 Lars König
Lars König Rebekka Schröder
Rebekka Schröder Tim Hamer1
Tim Hamer1- 1Stiftung Gesundheitswissen, Berlin, Germany
- 2Institut für Medizinische Soziologie und Rehabilitationswissenschaft, Charité – Universitätsmedizin Berlin, Berlin, Germany
Introduction: Eating disorders are associated with substantial burden for the affected individuals including negative health outcomes and increased mortality. So far, prevention programs for eating disorders have yielded mixed results concerning their efficacy. Therefore, more targeted prevention programs need to be developed. Health literacy has been identified as a potential influencing factor of eating disorders. This study aimed at exploring the relationship between likely cases of eating disorders and health literacy, alongside additional sociodemographic factors.
Materials and methods: Two large samples of adults (N = 3,011) and adolescents (N = 1,021) representative of the German-speaking population in Germany were recruited. Likely cases of eating disorders were identified using the SCOFF questionnaire. Health literacy was assessed with the HLS-EU-Q16 questionnaire. Sociodemographic information, including age, gender, social status and level of education, and subjective body image were obtained. χ2-tests of independence were calculated to determine the association between the investigated constructs.
Results: Suspected eating disorders were more likely in female than male adolescents but were not related to gender in adults. Rates of suspected eating disorders increased with increasing age in adolescents and decreased with increasing age in adults. While levels of education were unrelated to suspected eating disorders, low social status was associated with higher rates of suspected eating disorders in adults but not adolescents. Inadequate or problematic health literacy and negative body image were associated with higher rates of suspected eating disorders compared to adequate health literacy and more positive body image.
Discussion: Likely cases of eating disorders are related to health literacy and body image as well as sociodemographic factors. These constructs should therefore be addressed in future research to improve prevention programs.
1 Introduction
Eating disorders, such as anorexia nervosa, bulimia nervosa and binge-eating disorder, are severe psychiatric disorders associated with significant psychological and physical impairment (Treasure et al., 2020; World Health Organization, 2019). Eating disorders are characterized by abnormal eating or weight-control behaviors often accompanied by disturbed body image (Treasure et al., 2020). Patients with anorexia nervosa show a persistent pattern of restrictive eating or other behaviors that are aimed at establishing or maintaining abnormally low body weight (World Health Organization, 2019). Both bulimia nervosa and binge-eating disorder are characterized by recurrent binge-eating episodes, in which individuals experience loss of control over their eating behavior and consume large portions of food in a discrete period of time (Treasure et al., 2020; Giel et al., 2022; World Health Organization, 2019). For patients with bulimia nervosa, these episodes are accompanied by compensatory behaviors such as self-induced vomiting to prevent weight gain (Treasure et al., 2020), which do not regularly occur in binge-eating disorder (Giel et al., 2022).
On a global level, 12-months prevalences of all eating disorders are estimated at 2.2% for women and 0.7% for men (Galmiche et al., 2019). For a majority of patients with eating disorders, age of eating disorder onset is before 25 years with a peak age of 15 years (Preti et al., 2009; Solmi et al., 2022). Results concerning a potential increase in eating disorder prevalences in recent years are heterogeneous (Keski-Rahkonen and Mustelin, 2016; Steinhausen and Jensen, 2015). However, a rise in hospital admissions in patients with eating disorders, especially in anorexia nervosa, has been observed, which was further accelerated during the COVID-19 pandemic in recent years (Devoe et al., 2023; Holland et al., 2016).
Although eating disorder prevalences are still relatively low compared to other psychiatric conditions, eating disorders have serious implications, both at an individual and societal level (Chan et al., 2023; Chesney et al., 2014; GBD 2019 Mental Disorders Collaborators, 2022; Ágh et al., 2016). Specifically, eating disorders are associated with high rates of psychiatric comorbidities such as mood and anxiety disorders, physical conditions including cardiovascular and metabolic problems due to malnutrition, weight loss and compensatory behaviors as well as decreased quality of life (Keski-Rahkonen and Mustelin, 2016; Preti et al., 2009; Treasure et al., 2020; Westmoreland et al., 2016; Ágh et al., 2016). When compared to other mental disorders, eating disorders—after substance-abuse disorders—have the second highest number of years-of-potential-life-lost (Chan et al., 2023). Furthermore, eating disorders, particularly anorexia nervosa, are among the psychiatric disorders with the highest mortality rates (Harris and Barraclough, 1998; Arcelus et al., 2011), as evidenced by standardized mortality ratios five to six times that of the general population (Arcelus et al., 2011). Also, while many patients with eating disorders eventually recover, chronicity of the disorders occurs in almost a quarter of patients (Solmi et al., 2024).
The etiology of eating disorders is still subject of ongoing debate. In addition to biological risk factors (e.g., genetics, microbiome), environmental and psychological risk factors play a crucial role in developing eating disorders. These include sexual and physical abuse, trauma and childhood obesity, higher educational attainment, body image-related factors and use of appearance-focused social media, among others (Barakat et al., 2023; Solmi et al., 2021).
Although there are effective treatments available for all major eating disorders (Herpertz et al., 2018; Monteleone et al., 2022; Murray et al., 2019) not all individuals with eating disorders seek or receive treatment (Hart et al., 2011). Among the common barriers that prevent individuals from getting treatment are stigma and shame about the disorder, denial or failure to recognize the severity of symptoms, and practical barriers such as the cost and accessibility of treatments (Ali et al., 2017).
In a recent meta-analysis of a widely-used screening inventory that is also employed in the present study, 22.4% of children and adolescents (age 7–18 years) were identified as suspected of having an eating disorder, with rates in girls (30.0%) almost double those in boys (17.0%) (López-Gil et al., 2023). Similar or slightly lower rates of potential eating disorders were also found in three German-speaking samples (Herpertz-Dahlmann et al., 2008; Cohrdes et al., 2019; Zeiler et al., 2016). Critically, positive screens for eating disorders in younger age are not only predictive of potential underlying full-blown eating disorders but also of current quality of life (Zeiler et al., 2016), as well as overweight, obesity and depressive symptoms later in life (Herpertz-Dahlmann et al., 2015).
The numerous risk factors for eating disorders (Barakat et al., 2023; Solmi et al., 2021) and the substantial burden of the diseases (Ágh et al., 2016; Keski-Rahkonen and Mustelin, 2016; GBD 2019 Mental Disorders Collaborators, 2022) underline the need of preventive interventions (Herpertz-Dahlmann et al., 2015). Onset of most eating disorders in adolescence and the fact that recovery rates are higher in adolescents than in adults and in patients at earlier vs. later stages of the disorder suggest that targeted interventions for prevention or early detection and intervention in children and adolescents may prove to be particularly valuable (Steinhausen and Jensen, 2015; Ambwani et al., 2020; Preti et al., 2009; Kalindjian et al., 2022).
So far, a number of prevention programs to battle eating disorders have been developed with mixed results concerning their efficacy (Koreshe et al., 2023; Le et al., 2017). However, some interventions (e.g., media literacy interventions for universal prevention) have been identified as promising in terms of symptom reductions (Le et al., 2017) and certain intervention programs (e.g., dissonance-based prevention programs) were found to even prevent future onset of eating disorders (Stice et al., 2021). Therefore, identifying groups that might particularly benefit from prevention programs, is vital to improve the efficacy of these programs (Le et al., 2017). The present study was designed to address this need and to explore potential associations with health literacy.
Health literacy refers to the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health (Nutbeam, 1998). It has been associated with several health-related topics, including disordered eating (Fleary et al., 2018; Campanino et al., 2023; Boberová and Husárová, 2021; Bullivant et al., 2020). For example, it has been shown that individuals with anorexia nervosa and bulimia nervosa had lower levels of subjective health literacy and higher levels of objective health literacy when compared to healthy controls (Campanino et al., 2023). In addition, a negative relationship between health literacy and symptoms of eating disorders was found, particularly in participants who perceived themselves to be overweight (Boberová and Husárová, 2021). Therefore, targeting health literacy in prevention programs could be particularly promising.
