
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 27 October 2021
Sec. Public Mental Health
Volume 12 - 2021 | https://doi.org/10.3389/fpsyt.2021.733544
 Greta Castellini1,2
Greta Castellini1,2 Lorenzo Palamenghi1,2,3
Lorenzo Palamenghi1,2,3 Mariarosaria Savarese1,2*
Mariarosaria Savarese1,2* Serena Barello1,3,4
Serena Barello1,3,4 Salvatore Leone5
Salvatore Leone5 Enrica Previtali5Alessandro Armuzzi6Guendalina Graffigna1,2,3
Enrica Previtali5Alessandro Armuzzi6Guendalina Graffigna1,2,3Objective: This study aimed to evaluate the impact of the COVID-19 emergency on patients with IBD's psychological distress, understanding the role of patient engagement as a mediator.
Methods: An online questionnaire was created, measuring perceived risk susceptibility toward COVID-19, perceived stress, and patient engagement. The questionnaire was distributed to a purposive sample of IBD patients who belonged to the Italian Association for patients with IBD (AMICI Onlus) in April 2020. Structural equation models were implemented.
Results: The effect of the perceived risk susceptibility toward COVID-19 contagion on the perceived stress is fully mediated by patient engagement (β = 0.306, p < 0.001). Moreover, the patient engagement mitigates the perceived stress (β = −0.748, p < 0.001) in our sample of IBD patients, and it is negatively influenced by the perceived risk susceptibility toward COVID-19 (β = −0.410, p < 0.001).
Conclusion: Patient engagement is the key factor that explains how the perceived risk susceptibility toward COVID-19 affects the perceived psychological distress in patients with IBD, underlining that the perceived risk of contagion increases their perceived level of stress through a decrease of patient engagement.
On February 21, 2020, the pandemic of COVID-19 started to spread in Italy, with the first group of cases identified in the northern part of the country. In a few weeks, the disease spread all over the country: by the end of March, there were already more the 100,000 total cases, with more than 11,000 deaths. The pandemic itself, the constant media reports of deaths and new cases, and the measures enacted to slow down the spread (e.g., lockdown, wearing gloves and masks, social distancing, etc.) exerted an important psychological impact on the general population (1), also in terms of anxiety, depression, and distress (2–4).
These psychological outcomes are particularly relevant for more fragile populations, such as chronic patients: for instance, it is known that patients with inflammatory bowel diseases (IBD) normally have higher levels of general psychological distress when compared to the general population (5), in particular depending on the disease activity (6). Additionally, as previous research shows, patients with IBD—and in particular those with comorbidities or a suppressed immune system—have a high fear of infection and reported leaving their homes less (e.g., for going at the supermarket) (7), which combined with preventive measures enacted to prevent the spread of COVID-19 such as quarantines and lockdown, may have forced a change in daily habits of patients with IBD, potentially impacting their psychological ability to engage in effective health management.
This combination of high-perceived risk of infection and change in daily patterns may have exerted an important impact on patients with IBD's psychological well-being and, in particular, on their levels of perceived psychological distress. Perceived psychological distress should be monitored with caution in patients with IBD, as it is known to be associated with an increased disease activity (8).
It is then important to evaluate the impact that the COVID-19 emergency and, in particular, the perceived risk of infection may have exerted on patients with IBD's psychological distress, as understanding the dynamic behind this stressor-outcome relationship will help tailor more effective and targeted interventions to ease the burden. For this very reason, it is also important to understand whether there are other subjective, psychological characteristics of the patients that can help explain the existing relationship between patients' perceived risk of infection and the perceived psychological distress. Our claim is that the patients' engagement in health management during this COVID-19 emergency mediates the relationship between the perceived susceptibility to COVID-19 and the generated perceived distress. The ability to deal with a difficult situation and the consequent psychological adjustment, in fact, have been demonstrated to be mediators between risk perception and psychological well-being or other psychological outcomes (9, 10).
This could be due to the fact that a higher degree of perceived health risk (namely, in the case of COVID-19, the perceived susceptibility to the infection) could disrupt the psychological readiness of the patients to engage in one's health management and adapt to the new situation. In turn, it is well known that perception to be unable to actively engage in one's health management in unexpected situations—together with the consequent negative emotions elicited from this experience—can lead to high levels of psychological distress (11, 12). In particular, the research carried out by Liu et al. (13) during the COVID-19 emergency demonstrated that the psychological adaptation could be an important factor in identifying stress-prone individuals during a pandemic. Conversely, a more engaged patient has been identified as less distressed in response to a perceived risk or sudden change (14) and more capable of managing his own health (15), which are aspects particularly challenged by this pandemic. In particular, previous studies revealed that a higher level of patient engagement promotes important outcomes for IBD patients, such as an increased health-related quality of life (16), and has been proposed as an important ingredient to promote IBD patients' psychosocial wellbeing (17). Finally, a more engaged patient has been found to better cope with negative emotions and panic, even during quarantine (18, 19).
