
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 18 July 2022
Sec. Occupational Health and Safety
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.878396
This article is part of the Research Topic COVID-19: challenges, opportunities and lessons for occupational health View all 20 articles
 Nadia Mohamad1*Muhammad Alfatih Pahrol1Rafiza Shaharudin1Nik Khairol Reza Md Yazin2Yelmizaitun Osman3Haidar Rizal Toha4Normazura Mustapa5Zuraida Mohamed6Azyyati Mohammad6Rohaida Ismail1
Nadia Mohamad1*Muhammad Alfatih Pahrol1Rafiza Shaharudin1Nik Khairol Reza Md Yazin2Yelmizaitun Osman3Haidar Rizal Toha4Normazura Mustapa5Zuraida Mohamed6Azyyati Mohammad6Rohaida Ismail1Healthcare workers (HCWs) are at risk of contracting coronavirus disease-2019 (COVID-19) in their workplace. Infection prevention guidelines and standard operating procedures were introduced to reduce risk of exposure and prevent transmission. Safe practices during interaction with patients with COVID-19 are crucial for infection prevention and control (IPC). This study aimed to assess HCWs' compliance to IPC and to determine its association with sociodemographic and organizational factors. A cross-sectional study was conducted between March and April 2021 at public healthcare facilities in the east coast of Peninsular Malaysia. HCWs who were involved with COVID-19-related works were invited to participate in the online survey. The questionnaire was adapted from the World Health Organization (WHO) Interim Guidance: WHO Risk Assessment and Management of Exposure of Healthcare Workers in the Context of COVID-19. Respondents were categorized as compliant or non-compliant to IPC. A total of 600 HCWs involved in COVID-19-related works participated in the survey. Most of them (63.7%) were compliant to IPC as they responded to all items as “always, as recommended” during interaction with patients with COVID-19. The multivariate analysis showed that non-compliance was significantly associated with working in the emergency department (AOR = 3.16; 95% CI = 1.07–9.31), working as laboratory personnel (AOR = 15.13; 95% CI = 1.36–168.44), health attendant (AOR = 4.42; 95% CI = 1.74–11.24), and others (AOR = 3.63; 95% CI = 1.1–12.01), as well as work experience of more than 10 years (AOR = 4.71; 95% CI = 1.28–17.27). The odds of non-compliance among respondents without adequate new norms and personal protective equipment training were 2.02 (95% CI = 1.08–3.81) more than those with adequate training. Although most of the respondents complied to IPC protocols, compliance status differed according to department, work category, and years of service. Ensuring adequate training that will hopefully lead to behavioral change is crucial to prevent breach in IPC and thus minimize the risk of exposure to and transmission of COVID-19 in healthcare facilities.
The World Health Organization (WHO) declared coronavirus disease-2019 (COVID-19), which is caused by novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a pandemic in March 2020. At that time, COVID-19 had spread rapidly in 114 countries with more than 118,000 confirmed cases, causing 4,291 deaths (1). After more than a year, the disease showed no sign of mitigation. Up until 6 July 2021, cumulative cases globally were more than 183 million with almost 4 million total deaths and over 2.6 million new cases being reported in a week (2). The overwhelming number of cases increased the burden for frontline healthcare workers (HCWs) in patient-facing roles and placed them at greater risk as their work require close contact with patients with COVID-19 (3).
The main mode of transmission for COVID-19 is human to human with respiratory droplets as the primary route of transmission. The SARS-CoV-2 route of entry to the respiratory systems are either via inhalation or deposition of droplets to mucous membrane or touching mucous membrane with SARS-CoV-2 contaminated objects (4). Available prevention guidelines on how to prevent COVID-19 transmission has remained unchanged from the early phase of the pandemic (4). Generally, physical distancing, face mask usage, frequent hand washing, good indoor ventilation, and avoidance of crowded places have been recommended (5). Additional implementation of personal protective equipment such as usage of gloves, gowns, face or eye protections and N95 masks, along with other standard practices, had been recommended for HCWs who are involved or in contact with patients with COVID-19 as part of infection prevention and control (IPC) during the pandemic (6, 7).
Despite the availability of infection prevention guidelines to protect HCWs, they are not immune to the disease. Previous evidence had shown that during the SARS-CoV-1 outbreak in 2003, a total of 1,706 HCWs were infected globally, contributing to 21% of total SARS cases (8). The current pandemic has shown a similar situation with HCWs comprising 14% of all reported cases (9). Nearly 570,000 HCWs in America were reported positive for COVID-19, and more than 2,500 of them were deceased by September 2020 (10). The WHO had estimated that the number of HCW deaths globally could be more than 115,000 within 18 months of COVID-19 emergence, and this was derived by population-based estimations (11).
By February 2021, Malaysia had recorded a total of 4,756 confirmed COVID-19 cases among HCWs prior to the national COVID-19 vaccination program (12). Despite preventive measures and completed 2 doses of vaccination, 2,341 confirmed COVID-19 cases were detected among HCWs within 3 months post-vaccination (13). Public healthcare system is the main healthcare provider in Malaysia, and the system is overwhelmed with the surge of cases during COVID-19 waves (14). Quarantine centers were established, and some government hospitals were redesigned into full or partial COVID-19 hospitals (15). Similar studies on compliance of HCWs to IPC during care of patients with COVID-19 and their associated factors have been carried out (16–22). However, they were confined mostly to HCWs working in hospitals. In Malaysia, management of and exposure to patients with COVID-19 involved HCWs from various types of healthcare facilities including hospitals, health clinics, and state and district health offices. The HCWs had different job scopes and level of exposure to or interaction with patients with COVID-19. Furthermore, there were limited studies that looked at the impact of organizational support to IPC compliance among HCWs. Thus, it is crucial to understand the role of organizational support and how exposure to SARS-CoV-2 and safe practices could reduce the risk of COVID-19 among HCWs in different types of healthcare facilities. A comparison of similar studies on compliance to IPC is available in Supplementary Table S1.
