 Sharifa AlBlooshi
Sharifa AlBlooshi Maryam AlFalasi1
Maryam AlFalasi1 Zainab Taha
Zainab Taha Alia Khalid
Alia Khalid
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 13 February 2023
Sec. Public Health and Nutrition
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1123894
Introduction: COVID-19 is a virus that has spread rapidly and brought economic and social crises all around the world. The current study aimed to investigate the impact of COVID-19 quarantine on dietary habits, physical activity, food purchasing, smoking, and sleeping patterns in the United Arab Emirates.
Methods: A cross-sectional study was conducted using an online questionnaire between November 1st, 2020 and the end of January 2021. Citizens and residents of the UAE aged ≥ 18 years old were asked to complete an anonymous electronic questionnaire created via Google Forms and distributed on various platforms, such as WhatsApp, Twitter, and email. A total of 1682 subjects participated in the study.
Results: The results included that during the COVID-19 lockdown, more participants (44.4%) reported an increase in weight. This gain seems to be linked to increased food consumption [(Adjusted Odd Ratio) AOR = 1.68, 95% (Confidence Interval) CI = 1.12, 2.54, p = 0.022], decreased physical activity (AOR = 2.25, 95% CI = 1.58, 3.21, p < 0.001), and increased smoking (AOR = 1.90, 95% CI = 1.04, 3.50, p = 0.038). The groups that were most likely to gain weight included those who consumed more cereals (AOR = 1.67, 95% CI = 1.08, 2.57, p = 0.011), had an increased desire for sweets (AOR = 2.19, 95% CI = 1.50, 3.19, p < 0.001), and an increased desire for food (hunger) (AOR = 2.19, 95% CI = 1.53, 3.14, p < 0.001). In contrast, those who exercised more were more likely to lose weight (AOR = 0.61, 95% CI = 0.44, 0.86, p < 0.001) as well as those who slept over 9 h a day (AOR = 1.90, 95% CI = 0.45, 0.88, p = 0.006).
Discussion: Overall, it is essential to promote healthy habits and methods of healthy diet maintenance during stressful and unusual times when people might find it difficult to put effort into their health.
COVID-19 is an infectious disease caused by a newly discovered strain of coronavirus; a type of virus known to cause respiratory infections in humans. This new strain was unknown before December 2019, when an outbreak of pneumonia of unknown cause emerged in Wuhan, China (1). On March 11th, 2020, the World Health Organization (WHO) (1) declared that COVID-19 is a worldwide pandemic as the disease had spread enormously worldwide.
To combat COVID-19, many countries have applied preventive measures such as disinfection procedures and partial or complete lockdowns to slow the spread of the virus. For example, the United Arab Emirates (UAE) health authorities implemented preventative measures to protect public health in line with the WHO rules and regulations. On March 1st, 2020, the UAE authorities applied strict infection control and partial lockdown for more than 6 months, forcing many people to stay home (study and work from home). Nevertheless, such actions may cause a sudden and drastic change in the population's lifestyle. It has been reported that staying at home for a long time may lead to a change in dietary habits, physical activity, and sleep patterns, as well as psychological impact (2).
The economic impact of COVID-19 on diet quality and food security is also a concern. Healthy and nutrient-rich foods have become increasingly unaffordable and inaccessible, especially to people of lower socioeconomic status and informal workers (3).
The alteration of some life aspects and the new routine of people's daily life makes researchers want to study people during this critical period. For example, staying at home while news spreads about the COVID-19 pandemic can generate unpleasant emotions such as boredom, anxiety, and stress. These emotions are linked to increased food intake, especially “comfort” food known to be high in sugar and fat (4).
Such patterns have already been observed in several populations. Studies found that following the lockdown, eating habits and physical activity were negatively impacted (5–15). People reported an increase in main meals, frequent snacking, and experiencing a lack of motivation and control regarding food (5, 6). Additionally, they also showed reduced levels of physical activity and increased sedentary behavior. This suggests that many individuals cannot maintain appropriate levels of physical activity during quarantine (6–9). Likewise, studies done in the UAE found similar results (11–13). It is essential to determine the extent of such patterns in the UAE to address them and prevent the deterioration of the population's health.
As previously stated, the emergence of the COVID-19 pandemic has impacted almost every facet of life, including people's access to food and goods (16). As a result, many individuals have limited their outings, opting to shop for food online (17). During the height of the pandemic, many restaurants around the world were shuttered. However, delivery services were still available, which led to an increase in the usage of food delivery applications. Many individuals chose to have their groceries delivered to their homes to avoid crowds (18–22). This was especially true for those of higher income, higher levels of education, and those who find food-related online channels easier to use (16, 23). Similar patterns have been examined in the Middle East, including the UAE (24–31).
However, some populations appear to have some concerns regarding online food shopping. A study done in Brazil found that the preparation method was the primary worry among those who wouldn't rely on food delivery (32). Other studies also found that many responders were concerned about being unable to check the freshness and quality of the product when purchasing groceries online (26, 33). In addition, it was determined from a study conducted in Portland, United States, that lower-income consumers are less likely to employ internet delivery services (16). Furthermore, consumers stated that the complexity of using online tools for purchasing food goods alongside technological issues decreases their proclivity to use or re-use these technologies (23).
Another health aspect that has been influenced by the COVID-19 lockdown is smoking. The self-isolation induced by the COVID-19 pandemic seems to have increased the consumption of cigarettes per day (34). A study conducted in the UAE reported a rise in smoking in 21% of its 2060 respondents (13). Similar results have been determined in other studies around the world. This increase may be tied to the heightened stress levels during the COVID-19 pandemic (13, 35–38). However, findings included conflicting results where large percentages of participants did not change their smoking habits, reduce them, or even quit smoking entirely (35–38). A study in Italy attributed the reduction in smoking among its participants to their fear of the COVID-19 mortality risk (35).
Additionally, studies on the COVID-19 pandemic show that many people have been experiencing sleep difficulties that did not exist before the pandemic (39–43). The studies' populations commonly show a reduction in night-time sleeping, an increase in day-time napping, and a shift to a later bedtime (39, 42, 43). In addition, some people have slept more hours overall, but the quality of their sleep has declined (34, 37). For example, in a study done in the UAE, decreased sleep was reported among 20.8% of the 2,060 responders (13). Research also indicates that younger people and women were most likely to report sleep distress that may have arisen due to psychological distress during the COVID-19 pandemic (13, 43–45).
The novel coronavirus (COVID-19) pandemic has brought extraordinary challenges in various aspects of life. As a result, the United Arab Emirates has imposed stringent rules, including a lockdown that extended a nationwide daily curfew. Since the UAE is a multinational country, our results would be of great importance to health authorities when revising their health policies in pointing out the consequences on the local Emirati people. Therefore, it is important to investigate the consequences of the COVID-19 pandemic and quarantine on the health of the UAE population to create targeted interventions to improve people's lifestyles following the pandemic and to prevent similar outcomes in the case of emergencies. This is especially needed in the UAE because reports of unhealthy lifestyles were already high before the COVID-19 pandemic (13). This study aims to investigate the impact of COVID-19 quarantine on several health-related aspects among adults in the UAE. These aspects are dietary habits, physical activity, food purchasing patterns, smoking, and sleeping patterns.
This study used a quantitative cross-sectional study design with a questionnaire as a data collection tool.
This study used snowball sampling. The inclusion criteria were citizens and residents of the UAE aged ≥18 years old, both male and female. Participants were asked to complete an anonymous electronic questionnaire created via Google Forms and distributed on various platforms, such as WhatsApp, Twitter, and email. The questionnaire link was sent in Arabic and English for the participants to use the language they prefer as some preferred English language, this has been concluded from the pilot study. The principal investigator sent the questionnaire via email to students and to other Zayed University (ZU) faculties. It was shared with students and faculties in different colleges at ZU. Moreover, faculties sent it to their students via email and WhatsApp groups, and they were asked to share it with their friends and family members. We used Zayed University email addresses to reach the participants. The questionnaire was available between November 1st 2020 and the end of January 2021. A total of 118 questionnaires with missing answers were removed, and we ended with 1,682 completed questionnaires.
