
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 26 August 2022
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.972249
 Yin Cheng Lim1,2*
Yin Cheng Lim1,2* Ameerah Su'ad Abdul Shakor1
Ameerah Su'ad Abdul Shakor1 Nadia Mohamad1
Nadia Mohamad1 Muhammad Alfatih Pahrol1
Muhammad Alfatih Pahrol1 Rohaida Ismail1
Rohaida Ismail1 Zhuo Lin Chong3
Zhuo Lin Chong3 Mohd Hatta Abdul Mutalip3
Mohd Hatta Abdul Mutalip3 Mohd Azahadi Omar4
Mohd Azahadi Omar4 Mahmoud Danaee2Guo Tung Wan5
Mahmoud Danaee2Guo Tung Wan5 Rafiza Shaharudin1
Rafiza Shaharudin1Background: Existing anthropometric studies for respirator designs are based on the head and facial dimensions of Americans and Chinese nationals, with no studies for multi-ethnic countries like Malaysia. This study aimed to create head and facial morphological database for Malaysia, specifically to identify morphological differences between genders, ethnicities, and birthplaces, as well as predictors of the dimensions.
Design: A cross-sectional study.
Setting: Malaysia.
Participants: A nation-wide cross-sectional study using a complex survey design with two stage-stratified random sampling was conducted among 3,324 participants, aged 18 years and above who were also participants of the National Health and Morbidity Survey 2020.
Primary and secondary outcomes: The study collected data on sociodemographic, measurement of Body Mass Index (BMI) and 10 head and facial dimensions (3 dimensions were measured using direct measurement, and 7 others using Digimizer software for 2-dimension images). Linear regression was performed to determine the association between gender, ethnicity, birthplace, age and BMI and the dimensions.
Results: There were significant differences in all the dimensions between sex, birthplace and ethnicity (p < 0.005). Further analysis using linear regression showed sex, ethnicity, birthplace, age and BMI were significant predictors of the dimensions. In comparison to studies from the United States and China, our study population had a wider interpupillary distance and nose breadth for both male and female participants, but smaller bigonial breadth and smaller minimal frontal breadth.
Conclusion: These findings could assist in the design and sizing of respirators that will fit Malaysians and possibly other Southeast Asian population.
The respirator is an essential element of human respiratory Personal Protective Equipment (PPE) against airborne pollutants. However, in order to be an efficient PPE, respirators must appropriately suit the size and shape of users' faces; otherwise, pollutants will enter the users' respiratory system and endanger their lives. As a result, ensuring an appropriate fit of the respirator for the target population is a crucial challenge in developing respirators.
A correctly fitting respirator is determined by several factors, including user's head and facial size, design of the respirator, and user's activities while wearing the respirator. Among these, facial dimensions in relation to respirator design have been discovered to be critical in inward leakage of respirators (1, 2). Head and facial dimensions have been shown to differ depending on ethnicity, gender, age, BMI, and geographic location (3–6). The study among United State of America's population indicated significant differences in head and facial measurements across ethnic groups and sex (3). A study among lecturers and students at a University in China showed that Chinese have shorter and wider facial dimension than Americans (4). Even within China, the studies also showed there were differences in the measurements of bitragion chin arc, face length, nose length, and nose protrusion between workers born in the north as compared to workers born in the south (5). Another study compared facial dimensions between Koreans and Japanese and found that the later had greater minimal frontal breadth, interpupillary distance, face length, nose breath, and nose height (6). Differences in head and facial dimensions were observed as the population aged, with participants aged 45 years and older having greater size in 13 facial dimensions as compared to those aged between 18 and 29 years old, with the most prominent difference being in the lip length, nose breadth, and subnasale-sellion length (3).
To ensure proper fit of respirators to targeted or intended users, new models of respirators in the United States and China are required to meet the requirements of certification from National Institute Occupational Safety and Health (NIOSH) and the State Administration of Work Safety, respectively, prior to marketing (7). The facepiece of respirators is fit-tested on a panel of human subjects with head and facial sizes representative of the user population, conventionally being the population in the nation of the geographical area where the respirators are designed and manufactured. The respirator fit test panel (RFTP) is typically used as a matrix for selection of candidates to serve as the representative test subjects in this process (7). In the late 1960s, the Respirator Research and Development Section of the Los Alamos National Laboratory (LANL) developed RFTPs for fit testing based on head and facial anthropometrics of personnel serving in the United States' Air Force (8). The full facepiece fit test panel was based on the bivariate distribution of face length and face width while the half facepiece fit test panel was based on the bivariate distribution of the face length and lip length. There has long been a concern about the applicability of fit test panels, generated from military personnel, for civilian workers.
In 2003, the National Institute for Occupational Safety and Health (NIOSH) had conducted a head-and-face anthropometric survey on 3997 US civilian workers (9). Based on the results of this large-scaled anthropometric survey, a bivariate panel using face length and face width, as well as a principal component analysis (PCA) panel using 10 head and facial dimensions, were created. The study revealed that the 10 dimensions were associated with respirator fit and leakage and predicted well the remaining head and facial dimensions (9). Therefore, respirators designed to fit these panels were expected to suitably accommodate more than 95% of the current US civilian workers. The authors concluded that both panels were more representative of the US population than the existing LANL panel. The inclusion of the eight additional head and facial dimensions allows the PCA panel to provide better criteria for excluding extreme face sizes from being used. In China, two Chinese RFTPs were developed following the methods adopted in developing the NIOSH bivariate and PCA RFTPs (10). The RFTP was found to be able to accommodate at least 95% of the surveyed Chinese workers. The findings also showed that up to 35% of Chinese residents were excluded from test panels developed for an American workforce (10).
