
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychol. , 19 February 2025
Sec. Psychology of Aging
Volume 16 - 2025 | https://doi.org/10.3389/fpsyg.2025.1512175
 Jiajia Dai1,2
Jiajia Dai1,2 Mohan Wang3Han Zhang4Zhengfang Wang4Xue Meng5,6Yanan Sun1,2Yuan Sun1,2Wenhui Dong4Zhiying Sun4
Mohan Wang3Han Zhang4Zhengfang Wang4Xue Meng5,6Yanan Sun1,2Yuan Sun1,2Wenhui Dong4Zhiying Sun4 Kuo Liu1,2*
Kuo Liu1,2*Background: The prevalence of cognitive impairment in elderly diabetic patients is increasing, highlighting the importance of exploring strategies to prevent and ameliorate cognitive impairment in this population. Previous studies have focused mostly on improving cognition in elderly diabetic patients through three methods: medication, cognitive training, and lifestyle intervention. However, few studies have investigated the role of indoor biophilic environments in improving cognition. Biophilic environments improve human health by integrating natural elements into indoor architectural settings and have demonstrated efficacy in reducing stress and improving cognition. Therefore, it is worth exploring the effects of indoor biophilic environments on cognition in elderly diabetic patients. This study aims to investigate the effects of indoor biophilic environments on cognition in elderly diabetic patients, and the potential mechanisms.
Methods: This is a single-center, randomized controlled trial, which includes a short-term VR intervention and a long-term real environment intervention. In the short-term intervention trial, 64 diabetic patients over 60 years old are randomly assigned to 1 of 7 intervention groups or a control group. All intervention groups are constructed by single or various combinations of the 3 indoor biophilic elements: natural decorative paintings, indoor potted plants, and ornamental fish. The primary outcome of the short-term intervention trial is the cognitive scores assessed by DSST and BDS. In the long-term intervention trial, 240 diabetic patients over 60 years old will be randomly assigned to either the intervention group or the control group. The biophilic elements in long-term intervention will be determined based on the results of the short-term VR intervention trial. The primary outcomes of the long-term intervention trial are cognitive scores measured by DSST and MoCA, as well as concentrations of plasma p-tau181, esRAGE, and IL-6.
Conclusion: The findings will be utilized to develop a restorative living environment for elderly patients with diabetes to improve cognition.
Clinical trial registration: https://www.chictr.org.cn, identifier [ChiCTR2300072329].
Diabetes represents a global public health concern, posing an increasingly formidable challenge to healthcare systems worldwide. In 2021, the global age-standardized prevalence of diabetes reached 6.1%. Within the age range of 65–95 years, the prevalence of diabetes exceeded 20% in every five-year age interval (Ong et al., 2023). Cognitive impairment is a significant complication of diabetes and manifests as a decline in cognitive abilities related to diabetes, as well as mild cognitive impairment (MCI) and dementia (Biessels and Despa, 2018). Diabetes, cognitive impairment, and dementia often coexist within people older than 65 years (Srikanth et al., 2020). Approximately 26% of people over 60 with diabetes have MCI and 36.9% have dementia (Jia et al., 2020). Cognitive impairment weakens the ability of self-management in diabetes, while inadequate diabetes management increases the risk of cognitive dysfunction (Ojo and Brooke, 2015). Previous research also indicated that more severe cognitive impairment related to diabetes predominantly occurs in older people (Biessels and Despa, 2018). Elderly diabetes patients with coexisting cognitive impairment experience a significant reduction in quality of life because they face difficulties in performing diabetes self-care (American Diabetes Association Professional Practice Committee, 2024; Munshi, 2017). Since 2017, the American Diabetes Association has recommended screening for cognitive impairment in elderly diabetes to enhance diabetes self-management and quality of life (Sonne and Hemmingsen, 2017).
Previous studies have explored various approaches to improve cognitive function in diabetic patients: pharmacological interventions (Cukierman-Yaffe et al., 2020; Li et al., 2021; Parish et al., 2022; Ryan et al., 2006), cognitive training (Silverman et al., 2023; Wong et al., 2020), and lifestyle interventions (Chen Y. N. et al., 2023; Espeland et al., 2018; Kwok et al., 2017; Lotan et al., 2021). Some of the antidiabetic drugs had positive effects on cognitive function (Cukierman-Yaffe et al., 2020; Li et al., 2021; Ryan et al., 2006), however, the effects of pharmacological interventions are largely limited by the patients’ compliance (Chen P. C. et al., 2023; Zullig et al., 2019). Moreover, lifestyle interventions, such as increased physical activity can also improve cognitive performance in diabetic patients (Chen Y. N. et al., 2023). However, it is difficult for the patients to maintain healthy behaviors, because they often passively alter their habits through health behavior interventions (Deslippe et al., 2023).
Though physical activities (Rivera Miranda et al., 2024) and social engagement (Liebzeit et al., 2022; Parra Rizo and López Marin, 2020) have been found to contribute to cognitive health in older adults. However, maintaining long-term physical activities and engagement with social activities is a challenge for older adults due to physical limitations or lack of motivation (De Coninck et al., 2021; Franco et al., 2015). Similarly, although many studies have confirmed the positive effects of outdoor natural environments on cognition (Besser, 2021; Bratman et al., 2012; Chen et al., 2022; De Keijzer et al., 2018), the adaptive capacity and physical function of elderly individuals gradually decline with age. Consequently, they spend more time indoors, with limited exposure to natural environments (Lee and Park, 2021). It has been demonstrated that patients after cholecystectomy whose hospital room windows faced natural landscapes had shorter postoperative hospital stays, received fewer negative evaluations during their stay, and required less potent analgesics than patients with windows facing brick walls of the building (Ulrich, 1984). The study showed that even without direct contact with the outdoor natural environments, the indoor environments still have healing effects. Biophilic design aims at incorporating natural elements into interior design, thereby enhancing human connection with nature (Barbiero and Berto, 2021). Compared to pharmacological and lifestyle interventions, biophilic design improves cognitive function by creating accessible and sustainable environments that improve psychological and physiological responses (Felly and Susanto, 2020), with lower patient compliance requirements. Recent studies have demonstrated that biophilic design has potential benefits on cognition (Mostajeran et al., 2023; Wallmann-Sperlich et al., 2019; Yin et al., 2019), but few have shown which specific biophilic elements are most beneficial to cognition.
Constructing a therapeutic environment that incorporates various biophilic design elements in a real indoor environment is a challenging task, as the optimal biophilic elements remain ambiguous. Virtual reality (VR) technology can simulate the real environment and integrate various sensory stimuli (Riva et al., 2020), rendering the exploration of optimal biophilic elements or their combinations more cost-effective. In recent years, an increasing number of studies have utilized VR technology to construct biophilic environments and demonstrated its beneficial effects on cognitive performance (Latini et al., 2024; Yin et al., 2019). Thus, we first use VR technology to create biophilic environments with various biophilic elements and conduct a short-term trial to screen for the most effective biophilic elements or combinations. However, VR environments also have some limitations. Virtual environments have a side effect of motion sickness which will cause a biased evaluation of healing effects (Kiryu and So, 2007) and VR cannot replicate tactile sensations (Yu et al., 2019), which may miss the healing effects of touching biophilic elements (Hassan and Zhang, 2024; Jenkins, 1986). Additionally, conventional VR technology cannot mimic the comprehensive healing effect of biophilic elements. For example, it cannot simulate the air purifying effect of potted plants (Pettit et al., 2018) and the emotional support of companion animals (Amiot and Bastian, 2015; Liu et al., 2024; Acquadro Maran et al., 2022). In addition, VR also cannot simulate the effect of reducing sedentary time and increasing physical activity caused by watering plants (Dogra et al., 2017). Therefore, referring to the healing effect of each biophilic element in the short-term trial, appropriate biophilic elements will be selected for long-term indoor environment intervention. The specific arrangement of biophilic elements in the real environment will be designed to closely replicate the layout in the VR environment, ensuring the effects of the biophilic elements.
The mechanisms underlying the impact of biophilic environments on cognition are not yet clear. A study suggests that biophilic environments may reduce the occurrence of neuroinflammation by alleviating stress, thereby improving cognition (Valentine et al., 2024), which is crucial in mitigating cognitive impairment associated with the E4 variant of apolipoprotein E (APOE4). APOE4 is a strong genetic risk factor for cognitive impairment (Montagne et al., 2020). Previous studies have examined gene–environment interactions between APOE4 and other environmental risk factors on cognitive functions. These studies mainly explored the interactions between diet (van de Rest et al., 2016), residential greenness (Zhu et al., 2020), physical activity (Pa et al., 2022; Stringa et al., 2020), and socioeconomic position (Frank et al., 2021) with APOE4. Investigating the interaction between APOE4 and indoor biophilic elements on cognitive function helps us determine if biophilic interventions have different effects on populations with diverse genetic backgrounds.