An online questionnaire was designed to assess and explore changes in dietary habits, physical activity, food purchasing, smoking, and sleeping patterns during the COVID-19 pandemic in the UAE. This questionnaire was adopted from another similar study that used the questionnaire as a measurement tool. It has been modified from a survey by Di Renzo, which investigated the impact of the COVID-19 pandemic on eating habits and lifestyle changes among the Italian population aged ≥12 years. The study comprised a structured questionnaire that inquired about demographic information, anthropometric data (reported weight and height); dietary habits information and lifestyle habits information (2). The survey comprised 3 main sections with 32 questions in total. The platform used was Google Forms, and the link to the questionnaire was shared via WhatsApp, Twitter, Snapchat, and Instagram. The questionnaire was initially developed in English, then translated into Arabic and then pilot-tested with 30 students that were not familiar with the subject (not from the College of Natural and Health Sciences), and the errors were reviewed by the authors.
The first section included 10 questions regarding demographic data such as age, gender, nationality, occupation, medical history, weight, and height. The second section had 16 questions regarding dietary habits, such as the type of food consumed, the number of meals, and snacks. This section focused on assessing the participants' dietary intake during the lockdown and whether it underwent any changes. The third section had six questions regarding lifestyle habits such as exercise, smoking, and purchasing daily necessities. Individuals were also asked if their physical activities and weight had changed after the lockdown (after August 2020), COVID-19 lockdown period was defined as March 1st, 2020 to the End of August 2020 as per the Supreme Council for the National Security Emergency Crises and Disasters Management Authority in the UAE in August 2020.
Data were analyzed using the Statistical Package for Social Sciences, SPSS Version 27. Frequency distributions and percentages generated descriptive statistics to analyze the general characteristics of the participants. To better understand the relationship (association) between the dependent variable (weight change) and the independent variables (number of daily meals, number of snacks per day, consumption of cereals, consumption of sources of protein, consumption of fruits and vegetables, consumption of sweets and French fries, sense of hunger and satiety, level of physical activity), multiple Chi-square tests or Fisher exact tests were conducted whenever appropriate. Additionally, a contingency table was constructed to detail the food intake of the participants.
This study was approved by the Research Ethics Committee at Zayed University, UAE (ZU20_137_F) and the Research Ethics Committee at the Ministry of Health and Prevention (MOHAP/DXB-REC/ONN/No.147/2020). All study participants provided informed consent at the beginning of the online questionnaire.
A total of 1,682 participants were included in the analysis. Table 1 presents the general characteristics of the studied population. Most participants were aged 18–29 years old (69.7%), female (80.9%), from Dubai (51.4%), and the Northern Emirates (Sharjah, Ajman, Fujairah, Ras al-Khaimah, and Umm al-Quwain) (37.8%). Approximately half of the participants had a high school education (51.6%), and the rest had a university-level and higher education (45.4%). Around half of the participants were students (46.4), 19.1% were unemployed, and the rest were employed. In addition, the majority had a monthly income of <5,000 AED (63.2%).
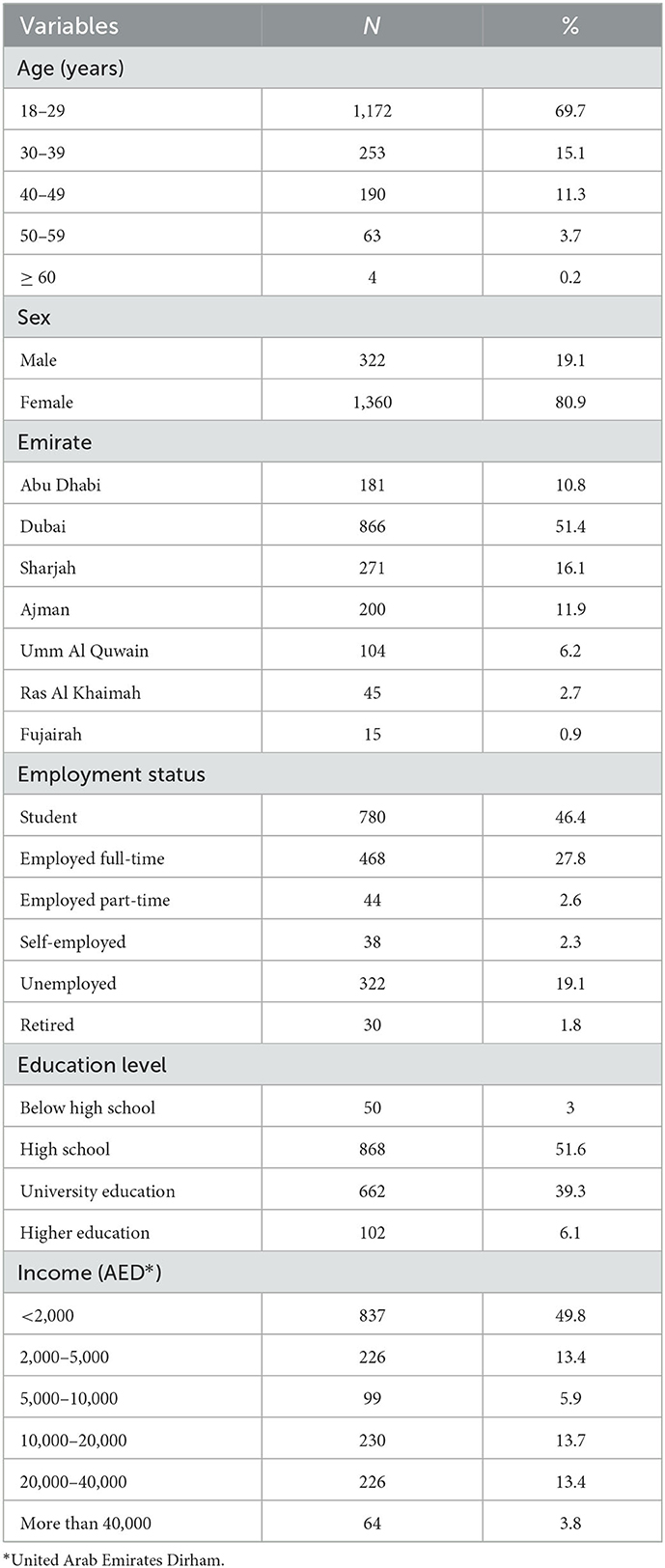
Table 1. General characteristics of the study participants (n = 1,682).
Figures 1, 2 present the participants' BMI and weight changes, respectively, during the COVID-19 lockdown period which was defined as the 1st of March 2020 to the End of August 2020 as per the Supreme Council for the National Security, National Emergency Crises and Disasters Management Authority in the UAE in August 2020. According to BMI categories, the majority of the participants had a normal weight (47.1%), followed by overweight (27.6%), obese (15.2%), and underweight (10.1%). Regarding weight changes during the COVID-19 lockdown, most participants (44.4%) reported an increase in weight, while 23.3% reported weight loss and 32.3% reported no change.
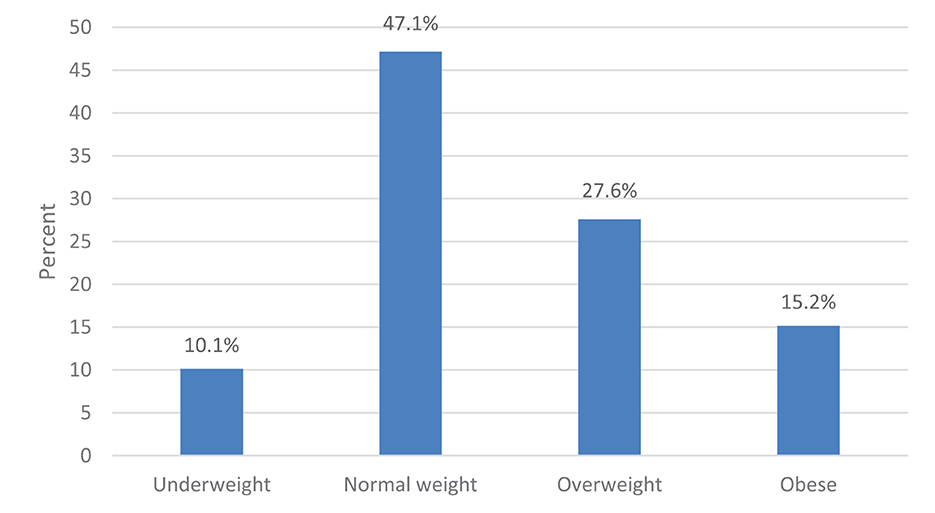
Figure 1. Participants' BMI during the COVID-19 lockdown (n = 1,682).
