
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychol. , 04 October 2024
Sec. Psychology for Clinical Settings
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1449150
This article is part of the Research Topic Present and Future of EMDR in Clinical Psychology and Psychotherapy – Volume III View all 11 articles
 S. Vock1
S. Vock1 A. Hofmann2
A. Hofmann2 M. Lehnung2,3
M. Lehnung2,3 K. Böhm4
K. Böhm4 S. Wieland1
S. Wieland1 G. H. Seidler5
G. H. Seidler5 E. Beiner1
E. Beiner1 M. Hermes1
M. Hermes1 H.-C. Friederich1,6
H.-C. Friederich1,6 W. Eich1
W. Eich1 J. Tesarz1,6,7*
J. Tesarz1,6,7*Background: Eye Movement Desensitization and Reprocessing (EMDR) is an evidence-based treatment, primarily established for post-traumatic stress disorder (PTSD). While it is increasingly being applied to chronic pain, its efficacy in this area is not yet supported by the same level of evidence as that which exists for PTSD. Studies in this area often show heterogeneous results with small case numbers, and the potential side effects of EMDR in the treatment of chronic pain are not well understood. Systematic documentation of treatment effects, potential predictors of treatment response and non-response, and side effects is crucial for progress in this field.
Aim: The primary aim is to establish a research framework to systematically investigate the delivery of EMDR therapies by outpatient clinicians in the field of pain. This study aims to provide a comprehensive analysis of treatment outcomes, side effects and determinants of treatment effectiveness, whether positive response or non-response.
Methods: This framework will oversee the documentation and evaluation of EMDR interventions delivered in outpatient settings using an Embedded Continuous Cumulative Evaluation Design (ECCED). It will focus on detailed characterisation of positive and negative therapeutic effects. It will also identify and analyse prognostic factors that influence individual variability in response to treatment. Treatment materials, standardised assessments and an intervision platform for regular exchange will be provided.
Discussion: The establishment of the EMDR Pain Network Germany and an interdisciplinary scientific-clinical platform is essential to promote clinical exchange and understanding of the effects of EMDR in pain therapy. This platform offers standardised treatment protocols, an online data collection system with anonymised data, comprehensive baseline assessments and an intervision platform for regular exchange. The knowledge gained is intended to personalise future therapies and serve as a basis for large randomised clinical trials.
Worldwide, pain represents a significant health problem affecting millions of people. Demographic changes and the increasing prevalence of chronic diseases have led to a rise in pain cases, resulting in a growing societal burden (Vos et al., 2020; Wettstein and Tesarz, 2023). It is estimated that more than 20% of adults worldwide suffer from chronic pain, and the number of new people suffering from this condition is increasing every year. This makes chronic pain one of the leading causes of long-term disability worldwide (Gatchel et al., 2007). Despite various effective therapeutic approaches for treating acute pain, therapy for chronic pain often remains insufficient, leading to significant impairments and reduced quality of life for those affected (Vos et al., 2020). The persistence of these pain conditions highlights the limitations of current treatment methods and the need for innovative approaches that address pain as a complex biopsychosocial phenomenon (Pinto et al., 2023).
A promising approach in the treatment of chronic pain is Eye Movement Desensitization and Reprocessing (EMDR), a method originally developed for treating post-traumatic stress disorder (PTSD). In recent years, the scope of EMDR has expanded beyond PTSD therapy, particularly in the treatment of chronic pain syndromes. This expansion is due to the potential of the method to target not only the pain symptoms themselves but also the associated psychological and emotional components such as anxiety, depression, and avoidance behaviour (Gilam et al., 2020; Hashmi et al., 2013; Matthijssen et al., 2020; Pinto et al., 2023).