Through the integrated approach of short-term VR and long-term real-environment interventions, we aim to explore the effects of indoor biophilic environments on cognitive function in elderly patients with diabetes. We use the results from the short-term VR trial as a reference for the long-term real environment intervention trial. The biophilic elements or combinations with the largest effect size and p < 0.1 in the short-term VR trial will be used in real indoor environments to validate their long-term effects on cognition in elderly diabetes. The findings of this research will not only contribute to supporting the design of VR scenarios for assessing the restorative impact of biophilic residential environments but also help develop cognitively improving living environments for elderly diabetic patients.
This study is a single-center, randomized controlled trial. It includes both a short-term VR intervention and a long-term real environment intervention. The study flowchart is depicted in Figure 1.
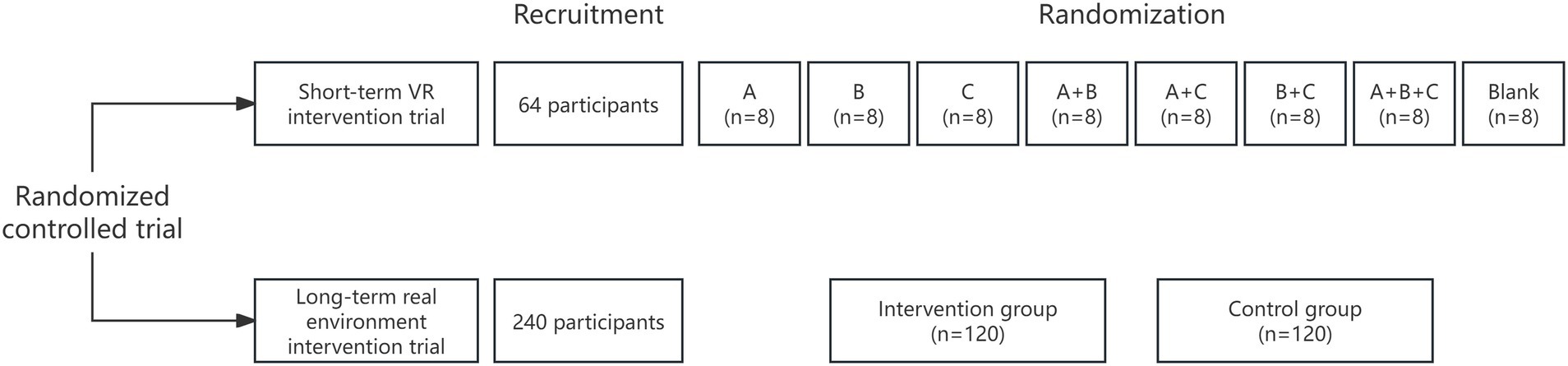
Figure 1. Study flow chart. VR, virtual reality; A, natural decorative paintings; B, indoor potted plants; C, ornamental fish.
As for the short-term VR intervention trial, a total of 64 participants over 60 years old with diabetes are recruited. The participants are randomly assigned to seven intervention groups or a control group using block randomization with randomly selected block sizes. The main objective of the short-term trial is to determine which biophilic elements or their combinations show the most significant improvement in cognitive function.
As for the long-term real environment intervention trial, a total of 240 participants over 60 years old with diabetes will be recruited. The participants will be randomly assigned in a 1:1 ratio to either the intervention or control group. The main objectives of this long-term trial are to provide evidence for the healing effects of biophilic environments on cognition, and whether the APOE4 genotype will modify the healing effects of biophilic environments on cognition in elderly diabetes.
Enrollment completion and final study visit are projected for December 2024 and December 2026, respectively.
This study was approved by the Ethics Committee of Capital Medical University (Approval No: Z2023SY019) and is conducted according to the ethical standards of the Helsinki Declaration. The study protocol was developed according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist.
This study is conducted in a subdistrict in Fengtai District, Beijing.
Participants are recruited at a subdistrict in Fengtai District, Beijing. The short-term trial project is promoted to the community population in two ways: (1) to conduct a seminar on the prevention and treatment of complications in diabetic patients in the community and introduce the project; (2) to introduce the project to diabetic patients who have their regular physical examinations or visit endocrine clinics in the subdistrict.
Patients who are interested and meet the criteria are asked to sign their contact information and initially agree on a date for the VR intervention. The participants are called 2 days before the date they have agreed on and asked to provide medical records when they come to participate in the trial.
Participants will also be recruited at the subdistrict in Fengtai District, Beijing. Researchers will introduce the program to diabetic patients who have regular physical examinations or visit endocrine clinics in the subdistrict. Eligible patients who agree to participate in the trial will be asked to sign an informed consent form and witnessed by a member of our research team.
Participants are eligible if they (1) are aged 60 years or older, (2) have been diagnosed with diabetes by a secondary or tertiary hospital or regularly take antidiabetic drugs, and (3) signed the informed consent form.
Participants are excluded if they (1) have been diagnosed with severe mental disorders, such as schizophrenia or hysterical psychosis; (2) have been diagnosed with dementia, cognitive impairment, severe physical disabilities such as paralysis, severe mobility impairments, or conditions that require full assistance for daily living, or language barriers that hinder their ability to successfully complete the questionnaire and physical examination; (3) have cognitive impairment resulting from various neurological disorders, including Parkinson’s disease, multiple sclerosis, traumatic brain injury, stroke, epilepsy, and intracranial space-occupying lesions.
In addition to the inclusion and exclusion criteria described for the short-term VR intervention trial, the long-term real environment intervention trial also has some additional exclusion criteria. Participants will be excluded from the long-term trial if they (1) have large size biophilic decorative paintings (larger than 40 cm × 60 cm) in their living room; (2) have more than 2 pots of plants in their homes, and care for these plants themselves; (3) have animals such as ornamental fish in their homes, and care for these animals themselves.
The VR residential environment used in this study includes three elements: natural decorative paintings (A), indoor potted plants (B), and ornamental fish (C). Biophilic design encompasses three patterns: nature in the space, natural analogues, and nature of the space (Hung and Chun, 2021). Current research primarily focuses on the first two patterns and has found that biophilic elements such as plants (Verzwyvelt et al., 2021; Yin et al., 2020), animals (Motooka et al., 2006), and natural decorations (Shen et al., 2020) help alleviate stress and improve cognitive function. Considering the lifestyle habits of local older adults and the feasibility of practical implementation, our study employs the three biophilic elements. A blank control VR scene without biophilic design elements and seven biophilic design VR scenes (A, B, C, A + B, A + C, B + C, A + B + C) are employed. The experiment follows the subsequent steps. The trial flowchart is illustrated in Figure 2.
I. Preparation Phase: first, researchers provide a concise introduction to the study procedures. Participants rest for 5 min, and heart rate and blood pressure are measured using an Omron medical electronic blood pressure monitor (HBP-1300). Then, baseline data are collected through a questionnaire survey. The structured questionnaire includes general demographic characteristics such as age, gender, height, weight, ethnicity, education level, marital status, and income. It also includes lifestyle behaviors such as smoking, alcohol consumption, and physical activity, medical histories such as hypertension, diabetes, and cardiovascular disease, and medication history. An assessment of mental health status is conducted using the Center for Epidemiologic Studies Depression Scale (10-item, CESD-10). Finally, cognitive scores are assessed using the Digit Symbol Substitution Test (DSST) and the Backward Digit Span (BDS) scale. After the measurements, researchers provide the VR headset to participants and allow them to adapt and learn basic operations for up to 5 min. All VR devices look the same shape and color.
II. Stress Phase: participants are exposed to a cluttered living environment through VR, with background noise from bustling traffic and mechanical devices. Then they undergo stress-inducing tests, including a memory test and an arithmetic test. The stress phase lasts for 5 min. After this phase, cognitive scores (DSST/BDS), heart rate, and blood pressure are re-measured.
III. VR Intervention Phase: participants will engage in a 10–15 min of VR scenario intervention according to their group allocation. Depending on their groups, some participants may simulate activities such as walking indoors, opening doors, pulling curtains, watering plants, or feeding fish. After completing the VR intervention, cognitive scores (DSST and BDS), heart rate, and blood pressure are measured again. Additionally, the Environmental Semantics Differential Scale (SD) and the Restoration Scale (RS) are also evaluated.