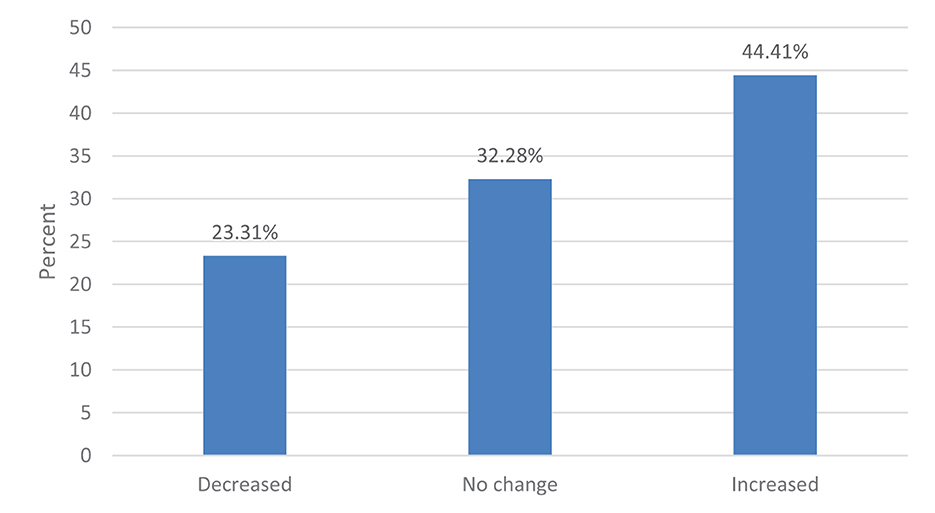
Figure 2. Participants' weight changes during the COVID-19 lockdown (n = 1,682).
In Table 2, the changes in weight during the COVID-19 lockdown according to age, gender, level of education, employment status, and monthly income are illustrated. Firstly, there was a significant association between changes in weight during the COVID-19 lockdown and age (p = 0.002). The youngest age group, aged 18–29 had the highest frequency across all weight change categories (gained, lost, and no change), with the highest being for weight loss (76.8%) followed by weight gain (69.3%). Those aged 30–39 had the second highest frequency for weight gain (15.8%), which was also the highest frequency for this age group across the weight change categories. Individuals over 60 made up the lowest frequency across the weight change groups, with the highest being for weight loss (0.5%).
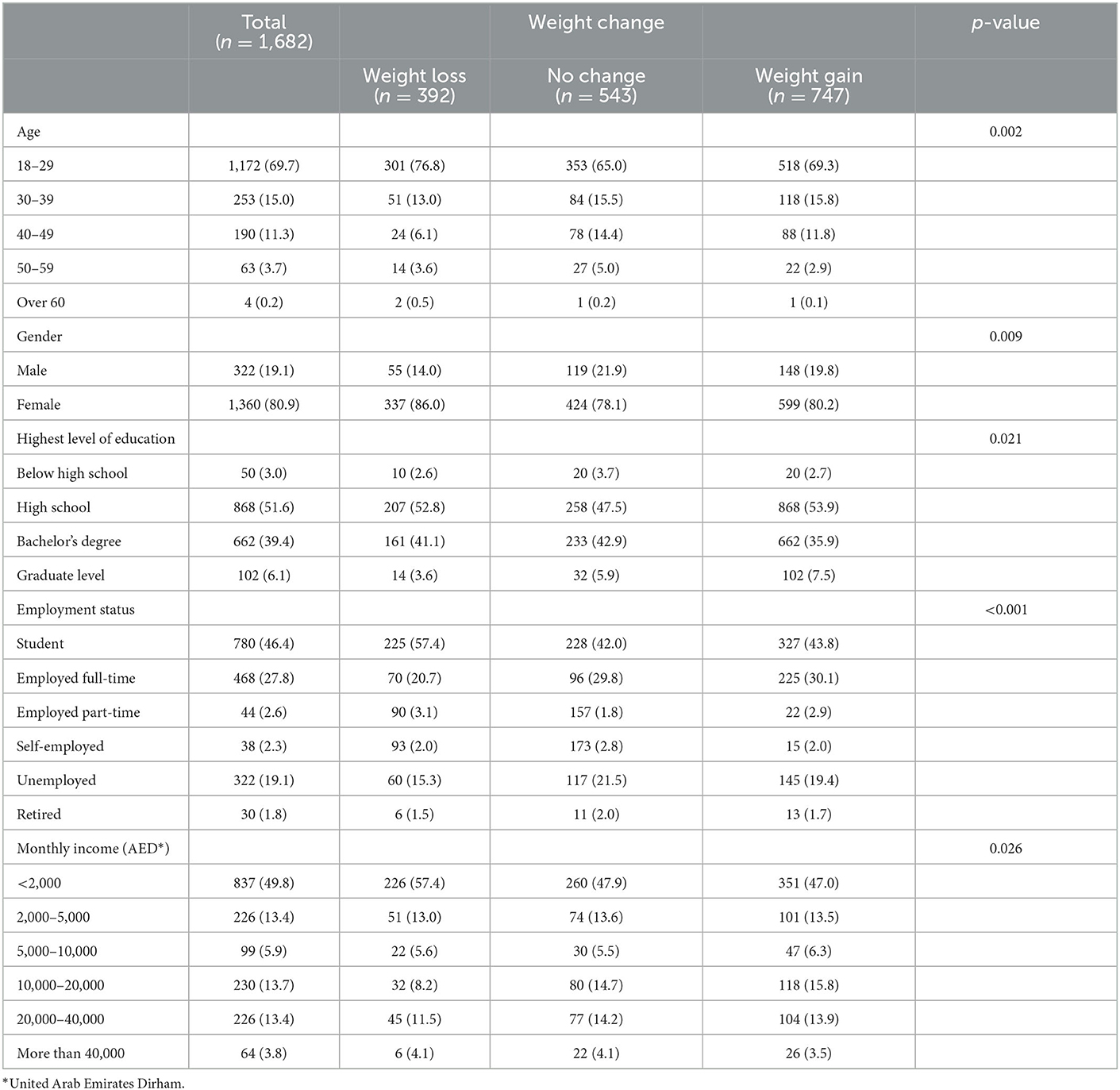
Table 2. Changes in weight during COVID-19 according to age, gender, level of education, employment status, and monthly income (n = 1,682).
Regarding gender, there was a significant association between changes in weight during the COVID-19 lockdown and gender (p = 0.009). Females had the highest frequencies in all weight change categories, with weight loss being the highest (86.0%) followed by weight gain (80.2%). Males made up a bigger percentage of the “no change” category (21.9%) compared to their frequency in weight gain (19.8%) and weight loss (14.0%). Level of education was also significantly associated with changes in weight during the COVID-19 lockdown (p = 0.021). The majority possessed a high school degree (51.6%). This group was the most frequent in all weight change categories, with the highest being in weight gain (53.9%) closely followed by weight loss (52.8%). Those with a bachelor's degree had their highest frequency in the no-change group (42.9%). Those below high school also had their highest frequency in the no-change group (3.7%). Finally, those at the graduate level had their highest frequency in the weight gain group (7.5%).
There was a significant association between weight changes during the COVID-19 lockdown and employment status (p < 0.001). Those who gained weight mainly were students (43.8%), followed by employed full-time (30.1%). The lowest percentage was retired people (1.7%). Among those who lost weight, most were students (57.4%), followed by employed full-time (20.7%). The last were retired (1.5%). Finally, those who experienced no change were mainly students (42.0%), then employed full-time (29.8%). The smallest percentage was retired (2.0%). Finally, monthly income is another variable significantly associated with weight changes during the lockdown (p = 0.026). Those who earned <2,000 AED had the highest frequency in all weight change categories. Among those, the highest was for weight loss (57.4%). The second highest frequency for weight gain, after those who earned <2,000 AED (45.0%), was for those who earned 10,000–20,000 AED (15.8%). This percentage was also the highest for this group across all weight change categories, meaning that this group mostly gained weight.
