 Luz M. Garcini1,2,3,4*
Luz M. Garcini1,2,3,4* Arlynn M. Ambriz2
Arlynn M. Ambriz2 Alejandro L. Vázquez5
Alejandro L. Vázquez5 Cristina Abraham6Vyas Sarabu2Ciciya Abraham6Autumn K. Lucas-Marinelli7Sarah Lill1Joel Tsevat1,2,8
Cristina Abraham6Vyas Sarabu2Ciciya Abraham6Autumn K. Lucas-Marinelli7Sarah Lill1Joel Tsevat1,2,8- 1Center for Research to Advance Community Health (ReACH), University of Texas Health Science Center at San Antonio, San Antonio, TX, United States
- 2Department of Medicine, Joe R. and Teresa Lozano Long School of Medicine, University of Texas Health Science Center at San Antonio, San Antonio, TX, United States
- 3Department of Psychiatry and Behavioral Sciences, Joe R. and Teresa Lozano Long School of Medicine, University of Texas Health Science Center at San Antonio, San Antonio, TX, United States
- 4Baker Institute Center for the United States and Mexico, Rice University, Houston, TX, United States
- 5Department of Psychology, Utah State University, Logan, UT, United States
- 6Department of Sciences, University of Texas at San Antonio, San Antonio, TX, United States
- 7Department of Psychology, Trinity University, San Antonio, TX, United States
- 8Department of Population Health and Internal Medicine, Dell Medical School, University of Texas, Austin, TX, United States
A critical step to reduce the spread of COVID-19 is vaccination. We conducted a mixed methods project that used online surveys and focus groups with 64 Community Health Workers and Promotor/as (CHW/Ps) located near the U.S.-Mexico border to identify barriers and facilitators to COVID-19 vaccination among Latino communities that have been historically underrepresented and medically underserved. Overall, personal barriers to vaccination included mistrust of manufacturers and administrators as well as fear of: becoming infected from the vaccine, discrimination/stigmatization from healthcare professionals administering the vaccine, exploitation/manipulation by the government or health authorities, and having personal information mishandled. Environmental and community barriers included being undocumented and fear-inducing myths and beliefs. Additional barriers included limited information and logistics pertaining to vaccination access. Targeted efforts are needed to overcome barriers in a culturally and contextually sensitive manner to prevent harm and reduce risk of infection among communities that have been historically underrepresented.
Introduction
The COVID-19 pandemic has disproportionately affected ethnic/racial underrepresented communities and has been particularly devastating for many Latino communities in the United States (U.S.) (1). According to the Centers for Disease Control and Prevention (CDC), Latinos in the U.S. are 1.5 times more likely to be infected with COVID-19 and 2.3 times more likely to be hospitalized for COVID-19 when compared to non-Latino Whites (2). In Texas, the U.S. state with the second largest Latino population (39.3% of the state's population) (3), Latinos represented 26.43% of all confirmed COVID-19 cases compared to 22.37% of Whites as of May 14, 2022 (4). Equally of concern is that when compared to non-Latino Whites, Latinos in the U.S. are 1.8 times more likely to die from COVID-19 (2). Latinos make up 583.2 of age-adjusted COVID-19 fatalities per 100,000 individuals in Texas, in comparison with only 309.0 fatalities per 100,000 for non-Latino Whites as of April 23, 2022 (5). The toll of COVID-19 among Latinos in the U.S. is also evident among younger Latinos, particularly those of working age (6). Indeed, estimates suggest that the Latino health advantage in all-cause mortality rates (a phenomenon known as the Latino paradox) is falling by over 70% due to COVID-19, a phenomenon that may persist beyond the current pandemic due to its related long-term health, social, and economic impacts (6).
An important way to control and end the COVID-19 pandemic is vaccination (7). To this end, equitable and sustainable vaccine administration requires identifying barriers to access and factors contributing to vaccine hesitancy among high risk groups, such as Latinos (8). According to the Kaiser Family Foundation, the current rate of at least one dose of the COVID-19 vaccine among Latinos in Texas is 65%, as of April 4, 2022, which is somewhat higher than the 54% vaccination rate among non-Latino White Americans and markedly higher than the 48% vaccination rate among African Americans (9). Asian Americans, meanwhile, have the highest vaccination rate at 75% (9). Barriers and facilitators to vaccination may differ across settings and populations depending on the contextual environment, available resources, and prevalent cultural myths, beliefs, and practices (10, 11).