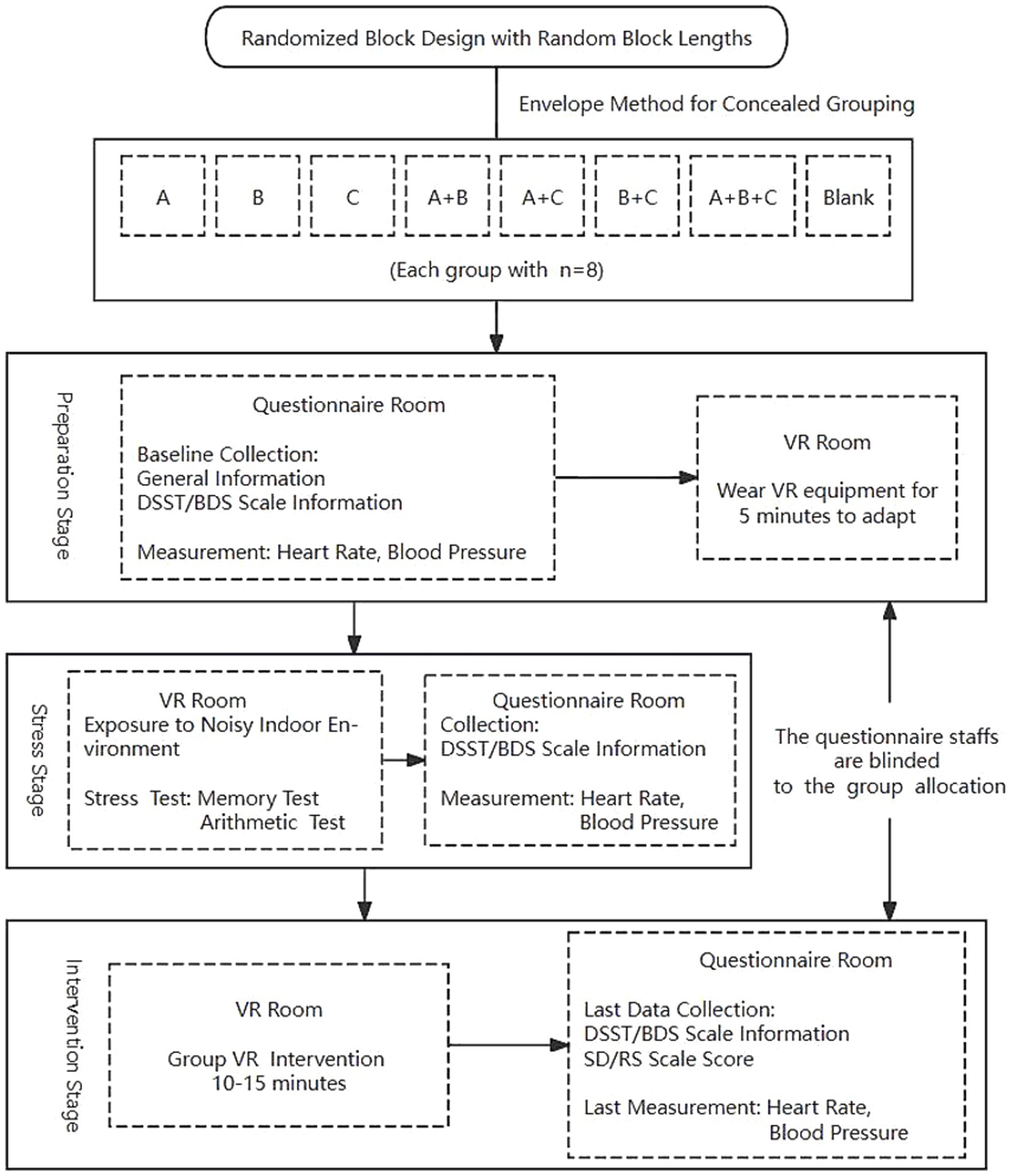
Figure 2. Short-term trial flow chart. A, natural decorative paintings; B, indoor potted plants; C, ornamental fish; VR, virtual reality; DSST, the Digit Symbol Substitution Test; BDS, the Backward Digit Span; SD, the Environmental Semantics Differential Scale; RS, the Restoration Scale.
During the VR experience, researchers record participants’ motion sickness. If participants feel nauseous or dizzy, they are instructed to remove the VR headset and take a two-minute break. Those who recover resume the trial, whereas those who remain symptomatic are withdrawn from the study.
VR interventions are deployed on the HTC Cosmos head-mounted display. The HTC Cosmos is a standalone device equipped with a high-resolution display that provides clear and realistic images. It also features built-in speakers and a microphone. The HTC Cosmos is equipped with a head tracking system and independent hand controllers, which enables users to perform various actions in VR, such as grabbing, moving, and rotating objects, enhancing immersion and interactivity.
We created nine distinct virtual residential environments for participants to explore and interact with, utilizing various 3D models and materials within the Unity game engine (version 2022.3.2f1c1). These VR scenes are arranged in the indoor living room and bedroom. The indoor residential environments serve as experimental scenarios, including a cluttered group (a cluttered house with traffic noise and no biophilic elements), a blank control group (a tidy house without any biophilic elements designed, blank), and seven intervention groups with a biophilic environment consisting of natural decorative paintings (A), indoor potted plants (B), ornamental fish (C) and their combinations (A + B, A + C, B + C, A + B + C).
The virtual environments are displayed on the HTC Cosmos head-mounted display (with a single-eye resolution of 1,440 × 1,700 pixels and a total resolution of 2,880 × 1,700 pixels; refresh rate of 90 Hz), and integrated headphones and controllers are used. To render the virtual environments, we utilize computers with a Windows 10 desktop system (NVIDIA GeForce RTX 2080 SUPER, Intel Core i7-8700K, 3.70 GHz).
The trial flowchart is depicted in Figure 3.
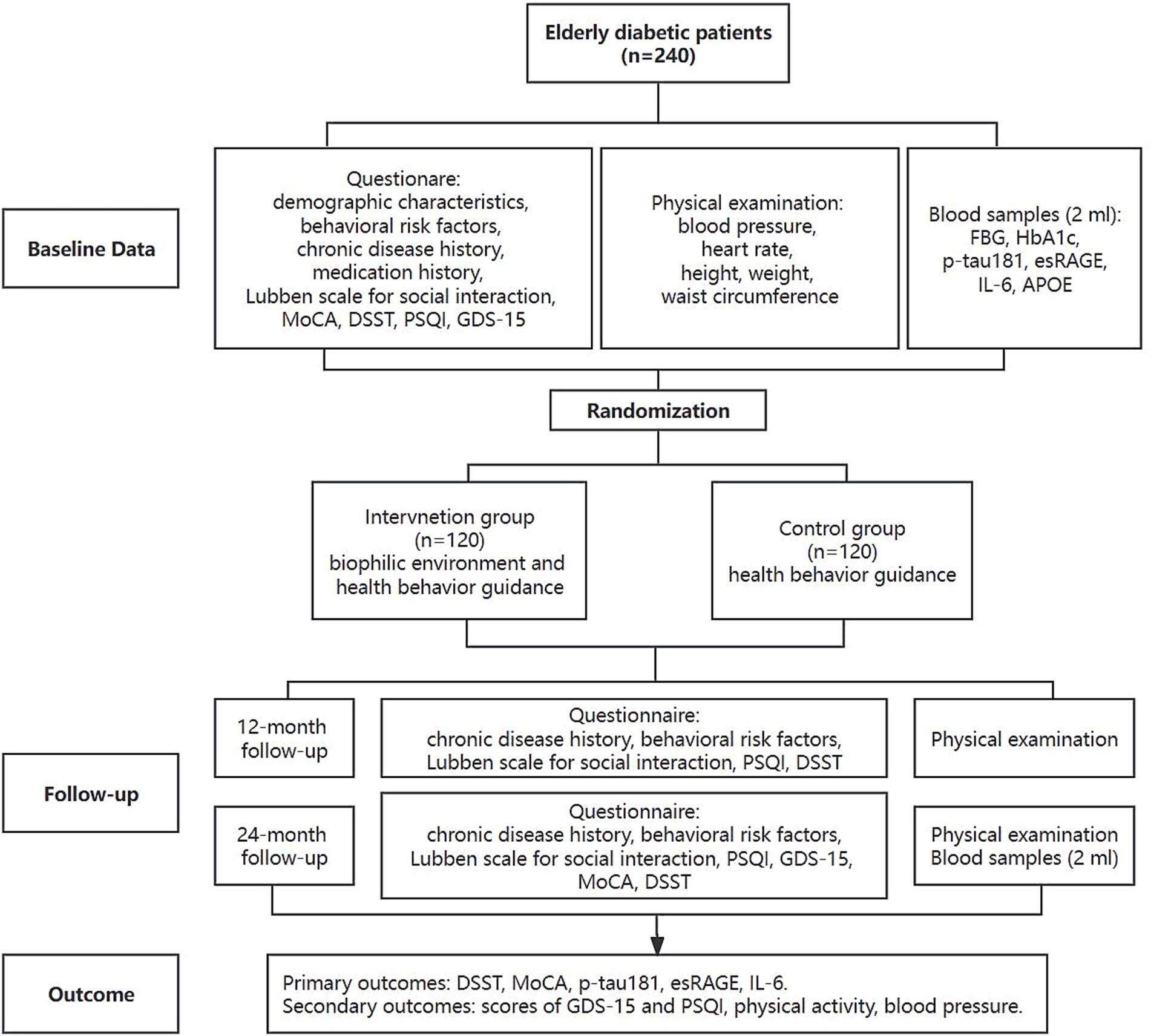
Figure 3. Long-term trial flow chart. MoCA, the Montreal Cognitive Assessment scale; DSST, the Digit Symbol Substitution Test; PSQI, the Pittsburgh Sleep Quality Index; GDS-15, 15-item Geriatric Depression Scale; FBG, fasting blood glucose; HbA1c, glycated hemoglobin; p-tau181, tau phosphorylated at threonine 181; esRAGE, endogenous secretory receptor for advanced glycation end-products; IL-6, interleukin-6; APOE, E4 variant of apolipoprotein E.
