
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 29 August 2024
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1444888
This article is part of the Research Topic Exploring the Multidimensional Impact of Homelessness on Health and Social Inclusion View all 9 articles
 Miguel A. Bedmar1
Miguel A. Bedmar1 Laura Capitán-Moyano1,2*
Laura Capitán-Moyano1,2* Miquel Bennasar-Veny1,2,3,4
Miquel Bennasar-Veny1,2,3,4 Cristina Moreno-Mulet2,3,5
Cristina Moreno-Mulet2,3,5 Alba Carrero-Planells2,3,5
Alba Carrero-Planells2,3,5 Aina M. Yáñez1,2,3,6
Aina M. Yáñez1,2,3,6Introduction: Homelessness is a phenomenon of social exclusion and poverty that has increased alarmingly during recent years. Homeless people (HP) experience violations of several basic human rights or needs that impact their well-being. Therefore, the aim of this research was to assess the health status and self-perceived health of HP and examining the impact of homelessness on their health.
Methods: We used an explanatory sequential mixed-methods approach that integrated a quantitative cross-sectional study within critical social and ethno-sociological qualitative frameworks. Data were collected in Palma, Spain, from December 1, 2020, to January 1, 2023. A total of 198 HP were recruited from the streets and public areas. Basic human needs (Virginia Henderson model), medical diagnoses, substance abuse (DAST-10), diet quality (IASE), depression (PHQ-9), and social support (SSQ-6) were assessed. Then, 17 semi-structured interviews were conducted and were analyzed using thematic content and discourse analysis. Quantitative and qualitative data were integrated and jointly analyzed.
Results: The 79.3% of the participants were men, mean age of 47.8 ± 12.2 years. The 76.4% were Spanish. The participants reported severe difficulties in accessing the labor market, and that this greatly affected their self-esteem and mental health. The 48.9% of the participants suffered from one or more chronic diseases, and 50.3% were diagnosed with a mental health disorder. The participants generally did not consider health problems as a central concern. The health needs that most affected the participants were related to food, safety, and social support. HP frequently felt unsafe, fearfully, and anxious.
Conclusion: Homelessness, unemployment, and social exclusion have significant negative impacts on the health and wellbeing of HP. Precarious work conditions and deficiencies in the welfare system contribute significantly to homelessness. These results highlight the need for systemic solutions that extend beyond short-term housing initiatives.
Homelessness has increased considerably in Western countries over the last decade (1). In Europe, at least 895,000 individuals live on the streets or in public spaces, spend nights in emergency shelters, or are accommodated in temporary facilities (2). Additionally, 21.6% of all Europeans (95.3 million people) are at risk of poverty or social exclusion (3). Spain ranks as is the third-worst among European countries (26%) on the At-Risk-Of-Poverty or Social Exclusion (AROPE) indicator (4). Specifically, 28,552 people in Spain are affected by homelessness, a 24.5% increase since 2012 (5). However, these data on housing exclusion only consider the most visible and severe cases, and do not include other situations related to housing insecurity (2).
The increase of homelessness can be attributed to world-wide social crises, armed conflicts, climate emergencies, and immigration, factors that are complex and interrelated (6). However, unaffordable housing is the central cause of all forms of homelessness. Between 2010 and 2022, housing and rental prices have increased in Spain, mirroring the trends throughout Europe (3). The transformation of housing into a speculative investment is a significant driver of this increase (7).
Housing is recognized as fundamental human right by international treaties and the Sustainable Development Goals (SDGs), and is considered pivotal for achieving physical, psychological, and social well-being (8). In response, the European Federation of National Organizations Working with the Homeless (FEANTSA) currently advocates for several legislative measures, such as regulation of the real estate market, prevention of forced evictions, and promoting public housing for vulnerable populations (2).
The consequences of homelessness are multi-dimensional, and social exclusion is one of the major effects. Housing deprivation extends beyond the purely physical dimension, because it can lead to the progressive loss of an individual’s affective, social, and personal niche (9). Homeless people (HP) have increased rates of mortality and morbidity (10, 11) that can be attributed to substantial health inequities (12, 13). For example, approximately 80% of HP struggle with mental health issues (5), about half of them have an elevated risk of suicide (14), and about half of them suffer from chronic diseases that affect the cardiovascular or respiratory systems (15). Chronic physical diseases in HP account for about two-thirds of the cases of premature mortality (16).
Homeless populations are highly susceptible to violence, and one study reported that three-quarters of them were victims of violence (5). Homeless women in particular face alarming rates of physical, psychological, and sexual assault (17, 18). The decreased accessibility of healthcare services and the difficult living conditions experienced by HP play pivotal roles in determining their health outcomes (19). The complexity of comorbidities and severe mental illnesses among HP (20), coupled with the lack of continuity and palliative care (21), pose significant challenges for healthcare systems.
Although the scientific community has quantified the number of HP, analyzed the economic causes of homelessness, and examined the prevalence of different health conditions among HP, there is comparatively little known about their self-perceived well-being, needs, and health.
As shown by previous studies (22) and advocated by Nussbaum and Sen (23), the theoretical approaches to studying homelessness often use the perspective of social justice. Sen (24) proposes the “capability approach” to address social justice in homelessness, since this approach recognizes that different individuals have different opportunities, resources, and freedoms to develop “doings and beings.” Nussbaum (25) emphasizes the role of capabilities in constructing a normative conception of social justice by specifying a specific set of capabilities that need the most protection. According to Nussbaum (26), the development of well-being is interconnected with the development of health. This understanding of the connection between well-being and health depends on an individual’s aspirations for a particular lifestyle, and on the individual’s preferences and priorities. Therefore, examination of the impact of homelessness on health requires study of the fundamental aspects that are valued by each person. The “capability empowerment” approach represents a rights-based evaluative approach that originated from studies of poverty and development.
However, Nussbaum’s capabilities theory has been criticized for its individualistic approach, because this approach may not adequately address the complexity of homelessness (27). Therefore, we combined the theoretical framework of the current study with a critical perspective that is based on the Social Determinants of Health (SDOH) approach (28) to better understand the relationship between homelessness and health (29). This approach explains the reasons for getting sick within a specific socioeconomic and political context and recognizes that this context generates an unequal power relationship that affects the number of opportunities. Specifically, the SDOH approach considers structural factors, such as employment, housing accessibility, political measures, healthcare systems, and gender to better understand the health of HP.
Finally, after exercising reflexivity and positionality, and following a defined theoretical approach, our research team faced the phenomenon of study as an active exercise of health advocacy (30, 31). This viewpoint considers the scientific community and professionals as groups that fight against social and health inequities. Therefore, we perceive homelessness as something that is avoidable, unfair, and repairable that requires a deep analysis from each individual’s point of view and includes consideration of the context (26, 32).
The aim of this study was to assess the health status and self-perceived health of individuals experiencing homelessness and to explore the effect of homelessness on health. We used an explanatory sequential mixed-methods approach (quan-QUAL) (33). Mixed-methods research allows exploration of divergent viewpoints on the same issue and provides contextual understandings that are shaped by real-life experiences and cultural influences (34). In particular, we used a cross-sectional and ethno-methodological design that included critical discourse analysis.
We aimed to reach all potentially HP in Palma, Spain (approximately 300 individuals according to 2019 data) (35). HP were defined as those living in the streets or other public areas, in an abandoned building, or in places that did not meet the minimum conditions for habitability. Notably, within the same week or month, a HP could live in the street, spend several nights in a municipal shelter, spend another week in the makeshift shelter of a friend, and then return to the streets. This approach considers homelessness as the continuous instability of an overnight location and classifies most participants in the “Roofless” category according to the ETHOS classification (36). Thus, if a person slept in an abandoned building or a makeshift shelter at the moment of recruitment, they were still considered as “Roofless” (although they would be in the “inadequate” or “insecure” conceptual category in the ETHOS classification). This classification is based on the perception of homelessness as a continuous (not a static) phenomenon.
Inclusion criteria were homelessness and age of at least 18 years. Exclusion criteria were staying overnight in a private or municipal shelter for more than 3 months (in contrast to housing instability), experiencing an acute mental health episode, or inability to answer the questionnaire.
