). We also showed that uHSP70 levels were excessively elevated during UTI, an acute disease, and decreased in response to antibiotic treatment. The presence of CAKUT did not preclude the use of uHSP70 as a biomarker for UTI.
An experimental study in rats showed that HSP70 levels increased after 10 days of unilateral obstruction in UPJ. After the obstruction was resolved, HSP70 levels returned to baseline. This suggests that HSP70 levels may be a specific and localized response to oxidative injury (16). Valles et al. (6) evaluated 22 children with congenital UPJO. Renal biopsies were obtained for immunohistochemical and western blot analyses at the time of surgery. Increased staining of HSP27 and HSP70 in the proximal tubules, cortical collecting ducts and medullary collecting ducts was detected using immunohistochemical method. This indicates that HSP27 and HSP70 could play a role in the adaptive response of the kidney to congenital UPJO (6). Oktar et al. (5) investigated the uHSP70 levels in 43 children with UPJO who underwent pyeloplasty, 25 patients with NOD, and 30 healthy children. The uHSP70 levels were higher in the pyeloplasty group than in the NOD and control groups. Additionally, the uHSP70 levels decreased postoperatively. It has been emphasized that uHSP70 can predict surgical indications for unilateral UPJO (5). Moreover, adult UPJO rats treated with α-tocopherol, a compound used to treat acute oxidative injury, showed decreased HSP70 expression in kidneys (17). In previous studies, the elevation of HSP70 in obstructive uropathy was explained by the increased intrarenal oxidative stress in UPJO, which includes kidney injury, and the increased synthesis of HSP70 from injured renal cells in response to this stress (18–20).
Because the number of patients with obstructive uropathy in our study was small (only 12 patients), we did not compare patients with obstructive uropathy to those with other subtypes of CAKUT according to uHSP70 levels. In our study, uHSP70 was evaluated separately according to the subtypes of CAKUT in every CAKUT group, including VUR, collecting system anomalies, and renal parenchymal malformations. Urine HSP70 levels were significantly higher in all CAKUT subtypes; we therefore concluded that uHSP70 levels were not specific to any of the CAKUT subgroups.
However, this study has some limitations. The number of patients in the CAKUT subgroups was not evenly distributed; therefore, we did not analyze the statistical significance between them.
Urine HSP70 levels in CAKUT patients were significantly high while they were diagnosed with UTI. uHSP70 levels can be used to predict UTI in patients with CAKUT. Moreover, uHSP70 levels were higher in children with CAKUT during the non-infectious period than in healthy controls. This suggests that children with CAKUT are at risk of chronic non-infectious damage.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by The ethical committee of Istanbul University Istanbul Faculty of Medicine approved the study for Turkish centers (2017/752). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
BAk: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AA, IA, HA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Writing – review & editing. BAt, OA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. SB, AB, MB, IB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. IKB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. AC, EC, BD, ND, OD, MD, HD, RD, AD: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. PE: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. AG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. NG, SG, DH, AJ, MK, SK, BUK, NK, BK, ML, GM, WM, LO, BO, EMO, NO, DP, CP, SSa, FSc SSc, FSo, YT, NT, MT, AT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. DT: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. RT, ST, OT, BU, MU, RV, Sya, Sye, TY: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. ZY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. NY, SYu, EY: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing – review & editing. AY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. UTILISE Study was supported by Scientific Research Projects Coordination Unit of Istanbul University (29652), by the European Society for Pediatric Nephrology (ESPN) (ESPN #5.2018), by the Society for Children’s Kidney Health (1.2018), and by Istanbul Faculty of Medicine Foundation.
We gratefully acknowledge that UTILISE was supported by Scientific Research Projects Coordination Unit of Istanbul University, by the European Society for Pediatric Nephrology (ESPN), by the Society for Children’s Kidney Health, and by Istanbul Faculty of Medicine Foundation. We are also very thankful to children participating in this study, our dedicated chemist Orhan Tepeli and diligent students of Istanbul University Istanbul Faculty of Medicine Zeynep Sakur, Sevgi Ipar, Isıl Gul for their great help and assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Schedl A. Renal abnormalities and their developmental origin. Nat Rev Genet (2007) 8(10):791–802. doi: 10.1038/nrg2205
2. Yilmaz A, Afonso AC, Akil I, Aksu B, Alpay H, Atmis B, et al. Urinary HSP70 improves diagnostic accuracy for urinary tract infection in children: UTILISE study. Pediatr Nephrol (2023) 38(3):791–9. doi: 10.1007/s00467-022-05664-5
3. Kim HJ, Hwang NR, Lee KJ. Heat shock responses for understanding diseases of protein denaturation. Mol Cells (2007) 23(2):123–31. doi: 10.1016/S1016-8478(23)07364-8
4. Kim HP, Morse D, Choi AMK. Heat-shock proteins: new keys to the development of cytoprotective therapies. Expert Opin Ther Targets (2006) 10(5):759–69. doi: 10.1517/14728222.10.5.759
5. Oktar T, Kucukgergin C, Donmez MI, Ozkuvanci U, Yilmaz A, Yildirim ZY, et al. Urinary HSP70 can predict the indication of surgery in unilateral ureteropelvic junction obstruction. Pediatr Surg Int (2022) 38:499–503. doi: 10.1007/s00383-021-05059-x
6. Valles P, Jorro F, Carrizo L, Manucha W, Oliva J, Cuello-Carrion FD, et al. Heat shock proteins HSP27 and HSP70 in unilateral obstructed kidneys. Pediatr Nephrol (2003) 18(6):527–35. doi: 10.1007/s00467-003-1096-2
7. Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics (2011) 128:595–610. doi: 10.1542/peds.2011-1330
8. Hodson EM, Craig JC. Urinary tract infections in children. In: Avner ED, Harmon WE, Niaudet P, Yoshikawa N, Emma F, Goldstein SL, editors. Pediatric nephrology, 7th ed. New York: Springer (2015). p. 1695–715.