Table 3 illustrates the relationship between changes in dietary habits (such as the frequency of meals, snacks, and the consumption of certain food groups) and the weight change groups (gain, loss, or no change). Approximately 35.7% of those who gained weight during quarantine showed an increase in the number of daily meals. Compared to 14.5% of those who lost weight and 14.5% of those who experienced no change. Similarly, the highest frequency of increased snacking 304 (40.7%) was in individuals who gained weight. Changes in the number of daily meals were significantly associated with changes in weight during the COVID-19 lockdown (p < 0.001).
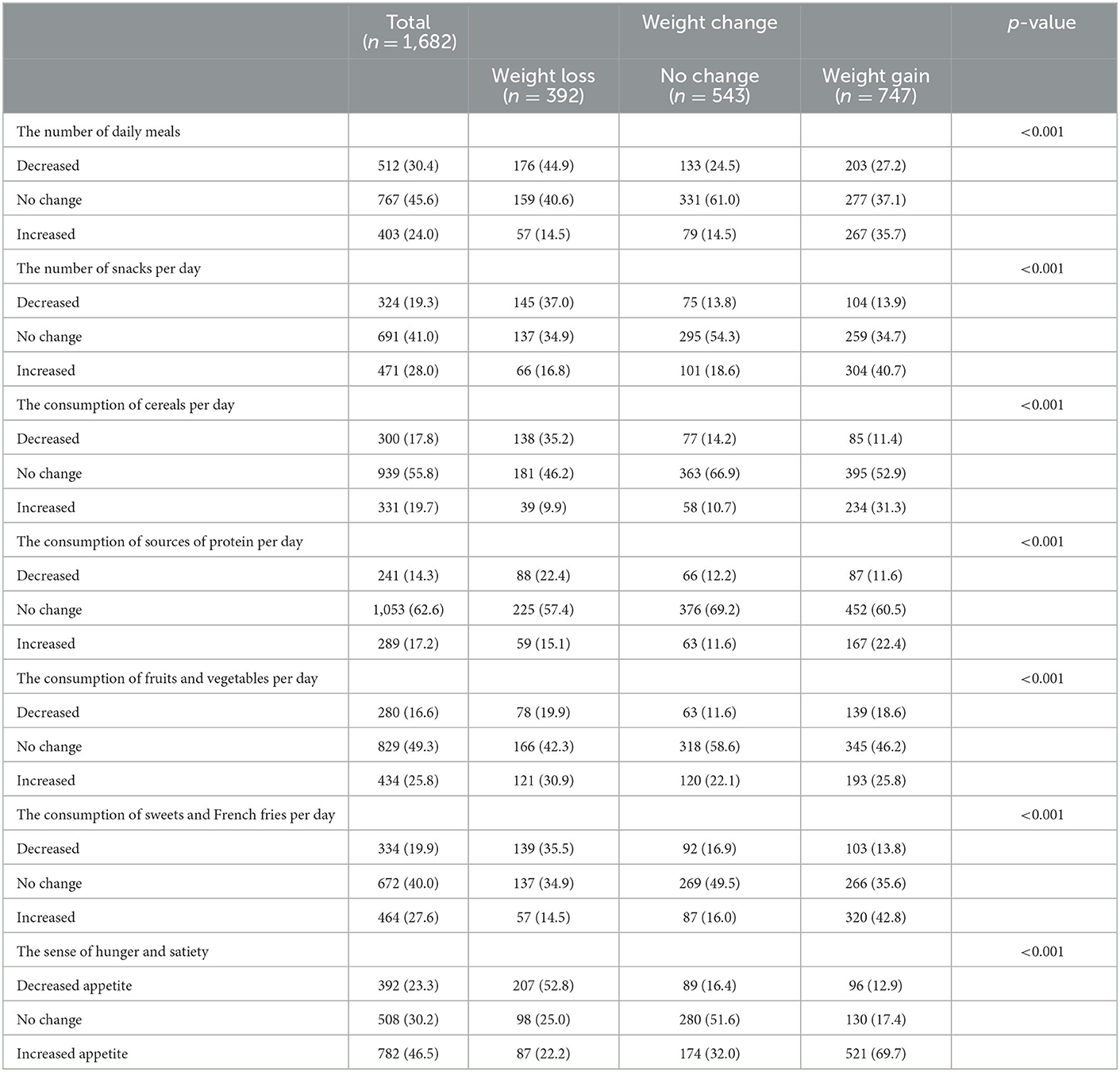
Table 3. Changes in dietary habits compared with weight changes during the COVID-19 lockdown in UAE (n = 1,682).
Consuming cereals, protein sources, fruits, and vegetables, sweets, and French fries during quarantine was significantly associated with changes in weight (p < 0.001 for all). Those who consumed more cereals and protein sources had their highest frequencies in the weight gain group (31.3% and 22.4%, respectively). On the other hand, those who increased their consumption of fruits and vegetables had the highest frequency in the weight loss group (30.9%). Most participants reported no change in their consumption of sweets and French fries (40.0%), while 27.6% reported an increase in consumption. However, 42.8% of those who gained weight reported an increase in consumption of this category.
During the quarantine, most participants reported an increase in appetite (46.5%). More than two-thirds (69.7%) of those who gained weight reported an increase in appetite. In contrast, 52.8% of those who lost weight reported a decrease in appetite. Changes in the sense of hunger and satiety were significantly related to changes in weight during the COVID-19 lockdown (p < 0.001).
Table 4 summarizes the changes in physical activity and smoking level compared to weight changes during the lockdown. Among the 1,682 participants, only 21.8% reported increased physical activity, 26.1% decreased physical activity, 22.8% reported no changes, and 29.4% never practiced physical activity. Among those who increased their physical activity (21.8%) during the lockdown, 38% lost weight, and 32% experienced no changes in their weight. On the other hand, among those who decreased their physical activity, 62.2% gained weight, and only 15.9% reported no body weight changes. Moreover, 41% reported no changes in their weight among those who didn't change their physical activity. Weight loss was reported by 23.5% of this group. There was a significant relationship between changes in levels of physical activity and changes in weight before and after lockdown (p < 0.001).
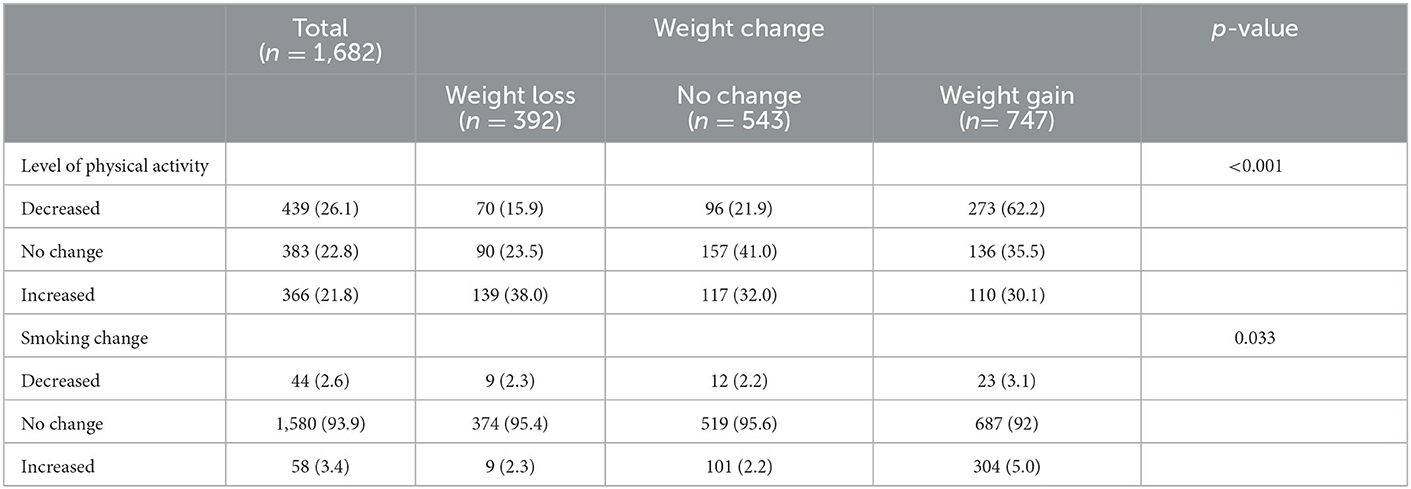
Table 4. Changes in the level of physical activity and smoking habits compared with weight changes during the COVID-19 lockdown in UAE (n = 1,682).
