
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychol. , 10 February 2025
Sec. Developmental Psychology
Volume 16 - 2025 | https://doi.org/10.3389/fpsyg.2025.1472646
This article is part of the Research Topic Innovative and Cutting-edge Approaches to the Identification and Management of Autism Spectrum Disorders View all 6 articles
 Alberto Sánchez-Pedroche1*
Alberto Sánchez-Pedroche1* Eva Aguilar-Mediavilla1
Eva Aguilar-Mediavilla1 Mario Valera-Pozo1
Mario Valera-Pozo1 Daniel Adrover-Roig1
Daniel Adrover-Roig1 Magdalena Valverde-Gómez2
Magdalena Valverde-Gómez2In the latest autism observation, autism spectrum disorder (ASD) is more frequently diagnosed in males than in females. Efforts have been made in recent years to detect specific clinical patterns in females, improving their detection and diagnosis. Despite advancements, there are still challenges in detecting ASD in females. This preliminary study explores whether the age at the time of diagnosis of ASD in females is related to a higher severity index compared to male participants. A total of 202 participants (52 females; M = 5.51) in Spain underwent ADOS-2 assessment for ASD clinical severity. The results indicate a significant inverse association between the severity index and the age of diagnosis, which was independent of sex. Despite this, the present results revealed that the age at diagnosis was higher in females compared to males. Further analyses also revealed a tendency toward higher severity levels in females. Factors contributing to this difference in the age of diagnosis of ASD between females and males are discussed concerning the presumed differential characteristics of ASD in females.
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by persistent difficulties in social communication and restrictive repetitive patterns of behavior, interests, or activities. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (American Psychiatric Association [APA], 2014), ASD includes a range of symptoms that vary in intensity and presentation in each individual. The symptoms are present early in development, but they may not fully manifest until social demands exceed the child’s limited abilities or are masked by learning strategies (World Health Organization, 2019). In the DSM-5, the severity is based on impairments in social communication and restricted and repetitive patterns of behavior, ranging from grade 1 (requiring support) to grade 3 (requiring very substantial support). This variability has led to the term “spectrum” in the grading of this disorder.
The prevalence of ASD varies in different studies and populations. Based on the most current data available, the prevalence data is 1 in 36–2.78%- (CDC, Maenner et al., 2023), similarly to a recent systematic review of the global prevalence of ASD, which reports a range of 0.1 to 2.9% (Zeidan et al., 2022). Nevison and Zahorodny (2019) further analyzed trends in ASD prevalence across different racial and ethnic groups, showing significant variations in diagnostic rates over time. Regarding Spain, the estimated prevalence of diagnosed ASD among preschool children is 2.52%, while the prevalence among primary school children was lower (1.12%), and the ratio between boys and girls was 4:1 (Morales-Hidalgo et al., 2018). Among girls, the prevalence ranged from 0.39 to 0.58%, which is much lower than the overall 1% prevalence of ASD. This difference may reflect that diagnostic efforts and tools are more focused on early childhood, leading to higher detection rates in preschool children. Additionally, some children, particularly females, may camouflage symptoms or present subtler characteristics, delaying diagnosis until adolescence or adulthood (Hull et al., 2017; Rutherford et al., 2016).