The aim of the present investigation was to explore the association between suspected cases of eating disorders and sociodemographic variables, body image and health literacy in two representative samples of German-speaking adolescents (12–17 years) and adults (≥ 16 years) in Germany.
2 Materials and methods
2.1 Ethical considerations
The study was designed to comply with the ethical principles for medical research involving human subjects as set out in the Declaration of Helsinki. A study protocol was submitted to the ethics committee of the Berlin Medical Association. The ethics committee had no ethical or professional objections to the study protocol (reference Eth-64/23). Before the study started, participants gave their informed consent to take part in the study. For participants aged 15 and younger, informed consent was provided by their parents. Participants could withdraw from the study at any time. Participants were not compensated for their participation by the independent non-profit foundation Stiftung Gesundheitswissen. Furthermore, only anonymized data was provided to the Stiftung Gesundheitswissen.
2.2 Survey methodology and data acquisition
For this study, data from two independent samples were collected by two market research institutes.
Data for the adult sample (≥ 16 years) was collected by forsa (Gesellschaft für Sozialforschung und statistische Analysen mbH) in December 2023 using the forsa.omninet online panel. The panel has around 100,000 participants and is representative of the German-speaking population with internet access in Germany. For the present investigation, a representative sample was drawn from the panelists 16 years and older. Data collection was carried out online with computer-assisted web interviews. A total of 3,011 participants provided complete questionnaires. Survey weights were calculated by forsa using an iterative proportional fitting approach according to the following weight variables and combinations: (a) gender × age (in the groups 16–29 years, 30–45 years, 46–64 years, ≥ 65 years) × region (West Germany and Berlin, East Germany) and (b) federal state. The weighting was based on the population census of the German Federal Statistical Office.
Data for the adolescent sample was collected by GIM (Gesellschaft für innovative Marktforschung mBH). The study population consisted of pupils aged 12 to 17 from Germany. Data collection was carried out with a mixed-mode approach (similar to representative German JIM-Studie 2023) using computer-assisted web interviews (about 2/3 of all interviews) and computer-assisted face-to-face interviews (about 1/3 of all interviews). A total of 1,021 complete questionnaires were obtained. Data collection was carried out in November and December 2023. Survey weights were calculated in an iterative procedure according to the following weight variables and combinations: age × gender, education and federal state. The weighting was based on data from the Federal Statistical Office and the ma Radio survey.
2.3 Measures
2.3.1 Sociodemographic information
Participants provided basic sociodemographic information including gender (male, female, diverse [in adolescents only]), age and federal state of residence (in the adult sample) or federal state of the currently attended schools (in the adolescent sample). For further analyses, individuals were divided into groups, according to age (16–29 years, 30–45 years, 46–64 years, ≥ 65 years, in the adult sample; 12–13 years, 14–15 years, 16–17 years, in the adolescent sample) and gender (male, female, diverse [in adolescents only]).
In addition, information on (subjective) social status and educational levels were obtained.
Adults were asked to indicate their highest level of formal education. Participants were then categorized into three groups, i.e., low (equivalent to no formal education or basic secondary school; ohne Haupt-/Volksschulabschluss, Haupt-/Volksschulabschluss), middle (equivalent to intermediate secondary school; Mittlere Reife, Realschulabschluss, Fachschulreife, Abschluss der Polytechnischen Oberschule, Fachhochschulreife, Abschluss einer Fachoberschule) and high formal level of education (equivalent to most advanced secondary school, e.g., grammar schools to obtain a general or specialized university entrance qualification, or university degree; Abitur, allgemeine oder fachgebundene Hochschulreife, Fach-/Hochschulstudium). To obtain level of education from adolescents, they were first asked to indicate the type of school they currently attend and then divided into two categories: high (equivalent to most advanced secondary school, e.g., grammar schools, where a general university entrance qualification can be obtained; Gymnasium) and low educational levels (all other school types).
Subjective social status of the adult participants was assessed using the German version of the MacArthur scale (Hoebel et al., 2015; Adler et al., 2000). The scale makes use of a ladder metaphor in which the top rung (rung 10) represents the individuals with highest status and the bottom rung (rung 1) represents the individuals with lowest status. The participants are asked to indicate on which of the 10 possible rungs they place themselves. Three categories of subjective social status were determined according to the respondents’ answers, i.e., low subjective social status (scores 1–4), middle subjective social status (scores 5–7) and high subjective social status (scores 8–10).
Social status in the adolescent sample was obtained using the German version of the Revised Family Affluence Scale (FAS III) (Torsheim et al., 2016). The scale consists of six items asking the participants about their family’s material assets, e.g., if they own a dishwasher or how often they have been on a holiday abroad in the past year. A total score is obtained by adding up answers across items. Cut-offs to determine categories were defined according to quintiles. Three categories were distinguished, e.g., low (bottom 20%, scores 0–5), middle (middle 60%, scores 6–9), and high (top 20%, scores 10–14) social status (Moor et al., 2024; Corell et al., 2021).
2.3.2 SCOFF
The Sick, Control, One Stone, Fat, Food (SCOFF) questionnaire is a questionnaire initially developed to screen for anorexia nervosa and bulimia nervosa (Morgan et al., 1999). Here, the German translation was used (Hölling and Schlack, 2007). The questionnaire consists of five items conveyed as questions, each addressing one the core features of anorexia nervosa and bulimia nervosa, e.g., concerning recent weight loss and loss of control when eating. Participants are asked to answer each question with “yes” or “no” and a sum score is calculated across all items. If two or more questions are answered with “yes,” participants are considered likely to have an eating disorder. Across validation studies, the SCOFF questionnaire has yielded high sensitivity and specificity (Kutz et al., 2020; Botella et al., 2013). In addition, moderate to high test–retest reliability coefficients were obtained (Garcia et al., 2011; Garcia-Campayo et al., 2005; Leung et al., 2009).
2.3.3 Body image
To assess the participants’ subjective body image, they were asked to indicate if they considered themselves to be exactly the right weight, a bit too thin, far too thin, a bit too fat or far too fat (Cohrdes et al., 2019). Three groups were determined: (1) individuals who consider themselves to have the right weight, (2) individuals who consider themselves to be a bit too thin or fat and (3) individuals who consider themselves to be far too thin or fat.
2.3.4 HLS-EU-Q16
Health literacy was assessed using the German translation of the short version of the European Health Literacy Survey instrument (HLS-EU-Q16) (Jordan and Hoebel, 2015; Pelikan et al., 2014; Sørensen et al., 2013). The questionnaire consists of 16 items, answered on a 4-point Likert scale ranging from “very easy,” over “fairly easy,” “fairly difficult” to “very difficult.” Questions address subjective difficulty in accessing, understanding, appraising and applying information concerning healthcare, disease prevention and health promotion (Sørensen et al., 2013). To calculate an overall sum score, item responses were first dichotomized (e.g., 1 = “fairly easy” and “very easy,” 0 = “fairly difficult” and “very difficult”) and then added up across all dichotomized items. Levels of health literacy were determined according to the overall scores, i.e., inadequate or problematic health literacy for scores from 0 to 12 and adequate health literacy for scores from 13 to 16. The HLS-EU-Q16 questionnaire has yielded high internal consistency and test–retest reliability coefficients (Jordan and Hoebel, 2015; Eronen et al., 2019; Bergman et al., 2023).
2.4 Statistical analysis
The statistical analyses were conducted with the statistical software SPSS (version 29.0.2.0, IBM). Individuals with missing data for one construct or questionnaire item were excluded from all analyses concerning these constructs or questionnaires. To analyze whether the proportions of individuals identified as likely having an eating disorder by the SCOFF questionnaire were independent of the categorical sociodemographic and psychological factors studied here (i.e., gender, age, education, social status, body image, health literacy), χ2-tests of independence were calculated. Effect sizes for these tests are reported as Cramer’s V. For χ2-tests of contingency tables larger than 2 × 2, significant results were followed up with post-hoc Bonferroni-adjusted z-tests.
