 Lucie Adélaïde1*
Lucie Adélaïde1* Sylvia Medina1
Sylvia Medina1 Vérène Wagner1Perrine de Crouy-Chanel1Elsa Real2
Vérène Wagner1Perrine de Crouy-Chanel1Elsa Real2 Augustin Colette2Florian Couvidat2
Augustin Colette2Florian Couvidat2 Bertrand Bessagnet3Maxime Alter4Amélie Durou1Sabine Host5Marion Hulin1
Bertrand Bessagnet3Maxime Alter4Amélie Durou1Sabine Host5Marion Hulin1 Magali Corso1Mathilde Pascal1
Magali Corso1Mathilde Pascal1- 1Santé Publique France, French Public Health Agency, Saint-Maurice, France
- 2Ineris, French National Institute for Industrial Environment and Risks, Parc Technologique ALATA, Verneuil-en-Halatte, France
- 3Citepa, Technical Reference Center for Air Pollution and Climate Change, Paris, France
- 4ATMO Grand Est, Certified Associations of Air Quality Monitoring, Schiltigheim, France
- 5ORS Île-de-France, Regional Health Observatory Île-de-France, Paris, France
Lockdown measures to limit the spread of Covid-19 in France in spring 2020 sharply reduced activities and lowered air-pollution concentrations. This study sought to determine the short- and long-term impacts on mortality in metropolitan France resulting from the temporary decrease in the population's exposure to air pollution. The reduction in exposure to air pollution was estimated by calculating the difference between modeled exposure of the population during the strict lockdown and the gradual lifting, and the simulated exposure that would have been observed in the absence of lockdown. A quantitative health impact assessment was used to estimate both the short-term impact of PM10 and NO2 reductions, and the long-term impact of PM2.5 and NO2 reductions on mortality. Reduced activities during the lockdown lowered NO2 and PM concentrations, resulting in about 2,300 deaths postponed for PM2.5 and nearly 1,200 for NO2, mainly due to avoided long-term effects. This study shows that, even in an unprecedented context that is certainly neither realistic nor desirable to improve air quality in the long run, public interventions appear to have a significant impact on health through reductions in air-pollution levels. In a long-term perspective, the study also reminds us that the total burden of air pollution on health remains a significant risk factor in France. Efforts to reduce ambient air pollution must thus be pursued sustainably for all sources of air pollution with suitably adapted but ambitious policies. Finally, the lockdown restrictions had other consequences, both positive and negative, on the population's health. These consequences highlight the need to conduct more integrated assessments of health impacts that include the multisectoral consequences of interventions, particularly in terms of population compliance with mitigating restrictions, behavior and mental health and, more broadly, climate change.
Introduction
The Covid-19 pandemic caused by SARS-CoV-2 has had a dramatic impact on public health, societies and economies around the world. As of March 3, 2021 France had totaled almost 4,000,000 confirmed cases of Covid-19 and over 88,000 deaths attributable to Covid-191.
To stem the spread of Covid-19, governments everywhere took unprecedented steps that had negative impacts on economic activity and travel behavior but positive impacts on air quality.
In France, to study these impacts on air quality, the national air-pollution monitoring network (Atmo France) analyzed the evolution of daily average concentrations of nitrogen oxides (NOx) from March 1 to 31, 2020 at monitoring stations representative of traffic exposure to air pollution in France's largest cities. Comparison of the month of March 2020 with previous years suggests that the lockdown led to a decrease in daily average NOx concentrations close to roads from 50% in Bordeaux to 70% in Toulouse. Illustrating the influence of the decrease in road traffic, areas with over 500,000 inhabitants observed decreases in NOx concentrations of 49% in Toulon, 69% in Nice, 72% in Grenoble, and 73% in Paris2. The figures provided by the French Institute for Industrial Environment and Risks (Ineris) at the end of the lockdown also support this view. Using an approach combining both models and observations, the Ineris assessment published in May 2020 indicated for the major French cities average decreases at traffic monitoring stations of 49% for nitrogen dioxide (NO2), 12% for PM2.5 and 10% for PM10. These findings confirm the greater decreases for nitrogen dioxides than for fine particles, due to the strong contribution for the latter of sectors of activity other than road transport3.
This study sought to determine the short and long-term impacts on mortality of lowered emissions and lowered background concentrations of outdoor-air pollutants resulting from the sharp fall in activities of all kinds from lockdown steps taken in France. A quantitative health impact assessment (QHIA) was carried out in metropolitan France following the recommendations of the QHIA guidelines on air pollution (QHIA-AP) of Santé publique France (the French public health agency) published in 2019 (Pascal et al., 2019).
Materials and Methods
Study Area and Period
The study was carried out in metropolitan France. It covered different periods according to the specific objectives of the QHIA. For the short-term effects of lockdown, it focused on two periods: strict lockdown (March 16 to May 11, 2020), and gradual lifting of the lockdown4 (May 11 to June 22, 2020). The QHIA on long-term effects analyzed 1 year of data, from July 2019 to June 2020, in order to include the lockdown period, with calculation of the long-term effects based on an annual average exposure.
Exposure Assessment
Regarding exposure assessment, the main objective was to estimate the difference between the actual exposure of the population during the periods of strict lockdown and gradual lifting, and the exposure that would have been observed in the absence of lockdown.
Short- and long-term effects of lockdown on exposure to the selected air-pollution indicators, PM10, PM2.5, and NO2, were therefore calculated following four steps:
1) Based on the methodology developed by the PREVAIR platform5, the CHIMERE air-quality model data (Mailler et al., 2017) and the concentrations measured by the air-pollution monitoring network (AASQA)6 are combined to retrospectively re-analyze the daily concentrations over the period of interest. The data obtained, combining modeling and measurements, are representative of the background levels observed during the study period.
2) Two CHIMERE simulations were also carried out to evaluate modeled average concentrations from emissions with and without lockdown. These simulations were carried out by Ineris using the emission inventory developed by Copernicus emissions (Guevara et al., 2020) (Copernicus Atmospheric Monitoring Service [CAMS] of the European Commission) and adapted with abatement factors due to the lockdown for France estimated by the French Technical Reference Center for Air Pollution and Climate Change (Citepa). Percentage reduction of daily average concentrations modeled for each pollutant from March 16 to June 22 was then calculated from these two simulations.
3) This percentage was then applied to the re-analyzed daily average concentrations (point 1) in order to obtain a daily mapping of background levels that should have been observed in the absence of lockdown.
4) The last step consisted of calculating the daily differences over the study period (population-weighted average) that were used for the QHIA at the municipal level.
Population-weighted average concentrations were used because they are good estimates of population exposure as they take into account the location and density of the population of each grid cell of a municipality in order to estimate its weighted pollution levels. Using this method, spaces with no or very low population density within a municipal territory are not given the same weight as densely populated spaces. The population database used in this study is the national Laboratoire Central de Surveillance de la Qualité de l'Air (LCSQA) population database (Létinois, 2014) established for 2016.
For the long-term assessment, we compared the impacts in a situation where the population would be exposed to the estimated annual average concentrations without the lockdown (i.e., the annual average concentrations on each day from July 1, 2019 to June 30, 2020 if the lockdown had not been implemented) and a situation where the population would be exposed to the estimated annual average concentrations with the lockdown (i.e., the annual average concentrations observed on the non-lockdown days and the concentrations observed on the lockdown days for the period July 1, 2019 to June 30, 2020).
We also compared the daily differences obtained with the method detailed in point 4 above (using concentration models with and without lockdown), to an alternative method based on historical reference periods. This method is discussed in Interpretation and Uncertainties Related to Exposure Modeling.
Presentation of the CHIMERE Model
The CHIMERE model (Mailler et al., 2017) is a chemistry-transport model developed by the National Centre for Scientific Research (CNRS) and Ineris used for air-quality forecasts and emission-reduction-scenario studies (Bessagnet et al., 2014). This numerical model brings together a set of equations representing the transportation and transformation of chemical compounds and allows quantifying the evolution of a pollutant plume as a function of time over different domains (from urban to continental). CHIMERE uses meteorological and emission flow data to calculate hourly three-dimensional fields of pollutant concentrations in the atmosphere. More than a hundred gaseous compounds are modeled including ozone and nitrogen oxides but also particles (see Supplementary Material 1 for more details).
Re-analyzed PREVAIR concentrations are generated each day for the previous day by combining forecasts developed using the CHIMERE model and observation data from measures made on a national level by the AASQA. More information on the methodology for preparing these re-analyzed data is available in Beauchamp et al. (2017) and Beauchamp et al. (2018).
Simulations with and without the lockdown effect were performed over the study period on an area covering France at about 4-km resolution with the CHIMERE version 2017β (Couvidat et al., 2018).
Regarding emissions, the CAMS-REG emissions inventory for the year 2015 covering all of Europe at a resolution of 0.1° × 0.05° was used. As these emissions do not take into account the effects of the lockdown, emission abatement factors were applied to each day of the time period. These abatement factors are based on CAMS data adapted for French regions by Citepa. More details on the model and its input data (meteorological data, boundary conditions and emissions) are given in Supplementary Material 1.
Emissions Calculations
The calculation of emissions is based on the daily emissions variations proposed by CAMS for the main sectors of activity (Guevara et al., 2020) in Europe. Guevara et al. in 2020, quantify the primary emission reductions due to lockdown measures in Europe (Guevara et al., 2020). The reduction factors by country are provided daily for each sector of activity: energy industry (power plants), manufacturing industry, road traffic, and aviation (landing and take-off cycle). The period covered is from February 21, 2020, when the first European localized lockdown was implemented in the Lombardy region of Italy, to April 26, 2020. The calculated reduction factors were combined with the European emission inventory of the CAMS using adjusted emission time profiles to derive time-resolved emission reductions by country and by pollutant sector. Calculations for France are thus partly influenced by the calculations in cross-border countries.