At baseline, after the participants sign the informed consent form, they will be administered a questionnaire to collect the following information: demographic characteristics (sex, date of birth, education), behavioral risk factors (dietary habits, smoking, alcohol consumption, physical activity, etc.), chronic disease history, medication history, the Lubben scale for social interaction, the Montreal Cognitive Assessment (MoCA) scale, DSST, the Pittsburgh Sleep Quality Index (PSQI), and the 15-item Geriatric Depression Scale (GDS-15). After completing the questionnaire, participants will undergo a physical examination (including blood pressure, heart rate, height, weight, and waist circumference), and then 2 mL blood samples will be collected by venipuncture. Then, researchers will distribute the wGT3x-BT accelerometer (Actigraph) to part of the participants. The wGT3x-BT accelerometer will objectively collect data regarding physical activity and sleep patterns, including time spent in light, moderate, and vigorous physical activity, sedentary time, sleep duration, and sleep efficiency. After completing the aforementioned steps, envelopes will be opened to decide which group the subjects would be enrolled in.
Both the intervention and control groups will receive health behavior guidance, while the intervention group will additionally receive an indoor biophilic environment intervention. Health behavior guidance includes personalized health behavior and dietary guidance based on the Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition) (Zhu and Society, 2021). Health promotion and personalized guidance will be conducted at each follow-up visit by medical doctors or professionals. The biophilic elements that are most effective in enhancing cognition during the short-term VR intervention trial will be used as the biophilic interventions in the long-term real environment intervention trial. Participants in the intervention group will be told to take the biophilic elements (such as indoor plants) home and place them in a visible place.
Long-term interventions will be followed up at 12 and 24 months. At the 12-month follow-up, behavioral risk factors, chronic disease history, Lubben scale for social interaction, PSQI, and DSST will be collected and a general physical examination will be performed. At the 24-month follow-up, behavioral risk factors, chronic disease history, Lubben scale for social interaction, PSQI, GDS-15, cognitive function (DSST, MoCA) will be assessed, a general physical examination will be performed, and blood samples will be collected again.
Blood samples will be collected in ethylenediaminetetraacetic acid (EDTA) anticoagulated vacutainer tubes. After centrifugation, blood cells and plasma will be stored separately. Plasma samples will be used for biomarker detection at both baseline and the 24-month follow-up, including glycated hemoglobin (HbA1c) levels, fasting blood glucose (FBG), tau phosphorylated at threonine 181 (p-tau181), endogenous secretory receptor for advanced glycation end-products (esRAGE), and interleukin-6 (IL-6). Blood cells will be used for DNA extraction and APOE genotyping. Blank control and duplicate samples will be used for quality control during the experiment.
At baseline and follow-up visits, we will fill out registration forms to record the use of the biophilic intervention facilities in the living room, in order to replace damaged biophilic elements in time and to provide persistent biophilic indoor environment intervention.
Participation is voluntary, and participants can withdraw consent at any time. Reasons for withdrawal will be documented.
In the event of any discomfort, including dizziness or nausea, experienced by a participant during the VR intervention, the intervention is promptly terminated. The participant is then given a two-minute break for recovery. If the discomfort continues post-rest, the participant is advised to withdraw from the study after a consultation.
Being lost to follow-up does not constitute withdrawal from the study. Research staffs will make efforts to re-engage participants for future assessments. For instance, if a participant is unreachable at the 12-month check-in, this is noted as a missed appointment, and attempts will be made to reach them for the 24-month follow-up.
Researchers from the survey group collect epidemiological data and assess participants’ cognitive function through questionnaires. Survey group researchers are blinded to the group allocation. The VR intervention process cannot be completed independently by participants. VR operators need to assist in the procedure and guide participants to fully engage with the VR scene. Therefore, it is not feasible to blind either the participants or the VR operators. To minimize bias, cognitive outcome assessments will be conducted by survey group researchers who are not involved in the VR intervention.
Since biophilic elements are easily identifiable, only questionnaire administrators, outcome assessors, and data analysts will be blinded to the group allocation.
1. Primary outcome: cognitive function, evaluated using the DSST and BDS scales.
2. Secondary outcome: scores of the SD and the RS scales, as well as blood pressure and heart rate.
1. Primary outcome: cognitive function assessed by the DSST and MoCA scales, as well as concentrations plasma of p-tau181, esRAGE and IL-6.
2. Secondary outcome: the amount of physical activity, blood pressure, scores of GDS-15 and PSQI. Participants will be asked to report the number of days per week they engage in vigorous physical activity (VPA), moderate physical activity (MPA), and walking, along with the daily duration of these activities. The metabolic equivalents (METs) of each study subject will be assigned and calculated based on the above information (Deng et al., 2008), and the amount of physical activity is the sum of METs.
The DSST and BDS tests have been widely used in the field of VR environments for cognitive function, and they are highly responsive to the immediate effects of short-term interventions (Liu et al., 2022; Yin et al., 2018). Therefore, cognitive function is assessed by DSST (score range: 0–90) and BDS (score range: 0–9) scales. The DSST test is a simple and fast assessment tool that measures the ability to link symbols with numbers in 90 s (Beres and Baron, 1981). The DSST score is the number of symbols correctly filled in consecutively within 90 s. In the BDS scale, testing begins with three-digit numbers, which are read aloud to the participant, who is then required to repeat them in reverse. The test progresses sequentially to nine-digit numbers, with each sequence allowing up to two attempts. If a participant fails to correctly repeat a sequence of a specified length twice consecutively, the test is stopped. The number of digits in the longest correctly repeated sequence serves as the measure of cognition.
Cognitive scores will be derived from the DSST and MoCA scales (score range: 0–30). The MoCA can track gradual, multidimensional cognitive decline over extended periods, complementing DSST’s focus on processing speed—a domain particularly impaired in diabetes-related cognitive dysfunction (Li et al., 2023; Rawlings et al., 2015). The DSST score measurement is the same as in the short-term trial. The MoCA is a brief cognitive screening tool with high sensitivity in detecting MCI (Nasreddine et al., 2005). It measures several cognitive domains, including attention, memory, delayed recall, language, executive function, abstraction, and orientation to time and place (Bischoff-Ferrari et al., 2020). The MoCA consists of 30 questions, and the score is equal to the number of correct answers out of the 30 items. If the individual reports 12 years of education or less, an additional point is added.
Randomization is conducted by a computer-generated list of random numbers made by independent statisticians without any clinical involvement in the study. The block randomization sequence is generated using SAS 9.4 software (PROC PLAN). The randomized block sizes are set to 8 and 16 for the short-term VR intervention trial and 2 and 4 for the long-term real environment intervention trial. After obtaining eligible patient consent, allocations are determined using sequentially numbered sealed envelopes containing information disclosing the type of intervention to be applied. Additionally, group assignments will be concealed until the intervention begins.
The randomized block analysis of the variance module of PASS 11.0 was used to calculate the sample size. According to previous literature (Liao et al., 2020), the MoCA scores would increase by 0.5 points, and the Chinese version of the Verbal Learning Test (CVVLT) immediate recall scores would increase by 1.0 point after VR intervention. The DSST has been found to be more sensitive than the MoCA and CVVLT. Thus, we conservatively assumed that the mean difference in DSST scores between the intervention and control groups would be 1.0, with a standard deviation of 1.2. The number of blocks was set at 8, the significance level was set at p < 0.05 and the statistical power was set at 90%. Based on the above parameters, the minimum sample size per block is six individuals. Considering the possibility of noncompliance or refusal to participate, the sample size was increased by 20%, resulting in eight individuals per block. Thus, there are eight blocks in the short-term trial, with each block containing eight individuals.