Preschool-aged children in Spain are diagnosed at around 45 months, and elementary school children at around 87 months (Hernández et al., 2005). These results reflect a high number of diagnoses in the early stages of childhood, indicating a tendency toward an early diagnosis of ASD in Spain, which may unveil more severe patterns in preschool-aged children. A disparity has been observed in the prevalence of ASD depending on sex, being diagnosed more frequently in boys as compared to girls (Van Wijngaarden-Cremers et al., 2014). However, this difference in sex-related prevalence has been the subject of debate since girls and women with ASD often present different characteristics and manifestations that could go unnoticed under traditional diagnostic criteria (Werling and Geschwind, 2013). In the same vein, it is becoming increasingly evident that ASD may present differently in males compared to females (Wood-Downie et al., 2021). For a considerable time, the clinical focus and most of the research has been on the behavior manifestations typically observed in males with ASD, due to the higher prevalence of ASD in males. However, this research has the potential to introduce a bias in how the diagnosis of ASD is understood and manifested clinically and symptomatically in females (Montagut et al., 2018; Tofani et al., 2023). For example, girls with ASD may exhibit more nuanced social communication difficulties, such as an intense interest in people rather than objects, which may be misinterpreted as typical social behavior (Lai et al., 2015). Furthermore, they may engage in imaginative play, albeit with repetitive and scripted patterns, which may result in the symptoms being overlooked (Hiller et al., 2014). Furthermore, girls are more likely to disguise or conceal their symptoms, which may result in a higher rate of undetected cases (Hull et al., 2017). It is also important to note that females are more likely to receive a diagnosis later in adolescence or adulthood, particularly when symptoms are masked (Rutherford et al., 2016; Duvekot et al., 2017). In recent years, specific screening tools focusing on females with ASD, such as the ASSQ Girl (Kopp and Gillberg, 2011), have been developed to improve early detection and diagnosis in females. Despite these advances, challenges remain in the detection of ASD in girls, which may result in later diagnoses for those with lower severity rates.
Following the above revised literature, the main objective of this preliminary study was to analyze the relationship between the severity index and the age at the time of diagnosis. We expected that (1) girls would show a higher severity index and a higher age at diagnosis of ASD as compared to boys; (2) a larger severity index would be associated with an earlier age of diagnosis, particularly in girls.
We departed from an initial sample of 647 participants referred for diagnosis as possible ASD in the Balearic Islands (Ibiza and Formentera, Spain) during the years 2020–2024. All participants were assessed in accordance with the comprehensive clinical protocol of the Balearic Institute of Child and Adolescent Mental Health (IBSMIA), that includes the consideration of each participant’s developmental history and the screening with the Modified Checklist for Autism in Toddlers (M-CHAT; Robins et al., 2009), the Social Communication Questionnaire (SCQ; Rutter et al., 2003) and the NICE (National Institute for Health and Care Excellence) tests, and subsequently administered the gold standard ADOS-2 test (Lord et al., 2015). Four hundred and forty-five participants did not meet the clinical criteria for a diagnosis of ASD and were discarded from the final sample. A total of 202 participants (52 females) with a mean age of 5.49 years (SD = 4.063, range 1–16 years) were included in the final sample. All participants older than 3 years were enrolled in mainstream schools.
A power analysis indicated that a sample size of approximately 103 participants per group is required to detect a small to medium effect size (d = 0.39) with a significance level of 0.05 and a statistical power of 0.80. As expected, due to the inherent imbalance in autism prevalence between males and females, the final sample included 150 males and 52 females. Although the female group did not meet the benchmark set by the power analysis, this sample size remains substantial in the context of autism research, where females are significantly underrepresented. Furthermore, the total sample size (N = 202) is close to the combined requirement of 206 participants, supporting the validity of the statistical analyses performed.
To assess the severity of ASD symptoms, we used the Autism Diagnostic Observation Schedule, ADOS-2 (Lord et al., 2015). This scale is one of the most used instruments for ASD diagnosis in clinical practice, becoming a gold standard. The ADOS-2 is a standardized semi-structured direct observation scale designed to detect social and communicative behaviors within the autism spectrum, as well as characteristics of restricted repetitive and stereotyped behaviors. The ADOS-2 samples quantify individual’s behaviors and provides a clear diagnostic score as well as severity scores. It consists of five different modules depending on the level of expressive language and/or the age of the individual, and several algorithms that combine specific scores in several items observations to classify the assessed behaviors. Each algorithm has specific criteria that are applied during the evaluation and are used to assign a final score or categorization on the ASD. The algorithm totals are compared to the diagnostic classification limits. The ADOS-2 is one of the best psychometrically (specificity 95%, sensitivity 95%, inter-rater reliability 84%) evaluation tools in the diagnosis of ASD and has excellent diagnostic validity according to multiple studies (Zander et al., 2016).