However, little is known about this aspect in patients with IBD in the specific context of COVID-19 emergency. Following from these premises, our hypotheses are that (Figure 1):
1. A higher level of perceived risk susceptibility toward COVID-19 contagion corresponds to a lower level of patient engagement in one's own health management during the COVID-19 emergency;
2. A higher level of patient engagement in one's own health management during the COVID-19 emergency is a precursor of a lower level of perceived stress;
3. As a consequence of the previous hypotheses, the study assumes that the effect of the perceived risk susceptibility toward COVID-19 contagion on the perceived stress is mediated, at least partially, by the patient engagement in one's own health management.
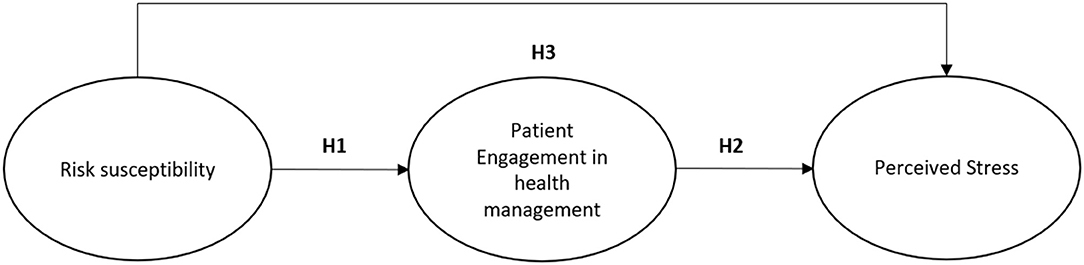
Figure 1. The hypothesized model.
This is a cross-sectional study that used a CAWI (Computer Assisted Web Interviewing) methodology. Data were collected using a questionnaire distributed between April 6 and April 13, 2020, to a mailing list of a purposive sample of patients who belonged to the Italian Association for Patients with IBD–AMICI Onlus. The questionnaire was sent to 4,187 patients with IBD subscribed to AMICI Onlus mailing list who were over 18 years old. A total of 1,014 (response rate 24%) were returned completed and they were used for the statistical analyses. All participants provided informed consent at the beginning of the questionnaire. The study was approved by the Ethical Commission of the Catholic University of the Sacred Heart (CERPS) and was conducted in accordance to the ethical standards of the Declaration of Helsinki and its following amendments.
In order to answer the research questions, the survey involved the measurement of the following variables:
• Socio-demographic variables: a series of socio-demographical data were collected, including age, gender, education, urban center size, geographical area, and marital status in order to describe the sample.
• Disease characteristics of the patients: some data relating to the year of diagnosis and the type of disease (Crohn's disease, Ulcerative colitis, IBD unclassified) were collected.
• Perceived risk susceptibility toward COVID-19 contagion: participants were asked to rate from 1 (very little) to 5 (a lot) their perceived risk of being personally infected by the new COVID-19 virus. Since the question was considered particularly sensitive, participants were also granted the possibility to answer “I'd rather not answer.”
• Perceived stress: this variable was measured using the Perceived Stress Scale (PSS) that was used in its 4-items version, validated by Cohen and colleagues (20). The PSS is designed to measure the experienced levels of stress caused by a stressful situation. All items were assessed on a 5-point Likert scale ranging from 0 (never) to 4 (very often). The higher score on this scale represents greater experienced levels of stress caused by a stressful situation. An example of item is, “In the last month, how often have you felt that you were unable to control the important things in your life?”
• The engagement in one's own health management during the COVID-19 emergency: This aspect was measures using the Patient Health Engagement Scale (PHE-s®), a measure that, developed according to the Patient Health Engagement model (21), assesses people health engagement level, defined as the “people psychological readiness and sense of mastery to become active player in their own health management and health risk prevention.” Previous studies demonstrated its robust psychometric properties (1). This scale is composed by 5 items measured on a 7-point Likert scale. Those who have higher score on this scale are completely aware of the characteristics and consequences of their disease condition, and assume a more responsible position in their behaviors and disease management experienced. In this research a slightly adapted version of the scale to the specific COVID-19 situation was adopted (22). The questionnaire's items are available in the Supplementary Materials (Online Resource 1).