The randomized block analysis of the variance module of PASS 11.0 was used to calculate the sample size. Due to the lack of long-term longitudinal studies on the impact of biophilic living environments on the MoCA scores in elderly diabetic patients, we referred to studies on the impact of natural environments on cognitive scores. Changes in cognitive scores ranged from 0.020 to 0.029 for each interquartile range shift in the Normalized Difference Vegetation Index (NDVI) (De Keijzer et al., 2018). Based on these findings, we set the between-group difference in cognitive scores at 0.02, with a standard deviation of 0.017, an intraclass correlation coefficient of 0.02, and the number of blocks was set at 2. With these parameters, achieving a statistical power of 90% at the 0.05 level of two-sided significant difference requires 99 participants per group. Accounting for about 20% loss to follow-up, each group will initially need to enroll at least 120 participants, totaling 240 participants across both intervention and control groups. Considering that our participants are older adults, the likelihood of noncompliance is higher than others. Therefore, we chose a 20% non-compliance rate to ensure the study has sufficient statistical power.
Furthermore, the logistic regression module of PASS11.0 was used to calculate the sample size required for analyzing the association between the APOE4 genotype and cognitive function. According to previous research, the prevalence of MCI in Chinese people aged 60 years and older is about 15% (Jia et al., 2020), the odds ratio of the association between APOE4 and cognitive impairment in the Chinese population was about 2.5 (Jiang et al., 2017), the R2 of APOE4 with other covariates, such as age and gender, is about 0.05, with the significance level was set at 0.05. Based on these parameters, achieving a power of 90% in a two-sided test requires 103 participants. In summary, the long-term trial will include at least 120 subjects in each group.
The analysis will be carried out according to the intention-to-treat principle. Given the short duration of this trial, missing data is expected to be minimal. Therefore, a single imputation will be used to process the incomplete data. Outliers will be identified using the interquartile range (IQR) method, defined as values below Q1 − (1.5 × IQR) or above Q3 + (1.5 × IQR), and will be replaced with Q1 − (1.5 × IQR) and Q3 + (1.5 × IQR), respectively. One-way analysis of variance (ANOVA) (for continuous and normally distributed variables) and chi-square test (for categorical variables) will be conducted to assess the baseline equivalence between the eight groups. If there are differences in characteristics between groups at baseline, the differences will be adjusted by performing multiple linear regression. ANOVA will be used to compare whether there are statistically significant differences in cognitive scores, heart rate and blood pressure among the eight groups. For each group, paired t-tests will be conducted to examine whether changes in cognitive scores, heart rate, and blood pressure are statistically significant between baseline, pre-intervention, and post-intervention. The identification of optimal biophilic elements will follow a two-stage analytic protocol. First, multiple linear regression models adjusted for covariates will be fitted to compare post-VR intervention cognitive scores between each intervention group and the control. Groups achieving a covariate-adjusted p < 0.1 in these pairwise comparisons will be considered statistically promising. Subsequently, among these candidate groups, the intervention demonstrating the largest adjusted mean difference in cognitive scores relative to the control group will be selected for long-term real environment intervention. Multiple linear regression will be used to evaluate the cognitive improvement in each group after adjusting for covariates. Continuous variables will be assessed for normality prior to analysis. If the data are not normally distributed, the Kruskal-Wallis H test will be used to compare the differences between the eight groups.
The modified intention-to-treat population (mITT) will be used for statistical analysis. Missing values will be imputed using multiple imputation. Firstly, two sample t-tests (for continuous and normally distributed variables) and chi-square test (for categorical variables) will be conducted to assess the baseline equivalence between the intervention and control groups. Two sample t-tests will be used to compare whether cognitive scores are statistically different between two groups. Multiple linear regression will be used to demonstrate whether the intervention is statistically associated with cognitive scores after adjusting for potential confounders. Repeated measures ANOVA will be used to compare cognitive scores across groups. The potential confounders will be corrected in the mixed-effect model to determine the association between intervention and cognitive scores. If the intervention has a direct effect on cognitive function, longitudinal causal mediation analysis will be further used to clarify the mediating factors through which the intervention may affect cognition.
To explore the interaction of APOE4 and the biophilic environment on cognition, we will perform stratified analysis according to groups to clarify the main effects of APOE4 on cognitive function. Then, mixed models will be used to adjust for potential covariates and to elucidate the main effect of APOE4 on cognitive function in each group. Finally, the interaction term between the APOE4 and the intervention group will be included in the mixed-effects model to identify the effect of the genetic-environmental interaction on cognitive function.
In our study, all statistical tests are two-tailed, with a significance level of p < 0.05.
Data collected from participants will remain confidential. To ensure participant confidentiality, all personal identifying information will be securely stored separately from the study data, and access will be restricted to authorized personnel only. All data will be scrutinized and double-entered by the researchers using EpiData 3.1 to ensure accuracy. After verification, the data will be imported into SAS 9.4 for cleaning and storage.
We developed investigation manuals and provided standardized training for all personnel involved in the project, including VR operators, data collectors, clinicians, and laboratory staffs. Sequentially numbered opaque sealed envelopes are used for allocation concealment, and epidemiological data collectors will be blinded to mitigate information bias. After the face-to-face questionnaire survey, quality control procedures, including preliminary variable range and logical error checks, are conducted at the investigation site. Make sure the age of the subjects is accurate by checking the date of birth on their ID cards. In order to ensure the accuracy of diabetes diagnosis, we will further check the medical records or medication records of the self-report diabetes.
To ensure that participants’ attention is maximally directed towards the biophilic elements during the VR experience, VR operators explain the VR environment to participants and guide them in observing the biophilic elements during the experience.
Biophilic intervention elements will be mailed to subjects, and project staffs will call them to confirm that they have received the intervention items. Usage instructions for the biophilic elements will be dispatched via cell phone message. Monthly follow-up will be conducted to ensure the maintenance of biophilic elements. Dead plants, animals, or damaged indoor decorations will be replaced to sustain the biophilic intervention.
A total of 2 mL whole blood sample will be collected by nurses with EDTA anticoagulant tubes. The blood samples will be centrifuged at room temperature at 1,500 rpm for 10 min. The separated plasma and blood cells will be stored in clearly labeled cryovials, respectively. Plasma and blood cells samples will be preserved in an ultra-low temperature freezer at −80°C. Plasma samples will be used for the quantitative detection of serum biomarkers (p-tau181, esRAGE, IL-6). Blood cells will be used for DNA extraction. Blank and positive controls will be incorporated into the experimental design to monitor non-specific reactions and reagent contamination.
To ensure follow-up rates, the following measures will be implemented: first, fully explain the purpose and procedures of the study to subjects during the recruitment phase. Second, participants will be asked to provide at least two types of contact information, including a mobile phone number, a fixed-line phone number, or a WeChat account. If participants do not reply during weekdays, attempts will be made on weekends. Third, appropriate incentives will be provided to the participants, including subject compensation and free health consultations offered by neurologists from tertiary hospitals.
The anticipated risk to participants in this study is lower than that of routine physical examinations. Participants will be instructed to remove the VR headset if they have any adverse effects or discomfort.
Diabetes has become an increasingly critical public health problem, with a rising prevalence and high rates of disability and mortality. Moreover, diabetes is a major risk factor for cognitive impairment (Cukierman-Yaffe et al., 2020). Approximately 26% of people over 60 with diabetes suffer from MCI, and 36.9% have dementia (Jia et al., 2020). Cognitive impairment not only diminishes quality of life but also hinders diabetes management (Ojo and Brooke, 2015). Consequently, it is necessary to explore effective interventions to curb the progression of cognitive impairment in the elderly diabetic population.
Current researches primarily focus on conventional glucose-lowering treatments (Cukierman-Yaffe et al., 2020; Li et al., 2021; Ryan et al., 2006), cognitive training (Silverman et al., 2023; Wong et al., 2020), dietary nutrition (Lotan et al., 2021), and physical exercise (Chen Y. N. et al., 2023). Each of the four methods mentioned above has positive effects on cognitive function in diabetic patients. A common problem with these approaches is that their effectiveness depends on patient adherence. Biophilic design, a method of natural intervention, solves the problem of patient compliance and compensates for the shortcomings of the above methods. An increasing number of studies investigate the effects of biophilic design in indoor environments on health conditions (Lei et al., 2021; Li et al., 2022; Yin et al., 2019). However, most of these studies have focused on incorporating green vegetation, with most biophilic interventions involving short-term exposure through VR environments. Few studies have explored long-term interventions in real environments. In our study, we will evaluate diverse indoor biophilic elements, including both biophilic decorations and ornamental fish. Our study aims to identify the most effective biophilic elements or combinations for improving cognitive function by VR technology in elderly diabetic patients, and then use optimal biophilic elements for long-term real indoor environmental interventions. The findings from this study will be utilized to design a healing living environment in this population to effectively protect cognitive function. Furthermore, these findings could be applied to the design of biophilic environments in hospitals, nursing homes, and even private homes, providing therapeutic spaces that promote cognitive health. This practical application of biophilic design could help guide clinicians, architects, and healthcare providers in creating spaces that optimize cognitive health outcomes.