3 Results
3.1 Adults
3.1.1 Sample characteristics adults
The adult sample consisted of N = 3,011 individuals. The sample characteristics. i.e., gender, age, level of education, social status, body image and health literacy categories, before (unweighted) and after (weighted) the weighting procedure can be found in Table 1.

Table 1. Sample characteristics of the weighted and unweighted sample of adults.
3.1.2 Associations with likely eating disorders in adults
In the weighted total samples of adults, 19.6% (N = 590) screened positive on the SCOFF suggesting an increased likelihood of having an eating disorder. 80.2% of participants (N = 2,414) screened negative and 0.2% (N = 7) had missing values in at least one SCOFF item impeding the calculation of the sum score.
An overview of the proportions of positive SCOFF screens for all sociodemographic and psychological categories in the adult sample can be found in Table 2.
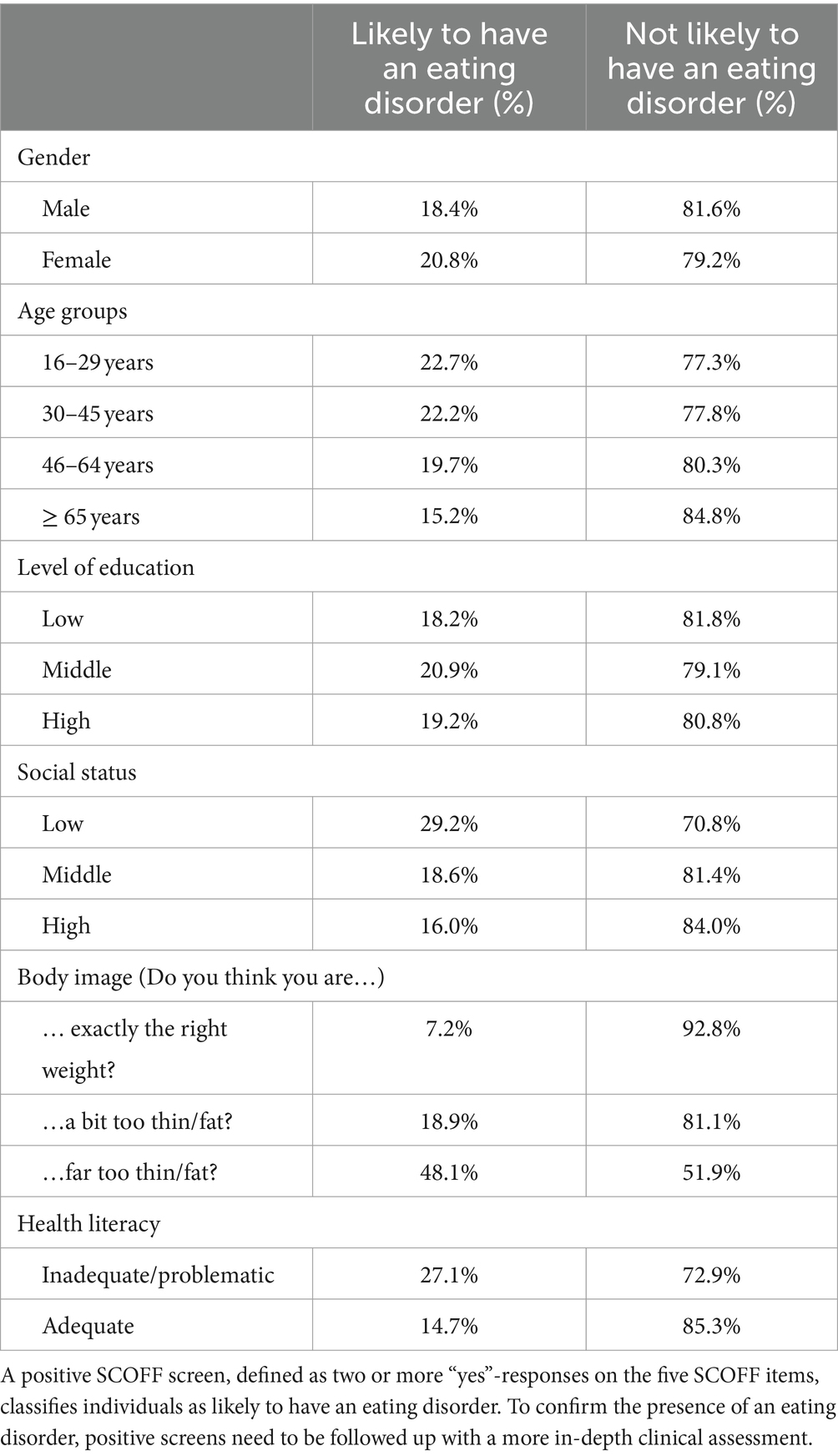
Table 2. Proportions of positive and negative SCOFF screens in the adult sample for the gender, age, level of education, social status, body image and health literacy categories.
At the descriptive level, women were more likely to screen positive for eating disorders (20.8%) than men (18.4%), but this association was not significant, χ2 (1, N = 3,004) = 2.71, p = 0.100, V = 0.03. There was a significant association between age and the SCOFF categories, χ2 (3, N = 3,004) = 15.66, p = 0.001, V = 0.07. Descriptively, the proportions of positive SCOFF screenings decreased with increasing age (16–29 years: 22.7%; 30–45 years: 22.2%; 46–64 years: 19.7%; ≥ 65 years: 15.2%). Post-hoc tests revealed that the 16–29 years and 30–45 years groups did not differ significantly from each other and from the 46–64 years group, but from the ≥65 years group. There were no further significant differences between the age groups. The proportion of individuals scoring positive on the SCOFF did not differ by level of education, χ2 (2, N = 3,001) = 2.24, p = 0.327, V = 0.03, with similar rates in low (18.2%), middle (20.9%) and high (19.2%) educational levels. However, there was a significant association between subjective social status and fulfilling the SCOFF screening criterion, χ2 (2, N = 3,001) = 30.58, p < 0.001, V = 0.10. Post-hoc tests revealed that participants with lower subjective social status were more likely to screen positive for eating disorders than participants with middle and high subjective social status (low: 29.2%, middle: 18.6%, high: 16.0%), whereas the middle and high subjective social status groups did not significantly differ from each other.
Body image was significantly associated with fulfilling the SCOFF screening criterion, χ2 (2, N = 3,004) = 303.27, p < 0.001, V = 0.32. Participants who considered themselves to be far too thin or far too fat were more likely to screen positive for eating disorders (48.1%) than those who considered themselves to be a bit too thin or fat (18.9%) and those who believed to have exactly the right weight (7.2%). Post-hoc tests revealed that these differences were significant for all three groups.
There was a significant association between the SCOFF and health literacy categories, χ2 (1, N = 2,983) = 69.26, p < 0.001, V = 0.15, indicating lower proportions of positive SCOFF screenings in individuals with adequate (14.7%) vs. inadequate and problematic health literacy (27.1%).
3.2 Adolescents
3.2.1 Sample characteristics adolescents
The adolescent sample consisted of N = 1,021 individuals. The sample characteristics. i.e., gender, age, level of education, social status, body image and health literacy categories, before (unweighted) and after (weighted) the weighting procedure can be found in Table 3.
