 Aboma Motuma1Tesfaye Gobena2Kedir Teji Roba1Yemane Berhane3Alemayehu Worku4Lemma Demissie Regassa5Abebe Tolera5*
Aboma Motuma1Tesfaye Gobena2Kedir Teji Roba1Yemane Berhane3Alemayehu Worku4Lemma Demissie Regassa5Abebe Tolera5*- 1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 2Department of Environmental Health Science, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 3Department of Epidemiology and Biostatics, Addis Continental Institute of Public Health, Addis Ababa, Ethiopia
- 4Department of Epidemiology and Biostatistics, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia
- 5School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Background: Both hypertension (HTN) and diabetes are public health concerns in low- and middle-income countries, particularly in sub-Saharan African countries. The co-occurrence of HTN and diabetes is associated with an increased risk of mortality, morbidity, and reduced productivity in the working force. In Ethiopia, there is limited evidence on the co-occurrence of HTN and type 2 diabetes (T2DM). Therefore, this study was conducted to assess the co-occurrence of HTN and T2DM and their associated factors among Haramaya University employees in Eastern Ethiopia.
Methods: A cross-sectional survey was conducted among 1,200 employees at Haramaya University using a simple random sampling technique from December 2018 to February 2019. Demographic and behavioral factors were collected on a semi-structured questionnaire, followed by measurement of anthropometry and blood pressure. Blood glucose and lipid profile measurements were performed by collecting 6 ml of venous blood samples after 8 h of overnight fasting. Data were entered into EpiData 3.1 version and analyzed using Stata 16 software. Bivariable and multivariable logistic regressions were applied to observe the association between independent variables with co-occurrence of HPN and T2DM using odds ratio, 95% confidence interval (CI), and p-values of ≤ 0.05 were considered statistically significant.
Results: The prevalence of HTN and T2DM was 27.3 and 7.4%, respectively. The co-occurrence of HTN and T2DM was 3.8%. The study found that being older (AOR = 3.97; 95 % CI: 1.80–8.74), khat chewing (AOR = 2.76; 95 % CI: 1.23–6.18), body mass index ≥ 25 kg/m2 (AOR = 5.11; 95 % CI: 2.06–12.66), and sedentary behavior ≥8 h per day (AOR = 6.44; 95 % CI: 2.89–14.34) were statistically associated with co-occurrence of HTN and T2DM. On the other hand, consuming fruits and vegetables (AOR = 0.10; 95 % CI: 0.04–0.22) and a higher level of education (AOR = 0.39; 95% CI: 0.17–0.89) were negatively statistically associated with the co-occurrence of HTN and T2DM.
Conclusion: The co-occurrence of HTN and T2DM was prevalent among the study participants. This may create a substantial load on the healthcare system as an end result of increased demand for healthcare services. Therefore, rigorous efforts are needed to develop strategies for screening employees to tackle the alarming increase in HTN and T2DM in university employees.
Introduction
Non-communicable diseases (NCDs) are the primary causes of morbidity and mortality globally. It causes 41 million death each year, equivalent to 71% of all deaths globally (1, 2). Almost 75% of all disease deaths and 82% of the 16 million people who died prematurely or before reaching 70 years of age occur in low- and middle-income countries (3) including 39.3% in Ethiopia (4).
Hypertension (HTN) and diabetes (DM) are global public health problems (5). They have been confirmed as two of the major risk factors for cardiocerebrovascular diseases as leading causes of death and disability among adults (6). It has been found that individuals with both HTN and DM have a greater risk of cardiocerebrovascular disease than those with only one condition (7). Hypertension (HTN) and DM are also the challenges of the healthcare system in low- and middle-income countries (8), due to changes in their diet habits and lifestyle and increased sedentary behavior (9, 10). Hypertension (HTN) and DM share common comorbidities and risk factors (11). Complications related to HTN and DM are reduced quality of life and productivity (12), such as the increased risk of stroke (13), cardiovascular diseases, end-stage renal disease (14, 15), retinopathy, depression, impaired health-related quality of life, and increased healthcare costs (16–18).
The coexistence of HTN and type 2 diabetes (T2DM) has been documented in previous studies (19, 20). Epidemiological studies have documented that DM predisposes to HTN (16, 17). For instance, a study in the USA showed that up to 75% of adults with diabetes also have hypertension (21), and in China, ~15 million people have both HTN and DM (22).
In Ethiopia, about 1.7 million cases and 23,157 deaths were related to DM in 2019 (23). Moreover, evidence shows that the pooled prevalence of HTN was 21.8%, which was the highest prevalence reported in Addis Ababa at 25.4% and the lowest in the Tigray region at 15.4% (24). In Ethiopia, reports indicate that among university employees and civil servants in Addis Ababa, the prevalence of HTN was 13.9 and 27.3%, respectively (25, 26). Similarly, studies showed that DM among university employees and governmental civil servants at Guji Zone was 4.7 and 3.9%, respectively (25, 26). Moreover, studies showed that co-occurrence of HTN and T2DM accounted for ~40–75% of patients (27).
Although the co-occurrence of HTN and T2DM is believed to be prevalent among university employees in Ethiopia, there is limited evidence. Therefore, this study aimed to assess the co-occurrence of HTN and T2DM among university employees in Eastern Ethiopia.
Materials and methods
Study area
This study was conducted among Haramaya University employees from December 2018 to February 2019. Haramaya University is located ~510 kilometers east of Addis Ababa, Ethiopia. The university has ~7,176 employees, 28.1% women and 71.9% men. In terms of job mix, 21.1% of the staff are academic and the other 78.9% are grouped under technical and administrative staff.
Study design and period
An institutional-based cross-sectional study was conducted among 1,200 university employees who were randomly selected. The study participants in the age range of 18 to 65 years and who were working for at least 6 months were included. Self-declared physical disability and pregnant women were excluded from the study. A single population proportion formula was used to calculate the sample size using OpenEpi 3.1. based on a previous study in China (22); double burdens of hypertension and T2DM were estimated as 3.8% with a 95% confidence level (the critical value Zα/2 = 1.96), a 2% margin of error, and a 10% non-response rate. Finally, a total of 1,200 study participants were recruited. The sample was drawn using simple random sampling techniques based on the proportion to the size of their respective departments using the payroll roster as the sampling frame.
Data collection and tools (questionnaire)
Data were collected by trained nurses and laboratory technicians using a structured questionnaire adapted from the WHO STEPS, through face-to-face interviews, physical measurements, and biochemical tests. A pre-test was conducted on 5% of the final sample size at another nearby public university. Data collectors were trained on how to conduct interviews, anthropometric measurements, and field data collection procedures before directing them to gather data needed from data providers. Then, study participants were appointed on the next day morning in fasting condition to collect blood samples at the university clinics by trained medical laboratory technologists. The field research supervisors closely supervised the data collection process and checked the completeness and accuracy of the filled data on a daily basis. A field guide and data collection manual were used as a reference during the training. Standard operating procedures (SOP) were followed starting from the sample collection up to reporting of the result.