This study aimed to assess HCWs' compliance to IPC and to identify the associated sociodemographic and organizational factors that contributed to their compliance. The findings are expected to assist in investigating the trends of COVID-19 infection among HCWs and to assist in developing mitigation strategies to reduce COVID-19 transmission and protect our HCWs in their workplace. The tools from this study could be used by stakeholders in assessing adequacy of control and preventive measures among HCWs to other contagious outbreaks in the future.
This was a cross-sectional study conducted at public healthcare facilities in a state in the east coast of Peninsular Malaysia involving 9 hospitals, 56 health clinics, and 10 district health offices. The online survey was emailed between March and April 2021 to all HCWs who were involved in COVID-19-related works including medical doctors, nurses, assistant medical officers, medical assistants, environmental health assistant officers, health attendants, laboratory personnel, and others (e.g., clerks, cleaners, and drivers). The survey link was sent through the occupational health unit of each facility. The link introduced briefly the study and approval that was obtained from the ethics committee and the state health department prior to commencement of this study. A detailed description of the study including objectives and participants' rights were explained in the first part after clicking the link, followed by informed consent. Respondents will be able to proceed to the questionnaire after providing their consent. A reminder for HCWs to fill up the questionnaire was sent by the occupational health unit at a 2-weeks interval throughout the 2-months study duration. Out of the 618 HCWs who responded to the questionnaire, 600 (97%) answered the questionnaire completely and met the criteria for involvement with COVID-19-related works. These included those who were directly involved in treating, managing or handling, and screening patients with COVID-19, conducting SAR-CoV-2 laboratory tests, transporting patients with COVID-19 and samples, cleaning COVID-19 facilities, and conducting epidemiological investigation on confirmed COVID-19 cases.
This study was approved by the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia [KKM/NIHSEC/P21–109(12)]. All participations were anonymous, and personal identifiers would not appear in any report.
The questionnaire was adapted from the WHO Risk Assessment and Management of Exposure of Healthcare Workers in the Context of COVID-19 (23), which was structured in 4 parts. The first part was for gathering sociodemographic and occupational profiles consisting of variables such as age, gender, marital status, medical and medication history, workplace, job category, and years of service. The second part was about HCWs' activities related to COVID-19 exposure in the workplace and their COVID-19 status such as tested for COVID-19 and the result. The third part was about adherence to IPC during interaction with possible, probable or confirmed COVID-19 cases, which included assessment of PPE usage (5 items) and hand hygiene (4 items). Scoring for compliance status was similar to the WHO tool with a 4-point Likert scale: “always as recommended,” “most of the time,” “occasionally,” and “rarely.” While the terms used in this study for “high-risk exposure” were “noncompliance” and “low risk exposure” were identified as “compliance.” Those who responded to all items with “Always, as recommended” were categorized as compliant to IPC, whereas those with response other than that were categorized as non-compliant to IPC. Another modification was in scoring, which did not include adherence to IPC while doing aerosol-generating procedures. The last part was about organizational support. It consisted of 7 items to assess whether higher management in health facilities provided their workers with adequate instruments, items, training, or enforcement needed to ensure a safe work environment during the pandemic.
The survey forms were made available bilingually, in English and in Malay. The questions were translated into Malay language by 2 native Malaysians with good English proficiency, and back-translations were conducted by another two bilingual individuals to verify accuracy. The questions were modified according to local circumstances and were validated by five panels with occupational and public health background. Each panel indicated its comment or decision to remove, keep, or modify each item. After modification, content validation was conducted by another five public health specialists working at Ministry of Health's headquarters and the State Health Department. All of them were managing the occupational health program, including HCWs' well-being during the pandemic. Prior to the study, the questionnaire was tested on 50 HCWs in the Ministry of Health (MOH) who had an experience with COVID-19-related works. This was performed to ensure the readability, understanding and comprehensiveness of this tool and accuracy in reflecting the factors. The Cronbach's alpha was 0.748, which signified acceptable reliability.
Data from the questionnaires were transferred to Microsoft Excel, and Statistical Package for the Social Sciences (SPSS) version 21 (IBM, United States) was used for analysis. The data were initially analyzed descriptively to determine the representativeness of the respondents in this study. Categorical data were presented as frequencies and percentages, whereas means and standard deviations were expressed for continuous data. Pearson chi-square or Fisher's exact test was carried out to analyze activities with high exposure to SARS-CoV-2 and COVID-19 status with IPC compliance status. Next, univariate and multivariate analyses were conducted by binary logistic regression to identify a sociodemographic association with IPC as well as organizational support and IPC. Then, multicollinearity terms were checked, and the Hosmer-Lemeshow test and classification table were applied to check for model fitness. Statistically significant result was set at p < 0.05.
A total of 600 HCWs who were involved in COVID-19-related works were included in the survey. They were predominantly women (73.8%), married (90.3%), diploma or certificate holder (60.8%), without pre-existing medical condition (59.0%), and not on regular medication (75.0%). Mean age was 39.9 ± 7.4 years old, and mean household number was 5 ± 1.8. Nearly half of the respondents worked in hospitals (49.0%) and were nurses (52.0%). More than two-thirds of them had work experience of more than 10 years (69.5%) with mean work duration of 15.3 ± 7.3 years.
Table 1 shows the reported adherence to IPC practices. Adherence to type of PPE used and hand hygiene practices ranged from 83.7 to 97.5%; the highest adherence was for using medical masks and the lowest adherence was for using disposable gowns and single-use gloves. Overall, 382 (63.7%) of the respondents were compliant and adhered fully to all PPE and hand hygiene items (answered “always, as recommended”), making 218 (36.3%) of the respondents non-compliant.