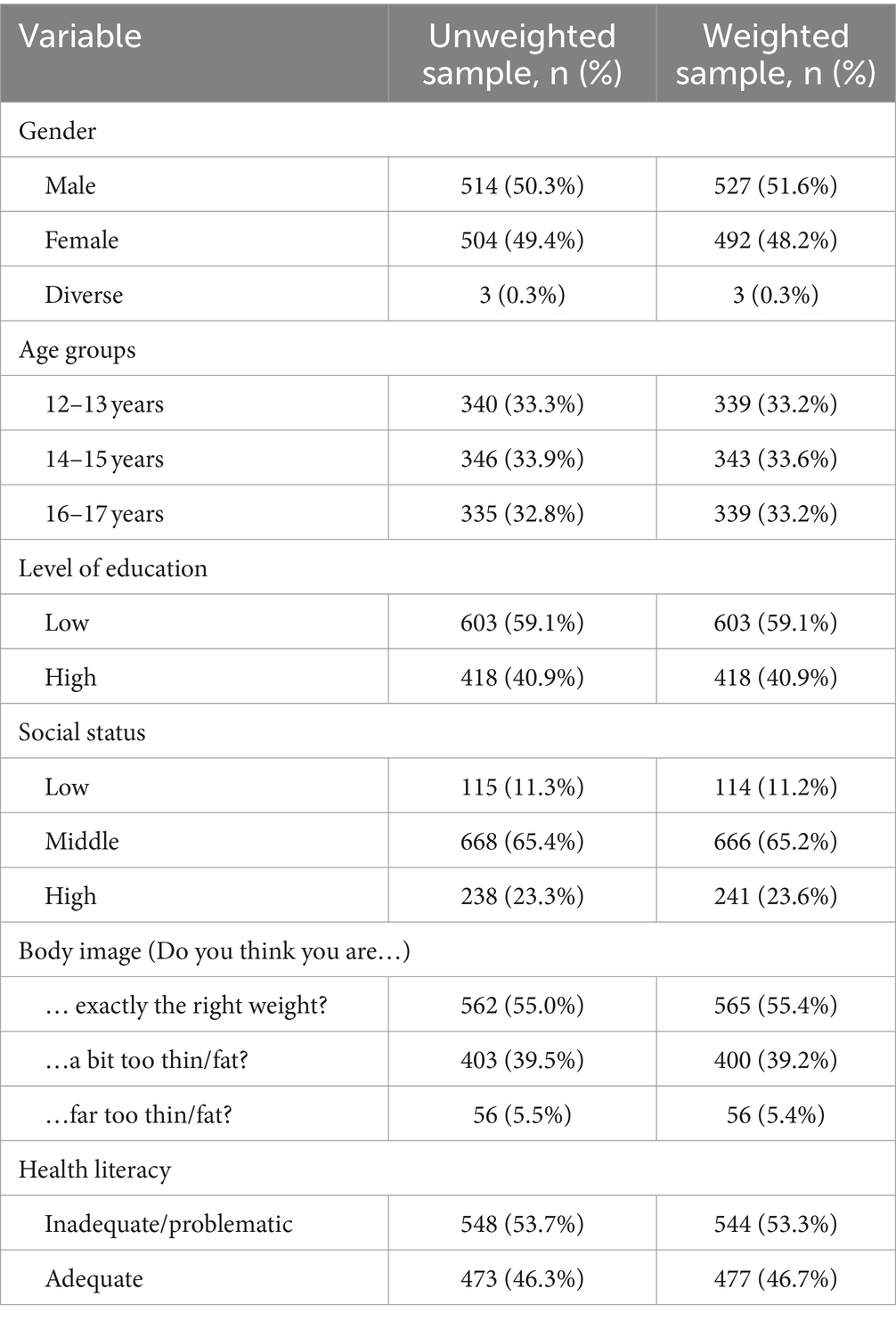
Table 3. Sample characteristics of the weighted and unweighted sample of adolescents.
3.2.2 Associations with likely eating disorders in adolescents
In the weighted total samples of adolescents, 18.9% (N = 193) screened positive on the SCOFF suggesting an increased likelihood of having an eating disorder. 81.1% of participants (N = 828) screened negative. There were no missing values.
An overview of the proportions of positive SCOFF screens for all sociodemographic and psychological categories in the adolescent sample can be found in Table 4.
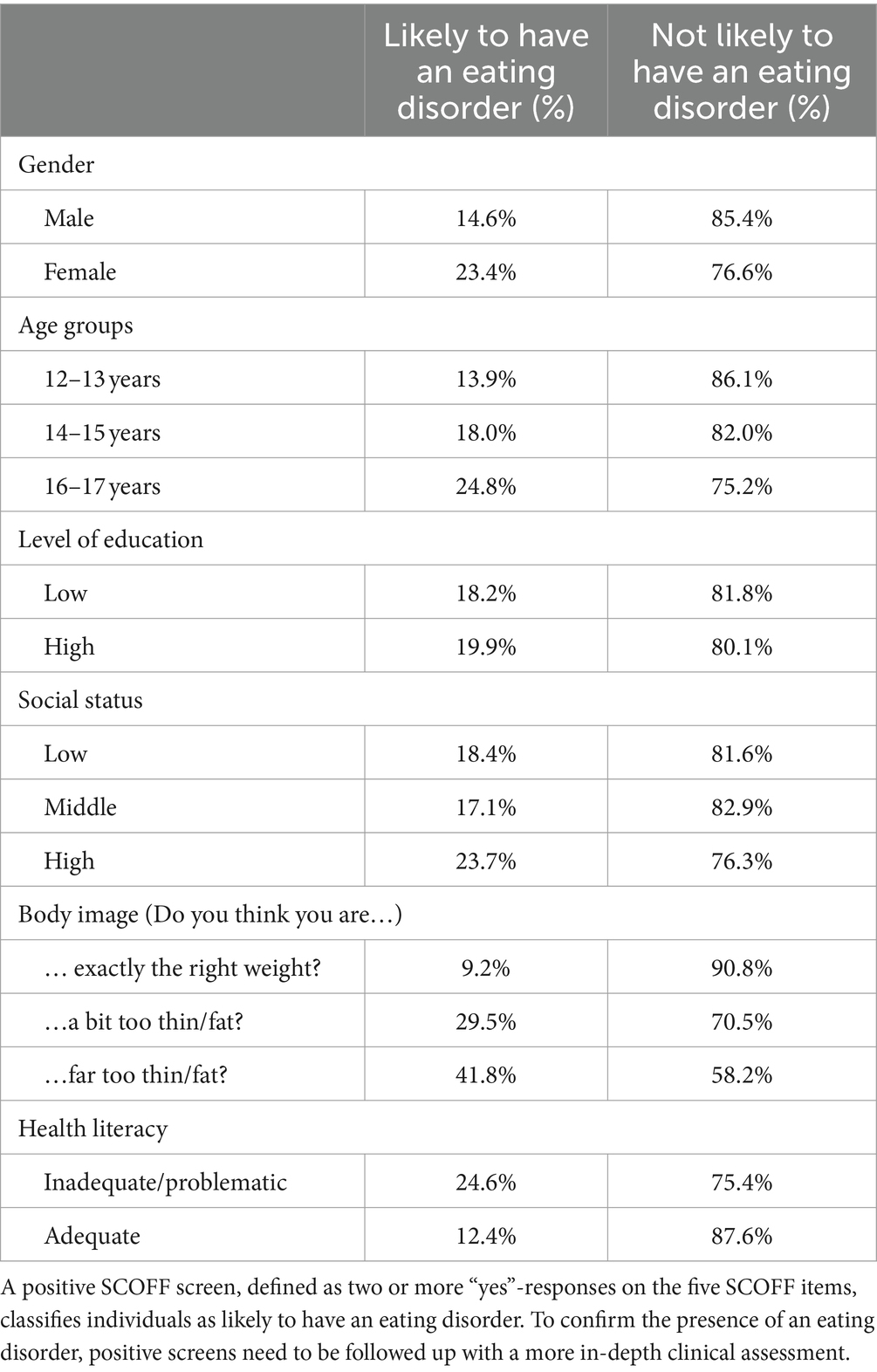
Table 4. Proportions of positive and negative SCOFF screens in the adolescent sample for the gender, age, level of education, social status, body image and health literacy categories.