We used an investigator-administered questionnaire that examined basic needs (an adaptation of Virginia Henderson’s approach to the specific needs of homeless individuals) (37), substance abuse (DAST-10, Drug Abuse Screening TEST), diet quality (IASE, Healthy Eating Index), depressive symptoms (PHQ-9, Patient Health Questionnaire), and perceived social support (SSQ-6, Social Support Questionnaire). Health data were obtained from the electronic medical records of the Health Service of the Balearic Islands. Data on the use of health care services and hospital admissions from 2019 to 2021 were retrieved from the PRISIB (the research platform on health information of the Balearic Islands). All participants were recruited in collaboration with different organizations that assist HP (Spanish Red Cross and Medicos del Mundo NGOs and public social service IMAS).
Surveys were conducted between December 2020 and September 2021 and lasted 20–40 min. Financial compensation was offered to all participants. Further details of the data collection procedures were provided elsewhere (38).
Continuous variables are presented as medians and interquartile ranges (IQR) because statistical normality could not be assumed based on the Kolmogorov–Smirnov test. Categorical variables are presented as absolute numbers and percentages. All statistical analyses were conducted using IBM SPSS Statistics version 26 (SPSS/IBM, Chicago, Illinois, United States).
Seventeen HP (5 women, 12 men) participated in the qualitative phase that were segmented according to gender, living conditions, age, and place of birth. The aim of this phase was to achieve the most significant heterogeneity participant discourse. We followed established criteria to set the sample size (39). These criteria are based on the “information power” of a sample, which depends on (a) the aim of the study, (b) sample specificity, (c) use of established theory, (d) quality of dialogue, and (e) analysis strategy.
Participants were selected using theoretical and purposive sampling according to their ability to provide a narrative that described their homelessness. Snowball sampling was used to select additional subjects. Key informants at social or homeless organizations recruited participants, and the main investigator (MAB, who has worked as a nurse in a shelter for HP), contributed to the recruitment process.
After initial analysis of data in the quantitative phase, semi-structured interviews were conducted (40). These data were collected using semi-structured interviews performed by MAB. To prevent the possible effects of power relationships during the interview, MAB did not reveal his background to the participants. All questions were inspired by the previously described theoretical frameworks, and covered perceived health status, access and use of health and social resources, the social environment, perceived social support, and perception of vulnerability and safety. The life history of each participant and its impact on homelessness was also analyzed.
Interviews were conducted between December 1, 2021 and January 1, 2023. We initially conducted three interviews, and then comprehensively analyzed the data collection and interview processes to refine the interview structure and the representativeness of participants’ profile. The discourse analysis was performed simultaneously to data collection. Finally, after 17 interviews, the data were saturated.
The interviews were conducted in a private room of the night shelter facilities of an NGO. All interviews lasted approximately 60–90 min and were audio-recorded, and then transcribed. We offered financial compensation to all participants. A more detailed description of the data collection procedures was provided elsewhere (38). The lead researcher (MAB) also recorded field notes during and after all interviews.
An abductive content and critical discourse analysis were carried out. Critical discourse analysis studies the ways in which social power abuse, dominance, and inequality are enacted, reproduced, and resisted, and focuses on communication by text and speech in the social and political contexts. This type of analysis seeks to understand, expose, and ultimately overcome social inequality (41).
The data analysis consisted of the following three steps: (I) familiarization with the data by repeated reading of the transcribed interviews; (ii) identification of codes and categories by inductive and deductive strategies; and (iii) analysis and interpretation according to the conceptual framework (SDOHs, and Nussbaum’s capabilities). Data were codified and analyzed independently by three researchers. Triangulation was then performed to compare codification, identify convergences and divergences, and reach a final consensus. Field notes were integrated into the interview transcripts and were also used in the analysis. A pseudonym for each participant was used to preserve the anonymity. The data analysis was systematized and optimized with ATLAS.ti software (version 9.0).
Techniques, such as saturation of the discourse, triangulation among researchers, data collection techniques, and theoretical frameworks were employed to ensure methodological rigor and validity (42). Reflexivity of the principal investigator was used throughout the research process by field diary (43).
The study design provided integration by use of an explanatory sequential design. Thus, the quantitative data were first gathered and analyzed (Phase 1), and these results were used to inform the collection of qualitative data (Phase 2). For integration at the methodological level, we used the following two approaches: (I) integration by “connecting” (connecting samples; some participants from Phase 1 continued to participate in Phase 2); and (ii) integration by “building” (results from the qualitative phase provided more insight and closed research gaps) (41, 44). Integration at the interpretation and reporting levels was provided by using the “weaving approach,” in which data from the quantitative and qualitative phases were reported side-by-side in narrative form (41, 44). This approach was used to identify consistencies and inconsistencies of the quantitative and qualitative data, and to determine when the qualitative data expanded the findings of the quantitative data, or vice versa. Finally, we used a joint display table to integrate and display all results (41).
We included 198 HP in the study (mean age: 47.8 ± 12.3 years; 79.3% males; Table 1), most of whom (76.5%) were born in Spain. A total of 29.8% of the participants had education below the level of secondary school, and the duration of homelessness was highly variable (median: 1 year, IQR: 4 years). More than half of the participants (81.9%) lived in public spaces or night shelters, and the others lived in abandoned buildings or similar places. The participants in the quantitative and qualitative phases had similar sociodemographic characteristics.
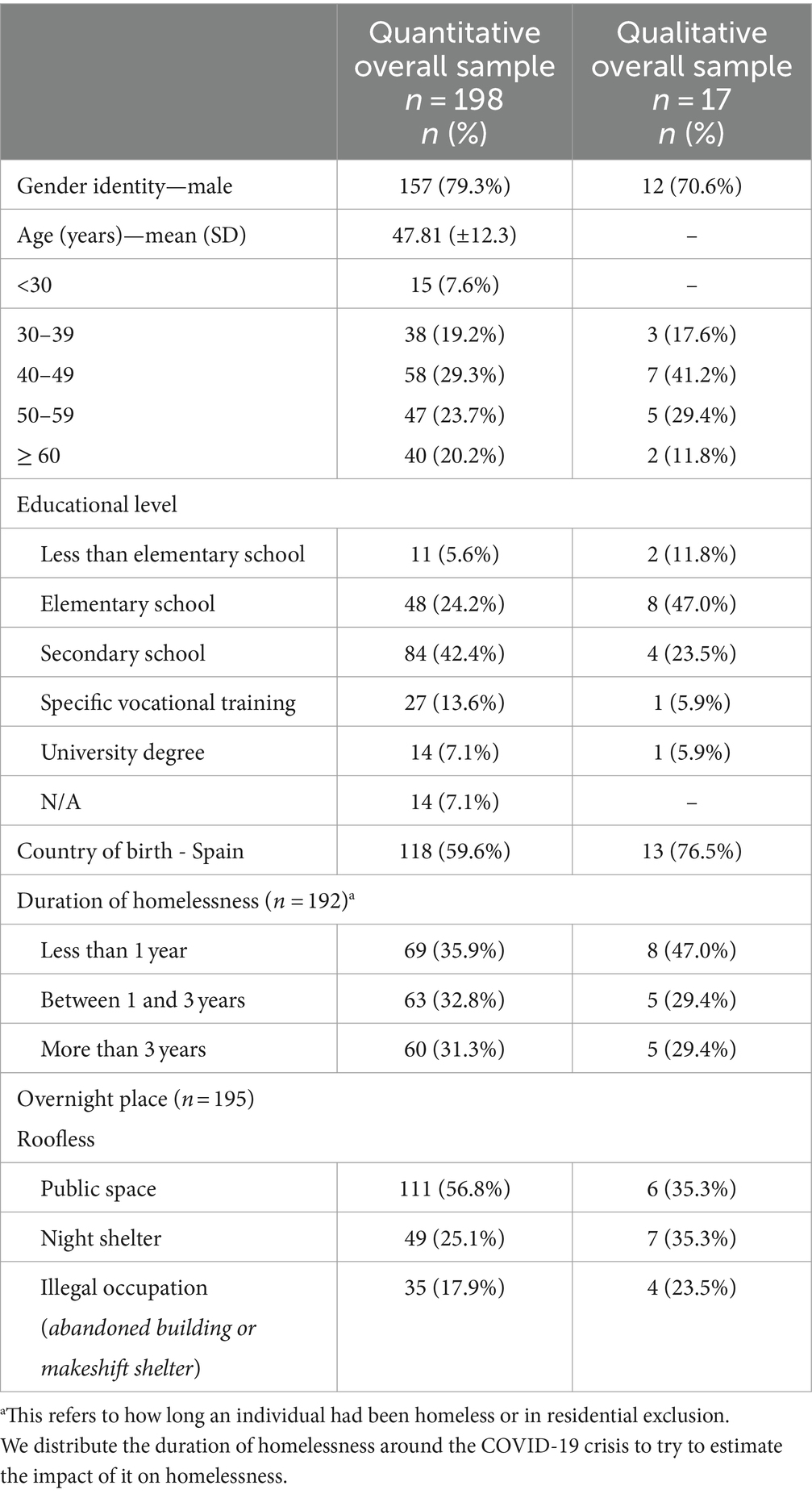
Table 1. Sociodemographic characteristics of the study population.