For France, Citepa has performed a finer calculation of emission variations by region for road-traffic emissions and a first estimate for the residential sector. Concerning road traffic, the variations are based on traffic data (number of vehicles on the road) from the Center for Studies and Expertise on Risks, the Environment, Mobility and Development (Cerema). The resulting monthly variations in road-traffic emissions are illustrated in Figure 1. Regarding residential emissions, household electricity consumption (daily data provided by RTE, the French Electric Transport Network) was used as a proxy to calculate the impact of the lockdown on heating emissions regardless of the heating method. More details on these calculations are given in Supplementary Material 2.
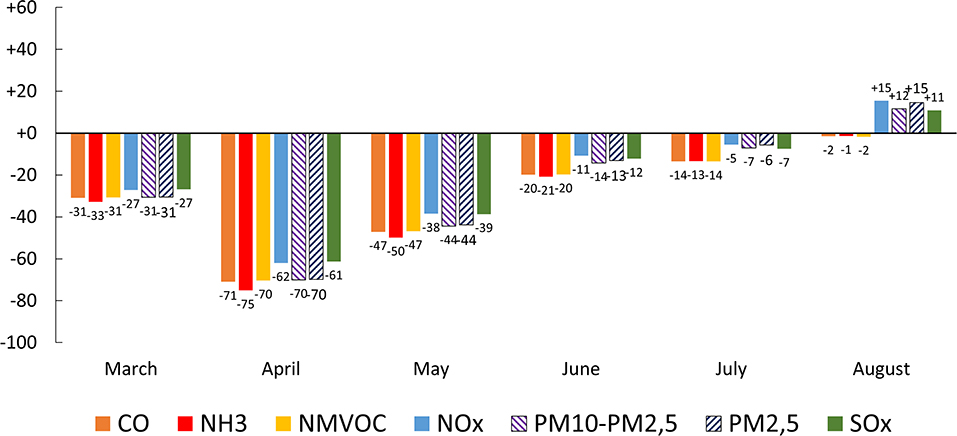
Figure 1. Variations in road traffic emissions in France between 2019 and 2020 (%).
Heath Indicators
In order to fit with the selected concentration-response functions (CRF) or relative risks (RR)7 required for QHIAs (see section Concentration-Response Functions (CRF) below), the study focuses on: (1) non-accidental mortality (International Classification of Diseases-10th revision, ICD-10 : A00-R99) for short-term effects of air pollution; (2) on all-cause mortality (ICD-10 : A00-Y98) in the 30 and over age group for the long-term effects. The data was obtained from the Epidemiology Centre on Medical Causes of Death (CépiDc-Inserm) for the most recent years available (2014–2016).
Short-term effects on mortality occur within a few days of exposure to pollution, reflecting that air pollution is responsible for acute worsening of health conditions or exacerbation of chronic diseases (heart attack, stroke, etc.), which may lead to death. Long-term effects on mortality can be defined as the contribution of exposure to air pollution to the development of chronic diseases (e.g., respiratory, cardiovascular, neurological, etc.), which may lead to death.
Population Data
The QHIA used the population data from the census (INSEE) at the municipal level. The latest data available was for 2016, spatialized on residential buildings using a method established by the LCSQA frequently used to capture the heterogeneous distribution of the population in a municipality (Létinois, 2014). The study areas were grouped by: rural areas (<2,000 inhabitants); sparsely populated urban areas (areas belonging to urban units of 2,000–20,000 inhabitants); populated urban areas (areas belonging to urban units of 20,000–100,000 inhabitants); highly populated urban areas (areas belonging to urban units with more than 100,000 inhabitants).
Quantitative Health Impact Assessment
QHIA is a method initially developed by the World Health Organization (WHO) to illustrate the impact of air pollution on public health. It provides information on the health impacts of air pollution on a population and estimates the benefits that can be achieved for different air-quality-improvement scenarios (Medina et al., 2004).
The preamble to any QHIA is based on the hypothesis of a causal link between exposure to air pollution and its health effects. This link can be assessed using the Bradford Hill criteria for causality (Hill, 1965). For our purposes, we mainly considered the concentration-response relationship (the higher the pollution levels, the greater the health effect and/or its probability), the temporal relationship (exposure precedes the effect), the consistency of the association (its repetition in time and space) and, above all, the notion of biological plausibility of the effect of air pollution on health. This plausibility is confirmed by numerous mechanistic, toxicological and epidemiological studies (WHO, 2013; EPA, 2016; Petit et al., 2017; Harmon et al., 2018; Jaligama et al., 2018; ERS, 2019).
Concentration-Response Functions (CRF)
The choice of the CRF (Table 1) among those available in the literature is based on the following criteria from the QHIA-AP guidelines of Santé publique France (Pascal et al., 2019):
- the levels of air pollution observed in the study area, the characteristics of the population, and the health-care system are as close as possible to those of the study providing the CRF. For example, a CRF obtained for South-East Asian cities was not used given the differences in context, lifestyles and concentration ranges;
- the CRFs used are the most robust to date and come from western-world studies including, as far as possible, French or European populations:
- Studies that have calculated meta-risks (relationship calculated from the results of several individual studies) from multicenter western-world studies including European and French studies are preferred;
- in the absence of western-world studies including French or European studies, North American or Canadian multicenter studies are selected, or we applied the recommendations of WHO in terms of CRF selection (WHO, 2013);
- Significant CRF with a narrow confidence interval are preferred as much as possible.
- Studies providing CRF are published in peer-reviewed journals.
The chosen CRFs (Table 1) match those recommended by the QHIA-AP guidelines of Santé publique France for mortality, i.e., those for which the level of uncertainty of the transposability of the risk is low and for which sufficient data are available to allow reliable quantification of the effects.
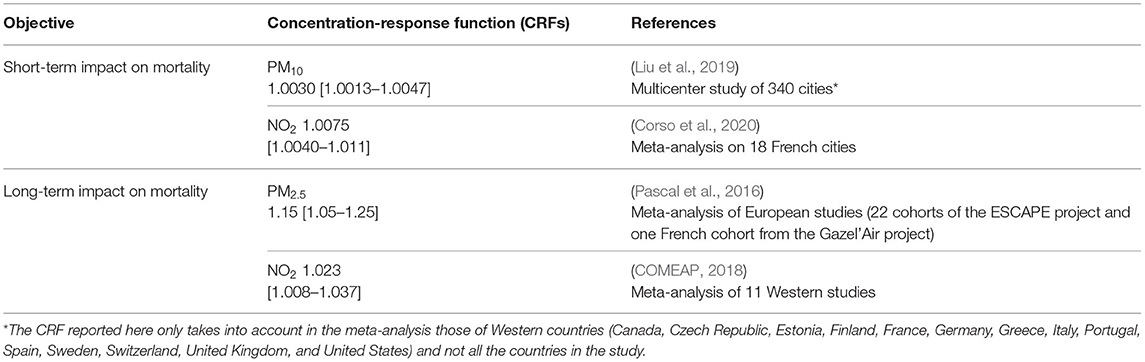
Table 1. Selected concentration-response functions (CRF).
These CRFs are formulated with a central value and a 95% confidence interval [95% CI] that expresses the random error and variability attributed to the heterogeneity of the CRF from epidemiological studies. This is a small part of the total uncertainty in the risk estimates produced by the QHIA. Other uncertainties exist related to, for example, air-pollution measurement and modeling (see Discussion section).
In accordance with the QHIA-AP guidelines, for short-term effects the study focuses on PM10 or NO2-non-accidental mortality, and for long-term effects on the PM2.5 or NO2-all-cause mortality in the 30 and over age group.
QHIA Equations
In our study, the decrease in mortality Δy for a given QHIA scenario is expressed as
where y0 is the observed mortality, (for a CRF expressed per 10 μg/m3 increase), and Δx represents the decrease in pollutant concentration in the scenario of interest.
Gain in life expectancy at 30 was estimated as the difference between the life expectancies at age 30 obtained from observed data during lockdown (high value) and expected data from modeling without lockdown (low value). For each age group, if pollutant concentration decreased, the probability of dying would be modified by a factor e−βΔx. Life expectancy was estimated from abridged mortality tables built for 5-year age groups for a theoretical cohort of 100,000 individuals.
Scenarios
Two scenarios were considered:
- Short-term impact on non-accidental mortality of modeled decreases in daily outdoor PM10 and NO2 levels caused by the measures taken to limit the spread of Covid-19 from March 16 to June 22, 2020;
- Long-term impact on all-cause mortality of reductions in annual PM2.5 and NO2 levels from July 2019 to June 2020, caused by the measures taken to limit the spread of Covid-19.
The decreases in concentrations, and the resulting population exposure, were modeled based on assumptions about the reduction in emissions during the period of reduction of activities.
In order to put the findings of these two scenarios into perspective, another scenario was considered on the total burden of air pollution on mortality of the French population from 2016 to 2019. These findings are presented in the discussion section.
Sensitivity Analysis
We explored the uncertainty surrounding the results of exposure modeling using population-weighted concentrations. We did so by transforming the concentration at the grid cell to an exposure at the municipality level. This method takes into account an average of each grid cell covering the municipality weighted by the covered area (i.e., surface-weighted concentrations) instead of the population (i.e., population-weighted concentrations).
We also performed a sensitivity analysis for the total burden of air pollution on mortality using different CRFs and reference values (findings presented in the discussion section).