Locally, there is a lack of evidence on head and facial anthropometric data, despite several published studies among Malaysian (11–16). Generally, their study sample size was quite small with <300 participants and it did not include all ethnicities. Two of the studies focused solely on nasolabial and mentolabial dimensions (11, 16), whereas another study attempted to compare differences in the nasofacial length and width between three races in Malaysia (15). Moreover, there are no available data from the neighboring countries as well, except one study conducted among Javanese females (17). The study found that there were significant disparities in the facial dimensions between Javanese and white women.
Given that findings from previous studies showed there were differences in the head and facial dimensions of population from different continents, and no previous head and facial anthropometric studies for multi-ethnicity nations such as Malaysia have been conducted, a study aimed to establish head and facial morphological database for Malaysians was conducted. It also aimed to identify morphological differences among gender, age, ethnicity and birthplace and to determine the predictors that may influence head and facial dimensions.
This was a nation-wide population based cross-sectional study using complex sample design involving direct measurement and analysis of 2D photogrammetry among participants in the National Health and Morbidity Survey (NHMS) 2020 by the Institute for Public Health, National Institute of Health Malaysia. The detailed description of sampling method had been described in NHMS 2020 report (18). Sampling frame for this study were based on the updated National Population and Housing Census 2020, provided by Department of Statistics Malaysia (DOSM). It included Malaysian residents of non-institutionalized living quarters in both rural and urban areas from all 13 states and three Federal Territories. Malaysia was divided into Enumeration Blocks (EB), which are arbitrarily geographically contiguous areas with defined boundaries. For each EB has an average of 80–120 Living Quarters (LQ) and a population of 500–600 people of all ages. A cluster size of 20 LQs were selected from each selected EB.
We employed two-stage stratified random sampling. The first stratum included all Malaysian states, and the second stratum included urban and rural localities within each state. The sampling processes was divided into two stages: the Primary Sampling Unit (PSU), which is the Enumeration Block (EBs), and the Secondary Sampling Unit (SSU), which is the Living Quarters (LQs) within the chosen EBs. The PSU and SSU were randomly selected by DOSM based on the required sample size. A total of 2,260 LQs were chosen from 113 EBs in Malaysia (83 EBs from Peninsular Malaysia, 13 EBs from Sabah, and 17 EBs from Sarawak). Participants were allocated proportionately to states, urban and rural, based on population size. Thus, more samples were allocated to states with larger population sizes, such as Selangor, Johor, Sabah, and Sarawak. A lesser number of samples were allocated to states with smaller population sizes, such as Perlis, Melaka, and Wilayah Persekutuan Putrajaya.
We used scouts to identify specific LQs from each EB. Scouting activities were based on DOSM-supplied maps and household lists. We identified selected LQs from each EB, updated the list of household members, and tagged the selected LQs. The survey was then informed to the head of household, household members, community leader and relevant government bodies. We contacted survey participants to schedule a team visit and survey appointment. Any Malaysian resident of the area who was 18 years old and older was eligible to participate. Participants with dental or facial deformities, as well as those who objected to shaving their beard and mustache, were excluded from taking part.
Socio-demographic data on age, sex, ethnicity and birthplaces was collected through a self-administered questionnaire.
Physical examination was performed by trained research assistants. Weight was measured to the nearest 0.1 kg using a digital scale (TANITA model HD 309) which has the intracluster Correlation (ICC) of 0.99 (19) and height was measured using a tape measure.
The 10 selected morphological points were located by inspection and/or palpation in accordance with the 1988 Anthropometric Survey of the US Army Personnel Project (20). Spreading calipers were used to measure head breadth, bizygomatic breadth and bigonial breadth, which is considered the gold standard for head and facial measurement (21) (Table 1). During the measurement process, the investigators attempted to ensure that the participants were comfortable and sitting with a natural head position and relaxed lips.