This study has the following strengths. First, the VR scene is designed based on a standard one-bedroom house displayed on a real estate platform in the project’s implementation area. Experiencing scenes close to real life in VR environments can weaken the bias of sensory experience caused by the strangeness of the virtual environments, and make the effect estimation of biophilic intervention more realistic and reliable. Second, the VR scene, including diverse biophilic design elements and interactive operations such as watering plants, feeding fish, opening doors, and pulling curtains, which provide a fully immersive VR experience, increases the authenticity of the VR environments and can maximize the simulation of the effect of the real environment intervention. Third, VR devices may impact cognitive function regardless of the specific VR intervention scene. To address this problem, cognitive tests will be conducted after participants use VR devices to experience both cluttered and clean environments. This approach may enable us to effectively control for potential confounding factors caused by the VR devices. Fourth, our study has both a short-term VR intervention and a long-term real environment intervention, which perfectly addresses the limitations of VR compared to real environments. Finally, since APOE4 is the strongest genetic predisposition factor for cognitive impairment, exploring its interactions with the biophilic environment could provide evidence for formulating personalized interventions.
This study also has several limitations. First, the study is conducted in a single center and focuses only on elderly diabetics, which limits the generalizability of the findings. Second, the VR scene contains many furnishings, which may cause participants to ignore specific intervention elements assigned to them. To avoid this issue, researchers in the VR group assist subjects in noticing the assigned elements through verbal guidance and cues. Third, the Mini-Mental State Examination (MMSE) (Tsoi et al., 2015) and MoCA (Nasreddine et al., 2005) are widely used scales that comprehensively assess cognitive function (Islam et al., 2023; Miura et al., 2024), however, they lack sensitivity to detect immediate cognitive changes. Therefore, we use the DSST and BDS scales to evaluate cognitive scores in the short-term VR intervention trial. The DSST primarily assesses working memory and processing speed, while the BDS focuses on memory capacity and attention. Although they are not as comprehensive as MMSE and MOCA, they are more sensitive to short-term cognitive changes and are widely used in cognitive assessments (Cukierman-Yaffe et al., 2020; Greendale et al., 2021; Tian et al., 2015).
This study received approval from the Ethics Committee of Capital Medical University (Approval No: Z2023SY019) on May 12, 2023. Subjects will receive a thorough explanation and be required to sign an informed consent form before participating in the study. The results of this trial will be disseminated through academic conferences and publications in international peer-reviewed journals. Any major protocol modifications will be communicated to the investigators, Ethics Committee, participants, trial registries, and journals. All methods will be performed in accordance with the Declaration of Helsinki.
JD: Investigation, Methodology, Writing – original draft, Writing – review & editing. MW: Conceptualization, Software, Writing – review & editing. HZ: Conceptualization, Writing – review & editing. ZW: Conceptualization, Writing – review & editing. XM: Conceptualization, Software, Writing – review & editing. YaS: Investigation, Writing – review & editing. YuS: Investigation, Writing – review & editing. WD: Conceptualization, Writing – review & editing. ZS: Conceptualization, Writing – review & editing. KL: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Natural Science Foundation of China, grant number 82273756.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Amiot, C. E., and Bastian, B. (2015). Toward a psychology of human-animal relations. Psychol. Bull. 141, 6–47. doi: 10.1037/a0038147
Acquadro Maran, D., Capitanelli, I., Cortese, C. G., Ilesanmi, O. S., Gianino, M. M., and Chirico, F. (2022). Animal-assisted intervention and health care Workers’ psychological health: a systematic review of the literature. Animals (Basel). 12:383. doi: 10.3390/ani12030383
American Diabetes Association Professional Practice Committee. Older Adults: Standards of Care in Diabetes - 2024. Diabetes care. (2024) 47, S244–S257. doi: 10.2337/dc24-S013
Barbiero, G., and Berto, R. (2021). Biophilia as evolutionary adaptation: an onto-and phylogenetic framework for biophilic design. Front. Psychol. 12:700709. doi: 10.3389/fpsyg.2021.700709
Beres, C. A., and Baron, A. (1981). Improved digit symbol substitution by older women as a result of extended practice. J. Gerontol. 36, 591–597. doi: 10.1093/geronj/36.5.591
Besser, L. (2021). Outdoor green space exposure and brain health measures related to Alzheimer's disease: a rapid review. BMJ Open 11:e043456. doi: 10.1136/bmjopen-2020-043456
Biessels, G. J., and Despa, F. (2018). Cognitive decline and dementia in diabetes mellitus: mechanisms and clinical implications. Nat. Rev. Endocrinol. 14, 591–604. doi: 10.1038/s41574-018-0048-7
Bischoff-Ferrari, H. A., Vellas, B., Rizzoli, R., Kressig, R. W., da Silva, J. A. P., Blauth, M., et al. (2020). Effect of vitamin D supplementation, Omega-3 fatty acid supplementation, or a strength-training exercise program on clinical outcomes in older adults the DO-HEALTH randomized clinical trial. J. Am. Med. Assoc. 324, 1855–1868. doi: 10.1001/jama.2020.16909
Bratman, G. N., Hamilton, J. P., and Daily, G. C. (2012). The impacts of nature experience on human cognitive function and mental health. Ann. New York Acad. Sci. 1249, 118–136. doi: 10.1111/j.1749-6632.2011.06400.x
Chen, P. C., Hong, C. T., Chen, W. T., Chan, L., and Chien, L. N. (2023). Metformin adherence reduces the risk of dementia in patients with diabetes: a population-based cohort study. Endocr. Pract. 29, 247–253. doi: 10.1016/j.eprac.2023.01.007
Chen, X., Lee, C., and Huang, H. (2022). Neighborhood built environment associated with cognition and dementia risk among older adults: a systematic literature review. Soc. Sci. Med. 292:114560. doi: 10.1016/j.socscimed.2021.114560
Chen, Y. N., Qin, J. W., Tao, L. Y., Liu, Z. Z., Huang, J., Liu, W. L., et al. (2023). Effects of tai chi Chuan on cognitive function in adults 60 years or older with type 2 diabetes and mild cognitive impairment in China: a randomized clinical trial. JAMA Netw. Open 6:14. doi: 10.1001/jamanetworkopen.2023.7004
Cukierman-Yaffe, T., Gerstein, H. C., Colhoun, H. M., Diaz, R., García-Pérez, L. E., Lakshmanan, M., et al. (2020). Effect of dulaglutide on cognitive impairment in type 2 diabetes: an exploratory analysis of the REWIND trial. Lancet Neurol. 19, 582–590. doi: 10.1016/S1474-4422(20)30173-3
De Coninck, L., Declercq, A., Bouckaert, L., Vermandere, M., Graff, M. J. L., and Aertgeert, B. (2021). Perspectives of older adults with a chronic condition on functioning, social participation and health: a qualitative study. BMC Geriatr. 21:12. doi: 10.1186/s12877-021-02365-w
De Keijzer, C., Tonne, C., Basagaña, X., Valentín, A., Singh-Manoux, A., Alonso, J., et al. (2018). Residential surrounding greenness and cognitive decline: a 10-year follow-up of the Whitehall II cohort. Environ. Health Perspect. 126:077003. doi: 10.1289/EHP2875
Deng, H. B., Macfarlane, D. J., Thomas, G. N., Lao, X. Q., Jiang, C. Q., Cheng, K. K., et al. (2008). Reliability and validity of the ipaq-chinese: the guangzhou biobank cohort study. Med Sci Sports Exerc. 40, 303–307. doi: 10.1249/mss.0b013e31815b0db5