Several randomised controlled trials have demonstrated the effectiveness of EMDR in various chronic pain syndromes, including musculoskeletal pain (Gerhardt et al., 2016), back pain (Gerhardt et al., 2016), headaches (Konuk et al., 2011), phantom pain (Rostaminejad et al., 2017), fibromyalgia (Borst et al., 2024; Friedberg, 2004; Zat Çiftçi et al., 2024), and rheumatoid arthritis (Matthijssen et al., 2020; Tesarz et al., 2019). The results of these studies indicate that EMDR can significantly reduce pain intensity and lead to a decrease in pain-related impairments and psychological distress (Leisner et al., 2014).
A key aspect that distinguishes EMDR from traditional pain therapeutic approaches is its direct analgesic effect. While conventional approaches often achieve only indirect effects by reducing anxiety and depression, more recent studies suggest that EMDR significantly reduces both pain symptoms and the extent of pain-related impairments. Additionally, the results indicate partially stable long-term effects of up to 2 years after the completion of therapy (Tesarz et al., 2014). These positive effects are attributed to the modulation of neural processes involved in both emotional and pain-related processing.
Research shows that in chronic pain, an “emotional shift” often occurs, where pain is no longer processed in the classical pain-processing regions of the brain but rather in the emotion-processing areas (Hashmi et al., 2013).This mechanism has parallels to the “flashbacks” experienced by trauma patients, making the use of EMDR in chronic pain particularly plausible.
At the same time, studies in this field also show heterogeneous results, often due to small sample sizes and a limited understanding of potential side effects (Matthijssen et al., 2020; Tesarz et al., 2013). These challenges underscore the need for a systematic approach to documenting and analysing treatment outcomes. Establishing regional networks to promote information exchange and systematically analyse the implementation of EMDR therapies in practice could significantly contribute to optimizing the use of EMDR in chronic pain.
The complexity of psychotherapeutic interventions and their outcomes in clinical studies also presents a significant challenge, particularly in terms of the reproducibility and generalisability of results (Lutz, 2003). Conventional randomized controlled trials often do not fully capture the nuances of psychotherapy, leading to a gap between research findings and clinical practice. Close collaboration between researchers and therapists could bridge this gap and ensure that research findings are practical and patient-centred (Asay et al., 2002).Given the time and cost constraints of psychotherapy research, which often lead to studies with small sample sizes (Williams et al., 2012), a collaborative research network promotes a continuous dialogue between researchers and therapists. This could help integrate new insights into clinical practice more quickly and improve the treatment of chronic pain through EMDR.
The ‘EMDR Pain Network Germany’ was founded with the aim of promoting and further developing the quality and scientific evidence of EMDR in pain therapy in accordance with the current state of research and to support the exchange between clinicians and thus promote and scientifically accompany the implementation of EMDR in the therapy of chronic pain. This network is a scientific cooperation project under the direction of the Department of General Internal Medicine and Psychosomatics at Heidelberg University Hospital in collaboration with the professional association EMDRIA Deutschland e.V. and the EMDR Institute Germany. It aims to facilitate (1) longitudinal research into the therapeutic effects of EMDR in the treatment of chronic pain at an individual level, including adverse effects, (2) the identification of potential predictors of individual response/non-response to treatment between participants, and (3) the facilitation and scientific monitoring of the implementation of EMDR in pain therapy.
This research initiative will thoroughly assess the implementation of Eye Movement Desensitization and Reprocessing (EMDR) therapies by outpatient clinicians. We will conduct a detailed follow-up that evaluates treatment results, documents adverse events, and identifies key factors influencing treatment effectiveness, which encompasses both positive responses and non-responses. Furthermore, we will promote the broad implementation and practical use of EMDR in managing pain. The ‘EMDR Pain Network Germany’ provides therapists with the resources they need to deliver effective EMDR treatments. Our standardised protocols, training materials and platform for professional interaction ensure uniformity and excellence in therapeutic practices, improving the effectiveness of EMDR treatments across diverse clinical environments.