Variables and measurements
The dependent variable is the co-occurrence of hypertension and T2DM. Blood pressure was measured using a digital measuring device (Microlife BP A50, Microlife AG, Switzerland) with participants sitting after resting for at least 10 min. Then, three times blood pressure measurements were taken in an interval of at least 5 min between consecutive measurements. In doing so, the mean systolic and diastolic BP from the second and third measurements was analyzed and diagnosed as hypertension when the mean systolic and diastolic blood pressure was greater or equal to 140/90 mm Hg (28). To determine blood glucose level and lipid profile, 6 ml of venous blood samples was collected from the participant's antecubital arm in a seating position after 8 h of overnight fasting. The collected samples were then directed into the sterile vacuum tube (Gel Clot Activator) and placed on the rack for 10–20 min for clotting formation.
The specimen tubes were then centrifuged at 3,000 revolutions per minute to extract the serum from the whole blood; fasting serum triglyceride and blood sugar were analyzed using the standard enzymatic colorimetric method (HUMAN Gesellschaft fur Biochemica und Diagnostica mbH Max-Planck-Ring, Germany), while HDL-c was analyzed using direct homogenous standard enzymatic assay colorimetric test (HUMAN Gesellschaft fur Biochemica und Diagnostica mbH Max-Planck-Ring, Germany) (29). Lipid profile and fasting blood glucose concentrations were reported in mg/dL (30). The prevalence of T2DM was defined as fasting blood glucose of ≥126 mg/dl or a self-reported diagnosis of diabetes (31).
Smoking status was categorized as never-smoking, current smoking (at least one cigarette per week), and former smoking (quit smoking more than 12 months) (32, 33). Current drinkers were those who drank once or more in the prior month of data collection. The habit of using Khat (Catha edulis) was grouped into never, occasional, and habitual (frequent). The total physical activity score was computed as the sum of all metabolic equivalent (MET)-minutes per week for vigorous-intensity physical activity, moderate-intensity physical activity, and walking. The sum of MET-minutes per week was categorized as high (3,000 MET-minutes or above), moderate (between 2,999 and 600 MET-minutes), and low (< 600 MET-minutes).
Anthropometric data (weight, height, waist, and hip circumference) were collected according to the WHO STEPS manual (28). A BMI of ≥25.0 was defined as overweight/obese according to the WHO STEPS (31). Waist circumference was measured midway between the costal margin and the iliac crest with a tape line (31).
Statistical analysis
Data were double-entered into EpiData version 3.1 and cleaned, coded, and then transferred to STATA version 16 for analysis. The data were checked for missing values and outliers. The magnitude of hypertension, T2DM, and co-occurrence were summarized using proportion and frequency. A binary logistic regression model was used to determine factors associated with the co-occurrence of hypertension and T2DM. Information criteria (AIC/BIC) were used to select the final optimal model. The multicollinearity was checked using a scatter matrix and VIF. Interaction between variables was also checked, and the effect of omitted variable effect was tested using “ovtest.” Model fitness was checked with Hosmer–Lemeshew test, overall model statistics were checked with “fitstat” command, and the p-value of the Hosmer–Lemeshew was found to be 0.25. The magnitude of variables with a p-value of < 0.25 in bivariate analysis results obtained were taken for the multivariable analysis. Associations between outcome variables and covariates were reported with an adjusted odds ratio with a 95% confidence interval, and finally, statistical significance was considered at a p-value of < 0.05.
Results
Socio-demographic characteristics of the study participants
A total of 1,200 employees were enrolled, with 1,164 providing data, resulting in a 97% response rate. The majority of study participants were men, 598 (51.4%) resulting in a sex ratio of 1:1.06. The mean age of the study participants was 35 (±9.4 SD) years, with a range of 20–60 years. In the majority of the study participants, 755 (64.9%) were non-office workers and 739 (63.5%) attended college and above education level. The mean reported per capita annual income of participants was 1,05,059.1 (±49,960.38 SD) (Table 1). Nearly 37 and 33% of study participants had high total cholesterol and triglyceride level.
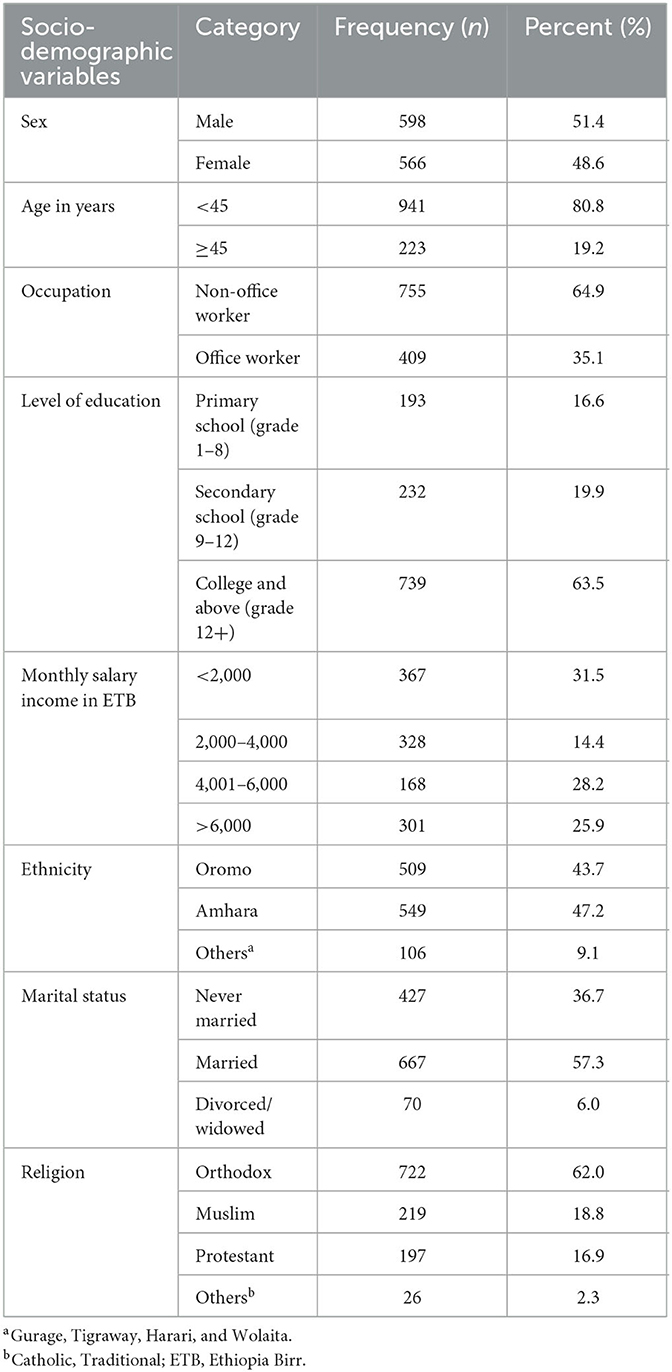
Table 1. Socio-demographic characteristics of civil servants of Haramaya University in Eastern Ethiopia, 2019 (n = 1,164).