Results
The QHIA was carried out for metropolitan France. The study covered the 35,228 municipalities, including 28,102 rural municipalities and 7,126 urban municipalities.
Short-Term Impact of the Lockdown on Non-accidental Mortality
Air Pollution Levels
There was a moderate decrease in background air-pollution levels that was greater during the strict lockdown than during the gradual lifting. On average, there was an exposure gradient from rural (lower decrease of the concentrations) to highly populated urban areas (greater decrease of the concentrations) that was greater for NO2 than for PM10 (Table 2). Figure 2 shows pollutant concentrations during the lockdown (A) and the modeled average difference in concentrations between lockdown and lifted levels (B).

Table 2. Daily mean differences [min; max] by period, pollutant and area in France from March 16 to June 22, 2020, and from July 1, 2019 to June 30, 2020.
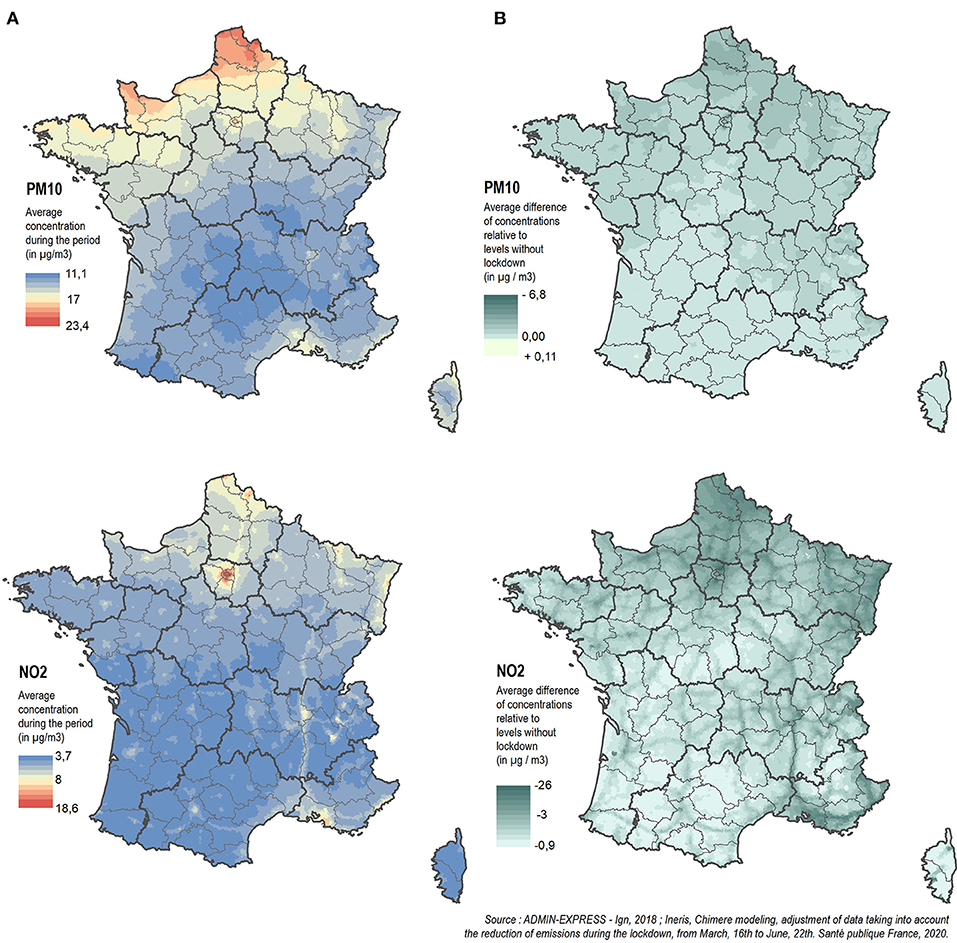
Figure 2. Pollutant concentrations during the lockdown (A) and modeled average difference in concentrations between lockdown and non-lockdown levels (B).
The daily mean differences obtained from surface-weighted concentrations in the sensitivity analysis were very close to those obtained from population-weighted concentrations (Supplementary Table 1).
Population and Mortality Descriptive Data
The average daily number of deaths from all non-accidental causes for persons living in metropolitan France for the period 2014–2016 was 1,453 (Table 3).
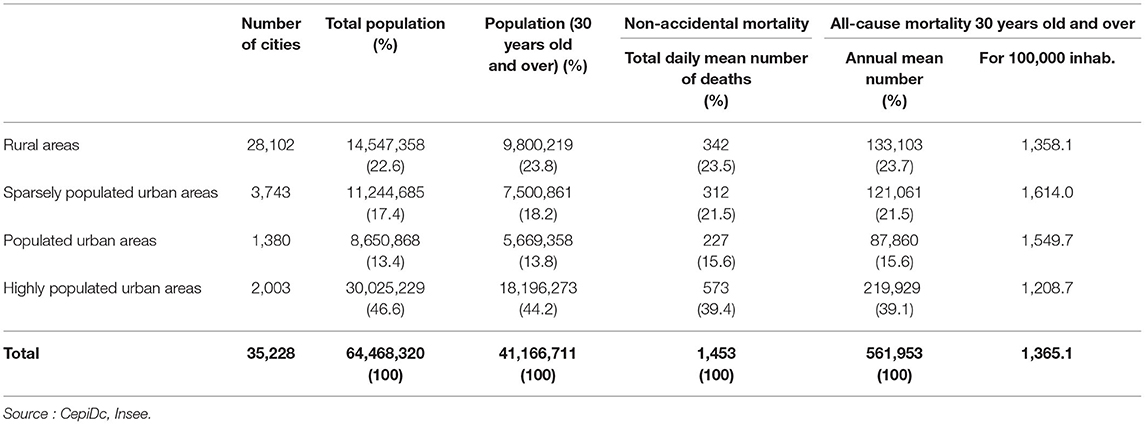
Table 3. Population and mortality by area in metropolitan France, 2014–2016.
Short-Term Impact of the Lockdown on Mortality
Under the short-term impact scenario, 243 and 61 deaths were postponed, respectively, thanks to the reductions in NO2 and PM10 concentrations during the strict lockdown in metropolitan France. In highly populated urban areas, the reduction in mortality was 0.3% for NO2 and 0.08% for PM10 over the study period (Table 4).

Table 4. Short-term impacts on mortality of PM10 and NO2 reductions in metropolitan France from March 16 to June 22, 2020.
During the gradual lifting, 39 and 8 deaths were postponed, respectively, thanks to the decreases in NO2 and PM10, which are about six and eight times less than during the strict lockdown. In highly populated urban areas, the reduction in mortality was 0.1% for NO2 and 0.01% for PM10 over the study period (Table 4).
Estimates obtained with daily mean differences using surface-weighted concentrations were very close to those obtained from daily mean differences using population-weighted concentrations (Supplementary Table 2).
Long-Term Impact of the Lockdown on All-Cause Mortality
Air Pollution Levels
On average, from July 1, 2019 to June 30, 2020, there was an exposure gradient from rural to highly populated urban areas that was higher for NO2 than for PM2.5 (Table 2, Figure 3).
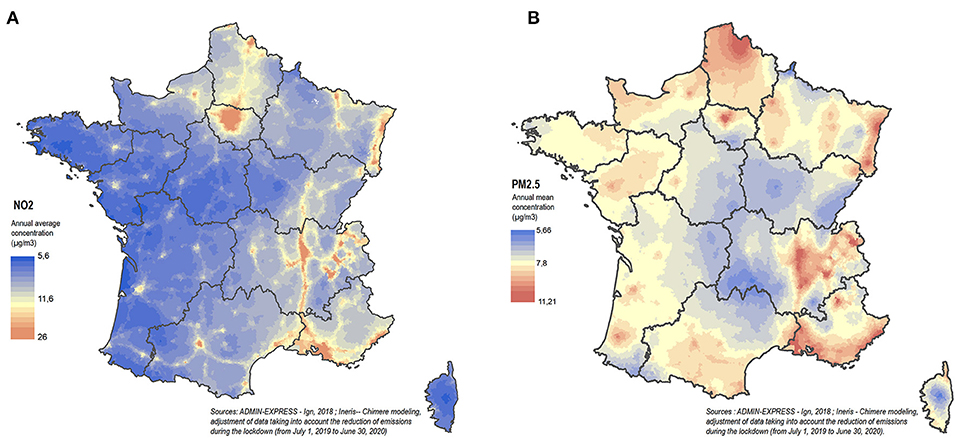
Figure 3. Distribution of average NO2 (A) and PM2.5 (B) concentrations by municipality from July 1, 2019 to June 30, 2020 (CHIMERE modeling, adjustment of data taking into account the lowered emissions during the lockdown).
The annual average of daily differences obtained from surface-weighted concentrations was also very close to averages obtained from population-weighted concentrations (Supplementary Table 1).
Population and Mortality Descriptive Data
The average annual number of deaths from all causes of persons aged 30 and over residing in metropolitan France for 2014–2016 was 561,953 (Table 3).
Long-Term Impact of the Lockdown on Mortality and Life Expectancy
Under the long-term impact scenario of the lockdown, from July 1, 2019 to June 30, 2020, 2,274 and 893 deaths were postponed, respectively, thanks to reductions in PM2.5 and NO2 concentrations in metropolitan France. In highly populated urban areas, the reduction in annual mortality was 0.4% for PM2.5 and 0.2% for NO2 (Table 5, Figure 4).