Similarly, changes in smoking habits were significantly associated with changes in weight during lockdown (p = 0.033). The majority reported no change in their smoking habits (93.9%). Those who increased their smoking had a higher frequency of weight gain (5.0%) than those who decreased their smoking (3.1%).
Table 5 presents the adjusted factors significantly associated with the change in weight. After adjusting for the other confounders, people who increased the number of meals consumed were more likely to gain weight (AOR = 1.68, 95% CI = 1.12, 2.54). While an increase in the cereals consumed was positively associated with the change in weight (AOR = 1.67, 95% CI = 1.08, 2.57), the persons who reduced the number of consumed cereals were more likely to lose weight (AOR = 0.53, 95% CI = 0.35, 0.81). The respondents who reported an increase in their sweets' consumption or their desire for food (hunger) had twice the odds of putting on more weight (AOR = 2.19, 95% CI = 1.50, 3.19) and (AOR = 2.19, 95% CI = 1.53, 3.14), respectively. On the other hand, compared to those who did not face any change in the desire for sweets or food (hunger), the persons who reported a decline in their sweets' consumption or their desire for food (hunger) are more likely to lose weight (AOR = 0.84, 95% CI = 0.58, 1.21) and (AOR = 0.54, 95% CI = 0.36, 0.81), respectively.
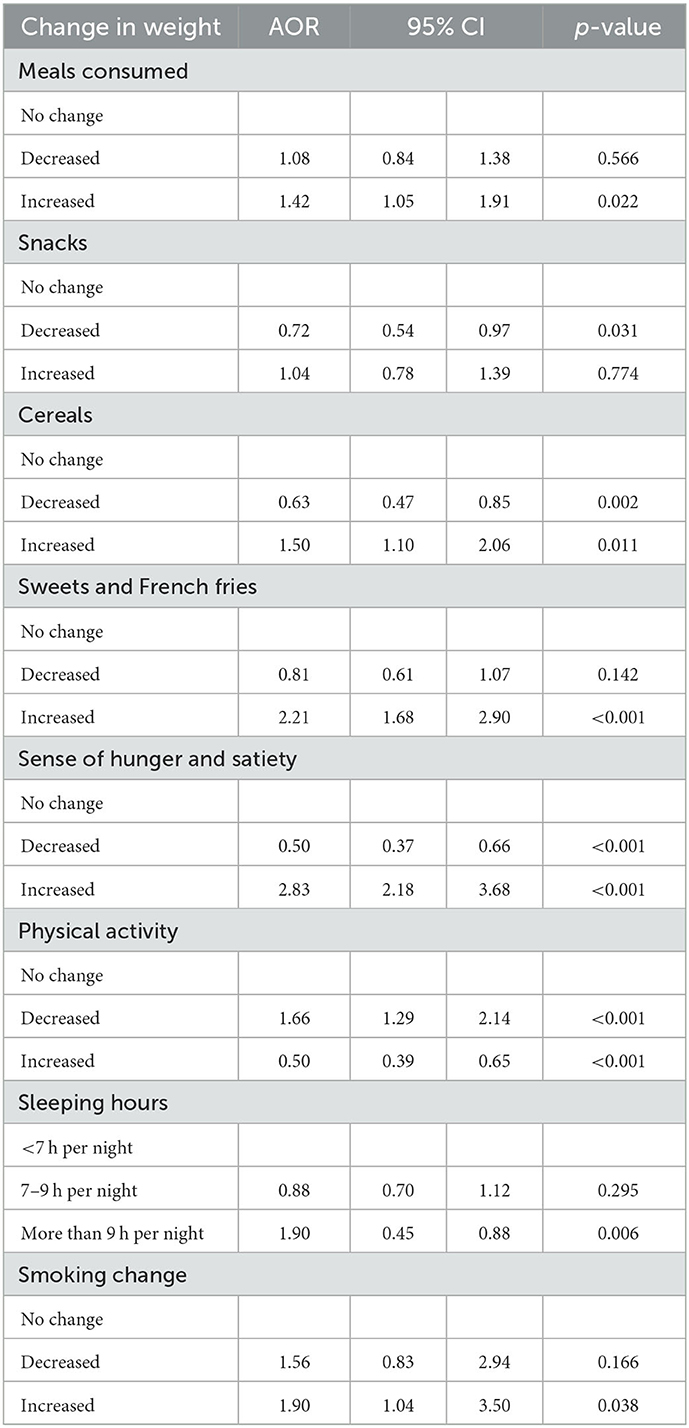
Table 5. Adjusted factors significantly associated with a change in weight.
Physical activity was negatively associated with the change in weight: increasing the level of physical activity was more likely to lead to a loss in weight (AOR = 0.61, 95% CI = 0.44, 0.86). On the contrary, persons who practiced fewer sports activities had twice the odds of gaining weight (AOR = 2.25, 95% CI = 1.58, 3.21). The consumption of protein was not significantly associated with the change in weight.
When it comes to sleeping patterns, those who slept more than 9 h per night were more likely to lose weight (AOR = 1.90, 95% CI = 0.45, 0.88). In terms of changes in smoking, those who stated rising in smoking were more likely to gain weight (AOR = 1.90, 95% CI = 1.04, 3.50).
The present study aimed to investigate the impact of COVID-19 quarantine on dietary habits, physical activity, food purchasing, smoking, and sleeping patterns in the UAE. Overall, this study has found that quarantine has negatively affected these health-related variables.
In terms of weight changes during the COVID-19 lockdown, most participants (44.4%) reported an increase in weight. This weight gain can be attributed to the general decrease in energy expenditure since quarantine limits people's ability to go to work, gyms, parks, and even to practice their regular daily routines. In addition, the emotional distress accompanied by having to remain at home for months, fear of novelty, and the high spread of COVID-19 might have provoked emotional eating and cravings (46). Other determinants leading to increased weight gain during the lockdown include prior behaviors, dietary habits, physical activity, type of work environment, psychosocial and socioeconomic factors, and co-morbidities (4). This result agrees with previous studies that evaluated weight gain relating to COVID-19 home confinement (2, 47, 48). In addition, studies in other countries revealed an increase in caloric intake and indicated weight gain during the COVID-19 lockdown (2, 49–51).
However, in this study, 32.3% of participants did not notice any weight change, and 23.3% reported weight loss. This could be due to high levels of awareness, or they may not have been as majorly affected by quarantine.
During the lockdown, those who gained weight had the highest frequency of participants who increased the number of their daily meals (35.7%), and the highest frequency of increased snacking (40.7%). This is compared to those who reported losing or no weight change. Further testing using logistic regression also showed that those who increased the number of consumed meals were more likely to gain weight (AOR = 1.68, 95% CI = 1.12, 2.54). Similarly, previous studies reported higher amounts of food intake during lockdown periods in Poland, Italy, and UK (5, 19). Consuming more cereals during quarantine was significantly associated with increased weight gain (p < 0.001) and with changes in weight (AOR = 1.67, 95% CI = 1.08, 2.57). Conversely, those who reduced the amount of consumed cereals were more likely to lose weight (AOR = 0.53, 95% CI = 0.35, 0.81). A significant difference was seen between the frequency of sweets and French fries' consumption and weight changes during quarantine (p < 0.001). The participants who reported increased intake of sweets had double the odds of putting on more weight (AOR = 2.19, 95% CI = 1.50, 3.19).