Girls were significantly more likely to screen positive for eating disorders (23.4%) than boys (14.6%), χ2 (1, N = 1,018) = 12.89, p < 0.001, V = 0.11. There was a significant association between age groups and the SCOFF categories, χ2 (2, N = 1,022) = 13.43, p = 0.001, V = 0.12. Descriptively, the proportions of positive SCOFF screenings increased with increasing age (12–13 years: 13.9%, 14–15 years: 18.0%, 16–17 years: 24.8%). Post-hoc tests revealed significant differences between the youngest and oldest groups, but not differences between the 14–15-year-olds and any other group. The proportion of adolescents scoring positive on the SCOFF did not differ by level of education, χ2 (1, N = 1,021) = 0.42, p = 0.517, V = 0.02, with similar rates in low (18.2%) and high (19.9%) educational levels. There was also no significant association between social status and fulfilling the SCOFF screening criterion, χ2 (2, N = 1,021) = 4.96, p = 0.084, V = 0.07. Descriptively, participants with lower and middle social status were less likely to screen positive for eating disorders than participants with high social status (low: 18.4%, middle: 17.1%, high: 23.7%).
Body image was significantly associated with fulfilling the SCOFF screening criterion, χ2 (2, N = 1,020) = 82.75, p < 0.001, V = 0.29. Participants who considered themselves to be a bit or far too thin or fat were significantly more likely to screen positive for eating disorders (29.5 and 41.8%, respectively) than individuals who believed to have exactly the right weight (9.2%). There was no significant difference between the individuals who considered themselves a bit vs. far too thin or fat.
There was a significant association between SCOFF and health literacy categories, χ2 (1, N = 1,021) = 24.93, p < 0.001, V = 0.16, indicating lower proportions of positive SCOFF screenings in adolescents with adequate (12.4%) vs. inadequate and problematic health literacy (24.6%).
4 Discussion
4.1 Principal findings
The present study investigated the suspected presence of eating disorders in two representative samples of the German-speaking population in Germany and its association with sociodemographic and psychological factors including body image and health literacy.
Overall, 19.6% of adults and 18.9% of adolescents screened positive for eating disorders. For adolescents, these proportions are largely in line with previous investigations in Germany (Herpertz-Dahlmann et al., 2008; Cohrdes et al., 2019). However, for adults, results are substantially higher than in a previous investigation (Richter et al., 2017). This discrepancy might reflect an increase in potential eating disorder prevalences in the last years, previously reported outside Germany (Romano et al., 2022) or it might be due to methodological differences between our own and the previous study (Richter et al., 2017). The same questionnaire might produce different results when used in an online compared to an offline sample, e.g., due to social desirability (Zhang et al., 2017; Richter et al., 2017).
Among adolescents, large and significant gender differences were delineated. Specifically, girls were more likely to screen positive for eating disorders than boys, which is consistent with previous meta-analytic findings from global data (López-Gil et al., 2023). In our sample, rates of positive screenings for eating disorders in boys were slightly lower than in the same meta-analysis (López-Gil et al., 2023) but broadly similar to previous investigations in German-speaking samples (Herpertz-Dahlmann et al., 2008; Cohrdes et al., 2019; Zeiler et al., 2016). In contrast, rates in girls were lower in our sample when compared to the meta-analysis and previous investigations in German-speaking samples (Herpertz-Dahlmann et al., 2008; Cohrdes et al., 2019; Zeiler et al., 2016), which might be cautiously interpreted as an overall negative trend over time, previously only observed in boys (Cohrdes et al., 2019). However, this can only be determined more in depth when screening questionnaires are followed up with detailed diagnostic interviews in positively screened individuals.
Surprisingly, there were no significant gender differences in the adult sample, which contrasts previous findings of increased prevalences of eating disorders in women vs. men (Solmi et al., 2014), but is consistent with previous reports of decreased gender differences in the SCOFF questionnaire with increasing age (Herpertz-Dahlmann et al., 2015; Richter et al., 2017).
In both samples, the likely presence of eating disorders was associated with age. In adolescents, an increase from the younger to the older age groups was observed, as in a previous meta-analysis (López-Gil et al., 2023) and other investigations in German speaking samples (e.g., Herpertz-Dahlmann et al., 2008). In the adult sample, the proportions of positive SCOFF screens decreased with increasing age, also in line with previous research (Solmi et al., 2014). Together, the results point to a peak of suspected eating disorder presence in late adolescence and early adulthood (Herpertz-Dahlmann, 2015). Prevention programs should therefore specifically target this age group.
Levels of education were not significantly associated with positive SCOFF screens in either sample. This finding is consistent with previous research with mixed or null results concerning the association of educational levels and eating disorders (Mitchison and Hay, 2014; Barakat et al., 2023; Solmi et al., 2014).
Social status was significantly associated with positive SCOFF screens only in adults, where higher proportions of suspected eating disorders were found in individuals with low compared to middle and high subjective social status. Descriptively, this pattern of results was reversed in adolescents (i.e., higher proportions with higher social status), but differences did not reach statistical significance. Importantly, social status was assessed differently in both samples, which is why results are not entirely comparable. In adults, social status was assessed with a subjective ranking, which might more closely mirror the perceived social structure of society. Conversely, the approach in adolescents might more specifically represent socioeconomic status as the items refer to material assets in the family. Overall, no clear associations of social status and eating disorders have been identified (Barakat et al., 2023).
As in previous studies (Cohrdes et al., 2019; Štefanová et al., 2020), subjective body image was significantly associated with suspected eating disorders in both groups. Critically, in both samples, proportions of positive eating disorder screens above 40% were found in those who considered themselves far too thin or far too fat. This is particularly worrying since shape or weight concerns are key features of both anorexia nervosa and bulimia nervosa (Treasure et al., 2020). However, no objective measure of weight or body mass index was obtained in this study, which is why subjective body image cannot be put into context of actual overweight or underweight. Cautiously, the results suggest that body image should be regarded as particularly important factors to address in future prevention programs. First approaches focusing on body image have been developed and evaluated but more high-quality research is needed to assess their effectiveness in reducing eating disorder symptoms or prevent onset of eating disorders (Yager and O'Dea, 2008; Le et al., 2017; Koreshe et al., 2023).
To our knowledge, this was the first study to link potential eating disorders with health literacy in large population-representative samples in Germany. In both our samples, higher proportions of suspected eating disorders were found in individuals with problematic or inadequate health literacy than in those with adequate health literacy. This finding is in line with previous research (Campanino et al., 2023; Boberová and Husárová, 2021). Although the cross-sectional design of our study precludes causal interpretation, our results suggest that health literacy may be an important factor to integrate into prevention strategies for eating disorders. First programs to enhance health literacy have been conceptualized and evaluated (Visscher et al., 2018; Walters et al., 2020). However, there is still a need for more targeted interventions, higher quality evaluations and a broader dissemination of positively-evaluated programs (Visscher et al., 2018; Walters et al., 2020).
4.2 Limitations
The results of this study have to be interpreted in the light of several limitations.
First, the cross-sectional design of the study does not allow causal interpretations of the association of the investigated constructs (Wang and Cheng, 2020). This means, for example, that we cannot unequivocally identify low health literacy as a risk factor for eating disorders as the direction of the association might be reversed.
Second, the adult sample is only representative of the German-speaking population with internet access in Germany. This means, that the results cannot be generalized to individuals without internet access or with limited knowledge of the German language.
Third, a recent meta-analysis points to reduced sensitivity of the SCOFF when applied in community samples compared to more homogeneous samples (such as young females) (Kutz et al., 2020), which has also been found in Germany (Richter et al., 2017).