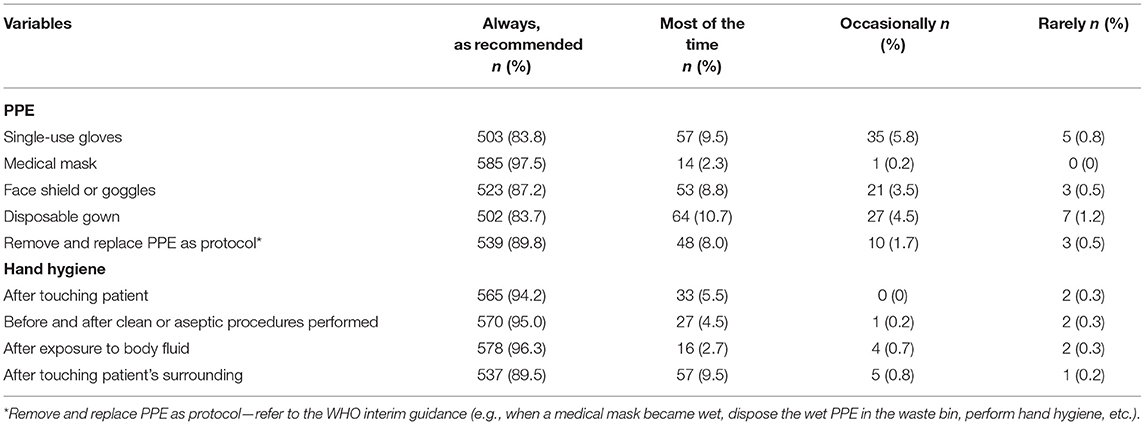
Table 1. HCW adherence to infection prevention and control practices during interaction with patients with COVID-19.
Majority of the HCWs in this study provided direct care to patients (84.8%), but only 26.5% had face-to-face contact with patients with COVID-19, and 14.5% were present during aerosol-generating procedures (Table 2). Nearly two-thirds of the respondents (65%) had direct contact with contaminated objects or environmental exposure (bed, linen, medical equipment, bathroom, etc.) while caring for patients with COVID-19, and 2.8% were exposed to splash accidents (6 cases to eyes, 6 cases to mouth, and 10 cases to non-intact skin) and sharps injuries (2 cases) involving patients with COVID-19. However, no significant difference was found (p > 0.05) between their involvement in activities with high exposure to SARS-CoV-2 and compliance status.
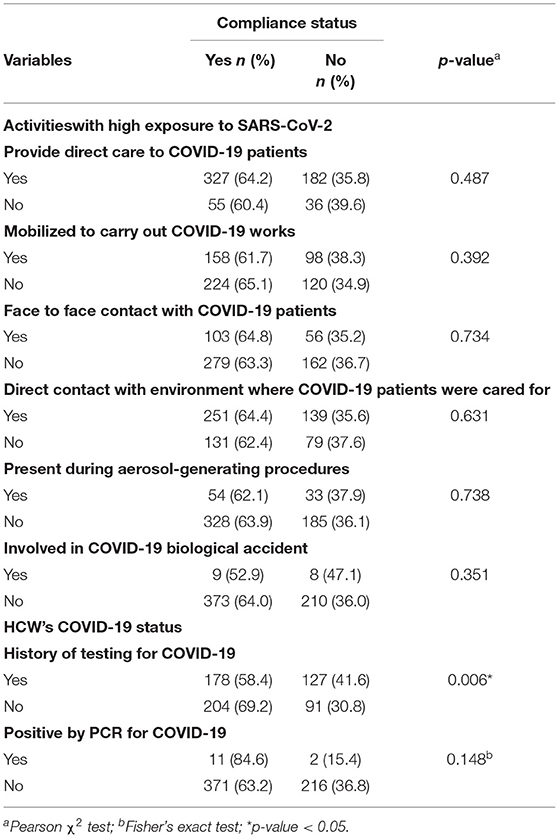
Table 2. Activities with high exposure to SARS-CoV-2 and COVID-19 status according to IPC compliance status.
Based on their COVID-19 status, Table 2 shows that out of 600 respondents, 305 (50.8%) had a history of taking a COVID-19 swab test either by procedural or asymptomatic screening or because they were in close contact to positive COVID-19 cases. Only 4.3% were positive for COVID-19. There was a significant difference in compliance status among respondents with history of swab testing, whereas compliance status was higher among those who had not undergone a swab test for COVID-19 (p = 0.006). However, there was no difference in compliance seen by positivity status to COVID-19.
Univariate and multivariate regression analysis were conducted to determine the association between sociodemographic and occupational factors, as well as organizational support and compliance status as shown in Tables 3, 4. The final model was checked for multicollinearity, and the variance inflation factor (VIF) for the variables was < 5, indicating no strong correlation between the variables. The Hosmer and Lemeshow tests were not significant (p > 0.05), which indicated that the model was fit. The overall correctly classified percentage is acceptable by the classification table.