Approximately half of the study participants, 571 (49.1%), had low physical activity and, 561 (48.25), were alcohol consumers. Moreover, 396 (34.5) were khat chewers, and 413 (35.5%) were overweight/obese. In addition, 131 (11.3) of the study participants were ever smokers. Table 2 shows details of the anthropometric, biochemical, and lifestyle characteristics of the subjects.
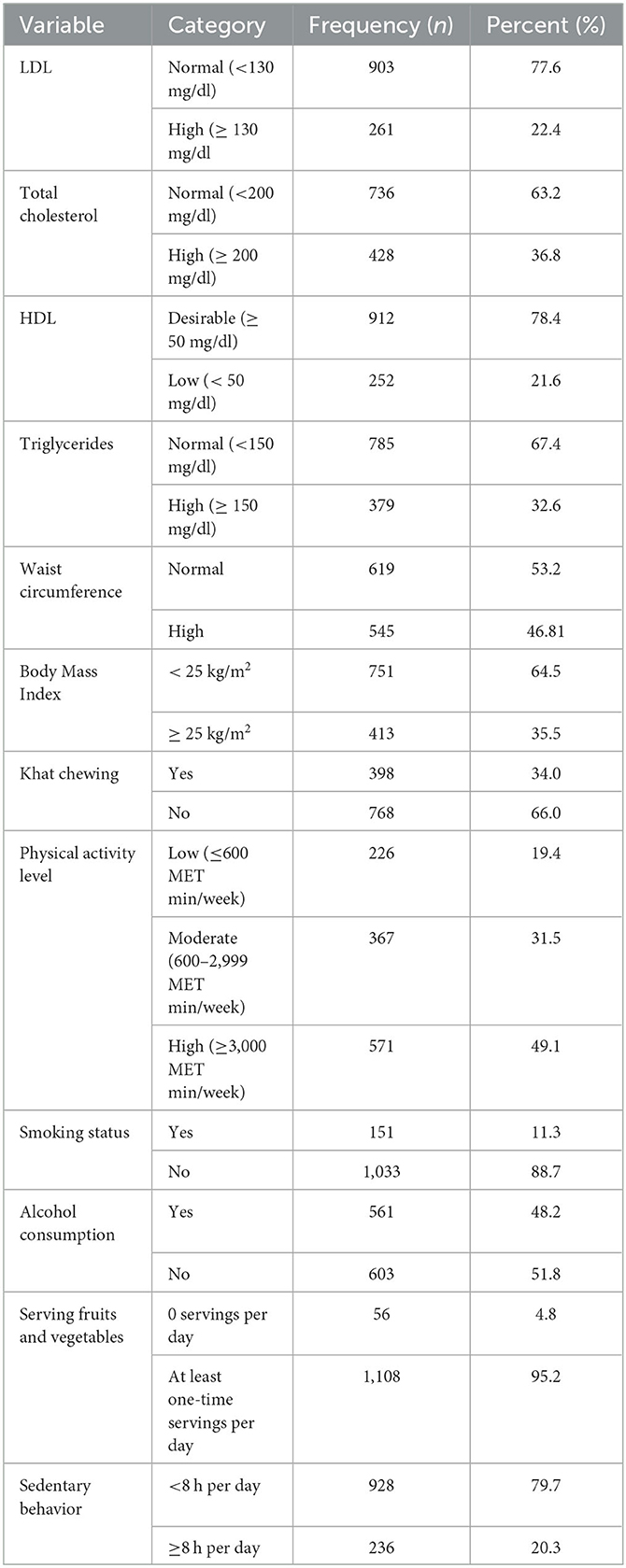
Table 2. Biochemical, anthropometric, and lifestyle characteristics of the study participants of Haramaya University employees, Eastern Ethiopia, 2019 (1,164).
The prevalence of HTN and T2DM
The mean systolic and diastolic blood pressure were 124.4 (±16.6SD) mmHg and 79.5 (±10.5SD) mmHg, respectively. The overall prevalence of HTN was 290 (27.3 %); of which, 128 (28.3 %) were women and 162 (27.1 %) were men. Of these, 246 (21.1 %) were previously unknown that they had hypertension, and only 44 (3.8%) were known hypertensive individuals. The mean and highest values of fasting blood glucose were 87.69 (±29.62SD) mg/dL and 341 g/dL, respectively. This study shows that the overall prevalence of T2DM (≥ 126 mg/dL) after overnight fasting was 86 (7.4 %); of which, 40 (7.1 %) were women and 46 (7.7 %) were men. From these, 2.3% were known T2DM individuals and 5.1% were individuals with undiagnosed T2DM.
Co-occurrence of HTN and T2DM and associated factors
Of the total study participants, 44 (3.8%) had both HTN and T2DM. Of these, 4.5% who had co-occurrence of HTN and T2DM were men (Figure 1).
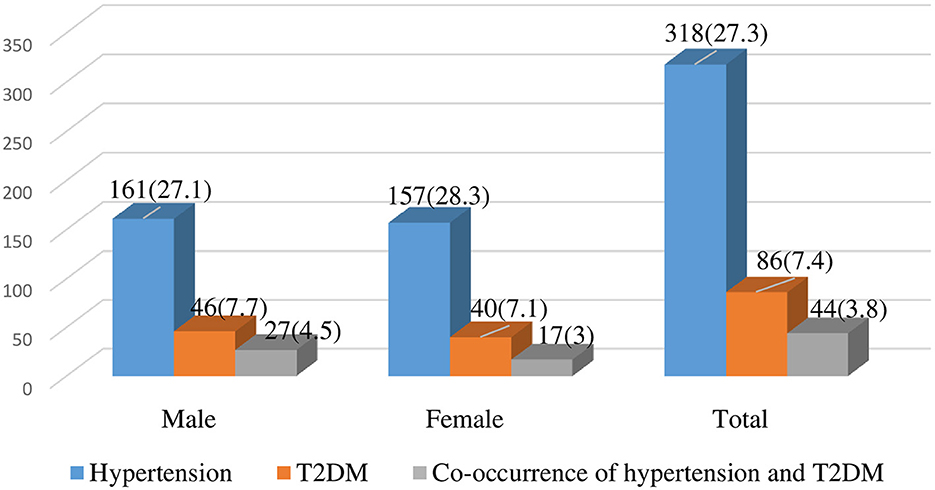
Figure 1. The prevalence of HTN, T2DM, and co-occurrence of HTN and T2DM among Haramaya University employees, Eastern Ethiopia, 2019.