Furthermore, those who experienced a decline in their desire for sweets were more likely to lose weight (AOR = 0.84, 95% CI = 0.58, 1.21) than those who didn't experience a change. This was in line with a previous study in Germany which demonstrated an increase in the consumption of foods that are high in sugar and fat such as sweets, and found that it was a significant determinant of weight changes during quarantine (52). This may be due to the increased stress caused by the pandemic. People tend to seek “comfort foods” while coping with stressful situations (52). Furthermore, during home confinement, people tended to stock their kitchens with food to reduce unnecessary grocery trips out of fear of contracting the infection (48). The availability of large quantities of food for many days might lead to overeating that is not necessarily due to hunger (53).
During the lockdown, changes in hunger and satiety were significantly related to weight changes (p < 0.001). The current study showed that 69.7% of those who gained weight reported an increase in appetite. In contrast, 52.8% of those who lost weight reported a reduction in appetite. Additionally, those who reported an increase in their desire for food (hunger) had twice the odds of weight gain (AOR = 2.19, 95% CI = 1.53, 3.14). Compared to those who didn't face any change, those who reported a decline in their desire for food (hunger) were more likely to lose weight (AOR = 0.54, 95% CI = 0.36, 0.81). These changes may be due to psychological and environmental stressors, consistent with other studies (46).
Regarding physical activity, the present study revealed that among the 1,682 participants, only 21.8% reported an increase in physical activity, 26.1% decreased their physical activity, 22.8% reported no changes, and 29.4% never practiced physical activity. Among those who gained weight, 36.5% reduced their levels of physical activity, and 30.5% had never practiced physical activity. These findings are consistent with recent studies highlighting many individuals (>50%) who reported changes in their physical activity and an increase in their sedentary behavior (8, 48, 49, 54). Previous studies have shown that reduced activity and increased sedentary time increase the risk of gaining weight both in general (55–57), and particularly during the COVID-19 pandemic, in both people with normal weight (4, 10, 58, 59) and with obesity (60).
Nevertheless, other studies have found that individuals had increased their physical activity levels during their lockdown periods. For example, 21.5% of those who maintained their weight had increased their level of physical activity, and 22.8% maintained the same level of physical activity. Among those who increased their physical activity (21.8%) during the lockdown, 38% lost weight, whereas 32% experienced no changes in their weight.
Physical activity was negatively associated with the change in weight. Increased physical activity increases the likelihood of weight loss (AOR = 0.61, 95% CI = 0.44, 0.86). On the other hand, those with lower physical activity levels had twice the odds of gaining weight (AOR = 2.25, 95% CI = 1.58, 3.21). This may be one of the ways of maintaining healthy behaviors and mitigating the negative impact of lockdown on mood and wellbeing (2, 55). Exercise positively impacts weight management, overall health, and mental wellbeing. It can improve mood, confidence, body image, motivation, and eating habits (61).
Results regarding smoking included that those who increased their smoking had a higher frequency of weight gain (5.0%) than those who decreased their smoking (3.1%). Results of logistic regression testing found the same association where those who smoked more were more likely to experience weight gain (AOR = 1.90, 95% CI = 1.04, 3.50). A similar study also showed a link between tobacco use and weight gain (62). Finally, the only finding regarding sleep was that those who sleep more than 9 h per night are more likely to lose weight (AOR = 1.90, 95% CI = 0.45, 0.88). Studies have found an association between sleep loss and irregular sleep, and weight gain during COVID-19 lockdowns around the world (63, 64).
Therefore, it is important to investigate the consequences of the COVID-19 pandemic and quarantine on the health of the UAE population to create targeted interventions to improve people's lifestyles following the pandemic and to prevent similar outcomes in the case of emergencies. This is especially needed in the UAE.
This study was subjected to several limitations. The study used snowball sampling by sending the survey to students who introduced an age bias. Most of the participants were women, as the survey was sent to Zayed University students who were mostly female. This makes the sample not representative of the UAE population. Another limitation is that the questionnaire questions were close-ended, meaning there might be other unexplored answers, and the choices might suggested answers that were otherwise not the participants' genuine opinions. Additionally, since it was an online questionnaire, the participants may have had a vague understanding of some questions, or they might have interpreted them differently than intended. However, this was minimized by using clear language and having the questions pilot tested by students that are not familiar with the subject (students not from the College of Natural and Health Sciences). Furthermore, this study did not examine the exact food habits and level of physical activity of the participants. Therefore, the data are lacking in these two areas, we didn't investigate all the components of Eating habits. For example, a Likert-type response of the consumption of specific food items, ranging from never to every day.
Overall, the present study found that most of the population has shown weight gain, increased food consumption, and decreased or no change in physical activity. The groups most likely to gain weight included those who consumed more meals and cereals, had an increased desire for sweets, and had an increased desire for food (hunger). In addition, changes in levels of physical activity were significantly associated with changes in weight during the lockdown. Those who exercised more were more likely to lose weight. Participants who slept more than 9 h were also more likely to lose weight. Finally, increases in smoking seem to be tied to weight gain. Interventions and awareness campaigns need to be conducted to encourage a healthier lifestyle for the people of the UAE. Not only is a healthy lifestyle important for immunity, it is also necessary to prevent chronic illnesses such as diabetes and heart disease. Preventing such illnesses has always been a goal of the UAE due to their high prevalence. Finally, further research can be done on the exact food habits and level of physical activity of the UAE population during the lockdown to find areas that need to be targeted.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
This study was approved by the Research Ethics Committee at Zayed University, UAE (ZU20_137_F) and the Research Ethics Committee at the Ministry of Health and Prevention (MOHAP/DXBREC/ONN/No. 147/2020). All study participants provided informed consent at the beginning of the online questionnaire. The patients/participants provided their written informed consent to participate in this study.
SA designed the study and manuscript writing. SA, MA, and AK recruited the participants and supervised the data collection. FE analyzed the data. SA, MA, ZT, and AK wrote the manuscript. All contributed authors of this original manuscript authorized the final version of the manuscript and read and approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sadeghi Dousari A, Taati Moghadam M, Satarzadeh N. COVID-19 (coronavirus disease 2019): a new coronavirus disease. Infection Drug Resist. (2020) 13:2819–28. doi: 10.2147/IDR.S259279
2. Renzo LD, Gualtieri P, Pivari F, Soldati L, Attinà A, Cinelli G, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J Transl Med. (2020) 18:1–15. doi: 10.21203/rs.3.rs-30403/v1
3. Picchioni F, Goulao LF, Roberfroid D. The impact of COVID-19 on diet quality, food security and nutrition in low and middle income countries: a systematic review of the evidence. Clin Nutr. (2021). doi: 10.1016/j.clnu.2021.08.015
4. Zachary Z, Brianna F, Brianna L, Garrett P, Jade W, Alyssa D, et al. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obesity Res Clin Pract. (2020) 14:210–6. doi: 10.1016/j.orcp.2020.05.004
5. Robinson E, Boyland E, Chisholm A, Harrold J, Maloney NG, Marty L, et al. Obesity, eating behavior and physical activity during COVID-19 lockdown: a study of UK adults. Appetite. (2021) 156:104853. doi: 10.1016/j.appet.2020.104853
6. Ammar A, Brach M, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. (2020) 12:1583.
7. Barrett S, Rodda K, Begg S, O'Halloran PD, Kingsley MI. Exercise and COVID-19: reasons individuals sought coaching support to assist them to increase physical activity during COVID-19. Aust N Z J Public Health. (2021) 45:133–7. doi: 10.1111/1753-6405.13089
8. Sidebottom C, Ullevig S, Cheever K, Zhang T. Effects of COVID-19 pandemic and quarantine period on physical activity and dietary habits of college-aged students. Sports Med Health Sci. (2021) 3:228–35. doi: 10.1016/j.smhs.2021.08.005
9. Dunton G, Do B, Wang S. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in US children. BMC Public Health. (2020) 20:1–13. doi: 10.33774/coe-2020-q6pz0
10. Cheikh Ismail L, Osaili TM, Mohamad MN, Al Marzouqi A, Jarrar AH, Abu Jamous DO, et al. Eating habits and lifestyle during COVID-19 lockdown in the United Arab Emirates: a cross-sectional study. Nutrients. (2020) 12:3314. doi: 10.3390/nu12113314
11. Sajwani NH, Qawas A, Al Ali N, Sajwani FH, Alrustamani AH, Al Maamari S, et al. The effect of lockdowns and distant learning on the health-related behaviours of school students in the United Arab Emirates. BMC Primary Care. (2022) 23:253. doi: 10.1186/s12875-022-01856-y
12. Radwan H, Kitbi MA, Hasan H, Hilali MA, Abbas N, Hamadeh R, et al. Diet and lifestyle changes during COVID-19 lockdown in the United Arab Emirates: results of a cross-sectional study. (2020). doi: 10.21203/rs.3.rs-76807/v1 [preprint].