Our current understanding of barriers to vaccination among Latino populations suggests four interconnected categories: (a) vaccine hesitancy among individuals and within communities, (b) inaccessibility of vaccine information, (c) structural issues relating to distribution and accessibility; and (d) concerns specific to certain groups within Latino communities, such as those of immigrant status (12–15). Many of the aforesaid barriers are rooted systemic inequalities in the healthcare system and cultural variations that disproportionately affect the health outcomes of Latino individuals (12).
Personal beliefs and concerns surrounding vaccination among Latinos often result in vaccine hesitancy (13), which prior research has attributed to historical mistreatment of racial and ethnic minority populations leading to lasting mistrust of the healthcare system (12), perceptions of limited vaccination supply in Latino communities (12), and vaccine misinformation (13). These aforementioned deterring beliefs often cluster within social networks and maintain myths that interfere with vaccination efforts within Latino communities (14). Coupled with widespread vaccine misinformation (14), myths and historically-rooted mistrust in the healthcare field work synergistically to foster challenges for widespread and equitable immunization (14).
Importantly, certain subpopulations within Latino communities, such as those with undocumented immigration legal status, those of lower socioeconomic status, and those without medical insurance, also face unique barriers to vaccine access (15). For example, Hamel et al. (16) found that over half of vaccinated Latino individuals reported being asked for government-issued identification prior to vaccination, and many unvaccinated Latinos expressed concerns with being asked to provide documentation (15). While immigration status does not preclude vaccination, having to present identification may pose a key obstacle to those of immigrant status (15). Additionally, Latinos of lower socioeconomic status may be deterred by their employers' lack of paid time off to recover from potential side effects of vaccination (15). These group-specific obstacles are important to consider given their ability to significantly limit vaccine participation. As the landscape of COVID-19 vaccination and the need for booster sessions continues to evolve, and in light of the disparate impact COVID-19 has had on Latino populations, a greater understanding of the barriers and facilitators to vaccination in underserved Latino communities is critical.
Purpose
This project was guided by principles of community-engaged research through collaboration with community health workers (CHWs) and Promotor/as (CHW/Ps) who serve the needs of communities that are medically underserved in South Texas, near the U.S.-Mexico border. Promotor/as are trained Latino community members who provide health education and resources to Latino communities. CHWs have played a key role in providing health information to Latino communities over the course of the COVID-19 pandemic, and are essential to support continued efforts to achieve health equity. Using the perspectives of CHW/Ps, the goal of this project was to identify cultural and contextual barriers and facilitators to vaccination for COVID-19 among Latino communities that have been historically underrepresented and/or that have been medically underserved, in particular those in remote or rural locations in proximity to the U.S.-Mexico border.
Methods
From its inception, the development of this project relied on shared cultural and contextual knowledge from collaborating CHW organizations, including two CHWs that were included as essential members of the research team. The collaborative process with local and regional CHW organizations began 3 months prior to the launching of this project; this time was used by the principal investigator to identify and learn about the priorities and needs of CHWs and their communities in the targeted region. In the process, the principal investigator along with collaborating CHWs visited community organizations and provided online psychoeducational webinars on self-care for local/regional CHWs. This provided an opportunity for CHWs in the region to become familiar with our work, while our team listened to their needs.
To facilitate obtaining diverse data, we recruited bilingual CHW/Ps using network-based referrals from the collaborating CHW organizations in communities that have been historically underrepresented and medically underserved in the region near the U.S.-Mexico border. Our collaborating CHW associations have an extensive history of facilitating outreach, research and the provision of various health services to Latino communities that have been historically marginalized. Specific strategies used in the recruitment included emails, social networks, and recruitment throughout online meetings for the local CHWs' associations. Eligibility criteria required that CHWs and/or Promotor/as be fluent in English and/or Spanish, and that they resided and worked with Latino communities that have been historically underserved.
We collected data from a sample of 64 CHW/Ps by using mixed methods, specifically qualitative and quantitative data (17). All data were collected remotely to avert person-to-person exposure during the pandemic. We collected quantitative data via an online Qualtrics survey (18), and qualitative data was collected using online focus groups via Zoom that were facilitated by a bilingual facilitator and two bilingual research assistants, including one of the two collaborating CHWs that were members of our research team. Surveys and focus group questions were first prepared in English, translated into Spanish, and then back-translated into English for consistency. The final survey and focus group questions were pre-tested in a small group of CHWs. A final version of the survey and focus group questions was established following feedback from the pre-test. All participants completed the online survey prior to attending a focus group. This strategy was helpful to introduce the topic to the participants and motivate in-depth discussion during the focus groups. Out of the five focus groups conducted, two were in done in English and three in Spanish. The online focus groups and the online survey each took about an hour to complete. Participants who completed the survey and participated in a focus group received $40 as compensation. Participants consented to audiotaping the focus groups, and all audiotapes were transcribed to facilitate data analysis. The blinded Institutional Review Board deemed this project non-regulated research on the basis of the project being a needs assessment project (HSC20200349N).