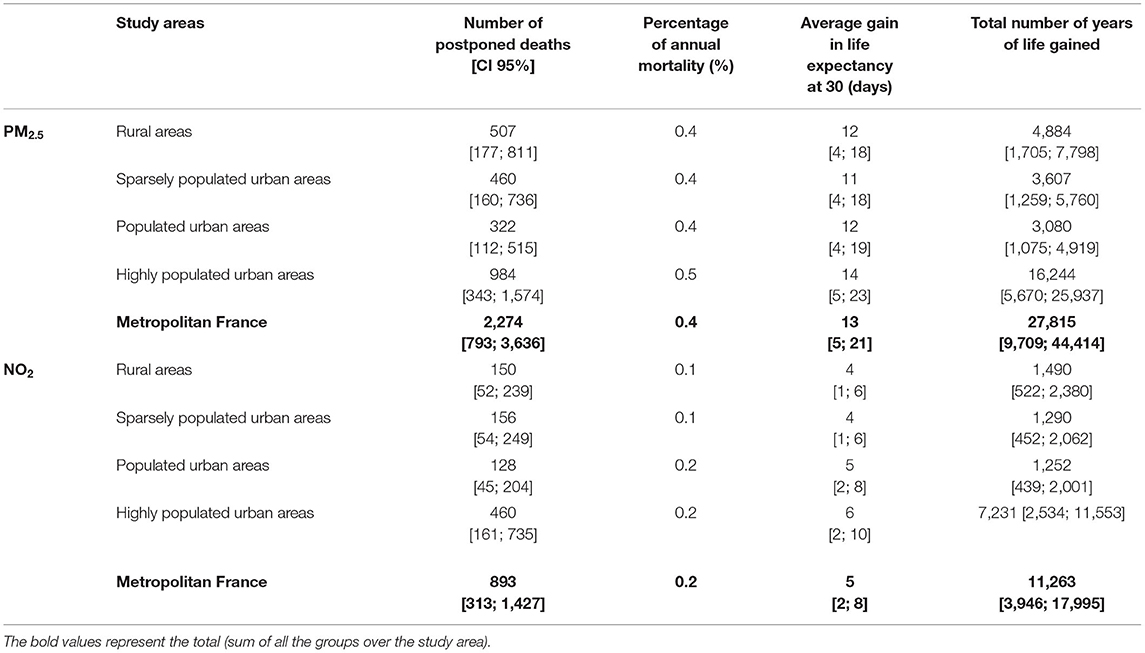
Table 5. Long-term impacts on mortality and life expectancy of PM2.5 and NO2 reductions in metropolitan France from July 1, 2019 to June 30, 2020.
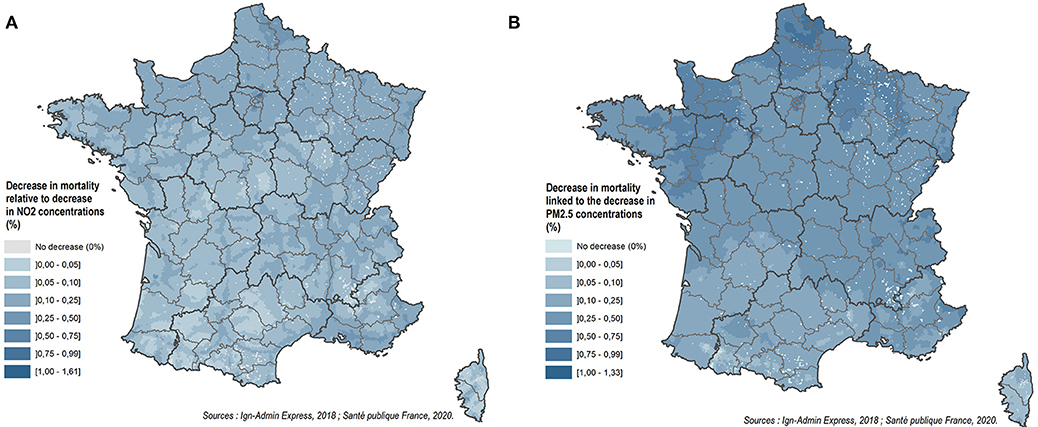
Figure 4. Impact of the decrease in NO2 (A) and PM2.5 (B) concentrations on mortality by municipality from July 1, 2019 to June 30, 2020 in metropolitan France.
People aged 30 would gain an average of 13 days of life expectancy resulting from the decrease in exposure to PM2.5 and 5 days resulting from the decrease in exposure to NO2, corresponding, respectively, to 27,815 and 11,263 years of life gained (Table 5).
Estimates obtained with annual average of daily differences using surface-weighted concentrations were very close to those obtained from annual differences using population-weighted concentrations (Supplementary Table 3).
Discussion
This QHIA focused on mortality, the most robust health indicator used in epidemiological studies establishing the role of air pollution in affecting health.
Summary of Findings
The results showed that the decrease in air pollution levels observed in metropolitan France during the spring 2020 lockdown led to a reduction in NO2 and PM concentrations. PM reductions were not as high as NO2 reductions. The daily mean difference between the estimated PM10 level during lockdown and its reference (modeled concentrations without lockdown) was −8.3 μg.m−3. This difference was −2.1 μg.m−3 for NO2. Moreover, the exposure reduction gradient from rural to urban areas was larger for NO2 than for PM10 and PM2.5.
The reduction in air pollution levels observed during the lockdown led to a non-negligible impact on mortality and life expectancy. In total, the benefits can be estimated at 2,300 deaths resulting from the decrease in the population's exposure to PM2.5 and 1,200 deaths resulting from the decrease in the population's exposure to NO2. These benefits are mainly due to avoided long-term effects (reduction in the contribution of pollution in the development of severe chronic diseases leading to death), and to a lesser extent to short-term effects (exacerbation of pre-existing diseases). Note that to avoid overlapping, the effects of NO2 and PM cannot be totaled together. The estimated benefits of the lockdown are mainly attributable to NO2 for short-term impacts and to PM2.5 for long-term impacts.
Comparison With the Global Burden of Air Pollution on Mortality in France
The results for the lockdown impacts on mortality must be put into perspective with the total burden on mortality of reductions in PM2.5 and NO2 levels resulting from sustainable interventions over the long term. For this purpose, we implemented another scenario on the long-term effects of PM2.5 and NO2 on all-cause mortality in the 30 plus age group in metropolitan France. We calculated the difference between the annual population-weighted average concentrations of PM2.5 and NO2, from the CHIMERE model data for the period 2016–2019, and reference values of 5 μg/m3 for PM2.5 and of 10 μg/m3 for NO2, the latter corresponding to a situation without anthropogenic sources of air pollution. Concerning PM2.5 levels, the chosen reference value is very close to the value of 4.9 μg/m3 used in the QHIA previously conducted during 2007–2008 in France, which represents the 5th percentile of the PM2.5 distribution observed only in mountainous areas (Pascal et al., 2016). For NO2, the reference value represents the 25th percentile of the NO2 distribution, and was chosen by the European Environment Agency (EEA) (EEA, 2020) for a sensitivity analysis based on the Raaschou-Nielsen et al. publication (Raaschou-Nielsen et al., 2012). We estimated that 39,541 [14,160; 61,690] deaths in the 30 plus age group were attributable to long-term exposure to PM2.5 and 6,790 [2,400; 10,763] deaths in the 30 plus age group for NO2.
A sensitivity analysis was performed to explore the influence of: (1) different reference values to estimate the anthropogenic part of pollution exposure; and (2) different CRFs. The findings show that besides exposure modeling, these two parameters play a key role in QHIA findings. For example, with an alternative reference level of 0 μg/m3 and a CRF of 1.06 [1.04; 1.08] for PM2.5 equivalent to the choices made by the EEA, we found comparable estimates for France (32,436 deaths and 33,100 deaths for the EEA). The minor difference is mostly due to differences in exposure modeling (EEA, 2020). Detailed findings are presented in Supplementary Table 4.
These findings on the global burden of air pollution on mortality show that, beside the ad-hoc health benefits related to the lockdown, long-term exposure to air pollution is still a significant risk factor for mortality in the French population.
Other QHIAs
These findings can also be compared to other studies (Table 6).