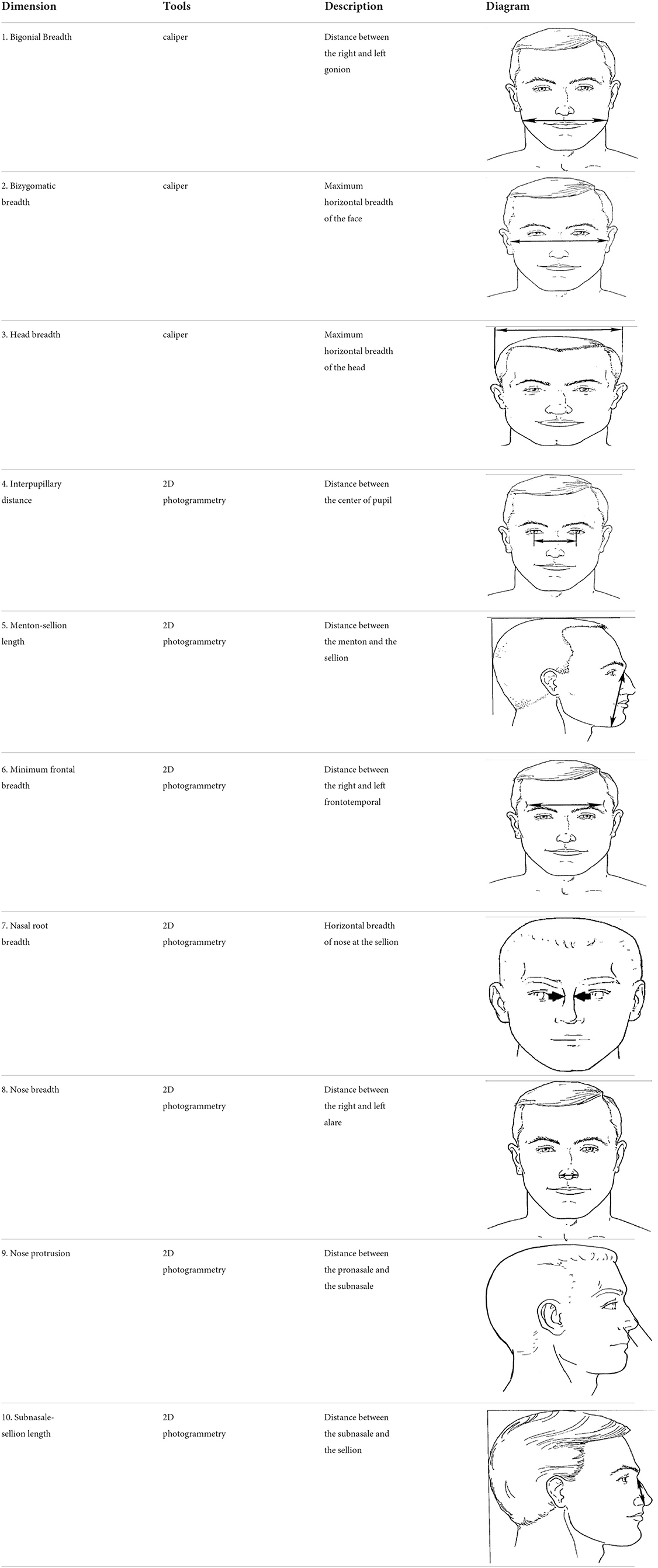
Table 1. Head and facial dimensions and landmarks [7].
The participants' images were captured using a 20.0-megapixel digital camera (Canon IXUS 190, Tokyo, Japan) positioned on a tripod (Manfrotto MKCOMPACTLT-BK, Cassola, Italy) at a fixed distance of 1.0 m. For each participant, one anterior and one lateral photo were taken.
All images were captured in JPEG format and were transferred to a computer after each day of shooting. The anthropometric dimensions were calculated using the software package Digimizer version 5.4.4. Details of 2D photogrammetry methods can be found in previously published paper (22). This method has been found to have high reliability (ICC ranged between 0.85 and 0.99), and high validity as demonstrated by the Bland-Altman analyses for the seven head and facial dimensions.
Complex sample analysis was used to obtain prevalence and population estimates with 95% confidence intervals. Prior to the analysis, sample weights were calculated for each respondent to improve the sample's representativeness in terms of the size, distribution, and characteristics of the study population. Basic weight for each sampled household would be the inverse of its selection probability (calculated by multiplying the probabilities at each sampling stage). To calculate the sample weights, the basic weight was adjusted based on the non-response and post-stratification factors.
Statistical Package for Social Science SPSS Statistics (SPSS) version 26 was used for analysis. Descriptive analysis for continuous data was presented as mean with standard deviation considering the dataset was large and normality was assumed. Categorical data were presented in frequency and column percentage. The independent sample t-test was used to calculate the difference in means between groups whereas Cohen's d was used to determine effect size due to the large sample size.
Linear regression analysis was conducted to determine the effect of age, gender, ethnicity, birthplace and BMI on head and facial dimensions. Ten head and facial dimensions served as dependent variables, while sex, ethnicity, birthplace, age, and BMI served as independent variables. Age and BMI were treated as continuous variables. Sex, ethnicity, and birthplaces were treated as categorical data with two categories. Female, non-Malay and birthplace in West Malaysia were treated as the reference group.
Cluster analysis was employed to optimize and group participants based on multivariate similarities across samples. The Multivariate Analysis of Variance (MANOVA) test was used to determine the number of groups that needed to be examined for the cluster analysis.
The study participants were not involved in the development of this study. The results of the study were not shared with the participants.
A total of 3,324 participants from all over Malaysia participated in this study. The mean age for participants was 43.0 ± 16.2, with a nearly equal male to female ratio. Majority of the participants were from West Malaysia (71.9%). Malay ethnic group accounted for 64.0% of the population, followed by Chinese (9.8%), Indigenous Sarawak (8.9%), Indigenous Sabah (7.8%), Indian (5.3%), and others (4.2%).