This study was conducted in accordance with the ethical guidelines set forth by the relevant authorities, and all data pertaining to the participants were collected as part of the routine clinical evaluations. The participants were recruited from the IBSMIA (Balearic Institute of Mental Health for Children and Adolescents), a public service where children are assessed to determine the presence of ASD or other developmental difficulties. Prior to their participation, written informed consent was obtained from the parents or legal guardians, which included a clause authorizing the use of anonymized data for research purposes.
All assessments were conducted in four 60-min sessions at the IBSMIA facilities. Two researchers from the research team possess official clinical accreditation for the administration of the ADOS-2, having obtained it through IGAIN (University of Barcelona) and the “Hospital Universitari Mútua de Terrassa.” To guarantee the fidelity of administration, the research team held regular peer review sessions to supervise adherence to standardized procedures and scoring consistency.
For the ADOS-2, the raw data were transformed into a Calibrated Severity Scores ranging from 0 to10 following the mapping table of the ADOS-2 as compiled by Gotham et al. (2009). This mapping table standardizes raw ADOS totals into severity scores for consistent interpretation (see Table 1). This classification framework was employed exclusively for research purposes, with the objective of facilitating comparisons between groups. It does not supersede the clinical judgment necessitated for DSM-5 diagnostic criteria, which are predicated on the level of support required by the individual (American Psychiatric Association [APA], 2014). This table also allows the classification of the Calibrated Severity Score into Severity Levels. These levels correspond to the diagnostic classification of autism (American Psychiatric Association [APA], 2014), being the following: calibrated severity scores ranging from 1 to 3 (both included) correspond to a non-diagnosis of ASD and were not considered for the final sample; calibrated severity scores between 4 and 5 would correspond to the level 1 ASD diagnostic category and was coded as 2; calibrated severity scores between 6 and 8 would correspond to the level 2 ASD diagnostic category and was coded as level 3; and finally, calibrated severity scores between 9 and 10 would correspond to the level 3 ASD diagnostic category, and was coded as 4.

Table 1. Sex-dependent distribution of severity level.
The SPSSv.28 statistical package was used for data analysis. As the Calibrated Severity Score is a categorization of the raw data of ADOS-2, we used a Spearman Rho correlation to assess the relation between this variable and the age at the diagnostic in all sample and split by sex. We also performed two t-tests to compare the Calibrated severity Score and the age of diagnostic between males and females; and χ2 to compare the frequency distribution of the severity index between males and females. Finally, we used an ANOVA (2 × 3) with the factors Sex and Severity Level on the age of diagnostic.
Table 2 shows the descriptive statistics for the main variables of the present study split by sex.

Table 2. Descriptive statistics.
The mean age at diagnosis for males was lower than for females [t(200) = −2.436, p = 0.016, d = 0.39]. Contrary, the Calibrated Severity Score mean did not show significant differences between males and females [t(200) = −0.839, p = 0.402, d = 0.14].
The results show a significant negative relation between the age at the diagnosis and the Calibrated Severity Score according to the ADOS-2 for the whole sample (rho = −0.168, p = 0.017), indicating that a higher severity score is associated with a younger age of diagnosis. Although the correlation value was slightly higher for females (rho = −0.207, p = 0.141), only a significant negative correlation was found in males (rho = −0.173, p = 0.019), probably due to the lack of statistical power given the moderately low number of females in the final sample. Accordingly, Fisher’s Z conducted to examine whether the correlation pattern differed between males and females was non-significant (Z = −0.21; p = 0.831). Thus, associations between the Calibrated Severity Score and the age of diagnosis were independent of sex.
To further explore the distribution of Severity Levels and Sex (Table 1), contingency analyses were conducted, and revealed a tendency of higher Severity Levels in females relative to males [χ2(2) = 5.44, p = 0.066].