In accordance with the ethical principles governing human research, all participants and therapists are required to provide written informed consent prior to enrolment. Ethical approval for data collection was obtained from the Research Ethics Committee II of the Medical Faculty of the University of Heidelberg (approval number S-696/2023), ensuring compliance with the ethical standards of the Declaration of Helsinki.
This study is an accompanying evaluation conducted in conjunction with the establishment and expansion of a national network for EMDR therapy focused on chronic pain management. Utilizing an Embedded Continuous Cumulative Evaluation Design (ECCED), the core scientific objective of this network is to carry out a comprehensive, real-time assessment of EMDR therapy as delivered by independent therapists in private healthcare settings. The ECCED represents an innovative research framework designed to seamlessly integrate evaluation into routine clinical practice. Developed as part of the PerPAIN research network (Beiner et al., 2022), it draws inspiration from existing cumulative assessment models, particularly those used in educational research (Kerdijk et al., 2013). This approach allows for ongoing and cumulative data collection throughout the therapeutic process, without a predetermined endpoint. The ECCED is crafted to ensure minimal disruption to the therapeutic process while facilitating continuous monitoring of both therapeutic outcomes and any adverse events that may occur.
In practice, ECCED embeds evaluation mechanisms directly into the everyday clinical activities, ensuring that data collection is a natural part of the therapy rather than an external add-on. Data is collected continuously, allowing for real-time tracking of patient progress and the identification of trends and patterns over time. This cumulative data collection provides a thorough understanding of treatment efficacy and safety. The design of ECCED emphasizes standardized procedures to maintain consistency and comparability across different settings and patients. Detailed descriptive analysis of therapeutic outcomes and adverse events is a key component, alongside systematic research into prognostic factors that may influence treatment responses. This approach enables the differentiation between positive responses and non-responses to therapy.