In multivariable logistic regression analysis, age, intake of fruits and vegetables, khat chewing, educational status, BMI, and sedentary behavior were significantly associated with the co-occurrence of HTN and T2DM.
Participants aged 45 years and above were almost four times more likely to have the co-occurrence of HTN and T2DM compared to participants aged younger than 45 years. Employees who attended college and above were 61% less likely to have the co-occurrence of HTN and T2DM than those who attended less than or equal to secondary school. Khat chewers were nearly three times more likely to have the co-occurrence of HTN and T2DM as compared to non-khat chewers. Moreover, the odds of co-occurrence of HTN and T2DM were five times higher among those whose BMI was >25 kg/m2 compared with those whose BMI was < 25 kg/m2. Similarly, the odds of co-occurrence of HTN and T2DM among participants having a sedentary lifestyle was approximately 6 times higher than those who do not live a sedentary life. On the other hand, study participants who had servings of fruits and vegetables at least once per day were 90% less likely to have co-occurrence of HTN and T2DM as compared to those who did not consume servings of fruits and vegetables (Table 3).
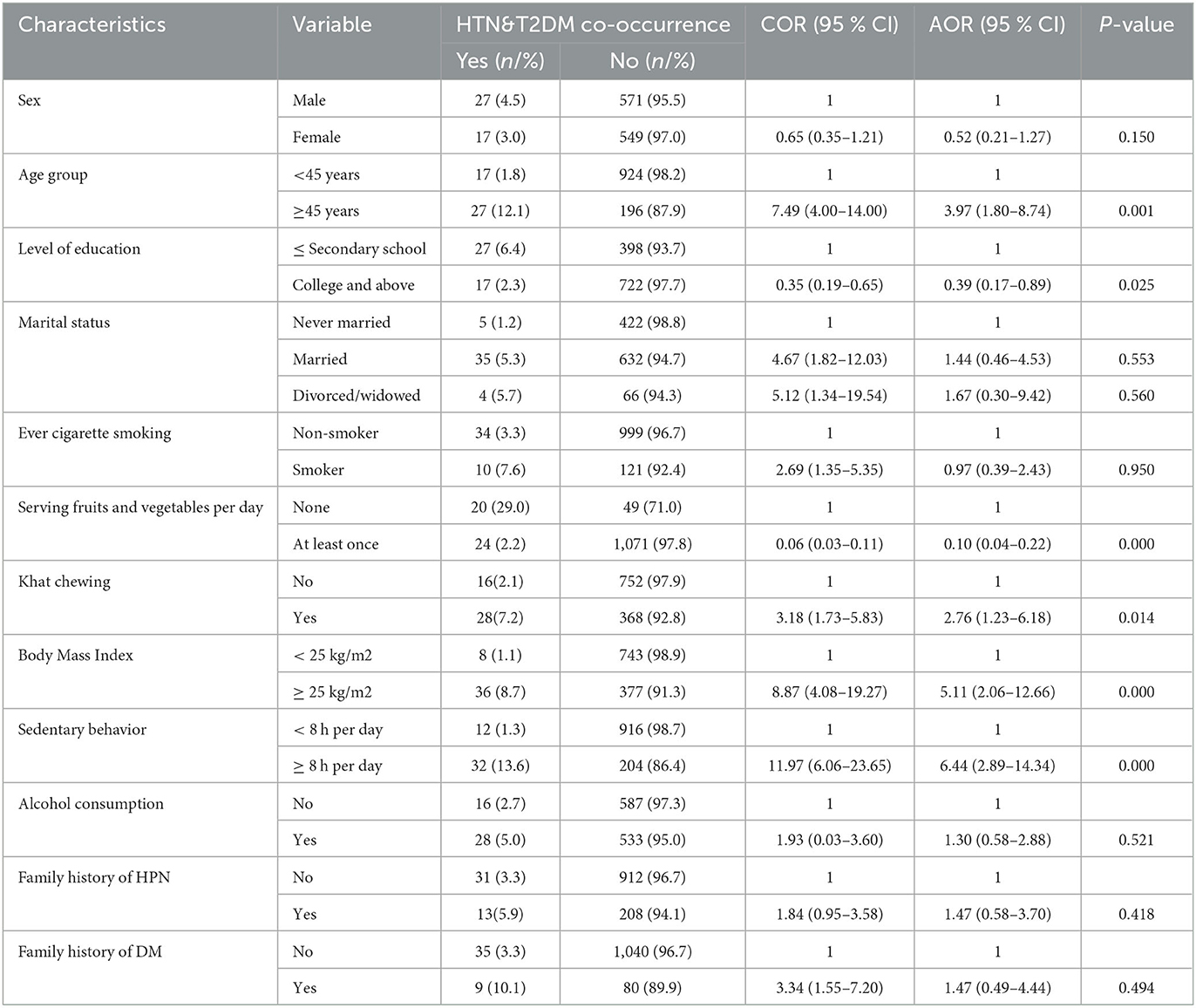
Table 3. Factors associated with co-occurrence of hypertension and type 2 diabetes among Haramaya University employees, Eastern Ethiopia, 2019 (n = 1,164).
Discussion
This study found the overall prevalence of HTN, T2DM, and co-occurrence of HTN and T2DM were 27, 8, and 4%, respectively. Co-occurrence of HTN and T2DM was significantly increased with advanced ages, body mass index >25 kg/m2, khat chewers, those with sedentary behaviors, and a higher level of education, while co-occurrence of HTN and T2DM was significantly lower among individuals those who reported consuming one or more servings of fruits and vegetables per day.
In this study, more than one in four employees had HTN. This finding is consistent with a study conducted in Wollo, North Ethiopia (34); Sidama, South Ethiopia (35); and Debre Birhan, North Ethiopia (36); and Addis Ababa, Ethiopia (25). However, the finding of this study is higher than that of the study conducted in Wolaita, Southern Ethiopia (37); Hawassa, Southern Ethiopia (38); and Togo (39). This may be due to the difference in study participant characteristics and study setting. For instance, our study population is university employees, whereas the others included working adults. In addition, the high prevalence of hypertension in our study could be due to a more sedentary lifestyle, increased pressure from the high workload, and changes in dietary patterns (40). However, the finding of this study is lower than study in Southern (41), northwestern (42) and northern Ethiopia (43), southern Nigeria (44) and Bangladeshi (45). This difference may be due to the sample size and setting of the study. Changing nutritional intake combined with increasingly sedentary lifestyles was reported to increase the emergence of chronic diseases such as hypertension in developing countries (9, 10).