Complementarily, a two-way ANOVA was conducted to examine the effect of Sex and Severity Level on Age at Diagnosis (see Figure 1). The results showed a significant main effect of Sex on Age at the Diagnosis [F(1,201) = 4.96, p = 0.027, η2 = 0.025], but only a tendency toward significance in the Severity Level [F(2,201) = 2.897, p = 0.058, η2 = 0.029], and a non-significant interaction between Sex and Severity Level [F(5,201) = 0.494, p = 0.611, η2 = 0.005].
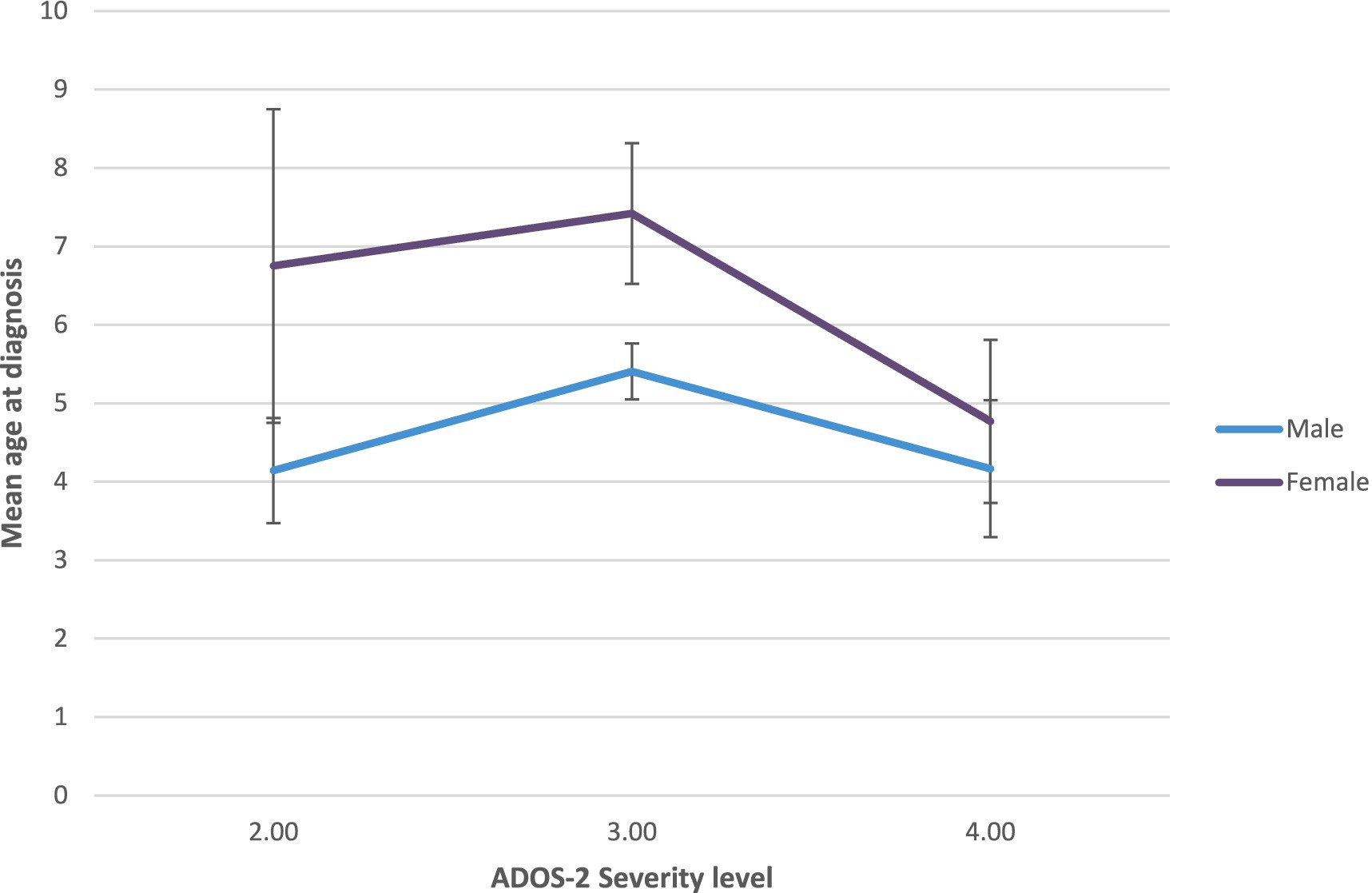
Figure 1. Age of diagnostic of ASD depending on calibrated severity score and sex.