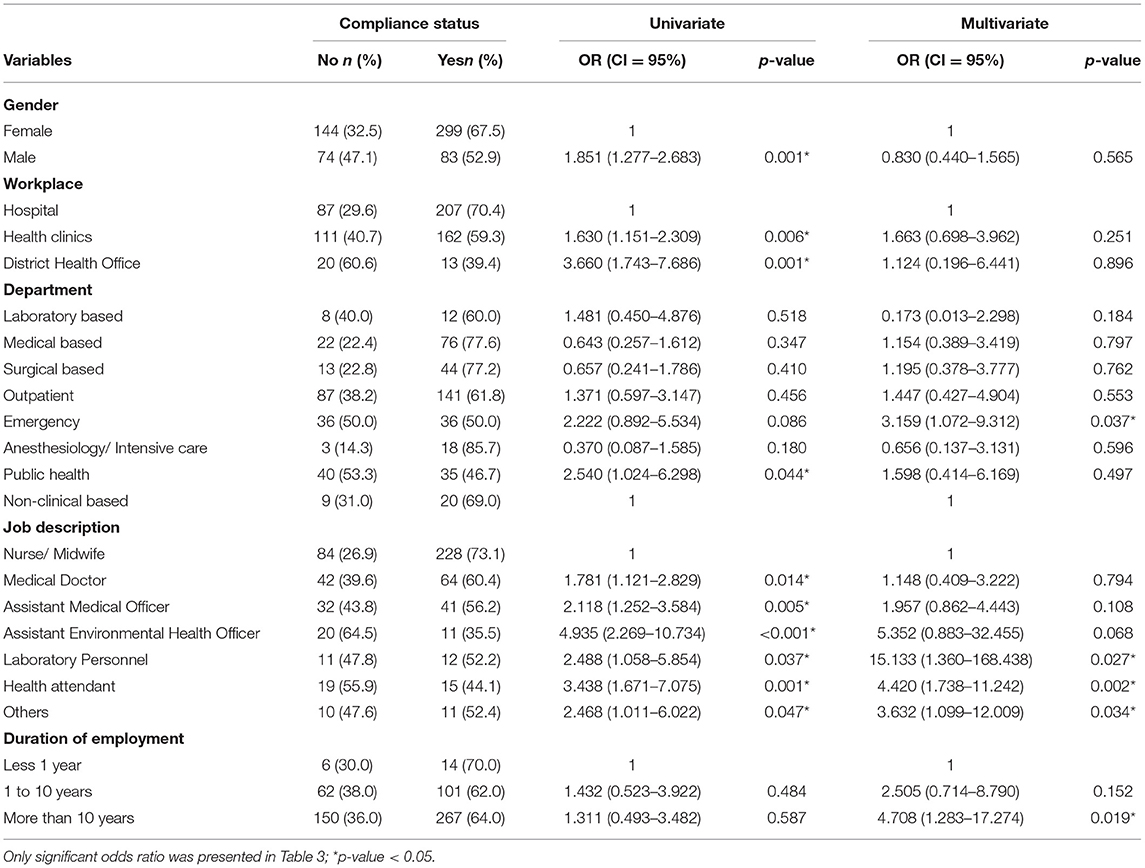
Table 3. Demographic and occupational factors associated with compliance status among healthcare workers.
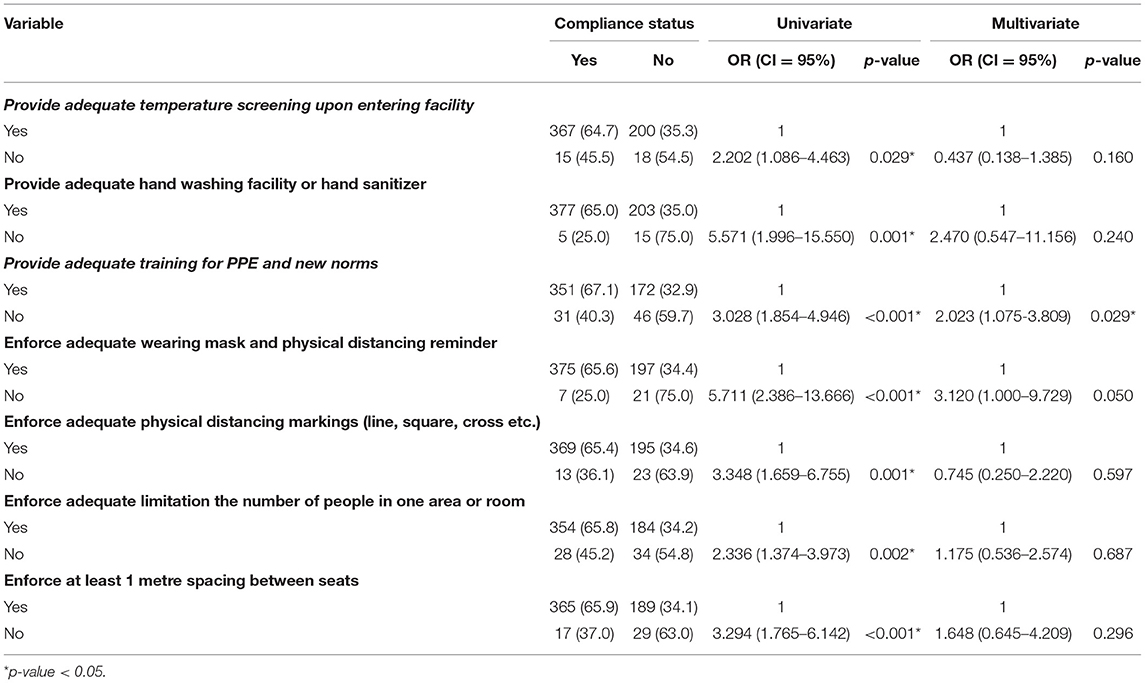
Table 4. Organizational support provided by management in healthcare facilities.
Age, educational level, number of households, preexisting medical condition, and taking regular medication showed no association with breach in IPC. There were five factors that were statistically significant for compliance status. Those who worked in the emergency department (AOR = 3.16; 95% CI = 1.07–9.31) had higher odds of non-compliance to IPC than those based in non-clinical departments. The odds of non-compliance to IPC were 15 times higher among laboratory personnel (AOR = 15.13; 95% CI = 1.36–168.44), 4.4 times higher among health attendants (AOR = 4.42; 95% CI = 1.74–11.24), and 3.6 times higher among other job categories (AOR = 3.63; 95% CI = 1.1–12.01) than nurses, whereas those who have a work experience of more than 10 years (AOR = 4.71; 95% CI = 1.28–17.27) had higher odds of non-compliance than those with < 1 year of work experience.