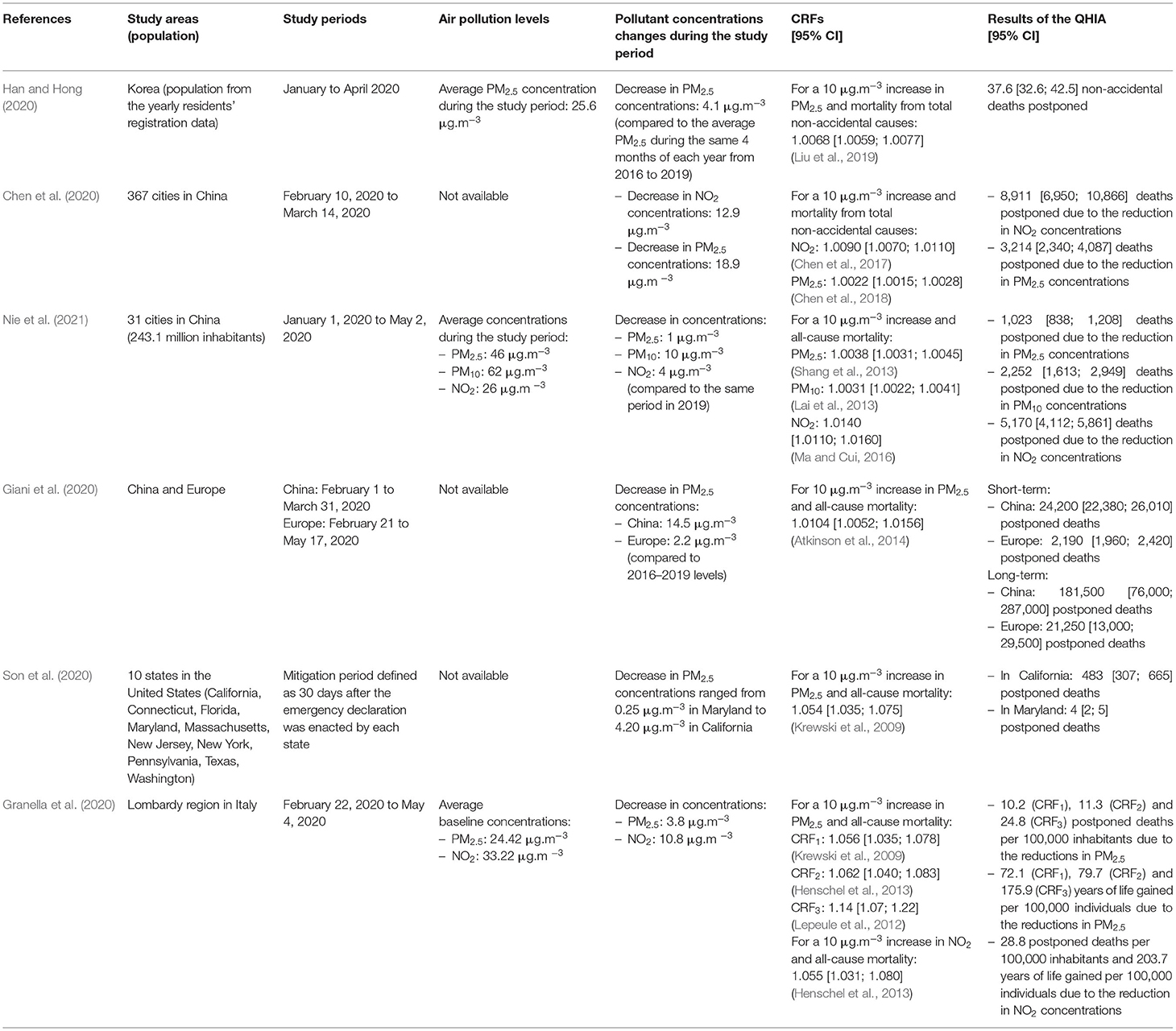
Table 6. Summary of published studies quantifying the impact of lockdown measures on reductions in ambient air pollutant concentrations and the resulting number of postponed deaths.
Han and Hong in 2020 estimated the short-term benefits of PM2.5 reduction and changes in public behavior during the Covid-19 crisis in Seoul, Korea. They estimated a decrease of 4.1 μg.m−3 of PM2.5 during the first 4 months of 2020 compared to the average PM2.5 concentration during the same 4 months of each year from 2016 to 2019. They estimated that 37.6 [32.6; 42.5] deaths were postponed due to this reduction (Han and Hong, 2020).
In May 2020, Chen et al. estimated that the lockdown led to improvements in air quality with a reduction of about 12.9 μg.m−3 of NO2 and 18.9 μg.m−3 of PM2.5 in 367 cities in China. This estimate is based on the comparison with the levels observed during the period from 2016 to 2019 before the lockdown, controlled for the long-term declining trend in air pollution. Approximately 9,000 and 3,000 non-Covid-related postponed deaths were estimated, respectively, in relation to these reductions in PM2.5 and NO2 concentrations in the short term. However, the authors state that their findings should take into account the effect on the mortality rate of the disruption in the use of health-care systems during lockdown that may have affected the treatment of patients with chronic diseases (Chen et al., 2020).
In addition, over the period from January 1 to May 2, 2020, as a result of lockdown measures Nie et al. in 2020 found an overall improvement in air quality in 31 cities in China compared to the same period in 2019 only considering the short-term effect. In total, 1,023 deaths were postponed linked to a reduction in PM2.5 concentrations, 2,252 deaths were postponed in relation with reductions in PM10 concentrations, and 5,170 deaths were postponed linked to reductions in NO2 concentrations. However, the comparison to a single historical year can lead to biases, and in their analyses the authors could not separate out the influence of meteorological factors on air pollutants (Nie et al., 2021).
Giani et al. (2020) estimated that lockdown measures led to a decrease in PM2.5 levels of 14.5 μg.m−3 in China and 2.2 μg.m−3 in Europe, when compared to levels from 2016 to 2019. In the short term, they estimate that 24,200 [22,380; 26,010] deaths were postponed throughout China between February 1 and March 31, 2020 and 2,190 [1,960; 2,420] deaths were postponed in Europe between February 21 and May 17, 2020. In the long term, 181,500 [76,000; 287,000] deaths were postponed in China and 21,250 [13,000; 29,500] for Europe in different prospective scenarios of economic recovery (from immediate resumption to permanent lockdown for the whole year 2020) (Giani et al., 2020).
Son et al. estimated changes in levels of PM2.5 during the lockdown period vs. the baseline period (pre-mitigation measure) in 10 states of the United States. PM2.5 reductions during the lockdown period ranged from 0.25 μg.m−3 in Maryland to 4.20 μg.m−3 in California. They estimated that these reductions led to 483 [307; 665] postponed deaths in the urban areas of California and 4 [2; 5] postponed deaths in Maryland. The main limit of this work mentioned by the authors is the adoption of a CRF from a long-term exposure study applied to a 30-day exposure period (Son et al., 2020).
In the Lombardy region in northern Italy, Granella et al. in 2020 estimated that the improvement in air quality during the lockdown permitted a decrease in PM2.5 concentrations of 3.8 and of 10.8 μg.m−3 for NO2. During the lockdown, the decrease in PM2.5 led to a number of postponed deaths ranging from 10.2 to 28.8 per 100,000 inhabitants depending on the CRF and to a gain of years of life ranging from 72.1 to 175.9 per 100, 000 inhabitants depending on the CRF (see Table 6 for more details). The decrease in NO2 postponed 28.8 deaths per 100,000 inhabitants and led to a gain of 203.7 years of life per 100,000 inhabitants. However, the estimations used a relative risk calculated for long-term effects applied to a decrease in concentrations observed over 2 months, which does not correspond to an annual decrease in long-term exposure. This may likely cause the benefits to be overestimated (Granella et al., 2020).
The results of these studies published internationally, notably in Seoul, China, Europe as a whole, Italy and the United States, show, like those of our study, that the lockdown measures led to reductions in ambient air pollutant concentrations and the resulting number of postponed deaths. However, the calculation assumptions differ, which limits the possibilities of comparison.
Interpretation and Uncertainties
Uncertainties Related to Health Indicators
The most recent mortality data available was for the period 2014–2016, which did not include the study periods. This delay in data availability is due to the time required by the CépiDC (service ensuring the coding and validation procedures) for data processing in order to guarantee the completeness and quality of the data. Some changes in demographics or health conditions may have occurred between 2014 and 2019. However, preliminary data show that population remained quite stable during this period in France (i.e., from 64 to 65 million people8) and that mortality increased only by 0.07%9 during this period.
Interpretation and Uncertainties Related to Exposure Modeling
As previously shown, observed PM reductions were not as high as NO2 reductions, and the exposure gradient from rural to urban areas was greater for NO2 than for PM10 and PM2.5.
Indeed, sharper gradients for NO2 are expected as NO2 is a pollutant with a shorter lifetime. The highest concentrations are obtained near the sources of emissions, mainly in urban areas (road traffic accounting for more than half of French NOx emissions).
Indeed, although road traffic has been drastically reduced, it has not completely disappeared, and emissions from other sectors (and especially the agricultural and residential sectors) have maintained background pollution. For example, emissions related to springtime agricultural sprays (manure/slurry and nitrogen fertilizers) remained at their usual levels. This was also observed for heating during cold days at the beginning of the epidemic, and for the burning of green waste (prohibited in France), which are major sources of PM emissions. The reduction in industrial emissions depended on the sector of activity. In addition, particles have a lifetime of a few days and can be formed in the atmosphere by oxidation and condensation processes. Particles can thus be transported away from their emission sources, explaining a less pronounced urban/rural gradient.
Regarding uncertainties, the assessment of exposure to ambient air pollution is based here on air quality models for which uncertainties can be distinguished between the input data and the model itself.
The main inputs are the meteorological variables (temperature, wind, precipitation, etc.) influencing the transport and transformation of pollutants and the emissions of pollutants and precursors. While meteorological uncertainties can be high for forecasts, here we have used reanalyzed data corresponding to past days and therefore corrected with measured concentrations, thereby minimizing uncertainties. On the contrary, uncertainties can be large for emissions of pollutants and precursors, and even greater when estimating to what extent restrictions on lockdown activities have led to emission reductions.
The chemistry-transport model itself has uncertainties related: to its ability to properly reproduce the physical and chemical mechanisms at work in the atmosphere; and to its spatial representativeness. Knowledge of physical and chemical mechanisms is imperfect, and their representation in numerical models is equally imperfect. These limitations are reduced using reanalyzed data, that is, combining simulation and data observed at monitoring stations. For historical data, the concentrations were evaluated by cross validation at the stations with satisfactory scores (correlations between 0.77 and 0.94, biases <20%). These corrections are however limited by the availability of monitoring stations, which are fewer in mountainous environments but fortunately more common in heavily populated areas.