According to the present study, our results support a difference in the age of diagnosis between females and males, being females diagnosed later as compared to males. Nevertheless, there is only a tendency for females to be more frequently classified into higher Severity Level categories of ASD compared to males, as measured by the ADOS-2. Besides, the relationship between symptom severity and age of diagnosis appears to be independent of sex, as reflected by the lack of interaction between these variables (see discussion about hypothesis 2 below). Despite the lack of interaction, a later age of diagnosis and a higher tendency in females to fall into the most severe categories according to the ADOS-2 may suggest a potential sex bias in diagnostic practices (Gesi et al., 2021). Therefore, these results aligned partially with several previous studies (Constantino and Charman, 2012; Giarelli et al., 2010; Van Wijngaarden-Cremers et al., 2014) that have also shown a sex bias in ASD diagnosis. These findings underscore the necessity of elucidating the sex-specific clinical manifestations. Late diagnoses in females may be associated with less overt, intricate symptoms or the capacity to disguise social challenges, as evidenced in prior investigations (Hull et al., 2017; Lai et al., 2015; Tofani et al., 2023). These observations highlight the need for sex-sensitive diagnostic approaches to improve early detection in females. Therefore, our first hypothesis, which stated that girls would show a higher severity index and be diagnosed with ASD at an older age than boys, was partially supported.
Besides, the present results reflect that there is a significant negative correlation between severity and age of diagnosis, although this correlation was not dependent on sex. This also partially supports our second hypothesis that a larger severity index would be associated with an earlier age of diagnosis, although undifferentiated between females and males. This was also confirmed by the lack of interaction between sex and severity over the age of diagnosis. These results differ somewhat from previous findings (Constantino and Charman, 2012; Giarelli et al., 2010; Van Wijngaarden-Cremers et al., 2014) which suggest that females require a greater degree of impairment than males to receive a diagnosis. The present results suggest a sex-biased diagnosis in females that is relatively independent of the severity level. This aligns with several previous findings showing that females are less likely to be correctly diagnosed with ASD and more likely to be misdiagnosed at first evaluation than men (Gesi et al., 2021).
Factors contributing to the higher age to be diagnosed with ASD in females relative to males may include a different manifestation of ASD in females than in males with less typical, atypical, and visible symptomatology than in males. For example, Van Wijngaarden-Cremers et al. (2014) reported significant sex differences with higher levels of repetitive and stereotyped behavior in males than in females. This lack of visibility could delay the diagnosis till females grow and new manifestations are added (Gesi et al., 2021; Mandy et al., 2012; Rutherford et al., 2016). Further discrepancies may be explained by additional factors, including societal biases in recognizing ASD symptoms in females or differences in developmental trajectories (Brickhill et al., 2023). It would be beneficial for future studies to consider broader cultural and socioeconomic influences on diagnostic timing (Begeer et al., 2013; Dworzynski et al., 2012).
Despite this sex bias in the age of diagnosis, probably a potentially real sex difference in ASD prevalence (Werling and Geschwind, 2013), as well an increased awareness in recent years about the detection of ASD in females and their distinct presentation profiles have also influenced the present results. Consequently, an increase in knowledge about the differential manifestation of ASD in men and women is needed to identify specific patterns of clinical presentation in females and improve both detection and diagnosis in females (Wood-Downie et al., 2021; Van Wijngaarden-Cremers et al., 2014).