Measures
In line with community-engaged research, the survey and focus group questions were developed in collaboration with community partners from local CHW associations. The online survey consisted of 80 questions and included structured and open-ended questions. The survey included questions to assess: (a) demographic information (i.e., gender, age, race, were used. ethnicity, and education); (b) working expertise and history as CHW (i.e., work status, work setting, credential/licensing information, years working as CHW, demographic characteristics of their clients/patients, types of communities where their work takes place, and financial support for their work); and (c) perceived willingness of people in their communities to engage in COVID-19 vaccination; and (d) barriers and facilitators to COVID-19 prevention efforts, including vaccination for COVID-19. To assess barriers to COVID-19 vaccination, we asked, “On a scale from 1 (not at all) to 4 (extremely), how likely is it that the following list of concerns may prevent people in your community from getting vaccinated for COVID-19?” Responses were provided using a Likert scale ranging from no concern or barrier to serious concern or barrier. Open-ended questions were used to assess for any domains that may have not been included in the lists of barriers and facilitators to COVID-19 vaccination.
For the qualitative data, a topic guide was developed in collaboration with local CHW associations, which was used to guide the discussions for the focus groups. Questions for the focus groups were semi-structured and were aimed at fostering discussion pertaining to: (a) beliefs, attitudes, and barriers to vaccination for COVID-19 among Latino communities that have been historically underrepresented and/or medically underserved, and (b) facilitators to increase knowledge about and willingness to get the vaccine. As recommended by our collaborating CHWs, at the end of each interview or group, we provided participants with an opportunity to provide us with anonymous feedback using a comments and suggestion sheet. This was extremely helpful and provided us with knowledge that we incorporated into subsequent groups (e.g., provide information about resources for local mental health and legal services; explain the importance of research; schedule future talks in the community; longer duration of the groups to allow for more in-depth discussion).
Analyses
Quantitative data were analyzed using SPSS software. Descriptive statistics were used to develop a demographic profile of participating CHWs and the communities they serve, as well as to analyze data on barriers and facilitators to COVID-19 vaccination. Over a 2-month period, weekly group meetings with the principal investigator, research assistants, and collaborating CHWs were scheduled to analyze the findings from the focus groups. Qualitative data were analyzed through systematic methods outlined by Miles and Huberman (13), including starting with specific questions previously developed and then proceeding through the steps of data categorization, data reduction, data display, and conclusion drawing and confirmation (19). To confirm the categorization and validity of the data, we triangulated the data by comparing survey data with data from the focus groups and notes from all members of our research team. Upon completion of data analyses, the results described below were presented and discussed with our collaborating CHW organizations, and modifications were made with the feedback provided.
Results
Participants
Overall 64 CHW/Ps participated in this project. Most CHW/Ps were women of Latino background. Their mean age was 45.7 (SD = 13.3). Most (84.4%) reported working with low-income communities; 46.9% regularly worked with immigrant communities; and most worked across various settings, including community locations (e.g., homes, schools, community organizations; 62.5%), non-profit offices or facilities (50.0%), churches or faith-based organizations (21.9%), and primary care clinics (14.1%) (see Table 1).
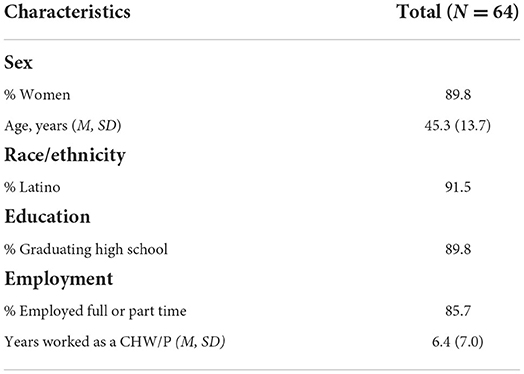
Table 1. Demographic characteristics of community health workers and Promotor/as.