Descriptive statistics were computed for each item (symmetry, kurtosis, mean, median, and standard deviation), and normality of distribution was checked. As suggested by Anderson and Gerbing (23) in order to check the adequacy of the measurement model a confirmatory factor analysis (CFA) was run using MPLUS 8. The models were estimated using Satorra-Bentler Correction (MLM) and evaluated using the chi-square (i.e., non-significant values of p-value indicate a good model) and approximate fit statistics, based on Hu and Bentler (24). These included Root Mean Square Error of Approximation (RMSEA) <0.08; Confirmatory Fit Index (CFI) ≥0.90; and Tucker-Lewis Index (TLI) ≥0.90. Moreover, structural equation modeling (SEM) was used to analyze the relationships between the perceived risk susceptibility toward COVID-19 contagion and the patient engagement in one's own health management during the COVID-19 emergency on perceived stress. In particular, the bootstrap technique (25) was used in order to confirm the mediation hypothesis (the indirect relationship between an independent variable and the dependent variable considering the presence of the mediator) with more statistical rigor than the Sobel test (26, 27). The Percentile bootstrapping was performed at a 95% confidence interval with 5,000 bootstrap samples (28).
Finally, a power analysis was conducted to understand whether the study sample size was adequate for the planned analyses. Since the sample size required for SEM depends on multiple factors not considered in rule-of-thumbs guidelines [i.e., the number of latent factors, the number of indicators, and the magnitude of factor loadings and correlations; (29)], we decided to use the pwrSEM app on Shiny (30) based on Monte Carlo simulation with 1,000 repetitions to estimate the power for the regression paths in our hypothesized model. The factor loadings of PSS and of PHE-s® were, respectively, set at 0.63 and at 0.69, and they were estimated using the Spearman-Brown prophecy formula that considers the scales' overall reliability to estimate the average factor loading strength of individual items in that measure. The results revealed that, with the sample size of 1,014 and alpha level of 0.05, the test has at least 93% power to detect indirect effect sizes equal to or larger than 0.03.
The sample is made up of 1,014 Italian patients with IBD of which 476 (46.9%) are male and 538 (53.1%) are female with an age between 18 and 84 years with an average of 48.35 years and a standard deviation of ±13.20. The demographic profile is presented in detail in Table 1.
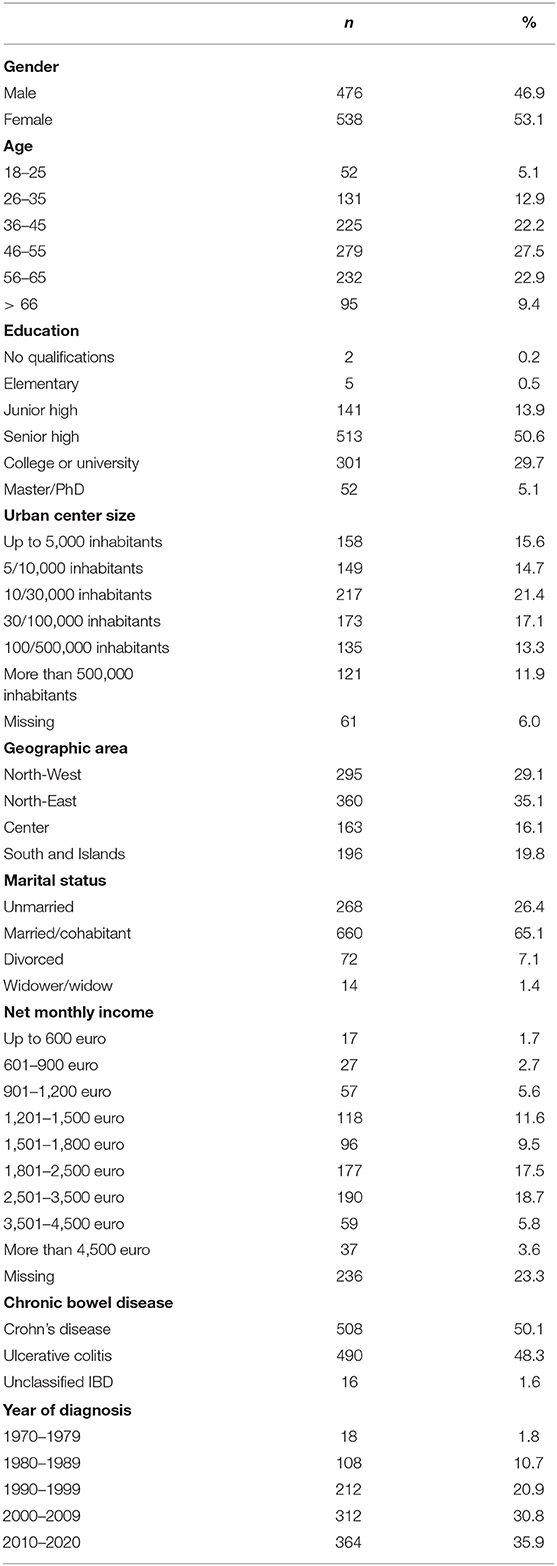
Table 1. Demographic and disease characteristics of the sample (N = 1,014).