All ten head-and-face anthropometric dimensions measured in males were larger than in females, with a significant difference (p < 0.005) in sizes (Table 2). The findings also revealed that all head-and-face anthropometric dimensions differed significantly across birthplaces and ethnicity. Effect size measurement using Cohen's d showed that the effect is large for all the dimensions between sex (Cohen's d ≥ 0.8).
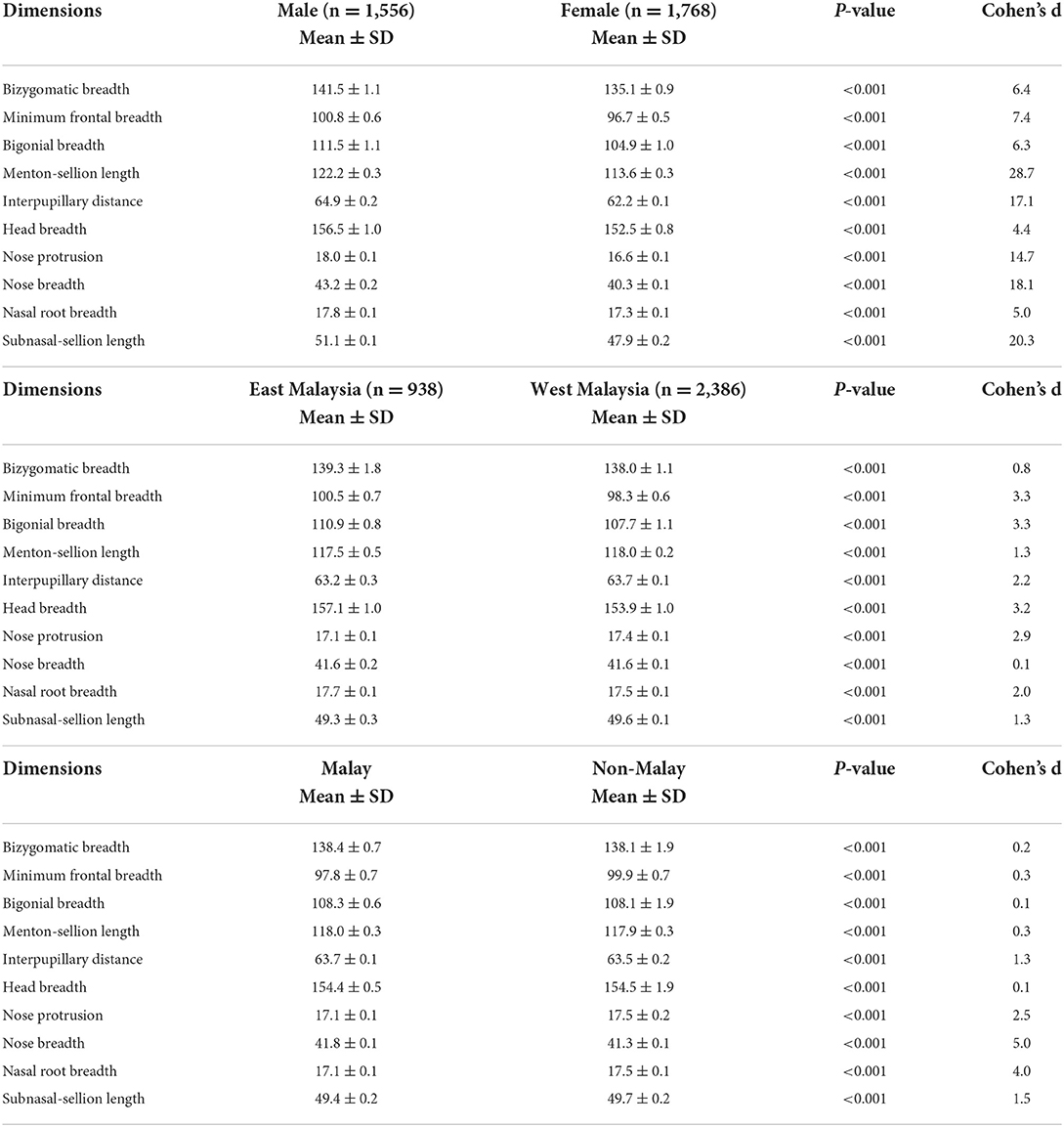
Table 2. Weighted head and facial dimensions according to sex, birthplace and race.
Table 3 showed a summary of anthropometric statistics for males and females based on Mean, SD, Minimum, Maximum, Skewness, Kurtosis and Percentiles P5, P50, and P95. It was worth noting that the mean and standard deviation has been weighted to represent the Malaysian population.