9. Goldberg B, Jantausch B. Kher KK, Schnaper HW, Greenbaum LA, editors. Clinical pediatric nephrology, 3rd ed. Berlin: Springer (2017). p. 967–93.
10. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis (2002) 39(2 Suppl 1):S1–266.
11. Buettcher M, Trueck J, Niederer-Loher A, Heininger U, Agyeman P, Asner S, et al. Swiss consensus recommendations on urinary tract infections in children. Eur J Pediatr (2021) 180(3):663–74. doi: 10.1007/s00431-020-03714-4
12. Daenen K, Andries A, Mekahli D, Van Schepdael A, Jouret F, Bammens B. Oxidative stress in chronic kidney disease. Pediatr Nephrol (2019) 34:975–91. doi: 10.1007/s00467-018-4005-4
13. Locatelli F, Canaud B, Eckardt KU, Stenvinkel P, Wanner C, Zoccali C. Oxidative stress in end-stage renal disease: an emerging threat to patient outcome. Nephrol Dial Transplant (2003) 18:1272–80. doi: 10.1093/ndt/gfg074
14. Yilmaz A, Gedikbasi A, Yildirim ZY, Pehlivanoglu C, Seker B, Sucu A, et al. Higher urine heat shock protein 70/creatinine ratio in type 1 diabetes mellitus. Ren Fail (2016) 38(3):404–10. doi: 10.3109/0886022X.2015.1136893
15. Yildirim ZY, Akgul SU, Alpay H, Aksu B, Oguz FS, Kiyak A, et al. PROGRESS STUDY: Progression of chronic kidney disease in children and heat shock proteins. Cell Stress Chaperones (2021) 26(6):973–87. doi: 10.1007/s12192-021-01239-9
16. Lin KC, Krieg RJ, Saborio P, Chan JC. Increased heat shock protein-70 in unilateral ureteral obstruction in rats. Mol Genet Metab (1998) 65:303–10. doi: 10.1006/mgme.1998.2770
17. Chan W, Krieg RJ, Ward K, Santos P, Lin KC, Chan JC. Progression after release of obstructive nephropathy. Pediatr Nephrol (2001) 16:238–44. doi: 10.1007/s004670000519
18. Ricardo SO, Diamond JD. The role of macrophages and reactive oxygen species in experimental hydronephrosis. Semin Nephrol (1998) 18:612–21.
19. Beck FX, Wolfgang N, Müller E. Molecular chaperones in the kidney: distribution, putative roles and regulation. Am J Physiol Renal Physiol (2000) 279:F203–15. doi: 10.1152/ajprenal.2000.279.2.F203
Keywords: children, congenital anomalies of the kidney and urinary tract, CAKUT, heat shock proteins, Hsp70, UTILISE study
Citation: Aksu B, Afonso AC, Akil I, Alpay H, Atmis B, Aydog O, Bakkaloglu S, Bayazıt AK, Bayram MT, Bilge I, Bulut IK, Cetinkaya APG, Comak E, Demir BK, Dincel N, Donmez O, Durmus MA, Dursun H, Dusunsel R, Duzova A, Ertan P, Gedikbasi A, Goknar N, Guven S, Hacihamdioglu D, Jankauskiene A, Kalyoncu M, Kavukcu S, Kenan BU, Kucuk N, Kural B, Litwin M, Montini G, Morello W, Obrycki L, Omer B, Misirli Ozdemir E, Ozkayin N, Paripovic D, Pehlivanoglu C, Saygili S, Schaefer F, Schaefer S, Sonmez F, Tabel Y, Tas N, Tasdemir M, Teixeira A, Tekcan D, Topaloglu R, Tulpar S, Turkkan ON, Uysal B, Uysalol M, Vitkevic R, Yavuz S, Yel S, Yildirim T, Yildirim ZY, Yildiz N, Yuksel S, Yurtseven E and Yilmaz A (2024) The relationship between urine heat shock protein 70 and congenital anomalies of the kidney and urinary tract: UTILISE study. Front. Urol. 3:1281081. doi: 10.3389/fruro.2023.1281081
Received: 21 August 2023; Accepted: 28 December 2023;
Published: 28 February 2024.
Edited by:
Sherry Ross, University of North Carolina at Chapel Hill, United StatesReviewed by:
Marcos Figueiredo Mello, Federal University of São Paulo, BrazilCopyright © 2024 Aksu, Afonso, Akil, Alpay, Atmis, Aydog, Bakkaloglu, Bayazıt, Bayram, Bilge, Bulut, Cetinkaya, Comak, Demir, Dincel, Donmez, Durmus, Dursun, Dusunsel, Duzova, Ertan, Gedikbasi, Goknar, Guven, Hacihamdioglu, Jankauskiene, Kalyoncu, Kavukcu, Kenan, Kucuk, Kural, Litwin, Montini, Morello, Obrycki, Omer, Misirli Ozdemir, Ozkayin, Paripovic, Pehlivanoglu, Saygili, Schaefer, Schaefer, Sonmez, Tabel, Tas, Tasdemir, Teixeira, Tekcan, Topaloglu, Tulpar, Turkkan, Uysal, Uysalol, Vitkevic, Yavuz, Yel, Yildirim, Yildirim, Yildiz, Yuksel, Yurtseven and Yilmaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bagdagul Aksu, YmFnZGFndWxAeWFob28uY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.