Means, standard deviations, medians, symmetry, and kurtosis of all the scales and items used in the model were calculated, showing that all the items were normally distributed, with the only exception of the last item of the Scale (PHE-s®) COVID-19 version (PHE_Item 5) (Table 2).
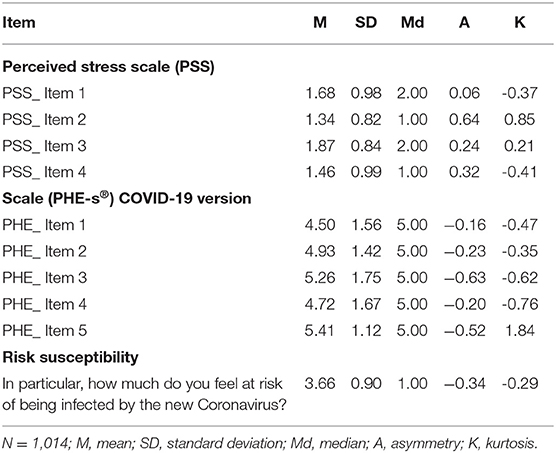
Table 2. Descriptive statistics of items.
Moreover, a confirmatory factor analysis (CFA) was carried out to understand whether the data conformed to the assumption that these latent variables (perceived stress and the patient engagement in one's own health management during the COVID-19 emergency) represent two separated constructs, validating the measurement model. For this purpose, the MLM method was used.
To determine goodness of fit, Beavers (31) proposed that the factor loadings <0.40 are weak and factor loadings >0.60 can be considered strong. Moreover, the acceptable threshold value for composite reliability (CR) is above 0.70, while that for average variance extracted (AVE) is above 0.50 (32). Results from the CFA confirmed the hypothesized two factor measurement model and also all of the loadings of the observed variables on the latent variables were also significant, revealing that all of the latent constructs were well operationalized by their indicators even if the AVE relating the Perceived Stress Scale is slightly under below the threshold (Table 3).
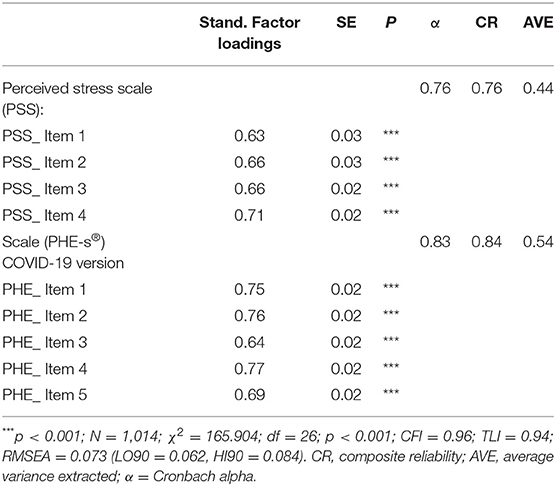
Table 3. Confirmatory factor analysis properties.
Finally, a structural equation model (SEM) was run in MPLUS 8 to assess the presented model. The model provided a very good fit to the data: χ2 = 170.102; df = 33; p ≤ 0.001; CFI = 0.96; TLI = 0.94; RMSEA = 0.065 (LO90 = 0.055, HI90 = 0.074). In accordance with the hypothesis, the patient engagement in one's own health management during the COVID-19 emergency was negatively influenced by the perceived risk susceptibility toward COVID-19 contagion (β = −0.410, p < 0.001), confirming hypothesis 1, and the perceived stress was negatively influenced by the patient engagement in one's own health management during the COVID-19 emergency (β = −0.748, p < 0.001), confirming hypothesis 2 (see Figure 2).
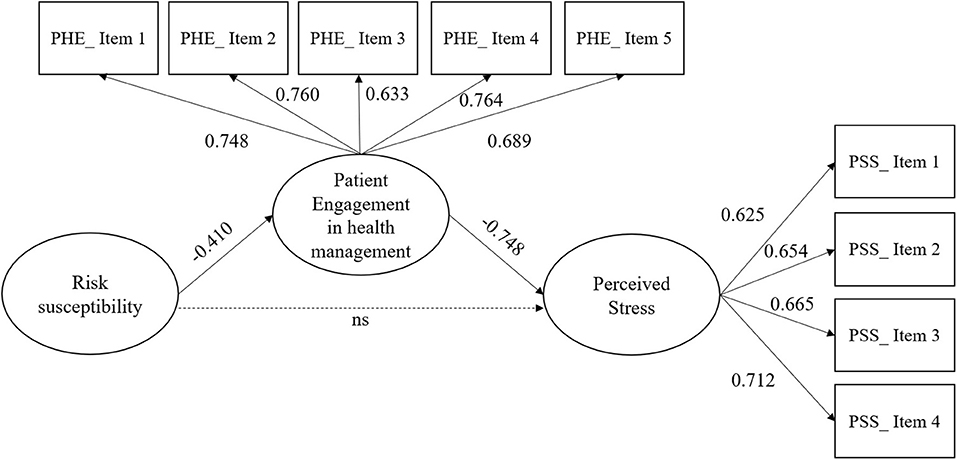
Figure 2. The results of structural equation model (SEM). ns, not significant.