Table 4 describes the association between organizational support and compliance status among the respondents. It was found that the odds of non-compliance to IPC was 2 times higher among HCWs who lacked training than those who received adequate training. It was also found that the odds of non-compliance to IPC was 3 times higher if there were inadequate enforcement reminders for wearing a mask and physical distancing (p = 0.05).
The existing IPC standard in Malaysia is applied in healthcare settings to minimize the risk of infection for both patients and HCWs, and this is supported by the Occupational Safety and Health (OSH) program (24). During the pandemic, the Annex 21 Management of HCWs During the COVID-19 Pandemic has been developed and regularly updated to address standard operating procedures (SOP) (25). It includes awareness and training, IPC practices, PPE usage, vaccination, surveillance, and management of HCWs contracting the disease. The implementation of SOPs including IPC is regularly monitored and audited by the OSH or IPC committee in respective healthcare facilities.
Compliance status is important in identifying breach in IPC among HCWs. This is especially because since the start of the pandemic up to February 2021, more than half of infected HCWs in Malaysia contracted the disease at work (26). Preventing infections among HCWs is crucial to ensure there are no disruption of healthcare delivery during the pandemic. Staff shortage occurred not only because HCWs are positive and need to be isolated or treated but also because their colleagues become close contacts and need to be quarantined as well to prevent further transmission to others as mentioned before. In this study, 4.3% of respondents who underwent testing for COVID-19 were confirmed positive. This was consistent with findings from other studies in Italy (3.5%), Germany (3.5%), and the United States (4.5%) (27–29), while another review showed a higher percentage from HCWs tested by RT-PCR and detection of antibodies, with the pool prevalence of SARS-CoV-2 reported as 11 and 7%, respectively (30).
Compliance to IPC in other studies showed mixed findings from low to high practices (16–19). The majority of HCWs in this study showed good adherence to single items in IPC practices. Use of disposable gowns (83.7%) scored the lowest compliance among all personal protective equipment (PPE) used, while items under hand hygiene showed better results except for hand hygiene after touching patient's surrounding (89.5%), which was the only item that scored below 90%. The result was probably due to the illusion of safety, as there was no direct contact with patients. However, it is important to take precaution as the virus could also be transmitted from contaminated surfaces (31). In our study, there was no significant difference in compliance to IPC among HCWs based on their work during management of patients with COVID-19. Most of the respondents complied to IPC practices regardless of involvement in activities with high risk of exposure to SARS-CoV-2 or not. This is a commendable practice, as adherence to IPC is important in other daily activities, considering they can be exposed and contract COVID-19 infection even from the community (32). However, it is quite worrying that there was non-compliance to IPC practices even among HCWs who were involved in high-risk works, as they could get infected and increase the risk of nosocomial transmission to others (33).
The univariate analysis showed a significant association among status of compliance by gender, profession, type of facility and department where HCWs worked. Non-compliance was higher among men (47.1%) than women (32.5%), with the odds among men being 1.9 times higher than those among women. This could be contributed by their profession, as most of the women involved in the study were nurses, and they were also found to be more compliant than those with other types of profession in this study. Other studies also found that nurses were better in utilizing PPE than those with other professions (16, 20, 34, 35), while a seroconversion study in Egypt reported that the odds of hazard in women were 1.63 times higher than the odds in men (36). The medical doctors in this study had lower compliance than the nurses. Gilbert and Kerridge (37) reported reasons for lower compliance among medical doctors as they tend to rely on clinical judgment and experience rather than follow rules and ignorance, and some chose to disregard IPC practices despite recognizing their importance (37). Atnafie et al. (22) found that the rate of HCWs infected with COVID-19 among hospital staff was lower than that of HCWs working in other health facilities. However, they did not find any significant association (22). In our study, the odds of non-compliance were higher in HCWs working in health clinics and district health offices than in HCW working in hospitals. This is probably because hospitals have established IPC guidelines and have been practicing standard operating procedures on IPC even before the pandemic (24) compared to other types of health facilities. Moreover, infectious disease physicians and nurses are also posted in hospitals, and they have regular training and monitoring of IPC practices there (38). Similarly, HCWs who worked in public health departments had a significant association with non-compliance. This might be because common infectious diseases in community were tropical diseases like dengue and other diseases that are not spread by air or droplets, which have different protocols for IPC (39, 40).
After adjusting for other demographic and occupational factors, it was found working in emergency department (ED), worked for more than 10 years, HCWs who were laboratory personnel, health attendant and occupation grouped as others had significant risk of noncompliance. Non-compliance among HCWs in the ED could be contributed by the hectic and busy nature of work in the ED where there are many varied patients with different severity, with some requiring emergency procedures, making it difficult for them to keep changing their PPE each time for different patients (35, 41). A study by Ezike et al. found that preventive measures were not strictly adhered to in medical wards, children wards, and clinic and maternity complexes (21). The finding of significant non-compliance among HCWS who had worked for more than 10 years was consistent with the findings by Osborne (42). Greater non-compliance was found to be associated with longer years of working experience and habit as they could lead to disinclination to changes (42). However, our findings contradicted with another study in Canada that reported experienced nurses were more compliant than new nurses (43). Non-compliance was also seen among health attendants, laboratory personnel, and non-clinical staff compared to nurses. This category of HCWs usually does not have a direct contact with patients and this could probably influence their IPC practices. Nevertheless, they are still at risk, and IPC training should include them to improve their compliance (16).