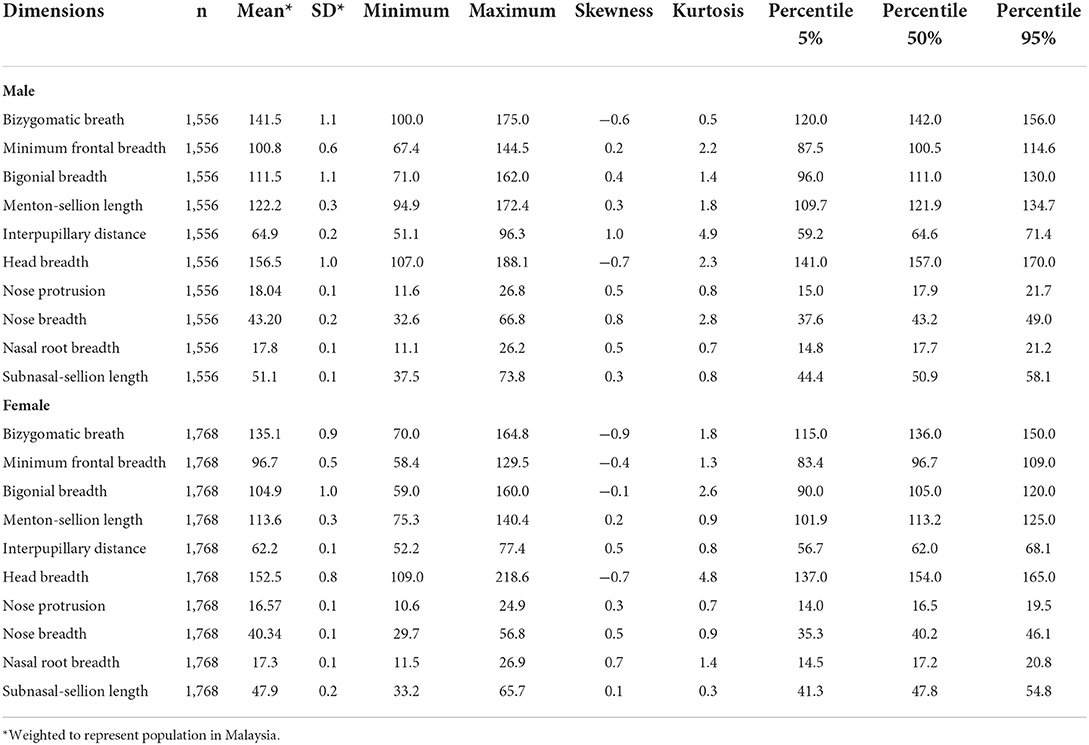
Table 3. Head and facial dimensions by sex according to Mean, Minimum, Maximum, Skewness, Kurtosis, Percentiles P5%, P50%, P95%.
Head and facial dimensions have been found to be affected by various factors including sex, ethnicity, birthplaces, age, and BMI (Table 4). Sex was found to be a significant predictor for all the ten head and facial dimensions, with p < 0.001. These predictors can explain 3–29 percent of the variation (adjusted R2) in the desired outcome, with the most variation seen for menton-sellion length.
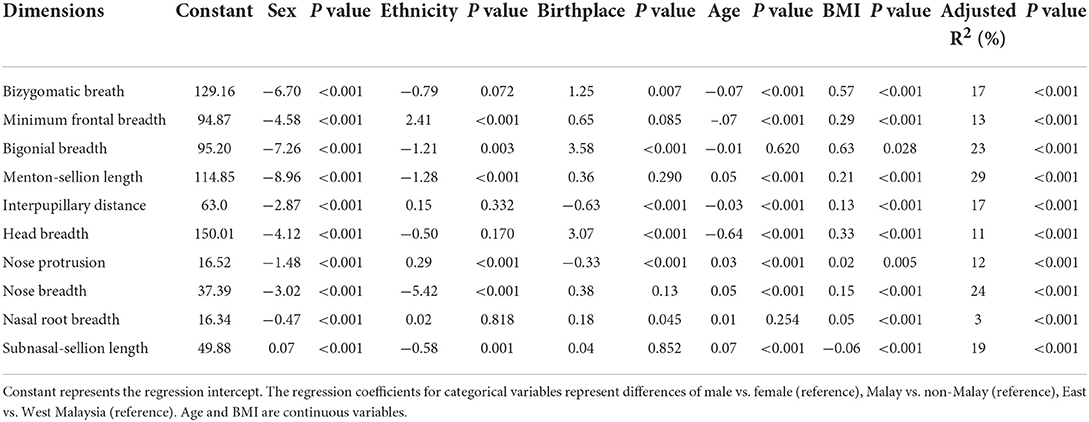
Table 4. The regression coefficients of regression analysis for anthropometric measurements by sex, ethnicity, birthplace, age, and BMI.
In Table 5, we compared our findings among males and females to two previous studies with large sample sizes (China and NIOSH respiratory participants from the United States). The male participants in our study had smaller bizygomatic breadth, minimal frontal breath, bigonial breadth, and nose protrusion than the male participants in the comparison studies. Only two facial dimensions, interpupillary distance and nose breadth, were greater than those of the Chinese and NIOSH respirator studies. The menton-sellion and subnasal-sellion lengths were found to be shorter in the Chinese study but longer in the NIOSH study, whereas head breath was found to be larger in the Chinese study but smaller in the NIOSH study. The Chinese study had a wider nasal root breadth than this study, whereas this data was not available for the NIOSH study.