Perceived relevance and importance of vaccination
Overall, using a scale from 1 (strongly disagree) to 5 (completely agree), 82.5% of CHW/Ps agreed or completely agreed that vaccination can provide important benefits to society. In addition, 77.2% of CHW/Ps agreed or completely agreed that people in their communities perceive vaccines in general as useful and effective. Yet, a substantial proportion of CHW/Ps (43.8%) agreed or completely agreed that people in their communities are likely to think of vaccines as having the potential for harmful side-effects. Indeed, 28.1% of CHW/Ps agreed or completely agreed that vaccines may sometimes cause illness or death. Nevertheless, most CHW/Ps (70.7%) reported that people in their communities would likely or definitely get vaccinated for COVID-19 if the vaccine were available to them. Of note, 8.6% of participants reported that people in their communities would be unlikely or extremely unlikely to get vaccinated for COVID-19, with 20.7% of participants reporting being unsure.
Barriers to vaccination for COVID-19 among underserved Latino communities
Personal fears or concerns
Survey results showed that the most frequently reported barriers to vaccination at the personal level were fear and mistrust, as well as concerns related to the COVID-19 vaccine itself. For instance, fear of getting exposed to COVID-19 from others at the vaccination site was identified as a salient concern (4-point Liker scale M = 2.39; SD = 0.71), followed by fear of contagion from the vaccine itself (M = 2.33; SD = 0.71), mistrust of vaccine manufacturers and distributors (M = 2.34; SD = 0.71); concerns about being discriminated by healthcare professionals administering the vaccine (M = 2.04; SD = 0.77); and worry about personal information being mishandled (M = 1.80; SD = 0.79).
In addition to the aforementioned fears and concerns, results from qualitative data identified exploitation and manipulation from government and health authorities as salient concerns associated with ethnic/racial social injustices and health inequities, as well as mistrust from the government in mishandling personal information. Another barrier identified pertained to the novelty of the COVID-19 vaccine: CHW/Ps emphasized that the unprecedented nature of COVID-19 along with limiting and confusing information surrounding the virus has magnified existing fears about COVID-19 vaccination. Moreover, CHW/Ps reported that some community members mistrust vaccine manufacturers for developing the vaccine without apparent sufficient time to undergo extensive safety testing, and mistrust healthcare workers administering the vaccine for perceived inadequate expertise or reputation for delivering vaccines. Some in their communities worried about vaccines being administered in hospital settings where the person going to get vaccinated could catch COVID-19 or other infectious diseases (Table 2).

Table 2. Personal, environmental, and community barriers to vaccination for COVID-19 according to CHW/Ps.
Environmental and community level factors
Survey results showed that a salient barrier at the environmental and community level was confusing information about the COVID-19 vaccines (M = 2.42; SD = 0.69). Difficulties in getting access to a vaccination site (e.g., due to lack of transportation and conflicting work schedules) (M = 2.36; SD = 0.73) was also identified as a barrier.
Qualitative data identified immigration legal status as interfering with willingness to get vaccinated. For instance, participants said that people with undocumented immigration legal status are concerned about not having the required documentation (e.g., driver license and other form of identification) to receive the vaccine and that they feared that disclosing personal information could result in detention and/or deportation. Also, certain myths and beliefs could interfere with vaccination, among them myths or religious beliefs precipitating fear, worry, shame, and guilt. For instance, one fear-inducing myths was that vaccination will be used as a surveillance strategy by the government to control the population and to manipulate information. Another myth was that vaccination was a coercive strategy to reduce people's sense of agency. A prevailing religious belief was that vaccination per se may go against God's will or fate, thus leading to a punishable sin. CHW/Ps also highlighted the preference for folk or traditional healing practices, such as herbal or natural remedies, instead of vaccination to fight off diseases.
Vaccine fears or concerns
A prevalent fear or concern related to the vaccine itself was the potential cost of the vaccine (M = 2.65; SD = 0.62), given that some people do not know that the vaccine is free and that they are concerned about possible money scams. Also, concerns about the safety of the vaccine, such as possible side effects (M = 2.37; SD = 0.68) and efficacy of the vaccine (M = 2.34; SD = 0.65), were reported as vaccine-related concerns. Results from qualitative data further identified concerns about vaccine efficacy, specifically a belief that people may contract the virus when exposed to others even if they have been vaccinated (see Table 3).