Fourth, the SCOFF was not designed to address other—arguably even more prevalent—eating disorders such as binge eating disorders (Morgan et al., 1999; Kutz et al., 2020). A revision and extension of the questionnaire covering this topic might be necessary in the future.
Fifth, this study focused on potential eating disorders. However, some of the constructs reported here, such as negative body image, might not only be related to eating disorders but also to other psychiatric conditions such as mood disorders that are not the focus of the present work (Paans et al., 2018). Future studies should address potential associations between body image, different psychiatric conditions and eating behaviors, especially due to their high comorbidity (Preti et al., 2009).
Lastly, a further limitation concerning the SCOFF questionnaire is a potential inaccuracy in the German translation, which has been pointed out before (Zeiler et al., 2016) and might inflate the number of positive SCOFF screenings. The English verb “dominates” in item 5 was translated to “beeinflusst sehr” which can be back-translated to “influences a lot.” In our sample, as in other German samples (Zeiler et al., 2016; Herpertz-Dahlmann et al., 2015), the rate of positive responses to this question is higher than in non-German speaking samples (Watson et al., 2015; e.g., Peat et al., 2015). Specifically, in the present study, 40.7% of adults and 26.0% of adolescents gave an affirmative response to this item. However, overall rates of positive SCOFF screenings in our samples are not higher than in a recent meta-analysis (López-Gil et al., 2023). This can be interpreted in two ways: either the inaccurate translation does not negatively impact the diagnostic accuracy of the SCOFF or prevalences of likely eating disorders are in fact lower in Germany but inflated by the disproportionate number of affirmations of item 5. Taken together, we propose a re-evaluation of the German version of the SCOFF to make it more comparable to other language versions.
4.3 Summary and conclusion
This was the first study to comprehensively investigate the associations of the suspected presence of eating disorders, particularly anorexia nervosa and bulimia nervosa, with several sociodemographic variables as well as body image and health literacy in two large and population-representative samples of German-speaking adolescents and adults. Suspected eating disorders were more likely in female than male adolescents but were not related to gender in adults. Highest rates of suspected eating disorders were found in late adolescence and early adulthood. While levels of education were unrelated to suspected eating disorders, low subjective social status was associated with higher rates of suspected eating disorders in adults but not adolescents. Individuals with low levels of health literacy and negative body image had higher levels of suspected eating disorders than individuals with adequate health literacy and more positive body image. The overall high rates of suspected eating disorders in both samples highlight the need for more preventive programs to lower the overall burden of the disorders. These could be targeted particularly at female individuals in late adolescence and early adulthood and should address aspects of body image and health literacy.
Data availability statement
The datasets generated and analyzed during this study are the property of the independent, nonprofit foundation Stiftung Gesundheitswissen and are available on reasonable request. Requests to access the datasets should be directed to bGFycy5rb2VuaWdAc3RpZnR1bmctZ2VzdW5kaGVpdHN3aXNzZW4uZGU=. This study was part of a larger study, and therefore the raw data set contains further variables that have not been described because they exceed the scope of this study.
Ethics statement
A study protocol was submitted to the ethics committee of the Berlin Medical Association. The ethics committee had no ethical or professional objections to the study protocol (reference Eth-64/23). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants and their legal guardians/next of kin if they were younger than 16 years.
Author contributions
LK: Writing – review & editing. RSc: Writing – original draft. TH: Writing – review & editing. RSu: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the independent, nonprofit foundation Stiftung Gesundheitswissen.
Acknowledgments
The authors want to thank the editor and the reviewers for taking the time and effort necessary to review the manuscript. Their insightful comments helped to improve the quality of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adler, N. E. /Epel, E. S., Castellazzo, G., and Ickovics, J. R. (2000). Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol. 19, 586–592. doi: 10.1037/0278-6133.19.6.586
Ágh, T., Kovács, G., Supina, D., Pawaskar, M., Herman, B. K., Vokó, Z., et al. (2016). A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat. Weight Disord. 21, 353–364. doi: 10.1007/s40519-016-0264-x
Ali, K., Farrer, L., Fassnacht, D. B., Gulliver, A., Bauer, S., and Griffiths, K. M. (2017). Perceived barriers and facilitators towards help-seeking for eating disorders: a systematic review. Int. J. Eat. Disord. 50, 9–21. doi: 10.1002/eat.22598
Ambwani, S., Cardi, V., Albano, G., Cao, L., Crosby, R. D., Macdonald, P., et al. (2020). A multicenter audit of outpatient care for adult anorexia nervosa: symptom trajectory, service use, and evidence in support of "early stage" versus "severe and enduring" classification. Int. J. Eat. Disord. 53, 1337–1348. doi: 10.1002/eat.23246
Arcelus, J., Mitchell, A. J., Wales, J., and Nielsen, S. (2011). Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch. Gen. Psychiatry 68, 724–731. doi: 10.1001/archgenpsychiatry.2011.74
Barakat, S., McLean, S. A., Bryant, E., Le, A., Marks, P., Touyz, S., et al. (2023). Risk factors for eating disorders: findings from a rapid review. J. Eat. Disord. 11:8. doi: 10.1186/s40337-022-00717-4
Bergman, L., Nilsson, U., Dahlberg, K., Jaensson, M., and Wångdahl, J. (2023). Validity and reliability of the arabic version of the HLS-EU-Q16 and HLS-EU-Q6 questionnaires. BMC Public Health 23:304. doi: 10.1186/s12889-023-15226-5
Boberová, Z., and Husárová, D. (2021). What role does body image in relationship between level of health literacy and symptoms of eating disorders in adolescents? Int. J. Environ. Res. Public Health 18:3482. doi: 10.3390/ijerph18073482
Botella, J., Sepúlveda, A. R., Huang, H., and Gambara, H. (2013). A meta-analysis of the diagnostic accuracy of the SCOFF. Span. J. Psychol. 16:E92. doi: 10.1017/sjp.2013.92
Bullivant, B., Rhydderch, S., Griffiths, S., Mitchison, D., and Mond, J. M. (2020). Eating disorders "mental health literacy": a scoping review. J Ment Health 29, 336–349. doi: 10.1080/09638237.2020.1713996
Campanino, C., Falone, A., Rossi, E., Angeletti, L. L., Cassioli, E., Gemignani, S., et al. (2023). Health literacy in female patients affected by anorexia nervosa and bulimia nervosa: a cross-sectional study with pair-matched controls. Eat. Weight Disord. 28:59. doi: 10.1007/s40519-023-01588-7
Chan, J. K., Correll, C., Wong, C., Chu, R., Fung, V., Wong, G., et al. (2023). Life expectancy and years of potential life lost in people with mental disorders: a systematic review and meta-analysis. EClinicalMedicine 65:102294. doi: 10.1016/j.eclinm.2023.102294
Chesney, E., Goodwin, G. M., and Fazel, S. (2014). Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry 13, 153–160. doi: 10.1002/wps.20128
Cohrdes, C., Göbel, K., Schlack, R., and Hölling, H. (2019). Essstörungssymptome bei Kindern und Jugendlichen: Häufigkeiten und Risikofaktoren: Ergebnisse aus KiGGS Welle 2 und Trends. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 62, 1195–1204. doi: 10.1007/s00103-019-03005-w