The 91.4% were unemployed and only 2 participants were legally employed (Table 2). The most important barriers to employment were health issues (27.3%), the COVID-19 crisis (25.7%), old age (12.6%), and undocumented immigrant status (12.1%). The last reported employment contract was an average of 5 years ago (before the onset of the COVID-19 pandemic).
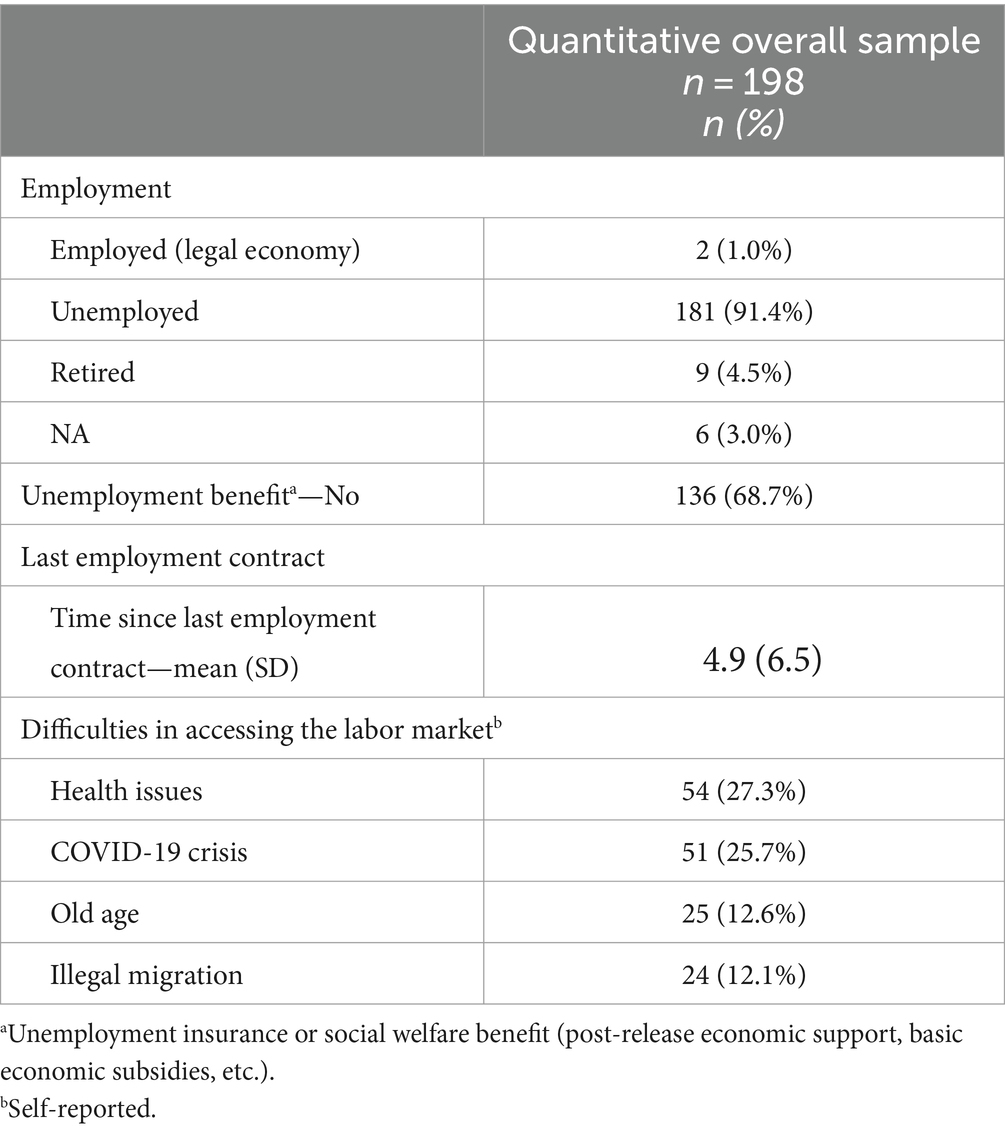
Table 2. Employment and access to the labor market.
Participants explained that health problems and the very physically demanding tasks typical of precarious jobs (e.g., construction or cleaning) prevented them from entering or continuing in legal employment. Furthermore, they reported job loss due to workplace accidents, aging, or chronic diseases.
“I work in construction, and when I was working, blood came out (rectal hemorrhage), and the doctor told me to not lift heavy weights. I left construction, but there was no other job. I didn’t know how to find anything else.” (Emmanuel, man, makeshift shelter)
Nearly 70% of the unemployed participants did not receive unemployment benefits from the Spanish public welfare system, and they explained the challenges encountered when seeking these benefits. They said that certain very strict requirements, such as the need to present a census certificate or have a legal administrative status, prevented access to these benefits. One participant mentioned the difficulties in getting social benefits due to his young age.
“Until you are 45 years old you have no rights to get any social benefit. (Antonio, man, abandoned building)
Even those who received unemployment benefits said that this financial support was insufficient for securing a permanent residence or purchasing food and other essential items, causing them to remain on the streets or in shelters.
On the other hand, the participants reported a heavy reliance on the underground economy as the sole source of income. These opportunities were limited to begging, scavenging for scrap materials (primarily men), engaging in cleaning tasks, and prostitution (primarily women).
“I worked so hard since I arrived in Spain, cleaning. Then, in a beach bar, I clean it, I do the shopping for them, or I decorate it for Christmas, and that’s how I earn money… Even prostitution” (Andrea, woman, abandoned building)
The lack of employment and the conditions at precarious jobs have serious emotional impacts on HP. Participants reported that unemployment, particularly over an extended period, had serious implications. They emphasized that employment provides financial stability, gives them social status and a sense of community, and these affect their identity and dignity.
“Well, I would also like to have a permanent job, or even if it is temporary, whatever … But having a job, that is what all normal people do” (Francisca, woman, abandoned building)
Approximately half of the participants (87/179, 48.9%) were diagnosed with one or more chronic diseases (Table 3), and liver diseases were the most prevalent (39/87, 44.8%) Other participants had high blood pressure (28/87, 32.2%), cardiovascular pathologies (14/87, 16.1%), COPD (11/87, 12.6%), asthma (10/87, 11.5%), and type 2 diabetes mellitus (10/87, 11.5%).