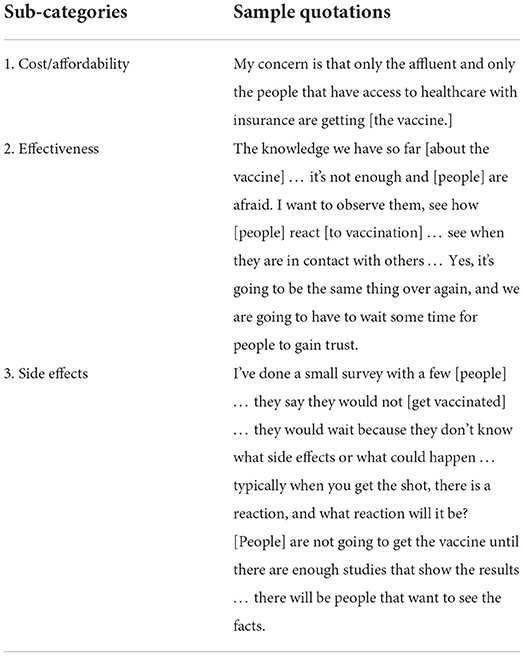
Table 3. Vaccine-related concerns as barriers to vaccination for COVID-19 according to community health workers/Promotor/as.
Facilitators to COVID-19 vaccination in underserved Latino communities
Knowledge about the COVID-19 vaccine
Survey results identified specific knowledge domains about the COVID-19 vaccine important to address among Latino communities that are medically underserved. First, any information about the vaccine needs to be available in English and Spanish (M = 2.86; SD = 0.35). Specific topics should include: (a) vaccine effectiveness (M = 2.82; SD = 0.49); (b) possible side effects (M = 2.80; SD = 0.44); (c) how the vaccine is administered (M = 2.79; SD = 0.49); (d) how long protection from the vaccine lasts (M = 2.75; SD = 0.51); (e) available vaccination sites and schedules (M = 2.72; SD = 0.53); (f) that vaccination is free of charge (M = 2.71; SD = 0.56); and (g) who will have access to vaccination records and related personal information (M = 2.62; SD = 0.59).
Environmental and community facilitators to vaccination for COVID-19
In addition to the need for information about the vaccine, quantitative results showed that the availability of bilingual staff to administer the vaccine is important (M = 2.91; SD = 0.29), as well as ensuring that there is ample supply of vaccines (M = 2.86; SD = 0.40). Moreover, convenient locations (M = 2.84; SD = 0.37), convenient vaccination schedules (M = 2.64; SD = 0.75), short wait times (M = 2.72; SD = 0.59), an option to get vaccinated at home (M = 2.37; SD = 0.87), and confidentiality are key (M = 2.47; SD = 0.89).
Findings from qualitative data emphasized that trusted networks are essential to delivering vaccine information, whether by building alliances with community partners or through testimonials from people in the community. In this regard, a CHW commented,
“We have to see that [the vaccine] worked with our own eyes because we can't just believe certain things when a lot of the stuff that's being said is here and there.”
The attitudes and personal attributes of people providing information and vaccinations, including medical providers, were cited as important. For instance, a CHW stated,
“Who are [people] going to trust? [People] are going to trust the worker that is genuine and compassionate. If they are not like that, patients don't trust… if [the provider] is abrupt or [if the provider] treats [people] like they're lower or that their education is low and they don't comprehend, then that's not a person that [people] are going to trust… genuine and compassionate is the name of the game.”
Discussion
Vaccination for COVID-19 is paramount to preventing the continued spread of the disease, yet many barriers continue to interfere with vaccination efforts among Latino communities that are marginalized or medically underserved (19). Research on COVID-19 has focused primarily on identifying disparities related to the pandemic (e.g., infection, death, and vaccination rates) and relevant demographic factors, with less consideration given to personal and community factors that may influence such disparities. This study identified personal, community and environmental barriers to vaccination for COVID-19 among Latino communities that have been historically underrepresented and/or medically underserved, as well as important facilitators to consider in order to propel vaccination efforts.