Similarly, ~8% of the study participants were found to have T2DM. This is consistent with the study conducted in northern Ethiopia (43) and Addis Ababa (46), but the percentage of prevalence was higher than the study conducted in southern Nigeria (44) and Taiwan (47). This may be due to a high level of physical inactivity and poor consumption of fruits and vegetables in the study area and an unhealthy diet due to the entry site of a processed and packed diet. However, this finding is lower than the percentage of prevalence found in eastern Sudan (48) and north Sudan (49), Spain (50), and France (51). This may be due to working types and conditions, income, and educational status in urban centers of high-income countries that predispose them to stay home, consume unhealthy diets, and have multiple behavioral risk factors.
This study showed that ~4% of the study participants had both HTN and T2DM. This finding is consistent with studies conducted in Bangladesh (19) and China (22). This finding coincides with the fact that the lifestyle of working adults in Ethiopia has radically changed in the last decade due to the changing working environment, concentration of the middle-aged population, urban dwellers, risk of sedentarism, less physical activities in the workplace, better access to technology, and leisure lifestyle status. However, this finding is lower than the percentage of prevalence found in Ghana (52) and the USA (53). This difference may be due to the study units used (public employees in this study and any adult in the other two studies) and other socio-demographic and dietary patterns of the study population. Accumulating evidence has shown that hypertension affects the majority of individuals with diabetes mellitus which dramatically increases the risk of morbidity and mortality from cardiovascular disease (54, 55). The co-existence of HTN and T2DM is a major contributor to the development and progression of microvascular and macrovascular complications, which in turn complicates the treatment strategy and increases healthcare costs.
This study showed that advanced age was significantly associated with the co-occurrence of HTN and T2DM. This finding is consistent with studies conducted in North Wollo Zone, Amhara Region (34); Wolaita Zone, Southern Ethiopia (37); Northwest Ethiopia (42) and Southern Ethiopia (38); Sidama Zone, South Ethiopia (35); and Ghana (56) where older age or advance in age is found to increase the risk of hypertension and/or diabetes. Over-abundant food consumption combined with a more sedentary lifestyle among older people mostly accounts for the increase in chronic non-communicable diseases (57, 58).
This study demonstrates that the co-occurrence of HTN and T2DM was 61% lower among public servants with a college and above education level. Consistent with this finding, studies showed that people who have a low socioeconomic status have a higher risk of non-communicable diseases (NCDs) than more advantaged groups. Social inequalities accounted for more than half of inequalities in major NCDs (59–61). Being educated is more effective in reducing unhealthy diet, substance use, physical inactivity, and better access to healthcare for timely diagnosis and treatment (62).
Study participants who chew khat were approximately three times more likely to have the co-occurrence of HTN and T2DM as compared to non-khat chewers. This finding is consistent with a study conducted in Southern Ethiopia (35) and Southwest Ethiopia (63), which indicates that the risk of either hypertension or diabetes was increased among people who chewed khat. Evidence shows that khat chewing has a significant effect on increasing fasting plasma glucose (64) and mean blood pressure (65).
Similarly, our study showed that employees who had sedentary behavior (≥8 h per day) are more likely to have the co-occurrence of HTN and T2DM than their counterparts. This finding is consistent with studies conducted in Southern Ethiopia (41) and China (66). Insufficient physical activity is one important cause of most chronic diseases and results in substantial disease in quality of life (67, 68). Physical activity primarily prevents or delays chronic diseases. Preventing sedentary behavior with increased promotion of physical activity needs to be part of any healthcare system. BMI≥25 Kg/m2 was among the modifiable risk factors found to increase co-occurrence of HTN and T2DM in this study. Similar studies in Ethiopia showed BMI≥25 Kg/m2 or being overweight or obese (35, 36, 38, 69) increased the risk of HTN or diabetes or both. This finding is also consistent with a study by Tseng where “BMI/obesity is significantly linked to blood pressure/hypertension throughout the range of BMI in diabetic patients in either sex regardless of a previous hypertension history” (70). Dietary mediators seem to play a significant role in the pathogenesis of cardiovascular disease, among different socioeconomic layers (71).
In this study, study participants who had servings of fruits and vegetables at least once per day were less likely to have both HTN and T2DM as compared to their counterparts who do not consume servings of fruits and vegetables. A study conducted in Ghana (56) showed high fruit intake was associated with a lower risk of hypertension. Several studies showed that unhealthy diets and physical inactivity are well-recognized modifiable behavioral risk factors for NCDs (72–74). Studies showed that the majority of cardiovascular diseases can be attributed to major risk factors, such as low intake of fruits and vegetables rather than consuming more foods that are nutritionally poor and consuming energy-dense foods high in sugar and/or saturated fats or excessively salty (22). People with type 2 diabetes are encouraged to optimize dietary patterns to reduce their risk for cardiovascular diseases, such as diabetes and related comorbidities (75). This study revealed very critical evidence on the co-occurrence of HTN and T2DM, which can be very useful for policymakers in low- and middle-income countries for early interventions to limit the pace of such non-communicable diseases.
Limitations and strengths of the study
The limitation of this study is reliance on self-reporting, which contributes to recall and social desirability bias that potentially underestimates behavioral factors. This study may not be generalizable to all employees in Eastern Ethiopia as the study population was drawn only from one institution. However, the strengths of this study include large sample size and a standardized questionnaire based on World Health Organization's (WHO) STEP approach to collect data. Moreover, this study was the first of its kind among university employees in Ethiopia and can be fairly generalized for this category of workers in areas where there are contextual working adults.
Conclusion
Approximately 4% of Haramaya University employees had co-occurrence of HTN and T2DM. Factors associated with the co-occurrence of HTN and T2DM were older age, overweight/obesity, sedentary behavior, higher level of education, consumption of khat, and less intake of fruits and vegetables. These findings call for the health promotion interventional strategies targeting the aforementioned determinants. Increasing awareness of controlled consumption of “khat,” lifestyle modifications, and strengthening job periodic screening programs of high-risk populations are recommended.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Institutional Health Research Ethics Review Committee (Ref. No. IHRERC/196/2018) of Haramaya University, College of Health and Medical Sciences. The patients/participants provided their written informed consent to participate in this study.