To guide future research and enhance comparability, a core assessment framework is proposed (see Table 1). This framework aims to standardize evaluations and facilitate data pooling, ultimately contributing to improved research quality and the optimization of EMDR therapy for chronic pain.
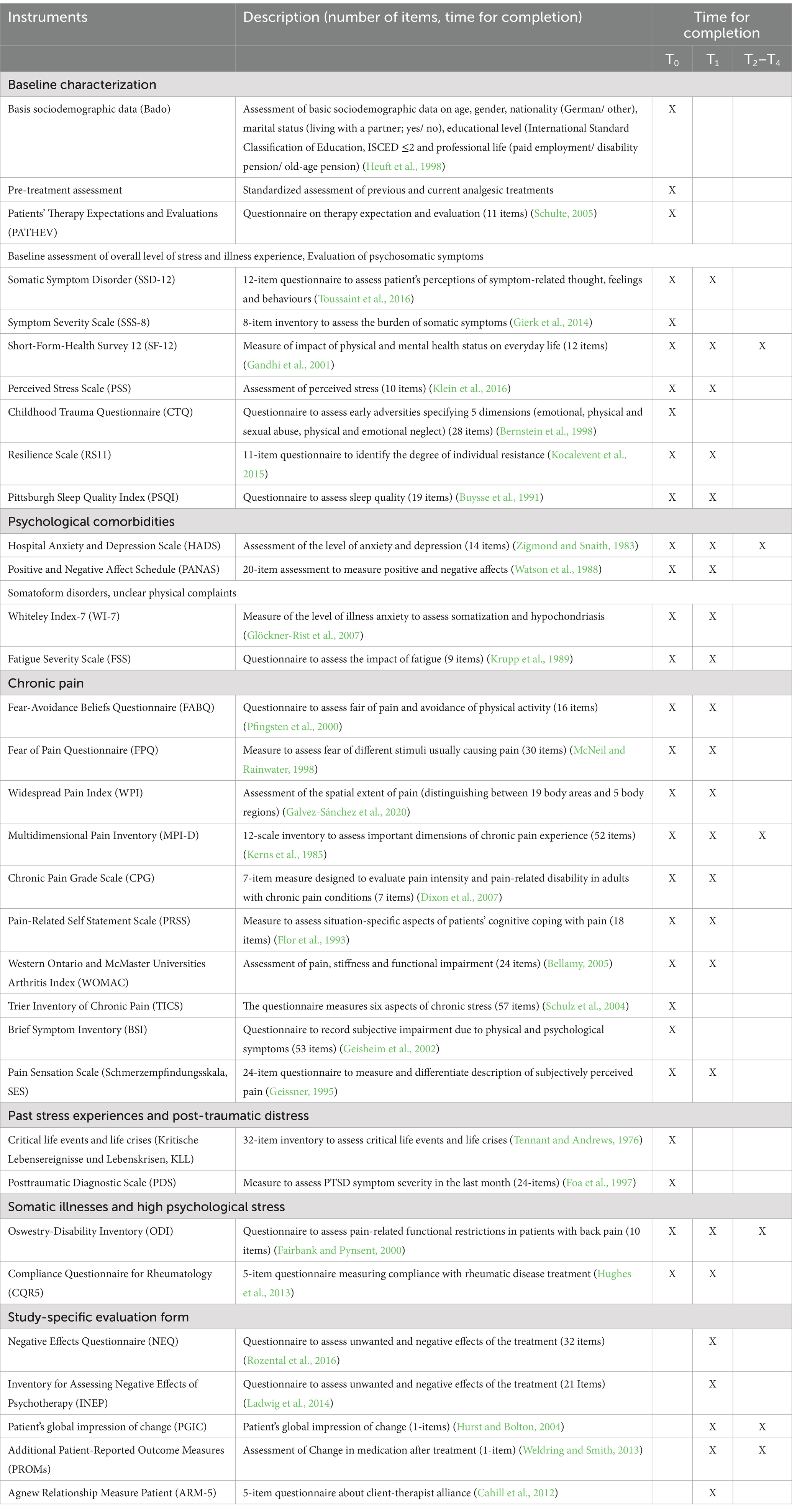
Table 1. Measures applied at different points of data acquisition.
EMDR therapy is a stress-reducing intervention that combines proven trauma intervention elements such as imaginal exposure, cognitive and self-control techniques with specific techniques such as bilateral sensory stimulation (e.g., left–right eye movements or bilateral tapping with the therapist’s hand). This is done according to the principle of dual focus of attention (Schubert et al., 2011). This principle describes how patients simultaneously focus on distressing memories and an external bilateral sensory stimulus (Laliotis et al., 2021). This process appears to facilitate the processing of emotionally distressing memories (e.g., traumatic events or pain sensations) and reduce or even eliminate the emotional distress associated with these memories (Laliotis et al., 2021). During each EMDR session, the patient deals with distressing traumatic or pain-related memories and the associated feelings, cognitions and body sensations while focusing on a series of external bilateral stimuli. In the subsequent phase, the patient’s attention is directed towards the emergence of new associations, which are then subjected to further scrutiny through a series of dual attention exercises. This process of dual attention and personal association is repeated throughout the session until the original target (trauma or pain-related memories) is no longer a significant source of distraction. The duration of a single session typically ranges from 50 to 90 min. All additional treatments are recorded in detail (Table 2, for more details see also Supplementary material). The therapists are afforded considerable flexibility in the organisation of their EMDR sessions, with the respective contents and potential deviations being briefly documented. However, in order to standardise case conceptualisation and treatment implementation, all participating therapists receive a treatment protocol and manual for orientation. The treatment protocol for this study is based on a standardised manual (Tesarz et al., 2015), and the possible goals for treatment include disturbing memories, current pain perceptions and pain-related fears and cognitions.