Mistrust and fear among Latino communities have been prevalent for years, yet this has escalated significantly over the past 5 years as a result of harmful rhetoric, stigmatization of Latino immigrants, discriminatory practices, and punitive governmental actions (20, 21). Consistent with this history, our findings showed that mistrust and fear of the government and of healthcare infrastructure were endorsed as significant personal level barriers to COVID-19 vaccination (e.g., fear that personal information may be mishandled; concerns about poor and/or differential treatment, including poor follow-up care if side-effects or symptoms develop; skepticism toward vaccine manufactures, etc.). Our findings also show that fears of exploitation and manipulation, such as concern that people are being experimented upon to test the vaccine, are also important barriers to COVID-19 vaccination and need to be addressed. Noteworthy is that mistrust and fear are especially common among Latino immigrants with undocumented immigration legal status, their family members with documented status, and people living in communities with a large proportion of immigrants with undocumented or temporary immigration legal status. People in those communities are concerned that not having proper identification or documentation (e.g., driver license, government or state issued identification) may prevent them from being eligible for vaccination, and that even if people have some form of identification, they may be at increased risk for detention, deportation, and/or family separation if they are “caught” being vaccinated. All of the aforementioned concerns are fuelling fear-inducing myths (e.g., vaccination is a tool used by the government as a surveillance strategy), myths that spread rapidly in the community leading some people to avoid vaccination. Future research is needed to identify strategies for building trust and reducing fear among historically marginalized Latino communities, including informing ways to deliver health messages in a manner that is contextually and culturally appropriate.
Adequate information about COVID-19 and COVID-19 vaccines is crucial to promoting community health, increasing vaccination rates, and countering fear-inducing myths and beliefs. Unfortunately, the spread of misinformation about COVID-19 and COVID-19 vaccines has caused confusion and adversely affected vaccination efforts among Latinos (22). Our findings corroborate that the dearth of factual information, especially in Spanish and in online or digital sources has undermined vaccination efforts among Latinos, particularly those that are marginalized or those living in remote or rural areas that are medically underserved. It is important to make information available about how different types of vaccines work and how they are made, including how new vaccine technology (e.g., mRNA) has been applied successfully in cancer treatments and other vaccines (e.g., Zika, rabies, etc.) (23, 24). Use of simple language and visual aids can be helpful to overcome concerns about the novelty of the vaccine and fears about experimentation (25). Future studies focusing on the use of an interdisciplinary approach that brings diverse perspectives from marketing, healthcare and the social sciences to identify best strategies for delivering health messages to underserved Latino communities are needed to fill existing knowledge gaps and to inform health equity efforts.
To reduce fear and increase trust, health providers and public health authorities should partner with non-traditional sources of service delivery in communities that have been historically underserved. In this regard, community non-profits and faith-based institutions can be key collaborators (26). Likewise, CHW/Ps are trusted members of the community who work in tandem with local healthcare, community, and government systems as an extension for providing services (27). CHW/Ps play a variety of roles in education and healthcare delivery, including acting as liaisons with their communities, assisting with health system navigation and case management, counseling, combating misinformation and myths, and collecting data for disease surveillance, among many other important activities (16, 27). CHW/Ps are not only trusted by members of their communities, but they also understand cultural and contextual factors and interpersonal dynamics important to address to increase vaccination rates among Latino communities that have been historically marginalized (27). CHW/Ps can inform and deliver vaccination messages and materials that appeal to Latino cultural values, such as that vaccination is an act of love and care toward one's family and community, while also leveraging testimonials from community members attesting to the benefits of vaccination. To maximize success, collaborations between public health authorities and non-traditional sources of service delivery have to be carefully and respectfully established, adequately funded, and provided with ongoing training, support, and resources during and beyond the pandemic.
Limitations
This study has several limitations. Our sample size was modest, and although drawn from a large region, represents Latino communities in South Texas that have been historically underrepresented and/or medically underserved. Latinos in the U.S. are a heterogeneous population, so a larger study to identify barriers and facilitators that may influence vaccination across different U.S. Latino communities is needed. Additionally, due to COVID-19, we conducted our survey and focus groups over a video conferencing platform (web-based and telephone-accessed), which may have excluded participants without access to the internet or reliable phone service. Nonetheless, we gathered diverse perspectives from a broad region in a manner that facilitated participation while complying with social distancing recommendations.
Also, data were collected in the summer of 2020, several months before COVID-19 vaccines first became available in the U.S. Future studies should compare results from this project with current trends to assess changes over time in barriers and facilitators to COVID-19 vaccination among historically marginalized Latino communities. This information is needed to inform continued prevention efforts and emergency preparedness for future events.