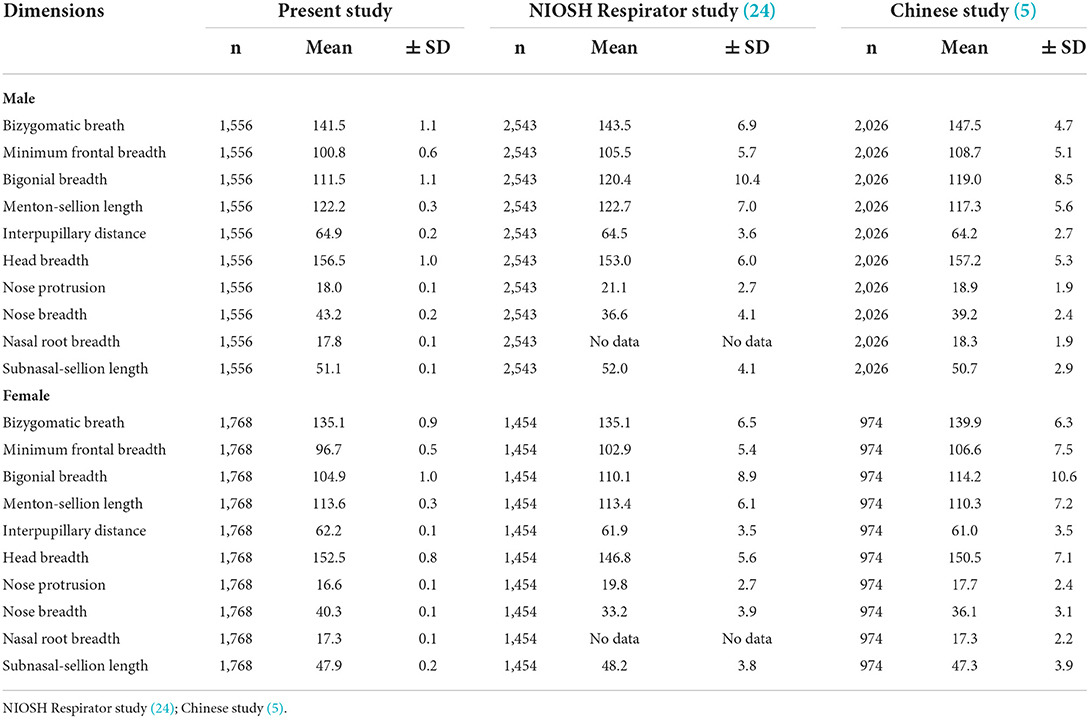
Table 5. Comparison of head and facial anthropometric measurement by sex in the current study, the NIOSH Respirator study, and the Chinese study.
Four of the head and facial dimensions (interpupillary distance, head breadth, nose breadth and menton sellion) in our female participants were found to be the largest when compared to participants in the NIOSH respirator and Chinese study (Table 5). The bizygomatic breadth was of similar length as the NIOSH respirator study, but shorter than the Chinese study. Both our study and the Chinese study had the same nasal root length, but no comparison could be made for the NIOSH study. Our study had a narrower frontal breadth, a narrower bigonial breadth, and a shorter nose protrusion than the other two studies.
The participants were divided into ten groups using cluster analysis based on their homogeneity (Supplementary Table 1). From the MANOVA, Wilk's Lamda of ten groups yielded the highest result. The first group contained 0.99% of the samples, the second group contained 0.5%, and the remaining eight groups contained 0.4%.
There were significant differences in means of the head and facial anthropometric dimensions between sex, ethnicity and birthplace. A large sample size of more than 3,000 participants may have contributed to the statistical significance across groups for this study. In contrast, effect size is independent of the sample size (23). Thus, effect size was examined in the current study. The findings of current study showed that the differences between sex had a large effect size (≥0.8) across all 10 dimensions. Our findings are in accordance with previous local and international studies that showed statistically and practically significant differences in dimensions between sex (5, 14, 24, 25). It is worth noting that we are the only study which examined effect size in comparison to previous studies, thus comparison cannot be made.
Further analysis using Linear model showed that sex, ethnicity, birthplace, age and BMI were predictors for head and facial dimensions. Analysis using backward deletion model showed that sex (independent variable) was a significant predictor for all the 10 head and facial dimensions, followed by birthplace (independent variable), which affected all dimensions except subnasale-sellion length and BMI (independent variable), which influenced all dimensions except minimal frontal breadth.
When compared to participants from the United States (3) and China (5), our study population had a wider interpupillary distance and nose breadth for both male and female participants, but smaller bigonial breadth and minimal frontal breadth. However, we were not able to determine the statistical difference, as we did not have individual data of previous studies. Differences in the head and facial dimensions between these studies may have been influenced by genetic (26), environmental factors (27) and even the interaction of these two factors (28). Genetic factors have been proposed to play a significant role in the variation of head and facial dimensions (26). Whilst, environmental factor such as extreme temperature and humidity in the winter have been found to be associated with mid-facial morphology (27).