Organizational support had been associated with compliance with using PPE in preventing respiratory diseases (43). This study demonstrated that all the organizational support provided had a significant association with compliance in the univariate analysis but after adjusting for confounders, only lack of adequate training was associated with non-compliance. Other studies had reported the importance of training and its influence on compliance with using PPE (44, 45). Inadequate training will lead to low knowledge of the importance and need for adherence to IPC among HCWs. Therefore, effective training in IPC should be endorsed to all medical staff (44) especially during this pandemic. Based on the findings, the questionnaire is able to assess IPC compliance among HCWs and would be useful to be incorporated in occupational health surveillance programs. Follow-up surveys should be carried out to observe whether there is improvement over time and to evaluate the effectiveness of intervention programs.
Among the limitations of this study was the use of self-administered questionnaire, which could lead to over- or under-reporting as compared to the real situation. Respondents will have to recall their practices when answering the question, which may contribute to recall bias. The IPC practices and compliance included in this study may also need to be revised in future studies with the emergence of new COVID-19 variants of concerns that are more transmissible (46–48).
Generally, most of the HCWs in this study complied with IPC. The compliance status differed among HCW location, profession, and their years of service. However, it is a cause of concern that more than a quarter of the respondents were non-compliant to IPC practices during interactions with patients with COVID-19, which may expose them to SARS-CoV-2 infection in their workplace, especially when there are new emerging variants that are more transmissible. As this study has identified HCWs who are more likely to be less compliant, it is imperative that administrators of these health facilities look into ways to improve IPC compliance, which should include an infection control committee and an occupational safety and health committee. They could plan intervention programs to target non-compliant workers by sending reminders at regular intervals or conducting regular training, nudging strategies, and rewarding those who comply. They should also review the effectiveness of their intervention program by conducting regular monitoring of compliance.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia [KKM/NIHSEC/P21-109(12)]. The patients/participants provided their written informed consent to participate in this study.
All the authors were involved in the conception and design of the investigation. YO, HT, NMu, ZM, and AM participated in the acquisition of the data. NMo, RS, and RI analyzed the data and interpreted the results. NMo, MP, RS, and RI wrote the manuscript, and all the other authors critically revised it. All the authors approved the final version of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the Director General of Health Malaysia for his permission to publish this article, and the Director of Institute for Medical Research for all the support given toward the development of this article. We also acknowledge the National Institutes of Health (NIH), Ministry of Health Malaysia for approving the research protocol under the code NMRR-20-2757-57599.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.878396/full#supplementary-material
COVID-19, coronavirus disease-2019; HCWs, healthcare workers; IPC, infection prevention and control; MOH, Ministry of Health; PPE, personal protective equipment; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SPSS, Statistical Package for the Social Sciences; WHO, World Health Organization.
1. World Health Organization. WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. (2020). Available online at https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−11-march-2020 (accessed July 8, 2021).
2. World Health Organization. Weekly epidemiological update on COVID-19 - 6 July 2021. (2021). Available online at https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19-6-july-2021 (accessed July 8, 2021).
3. Nguyen LH, Drew DA, Graham MS, Joshi AD, Guo CG, Ma W, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. (2020) 5:e475–83. doi: 10.1016/S2468–2667(20)30164–X
4. Centers for Disease Control Prevention. Scientific Brief: SARS-CoV-2 Transmission. Centers for Disease Control and Prevention. (2021). Available online at https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/SARS-CoV-2-transmission.html (accessed July 8, 2021).
5. World Health Organization. Coronavirus disease (COVID-19): How is it transmitted? (2021). Available online at https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-how-is-it-transmitted (accessed July 8, 2021).
6. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Centers for Disease Control and Prevention. (2021). Available online at https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (accessed July 8, 2021).
7. Occupational Safety Health Administration. COVID-19 - Control and Prevention - Healthcare Workers and Employers Occupational Safety and Health Administration. (2021). Available online at https://www.osha.gov/coronavirus/control-prevention/healthcare-workers (accessed July 8, 2021).
8. World Health Organization. Summary of Probable SARS Cases With Onset of Illness From 1 November 2002 to 31 July 2003. (2003). Available online at https://www.who.int/publications/m/item/summary-of-probable-sars-cases-with-onset-of-illness-from-1-november-2002-to-31-july-2003 (accessed July 8, 2021).
9. World Health Organization. Keep Health Workers Safe to Keep Patients Safe: WHO. (2020). Available online at https://www.who.int/news/item/17-09-2020-keep-health-workers-safe-to-keep-patients-safe-who (accessed January 5, 2022).
10. Pan American Health Organization. COVID-19 has Infected Some 570,000 Health Workers and Killed 2,500 in the Americas, PAHO Director Says—PAHO/WHO Pan American Health Organization. (2021). Available online at https://www.paho.org/en/news/2-9-2020-covid-19-has-infected-some-570000-health-workers-and-killed-2500-americas-paho (accessed July 14, 2021).
11. World Health Organization. The Impact of COVID-19 on Health and Care Workers: A Closer Look at Deaths. Report No.: WHO/HWF/WorkingPaper/2021.1. (2021). Available online at https://apps.who.int/iris/handle/10665/345300 (accessed January 5, 2022).
12. Ministry of Health Malaysia. COVID-19 Malaysia Updates; Lebih 4,000 Petugasbarisanhadapan KKM Dijangkiti COVID-19 - KP Kesihatan. COVID-19 Malaysia. (2021). Available online at http://covid-19.moh.gov.my (accessed July 9, 2021).
13. Covid-19: Over 2 300 Health Workers Infected but None had Severe Symptoms Says Says Adham Baba The Star. TheStar. (2021). Available online at https://www.thestar.com.my/news/nation/2021/07/10/covid-19-over-2300-health-workers-infected-but-none-had-severe-symptoms-says-adham-baba (accessed July 14, 2021).