Conclusion
Vaccinations play an essential role in maintaining the health of our communities. Vaccination for COVID-19 among Latino communities that have been historically marginalized is multifaceted, however. Targeted efforts that build upon collaboration with non-traditional sources of service delivery that are trusted by communities that have been underrepresented are needed to overcome barriers in a culturally and contextually sensitive manner. Not all of the barriers identified in this study are unique to COVID-19 vaccination efforts, but they highlight problems in the availability and accessibility of healthcare more broadly among Latino communities that have been historically marginalized. Advocacy and policy efforts aimed at increasing access to vaccination and preventive efforts to promote and maintain good health for this vulnerable population should be prioritized.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This project was reviewed and approved by UTHSCSA Institutional Review Board and was deemed non-regulated research on the basis of the project being a needs assessment project (HSC20200349N). The patients/participants provided their written informed consent to participate in this study.
Author contributions
The first draft of the manuscript was written by LG and AA. All authors contributed to the study conception and design, material preparation, analysis, commented and edited on previous versions of the manuscript, read, and approved the final manuscript.
Funding
This study was funded by a grant from the National Institutes of Health, National Heart, Lung, and Blood Institute (NHLBI) (K01HL150247; PI: LG) and was also supported with funds from the Joaquin G. Cigarroa, Jr. M. D. Distinguished Chair at the University of Texas Health Science Center at San Antonio.
Acknowledgments
The authors acknowledge Raquel Romero and Ludivina Hernandez for their support in data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
1. Garcini LM, Domenech Rodríguez MM, Mercado A, Paris M. A tale of two crises: the compounded effect of COVID-19 and anti-immigration policy in the United States. Psychol Trauma Theor Res Pract Policy. (2020) 12(S1):S230–2. doi: 10.1037/tra0000775
2. Centers for Diseases Control and Prevention. Risk for COVID-19 Infection, Hospitalization and Death by Race/Ethnicity. (2022). Retrieved online at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed September 10, 2022).
3. U.S. Census Bureau. Race and Ethnicity in the United States: 2010 Census and 2020 Census. (2021). Available online at: https://www.census.gov/library/visualizations/interactive/race-and-ethnicity-in-the-united-state-2010-and-2020-census.html (accessed January 4, 2022).
4. Texas Department of State Health Services. COVID-19 - Cases (Dashboard). (2022). Available online at: https://www.arcgis.com/apps/dashboards/45e18cba105c478697c76acbbf86a6bc (accessed May 14, 2022).
5. Andrasfay T, Goldman N. Reductions in 2020 US life expectancy due to COVID-19 and the disproportionate impact on the Black and Latino populations. Proc Natl Acad Sci. (2021) 118:118. doi: 10.1073/pnas.2014746118
6. Nguyen KH, Srivasta A, Razzaghi H, Williams W, Lindley M, Jorgensen C, et al. COVID-19 vaccination intent, perceptions, reasons for not vaccinating among groups prioritized for early vaccination—United States, September December 2020. MMWR. (2021) 70:217–22. doi: 10.15585/mmwr.mm7006e3
7. Painter EM, Ussery EN, Patel A, Hughes MM, Zell ER, Moulia DL, et al. Demographic characteristics of persons vaccinated during the first month of the COVID-19 vaccination program—United States, December 14, 2020–January 14, 2021. MMWR. (2021) 70:174–77. doi: 10.15585/mmwr.mm7005e1
8. Ndugga N, Hill L, Artiga S, Haldar S. Latest Data on COVID-19 Vaccinations by Race/Ethnicity. KFF (2022). Available online at: https://www.kff.org/coronavirus-covid-19/issue-brief/latest-data-on-covid-19-vaccinations-by-race-ethnicity/ (accessed September 10, 2022).
9. Wang ML, Behrman P, Dulin A, Baskin ML, Buscemi J, Alcaraz KI, et al. Addressing inequities in COVID-19 morbidity and mortality: research and policy recommendations. Transl Behav Med. (2020) 10:516–9. doi: 10.1093/tbm/ibaa055
10. Romer D, Jamieson KH. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. So Sci Med (1982). (2020) 263:113356. doi: 10.1016/j.socscimed.2020.113356
11. Palinkas LA, Aarons GA, Horwitz S, Chamberlain P, Hurlburt M, Landsverk J. Mixed method designs in implementation research. Admin Policy Mental Health. (2011) 38:44–53. doi: 10.1007/s10488-010-0314-z
12. Qualtrics [Computer Software]. Qualtrics. Available online at: https://www.qualtrics.com (accessed September 10, 2022).