We acknowledge that the current study had some limitations. Head and facial anthropometry was not measured using the 3D stereophotogrammetry, but it should be noted that direct measurement and 2D photogrammetry were both validated tools for measuring head and facial anthropometry, and they are more feasible for a nationwide population study, particularly when conducted during the COVID-19 pandemic in 2020 to reduce contact time with participants. Another limitation is the lack of occupational information, which has been shown to be a significant predictor of head and facial dimensions (3). Our study population differed from previous study in that it was conducted among communities rather than across workplace sectors (3). Notably, while respirators are typically employed to protect workers against chemical and biological hazards in the workplace, respirators are particularly crucial during pandemics caused by airborne transmission, such as SARS-CoV-2. Furthermore, respirators are usually designed based on head and facial dimensions rather than occupations. Finally, the height was measured with a tape measure rather than a stadiometer. The main issue is that because our study was conducted in a community context, the rod could not be installed in certain locations due to uneven flooring. To minimize measurement bias, we used measurement tape that was specifically printed with stickers and taped to the walls and tent poles.
The main strength of current study is that it is the first large nationwide study on head and facial anthropometry of different ethnic groups in Malaysia with over 3,000 participants. Our total number of participants (3,324) was higher than that of the Chinese study (3,000) (5), but lower than that of the NIOSH study (3,997) (3). In comparison to the previous two large nationwide studies, our participants have almost equal number of male and female. Other strength of this study is the combination of direct and 2D measurement methods. This also indicate the important role that 2D photogrammetry, which has been shown to have high validity and reliability, can play in assessing specific head and facial morphologies in countries with limited 3D scanner resources. Another highlight of this study was the use of complex sample for analysis. It is essential in a multi-stage stratified sampling because it increases the precision of sample and ensures a representative sample from key groups (29).
Despite the fact that we have a multi-ethnic population, the cluster analysis revealed that our samples were very homogeneous, with more than 0.99% of our samples classified into the same group. This is surprising given that we have observed significant differences in the majority of head and facial dimensions across ethnicities and birthplaces. This data, however, indicated that, despite our different ethnicities, our genetics (28) affecting head and facial dimensions between ethnicities are likely to be comparable. The significance of this study was that the findings enabled us to uncover differences in dimensions between populations. We could use this information to consider the need of developing our own local respirators against biological and chemical hazards. We believe that our findings could assist in the design and sizing of respirators for Malaysians and possibly other Southeast Asian population because we share certain similarities.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical approval was obtained from Medical Research and Ethics Committee (NMRR-20-1217-55489). Informed consent was obtained from all individual participants included in the study. The patients/participants provided their written informed consent to participate in this study.
The study conception was by YCL, RS, and GTW. YCL and RS designed the study. YCL, ASAS, NM, MAP, RI, ZLC, and MHAM collected the data. YCL, ASAS, NM, MAP, MAO, MD, and RS conducted the statistical analysis and interpreted the results. YCL, ASAS, NM, and RS drafted the manuscript. All authors have read and approved the final version of the submitted manuscript.
Funding for this study and publication were by the Ministry of Health, Malaysia.
The authors would like to thank the Director General of Health, Malaysia, for his permission to publish this paper. The authors are most grateful to all the participants of this study. We would also like to thank Dr. Ziqing Zhuang for his valuable inputs about his studies that assisted us in conducting ours.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.972249/full#supplementary-material
1. Lin YC, Chen CP. Characterization of small-to-medium head-and-face dimensions for developing respirator fit test panels and evaluating fit of filtering facepiece respirators with different faceseal design. PLoS ONE. (2017) 12:e0188638. doi: 10.1371/journal.pone.0188638
2. Kim H, Han DH, Roh YM, Kim K, Park YG. Facial anthropometric dimensions of Koreans and their associations with fit of quarter-mask respirators. Ind Health. (2003) 41:8–18. doi: 10.2486/indhealth.41.8
3. Zhuang Z, Landsittel D, Benson S, Roberge R, Shaffer R. Facial anthropometric differences among gender, ethnicity, and age groups. Ann Occup Hyg. (2010) 54:391–402. doi: 10.1093/annhyg/meq007
4. Yang L, Shen H, Wu G. Racial differences in respirator fit testing: a pilot study of whether American fit panels are representative of Chinese faces. Ann Occup Hyg. (2007) 51:415–21. doi: 10.1093/annhyg/mem005
5. Du L, Zhuang Z, Guan H, Xing J, Tang X, Wang L, et al. Head-and-face anthropometric survey of Chinese workers. Ann Occup Hyg. (2008)52:773–82. doi: 10.1093/annhyg/men056
6. Lee H-J, Park S-J. Comparison of Korean and Japanese head and face anthropometric characteristics. Hum Biol. (2008) 80:313–30. doi: 10.3378/1534-6617-80.3.313
7. Zhuang Z, Bradtmiller B, Shaffer RE. New respirator fit test panels representing the current U. S civilian work force. J Occup Environtal Hygiene. (2007) 4:647–59. doi: 10.1080/15459620701497538
8. Hack AL, Bradley OD, Trujillo A. Respirator protection factors: Part II-protection factors of supplied-air respirators. Am Ind Hyg Assoc J. (1980) 41:376–81. doi: 10.1080/15298668091424915
9. Zhuang Z, Coffey CC, Ann RB. The effect of subject characteristics and respirator features on respirator fit. J Occup Environ Hyg. (2005) 2:641–49. doi: 10.1080/15459620500391668
10. Chen W, Zhuang Z, Benson S, Du L, Yu D, Landsittel D, et al. New respirator fit test panels representing the current Chinese civilian workers. Ann Occup Hyg. (2009) 53:297–305. doi: 10.1093/annhyg/men089
11. Al-Khatib AR, Rajion ZA, Masudi SA, Hassan R, Anderson PJ, Townsend GC. Stereophotogrammetric analysis of nasolabial morphology among Asian Malays: influence of age and sex. Cleft Palate Craniofac J. (2012) 49:463–71. doi: 10.1597/11-151
12. Ngeow WC, Aljunid S. Craniofacial anthropometric norms of Malaysian Indians. Indian J Dental Res. (2009) 20:313. doi: 10.4103/0970-9290.57372