Our results show some limitations. Although the sample size is sufficient based on the power analysis, a larger sample would help to draw more robust and generalizable conclusions about the prevalence and age of diagnosis of ASD in female population. A further limitation pertains to the unequal sample sizes between males and females, which mirrors the inherent sex-based discrepancy in autism prevalence. Despite the female group exhibiting smaller sample sizes than the benchmark stipulated in the power analysis, it remains a substantial and meaningful sample within the context of autism research. This is particularly salient when one considers the challenges associated with the recruitment of females with autism. This disparity has been acknowledged, and it is emphasized that the findings should be interpreted with caution, particularly in the context of generalizing sex-specific differences.
Besides, including additional factors such as the socioeconomic status of the family and parental concerns in future analyses could provide a more comprehensive understanding of the variables influencing the age at diagnosis. We acknowledge that the current study did not include these factors, which may limit the generalizability of the findings, and for this reason it may have to be taken with caution. Longitudinal studies would also be beneficial to track changes in diagnostic criteria and their impact on sex differences in ASD diagnosis over time.
A further limitation of the study is its exclusive reliance on ADOS-2 scores for the assessment of symptoms severity. This decision was taken to ensure objectivity and consistency in comparing severity of symptoms between male and female participants. However, it must be noted that cut-off scores for ADOS-2 are primarily based on male participants, which might reflect the current disproportion in the prevalence of ASD between males and females. This limitation must also be considered when interpreting findings, particularly the comparison of symptom severity levels across sexes. Furthermore, the use of specific screening tools focused on females with ASD, such as ASSQ Girl (Kopp and Gillberg, 2011), could help improve early detection and diagnosis in females.
In conclusion, our study supports the existence of a sex difference in the age of ASD diagnosis and a tendency toward a distribution of higher severity levels in girls than in boys. The present findings highlight the need for continued research and awareness of the unique presentation of ASD in females.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Balearic Institute for Mental Health in Childhood and Adolescence (IBSMIA, in Spanish) in Ibiza and Formentera. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
AS-P: Conceptualization, Data curation, Investigation, Methodology, Project administration, Writing – review & editing. EA-M: Formal analysis, Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing. MV-P: Supervision, Writing – review & editing. DA-R: Supervision, Writing – review & editing. MV-G: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Grant PID2021-123770OB-I00 funded by MCIN/AEI/10.13039/501100011033 and by “ERDF A way of making Europe” and the Institute of Educational Research and Innovation (IRIE) of the University of the Balearic Islands. The funding sources were not involved in the study design, analysis, and interpretation of data, nor in the writing of the report or submission for publication.
First, we would like to thank all participants of the present study and their families for their valuable time. This research would not have been possible without the interdisciplinary work between the Department of Applied Pedagogy and Educational Psychology and the Institute of Educational Research and Innovation (IRIE) of the University of the Balearic Islands and by the Balearic Institute for Mental Health in Childhood and Adolescence (IBSMIA, in Spanish) in Ibiza and Formentera.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
American Psychiatric Association [APA] (2014). DSM-5. Manual diagnóstico y estadístico de los trastornos Mentales. 5th Edn. Buenos Aires: Panamericana.