14. Tan CS, Lokman S, Rao Y, Kok SH, Ming LC. Public and private sectors collective response to combat COVID-19 in Malaysia. J Pharm Policy Prac. (2021) 14:40. doi: 10.1186/s40545-021-00322-x
15. World Health Organization Western Pacific Region. Universal Health Coverage and COVID-19 Preparedness & Response in Malaysia. (2020). Available online at https://www.who.int/malaysia/news/detail/04-09-2020-universal-health-coverage-and-covid-19-preparedness-response-in-malaysia (accessed January 5, 2022).
16. Ashinyo ME, Dubik SD, Duti V, Amegah KE, Ashinyo A, Asare BA, et al. Infection prevention and control compliance among exposed healthcare workers in COVID-19 treatment centers in Ghana: a descriptive cross-sectional study. PLoS ONE. (2021) 16:e0248282. doi: 10.1371/journal.pone.0248282
17. Abed Alah M, Abdeen S, Selim N, Hamdani D, Radwan E, Sharaf N, et al. Compliance and barriers to the use of infection prevention and control measures among health care workers during COVID-19 pandemic in Qatar: a national survey. J Nurs Manag. (2021) 29:2401–11. doi: 10.1111/jonm.13440
18. Wong ELY, Ho KF, Dong D, Cheung AWL, Yau PSY, Chan EYY, et al. Compliance with standard precautions and its relationship with views on infection control and prevention policy among healthcare workers during COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:3420. doi: 10.3390/ijerph18073420
19. Michel-Kabamba N, Ngatu N, Leon-Kabamba N, Katumbo-Mukemo A, Mukuku O, Ngoyi-Mukonkole J, et al. Occupational COVID-19 prevention among congolese healthcare workers: knowledge, practices, PPE compliance, and safety imperatives. Tropical Med. (2020) 6:6. doi: 10.3390/tropicalmed6010006
20. Tsehay A, EndashawHareru H, Molla W, Mengistu N, Kaso AW, Ashuro Z, et al. Factors associated with preventive practices of COVID-19 among health care workers in Dilla University Hospital, Southern Ethiopia. Environ Challenges. (2021) 5:100368. doi: 10.1016/j.envc.2021.100368
21. Ezike OC, Odikpo LC, Onyia EN, Egbuniwe MC, Ndubuisi I, Nwaneri AC, et al. Risk perception, risk involvement/ exposure and compliance to preventive measures to COVID-19 among nurses in a tertiary hospital in Asaba, Nigeria. Int J Africa Nurs Sci. (2022) 16:100385. doi: 10.1016/j.ijans.2021.100385
22. Atnafie SA, Anteneh DA, Yimenu DK, Kifle ZD. Assessment of exposure risks to COVID-19 among frontline health care workers in Amhara Region, Ethiopia: a cross-sectional survey. PLoS ONE. (2021) 16:e0251000. doi: 10.1371/journal.pone.0251000
23. World Health Organization. Risk Assessment and Management of Exposure of Health Care Workers in the Context of COVID-19: Interim Guidance. (2020). Available online at https://apps.who.int/iris/handle/10665/331496 (accessed July 21, 2021).
24. Ministry of Health Malaysia. Policies and Procedures on Infection Prevention and Control. (2019). Available online at https://www.moh.gov.my/moh/press_releases/KKM%20Policies%20&%20Procedures%20on%20Infection%20Prevention%20and%20Control%202019.pdf (accessed January 5, 2022).
25. Ministry of Health Malaysia. Annex 21: Management of Healthcare Workers (HCW) During the COVID-19 Pandemic. (2022). Available online at https://covid-19.moh.gov.my/garis-panduan/garis-panduan-kkm/ANNEX-21-MANAGEMENT-OF-HEALTHCARE-WORKERS-HCW-DURING-THE-COVID-19-PANDEMIC-20022022.pdf (accessed June 6, 2022).
26. Chin ESM. Covid-19: Almost 5,000 healthcare workers infected so far, two-thirds of them women Malay Mail. (2021). Available online at https://www.malaymail.com/news/malaysia/2021/02/05/covid-19-almost-5000-healthcare-workers-infected-so-far-two-thirds-of-them/1947328 (accessed July 14, 2021).