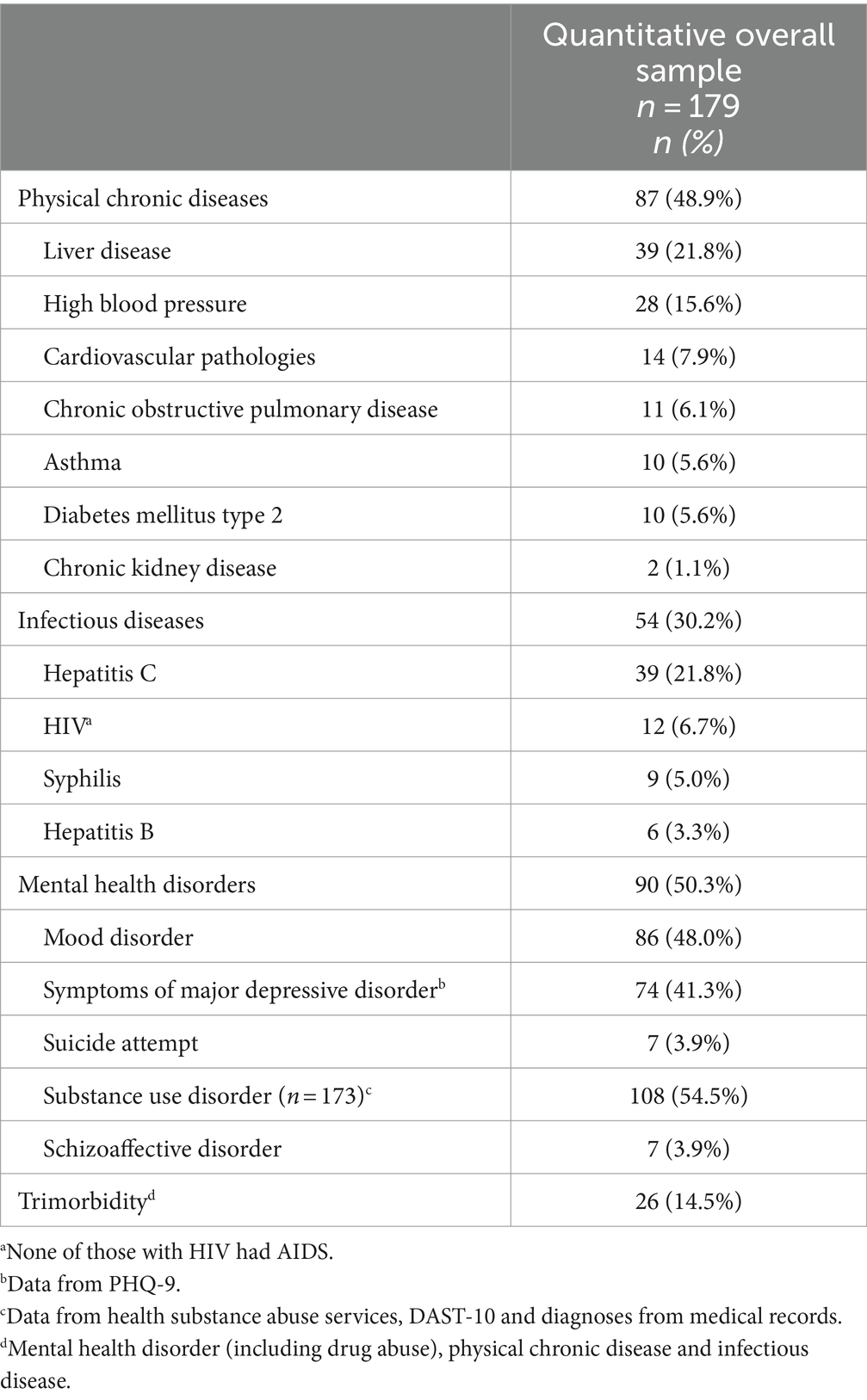
Table 3. Physical and mental health conditions.
A total of 30.2% of the participants (54/179) presented with a communicable disease, and 72.2% of these individuals (39/54) had hepatitis C, and 22.2% (12/54) had HIV, although none had AIDS.
More than half of the participants (90/179, 50.3%) were diagnosed with a mental health disorder. Among these 90 participants, mood disorders were the most prevalent (86, 95.6%), 7 participants (3.9%) had schizoaffective disorder, and 74 participants (41.3%) had symptoms of depression according to the PHQ-9. Overall, 108 of 173 participants (54.5%) had substance abuse disorders, although we did not identify the specific substances. Moreover, 26 of 179 participants (14.5%) suffered from trimorbidity (physical health, mental health, substance abuse) which included communicable diseases.
Although multiple physical and mental health disorders were common among the participants, and they refer it has an impact in their daily lives, they generally did not perceive themselves as having health problems. For them, health and well-being were transcended by other needs, and physical health and chronic pathologies had low priority. Instead, they said that management of social relationships, emotional health, and stress were central to achieving health and wellbeing.
“For me, being healthy is being well, being okay with people, with myself and my surroundings, not seeing myself excluded, meaning that people don’t see me and say, “Look, this man is in the street and … damn “It’s disgusting, if he comes, I’ll leave.” (Javier, man, public space)
“Tranquility is better than a doctor. I’m not afraid of getting ill. I’m already like “dead”, just as I’m right now, there’s no life. If I’m well organized, I don’t take pills. Because if I work, I will eat better, peace of mind…What does sugar mean? Sugar means nervousness and stress. This means sugar rises.” (Mohamed, man, makeshift shelter)
Nearly all the participants had a health card or a health insurance number (Figure 1), although those who never contacted the system for these documents or were undocumented immigrants did not. The participants reported that barriers to accessing the healthcare system were related to administrative procedures, such as making appointments, obtaining test results, and the general function of the healthcare system, and they sought help from NGOs or social services to overcome these barriers.
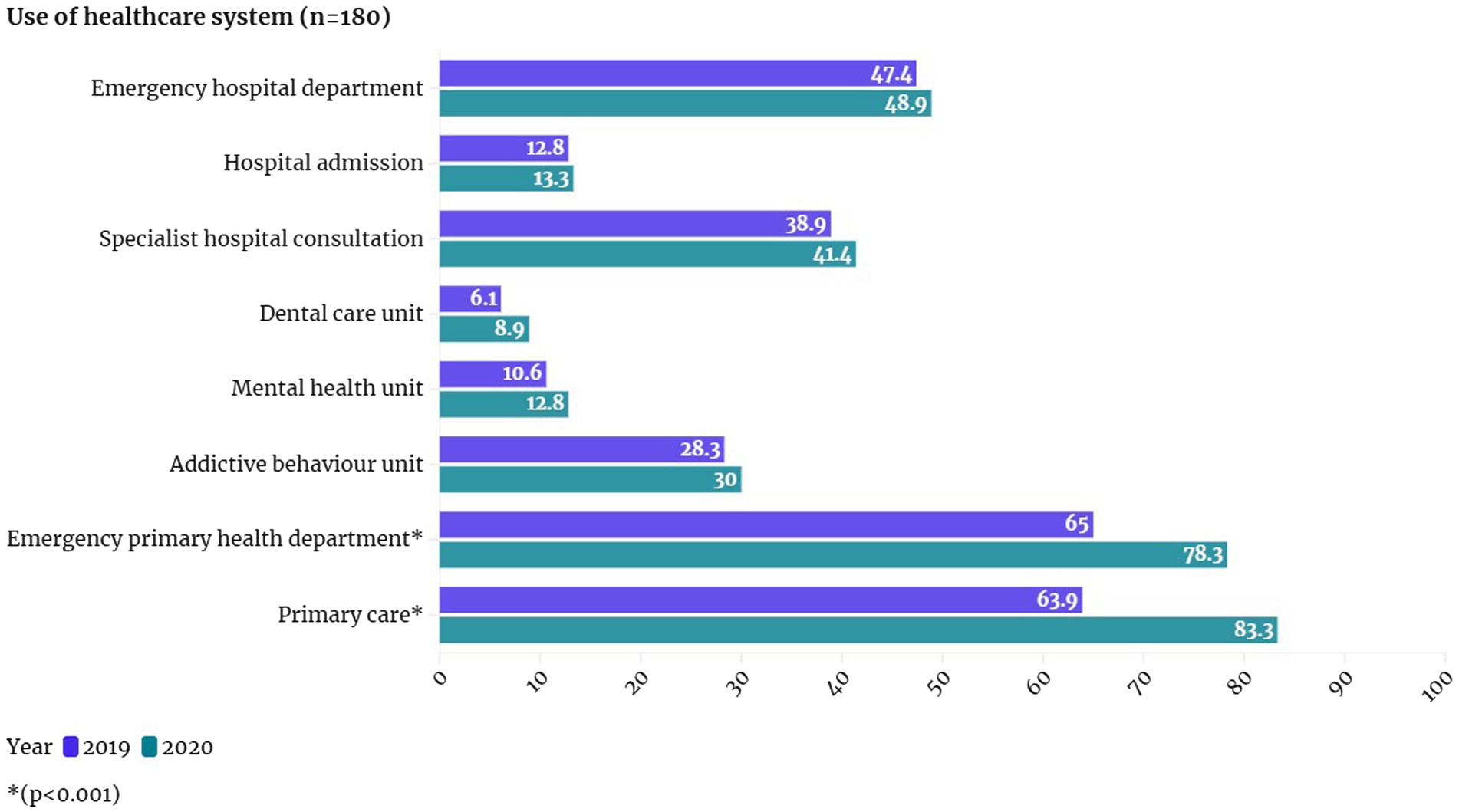
Figure 1. Use and access to the healthcare system.
“The first thing I do is go to the doctor, and if he doesn’t listen to me, I go to the social services, and at night, they have to accompany me to the hospital” (Javier, man, public space)
Primary care was the healthcare service visited by most participants, with utilization rates of 63.9% in 2019 and 83.3% in 2020. Moreover, the participants also frequently visited emergency departments at primary care centers, with rates of 65.0% in 2019 and 78.3% in 2020; this was followed by emergency departments (47.2% in 2019 and 48.9% in 2020) and specialist hospital consultation (38.9% in 2019 and 41.4% in 2020). Something to highlight is that most of them (97.4%) has a sanitary card or ID, and that more than half (60.3%) had a prescription of chronic medication.