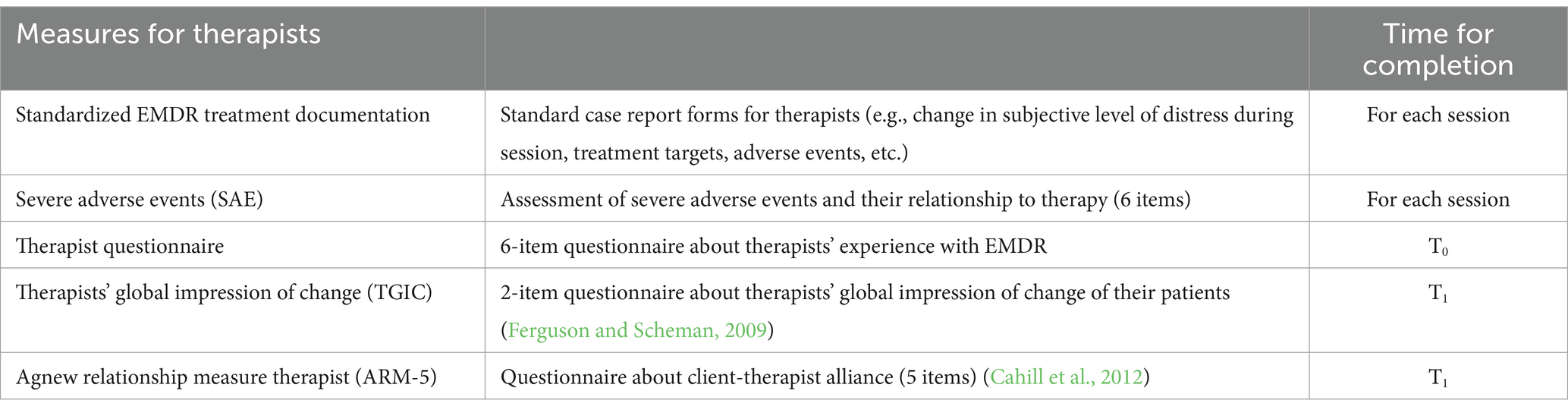
Table 2. Therapists’ documentation.
The proposed case conceptualisation in the treatment of chronic pain follows a three-stage approach according to the standard model of past, present and future, distinguishing between pain-related and non-pain-related trauma.
The classic protocol provides for a systematised target selection, in which, in cases in where the pain is associated with traumatic and (even today!) stressful experiences, desensitisation and reprocessing of these experiences should be started first (Borst et al., 2024; Tesarz et al., 2015). In cases where either no traumatic experience can be identified as the trigger or where the traumatic event has been reprocessed more successfully in the meantime, the distressing memories and thoughts associated with the pain should be processed. After processing distressing memories and thoughts, and in cases where no distressing memories or thoughts can be identified initially, the pain can also be focussed on directly using the specific pain protocol. In cases where patients gain access to new, previously repressed experiences during pain processing, reactivated memories can be revisited and further processed during the course of therapy using the standard protocol or a modified standard protocol. Finally, or in addition, it is possible to use the standard protocol, modified standard protocol, the absorption exercise or the flash-forward protocol to alleviate dysfunctional fears of illness, future pain crises and potential pain triggers.
In practice, however, it has been shown that other targets are relevant in the treatment of patients with pain in addition to classic traumas and the pain itself.
For example, interpersonal conflicts and maladaptive health fears often play also a central role in patients with chronic pain. Thus, in contrast to patients with post-traumatic stress symptoms, the focus of treatment for patients with chronic pain is often initially on the present. This includes processing the current pain as well as dealing with pain-related fears, with a particular focus on dysfunctional health fears. Health fears reinforce the perception of the threat posed by one’s own body, whereby it is not only about the fear of possible illnesses, but also about frightening ‘misconceptions’ about one’s own body (e.g., ‘damaged intervertebral disc’ or ‘worn joint surface’). It is of the utmost importance to ascertain the patient’s individual understanding of the illness, to identify defect-oriented perceptions of their own body and, if necessary, to correct them so that the patient can regain confidence in their own body. Furthermore, relevant interpersonal conflict situations of the patient are considered in treatment planning. The network deliberately avoids standardised guidelines for case conceptualisation in order to reflect the real-world setting as well as possible and at the same time not to restrict the therapists too much. Instead, systematic documentation of the target selection by the therapist is planned in order to be able to explore possible peculiarities in the case conceptualisation in greater depth.