Author contributions
AM conceived the study and drafted the proposal. AT, AM, and LR had substantial contributions to the study design and development of the data collection checklist and drafted, wrote, and corrected the manuscript. All authors read the manuscript and approved it.
Funding
Haramaya University provided the financial support for this study. But the funding agency had no role in the collection, analysis, and interpretation of the data as well as the writing of the manuscript.
Acknowledgments
We would like to thank all of the staff at Haramaya University for providing organizational support. We would like to extend our appreciation to all of our data collectors and supervisors. Finally, we would like to acknowledge Haramaya University for funding this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO. Noncommunicable Diseases. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed January 29, 2022).
2. Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Global Health. (2019) 7:e1295–6. doi: 10.1016/S2214-109X(19)30370-5
3. Zenu S, Abebe E, Dessie Y, Debalke R, Berkessa T, Reshad M. Co-occurrence of behavioral risk factors of non-communicable diseases and social determinants among adults in urban centers of Southwestern Ethiopia in 2020: a community-based cross-sectional study. J Multidiscip Healthc. (2021) 14:1561. doi: 10.2147/JMDH.S313741
4. Girum T, Mesfin D, Bedewi J, Shewangizaw M. The Burden of Noncommunicable Diseases in Ethiopia, 2000–2016: analysis of evidence from global burden of disease study 2016 and global health estimates 2016. Int J Chronic Dis. (2020) 2020:3679528. doi: 10.1155/2020/3679528
5. Roglic G, WHO. Global report on diabetes: a summary. Int J Noncommun Dis. (2016) 1:3. doi: 10.4103/2468-8827.184853
6. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. (2012) 380:2224–60. doi: 10.1016/S0140-6736(12)61766-8
7. Sunkara N, Ahsan CH. Hypertension in diabetes and the risk of cardiovascular disease. Cardiovasc Endocrinol. (2017) 6:33. doi: 10.1097/XCE.0000000000000114
8. Larejani B, Zahedi F. Epidemiology of diabetes mellitus in Iran. ijdld. (2001) 1:1–8. Available online at: http://ijdld.tums.ac.ir/article-1-490-en.html
9. Grosso G. Impact of nutritional risk factors on chronic non-communicable diseases. Eur J Public Health. (2019) 29(Suppl. 4):ckz185–197. doi: 10.1093/eurpub/ckz185.197
10. Di Cesare M. Global trends of chronic non-communicable diseases risk factors. Eur J Public Health. (2019) 29(Suppl. 4):ckz185–196. doi: 10.1093/eurpub/ckz185.196
11. Channanath AM, Farran B, Behbehani K, Thanaraj TA. State of diabetes, hypertension, and comorbidity in Kuwait: showcasing the trends as seen in native versus expatriate populations. Diabetes Care. (2013) 36:e75–e75. doi: 10.2337/dc12-2451
12. Tesfaye B, Alebel A, Gebrie A, Zegeye A, Leshargie CT, Ferede A, et al. Diabetes mellitus and its association with hypertension in ethiopia: a systematic review and meta-analysis. Diabetes Res Clin Pract. (2019) 156:107838. doi: 10.1016/j.diabres.2019.107838
13. Alloubani A, Saleh A, Abdelhafiz I. Hypertension and diabetes mellitus as a predictive risk factors for stroke. Diab Metabol Synd Clin Res Rev. (2018) 12:577–84. doi: 10.1016/j.dsx.2018.03.009
14. Ye N, Jardine MJ, Oshima M, Hockham C, Heerspink HJL, Agarwal R, et al. Blood pressure effects of Canagliflozin and clinical outcomes in type 2 diabetes and chronic kidney disease : insights from the CREDENCE trial. Circulation. (2021) 143:1735–49. doi: 10.1161/CIRCULATIONAHA.120.048740
15. Singal AK, Hasanin M, Kaif M, Wiesner RW, Kuo Y-F, MELD. Stratified outcomes among recipients with diabetes or hypertension. J Clin Gastroenterol. (2018) 52:67–72. doi: 10.1097/MCG.0000000000000818
16. Jia G, Sowers JR. Hypertension in diabetes: an update of basic mechanisms and clinical disease. Hypertension. (2021) 78:1197–205. doi: 10.1161/HYPERTENSIONAHA.121.17981
17. Ferrannini E, Cushman WC. Diabetes and hypertension: the bad companions. Lancet. (2012) 380:601–10. doi: 10.1016/S0140-6736(12)60987-8
18. Levin G, Kestenbaum B, Ida Chen YD, Jacobs DR Jr, Psaty BM, Rotter JI, et al. Glucose, insulin, and incident hypertension in the multi-ethnic study of atherosclerosis. Am J Epidemiol. (2010) 172:1144–54. doi: 10.1093/aje/kwq266
19. Kibria GMA, Hashan MR, Hossain MM, Zaman SB, Stennett CA. Clustering of hypertension, diabetes and overweight/obesity according to socioeconomic status among Bangladeshi adults. J Biosoc Sci. (2021) 53:157–66. doi: 10.1017/S0021932020000085
20. Hertz JT, Sakita FM, Manavalan P, Madut DB, Thielman NM, Mmbaga BT, et al. The burden of hypertension and diabetes in an emergency department in Northern Tanzania. Ethn Dis. (2019) 29:559–66. doi: 10.18865/ed.29.4.559
21. Long AN, Dagogo-Jack S. Comorbidities of diabetes and hypertension: mechanisms and approach to target organ protection. J Clin Hypertens. (2011) 13:244–51. doi: 10.1111/j.1751-7176.2011.00434.x
22. Wang Z, Hanlin TY. Prevalence of diabetes and hypertension and their interaction effects on cardiocerebrovascular diseases: a cross-sectional study BMC Public Health. (2021) 21:1224. doi: 10.1186/s12889-021-11122-y
23. Kotiso KS, Degemu N, Gebremedhin S, Taye M, Petros A, Belayneh F, et al. Determinants of hypertension among patients with type 2 diabetes mellitus on follow-up at Tikur Anbessa Specialized Hospital, Addis Ababa: a case-control study. PLoS ONE. (2021) 16:e0256399. doi: 10.1371/journal.pone.0256399
24. Tiruneh SA, Bukayaw YA, Yigizaw ST, Angaw DA. Prevalence of hypertension and its determinants in Ethiopia: a systematic review and meta-analysis. PLoS ONE. (2020) 15:e0244642. doi: 10.1371/journal.pone.0244642
25. Angaw K, Dadi AF, Alene KA. Prevalence of hypertension among federal ministry civil servants in Addis Ababa, Ethiopia: a call for a workplace-screening program. BMC Cardiovasc Disord. (2015) 15:76. doi: 10.1186/s12872-015-0062-9
26. Janakiraman B, Abebe SM, Chala MB, Demissie SF. Epidemiology of general, central obesity and associated cardio-metabolic risks among University Employees, Ethiopia: a cross-sectional study. Diab. Metabol. Synd. Obes. Targets Therapy. (2020) 13:343. doi: 10.2147/DMSO.S235981
27. Sowers JR, Epstein M, Frohlich ED. Diabetes, hypertension, and cardiovascular disease. Hypertension. (2001) 37:1053–9. doi: 10.1161/01.HYP.37.4.1053
28. Riley L, Guthold R, Cowan M, Savin S, Bhatti L, Armstrong T, et al. The World Health Organization STEPwise approach to noncommunicable disease risk-factor surveillance: methods, challenges, and opportunities. Am J Public Health. (2016) 106:74–8. doi: 10.2105/AJPH.2015.302962