In Table 4, the results of the total effect, indirect effect, and direct effect are shown. We note that the patient engagement in one's own health management during the COVID-19 emergency plays a full mediating role in the relationships between the perceived risk susceptibility toward COVID-19 contagion and perceived stress (indirect effect = 0.306, CI = 0.254; 0.361). Hence, hypothesis 3 is supported by the results.
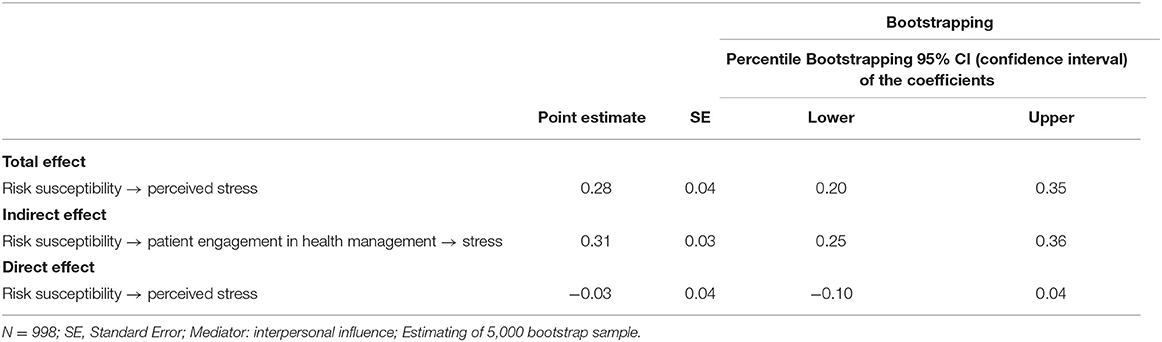
Table 4. Standardized indirect effect of the model.
The results from the confirmatory factor analyses show that the measures used to assess the patient engagement in one's own health management during the COVID-19 emergency and perceived stress were reliable.
The analyses conducted via the structural equation model, indeed, confirmed our initial hypotheses. In particular, our research showed that higher levels of perceived risk of contagion from COVID-19 negatively affects the ability of patients with IBD to psychologically engage in their health management. Recent research carried out on the Italian population (33) of patients with IBD confirmed these results, showing that patients with IBD with higher levels of perceived risk of contagion from COVID-19 have significantly lower levels of patient engagement. In line with these results, other research on chronic diseases demonstrated that the impact of the perception of risk on patient engagement could lead to inadequate preventive behaviors (14, 34, 35). Our results also suggest that in the case of Italian patients with IBD coping with their disease during COVID-19 emergency, the perception of risk of contagion impacts the ability to engage in their health management. Investigating this relation is indeed necessary to support patients in dealing with the perception of risk contagion and prevent possible misconducts, such as under- or over-estimation of the importance of preventive measures.
Moreover, this research demonstrated that in the Italian patients with IBD the ability to engage in health management during this emergency influences the level of perceived stress. These findings are supported by other studies that pointed out that the level of stress and anxiety experienced by patients are significantly correlated with the level of engagement that patients have of their disease (36, 37). Our results also showed that in patients with IBD the perceived susceptibility to COVID-19 has a positive relationship with perceived psychological distress, hence showing that those patients who feel more vulnerable to COVID-19 also show higher levels of psychological distress. These results have also been confirmed by other studies that have tried to understand the connection between the risk of contagion from COVID-19 and perceived stress (38, 39), on different patients. In Italy, a research carried out by Di Crosta et al. (40) on the healthy Italian population showed that higher levels of risk of contagion by COVID-19 could significantly impact on the level of perceived stress and its symptoms (40). These results suggest to monitor patients' susceptibility to stressful events as they may manifest worse symptoms and experiment poorer quality of life.