The general opinion of the participants was gratitude toward the healthcare system and professionals. At the hospital, they felt comfortable and satisfied with the care provided, and believed they were treated with affection and respect. Participants mainly focused on their experiences during hospital admissions when were asked about this topic. One participant also emphasized that the care provided to him ended the moment he was discharged from the hospital.
“Do you know where they’ve been good? ‘You are an exceptional patient.’ Until the day they discharged me. What happens after being discharged, it’s not their problem. What matters to them is that you get out of there on your own feet”. (Jose, man, public space)
The most unsatisfied basic human needs were related to the availability of food, basic hygiene, toilets, and rest, and the avoidance of danger and social isolation (Table 4). The constant search for resources and shelter shaped the daily routine of most participants. This situation created emotional instability that prevented them from establishing a regular routine or achieving a long-term solution that would guarantee fulfillment of their basic needs.
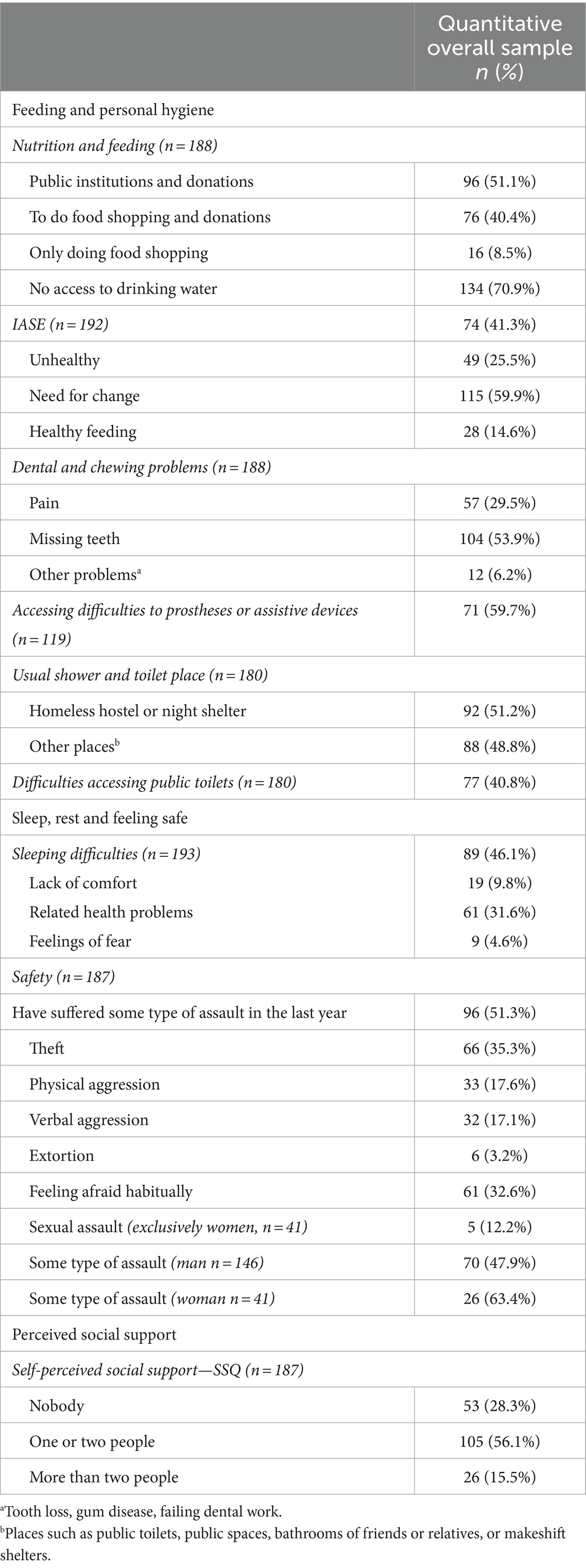
Table 4. Basic human needs affected by homelessness.
According to the IASE measurement of diet quality, most participants have a need to change their diets (59.9%) or have diets with low nutritional value (25.5%). In addition, 53.9% of participants had missing teeth, 29.5% reported dental pain, and 59.7% expressed difficulties accessing prostheses, glasses, or dental prostheses.
Half of the participants relied on formal or informal help from public institutions and citizens to get food, and 40.4% of them shopped for food but also relied on charity for access to food. Many participants (70.9%) reported having limited access to drinking water near their living places and at public overnight shelters.
About half of the participants reported using homeless emergency shelters or hostels as the usual places for showers, and the others reported using public toilets or makeshift shelters to shower using buckets of water or other handmade systems. A small number of participants used the bathrooms of friends or relatives for showers.
“In shelters you have your three meals a day, you have a shower, social workers give you your shampoo, your towel, they give you your sheets whenever you want, they give you everything man!” (Paco, man, night shelter)
Despite the risk that these needs would remain unmet, the participants used diverse strategies to meet their basic needs. Specifically, the use of homeless shelters and support from their social environment were perceived as essential.
Almost half of the participants had problems maintaining or falling asleep (Table 4). One-third of them reported this was caused by mood disorders or physical health problems, and the others reported this was related to physical discomfort (9.8%) or being afraid at night (4.6%). In addition, one third of them (32.6%) said they often felt afraid, 51.3% reported being victims of assault, 68.75% were victims of theft, 34.3% were victims of physical aggression, and 33.3% were victims of verbal aggression.
The consequences of the unmet basic human needs adversely impacted the participants’ lives, social relationships, and daily routines, and generated feelings of anxiety and a continuous state of stress.
“Being able to rest, be calm … Because now you cannot be calm there (abandoned building). Being homeless has affected me a lot (emphasis). A lot, because before, I had friends, we went to buy clothes … now what am I doing here? You cannot move much here. Here, I am surrounded by people you cannot trust much”. (Francisca, woman, abandoned building)
Moreover, homeless women suffered more assaults than homeless men (63.4% vs. 47.9%); 12.2% of homeless women experienced sexual assault; and 14.6% were diagnosed as victims of gender-based violence while in primary care. This problem is so serious that one woman who was previously in prison said that she preferred being in prison rather than on the streets.
“But it is tough to live on the street. It is the hardest thing that has happened to me in my life. I prefer jail than living on the street.” (Ana, woman, public space)
In contrast to feeding and hygiene, participants could not find coping strategies that addressed the need to feel safe and get adequate sleep through social services. The participants who previously or were currently using emergency or night shelters said they felt afraid and insecure while staying there. They also complained about theft and physical aggression.
“If I were to tell you what happened to me here (shelter) … Everything … €60 has been stolen from me, my wallet with my credit card, with my ID, with the medical card … Last night, they stole all my medication…” (Pedro, man, night shelter)
The participants had difficulty in maintaining their social environment (Table 4). According to the SSQ, 28.3% of the participants did not have anybody to trust or ask for help, and 56.1% could only rely on one or two people (typically social workers). For those who did have social support, other people provided essential help to cover their needs for food or hygiene. Moreover, even informal social relationships in the neighborhood from local mechanics, librarians, bar owners, waiters, or people who saw them daily, were crucial for maintaining a sense of well-being.
“There is a man who owns a garage, and one day I was not here, and he called me to see if I was okay, he was worried, and that gives me strength to keep going, you know?” (Javier, man, public space)
The participants explained that being homeless led them to lose relationships with friends, and even family. Also, being homeless made them lose trust in people, and made it difficult for them to form new relationships.
“The friends that I had … They all left. They did not want to talk to me if I lived on the street.” (Laura, woman, public space)
Additional verbatims about all categories supporting the results can be found at Supplementary Table S1.
Overall, the results from the quantitative and qualitative analyses were consistent and, in some instances the qualitative results expanded upon the qualitative results. For example, when the quantitative results indicated a relationship between access to the labor market and health, the qualitative results confirmed and expanded upon these findings. However, there were also some notable discrepancies, such as the high prevalence of morbidities in the quantitative analysis and a lack of concern about health issues in the qualitative analysis (Supplementary Table S2).
Our results suggest that structural determinants, particularly the socioeconomic context, were the major determinants of homelessness. Furthermore, homelessness limits the opportunities of HP to attain basic human needs and undermines their health and dignity. Specifically, our findings indicate close interconnections among working conditions, health, labor rights, and housing for individuals experiencing homelessness.