13. Radwan H, Al Kitbi M, Hasan H, Al Hilali M, Abbas N, Hamadeh R, et al. Indirect health effects of COVID-19: unhealthy lifestyle behaviors during the lockdown in the United Arab Emirates. Int J Environ Res Public Health. (2021) 18:1964. doi: 10.3390/ijerph18041964
14. Dergaa I, Ammar A, Souissi A, Fessi MS, Trabelsi K, Glenn JM, et al. COVID-19 lockdown: impairments of objective measurements of selected physical activity, cardiorespiratory and sleep parameters in trained fitness coaches. Excli J. (2022) 21:1084–98. doi: 10.17179/excli2022-4986
15. Dergaa I, Abdelrahman H, Varma A, Yousfi N, Souissi A, Ghram A, et al. COVID-19 vaccination, herd immunity and the transition toward normalcy: challenges with the upcoming sports events. Ann Appl Sport Sci. (2021) 9. doi: 10.52547/aassjournal.1032
16. Figliozzi M, Unnikrishnan A. Home-deliveries before-during COVID-19 lockdown: Accessibility, Environmental Justice, equity, and policy implications. Transp Res Part D Transp Environ. (2021) 93:102760. doi: 10.1016/j.trd.2021.102760
17. Chen J, Zhang Y, Zhu S, Liu L. Does COVID-19 affect the behavior of buying fresh food? Evidence from Wuhan, China. Int J Environ Res Public Health. (2021) 18:4469. doi: 10.3390/ijerph18094469
18. Espinoza-Ortega A, Martínez-García CG, Rojas-Rivas E, Fernández-Sánchez Y, Escobar-López SY, Sánchez-Vegas L. Consumer and food changes in Mexican households during maximal contingency in the COVID-19 pandemic. Int J Gastron Food Sci. (2021) 24:100357. doi: 10.1016/j.ijgfs.2021.100357
19. Zanetta LDA, Hakim MP, Gastaldi GB, Seabra LMA, Rolim PM, Nascimento LG, et al. The use of food delivery apps during the COVID-19 pandemic in Brazil: the role of solidarity, perceived risk, and regional aspects. Food Res Int. (2021) 149:110671. doi: 10.1016/j.foodres.2021.110671
20. Rodrigues JF, dos Santos Filho MT, de Oliveira LE, Siman IB, de Fátima Barcelos A, Ramos GL, et al. Effect of the COVID-19 pandemic on food habits and perceptions: a study with Brazilians. Trends Food Sci Technol. (2021) 116:992–1001. doi: 10.1016/j.tifs.2021.09.005
21. Poelman MP, Gillebaart M, Schlinkert C, Dijkstra SC, Derksen E, Mensink F, et al. Eating behavior and food purchases during the COVID-19 lockdown: a cross-sectional study among adults in the Netherlands. Appetite. (2021) 157:105002. doi: 10.1016/j.appet.2020.105002
22. Ziółko M, Sułek K, Suprunenko Y, Werońska K, Dziedzic D. The increasing popularity and service quality assessment of online food ordering applications in the COVID-19 pandemic. A study of Uber Eats in Poland. Ann Univ Mariae Curie-Skłodowska Oecon. (2022) 55:73–95. doi: 10.17951/h.2021.55.4.73-95
23. Alaimo LS, Fiore M, Galati A. How the COVID-19 pandemic is changing online food shopping human behaviour in Italy. Sustainability. (2020) 12:9594. doi: 10.3390/su12229594
24. Asfahani A. The impact of COVID-19 on the decision making for the customer relation management in the Middle East. J Manag Inform Decis Sci. (2021) 24:3.
25. Faour-Klingbeil D, Osaili TM, Al-Nabulsi AA, Jemni M, Todd ECD. An on-line survey of the behavioral changes in Lebanon, Jordan and Tunisia during the COVID-19 pandemic related to food shopping, food handling, and hygienic practices. Food Control. (2021) 125:107934. doi: 10.1016/j.foodcont.2021.107934
26. Ben Hassen T, El Bilali H, Allahyari MS, Charbel L. Food shopping, preparation and consumption practices in times of COVID-19: case of Lebanon. J Agribus Dev Emerg Econ. (2021) 12:281–303. doi: 10.1108/JADEE-01-2021-0022
27. Ben Hassen T, El Bilali H, Allahyari MS. Impact of COVID-19 on food behavior and consumption in Qatar. Sustainability. (2020) 12:6973. doi: 10.3390/su12176973
28. AlTarrah D, AlShami E, AlHamad N, AlBesher F, Devarajan S. The impact of coronavirus COVID-19 pandemic on food purchasing, eating behavior, and perception of food safety in Kuwait. Sustainability. (2021) 13:8987. doi: 10.3390/su13168987
29. Hoteit M, Mortada H, Al-Jawaldeh A, Mansour R, Yazbeck B, AlKhalaf M, et al. Dietary diversity in the eastern Mediterranean region before and during the COVID-19 pandemic: disparities, challenges, and mitigation measures. Front Nutr. (2022) 9:813154.