27. Fusco FM, Pisaturo M, Iodice V, Bellopede R, Tambaro O, Parrella G, et al. COVID-19 among healthcare workers in a specialist infectious diseases setting in Naples, Southern Italy: results of a cross-sectional surveillance study. J Hosp Infect. (2020) 105:596–600. doi: 10.1016/j.jhin.2020.06.021
28. Kindgen-Milles D, Brandenburger T, Braun JFW, Cleff C, Moussazadeh K, Mrosewski I, et al. Prevalence of SARS-CoV-2 positivity in 516 German intensive care and emergency physicians studied by seroprevalence of antibodies National COVID survey Germany (NAT-COV-SURV). PLoS ONE. (2021) 16:e0248813. doi: 10.1371/journal.pone.0248813
29. Oda G, Sharma A, Lucero-Obusan C, Schirmer P, Sohoni P, Holodniy M. COVID-19 infections among healthcare personnel in the United States veterans health administration, March to August, 2020. J Occup Environ Med. (2021) 63:291–5. doi: 10.1097/JOM.0000000000002109
30. Gómez-Ochoa SA, Franco OH, Rojas LZ, Raguindin PF, Roa-Díaz ZM, Wyssmann BM, et al. COVID-19 in healthcare workers: a living systematic review and meta-analysis of prevalence, risk factors, clinical characteristics, and outcomes. Am J Epidemiol. (2021) 190:187. doi: 10.1093/aje/kwaa191
31. Cheng VCC, Wong SC, Chen JHK, Yip CCY, Chuang VWM, Tsang OTY, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. (2020) 41:493–8. doi: 10.1017/ice.2020.58
32. Barry M, Robert AA, Temsah MH, Abdul Bari S, Akhtar MY, Al Nahdi F, et al. COVID-19 community transmission among healthcare workers at a tertiary care cardiac center. Med Sci. (2021) 9:49. doi: 10.3390/medsci9030049
33. Shatnawi NJ, Mesmar Z, Al-Omari GA, AL-Sheyab W, AlZoubi NA, AL-Ghazo M, et al. Compliance with safety measures and risk of COVID-19 transmission among healthcare workers. Future Sci OA. (2022) 8:FSO762. doi: 10.2144/fsoa-2021-0094
34. Alao MA, Durodola AO. Ibrahim OR, Asinobi OA. Assessment of health workers' knowledge, beliefs, attitudes, and use of personal protective equipment for prevention of COVID-19 infection in low-resource settings. Adv Public Health. (2020) 2020:e4619214. doi: 10.1155/2020/4619214
35. Turnberg W, Daniell W, Seixas N, Simpson T, Van Buren J, Lipkin E, et al. Appraisal of recommended respiratory infection control practices in primary care and emergency department settings. Am J Infect Control. (2008) 36:268–75. doi: 10.1016/j.ajic.2007.08.004
36. Mostafa A, Kandil S, El-Sayed MH, Girgis S, Hafez H, Yosef M, et al. SARS-CoV-2 seroconversion among 4040 Egyptian healthcare workers in 12 resource-limited healthcare facilities: A prospective cohort study. Int J Infect Dis. (2021) 104:534–42. doi: 10.1016/j.ijid.2021.01.037
37. Gilbert GL, Kerridge I. The politics and ethics of hospital infection prevention and control: a qualitative case study of senior clinicians' perceptions of professional and cultural factors that influence doctors' attitudes and practices in a large Australian hospital. BMC Health Serv Res. (2019) 19:212. doi: 10.1186/s12913-019-4044-y
38. Temsah MH, Alrabiaah A, Al-Eyadhy A, Al-Sohime F, Al Huzaimi A, Alamro N, et al. COVID-19 critical care simulations: an international cross-sectional survey. Front Public Health. (2021) 9:700769. doi: 10.3389/fpubh.2021.700769
39. Arokiasamy JT. Communicable diseases: a continuing threat in Malaysia. Med J Malaysia. (1990) 45:181–6. Available online at: http://www.e-mjm.org/1990/v45n3/Communicable_diseases.pdf
40. Malaysia Major infectious diseases. Indexmundi. (2020). Available online at https://www.indexmundi.com/malaysia/major_infectious_diseases.html (accessed July 15, 2021).
41. Lamhoot T, Ben Shoshan N, Eisenberg H, Fainberg G, Mhiliya M, Cohen N, et al. Emergency department impaired adherence to personal protective equipment donning and doffing protocols during the COVID-19 pandemic. Isr J Health Policy Res.(2021) 10:41. doi: 10.1186/s13584-021-00477-7
42. Osborne S. Influences on compliance with standard precautions among operating room nurses. Am J Infect Control. (2003) 31:415–23. doi: 10.1067/mic.2003.68
43. Nichol K, Bigelow P, O'Brien-Pallas L, McGeer A, Manno M, Holness DL. The individual, environmental, and organizational factors that influence nurses' use of facial protection to prevent occupational transmission of communicable respiratory illness in acute care hospitals. Am J Infect Control. (2008) 36:481–7. doi: 10.1016/j.ajic.2007.12.004
44. Ganczak M, Szych Z. Surgical nurses and compliance with personal protective equipment. J Hosp Infect. (2007) 66:346–51. doi: 10.1016/j.jhin.2007.05.007
45. Yassi A, Lockhart K, Copes R, Kerr M, Corbière M, Bryce E, et al. Determinants of healthcare workers' compliance with infection control procedures. Healthc Q. (2007) 10:44–52. doi: 10.12927/hcq.2007.18648
46. Klompas M, Karan A. Preventing SARS-CoV-2 transmission in health care settings in the context of the omicron variant. JAMA. (2022) 327:619–20. doi: 10.1001/jama.2022.0262
47. Temsah MH, Alenezi S, Alarabi M, Aljamaan F, Alhasan K, Assiri R, et al. Healthcare workers' SARS-CoV-2 omicron variant uncertainty-related stress, resilience, and coping strategies during the first week of the world health organization's alert. Int J Environ Res Public Health. (2022) 19:1944. doi: 10.3390/ijerph19041944
48. Temsah MH, Aljamaan F, Alenezi S, Alhasan K, Alrabiaah A, Assiri R, et al. SARS-CoV-2 omicron variant: exploring healthcare workers' awareness and perception of vaccine effectiveness: a national survey during the first week of who variant alert. Front Public Health. (2022) 10:878159. doi: 10.3389/fpubh.2022.878159
Keywords: healthcare workers, infection control practices, risk, pandemic, COVID-19
Citation: Mohamad N, Pahrol MA, Shaharudin R, Md Yazin NKR, Osman Y, Toha HR, Mustapa N, Mohamed Z, Mohammad A and Ismail R (2022) Compliance to Infection Prevention and Control Practices Among Healthcare Workers During COVID-19 Pandemic in Malaysia. Front. Public Health 10:878396. doi: 10.3389/fpubh.2022.878396
Received: 18 February 2022; Accepted: 20 June 2022;
Published: 18 July 2022.
Edited by:
Thomas H. Gassert, Harvard University, United StatesReviewed by:
Kun-Shan Wu, Tamkang University, TaiwanCopyright © 2022 Mohamad, Pahrol, Shaharudin, Md Yazin, Osman, Toha, Mustapa, Mohamed, Mohammad and Ismail. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nadia Mohamad, nadia@moh.gov.my
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.