Begeer, S., Mandell, D., Wijnker-Holmes, B., Venderbosch, S., Rem, D., Stekelenburg, F., et al. (2013). Sex differences in the timing of identification among children and adults with autism spectrum disorders. J. Autism Dev. Disord. 43, 1151–1156. doi: 10.1007/s10803-012-1656-z
Brickhill, R., Atherton, G., Piovesan, A., and Cross, L. (2023). Autism, thy name is man: exploring implicit and explicit gender bias in autism perceptions. PLoS One 18:e0284013. doi: 10.1371/journal.pone.0284013
Constantino, J. N., and Charman, T. (2012). Gender bias, female resilience, and the sex ratio in autism. J. Am. Acad. Child Adolesc. Psychiatry 51, 756–758. doi: 10.1016/j.jaac.2012.05.017
Duvekot, J., van der Ende, J., Verhulst, F. C., Slappendel, G., van Daalen, E., Maras, A., et al. (2017). Factors influencing the probability of a diagnosis of autism spectrum disorder in girls versus boys. Autism 21, 646–658. doi: 10.1177/1362361316672178
Dworzynski, K., Ronald, A., Bolton, P., and Happé, F. (2012). How different are girls and boys above and below the diagnostic threshold for autism spectrum disorders? J. Am. Acad. Child Adolesc. Psychiatry 51, 788–797. doi: 10.1016/j.jaac.2012.05.018
Gesi, C., Migliarese, G., Torriero, S., Capellazzi, M., Omboni, A. C., Cerveri, G., et al. (2021). Gender differences in misdiagnosis and delayed diagnosis among adults with autism Spectrum disorder with no language or intellectual disability. Brain Sci. 11:912. doi: 10.3390/brainsci11070912
Giarelli, E., Wiggins, L. D., Rice, C. E., Levy, S. E., Kirby, R. S., Pinto-Martin, J., et al. (2010). Sex differences in the evaluation and diagnosis of autism spectrum disorders among children. Disabil. Health J. 3, 107–116. doi: 10.1016/j.dhjo.2009.07.001
Gotham, K., Pickles, A., and Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. J. Autism Dev. Disord. 39, 693–705. doi: 10.1007/s10803-008-0674-3
Hernández, J. M., Artigas Pallarés, J., Martos Pérez, J., Palacios Antón, S., Fuentes Biggi, J., Belinchón Carmona, M., et al. (2005). Guía de buena práctica para la detección temprana de los trastornos del espectro autista (I). Rev. Neurol. 41:237. doi: 10.33588/rn.4104.2005056
Hiller, R. M., Young, R. L., and Weber, N. (2014). Sex differences in autism Spectrum disorder based on DSM-5 criteria: evidence from clinician and teacher reporting. J. Abnorm. Child Psychol. 42, 1381–1393. doi: 10.1007/s10802-014-9881-x
Hull, L., Petrides, K. V., Allison, C., Smith, P., Baron-Cohen, S., Lai, M.-C., et al. (2017). “Putting on my best Normal”: social camouflaging in adults with autism Spectrum conditions. J. Autism Dev. Disord. 47, 2519–2534. doi: 10.1007/s10803-017-3166-5
Kopp, S., and Gillberg, C. (2011). The autism Spectrum screening questionnaire (ASSQ)-revised extended version (ASSQ-REV): an instrument for better capturing the autism phenotype in girls? A preliminary study involving 191 clinical cases and community controls. Res. Dev. Disabil. 32, 2875–2888. doi: 10.1016/J.RIDD.2011.05.017
Lai, M.-C., Lombardo, M. V., Auyeung, B., Chakrabarti, B., and Baron-Cohen, S. (2015). Sex/gender differences and autism: setting the scene for future research. J. Am. Acad. Child Adolesc. Psychiatry 54, 11–24. doi: 10.1016/j.jaac.2014.10.003
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., and Bishop, S. L. (2015). “Autism diagnostic observation schedule (ADOS-2)”. T. Luque. 2nd ed (Madrid: TEA Ediciones).