30. World Health O. Laboratory Quality Management System: Handbook. Geneva: World Health Organization (2011).
31. WHO. WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance. Geneva: World Health Organization (2005).
32. Sohn S, Savova GK. Mayo clinic smoking status classification system: extensions and improvements. AMIA Annu Symp Proc. (2009) 2009:619–23.
33. CDC. U.S. Department of Health & Human Services. Center for Disease prevention and Control (CDC), Special Topics: Adult Tobacco Use Information. National Center for Health Statistics. (2017). Available online at: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm#print (accessed June 2019).
34. Gedamu DK, Sisay W. Prevalence of hypertension and associated factors among public servants in North Wollo Zone, Amhara Region, Ethiopia, 2020. Vasc Health Risk Manag. (2021) 17:363. doi: 10.2147/VHRM.S298138
35. Badego B, Yoseph A, Astatkie A. Prevalence and risk factors of hypertension among civil servants in Sidama Zone, south Ethiopia. PLoS ONE. (2020) 15:e0234485–e0234485. doi: 10.1371/journal.pone.0234485
36. Geset Haile D, Sharew NT, Mekuria AD, Abebe AM, Mezemir Y. Prevalence of hypertension and associated factors among adults in Debre Berhan Town, North Shoa Zone, Ethiopia, 2020. Vasc Health Risk Manag. (2021) 17:203–10. doi: 10.2147/VHRM.S297403
37. Anjulo U, Haile D, Wolde A. Prevalence of hypertension and its associated factors among adults in Areka Town, Wolaita Zone, Southern Ethiopia. Integr Blood Press Control. (2021) 14:43–54. doi: 10.2147/IBPC.S295574
38. Wachamo D, Geleta D, Woldesemayat EM. Undiagnosed hypertension and associated factors among adults in Hawela Tula Sub-City, Hawassa, Southern Ethiopia: a community-based cross-sectional study. Risk Manag Healthc Policy. (2020) 13:2169–77. doi: 10.2147/RMHP.S276955
39. Damorou F, Togbossi E, Pessinaba S, Soussou B. [Epidemiology and diagnostic circumstances of arterial hypertension in the hospital environment in Kpalime (second largest city in Togo)]. Mali Med. (2008) 23:17–20.
40. Motuma A, Gobena T, Roba KT, Berhane Y, Worku A. Sedentary behavior and associated factors among working adults in Eastern Ethiopia. Front Public Health. (2021) 9:1252. doi: 10.3389/fpubh.2021.693176
41. Kebede B, Ayele G, Haftu D, Gebremichael G. The prevalence and associated factors of hypertension among adults in Southern Ethiopia. Int J Chronic Dis. (2020) 2020:8020129–8020129. doi: 10.1155/2020/8020129
42. Abebe SM, Andargie G, Shimeka A, Alemu K, Kebede Y, Wubeshet M, et al. The prevalence of non-communicable diseases in northwest Ethiopia: survey of Dabat health and demographic surveillance system. BMJ Open. (2017) 7:e015496. doi: 10.1136/bmjopen-2016-015496
43. Gebremariam LW, Chiang C, Yatsuya H, Hilawe EH, Kahsay AB, Godefay H, et al. Non-communicable disease risk factor profile among public employees in a regional city in northern Ethiopia. Sci Rep. (2018) 8:9298. doi: 10.1038/s41598-018-27519-6
44. Isara AR, Okundia PO. The burden of hypertension and diabetes mellitus in rural communities in southern Nigeria. Pan Afr Med J. (2015) 20:103. doi: 10.11604/pamj.2015.20.103.5619
45. Ali N, Akram R, Sheikh N, Sarker AR, Sultana M. Sex-specific prevalence, inequality and associated predictors of hypertension, diabetes, and comorbidity among Bangladeshi adults: results from a nationwide cross-sectional demographic and health survey. BMJ Open. (2019) 9:e029364. doi: 10.1136/bmjopen-2019-029364
46. Nshisso LD, Reese A, Gelaye B, Lemma S, Berhane Y, Williams MA. Prevalence of hypertension and diabetes among Ethiopian adults. Diabetes Metab Syndr. (2012) 6:36–41. doi: 10.1016/j.dsx.2012.05.005
47. Shih DP, Lin PY, Liang WM, Tseng PC, Kuo HW, Wang JY. Sleep duration and effort-reward imbalance (ERI) associated with obesity and type ii diabetes mellitus (T2DM) among Taiwanese middle-aged public servants. Int J Environ Res Public Health. (2020) 17:6577. doi: 10.3390/ijerph17186577
48. Omar SM, Musa IR, ElSouli A, Adam I. Prevalence, risk factors, and glycaemic control of type 2 diabetes mellitus in eastern Sudan: a community-based study. Ther Adv Endocrinol Metab. (2019) 10:2042018819860071. doi: 10.1177/2042018819860071
49. Eltom MA, Mohamed AHB, Elrayah-Eliadarous H, Yassin K, Noor SK, Elmadhoun WM, et al. Increasing prevalence of type 2 diabetes mellitus and impact of ethnicity in north Sudan. Diabetes Res Clin Pract. (2018) 136:93–9. doi: 10.1016/j.diabres.2017.11.034
50. Castañ-Abad MT, Montserrat-Capdevila J, Godoy P, Marsal JR, Ortega M, Alsedà M, et al. Diabetes as a risk factor for severe exacerbation and death in patients with COPD: a prospective cohort study. Eur J Public Health. (2020) 30:822–7. doi: 10.1093/eurpub/ckz219
51. Frison E, Proust-Lima C, Mangin J-F, Habert M-O, Bombois S, Ousset P-J, et al. Diabetes mellitus and cognition: pathway analysis in the MEMENTO cohort. Neurology. (2021) 97:e836–48. doi: 10.1212/WNL.0000000000012440
52. Atuahene M, Ganle JK, Adjuik M, Atuahene NF, Kampitib GB. Overweight and obesity prevalence among public servants in Nadowli district, Ghana, and associated risk factors: a cross-sectional study. BMC obesity. (2017) 4:15. doi: 10.1186/s40608-017-0153-5
53. Selby JV, Peng T, Karter AJ, Alexander M, Sidney S, Lian J, et al. High rates of co-occurrence of hypertension, elevated low-density lipoprotein cholesterol, and diabetes mellitus in a large managed care population. Am J Manag Care. (2004) 10:163–70.