Finally, our results highlighted the key role of Patient Health Engagement, which fully mediates the relationship between perceived risk of contagion from COVID-19 and level of perceived stress in patients with IBD. These results underlined that the perceived risk impacts on the ability of patients with IBD to be psychologically engaged in their health management which, in turn, affects the level of perceived stress. In other words, this means that the risk of contagion from COVID-19 increases the level of stress through the decrease of the patient engagement in health management. These results are important from both a scientific and a pragmatic point of view. From a scientific point of view, they explained the relationship between level of perceived stress and risk of contagion from COVID-19 in patients with IBD. In particular, this study highlighted the key role of the patient engagement in influencing the level of stress, showing how risk of contagion from COVID-19 has only an indirect effect on it. However, most studies have investigated the direct relationship between risk of contagion from COVID-19 and perceived stress without deepening the process that links these two psychological phenomena (41, 42). Moreover, these findings have some practical implications. Specifically, they showed how important it is for healthcare professionals, involved in IBD patient care, to monitor patients' perceived risk of contagion from COVID-19 in order to avoid worsening in their health management ability which, in turn, can cause high levels of stress. Indeed, high level of stress in patients with IBD can determine negative health outcomes (8, 43) and a poorer health-related quality of life (44). Furthermore, it is important not only to monitor but try to contain the risk of contagion from COVID-19 perceived by patients with IBD. In particular, some studies (45, 46) showed how through a clear and effective communication that describes the preventive actions necessary to reduce the infection from COVID-19 it is possible to reduce the perception of risk felt by people and the consequent negative effects.
Nonetheless, the present study has several limitations: first, the level of psychological distress (as well as the other variables) was assessed through self-report measures, which may suffer from biases. However, through self-reported measures it is possible to assess patients' direct experience, which is required in a context that calls for giving voice to the patients, for example, through patient-reported measures of experiences and outcomes. For this reason, we have anyway privileged for this type of data collection. In addition, the PSS scale was adapted from English, and although the CFA showed a good reliability, a proper Italian validation should be carried out to assess the translated version's psychometric properties. Moreover, the sample was recruited with a non-random method, which may have hampered its representativeness of the Italian population of patients with IBD. The patients involved in our research, indeed, belonged to the Italian Association for Patients with IBD: on the one hand, it can be a limitation of the study, on the other this sample has a very similar care experience and they can be considered as expert patients. The participation to the survey was free, so the patients who answered were convinced and inclined to complete the questionnaire.
Our study has allowed an understanding of the process that explains the relationship between the risk of contagion from COVID-19 and the level of stress perceived by patients with IBD during this emergency situation. Understanding this psychological process is of paramount importance for these patients because, as shown by previous studies, high levels of perceived stress could lead to an increase in anxiety and depressive states causing worsening not only of their quality of life but also of their intestinal symptoms. The innovative result of this research is that the perceived risk of contagion from COVID-19 increases the level of stress of patients with IBD through the decrease of their engagement in health management. Consequently, from a scientific point of view, this study allows us to explain the psychological process that links the risk of contagion from COVID-19 to perceived stress in patients with IBD by showing how the patient engagement in health management is the key variable that directly affects perceived stress while the level of perceived risk influences it indirectly. Furthermore, these results highlight the importance of monitoring and managing the risk of contagion from COVID-19 perceived by patients with IBD to avoid increasing stress levels through a decrease in their health management capacity.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the study was approved by the Ethical Commission of the Catholic University of the Sacred Heart (CERPS), and was conducted in accordance to the ethical standards of the Declaration of Helsinki and its following amendments. The patients/participants provided their written informed consent to participate in this study.