Maenner, M. J., Warren, Z., Williams, A. R., Amoakohene, E., Bakian, A. V., Bilder, D. A., et al. (2023). Prevalence and characteristics of autism Spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2020. MMWR Surveill. Summ. 72, 1–14. doi: 10.15585/mmwr.ss7202a1
Mandy, W., Chilvers, R., Chowdhury, U., Salter, G., Seigal, A., and Skuse, D. (2012). Sex differences in autism Spectrum disorder: evidence from a large sample of children and adolescents. J. Autism Dev. Disord. 42, 1304–1313. doi: 10.1007/s10803-011-1356-0
Montagut, M., Mas, R. M., Fernández, M. I., and Pastor, G. (2018). Influencia del sesgo de género en el diagnóstico de trastorno de espectro autista: una revisión. Escritos Psicol. 11, 42–54. doi: 10.5231/psy.writ.2018.2804
Morales-Hidalgo, P., Roigé-Castellví, J., Hernández-Martínez, C., Voltas, N., and Canals, J. (2018). Prevalence and characteristics of autism Spectrum disorder among Spanish school-age children. J. Autism Dev. Disord. 48, 3176–3190. doi: 10.1007/s10803-018-3581-2
Nevison, C., and Zahorodny, W. (2019). Race/ethnicity-resolved time trends in United States ASD prevalence Estimates from IDEA and ADDM. J. Autism Dev. Disord. 49, 4721–4730. doi: 10.1007/s10803-019-04188-6
Robins, D. L., Fein, D., and Barton, M. L. (2009). The modified checklist for autism in toddlers, revised with follow-up (M-CHAT-R/F). Storrs, CT: Self-Published.
Rutherford, M., McKenzie, K., Johnson, T., Catchpole, C., O’Hare, A., McClure, I., et al. (2016). Gender ratio in a clinical population sample, age of diagnosis and duration of assessment in children and adults with autism spectrum disorder. Autism 20, 628–634. doi: 10.1177/1362361315617879
Rutter, M., Bailey, A., and Lord, C. (2003). Social communication questionnaire (SCQ). Storrs, CT: Western Psychological Services.
Tofani, M., Scarcella, L., Galeoto, G., Giovannone, F., and Sogos, C. (2023). Behavioral gender differences across pre-school children with autism Spectrum disorders: a cross-sectional study. J. Autism Dev. Disord. 53, 3301–3306. doi: 10.1007/s10803-022-05498-y
Van Wijngaarden-Cremers, P. J. M., van Eeten, E., Groen, W. B., Van Deurzen, P. A., Oosterling, I. J., and Van der Gaag, R. J. (2014). Gender and age differences in the Core triad of impairments in autism Spectrum disorders: a systematic review and Meta-analysis. J. Autism Dev. Disord. 44, 627–635. doi: 10.1007/s10803-013-1913-9
Werling, D. M., and Geschwind, D. H. (2013). Sex differences in autism spectrum disorders. Curr. Opin. Neurol. 26, 146–153. doi: 10.1097/WCO.0b013e32835ee548
Wood-Downie, H., Wong, B., Kovshoff, H., Mandy, W., Hull, L., and Hadwin, J. A. (2021). Sex/gender differences in camouflaging in children and adolescents with autism. J. Autism Dev. Disord. 51, 1353–1364. doi: 10.1007/s10803-020-04615-z
World Health Organization (2019). International statistical classification of diseases and related health problems. 11th Edn. (Geneva, Switzerland: World Health Organization).
Zander, E., Willfors, C., Berggren, S., Choque-Olsson, N., Coco, C., Elmund, A., et al. (2016). The objectivity of the autism diagnostic observation schedule (ADOS) in naturalistic clinical settings. Eur. Child Adolesc. Psychiatry 25, 769–780. doi: 10.1007/s00787-015-0793-2
Keywords: ASD, female gender, diagnosis, severity index, child and adolescent, sex differences
Citation: Sánchez-Pedroche A, Aguilar-Mediavilla E, Valera-Pozo M, Adrover-Roig D and Valverde-Gómez M (2025) A preliminary study on the relationship between symptom severity and age of diagnosis in females versus males with autistic spectrum disorder. Front. Psychol. 16:1472646. doi: 10.3389/fpsyg.2025.1472646
Edited by:
Sabri Hergüner, Ankara Autism Center, TürkiyeReviewed by:
Amy Keefer, Kennedy Krieger Institute, United StatesCopyright © 2025 Sánchez-Pedroche, Aguilar-Mediavilla, Valera-Pozo, Adrover-Roig and Valverde-Gómez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto Sánchez-Pedroche, YWxiZXJ0by5zYW5jaGV6QHVpYi5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.