54. Oktay AA, Akturk HK, Jahangir E. Diabetes mellitus and hypertension: a dual threat. Curr Opin Cardiol. (2016) 31:402–9. doi: 10.1097/HCO.0000000000000297
55. Holtrop J, Spiering W, Nathoe HM, De Borst GJ, Kappelle LJ, De Valk HW, et al. Apparent therapy-resistant hypertension as risk factor for the development of type 2 diabetes mellitus. J Hypertens. (2020) 38:45–51. doi: 10.1097/HJH.0000000000002227
56. Agongo G, Nonterah EA, Amenga-Etego L, Debpuur C, Kaburise MB, Ali SA, et al. Blood pressure indices and associated risk factors in a rural West African Adult population: insights from an AWI-Gen substudy in Ghana. Int J Hypertens. (2020) 2020:4549031–4549031. doi: 10.1155/2020/4549031
57. Suzman R, Beard JR, Boerma T, Chatterji S. Health in an ageing world—what do we know? Lancet. (2015) 385:484–6. doi: 10.1016/S0140-6736(14)61597-X
58. Ruthsatz M, Candeias V. Non-communicable disease prevention, nutrition and aging. Acta Bio Medica. (2020) 91:379. doi: 10.23750/abm.v91i2.9721
59. Di Cesare M, Khang Y-H, Asaria P, Blakely T, Cowan MJ, Farzadfar F, et al. Inequalities in non-communicable diseases and effective responses. Lancet. (2013) 381:585–97. doi: 10.1016/S0140-6736(12)61851-0
60. Oshio T, Kan M. Educational level as a predictor of the incidences of non-communicable diseases among middle-aged Japanese: a hazards-model analysis. BMC Public Health. (2019) 19:852. doi: 10.1186/s12889-019-7182-6
61. Marmot M, Bell R. Social determinants and non-communicable diseases: time for integrated action. BMJ. (2019) 364:l251. doi: 10.1136/bmj.l251
62. Singh A, Bassi S, Nazar GP, Saluja K, Park M, Kinra S, et al. Impact of school policies on non-communicable disease risk factors – a systematic review. BMC Public Health. (2017) 17:292. doi: 10.1186/s12889-017-4201-3
63. Abdissa D, Kene K. Prevalence and determinants of hypertension among diabetic patients in Jimma University Medical Center, Southwest Ethiopia, (2019). Diabetes Metab Syndr Obes. (2020) 13:2317–25. doi: 10.2147/DMSO.S255695
64. Mengistu Y, Dedefo G, Arkew M, Asefa G, Jebessa G, Atnafu A, et al. Effect of regular khat chewing on serum fasting sugar level in diabetic patients versus healthy individuals; a comparative study. Nutr Metab Insights. (2021) 14:11786388211035220. doi: 10.1177/11786388211035220
65. Damtie D, Bereket A, Bitew D, Kerisew B. The prevalence of hypertension and associated risk factors among secondary school teachers in Bahir Dar City Administration, Northwest Ethiopia. Int J Hypertens. (2021) 2021:5525802. doi: 10.1155/2021/5525802
66. Gao Y, Xie X, Wang S-X, Li H, Tang H-Z, Zhang J, et al. Effects of sedentary occupations on type 2 diabetes and hypertension in different ethnic groups in North West China. Diab Vasc Dis Res. (2017) 14:372–5. doi: 10.1177/1479164117696050
67. Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Comprehens Physiol. (2012) 2012:1143–211. doi: 10.1002/cphy.c110025
68. Booth FW, Roberts CK, Thyfault JP, Ruegsegger GN, Toedebusch RG. Role of inactivity in chronic diseases: evolutionary insight and pathophysiological mechanisms. Physiol Rev. (2017) 97:1351–402. doi: 10.1152/physrev.00019.2016
69. Shumye MW, Tegegne B, Ademe S, Workneh M, Abera M, Nemera G, et al. The magnitude of diabetes mellitus in adult hypertensive patients in Northeast Ethiopia. Diabetes Metab Syndr Obes. (2021) 14:37–45. doi: 10.2147/DMSO.S283158
70. Tseng CH. Body mass index and blood pressure in adult type 2 diabetic patients in Taiwan. Circ J. (2007) 71:1749–54. doi: 10.1253/circj.71.1749
71. Psaltopoulou T, Hatzis G, Papageorgiou N, Androulakis E, Briasoulis A, Tousoulis D. Socioeconomic status and risk factors for cardiovascular disease: impact of dietary mediators. Hellenic J Cardiol. (2017) 58:32–42. doi: 10.1016/j.hjc.2017.01.022
72. Li D. Effect of the vegetarian diet on non-communicable diseases. J Sci Food Agric. (2014) 94:169–73. doi: 10.1002/jsfa.6362
73. Popkin BM, Horton S, Kim S, Mahal A, Shuigao J. Trends in diet, nutritional status, and diet-related noncommunicable diseases in China and India: the economic costs of the nutrition transition. Nutr Rev. (2001) 59:379–90. doi: 10.1111/j.1753-4887.2001.tb06967.x
74. Ezzati M, Riboli E. Behavioral and dietary risk factors for noncommunicable diseases. N Engl J Med. (2013) 369:954–64. doi: 10.1056/NEJMra1203528
Keywords: co-occurrence, hypertension, diabetes mellitus, university employees, Ethiopia
Citation: Motuma A, Gobena T, Roba KT, Berhane Y, Worku A, Regassa LD and Tolera A (2023) Co-occurrence of hypertension and type 2 diabetes: prevalence and associated factors among Haramaya University employees in Eastern Ethiopia. Front. Public Health 11:1038694. doi: 10.3389/fpubh.2023.1038694
Received: 07 September 2022; Accepted: 19 June 2023;
Published: 11 July 2023.
Edited by:
Pranav Kumar Prabhakar, Lovely Professional University, IndiaReviewed by:
Chin-Hsiao Tseng, National Taiwan University, TaiwanSamson Duresso, University of Tasmania, Australia
Copyright © 2023 Motuma, Gobena, Roba, Berhane, Worku, Regassa and Tolera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abebe Tolera, komiintolera@gmail.com