13. Ngeow WC, Aljunid S. Craniofacial anthropometric norms of Malays. Singapore Med J. (2009) 50:525.
14. Othman SA, Majawit LP, Wan Hassan WN, Wey MC, Mohd Razi R. Anthropometric study of three-dimensional facial morphology in Malay adults. PLoS ONE. (2016) 11:e0164180. doi: 10.1371/journal.pone.0164180
15. Wai MM, Thwin SS, Yesmin T, Ahmad A, Adnan AS, Hassan AA, et al. Nasofacial anthropometric study among university students of three races in Malaysia. Adv Anatom. (2015) 2015:780–86. doi: 10.1155/2015/780756
16. Lin CS, Shaari R, Alam MK, Rahman SA. Photogrammetric analysis of nasolabial angle and mentolabial angle norm in Malaysian adults. Bangl J Med Sci. (2013) 12:209–19. doi: 10.3329/bjms.v12i2.14951
17. Reksodiputro MH, Koento T. Boedhihartono, Sclafani AP. Facial anthropometric analysis of the Javanese female. Arch Facial Plast Surg. (2009) 11:347–9. doi: 10.1001/archfaci.2009.59
18. Institute for Public Health. National Health and Morbidity Survey (NHMS) 2020: Communicable Diseases. National Institutes of Health (NIH) (2020).
19. Geeta A, Jamaiyah H, Safiza MN, Khor GL, Kee CC, Ahmad AZ, et al. Reliability, technical error of measurements and validity of instruments for nutritional status assessment of adults in Malaysia. Singapore Med J. (2009) 50:1013.
20. Gordon CC, Churchill T, Clauser CE, Bradtmiller B, McConville JT. Anthropometric Survey of US Army Personnel: Methods and Summary Statistics 1988. Yellow Springs, OH: Anthropology Research Project Inc (1989).
21. Farkas LG, Posnick JC, Hreczko TM. Anthropometric growth study of the head. Cleft Palate-Craniofacial J. (1992) 29:303–08. doi: 10.1597/1545-1569_1992_029_0303_agsoth_2.3.co_2
22. Lim YC, Abdul Shakor AS, Shaharudin R. Reliability and accuracy of 2D photogrammetry: a comparison with direct measurement. Front Public Health. (2021) 9:813058. doi: 10.3389/fpubh.2021.813058
24. Zhuang Z, Bradtmiller B. Head-and-face anthropometric survey of U. S. respirator users. J Occup Environ Hyg. (2005) 2:567–76. doi: 10.1080/15459620500324727
25. Zhuang Z, Shu C, Xi P, Bergman M, Joseph M. Head-and-face shape variations of U. S civilian workers. Appl Ergon. (2013) 44:775–84. doi: 10.1016/j.apergo.2013.01.008
26. Roosenboom J, Hens G, Mattern BC, Shriver MD, Claes P. Exploring the underlying genetics of craniofacial morphology through various sources of knowledge. Biomed Res Int. (2016) 2016:3054578. doi: 10.1155/2016/3054578
27. Evteev A, Cardini AL, Morozova I, O'Higgins P. Extreme climate, rather than population history, explains mid-facial morphology of Northern Asians. Am J Phys Anthropol. (2014) 153:449–62. doi: 10.1002/ajpa.22444
28. Hallgrimsson B, Mio W, Marcucio RS, Spritz R. Let's face it—complex traits are just not that simple. PLoS Genet. (2014) 10:e1004724. doi: 10.1371/journal.pgen.1004724
Keywords: bivariate, face dimensions, facial size, respiratory fits test, respirators sizing, craniofacial
Citation: Lim YC, Abdul Shakor AS, Mohamad N, Pahrol MA, Ismail R, Chong ZL, Abdul Mutalip MH, Omar MA, Danaee M, Wan GT and Shaharudin R (2022) Head and face anthropometric study for respirators in the multi-ethnic Asian population of Malaysia. Front. Public Health 10:972249. doi: 10.3389/fpubh.2022.972249
Received: 27 June 2022; Accepted: 02 August 2022;
Published: 26 August 2022.
Edited by:
Kewal Krishan, Panjab University, IndiaReviewed by:
Chiranjivi Adhikari, Indian Institute of Public Health Gandhinagar (IIPHG), IndiaCopyright © 2022 Lim, Abdul Shakor, Mohamad, Pahrol, Ismail, Chong, Abdul Mutalip, Omar, Danaee, Wan and Shaharudin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yin Cheng Lim, bGlteWNAdW1tYy5lZHUubXk=; eWNsaW01MjlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.