30. Alhefeiti A, Aldhanhani H, Almatrooshi R, Singh Sisodia G. The impact of COVID-19 on the food industry. Rev Estrat Organ. (2021) 10:e4959. doi: 10.22490/25392786.4959
31. Alichleh AL-Ali AS, Sisodia GS, Gupta B, Venugopalan M. Change management and innovation practices during pandemic in the Middle East e-commerce industry. Sustainability. (2022) 14:4566. doi: 10.3390/su14084566
32. De Carvalho NC, Amaral CA, Liboredo JC. Cooking or consuming food from away home after the COVID-19 lockdown in Brazil? J Culinary Sci Technol. (2022) 2022:1–24. doi: 10.1080/15428052.2022.2104772
33. Ben Hassen T, El Bilali H, Allahyari MS, Morrar R. Food attitudes and consumer behavior towards food in conflict-affected zones during the COVID-19 pandemic: case of the Palestinian Territories. Br Food J. (2021) 124:2921–36. doi: 10.1108/BFJ-05-2021-0590
34. Bourdas DI, Zacharakis ED, Travlos AK, Souglis A, Georgali TI, Gofas DC, et al. Impact of lockdown on smoking and sleeping in the early COVID-19 presence: datasets of Greek adults sample. Data Brief. (2021) 39:107480. doi: 10.1016/j.dib.2021.107480
35. Munarini E, Stival C, Boffi R, Lugoboni F, Veronese C, Tinghino B, et al. Factors associated with a change in smoking habit during the first COVID-19 lockdown: an Italian cross-sectional study among ever-smokers. BMC Public Health. (2022) 22:1–15. doi: 10.1186/s12889-022-13404-5
36. Gendall P, Hoek J, Stanley J, Jenkins M, Every-Palmer S. Changes in tobacco use during the 2020 COVID-19 lockdown in New Zealand. Nicotine Tobacco Res. (2021) 23:866–71. doi: 10.1093/ntr/ntaa257
37. Bar-Zeev Y, Shauly M, Lee H, Neumark Y. Changes in smoking behaviour and home-smoking rules during the initial COVID-19 lockdown period in Israel. Int J Environ Res Public Health. (2021) 18:1931. doi: 10.3390/ijerph18041931
38. Carreras G, Lugo A, Stival C, Amerio A, Odone A, Pacifici R, et al. Impact of COVID-19 lockdown on smoking consumption in a large representative sample of Italian adults. Tob Control. (2021) 31:615–22. doi: 10.1136/tobaccocontrol-2020-056440
39. Janati Idrissi A, Lamkaddem A, Benouajjit A, Ben El Bouaazzaoui M, El Houari F, Alami M, et al. Sleep quality and mental health in the context of COVID-19 pandemic and lockdown in Morocco. Sleep Med. (2020) 74:248–53. doi: 10.1016/j.sleep.2020.07.045
40. Altena E, Baglioni C, Espie CA, Ellis J, Gavriloff D, Holzinger B, et al. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: practical recommendations from a task force of the European CBT-I Academy. J Sleep Res. (2020) 29:e13052. doi: 10.1111/jsr.13052
41. Ahmed Alhayyani RM, Qassem MY, Ahmed Alhayyani AM, Al-Garni AM, Raffaa HS, et al. Sleep patterns and predictors of poor sleep quality among Saudi commission residents in the ASEER region, Saudi Arabia before and during COVID-19 pandemic. J Fam Med Primary Care. (2022) 11:2768. doi: 10.4103/jfmpc.jfmpc_1946_21
42. Krishnan V, Gupta R, Grover S, Basu A, Tripathi A, Subramanyam A, et al. Changes in sleep pattern and sleep quality during COVID-19 lockdown. Indian J Psychiatry. (2020) 62:370. doi: 10.4103/psychiatry.IndianJPsychiatry_523_20
43. Mandelkorn U, Genzer S, Choshen-Hillel S, Reiter J, Meira e Cruz M, Hochner H, et al. Escalation of sleep disturbances amid the COVID-19 pandemic: a cross-sectional international study. J Clin Sleep Med. (2021) 17:45–53. doi: 10.5664/jcsm.8800
44. Kokou-Kpolou CK, Megalakaki O, Laimou D, Kousouri M. Insomnia during COVID-19 pandemic and lockdown: prevalence, severity, and associated risk factors in French population. Psychiatry Res. (2020) 290:113128. doi: 10.1016/j.psychres.2020.113128
45. Brougham RR, Zail CM, Mendoza CM, Miller JR. Stress, sex differences, and coping strategies among college students. Curr Psychol. (2009) 28:85–97. doi: 10.1007/s12144-009-9047-0
46. Lima CK, Carvalho PM, Lima Ide, Nunes JV, Saraiva JS, de Souza RI, et al. The emotional impact of coronavirus 2019-ncov (new coronavirus disease). Psychiatry Res. (2020) 287:112915. doi: 10.1016/j.psychres.2020.112915
47. Khan MAB, Menon P, Govender R, Samra A, Nauman J, Ostlundh L, et al. Systematic review of the effects of pandemic confinements on body weight and their determinants. Br J Nutr. (2021) 127:298–317. doi: 10.1101/2021.03.03.21252806
48. Sidor A, Rzymski P. Dietary choices and habits during COVID-19 lockdown: experience from Poland. Nutrients. (2020) 12:1657. doi: 10.3390/nu12061657
49. Deschasaux-Tanguy M, Druesne-Pecollo N, Esseddik Y, de Edelenyi FS, Allès B, Andreeva VA, et al. Diet and physical activity during the COVID-19 lockdown period (March–May 2020): results from the French NutriNet-Santé Cohort Study. medRxiv. (2020). doi: 10.1101/2020.06.04.20121855
50. Bhutani S, Cooper JA. COVID-19-related home confinement in adults: weight gain risks and opportunities. Obesity. (2020) 28:1576–7. doi: 10.1002/oby.22904
51. Husain W, Ashkanani F. Does COVID-19 change dietary habits and lifestyle behaviours in Kuwait: a community-based cross-sectional study. Environ Health Prev Med. (2020) 25:1–13. doi: 10.1186/s12199-020-00901-5
52. Palmer K, Bschaden A, Stroebele-Benschop N. Changes in lifestyle, diet, and body weight during the first COVID 19 'lockdown' in a student sample. Appetite. (2021) 167:105638. doi: 10.1016/j.appet.2021.105638
53. Rolls BJ, Roe LS, Meengs JS. The effect of large portion sizes on energy intake is sustained for 11 days. Obesity. (2007) 15:1535–43. doi: 10.1038/oby.2007.182
54. Rodríguez-Pérez C, Molina-Montes E, Verardo V, Artacho R, García-Villanova B, Guerra-Hernández EJ, et al. Changes in dietary behaviours during the COVID-19 outbreak confinement in the Spanish COVID study. Nutrients. (2020) 12:1730. doi: 10.3390/nu12061730
55. López-Bueno R, Calatayud J, Casaña J, Casajús JA, Smith L, Tully MA, et al. COVID-19 confinement and health risk behaviors in Spain. Front Psychol. (2020) 11:1426. doi: 10.3389/fpsyg.2020.01426
56. Slentz CA, Duscha BD, Johnson JL, Ketchum K, Aiken LB, Samsa GP, et al. Effects of the amount of exercise on body weight, body composition, and measures of central obesity. Arch Intern Med. (2004) 164:31. doi: 10.1001/archinte.164.1.31
57. AlMughamis N, AlAsfour S, Mehmood S. Poor eating habits and predictors of weight gain during the COVID-19 quarantine measures in Kuwait: a cross sectional study. F1000Research. (2020) 9:914. doi: 10.12688/f1000research.25303.1
58. Drywień ME, Hamulka J, Zielinska-Pukos MA, Jeruszka-Bielak M, Górnicka M. The COVID-19 pandemic lockdowns and changes in body weight among Polish women. A cross-sectional online survey PLIFECOVID-19 study. Sustainability. (2020) 12:7768. doi: 10.3390/su12187768
59. Reyes-Olavarría D, Latorre-Román PÁ, Guzmán-Guzmán IP, Jerez-Mayorga D, Caamaño-Navarrete F, Delgado-Floody P. Positive and negative changes in food habits, physical activity patterns, and weight status during COVID-19 confinement: associated factors in the Chilean population. Int J Environ Res Public Health. (2020) 17:5431. doi: 10.3390/ijerph17155431
60. Pellegrini M, Ponzo V, Rosato R, Scumaci E, Goitre I, Benso A, et al. Changes in weight and nutritional habits in adults with obesity during the “lockdown” period caused by the COVID-19 virus emergency. Nutrients. (2020) 12:2016. doi: 10.3390/nu12072016
61. Dor-Haim H, Katzburg S, Revach P, Levine H, Barak S. The impact of COVID-19 lockdown on physical activity and weight gain among active adult population in Israel: a cross-sectional study. BMC Public Health. (2021) 21:1–10. doi: 10.1186/s12889-021-11523-z
62. Mulugeta W, Desalegn H, Solomon S. Impact of the COVID-19 pandemic lockdown on weight status and factors associated with weight gain among adults in Massachusetts. Clin Obes. (2021) 11:e12453. doi: 10.1111/cob.12453
63. Pillai K, Pillai M, Doddi S. Impact of COVID-19 pandemic lockdown on weight of patients in outpatient setting. Obesity Pillars. (2022) 3:100028. doi: 10.1016/j.obpill.2022.100028
Keywords: COVID-19, physical activity, weight, dietary habits, food consumption, smoking, sleeping patterns, food purchasing patterns
Citation: AlBlooshi S, AlFalasi M, Taha Z, El Ktaibi F and Khalid A (2023) The impact of COVID-19 quarantine on lifestyle indicators in the United Arab Emirates. Front. Public Health 11:1123894. doi: 10.3389/fpubh.2023.1123894
Received: 14 December 2022; Accepted: 24 January 2023;
Published: 13 February 2023.
Edited by:
Shoug Alashmali, King Abdulaziz University, Saudi ArabiaReviewed by:
Morteza Taheri, Imam Khomeini International University, IranCopyright © 2023 AlBlooshi, AlFalasi, Taha, El Ktaibi and Khalid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sharifa AlBlooshi,  c2hhcmlmYS5hbGJsb29zaGlAenUuYWMuYWU=
c2hhcmlmYS5hbGJsb29zaGlAenUuYWMuYWU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.