Deslippe, A. L., Soanes, A., Bouchaud, C. C., Beckenstein, H., Slim, M., Plourde, H., et al. (2023). Barriers and facilitators to diet, physical activity and lifestyle behavior intervention adherence: a qualitative systematic review of the literature. Int. J. Behav. Nutr. Phys. Act. 20:25. doi: 10.1186/s12966-023-01424-2
Dogra, S., Ashe, M. C., Biddle, S. J. H., Brown, W. J., Buman, M. P., Chastin, S., et al. (2017). Sedentary time in older men and women: an international consensus statement and research priorities. Br. J. Sports Med. 51, 1526–1532. doi: 10.1136/bjsports-2016-097209
Espeland, M. A., Carmichael, O., Hayden, K., Neiberg, R. H., Newman, A. B., Keller, J. N., et al. (2018). Long-term impact of weight loss intervention on changes in cognitive function: exploratory analyses from the action for health in diabetes randomized controlled clinical trial. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 73, 484–491. doi: 10.1093/gerona/glx165
Felly, R., and Susanto, D. (2020). The changing effects through biophilic design in increasing elderly memory capacity. Case study: Sasana Tresna Werdha Yayasan Karya Bakti ria Pembangunan, Cibubur. IOP Conf. Ser.: Earth environ. Sci 452:012110. doi: 10.1088/1755-1315/452/1/012110
Franco, M. R., Tong, A., Howard, K., Sherrington, C., Ferreira, P. H., Pinto, R. Z., et al. (2015). Older people's perspectives on participation in physical activity: a systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 49, 1268–1276. doi: 10.1136/bjsports-2014-094015
Frank, M., Hensel, J., Baak, L., Schramm, S., Dragano, N., Weimar, C., et al. (2021). Interaction of Alzheimer's disease-associated genetic risk with indicators of socioeconomic position on mild cognitive impairment in the Heinz Nixdorf recall study. J. Alzheimers Dis. 82, 1715–1725. doi: 10.3233/JAD-210244
Greendale, G. A., Han, W. J., Huang, M. H., Upchurch, D. M., Karvonen-Gutierrez, C., Avis, N. E., et al. (2021). Longitudinal assessment of physical activity and cognitive outcomes among women at midlife. JAMA Netw. Open 4:18. doi: 10.1001/jamanetworkopen.2021.3227
Hassan, A., and Zhang, D. S. (2024). Psychophysiological impact of touching landscape grass among older adults. J. Urban Health Bull. New York Acad. Med. 101, 792–803. doi: 10.1007/s11524-024-00875-7
Hung, S.-H., and Chun, Y. (2021). Health benefits of evidence-based biophilic-designed environments: a review. J. People Plants Environ. 24, 1–16. doi: 10.11628/ksppe.2021.24.1.1
Islam, N., Hashem, R., Gad, M., Brown, A., Levis, B., Renoux, C., et al. (2023). Accuracy of the Montreal cognitive assessment tool for detecting mild cognitive impairment: a systematic review and meta-analysis. Alzheimers Dement. 19, 3235–3243. doi: 10.1002/alz.13040
Jenkins, J. L. (1986). Physiological effects of petting a companion animal. Psychol. Rep. 58, 21–22. doi: 10.2466/pr0.1986.58.1.21
Jia, L. F., Du, Y. F., Chu, L., Zhang, Z. J., Li, F. Y., Lyu, D. Y., et al. (2020). Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health 5, E661–E671. doi: 10.1016/S2468-2667(20)30185-7
Jiang, Y. X., He, T., Deng, W. S., and Sun, P. (2017). Association between apolipoprotein E gene polymorphism and mild cognitive impairment: a meta-analysis. Clin. Interv. Aging 12, 1941–1949. doi: 10.2147/CIA.S143632
Kiryu, T., and So, R. H. Y. (2007). Sensation of presence and cybersickness in applications of virtual reality for advanced rehabilitation. J. Neuroeng. Rehabil. 4:5. doi: 10.1186/1743-0003-4-34
Kwok, T., Lee, J., Ma, R. C., Wong, S. Y., Kung, K., Lam, A., et al. (2017). A randomized placebo controlled trial of vitamin B12 supplementation to prevent cognitive decline in older diabetic people with borderline low serum vitamin B12. Clin. Nutr. 36, 1509–1515. doi: 10.1016/j.clnu.2016.10.018
Latini, A., Marcelli, L., Di Giuseppe, E., and D'Orazio, M. (2024). Investigating the impact of greenery elements in office environments on cognitive performance, visual attention and distraction: an eye-tracking pilot-study in virtual reality. Appl. Ergon. 118:104286. doi: 10.1016/j.apergo.2024.104286
Lee, E. J., and Park, S. J. (2021). A preference-driven smart home service for the elderly's biophilic experience. Sensors 21:22. doi: 10.3390/s21155108
Lei, Q., Yuan, C., and Lau, S. S. Y. (2021). A quantitative study for indoor workplace biophilic design to improve health and productivity performance. J. Clean. Prod. 324:129168. doi: 10.1016/j.jclepro.2021.129168
Li, Q., Jia, M. X., Yan, Z. C., Sun, F., He, C. K., Li, Y. S., et al. (2021). Activation of glucagon-like Peptide-1 receptor ameliorates cognitive decline in type 2 diabetes mellitus through a metabolism-independent pathway. J. Am. Heart Assoc. 10:17. doi: 10.1161/JAHA.120.020734
Li, Z., Wang, Y., Liu, H., and Liu, H. (2022). Physiological and psychological effects of exposure to different types and numbers of biophilic vegetable walls in small spaces. Build. Environ. 225:109645. doi: 10.1016/j.buildenv.2022.109645
Li, Q., Zhao, Y. J., Guo, H. Y., Li, Q., Yan, C. Y., Li, Y. S., et al. (2023). Impaired lipophagy induced-microglial lipid droplets accumulation contributes to the buildup of TREM1 in diabetes-associated cognitive impairment. Autophagy 19, 2639–2656. doi: 10.1080/15548627.2023.2213984
Liao, Y.-Y., Tseng, H.-Y., Lin, Y.-J., Wang, C.-J., and Hsu, W.-C. (2020). Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 56, 47–57. doi: 10.23736/S1973-9087.19.05899-4
Liebzeit, D., Kuo, W. C., Carlson, B., Mueller, K., Koscik, R. L., Smith, M., et al. (2022). Relationship of cognitive and social engagement to health and psychological outcomes in community-dwelling older adults. Nurs. Res. 71, 295–302. doi: 10.1097/NNR.0000000000000589
Liu, Z., He, Z., Yuan, J., Lin, H., Fu, C., Zhang, Y., et al. (2022). Application of immersive virtual-reality-based puzzle games in elderly patients with post-stroke cognitive impairment: a pilot study. Brain Sci. 13:79. doi: 10.3390/brainsci13010079
Liu, H., Lin, J., and Lin, W. (2024). Cognitive mechanisms and neurological foundations of companion animals' role in enhancing human psychological well-being. Front. Psychol. 15:1354220. doi: 10.3389/fpsyg.2024.1354220
Lotan, R., Ganmore, I., Livny, A., Itzhaki, N., Waserman, M., Shelly, S., et al. (2021). Effect of advanced glycation end products on cognition in older adults with type 2 diabetes: results from a pilot clinical trial. J. Alzheimers Dis. 82, 1785–1795. doi: 10.3233/JAD-210131
Miura, K. W., Kudo, T., and Otake-Matsuura, M. (2024). Web-based group conversational intervention on cognitive function and comprehensive functional status among Japanese older adults: protocol for a 6-month randomized controlled trial. JMIR Res. Protoc. 13:e56608. doi: 10.2196/56608
Montagne, A., Nation, D. A., Sagare, A. P., Barisano, G., Sweeney, M. D., Chakhoyan, A., et al. (2020). APOE4 leads to blood–brain barrier dysfunction predicting cognitive decline. Nature 581:71. doi: 10.1038/s41586-020-2247-3
Mostajeran, F., Steinicke, F., Reinhart, S., Stuerzlinger, W., Riecke, B. E., and Kühn, S. (2023). Adding virtual plants leads to higher cognitive performance and psychological well-being in virtual reality. Sci. Rep. 13:8053. doi: 10.1038/s41598-023-34718-3
Motooka, M., Koike, H., Yokoyama, T., and Kennedy, N. L. (2006). Effect of dog-walking on autonomic nervous activity in senior citizens. Med. J. Aust. 184, 60–63. doi: 10.5694/j.1326-5377.2006.tb00116.x
Munshi, M. N. (2017). Cognitive dysfunction in older adults with diabetes: what a clinician needs to know. Diabetes Care 40, 461–467. doi: 10.2337/dc16-1229
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Ojo, O., and Brooke, J. (2015). Evaluating the association between diabetes, cognitive decline and dementia. Int. J. Environ. Res. Public Health 12, 8281–8294. doi: 10.3390/ijerph120708281
Ong, K. L., Stafford, L. K., McLaughlin, S. A., Boyko, E. J., Vollset, S. E., Smith, A. E., et al. (2023). Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the global burden of disease study 2021. Lancet 402, 203–234. doi: 10.1016/S0140-6736(23)01301-6