Corell, M., Chen, Y., Friberg, P., Petzold, M., and Löfstedt, P. (2021). Does the family affluence scale reflect actual parental earned income, level of education and occupational status? A validation study using register data in Sweden. BMC Public Health 21:1995. doi: 10.1186/s12889-021-11968-2
Devoe, D. J., Han, A., Anderson, A., Katzman, D. K., Patten, S. B., Soumbasis, A., et al. (2023). The impact of the COVID-19 pandemic on eating disorders: a systematic review. Int. J. Eat. Disord. 56, 5–25. doi: 10.1002/eat.23704
Eronen, J., Paakkari, L., Portegijs, E., Saajanaho, M., and Rantanen, T. (2019). Assessment of health literacy among older Finns. Aging Clin. Exp. Res. 31, 549–556. doi: 10.1007/s40520-018-1104-9
Fleary, S. A., Joseph, P., and Pappagianopoulos, J. E. (2018). Adolescent health literacy and health behaviors: a systematic review. J. Adolesc. 62, 116–127. doi: 10.1016/j.adolescence.2017.11.010
Galmiche, M., Déchelotte, P., Lambert, G., and Tavolacci, M. P. (2019). Prevalence of eating disorders over the 2000-2018 period: a systematic literature review. Am. J. Clin. Nutr. 109, 1402–1413. doi: 10.1093/ajcn/nqy342
Garcia, F. D., Grigioni, S., Allais, E., Houy-Durand, E., Thibaut, F., and Déchelotte, P. (2011). Detection of eating disorders in patients: validity and reliability of the French version of the SCOFF questionnaire. Clin. Nutr. 30, 178–181. doi: 10.1016/j.clnu.2010.09.007
Garcia-Campayo, J., Sanz-Carrillo, C., Ibañez, J. A., Lou, S., Solano, V., and Alda, M. (2005). Validation of the Spanish version of the SCOFF questionnaire for the screening of eating disorders in primary care. J. Psychosom. Res. 59, 51–55. doi: 10.1016/j.jpsychores.2004.06.005
GBD 2019 Mental Disorders Collaborators (2022). Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry 9, 137–150. doi: 10.1016/S2215-0366(21)00395-3
Giel, K. E., Bulik, C. M., Fernandez-Aranda, F., Hay, P., Keski-Rahkonen, A., Schag, K., et al. (2022). Binge eating disorder. Nat. Rev. Dis. Primers 8:16. doi: 10.1038/s41572-022-00344-y
Harris, E. C., and Barraclough, B. (1998). Excess mortality of mental disorder. Br. J. Psychiatry J. Ment. Sci. 173, 11–53. doi: 10.1192/bjp.173.1.11
Hart, L. M., Granillo, M. T., Jorm, A. F., and Paxton, S. J. (2011). Unmet need for treatment in the eating disorders: a systematic review of eating disorder specific treatment seeking among community cases. Clin. Psychol. Rev. 31, 727–735. doi: 10.1016/j.cpr.2011.03.004
Herpertz, S., Fichter, M., Herpertz-Dahlmann, B., Hilbert, A., Tuschen-Caffier, B., Vocks, S., et al. (2018). S3-Leitlinie Diagnostik und Behandlung der Essstörungen. Berlin, Heidelberg.
Herpertz-Dahlmann, B. (2015). Adolescent eating disorders: update on definitions, symptomatology, epidemiology, and comorbidity. Child Adolesc. Psychiatr. Clin. N. Am. 24, 177–196. doi: 10.1016/j.chc.2014.08.003
Herpertz-Dahlmann, B., Dempfle, A., Konrad, K., Klasen, F., and Ravens-Sieberer, U. (2015). Eating disorder symptoms do not just disappear: the implications of adolescent eating-disordered behaviour for body weight and mental health in young adulthood. Eur. Child Adolesc. Psychiatry 24, 675–684. doi: 10.1007/s00787-014-0610-3
Herpertz-Dahlmann, B., Wille, N., Hölling, H., Vloet, T. D., and Ravens-Sieberer, U. (2008). Disordered eating behaviour and attitudes, associated psychopathology and health-related quality of life: results of the BELLA study. Eur. Child Adolesc. Psychiatry 17, 82–91. doi: 10.1007/s00787-008-1009-9
Hoebel, J., Müters, S., Kuntz, B., Lange, C., and Lampert, T. (2015). Messung des subjektiven sozialen Status in der Gesundheitsforschung mit einer deutschen Version der MacArthur Scale. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 58, 749–757. doi: 10.1007/s00103-015-2166-x
Holland, J., Hall, N., Yeates, D. G. R., and Goldacre, M. (2016). Trends in hospital admission rates for anorexia nervosa in Oxford (1968-2011) and England (1990-2011): database studies. J. R. Soc. Med. 109, 59–66. doi: 10.1177/0141076815617651
Hölling, H., and Schlack, R. (2007). Essstörungen im Kindes- und Jugendalter. Erste Ergebnisse aus dem Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 50, 794–799. doi: 10.1007/s00103-007-0242-6
Jordan, S., and Hoebel, J. (2015). Gesundheitskompetenz von Erwachsenen in Deutschland: Ergebnisse der Studie “Gesundheit in Deutschland aktuell” (GEDA). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 58, 942–950. doi: 10.1007/s00103-015-2200-z
Kalindjian, N., Hirot, F., Stona, A.-C., Huas, C., and Godart, N. (2022). Early detection of eating disorders: a scoping review. Eat. Weight Disord. 27, 21–68. doi: 10.1007/s40519-021-01164-x
Keski-Rahkonen, A., and Mustelin, L. (2016). Epidemiology of eating disorders in Europe: prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr. Opin. Psychiatry 29, 340–345. doi: 10.1097/YCO.0000000000000278
Koreshe, E., Paxton, S., Miskovic-Wheatley, J., Bryant, E., Le, A., Maloney, D., et al. (2023). Prevention and early intervention in eating disorders: findings from a rapid review. J. Eat. Disord. 11:38. doi: 10.1186/s40337-023-00758-3
Kutz, A. M., Marsh, A. G., Gunderson, C. G., Maguen, S., and Masheb, R. M. (2020). Eating disorder screening: a systematic review and Meta-analysis of diagnostic test characteristics of the SCOFF. J. Gen. Intern. Med. 35, 885–893. doi: 10.1007/s11606-019-05478-6
Le, L. K.-D., Barendregt, J. J., Hay, P., and Mihalopoulos, C. (2017). Prevention of eating disorders: a systematic review and meta-analysis. Clin. Psychol. Rev. 53, 46–58. doi: 10.1016/j.cpr.2017.02.001
Leung, S. F., Lee, K. L., Lee, S. M., Leung, S. C., Hung, W. S., Lee, W. L., et al. (2009). Psychometric properties of the SCOFF questionnaire (Chinese version) for screening eating disorders in Hong Kong secondary school students: a cross-sectional study. Int. J. Nurs. Stud. 46, 239–247. doi: 10.1016/j.ijnurstu.2008.09.004
López-Gil, J. F., García-Hermoso, A., Smith, L., Firth, J., Trott, M., Mesas, A. E., et al. (2023). Global proportion of disordered eating in children and adolescents: a systematic review and Meta-analysis. JAMA Pediatr. 177, 363–372. doi: 10.1001/jamapediatrics.2022.5848
Mitchison, D., and Hay, P. J. (2014). The epidemiology of eating disorders: genetic, environmental, and societal factors. Clin. Epidemiol. 6, 89–97. doi: 10.2147/CLEP.S40841
Monteleone, A. M., Pellegrino, F., Croatto, G., Carfagno, M., Hilbert, A., Treasure, J., et al. (2022). Treatment of eating disorders: a systematic meta-review of meta-analyses and network meta-analyses. Neurosci. Biobehav. Rev. 142:104857. doi: 10.1016/j.neubiorev.2022.104857
Moor, I., Herke, M., Markert, J., Böhm, M., Reiß, F., Bilz, L., et al. (2024). Trends in health inequalities in childhood and adolescence in Germany: results of the HBSC study 2009, 10 - 2022. J. Health Monit. 9, 79–98. doi: 10.25646/11876
Morgan, J. F., Reid, F., and Lacey, J. H. (1999). The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ 319, 1467–1468. doi: 10.1136/bmj.319.7223.1467
Murray, S. B., Quintana, D. S., Loeb, K. L., Griffiths, S., and Le Grange, D. (2019). Treatment outcomes for anorexia nervosa: a systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 49, 535–544. doi: 10.1017/S0033291718002088
Nutbeam, D. (1998). Health promotion glossary. Health Promot. Int. 13, 349–364. doi: 10.1093/heapro/13.4.349
Paans, N. P. G., Bot, M., Brouwer, I. A., Visser, M., and Penninx, B. W. J. H. (2018). Contributions of depression and body mass index to body image. J. Psychiatr. Res. 103, 18–25. doi: 10.1016/j.jpsychires.2018.05.003
Peat, C. M., Von Holle, A., Watson, H., Huang, L., Thornton, L. M., Zhang, B., et al. (2015). The association between internet and television access and disordered eating in a Chinese sample. Int. J. Eat. Disord. 48, 663–669. doi: 10.1002/eat.22359
Pelikan, J. M., Röthlin, F., and Ganahl, K. (2014). Measuring comprehensive health literacy in general populations: Validation of instrument, indices and scales of the HLS-EU study : Bethesda, MD Available at: https://www.bumc.bu.edu/healthliteracyconference/files/2014/06/pelikan-et-al-harc-2014-fin.pdf.