Outpatient therapists will identify patients with chronic pain conditions for whom they would like to provide an EMDR intervention as part of their regular psychotherapy. In a first step, these patients will be informed by the therapists and will give their written consent to be contacted by the study team at the University Hospital of Heidelberg. There will be no specific recruitment; rather, therapists will decide which patients to admit for outpatient therapy and which to report to the EMDR network. Within a further diagnostic appointment, the Structured Clinical Interview for the Diagnostic and Statistical Manual for Mental Disorders (SCID-5) (First et al., 2015) will be conducted by trained research assistants via telephone. Figure 1 illustrates the subsequent steps of data acquisition, which will be conducted online using the web application REDCap (Harris et al., 2019). First, eligible patients undergo a comprehensive baseline assessment (T0), including a broad range of self-rating instruments on various domains of relevant symptomatology, physical and emotional functioning, and other potential mechanistic and predictive factors. When patients and therapists decide to end the therapy, we will conduct a post-treatment outcome assessment (T1) including main outcomes, relevant measures from the baseline assessment, therapeutic alliance, therapy evaluation, and potential adverse effects associated with the treatment. Finally, three follow-up assessments (T2–T4) will be implemented 4 weeks and 3 months and 12 months post-treatment.
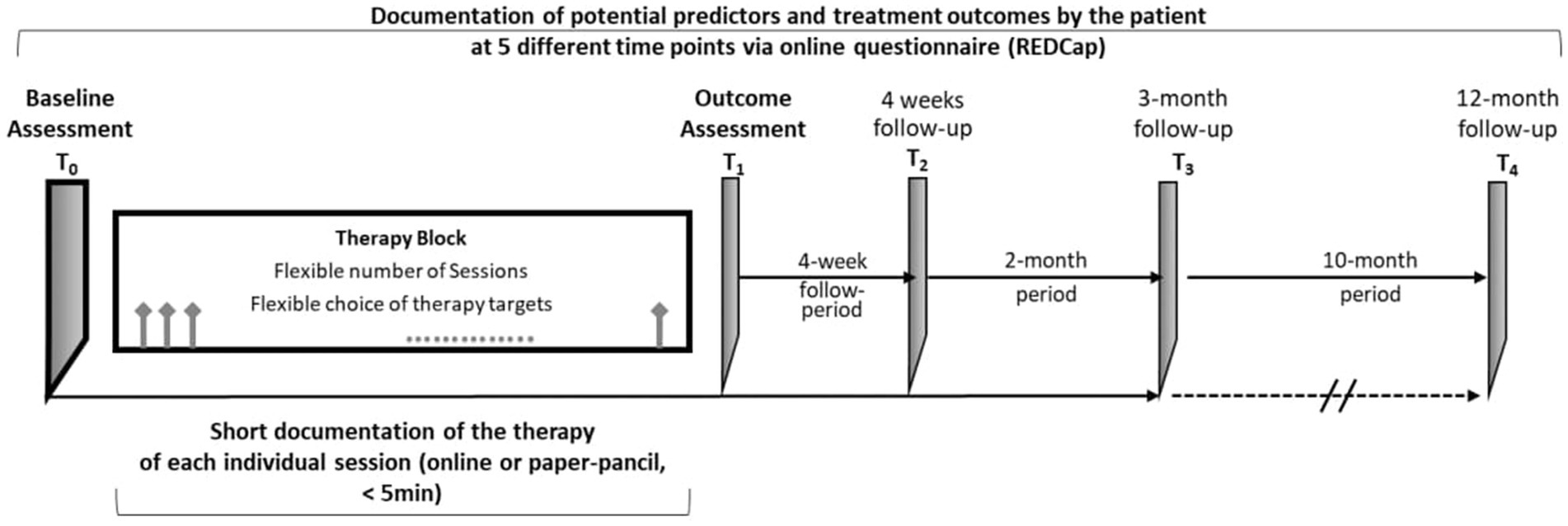
Figure 1. Flow chart of data acquisition. T0, baseline assessment; T1, post-treatment outcome assessment; T2–T4, 4-month follow-up assessment.