Pa, J., Aslanyan, V., Casaletto, K. B., Rentería, M. A., Harrati, A., Tom, S. E., et al. (2022). Effects of sex, APOE4, and lifestyle activities on cognitive reserve in older adults. Neurology 99, E789–E798. doi: 10.1212/WNL.0000000000200675
Parish, S., Mafham, M., Offer, A., Barton, J., Wallendszus, K., Stevens, W., et al. (2022). Effects of aspirin on dementia and cognitive function in diabetic patients: the ASCEND trial. Eur. Heart J. 43, 2010–2019. doi: 10.1093/eurheartj/ehac179
Parra Rizo, M. A., and López Marin, P. (2020). Efecto y adecuación del ejercicio para la mejora cardiovascular de la población mayor de 65 años. Revista de Psicología de la Salud (New Age) 8, 1–15. doi: 10.21134/pssa.v8i1.670
Pettit, T., Irga, P. J., and Torpy, F. R. (2018). Towards practical indoor air phytoremediation: a review. Chemosphere 208, 960–974. doi: 10.1016/j.chemosphere.2018.06.048
Rawlings, A. M., Sharrett, A. R., Schneider, A. L., Coresh, J., Albert, M., Couper, D. J., et al. (2015). Diabetes in midlife and cognitive change over 20 years: the atherosclerosis risk in communities neurocognitive study. Ann. Internal Med., 161, 785–193. doi: 10.7326/M14-0737
Riva, G., Mancuso, V., Cavedoni, S., and Stramba-Badiale, C. (2020). Virtual reality in neurorehabilitation: a review of its effects on multiple cognitive domains. Expert Rev. Med. Devices 17, 1035–1061. doi: 10.1080/17434440.2020.1825939
Rivera Miranda, P., Trujillo Altamirano, C., Yáñez-Yáñez, R., Draguicevic, N., Ardle, M., Quintana-Peña, P., et al. (2024). Strength training to prevent falls on the elderly: a systematic review. Revista Salud Uninorte 40, 216–238. doi: 10.14482/sun.40.01.650.452
Ryan, C. M., Freed, M. I., Rood, J. A., Cobitz, A. R., Waterhouse, B. R., and Strachan, M. W. J. (2006). Improving metabolic control leads to better working memory in adults with type 2 diabetes. Diabetes Care 29, 345–351. doi: 10.2337/diacare.29.02.06.dc05-1626
Shen, J., Zhang, X., and Lian, Z. (2020). Impact of wooden versus nonwooden interior designs on office Workers' cognitive performance. Percept. Mot. Skills 127, 36–51. doi: 10.1177/0031512519876395
Silverman, J. M., Zhu, C. W., Schmeidler, J., Lee, P. G., Alexander, N. B., Guerrero-Berroa, E., et al. (2023). Does computerized cognitive training improve diabetes self-management and cognition? A randomized control trial of middle-aged and older veterans with type 2 diabetes. Diabetes Res. Clin. Pract. 195:110149. doi: 10.1016/j.diabres.2022.110149
Sonne, D. P., and Hemmingsen, B. (2017). Standards of medical Care in Diabetes-2017. Diabetes care 2017;40(Suppl. 1):S1-S135. Diabetes Care 40, E92–E93. doi: 10.2337/dc17-0299
Srikanth, V., Sinclair, A. J., Hill-Briggs, F., Moran, C., and Biessels, G. J. (2020). Type 2 diabetes and cognitive dysfunction—towards effective management of both comorbidities. Lancet Diab. Endocrinol. 8, 535–545. doi: 10.1016/S2213-8587(20)30118-2
Stringa, N., van Schoor, N. M., Milaneschi, Y., Ikram, M. A., Del Panta, V., Koolhaas, C. M., et al. (2020). Physical activity as moderator of the association between APOE and cognitive decline in older adults: results from three longitudinal cohort studies. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 75, 1880–1886. doi: 10.1093/gerona/glaa054
Tian, Q., Simonsick, E. M., Resnick, S. M., Shardell, M. D., Ferrucci, L., and Studenski, S. A. (2015). Lap time variation and executive function in older adults: the Baltimore longitudinal study of aging. Age Ageing 44, 796–800. doi: 10.1093/ageing/afv076
Tsoi, K. K. F., Chan, J. Y. C., Hirai, H. W., Wong, S. Y. S., and Kwok, T. C. Y. (2015). Cognitive tests to detect dementia A systematic review and meta-analysis. JAMA Intern. Med. 175, 1450–1458. doi: 10.1001/jamainternmed.2015.2152
Ulrich, R. S. (1984). View through a window may influence recovery from surgery. Science (New York, N.Y.) 224, 420–421. doi: 10.1126/science.6143402
Valentine, C., Steffert, T., Mitcheltree, H., and Steemers, K. J. B. (2024). Architectural neuroimmunology: a pilot study examining the impact of biophilic architectural design on neuroinflammation. Buildings 14:1292. doi: 10.3390/buildings14051292
van de Rest, O., Wang, Y. M., Barnes, L. L., Tangney, C., Bennett, D. A., and Morris, M. C. (2016). APOE ε4 and the associations of seafood and long-chain omega-3 fatty acids with cognitive decline. Neurology 86, 2063–2070. doi: 10.1212/WNL.0000000000002719
Verzwyvelt, L. A., McNamara, A., Xu, X. H., and Stubbins, R. (2021). Effects of virtual reality v. biophilic environments on pain and distress in oncology patients: a case-crossover pilot study. Sci. Rep. 11:7. doi: 10.1038/s41598-021-99763-2
Wallmann-Sperlich, B., Hoffmann, S., Salditt, A., Bipp, T., and Froboese, I. (2019). Moving to an "active" biophilic designed office workplace: a pilot study about the effects on sitting time and sitting habits of office-based workers. Int. J. Environ. Res. Public Health 16:13. doi: 10.3390/ijerph16091559
Wong, C. W., O, W. W., Wong, K. S., Ma, R., Hui, E., and Kwok, C. T. (2020). Randomized trial of a patient empowerment and cognitive training program for older people with diabetes mellitus and cognitive impairment. Geriatr Gerontol Int 20, 1164–1170. doi: 10.1111/ggi.14062
Yin, J., Arfaei, N., MacNaughton, P., Catalano, P. J., Allen, J. G., and Spengler, J. D. (2019). Effects of biophilic interventions in office on stress reaction and cognitive function: a randomized crossover study in virtual reality. Indoor Air 29, 1028–1039. doi: 10.1111/ina.12593
Yin, J., Yuan, J., Arfaei, N., Catalano, P. J., Allen, J. G., and Spengler, J. D. (2020). Effects of biophilic indoor environment on stress and anxiety recovery: a between-subjects experiment in virtual reality. Environ. Int. 136:105427. doi: 10.1016/j.envint.2019.105427
Yin, J., Zhu, S. H., MacNaughton, P., Allen, J. G., and Spengler, J. D. (2018). Physiological and cognitive performance of exposure to biophilic indoor environment. Build. Environ. 132, 255–262. doi: 10.1016/j.buildenv.2018.01.006
Yu, X. G., Xie, Z. Q., Yu, Y., Lee, J., Vazquez-Guardado, A., Luan, H. W., et al. (2019). Skin-integrated wireless haptic interfaces for virtual and augmented reality. Nature 575:473-+. doi: 10.1038/s41586-019-1687-0
Zhu, D., and Society, C. (2021). Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chinese J. Endocrinol. Metab. 37, 311–398. doi: 10.3760/cma.j.cn311282-20210304-00142
Zhu, A. N., Yan, L. J., Shu, C., Zeng, Y., and Ji, J. S. (2020). APOE ε4 modifies effect of residential greenness on cognitive function among older adults: a longitudinal analysis in China. Sci. Rep. 10:8. doi: 10.1038/s41598-019-57082-7
Zullig, L. L., Deschodt, M., Liska, J., Bosworth, H. B., and De Geest, S. (2019). “Moving from the trial to the real world: improving medication adherence using insights of implementation science” in Annual review of pharmacology and toxicology. ed. P. A. Insel, Annual review of pharmacology and toxicology, vol. 59 (Palo Alto: Annual Reviews), 423–445.
Keywords: indoor biophilic elements, cognition, elderly diabetic patients, virtual reality, APOE4
Citation: Dai J, Wang M, Zhang H, Wang Z, Meng X, Sun Y, Sun Y, Dong W, Sun Z and Liu K (2025) Effects of indoor biophilic environments on cognitive function in elderly patients with diabetes: study protocol for a randomized controlled trial. Front. Psychol. 16:1512175. doi: 10.3389/fpsyg.2025.1512175
Edited by:
Xinyi Zhu, Chinese Academy of Sciences (CAS), ChinaReviewed by:
María Antonia Parra Rizo, Miguel Hernández University of Elche, SpainCopyright © 2025 Dai, Wang, Zhang, Wang, Meng, Sun, Sun, Dong, Sun and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kuo Liu, bGl1a3VvQGNjbXUuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.