MS, SL, EP, AA, and GG: conceptualization. MS, GC, and GG: methodology. GC: formal analysis and data curation. GC, LP, and SB: writing—original draft preparation. LP, SB, GC, GG, and MS: writing—review and editing. GG: supervision and project administration. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2021.733544/full#supplementary-material
1. Graffigna G, Barello S, Savarese M, Palamenghi L, Castellini G, Bonanomi A, et al. Measuring Italian citizens' engagement in the first wave of the COVID-19 pandemic containment measures: a cross-sectional study. PLoS ONE. (2020) 15:e0238613. doi: 10.1371/journal.pone.0238613
2. Zhang J, Lu H, Zeng H, Zhang S, Du Q, Jiang T, et al. The differential psychological distress of populations affected by the COVID-19 pandemic. Brain Behav Immun. (2020) 87:49–50. doi: 10.1016/j.bbi.2020.04.031
3. Mazza C, Ricci E, Biondi S, Colasanti M, Ferracuti S, Napoli C, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. (2020) 17:3165. doi: 10.3390/ijerph17093165
4. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatry. (2020) 33:e100213. doi: 10.1136/gpsych-2020-100213
5. Graff LA, Walker JR, Clara I, Lix L, Miller N, Rogala L, et al. Stress coping, distress, and health perceptions in inflammatory bowel disease and community controls. Am J Gastroenterol. (2009) 104:2959–69. doi: 10.1038/ajg.2009.529
6. Porcell P, Leoci C, Guerra V. A prospective study of the relationship between disease activity and psychologic distress in patients with inflammatory bowel disease. Scand J Gastroenterol. (1996) 31:792–6. doi: 10.3109/00365529609010354
7. Grunert PC, Reuken PA, Stallhofer J, Teich N, Stallmach A. Inflammatory bowel disease in the COVID-19 pandemic: the patients' perspective. J Crohn's Colitis. (2020) 14:1702–8 doi: 10.1093/ecco-jcc/jjaa126
8. Mawdsley JE, Rampton DS. The role of psychological stress in inflammatory bowel disease. Neuroimmunomodulation. (2006) 13:327–36. doi: 10.1159/000104861
9. Krok D, Zarzycka B. Risk perception of COVID-19, meaning-based resources and psychological well-being amongst healthcare personnel: the mediating role of coping. J Clin Med. (2020) 9:3225. doi: 10.3390/jcm9103225
10. Cheng SKW, Chong GHC, Chang SSY, Wong CW, Wong CSY, Wong MTP, et al. Adjustment to severe acute respiratory syndrome (SARS): roles of appraisal and post-traumatic growth. Psychol Health. (2006) 21:301–17. doi: 10.1080/14768320500286450
11. Dulai PS, Singh S, Ohno-Machado L, Sandborn WJ. Population health management for inflammatory bowel disease. Gastroenterology. (2018) 154:37–45. doi: 10.1053/j.gastro.2017.09.052
12. Shah SL, Siegel CA. Increasing patient activation could improve outcomes for patients with inflammatory bowel disease. Inflamm Bowel Dis. (2015) 21:2975–8. doi: 10.1097/MIB.0000000000000575
13. Liu S, Lithopoulos A, Zhang CQ, Garcia-Barrera MA, Rhodes RE. Personality and perceived stress during COVID-19 pandemic: testing the mediating role of perceived threat and efficacy. Pers Individ Dif. (2021) 168:110351. doi: 10.1016/j.paid.2020.110351
14. Everett B, Salamonson Y, Rolley JX, Davidson PM. Underestimation of risk perception in patients at risk of heart disease. Eur J Cardiovasc Nurs. (2014) doi: 10.1177/1474515114556712
15. Jordan JE, Briggs AM, Brand CA, Osborne RH. Enhancing patient engagement in chronic disease self-management support initiatives in Australia: the need for an integrated approach. Med J Aust. (2008) 189. doi: 10.5694/j.1326-5377.2008.tb02202.x
16. Barello S, Guida E, Leone S, Previtali E, Graffigna G. Does patient engagement affect IBD patients' health-related quality of life? findings from a cross-sectional study among people with inflammatory bowel diseases. Heal Qual Life Outcomes. (2021) 19:1–9. doi: 10.1186/s12955-021-01724-w
17. Graffigna G, Bosio C, Pagnini F, Volpato E, Previtali E, Onlus A, et al. Italian consensus statement for promoting psycho-social wellbeing and engagement in the care of inflammatory bowel disease patients (preprint). Researchsquare. (2021) doi: 10.21203/rs.3.rs-587615/v1
18. Zheng X, Chu H, Cong Y, Deng Y, Long Y, Zhu Y, et al. Self-reported lactose intolerance in clinic patients with functional gastrointestinal symptoms: prevalence, risk factors, and impact on food choices. Neurogastroenterol Motil. (2015) 27:1138–46. doi: 10.1111/nmo.12602
19. Di Giacomo D. Public health emergencies and quarantine: virtual patient engagement as challenge and opportunity for mental health strategy. Mediterr J Clin Psychol. (2020) 2:1–5. doi: 10.6092/2282-1619/mjcp-2533
20. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) doi: 10.1037/t02889-000
21. Graffigna G, Barello S, Bonanomi A, Lozza E. Measuring patient engagement: development and psychometric properties of the patient health engagement (PHE) scale. Front Psychol. (2015) 6:274. doi: 10.3389/fpsyg.2015.00274
22. Graffigna G, Barello S, Savarese M, Palamenghi L, Castellini G, Bonanomi A, et al. Measuring Italian citizens′ engagement in the first wave of the COVID-19 pandemic containment measures a cross-sectional study. medRxiv. (2020) doi: 10.1101/2020.04.22.20075234
23. Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. (1988) 103:411–23. doi: 10.1037/0033-2909.103.3.411
24. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model A Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
25. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/BRM.40.3.879
26. MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. (2002) 7:83–104. doi: 10.1037/1082-989X.7.1.83
27. MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. (2004) 39:99–128. doi: 10.1207/s15327906mbr3901_4
28. Taylor AB, MacKinnon DP, Tein JY. Tests of the three-path mediated effect. Organ Res Methods. (2008) 11:241–69. doi: 10.1177/1094428107300344
29. Wolf EJ, Harrington KM, Clark SL, Miller MW. Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas. (2013) 73:913–34. doi: 10.1177/0013164413495237
30. Wang YA, Rhemtulla M. Power analysis for parameter estimation in structural equation modeling: a discussion and tutorial. Adv Methods Pract Psychol Sci. (2021) 4:1–7. doi: 10.31234/osf.io/pj67b
31. Beavers AS, Lounsbury JW, Richards JK, Huck SW, Skolits GJ, Esquivel SL. Practical considerations for using exploratory factor analysis in educational research. Pract Assessment, Res Eval. (2013) 18:1–3. doi: 10.7275/qv2q-rk76
32. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. (1981) 18:39–50. doi: 10.1177/002224378101800104
33. Castellini G, Savarese M, Leone S, Previtali E, Armuzzi A, Graffigna G. Italian IBD patients coping with Covid-19 emergency: the mitigating role of psychological readiness to engage in self-care. Inflamm Bowel Dis. (2020) 26: e130–1. doi: 10.1093/ibd/izaa185
34. Katapodi MC, Lee KA, Facione NC, Dodd MJ. Predictors of perceived breast cancer risk and the relation between perceived risk and breast cancer screening: a meta-analytic review. Prev Med (Baltim). (2004) 38:388–402. doi: 10.1016/j.ypmed.2003.11.012
35. Haber G, Ahmed NU, Pekovic V. Family history of cancer and its association with breast cancer risk perception and repeat mammography. Am J Public Health. (2012) 102:2322–9. doi: 10.2105/AJPH.2012.300786
36. Zhang M, Hong L, Zhang T, Lin Y, Zheng S, Zhou X, et al. Illness perceptions and stress: mediators between disease severity and psychological well-being and quality of life among patients with Crohn's disease. Patient Prefer Adherence. (2016) 10:2387–96. doi: 10.2147/PPA.S118413
37. Vivian E, Oduor H, Lundberg L, Vo A, Mantry PS. A cross-sectional study of stress and the perceived style of decision-making in clinicians and patients with cancer. Heal Serv Res Manag Epidemiol. (2019) 6:233339281985539. doi: 10.1177/2333392819855397
38. Sher L. The impact of the COVID-19 pandemic on suicide rates. QJM. (2020) 113:707–12. doi: 10.1093/qjmed/hcaa202
39. Elbay RY, Kurtulmuş A, Arpacioglu S, Karadere E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. (2020) 290:113130. doi: 10.1016/j.psychres.2020.113130
40. Di Crosta A, Palumbo R, Marchetti D, Ceccato I, La Malva P, Maiella R, et al. Individual differences, economic stability, and fear of contagion as risk factors for PTSD symptoms in the COVID-19 emergency. Front Psychol. (2020) 11:567367. doi: 10.3389/fpsyg.2020.567367
41. Nass BYS, Dibbets P, Markus CR. Impact of the COVID-19 pandemic on inflammatory bowel disease: the role of emotional stress and social isolation. Stress Heal. (2021) 8:1–2. doi: 10.1002/smi.3080
42. Cheema M, Mitrev N, Hall L, Tiongson M, Ahlenstiel G, Kariyawasam V. Depression, anxiety and stress among patients with inflammatory bowel disease during the COVID-19 pandemic: australian national survey. BMJ Open Gastroenterol. (2021) 8:e000581. doi: 10.1136/bmjgast-2020-000581
43. Goodhand JR, Wahed M, Mawdsley JE, Farmer AD, Aziz Q, Rampton DS. Mood disorders in inflammatory bowel disease: relation to diagnosis, disease activity, perceived stress, and other factors. Inflamm Bowel Dis. (2012) 18:2301–9. doi: 10.1002/ibd.22916
44. Tabibian A, Tabibian JH, Beckman LJ, Raffals LL, Papadakis KA, Kane S V. Predictors of health-related quality of life and adherence in Crohn's disease and ulcerative colitis: implications for clinical management. Dig Dis Sci. (2015) 60:1366–74. doi: 10.1007/s10620-014-3471-1
45. Kim DKD, Kreps GL. An analysis of government communication in the United States during the COVID-19 pandemic: recommendations for effective government health risk communication. World Med Heal Policy. (2020) 12:398–412. doi: 10.1002/wmh3.363
Keywords: COVID-19, inflammatory bowel disease, patient engagement, stress, structural equation model-SEM
Citation: Castellini G, Palamenghi L, Savarese M, Barello S, Leone S, Previtali E, Armuzzi A and Graffigna G (2021) Patient Engagement in Health Management as a Mediator Between Perceived Risk and COVID-19 Related Distress in Patients With IBD: A Structural Equation Model. Front. Psychiatry 12:733544. doi: 10.3389/fpsyt.2021.733544
Received: 01 July 2021; Accepted: 23 September 2021;
Published: 27 October 2021.
Edited by:
Adriana Mihai, George Emil Palade University of Medicine, RomaniaReviewed by:
Hiu Tin Leung, The University of Hong Kong, Hong Kong SAR, ChinaCopyright © 2021 Castellini, Palamenghi, Savarese, Barello, Leone, Previtali, Armuzzi and Graffigna. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariarosaria Savarese, bWFyaWFyb3NhcmlhLnNhdmFyZXNlQHVuaWNhdHQuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.