Our results showed that when someone cannot obtain and maintain housing, then the circumstances caused by homelessness lead to an emphasis on survival and fulfillment of basic human needs. These basic needs are focused on food, safety (avoiding dangers and aggression), and shelter for rest, as previously observed (1, 45). To cover these basic needs, HP are often forced to constantly move, and they adopt what could be called a Nomad-Paleolithic lifestyle.
This interpretation considers the challenges in classifying HP, because their overnight locations are constantly changing (46). The Nomad-Paleolithic lifestyle could increase the morbidity and mortality of HP (47), and also adversely affect their mental health (45). Moreover, the Nomad-Paleolithic lifestyle reduces and limits their capabilities, and also decreases the possibility of achieving a minimum level of individual human dignity (25).
The participants in our study show very similar demographic characteristics to other Spanish contexts (48). They also had various physical health problems, such as chronic and infectious diseases (49). In addition, half of them suffered from mood disorders. As previously suggested, elevated levels of anxiety can exacerbate mental and physical health disorders (50). Furthermore, we found that more than half of the participants suffered from episodes of violence and assault (theft, physical violence, verbal threats, and sexual abuse), in agreement with other studies (51). The homeless women in our study were most affected by violence and assault, same as in other studies (52).
Most of our participants visited emergency departments at hospitals or healthcare centers during the two-year study period. Other researchers found that HP tended to use these departments more frequently than the general population (12). The extensive use of these healthcare services by HP could be explained by their higher rates of morbidity and injuries, and their inadequate living conditions. Additionally, the COVID-19 crisis further increased the health risks of HP (53), and likely led to their increased need for healthcare and use of emergency departments during 2019 and 2020. Finally, although the healthcare system of Spain provides universal healthcare coverage, HP are not guaranteed continuous care after discharge from a hospital. Thus, to effectively address health inequities, the healthcare system needs to implement more holistic interventions that prioritize the social aspects of health (54, 55). This approach considers the health and well-being of HP, and our participants reported that emotional health and the social environment were important health-related priorities.
Housing affordability (56), poverty, and social exclusion all affect homelessness (3). Our study was performed in Spain, which adheres to a welfare state model (57), whose foundations are universal healthcare, free public education, protection from unemployment and dependency, and a public pension system (58). Despite these measures, Spain faces structural unemployment and a lack of housing, conditions exacerbated by social and economic crises, such as the COVID-19 pandemic (59). Moreover, Spain is the third-worst country among the EU-27 in terms of people renting at market prices, and on average more than 40% of household income is devoted to housing in Spain (4). This situation shows that although many policies in Spain emphasize the right to adequate housing, its current social welfare model lacks legislation that effectively addresses matters of housing and poverty.
The participants in our study reported that several barriers prevented them from accessing the labor market (long-term unemployment, age of 55 years or more, and lacking higher education), as previously shown (60) to guarantee steady housing, because low-paying jobs do not allow some people to escape poverty or homelessness (61). Other factors that may contribute to homelessness are price inflation, job insecurity, income inequalities, and a poor working environment (4), all of which were identified by our study participants. Moreover, the participants who received social welfare subsidies complained that these benefits were insufficient to guarantee housing, and those who reported receiving no subsidies said there were bureaucratic difficulties in applying for these benefits, as previously reported (62).
Furthermore, as stated by our participants, unemployment has a severe emotional impact because it causes a loss of self-esteem and defines their identity homeless, consistent with other studies (63). This reinforces the assumption that unemployment justifies homelessness (64).
Lastly, in our context, the main intervention for addressing homelessness is a system of shelters. Although shelters provide a place to sleep, eat food, and take showers, many participants said they tended to avoid them because they did not feel safe as shown in other studies (65). They reported preferring to sleep in the open, a behavior leads to maintenance of the Nomad-Paleolithic lifestyle (66).
Shelters are the first step of the Spanish public social services system for HP, which is based on the ladder model (67). This model assumes that once people have their basic needs covered (food, rest, and safety) and comply with certain behavioral norms or conditions, then they can achieve economic emancipation only by employment. However, shelters and its hostile environment does not work for some HP and could contribute to perpetuate homelessness (68). Interestingly, given the present system, some participants expressed preferences for being in prison or a hospital, rather than a shelter. By contrast, “Housing First,” a holistic, highly effective, and efficient intervention (69) recently began in Spain (70). This intervention recognizes the importance of providing stable and long-term solutions to people experiencing homelessness, recognizes basic human rights and needs, and prioritizes direct access to permanent housing without preconditions.
Finally, we must point out that the results unexpectedly led us to question the design of our data collection. During the qualitative phase, we observed that the participants considered work and labor conditions, along with survival needs (shelter, safety, and food), to have greater importance and relevance for their health. Although we included these in the quantitative phase, we believe these factors should be prioritized in a qualitative analysis.
Although we tried to reach all of the potentially eligible HP in Palma, our sample selection may have been biased because the HP who participated had some form of contact with social services. Consequently, the HP who did not receive assistance from social services were not represented. A second limitation is that the results should be considered valid only within the specific time frame and environment in which the study was conducted.
Policies that aim to eradicate homelessness should consider employment, housing affordability, and the social welfare system, and should also consider the SDOH. Therefore, it is likely that policies which focus on individual aspects, such as the ladder model, will perpetuate or even increase homelessness.
Our study also highlights the relationship between access to the labor market and physical health, especially for those whose income depends on manual labor. These individuals face exclusion when health issues prevent them from working. Therefore, it is essential to provide stronger protections against occupational hazards associated with manual labor and to implement policies that offer alternative work opportunities for these individuals.
The healthcare system should implement an interdisciplinary model that uses a holistic approach to address homelessness. Also, the healthcare system and public and private social organizations should implement health advocacy programs by considering the SDOH and creating a dynamic and opportunities for professionals to implement these programs, with a final goal of contributing to the well-being of everyone.
Our results could serve as a foundation for further analysis of the relationship between housing exclusion, unemployment, and poor health. Longitudinal studies are also needed to examine the consequences of persistent homelessness. In addition, there is a need to evaluate the relationship of gender and homelessness and examine the topics of gender violence and prostitution in this population.
The health and wellbeing of HP are seriously affected by unemployment and social exclusion. This underscores the relevance of precarious working conditions and the failure of the current welfare system, which may trigger a fall into homelessness or perpetuate homelessness. We found that the main concerns of HP were feeling unsafe and social isolation. We understand that most HP lead a Nomad-Paleolithic lifestyle, and this adversely affects their health and increases the risk of premature death. HP are in vulnerable situations and may be denied basic human needs and rights, and many of them cannot attain adequate health-related needs beyond those required for basic survival.
The current system of shelters and other social interventions are insufficient for addressing homelessness because they use paternalistic and individualistic approaches. Moreover, HP perceive shelters as unsafe options that hinder their free will, autonomy, and privacy. Although “Housing First” may provide a better short-term solution, it does not address all of the underlying structural determinants that generate and entrench homelessness.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Research Ethics Committee of the Balearic Islands (CEI-IB). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MB: Conceptualization, Data curation, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing. LC-M: Conceptualization, Formal analysis, Software, Writing – original draft, Writing – review & editing. MB-V: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. CM-M: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. AC-P: Data curation, Writing – original draft, Writing – review & editing. AY: Conceptualization, Formal analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Office for Cooperation, Development, and Solidarity of the University of the Balearic Islands and the Government of the Balearic Islands (award no. OCDS-CUD2020/05), as well as by the Royal College of Nurses of the Balearic Islands (Ref. 2020-0576).
We wish to acknowledge the collaboration of the participants and the organizations that work alongside them (Medicos del Mundo and Cruz Roja).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1444888/full#supplementary-material
1. De Sousa, T., Andrichik, A., Cuellar, M., and Marson, J. (2022). The 2022 annual homelessness assessment report (AHAR) to congress. The U.S. Department of Housing and Urban Development. Available at: https://www.huduser.gov/portal/sites/default/files/pdf/2022-ahar-part-1.pdf (Accessed June 25, 2023).
2. Horvat, N., and Coupechoux, S. (2023). Eighth overview of housing exclusion in Europe. FEANTSA and The Abbé Pierre Foundation. Available at: https://www.feantsa.org/public/user/Resources/reports/2023/OVERVIEW/Rapport_EN.pdf (Accessed May 5, 2023).
3. Eurostat (2023). Living conditions in Europe - housing. Available at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Living_conditions_in_Europe_-_housing (Accessed April 26, 2023).