During the treatment period, therapists will meticulously document each therapy session to ensure comprehensive data collection and analysis. This documentation includes recording severe potential adverse events (e.g., hospital admissions, suicidality) and specific features of the EMDR treatment, such as the therapeutic target, the bilateral stimulation technique used, and the subjective units of distress. Additionally, therapists will complete a questionnaire regarding their prior experience with EMDR and the frequency with which they treat patients with chronic pain.
The documentation process involves capturing detailed information on critical aspects of each EMDR session, including the patient’s distress levels and beliefs about their symptoms before and after the session. Therapists will also assess and record the patient’s acceptance of the psychological model and provide a brief summary of the session’s content.
By systematically documenting these elements, therapists will create a comprehensive data set that facilitates detailed analysis of the processes and outcomes of EMDR therapy. This rigorous approach enhances the validity of the trial and contributes to the growing evidence base for EMDR therapy in the treatment of chronic pain and associated psychological conditions.
The network includes both patients and therapists, each meeting specific inclusion and exclusion criteria to ensure the reliability and validity of the study outcomes.
• Therapists: Must have completed formal training in psychotherapy and possess an officially recognized certification in EMDR therapy. Only therapists who meet these stringent professional qualifications are included to ensure the consistency and quality of EMDR delivery.
• Patients: Eligible patients are those who have sufficient proficiency in the German language, as effective communication is essential for the therapeutic process and for providing informed consent. Patients must report experiencing chronic pain and must be commencing therapy with a therapist participating in this network. The prerequisite is that the patients have already started psychotherapy, but the planned EMDR treatment has not yet taken place as part of this therapy but is planned in the further course of therapy. Completed previous therapies, including EMDR, are not an exclusion criterion, but will be documented systematically. Patients must be at least 18 years old, with no upper age limit, and be able to give informed consent.
• Severe Psychiatric Comorbidity: Patients exhibiting severe psychiatric conditions that impair their ability to provide informed consent, including suicidality and psychosis spectrum disorders, are excluded. These conditions can significantly interfere with the patient’s ability to participate effectively in the study and can complicate the assessment of EMDR’s efficacy.
• Language Proficiency: Patients lacking sufficient proficiency in the German language are excluded to ensure clear communication and accurate understanding of the therapy and study requirements. This criterion is critical for maintaining the integrity of the therapeutic process and the reliability of the study data.
By establishing these inclusion and exclusion criteria, the study aims to create a representative sample of patients with chronic pain that can provide robust and reliable data on the efficacy of EMDR therapy in treating chronic pain. The dual focus on therapists’ qualifications and patients’ characteristics ensures a high standard of therapeutic intervention and data collection. This methodological rigour is essential for drawing valid conclusions about the therapeutic benefits of EMDR in this specific patient population.
The sample size calculation for the present exploratory and feasibility evaluation within the ‘EMDR Pain Therapy Network’ is primarily based on the need to obtain meaningful data on the feasibility and efficiency of the network structures. Considering the aim of assessing the feasibility of a possible future randomised controlled trial, a minimum number of 20 therapists will be recruited, each of whom should enrol at least 10 patients in the trial. This results in a total of at least 200 patients.
This sample size is appropriate for the following reasons:
• It enables a comprehensive assessment of the efficacy and side effect profiles of EMDR therapy for chronic pain.
• It is suitable for testing the feasibility of an accompanying evaluation in the outpatient setting, including documentation quality and patient satisfaction.