Preti, A., De Girolamo, G., Vilagut, G., Alonso, J., De Graaf, R., Bruffaerts, R., et al. (2009). The epidemiology of eating disorders in six European countries: results of the ESEMeD-WMH project. J. Psychiatr. Res. 43, 1125–1132. doi: 10.1016/j.jpsychires.2009.04.003
Richter, F., Strauss, B., Braehler, E., Adametz, L., and Berger, U. (2017). Screening disordered eating in a representative sample of the German population: usefulness and psychometric properties of the German SCOFF questionnaire. Eat. Behav. 25, 81–88. doi: 10.1016/j.eatbeh.2016.06.022
Romano, K. A., Lipson, S. K., Beccia, A. L., Quatromoni, P. A., Gordon, A. R., and Murgueitio, J. (2022). Changes in the prevalence and sociodemographic correlates of eating disorder symptoms from 2013 to 2020 among a large national sample of U.S. young adults: a repeated cross-sectional study. Int. J. Eat. Disord. 55, 776–789. doi: 10.1002/eat.23709
Solmi, F., Hatch, S. L., Hotopf, M., Treasure, J., and Micali, N. (2014). Prevalence and correlates of disordered eating in a general population sample: the South East London community health (SELCoH) study. Soc. Psychiatry Psychiatr. Epidemiol. 49, 1335–1346. doi: 10.1007/s00127-014-0822-3
Solmi, M., Monaco, F., Højlund, M., Monteleone, A. M., Trott, M., Firth, J., et al. (2024). Outcomes in people with eating disorders: a transdiagnostic and disorder-specific systematic review, meta-analysis and multivariable meta-regression analysis. World Psychiatry 23, 124–138. doi: 10.1002/wps.21182
Solmi, M., Radua, J., Olivola, M., Croce, E., Soardo, L., de Pablo, S., et al. (2022). Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 27, 281–295. doi: 10.1038/s41380-021-01161-7
Solmi, M., Radua, J., Stubbs, B., Ricca, V., Moretti, D., Busatta, D., et al. (2021). Risk factors for eating disorders: an umbrella review of published meta-analyses. Braz. J. Psychiatry 43, 314–323. doi: 10.1590/1516-4446-2020-1099
Sørensen, K., van den Broucke, S., Pelikan, J. M., Fullam, J., Doyle, G., Slonska, Z., et al. (2013). Measuring health literacy in populations: illuminating the design and development process of the European health literacy survey questionnaire (HLS-EU-Q). BMC Public Health 13:948. doi: 10.1186/1471-2458-13-948
Štefanová, E., Bakalár, P., and Baška, T. (2020). Eating-disordered behavior in adolescents: associations with body image, body composition and physical activity. Int. J. Environ. Res. Public Health 17:6665. doi: 10.3390/ijerph17186665
Steinhausen, H.-C., and Jensen, C. M. (2015). Time trends in lifetime incidence rates of first-time diagnosed anorexia nervosa and bulimia nervosa across 16 years in a Danish nationwide psychiatric registry study. Int. J. Eat. Disord. 48, 845–850. doi: 10.1002/eat.22402
Stice, E., Onipede, Z. A., and Marti, C. N. (2021). A meta-analytic review of trials that tested whether eating disorder prevention programs prevent eating disorder onset. Clin. Psychol. Rev. 87:102046. doi: 10.1016/j.cpr.2021.102046
Torsheim, T., Cavallo, F., Levin, K. A., Schnohr, C., Mazur, J., Niclasen, B., et al. (2016). Psychometric validation of the revised family affluence scale: a latent variable approach. Child Indic. Res. 9, 771–784. doi: 10.1007/s12187-015-9339-x
Treasure, J., Duarte, T. A., and Schmidt, U. (2020). Eating disorders. Lancet 395, 899–911. doi: 10.1016/S0140-6736(20)30059-3
Visscher, B. B., Steunenberg, B., Heijmans, M., Hofstede, J. M., Devillé, W., van der Heide, I., et al. (2018). Evidence on the effectiveness of health literacy interventions in the EU: a systematic review. BMC Public Health 18:1414. doi: 10.1186/s12889-018-6331-7
Walters, R., Leslie, S. J., Polson, R., Cusack, T., and Gorely, T. (2020). Establishing the efficacy of interventions to improve health literacy and health behaviours: a systematic review. BMC Public Health 20:1040. doi: 10.1186/s12889-020-08991-0
Wang, X., and Cheng, Z. (2020). Cross-sectional studies: strengths, weaknesses, and recommendations. Chest 158, S65–S71. doi: 10.1016/j.chest.2020.03.012
Watson, H. J., Hamer, R. M., Thornton, L. M., Peat, C. M., Kleiman, S. C., Du, S., et al. (2015). Prevalence of screening-detected eating disorders in chinese females and exploratory associations with dietary practices. Eur. Eat. Disord. Rev. 23, 68–76. doi: 10.1002/erv.2334
Westmoreland, P., Krantz, M. J., and Mehler, P. S. (2016). Medical complications of anorexia nervosa and bulimia. Am. J. Med. 129, 30–37. doi: 10.1016/j.amjmed.2015.06.031
World Health Organization (2019). International classification of diseases, eleventh revision (ICD-11). The global standard for diagnostic health information. Available at: https://icd.who.int/browse11.
Yager, Z., and O'Dea, J. A. (2008). Prevention programs for body image and eating disorders on university campuses: a review of large, controlled interventions. Health Promot. Int. 23, 173–189. doi: 10.1093/heapro/dan004
Zeiler, M., Waldherr, K., Philipp, J., Nitsch, M., Dür, W., Karwautz, A., et al. (2016). Prevalence of eating disorder risk and associations with health-related quality of life: results from a large school-based population screening. Eur. Eat. Disord. Rev. 24, 9–18. doi: 10.1002/erv.2368
Keywords: eating disorder, health literacy, body image, health, representative, Germany, adolescents, adults
Citation: König L, Schröder R, Hamer T and Suhr R (2024) Eating disorders and health literacy in Germany: results from two representative samples of adolescents and adults. Front. Psychol. 15:1464651. doi: 10.3389/fpsyg.2024.1464651
Edited by:
Sebastian Gustavo Soneira, Fundación Para la Lucha Contra las Enfermedades Neurológicas de la Infancia (FLENI), ArgentinaReviewed by:
Delfina Lahitou Herlyn, National Scientific and Technical Research Council (CONICET), ArgentinaLeticia Fiorentini, Fundación Para la Lucha Contra las Enfermedades Neurológicas de la Infancia (FLENI), Argentina
Copyright © 2024 König, Schröder, Hamer and Suhr. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lars König, bGFycy5rb2VuaWdAc3RpZnR1bmctZ2VzdW5kaGVpdHN3aXNzZW4uZGU=
†These authors have contributed equally to this work and share first authorship