We also tested an alternative method to estimate the decrease (or increase) in air pollution during the studied period. We compared the variations of exposure obtained using historical references to those obtained from modeled references during the hypothetical period without lockdown and shown in the findings section. Discrepancies were observed between the two methods (Supplementary Tables 5, 6). Historical differences refer, for short-term impact of the lockdown, to the calculation of daily differences between the concentrations observed during the lockdown (from March 16 to June 22, 2020) and the daily average concentrations from March 16 to June 22, 2017–2019. Concerning the daily mean differences, decreases in pollutant concentrations are observed with both methods, except for PM10 levels for which an increase in concentrations during the strict lockdown is observed with the historical references method.
For the long-term impact of the lockdown, for each quarter of the year historical references refer to the daily differences between the concentrations observed from July 1, 2019 to June 30, 2020 and the daily average concentrations from July 1, 2016 to June 30, 2019. Decreases in pollutant concentrations are observed for each quarter of the year (from July 2019 to June 2020). This analysis suggests a persistent decline in pollution levels since 2016. The maximum decrease is reached during the fourth quarter of 2019 (October to December 2019).
With the historical references method it was not possible to distinguish the decline in long-term pollutant levels from the decrease related to the lockdown alone.
These variations could be explained by meteorological factors. Menut et al. in 2020 show that in Europe the effect of lockdown measures was smaller for PM concentrations than for NO2, and from 1 year to another the weather effect can probably compensate for the expected reductions in concentrations related to the lockdown (Menut et al., 2020).
It is therefore difficult to separate out precisely the relative importance of weather and of temporary and long-term variations in emissions (Barré et al., 2020). This is why the method of differences obtained from simulations with and without lockdown was chosen in order to be free from the meteorological influence.
Unusual Factors and Consequences of the Lockdown
When interpreting the results of this QHIA we should keep in mind that the lockdown has created an exceptional change in the conditions of exposure of the population to outdoor air pollution. There has been a reduction in travel, much more time spent in indoor environments, changes in noise, lifestyle and behavior, and decrease or delay in screening and access to healthcare that may lead to subsequent increases in morbidity and mortality. Our analysis could not quantify the influence of these exceptional factors, but they are examined qualitatively hereafter.
Population Exposure to Outdoor Air Pollution
The major economic downturn has resulted in lower emissions and pollutant concentrations during lockdowns, which may have led to a change in the composition of PM. The health effects of PM2.5 appear to differ according to their chemical composition (Bell, 2012; Adams et al., 2015; Daellenbach et al., 2020; Son et al., 2020). Thus, it can be assumed that changes in baseline activities and transportation because of lockdown policies may have altered the chemical composition of PM, and these changes would also have different characteristics in different regions. Thus, CRFs for PM may have changed during our study period compared to usual exposures (Son et al., 2020). This QHIA does not account for this possible change in chemical composition and sources of PM as the CRFs used could not be calculated for the lockdown period. In addition, the chemical composition of PM may vary by location, time and season due to differences in pollutant sources (Adams et al., 2015; Bates et al., 2018).
Population Exposure to Indoor Air Pollution
Lockdown measures may have had the opposite effect from outdoor air pollution. Indeed, indoor air quality depends not only on the transfer of pollutants from outside to inside but also on the emission of various pollutants via building materials and furnishings as well as lifestyle habits (heating and cooking methods, cleaning or ambient products, smoking, etc.) (OQAI, 2007). The increase in the time spent at home and the activities carried out in this space (cooking, home repairs, etc.) may therefore have led to greater exposure of the population (Son et al., 2020). One example is the 20% increase in calls to poison control centers, which was attributed to an increase in accidents involving cleaning products and disinfectants (Chang et al., 2020). Initial data, from micro-sensor measurements in about 1,000 households in Europe, have thus revealed an increase of 15–30% in CO2 and volatile organic compounds concentrations between March and May10. Pollutants present in indoor environments have a significant impact on health, especially respiratory health (Hulin et al., 2012). In addition, these changes in indoor activities may have caused a change in noise exposure. Additional data on a larger scale would be necessary to confirm these initial observations and to take into account the health impact of these changes in indoor environments in epidemiological studies providing CRFs for QHIAs of outdoor air pollution.
Impacts on Mental Health
During the lockdown, increases in violence and stress have been observed (WHO, 2020). Since the beginning of the epidemic, several authors studied the measures taken to limit the spread of Covid-19 (strict lockdown, physical distancing, quarantines, etc.) and their psychological impacts on the population, as seen during previous epidemics due to MERS-Cov and SARS. These effects include psychological distress, anxiety-depressive disorders, post-traumatic stress symptoms and sleep disorders, some of which could last up to several years after the end of lockdown (Brooks et al., 2020; Mukhtar, 2020). In addition, unverified claims on social media about the uncertainty and unpredictability surrounding Covid-19 create anxiety among people. Furthermore, among physicians and nurses, significant deterioration in mental health is reported with burnout, frustration, hopelessness, and discrimination, coupled with fear of contracting the disease due to inadequate personal protective equipment (Kang et al., 2020).
Millions of people have lost their jobs. People employed in the informal and unorganized sectors are worst hit as they struggle for food, shelter and their livelihoods, creating uncertainty leading to depression, suicide, self-harm, etc. (Kumar and Nayar, 2020).
In France, in March 2020 Santé publique France launched the CoviPrev11 survey of the general population to monitor changes in behavior and mental health. The survey observed that mental health, which deteriorated at the beginning of the lockdown, then improved significantly except for sleep problems. Current life satisfaction gradually improved after the second week of lockdown, with a significant improvement observed when the lockdown was lifted. Anxiety decreased significantly during the first weeks of the lockdown and then remained stable. Depressive states, after an increase observed in the middle of April, decreased significantly following lifting of the lockdown. Depressive prevalence continued to decrease significantly until the end of September.
Again, these changes in behaviors and their consequences for mental health could not be quantified in our QHIA.
Impacts of Reduced Physical Activity
During the lockdown in France, half the population did <30 min of daily physical activity, while one third reported high levels of sedentary lifestyle (over 7 h seated). People in poorer socio-economic categories and women with lower levels of education, temporarily or long-term unemployed, were more affected by the lack of physical activity. In terms of mental health, the lack of and decrease in physical activity and high levels of sedentary lifestyle compared to before the lockdown were associated differently by gender with anxiety, depression and sleep problems reported during the lockdown (Escalon et al., 2021).
Impacts in Screening and Access to Healthcare
During the lockdown and out of fear of COVID-19, there was a decrease in the use of healthcare use with the risk of an aggravation of certain diseases. In the United States, a study by Graciano et al. in 2020 observed a sharp decline in admissions to pediatric intensive care units during lockdown, mainly due to a decrease in respiratory infections (Graciano et al., 2020). However, the authors interpret this in a multifactorial way: there was less person-to-person contact, better air quality, and perhaps the fear of going to the hospital during the pandemic. Indeed, healthcare professionals in the U.S. and elsewhere have expressed concern about the drop in the number of patients going to emergency departments for heart attacks, strokes and other conditions.
Santé publique France reports a significant decrease in the number of doctors' appointments from the beginning of the lockdown to mid-April 2020, compared to the data for 2019. There was a decrease of 51% among specialized physicians, slightly less marked among general practitioners (25%). In addition, less use of health care for people with chronic illnesses and acute pathologies was observed. At the beginning of the lockdown, a decrease was observed in the number of emergency-room visits and hospitalizations for cardio- and neurovascular pathologies likely to represent vital emergencies requiring immediate care. On the other hand, later on an increase in hospitalizations in the emergency department for these same pathologies was observed, suggesting a delay in treatment for patients who had waited to go to the emergency department, particularly from fear of contamination12.
Improvements in Health
Some beneficial consequences of lockdown for health and well-being related to the reduction in activities are seen in diet and noise. In Spain, an online questionnaire with 7,514 participants was conducted to determine if dietary behaviors of the Spanish adult population changed during the lockdown (Rodríguez-Pérez et al., 2020). Compared with previous habits, it observed that participants adopted healthier dietary behaviors, like decreased intake of fried foods, snacks and fast foods, and increased consumption of food such as vegetables, fruits, and olive oil.
In France, the Acoucité study reports measurements reflecting a significant decrease in noise levels during lockdown of 4–6 dB, corresponding to a 60–75% decrease in sound energy (Acoucité, 2020). These results are consistent with inhabitants' perceptions. The results of the online perception survey conducted during the lockdown show that, on a scale of 0 to 10, the perceived noise level, all sources combined, went from 6.3 points on average to 2.4 points; it thus decreased by 3.9 points with regional differences. In addition to the impact identified or perceived in decibel levels, the composition of the noise environment in cities has been profoundly modified. The dominant presence of transport noise and sounds linked to other human activities (deliveries, shops, voices, etc.) was now receding, giving way to sounds that were already present but still barely perceptible. The results of the perception survey clearly show how naturally occurring sounds have become predominant during lockdown periods. This change in the soundscape is accompanied by positive adjectives (“calm,” “pleasant,” “peaceful”) chosen by the respondents (Acoucité, 2020).
In addition, traffic mortality rates were exceptionally low in France during the lockdown. In April and May the numbers of road deaths were, respectively, 103 (55.8% less than in April 2019) and 205 (a 15.6% decrease compared to May 2019)13.
In total, despite the tragic consequences of the Covid-19, the lockdown in spring 2020 showed benefits in terms of diet, reduction in noise and air pollution levels and lower road accidents, but also negative consequences in terms of mental health, decrease in physical activity, increase in sedentary lifestyle, decrease or delay in screening and access to healthcare or poorer indoor air quality. All these changes induced by the lockdown highlight the importance of considering the combined effects of multiple factors that can improve or worsen our health, but our analysis was unable to quantify the influence of these factors due to the lack of perspective and availability of data. Methodological developments in terms of CRFs integrating multiple exposures and their health impacts in line with those designed by the Global Burden of Disease on competing risks (Causey et al., 2021) should be deployed in order to implement effective outdoor air-pollution reduction measures.