4. Canals Botas, L., Llano Ortiz, J. C., Sanz, A. A., and Urbano Molina, C. (2023). El estado de la pobreza. Seguimiento de los indicadores de la Agenda UE 2023. 13th report. Available at: https://www.eapn.es/estadodepobreza/ARCHIVO/documentos/informe-AROPE-2023-el-estado-de-la-pobreza.pdf (Accessed August 25, 2023).
5. Instituto Nacional de Estadística (INE) (2022). Encuesta a las personas sin hogar. Available at: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=estadistica_C&cid=1254736176925&menu=ultiDatos&idp=1254735976608 (Accessed June 12, 2023).
6. Chancel, L., Piketty, T., Saez, E., and Zucman, G. (2022). World inequality report 2022. The world inequality lab at the Paris School of Economics. Available at: https://wir2022.wid.world/www-site/uploads/2021/12/WorldInequalityReport2022_Full_Report.pdf (Accessed April 16, 2023).
7. Gao, Z, Sockin, M, and Xiong, W. Economic consequences of housing speculation. Rev Financ Stud. (2020) 33:5248–87. doi: 10.1093/rfs/hhaa030
8. Harland, JM, Adams, EA, Boobis, S, Cheetham, M, Wiseman, A, and Ramsay, SE. Understanding the life experiences of people with multiple complex needs: peer research in a health needs assessment. Eur J Pub Health. (2022) 32:176–90. doi: 10.1093/eurpub/ckab142
9. Mejia-Lancheros, C, Lachaud, J, Woodhall-Melnik, J, O’Campo, P, Hwang, SW, and Stergiopoulos, V. Longitudinal interrelationships of mental health discrimination and stigma with housing and well-being outcomes in adults with mental illness and recent experience of homelessness. Soc Sci Med. (2020) 268:113463. doi: 10.1016/j.socscimed.2020.113463
10. Singh, A, Daniel, L, Baker, E, and Bentley, R. Housing disadvantage and poor mental health: a systematic review. Am J Prev Med. (2019) 57:262–72. doi: 10.1016/j.amepre.2019.03.018
11. Aldridge, RW, Story, A, Hwang, SW, and Nordentoft, M. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. Lancet Public Health. (2018) 391:241–50. doi: 10.1016/S0140-6736(17)31869-X
12. Ontario Agency for Health Protection and Promotion (Public Health Ontario, (PHC))Berenbaum, E ., (2019). Evidence brief: homelessness and health outcomes: what are the associations? Queen’s printer for Ontario. Available at: https://www.publichealthontario.ca/-/media/documents/E/2019/eb-homelessness-health.pdf (Accessed April 16, 2023).
13. Omerov, P, Craftman, AG, Mattsson, E, and Klarare, A. Homeless persons’ experiences of health- and social care: a systematic integrative review. Health Soc Care Commun. (2020) 28:1–11. doi: 10.1111/hsc.12857
14. Ayano, G, Tsegay, L, Abraha, M, and Yohannes, K. Suicidal ideation and attempt among homeless people: a systematic review and meta-analysis. Psychiatry Q. (2019) 90:829–42. doi: 10.1007/s11126-019-09667-8
15. Zhang, L, Norena, M, Gadermann, A, Hubley, A, and Russell, L. Concurrent disorder and health care utilization among homeless and vulnerability housed persons in Canada. J Dual Diagn. (2018) 14:21–31. doi: 10.1080/15504263.2017.1392055
16. Ngo, AN, and Turbow, DJ. Principal component analysis of morbidity and mortality among the United States homeless population: a systematic review and Meta-analysis. Int Arch Public Health Community. (2019) 3:025. doi: 10.23937/2643-4512/1710025
17. Bhattacharya, P, and Ravi Priya, K. Stakeholders facilitating hope and empowerment amidst social suffering: a qualitative documentary analysis exploring lives of homeless women with mental illness. Int J Soc Psychiatry. (2021) 68:908–18. doi: 10.1177/00207640211011186
18. Calvo, F, Watts, B, Panadero, S, and Giralt, C. The prevalence and nature of violence against women experiencing homelessness: a quantitative study. Violence Against Women. (2021) 28:1464–82. doi: 10.1177/10778012211022780
19. Moschion, J, and van Ours, JC. Do transitions in and out of homelessness relate to mental health episodes? A longitudinal analysis in an extremely disadvantaged population. Soc Sci Med. (2021) 279:113667. doi: 10.1016/j.socscimed.2020.113667
20. Choi, KR, Castillo, EG, Seamans, MJ, Grotts, JH, Rab, S, and Kalafonos, I. Mental health conservatorship among homeless people with serious mental illness. Psychiatr Serv. (2022) 73:613–9. doi: 10.1176/appi.ps.202100254
21. Reid, N, Mason, J, and Kuryak, P. Evaluating the impact of a critical time intervention adaptation on health care utilization among homeless adults with mental health needs in a large Urban Center. Can J Psychiatry. (2021) 67:57–66. doi: 10.1177/0706743721996114
22. Loosemore, M, Bridgeman, J, Russell, H, and Zaid Alkilani, S. Preventing youth homelessness through social procurement in construction: a capability empowerment approach. Sustain For. (2021) 13:3127. doi: 10.3390/su13063127
23. Nussbaum, M, and Sen, A. The quality of life. 1st ed. New York, United States: Oxford University Press (1993).
24. Sen, A . The idea of justice. 1st ed. Cambridge: The Belknap Press of Harvard University Press (2009).
25. Nussbaum, MC . Capabilities as fundamental entitlements: Sen and social justice. Fem Econ. (2003) 9:33–59. doi: 10.1080/1354570022000077926
26. Nussbaum, MC . Creating capabilities: The human development approach. 1st ed. Massachusetts: The Belknap Press (2013).
27. Prendergast, R . The concept of freedom and its relation to economic development—a critical appreciation of the work of Amartya Sen. Camb J Econ. (2005) 29:1145–70. doi: 10.1093/cje/bei081
28. Stafford, A, and Wood, L. Tackling health disparities for people who are homeless? Start with social determinants. Int J Environ Res Public Health. (2017) 14:1535. doi: 10.3390/ijerph14121535
29. Hamiduzzaman, M, De-Bellis, A, Abigail, W, and Fletcher, A. Critical social framework on the determinants of primary healthcare access and utilisation. Family medicine and community. Health. (2021) 9:e001031. doi: 10.1136/fmch-2021-001031
30. Bonal Ruiz, R . Health advocacy, the forgotten part of health promotion in family medicine. Rev. Cub. Med. Gen. Integ. (2019) 35:1–19.
31. Venkatapuram, S . Health justice: an argument from the capabilities approach. 2nd ed. Oxford: Wiley (2011).
32. Restrepo-Ochoa, DA . Health and the good life: contributions by Amartya Sen’s capability approach to ethical reasoning in public health. Cad Saude Publica. (2013) 29:2371–82. doi: 10.1590/0102-311x00069913
33. Jogulu, U, and Pansiri, J. Mixed methods: a research design for management doctoral dissertations. Manag Res Rev. (2011) 34:687–701. doi: 10.1108/01409171111136211
34. Ivankova, NW, and Wingo, N. Appliying mixed methods in action research: methodological potentials and advantages. Am Behav Sci. (2018) 62:978–97. doi: 10.1177/0002764218772673
35. Lluch Cerda, ME, and Salvà Serra, H. Les xifres en el III Recompte de persones sense sostre de Mallorca de persones en situació de carrer, 2019. Alimara. (2019) 60:7–24.
36. Amore, K, Baker, M, and Hoeden-Chapman, P. The ETHOS definition and classification of homelessness: an analysis. Eur. J. Homeless. (2011) 5:19–37.