14. Botti-Lodovico Y, Rosenberg E, Sabeti PC. Testing in a Pandemic—Improving Access, Coordination, and Prioritization. New Engl J Med. (2021) 384:197–9. doi: 10.1056/NEJMp2025173
15. Sanchez GR, Peña JM. Skepticism and Mistrust Challenge COVID Vaccine Uptake for Latinos. Brookings (2021). Available online at: https://www.brookings.edu/blog/how-we-rise/2021/01/25/skepticism-and-mistrust-challenge-covid-vaccine-uptake-for-latinos/ (accessed September 10, 2022).
16. Hamel L, Artiga S, Safarpour A, Stokes M, Brodie M. KFF COVID-19 Vaccine Monitor: COVID-19 Vaccine Access, Information, Experiences Among Hispanic Adults in the U.S. KFF (2021). Available online at: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-access-information-experiences-hispanic-adults/ (accessed September 10, 2022).
17. Langer Research Associates. COVID Collaborative Survey: Coronavirus Vaccination Hesitancy in the Black and Latinx Communities. (2020). Available online at: https://www.covidcollaborative.us/content/vaccine-treatments/coronavirus-vaccine-hesitancy-in-black-and-latinx-communities (accessed September 10, 2022).
18. Morales C. Black and Latino Americans Confront Many Challenges to Vaccinations. The New York Times (2021). Available online at: https://www.nytimes.com/2021/02/18/world/us-coronavirus-vaccine-minorities.html (accessed September 10, 2022).
19. Lint SV, Renmans D, Broos K, Dewitte H, Lentacker I, Heirman C, et al. The ReNAissanCe of mRNA-based cancer therapy. Expert Rev Vac. (2015) 14:235–51. doi: 10.1586/14760584.2015.957685
20. National Academies of Sciences, Engineering, Medicine, Health Medicine Division, Board Board on Population Health Public Health Practice, Committee on Community-Based Solutions to Promote Health Equity in the United States, Baciu A, Negussie Y, Geller A, Weinstein JN, editors. Communities in Action: Pathways to Health Equity. Washington, DC: National Academies Press (US) (2017).
21. Landers S, Levinson M. Mounting evidence of the effectiveness and versatility of community health workers. Am J Public Health. (2016) 106:591–2. doi: 10.2105/AJPH.2016.303099
22. Peretz PJ, Islam N, Matiz LA. Community health workers and Covid-19—addressing social determinants of health in times of crisis and beyond. N Engl J Med. (2020) 383:e108. doi: 10.1056/NEJMp2022641
23. Pardi N, Hogan MJ, Porter FW, Weissman D. mRNA vaccines—A new era in vaccinology. Nat Rev Drug Discov. (2018) 17:261–79. doi: 10.1038/nrd.2017.243
24. National Center for Health Statistics. Provisional COVID-19 Deaths by Race and Hispanic Origin, and Age. (2022). Available online at: https://data.cdc.gov/d/ks3g-spdg (accessed May 14, 2022).
25. Balasuriya L, Santilli A, Morone J, Ainooson J, Roy B, Njoku A, et al. COVID-19 vaccine acceptance and access among Black and Latinx Communities. JAMA Network Open. (2021) 4:e2128575. doi: 10.1001/jamanetworkopen.2021.28575
26. Guzman-Holst A, DeAntonio R, Prado-Cohrs D, Juliao P. Barriers to vaccination in Latin America: a systematic literature review. Vaccine. (2020) 38:470–81. doi: 10.1016/j.vaccine.2019.10.088
Keywords: vaccine, COVID-19, Latinos/Hispanics, community, health disparities, hesitancy
Citation: Garcini LM, Ambriz AM, Vázquez AL, Abraham C, Sarabu V, Abraham C, Lucas-Marinelli AK, Lill S and Tsevat J (2022) Vaccination for COVID-19 among historically underserved Latino communities in the United States: Perspectives of community health workers. Front. Public Health 10:969370. doi: 10.3389/fpubh.2022.969370
Received: 14 June 2022; Accepted: 30 September 2022;
Published: 18 October 2022.
Edited by:
Victoria Team, School of Nursing and Midwifery, Monash University, AustraliaReviewed by:
Theresa Byrd, Texas Tech University Health Sciences Center, United StatesRosemary M. Caron, University of New Hampshire, United States
Copyright © 2022 Garcini, Ambriz, Vázquez, Abraham, Sarabu, Abraham, Lucas-Marinelli, Lill and Tsevat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luz M. Garcini, Z2FyY2luaUB1dGhzY3NhLmVkdQ==