Conclusion
This study estimates the consequences for mortality among the French population linked to the reduction in ambient air pollution observed during the first lockdown in spring 2020. The benefits of the observed reduction can be estimated as 2,300 postponed deaths for PM2.5 and 1,200 for NO2, mainly due to avoided long-term effects. These findings must be viewed in perspective with the 40,000 deaths attributable to long-term exposure to PM2.5 and almost 7,000 deaths attributable to NO2, estimated over a 3-year period.
The results of this study confirm that, in a new context that is certainly neither realistic nor desirable for improving air quality in the long term, public-action measures reduce air pollution levels and therefore both the population's exposure and pollution's impact on health. Some lessons can already be learned in terms of public-action measures and behavioral changes that are likely to be lasting in France.
Moreover, in a broader and long-term perspective, this study reminds us, and underlines the fact that the total burden of air pollution on health remains a significant and still relevant risk factor in France. Thus, efforts to reduce ambient air pollution must be pursued sustainably for all sources of air pollution with suitably adapted but nonetheless ambitious change.
These efforts include: continuing public action to reduce traffic in urban areas and industrial emissions; faster changes in population behavior such as teleworking, travel patterns and emission-free travel. Other actions contributing to the reduction of air pollution include: improvement in wood-based heating practices (use of high-performance appliances, choice of good quality fuels, overhead lighting, etc.); thermal renovation of dwellings; and the development of good agricultural practices to reduce ammonia emissions.
Finally, the activity restrictions imposed to limit the spread of Covid-19 have had several consequences for the health of the general population, both positive and negative. These consequences highlight the need to conduct more integrated assessments of health impacts that include the multisectoral consequences of interventions, particularly in terms of population compliance with mitigating restrictions, behavior and mental health and, more broadly, climate change.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: Exposure data were modelised just for this study. Mortality by causes data are not available without a CNIL agreement. Requests to access these datasets should be directed to https://www.ineris.fr/en (exposure data); https://snds.gouv.fr/SNDS/Accueil (mortality data).
Author Contributions
SM, VW, MP, and SH: conceptualization. VW, LA, PC, AC, BB, and ER: methodology. VW, PC, and LA: analysis. MC: data curation. SM, AD, FC, MA, MH, and MC: writing—original draft preparation—review. SM and LA: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
A special thank you to Michael Saklad for careful reviewing and editing.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frsc.2021.643821/full#supplementary-material
Footnotes
1. ^https://www.santepubliquefrance.fr/dossiers/coronavirus-covid-19
2. ^https://atmo-france.org/covid-19-focus-sur-lexposition-des-riverains-a-la-pollution-automobile-pres-des-grands-axes-avant-pendant-le-confinement-21-avril-2020/
3. ^https://www.ineris.fr/fr/ineris/actualites/impact-confinement-amelioration-qualite-air-bilan
4. ^Gradual lifting corresponds to a gradual resumption of economic activity following the strict lockdown.
7. ^Concentration-response functions (CRF) or relative risks (RR) represent the relationship between an air-pollution indicator and a health effect estimated by epidemiological studies.
8. ^https://www.ined.fr/fr/tout-savoir-population/graphiques-cartes/population_graphiques/
9. ^https://www.insee.fr/fr/statistiques/2383440#tableau-figure1
10. ^https://www.scientificamerican.com/article/coronavirus-lockdowns-may-raise-exposure-to-indoor-air-pollution/
11. ^https://www.santepubliquefrance.fr/etudes-et-enquetes/covid-19-une-enquete-pour-suivre-l-evolution-des-comportements-et-de-la-sante-mentale-pendant-l-epidemie
12. ^https://www.santepubliquefrance.fr/presse/2020/covid-19-et-continuite-des-soins-continuer-de-se-soigner-un-imperatif-de-sante-publique
13. ^https://www.onisr.securite-routiere.gouv.fr/etat-de-l-insecurite-routiere
References
Acoucité (2020). “Confinement suite à la pandémie COVID-19 - Conséquences sur l'environnement sonore”. Lyon: Observatoire de l'environement sonore.
Adams, K., Greenbaum, D. S., Shaikh, R., van Erp, A. M., and Russell, A. G. (2015). Particulate matter components, sources, and health: systematic approaches to testing effects. J. Air Waste Manag. Assoc. 65, 544–558. doi: 10.1080/10962247.2014.1001884
Atkinson, R. W., Kang, S., Anderson, H. R., Mills, I. C., and Walton, H. A. (2014). Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: a systematic review and meta-analysis. Thorax 69, 660–665. doi: 10.1136/thoraxjnl-2013-204492
Barré, J., Petetin, H., Colette, A., Guevara, M., Peuch, V. H., Rouil, L., et al. (2020). Estimating lockdown induced European NO2 changes. Atmos. Chem. Phys. Discuss. 2020, 1–28. doi: 10.5194/acp-2020-995
Bates, J. T., Weber, R. J., Verma, V., Fang, T., Ivey, C., Liu, C., et al. (2018). Source impact modeling of spatiotemporal trends in PM2.5 oxidative potential across the eastern United States. Atmos. Environ. 193, 158–167. doi: 10.1016/j.atmosenv.2018.08.055
Beauchamp, M., Bessagnet, B., de Fouquet, C., Malherbe, L., Meleux, F., and Ung, A. (2018). An additive geostatistical model for mixing total and partial PM10 observations with CHIMERE rCTM. Atmos. Environ. 189, 61–79. doi: 10.1016/j.atmosenv.2018.06.035
Beauchamp, M., de Fouquet, C., and Malherbe, L. (2017). Dealing with non-stationarity through explanatory variables in kriging-based air quality maps. Spat. Stat. 22, 18–46. doi: 10.1016/j.spasta.2017.08.003
Bell, M. L. (2012). Assessment of the Health Impacts of Particulate Matter Characteristics. Boston, MA: Health Effects Institute.
Bessagnet, B., Beauchamp, M., Guerreiro, C., de Leeuw, F., Tsyro, S., Colette, A., et al. (2014). Can further mitigation of ammonia emissions reduce exceedances of particulate matter air quality standards? Environ. Sci. Policy 44, 149–163. doi: 10.1016/j.envsci.2014.07.011
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/S0140-6736(20)30460-8
Causey, K., Burkart, K., Collman, G., Hu, H., Brauer, M., and London, S. J. (2021). Increasing the impact of environmental epidemiology in the global burden of disease project. Epidemiology 32, 1–5. doi: 10.1097/EDE.0000000000001273
Chang, A., Schnall, A. H., Law, R., Bronstein, A. C., Marraffa, J. M., Spiller, H. A., et al. (2020). Cleaning and disinfectant chemical exposures and temporal associations with COVID-19 - National Poison Data System, United States, January 1, 2020-March 31, 2020. MMWR Morb. Mortal. Wkly Rep. 69, 496–498. doi: 10.15585/mmwr.mm6916e1
Chen, K., Wang, M., Huang, C., Kinney, P. L., and Anastas, P. T. (2020). Air pollution reduction and mortality benefit during the COVID-19 outbreak in China. Lancet Planet. Health 4, e210–e212. doi: 10.1016/S2542-5196(20)30107-8
Chen, R., Yin, P., Meng, X., Liu, C., Wang, L., Xu, X., et al. (2017). Fine particulate air pollution and daily mortality. a nationwide analysis in 272 Chinese cities. Am. J. Respir. Crit. Care Med. 196, 73–81. doi: 10.1164/rccm.201609-1862OC
Chen, R., Yin, P., Meng, X., Wang, L., Liu, C., Niu, Y., et al. (2018). Associations between ambient nitrogen dioxide and daily cause-specific mortality: evidence from 272 Chinese cities. Epidemiology 29, 482–489. doi: 10.1097/EDE.0000000000000829
COMEAP (2018). Associations of Long-Term Average Concentrations of Nitrogen Dioxide With Mortality. London: Public Health England.
Corso, M., Blanchard, M., Medina, S., and Wagner, V. (2020). Short-term associations of nitrogen dioxide (NO2) on mortality in 18 French cities, 2010-2014. Atmosphere 11, 1–18. doi: 10.3390/atmos11111198
Couvidat, F., Bessagnet, B., Garcia-Vivanco, M., Real, E., Menut, L., and Colette, A. (2018). Development of an inorganic and organic aerosol model (CHIMERE 2017β v1.0): seasonal and spatial evaluation over Europe. Geosci. Model Dev. 11, 165–194. doi: 10.5194/gmd-11-165-2018
Daellenbach, K. R., Uzu, G., Jiang, J., Cassagnes, L. E., Leni, Z., Vlachou, A., et al. (2020). Sources of particulate-matter air pollution and its oxidative potential in Europe. Nature 587, 414–419. doi: 10.1038/s41586-020-2902-8
EPA (2016). Integrated Science Assessment (ISA) for Oxides of Nitrogen-Health Criteria. Washington, DC: U.S. Environmental Protection Agency (EPA).
ERS (2019). Air Pollution And Health Facts & Myths. Available online at: https://www.ogp.at/wp_ogp/wp-content/uploads/ERS-Factsheet-on-air-pollution.pdf (accessed April 21, 2021).
Escalon, H., Deschamps, V., and Verdot, C. (2021). Activité physique et sédentarité des adultes pendant la période de confinement lié à l'épidémie de Covid-19 : état des lieux et évolutions perçues (CoviPrev, 2020). Bull. Epidémiol. Hebd. 3, 2–13.