37. Martin-Baena, D, Montero-Pinar, I, and Fuertes-Lanzuela, MI. Factors associated to health needs from homeless perspective in Spain. Int. J. Stud. Nurs. (2016) 1:61–9. doi: 10.20849/ijsn.v1i1.102
38. Bedmar, MA, Bennasar-Veny, M, Artigas-Lelong, B, Salvà-Mut, F, Pou, J, Capitán-Moyano, L, et al. Health and access to healthcare in homeless people. Medicine. (2022) 101:e28816. doi: 10.1097/MD.0000000000028816
39. Malterud, K, Dirk Siersma, V, and Dorrit Guassora, A. Sample size in qualitative interview studies: guided by information power. Qual Health Res. (2016) 26:1753–60. doi: 10.1177/1049732315617444
40. Ivankova, NW, Creswell, JW, and Stick, SL. Using mixed-methods sequential explanatory design: from theory to practice. Field Methods. (2006) 18:3–20. doi: 10.1177/1525822X05282260
41. Othman, S, Steen, M, and Fleet, J-A. A sequential explanatory mixed methods study design: an example of how to integrate data in a midwifery research project. J Nurs Educ Pract. (2021) 11:75–89. doi: 10.5430/jnep.v11n2p75
42. Renjith, V, Yesodharan, R, Noronha, JA, Ladd, E, and George, A. Qualitative methods in health care research. Int. J Prev Med. (2021) 12:20. doi: 10.4103/ijpvm.IJPVM_321_19
43. Green, J, and Thorogood, N. Qualitative methods for health research. 4th ed. London: Sage Publications (2018).
44. Fetters, MD, Curry, LA, and Creswell, JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. (2013) 48:2134–56. doi: 10.1111/1475-6773.12117
45. Oliveira, DM, Expedito, AC, Aleixo, MT, Carneiro, NS, Jesus, MCP, and Merighi, MAB. Needs, expectations and care production of people in street situation. Rev Bras Enferm. (2018) 71:2689–97. doi: 10.1590/0034-7167-2017-0612
46. Elder, NC, and Tubb, MR. Diabetes in homeless persons: barriers and enablers to health as perceived by patients, medical, and social service providers. Soc Work Public Health. (2014) 29:220–31. doi: 10.1080/19371918.2013.776391
47. Song, J, Gray, C, and Davies, A. Creating an e-cohort of individuals with lived experience of homelessness and subsequent mortality in Wales. UK J. Public Health. (2022) 44:805–9. doi: 10.1093/pubmed/fdab180
48. Zerbitzuak, G . II Estrategia Vasca Contra la Exclusión Residencial Grave 2024 - 2028 In: Gobierno de Euskadi (2024) Available at: https://www.euskadi.eus/contenidos/noticia/xiileg_planes_departamentales/es_def/Estrategia-exclusion-residencial.pdf
49. Bensken, WP, Krieger, NI, Berg, KA, Einstadter, D, Dalton, JE, and Perzynski, A. Health status and chronic disease burden of the homeless population: an analysis of two decades of multi-institutional electronic medical records. J. Health Care Poor Unders. (2021) 32:1619–34. doi: 10.1353/hpu.2021.0153
50. Gutwinski, S, Schreiter, S, Deutscher, K, and Fazel, S. The prevalence of mental disorders among homeless people in hight-income countries: an updated systematic review and metaregressión analysis. PLoS Med. (2021) 18:e1003750. doi: 10.1371/journal.pmed.1003750
51. Vázquez, JJ, Panadero, S, and Pascual, I. The particulary vulnerable situation of women living homeless in Madrid (Spain). Span J Psychol. (2019) 22:1–9. doi: 10.1017/sjp.2019.58
52. Mayock, P, and Bretherton, J. Women’s homelessness in Europe. 1st ed. London, United Kingdom: Palgrave Macmillan (2016).
53. Mosites, E, Harrison, B, Montgomery, MP, Meehan, AA, Leopold, J, Barranco, L, et al. Public health lessons learned in responding to COVID-19 among people experiencing homelessness in the United States. Public Health Rep. (2022) 137:625–9. doi: 10.1177/00333549221083643
54. Hirmas, AM, Poffald, AL, Jasmen Sepulveda, AM, Aguilera Sanhueza, X, and Delgado Becerra, I. Barreras y facilitadores de acceso a la atención de salud: una revisión sistemática cualitativa. Rev Panam Salud Publica. (2013) 33:223–9. doi: 10.1590/S1020-49892013000300009
55. MacDonald, S-A, and Cote, P-B. Navigating and negotiating health and social Services in the Context of homelessness: resistance and resilience. Int. J. Homeless. (2021) 1–14:1–14. doi: 10.5206/ijoh.2022.1.13647
56. Frayne, C., and Szczypinska, A., (2022). Housing market developments in the euro area: focus on housing affordability (171), European Commission. Available at: https://economy-finance.ec.europa.eu/system/files/2022-09/dp171_en.pdf (Accessed April 30, 2023).
57. Béland, D, Leibfried, S, Morgan, KJ, Obinger, H, and Pierson, C. The Oxford handbook of the welfare state. 2nd ed. London: Oxford University Press. (2021).
58. Calero, J . El estado del bienestar español: valoración y perspectivas de futuro. Araucaria. (2021) 23:457–78. doi: 10.12795/araucaria.2021.i47.20
59. Foessa, F . (2019). Exclusión y desarrollo social en España. Eighth report. Cáritas Española Editores. Available at: https://www.foessa.es/main-files/uploads/sites/16/2019/06/Informe-FOESSA-2019_web-completo.pdf (Accessed May 11, 2023).
60. Aguilar Gonzálvez, MC . Long-term unemployment, vulnerable groups and the reformulation of active employment policies. Lan Harremanak. (2021) 46:114–43. doi: 10.1387/lan-harremanak.23178
61. Shier, ML, Jones, ME, and Graham, JR. Employment difficulties experienced by employed homeless people: labor market factors that contribute to and maintain homelessness. J Poverty. (2012) 16:27–47. doi: 10.1080/10875549.2012.640522
62. Calzada Gutiérrez, I., Gómez Garrido, M., Gutiérrez Sastre, M., and Hernández Cordero, A. L. (2021). Monitor de Impacto de la Covid-19 sobre los Servicios Sociales. Instituto Nacional de Administración Pública. Available at: https://www.ucm.es/monitorss/file/informe-monitor-de-impacto-septiembre/?ver (Accessed April 4, 2023).
63. Marshall, CA, Boland, L, Westover, LA, Wickett, S, Roy, L, Mace, J, et al. Occupational experiences of homelessness: a systematic review and meta-aggregation. Scand J Occup Ther. (2020) 27:394–407. doi: 10.1080/11038128.2019.1689292
64. Annand, PJ, Platt, L, Rathod, SD, Hosseini, P, and Guise, A. “Progression capitals”: how homeless health peer advocacy impacts peer advocates. Soc Sci Med. (2022) 298:114770. doi: 10.1016/j.socscimed.2022.114770
65. Kerman, N, Kidd, SA, Voronov, J, Marshall, CA, O’Shaughnessy, B, Abramovich, A, et al. Victimization, safety, and overdose in homeless shelters: a systematic review and narrative synthesis. Health Place. (2023) 83:103092. doi: 10.1016/j.healthplace.2023.103092
66. Paudyal, V, MacLure, K, Buchanan, C, Wilson, L, Macleod, J, and Stewart, D. ‘When you are homeless, you are not thinking about your medication, but your food, shelter or heat for the night’: behavioural determinants of homeless patients’ adherence to prescribed medicines. Public Health. (2017) 148:1–8. doi: 10.1016/j.puhe.2017.03.002
67. Sahlin, I . The staircase of transition. Innovation. (2005) 18:115–36. doi: 10.1080/13511610500096400
68. Mackie, P, Johnsen, S, and Wood, J. Ending street homelessness: what works and why we Don’t do it. Eur. J. Homeless. (2019) 13:85–96.
69. Onapa, H, Sharpley, CF, Bitsika, V, McMillan, ME, MacLure, K, Smith, L, et al. The physical and mental health effects of housing homeless people: a systematic review. Health Soc Care Community. (2022) 30:448–68. doi: 10.1111/hsc.13486
70. Panadero Herrero, S., Martín Fernández, J., and Martínez Cantos, J. (2021). Evaluación de la metodología Housing First en España. In European anti poverty network. Available at: https://solucionesalsinhogarismo.org/wp-content/uploads/2021/10/Housing_first_Informe_completo.pdf (Accessed July 20, 2023).
Keywords: homelessness, social justice, employment, social exclusion, health inequities, social determinants of health
Citation: Bedmar MA, Capitán-Moyano L, Bennasar-Veny M, Moreno-Mulet C, Carrero-Planells A and Yáñez AM (2024) Health status and self-perception of health among homeless people in Spain: a mixed-methods study. Front. Public Health. 12:1444888. doi: 10.3389/fpubh.2024.1444888
Edited by:
Evasio Pasini, University of Brescia, ItalyReviewed by:
Giovanni Corsetti, University of Brescia, ItalyCopyright © 2024 Bedmar, Capitán-Moyano, Bennasar-Veny, Moreno-Mulet, Carrero-Planells and Yáñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Capitán-Moyano, bGF1cmEuY2FwaXRhbkB1aWIuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.