Giani, P., Castruccio, S., Anav, A., Howard, D., Hu, W., and Crippa, P. (2020). Short-term and long-term health impacts of air pollution reductions from COVID-19 lockdowns in China and Europe: a modelling study. Lancet Planet. Health 4, e474–e482. doi: 10.1016/S2542-5196(20)30224-2
Graciano, A. L., Bhutta, A. T., and Custer, J. W. (2020). Reduction in paediatric intensive care admissions during COVID-19 lockdown in Maryland, USA. BMJ Paediatr. Open 4:e000876. doi: 10.1136/bmjpo-2020-000876
Granella, F., Reis, L. A., Bosetti, V., and Tavoni, M. (2020). COVID-19 lockdown only partially alleviates health impacts of air pollution in Northern Italy. Environ. Res. Lett. 16, 1–19. doi: 10.31219/osf.io/b38h2
Guevara, M., Jorba, O., Soret, A., Petetin, H., Bowdalo, D., Serradell, K., et al. (2020). Time-resolved emission reductions for atmospheric chemistry modelling in Europe during the COVID-19 lockdowns. Atmos. Chem. Phys. Discuss. 2020, 1–37. doi: 10.5194/acp-2020-686-supplement
Han, C., and Hong, Y. C. (2020). Decrease in ambient fine particulate matter during COVID-19 crisis and corresponding health benefits in Seoul, Korea. Int. J. Environ. Res. Public Health 17:5279. doi: 10.3390/ijerph17155279
Harmon, A. C., Hebert, V. Y., Cormier, S. A., Subramanian, B., Reed, J. R., Backes, W. L., et al. (2018). Particulate matter containing environmentally persistent free radicals induces AhR-dependent cytokine and reactive oxygen species production in human bronchial epithelial cells. PLoS ONE 13:e0205412. doi: 10.1371/journal.pone.0205412
Henschel, S., Chan, G., and WHO (2013). Health Risks of Air Pollution in Europe - HRAPIE Project: New Emerging Risks to Health From Air Pollution - Results From the Survey Of Experts. Copenhagen: WHO Regional Office for Europe. doi: 10.1289/isee.2013.P-2-02-06
Hill, A. B. (1965). The environment and disease: association or causation? Proc. R. Soc. Med. 58, 295–300. doi: 10.1177/003591576505800503
Hulin, M., Simoni, M., Viegi, G., and Annesi-Maesano, I. (2012). Respiratory health and indoor air pollutants based on quantitative exposure assessments. Eur. Respir. J. 40, 1033–1045. doi: 10.1183/09031936.00159011
Jaligama, S., Patel, V. S., Wang, P., Sallam, A., Harding, J., Kelley, M., et al. (2018). Radical containing combustion derived particulate matter enhance pulmonary Th17 inflammation via the aryl hydrocarbon receptor. Part. Fibre Toxicol. 15:20. doi: 10.1186/s12989-018-0255-3
Kang, L., Li, Y., Hu, S., Chen, M., Yang, C., Yang, B. X., et al. (2020). The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry 7:e14. doi: 10.1016/S2215-0366(20)30047-X
Krewski, D., Jerrett, M., Burnett, R. T., Ma, R., Hughes, E., Shi, Y., et al. (2009). Extended Follow-up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality. Boston: Health Effects Institute.
Kumar, A., and Nayar, K. R. (2020). COVID 19 and its mental health consequences. J. Ment. Health 30, 1–2. doi: 10.1080/09638237.2020.1757052
Lai, H.-K., Tsang, H., and Wong, C.-M. (2013). Meta-analysis of adverse health effects due to air pollution in Chinese populations. BMC Public Health 13, 360–360. doi: 10.1186/1471-2458-13-360
Lepeule, J., Laden, F., Dockery, D., and Schwartz, J. (2012). Chronic exposure to fine particles and mortality: an extended follow-up of the Harvard Six Cities study from 1974 to 2009. Environ. Health Perspect. 120, 965–970. doi: 10.1289/ehp.1104660
Létinois, L. (2014). Méthodologie de Répartition Spatiale de la Population. Verneuil-en-Halatte: LCSQA.
Liu, C., Chen, R., Sera, F., Vicedo-Cabrera, A. M., Guo, Y., Tong, S., et al. (2019). ambient particulate air pollution and daily mortality in 652 cities. N. Engl. J. Med. 381, 705–715. doi: 10.1056/NEJMoa1817364
Ma, H.-Q., and Cui, L.- H. (2016). Meta-analysis on health effects of air pollutants (SO2 and NO2) in the chinese population. Occup. Health 32, 1038–1044.
Mailler, S., Menut, L., Khvorostyanov, D., Valari, M., Couvidat, F., Siour, G., et al. (2017). CHIMERE-2017: from urban to hemispheric chemistry-transport modeling. Geosci. Model Dev. 10, 2397–2423. doi: 10.5194/gmd-10-2397-2017
Medina, S., Plasencia, A., Ballester, F., Mücke, H. G., and Schwartz, J. (2004). Apheis: public health impact of PM10 in 19 European cities. J. Epidemiol. Commun. Health 58, 831–836. doi: 10.1136/jech.2003.016386
Menut, L., Bessagnet, B., Siour, G., Mailler, S., Pennel, R., and Cholakian, A. (2020). Impact of lockdown measures to combat Covid-19 on air quality over western Europe. Sci. Total Environ. 741:140426. doi: 10.1016/j.scitotenv.2020.140426
Mukhtar, S. (2020). Psychological health during the coronavirus disease 2019 pandemic outbreak. Int. J. Soc. Psychiatry 66, 512–516. doi: 10.1177/0020764020925835
Nie, D., Shen, F., Wang, J., Ma, X., Li, Z., Ge, P., et al. (2021). Changes of air quality and its associated health and economic burden in 31 provincial capital cities in China during COVID-19 pandemic. Atmos. Res. 249:105328. doi: 10.1016/j.atmosres.2020.105328
OQAI (2007). Campagne nationale logements : Etat de la qualité de l'air dans les logements français - rapport Final. Champs-sur-Marne: Observatoire de la Qualité de l'Air Intérieur (OQAI).
Pascal, M., de Crouy Chanel, P., Wagner, V., Corso, M., Tillier, C., Bentayeb, M., et al. (2016). The mortality impacts of fine particles in France. Sci. Total Environ. 571, 416–425. doi: 10.1016/j.scitotenv.2016.06.213
Pascal, M., Yvon, J.-M., and Medina, S. (2019). Pollution atmosphérique. Guide pour la réalisation d'une Évaluation Quantitative des Impacts sur la santé (EQIS). EQIS avec une exposition modélisée. Saint-Maurice: Santé publique France.
Petit, P. C., Fine, D. H., Vasquez, G. B., Gamero, L., Slaughter, M. S., and Dasse, K. A. (2017). The pathophysiology of nitrogen dioxide during inhaled nitric oxide therapy. ASAIO J. 63, 7–13. doi: 10.1097/MAT.0000000000000425
Raaschou-Nielsen, O., Andersen, Z. J., Jensen, S. S., Ketzel, M., Sorensen, M., Hansen, J., et al. (2012). Traffic air pollution and mortality from cardiovascular disease and all causes: a Danish cohort study. Environ. Health 11:60. doi: 10.1186/1476-069X-11-60
Rodríguez-Pérez, C., Molina-Montes, E., Verardo, V., Artacho, R., García-Villanova, B., Guerra-Hernández, E. J., et al. (2020). Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 12:1730. doi: 10.3390/nu12061730
Shang, Y., Sun, Z., Cao, J., Wang, X., Zhong, L., Bi, X., et al. (2013). Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ. Int. 54, 100–111. doi: 10.1016/j.envint.2013.01.010
Son, J. Y., Fong, K. C., Heo, S., Kim, H., Lim, C. C., and Bell, M. L. (2020). Reductions in mortality resulting from reduced air pollution levels due to COVID-19 mitigation measures. Sci. Total Environ. 744:141012. doi: 10.1016/j.scitotenv.2020.141012
WHO (2013). Health Risks of Air Pollution in Europe - HRAPIE Project - Recommandations for Concentration-Response Functions for Cost-Benefits Analysis of Particulate Matter, Ozone and Nitrogen Dioxide. Copenhagen: WHORegional office for Europe.
Keywords: health impact assessment, air pollution, mortality, lockdown, COVID-19, France
Citation: Adélaïde L, Medina S, Wagner V, de Crouy-Chanel P, Real E, Colette A, Couvidat F, Bessagnet B, Alter M, Durou A, Host S, Hulin M, Corso M and Pascal M (2021) Covid-19 Lockdown in Spring 2020 in France Provided Unexpected Opportunity to Assess Health Impacts of Falls in Air Pollution. Front. Sustain. Cities 3:643821. doi: 10.3389/frsc.2021.643821
Received: 18 December 2020; Accepted: 03 May 2021;
Published: 10 June 2021.
Edited by:
Sotiris Vardoulakis, Australian National University, AustraliaReviewed by:
Guy Coulson, National Institute of Water and Atmospheric Research (NIWA), New ZealandFerran Ballester, University of Valencia, Spain
Copyright © 2021 Adélaïde, Medina, Wagner, de Crouy-Chanel, Real, Colette, Couvidat, Bessagnet, Alter, Durou, Host, Hulin, Corso and Pascal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucie Adélaïde, bHVjaWUuYWRlbGFpZGVAc2FudGVwdWJsaXF1ZWZyYW5jZS5mcg==