The results of the evaluation of the initial sample of 200 patients will be crucial in planning a larger multicentre trial. They should show whether the network is able to recruit enough patients and provide high quality data, and whether the therapeutic practices within the network are sufficiently standardised to conduct a randomised controlled trial.
It is important to note that this number of cases does not have to be the definitive end of the trial. Rather, once this initial target number has been reached, an interim analysis should be carried out to assess the logistical and administrative aspects of the study implementation, in addition to the scientific aspects. On this basis, an adapted or expanded recruitment strategy can be developed for the next phase of the study.
Therapists participating in the study will be recruited via the EMDRIA Germany or will be referred by other participating therapists. Additionally, the project will presented at national and international conferences, gaining exposure to a broader audience, and an article about the project has been published in the EMDRIA journal. The study is open to all psychotherapists and physicians with formal psychotherapeutic training and accredited EMDR certification.
To promote the implementation of EMDR in pain therapy, the network emphasises supporting the application of EMDR in pain management according to scientific standards. This is achieved by providing validated EMDR treatment protocols free of charge (see Supplementary material) and offering practical working materials for therapists. These measures not only enhance the appeal of network membership but also encourage the standardisation of treatment approaches and facilitate the specialisation of EMDR therapists in treating patients with complex pain disorders.
Additionally, the network has launched a virtual platform where therapists can connect, share experiences, and participate in bimonthly online peer supervision meetings. During these meetings, they discuss complex patient cases and receive supervisory feedback. The platform is supplemented by a regularly updated newsletter that informs about the latest developments, research findings, and relevant events in the field of pain therapy. The newsletter provides lay-friendly summaries of current scientific studies and contextualises them within the clinical setting, thus aiding the translation of scientific knowledge into clinical practice.
In this study, we aim to identify factors that predict a significant treatment response to EMDR therapy for chronic pain. We will follow established recommendations for outcome measures in clinical chronic pain trials and recommendations for interpreting clinical importance of group differences [Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials, IMMPACT (Dworkin et al., 2008; Turk et al., 2003)]. Core outcome domains include pain intensity, physical functioning, emotional functioning, stress experience, and both patient and therapist ratings of patients improvement and satisfaction.
The effectiveness of EMDR therapy will be quantified by determining effect sizes and response and non-response rates on various outcome variables.
Global ratings of change of the overall situation due to treatment was evaluated using the Patient Global Impression of Change (PGIC) scale, which is a single-item rating on a 7-point scale ranging from “very much improved” to “very much worse” (Ferguson and Scheman, 2009). Changes of “much improved” and “very much improved” are considered as clinically relevant. Similarly, therapists should perceive that at patients show at least 60% of improvement, as measured by a score of greater than or equal to 5 on the Therapist Global Impression of Change Scale (TGIC).
A multidimensional phenotyping of patients will be performed, including various aspects such as clinical symptoms, psychological comorbidity, personality factors, therapy expectations and functionality. The aim is to identify predictors that can be used to predict treatment success or failure.
The EMDR Pain Network will evaluate the structures and processes of the network for conducting larger multi-centre clinical trials. This will include the assessment of inclusion rates per therapist, the quality of documentation of outcome variables, and patient satisfaction with the adjunctive evaluation.
1. Negative Effects: These are intended to be captured using the Negative Effects Questionnaire (NEQ) and the Inventory for Assessing Negative Effects of Psychotherapy (INEP).
2. Severe Adverse Events (SAEs): These will be documented and examined for potential causal relationships with EMDR therapy.
Table 1 shows all measures used during the different points of data acquisition. In addition to the assessment of core-outcome domains, an extensive baseline assessment is performed using standardised and validated questionnaires (see Table 1). The aim is to identify possible predictors in the areas of psychological comorbidity (anxiety, depression, somatization and sleep disorders), catastrophizing, fear of illness and fear avoidance behaviour, past stress experiences and post-traumatic distress, therapy expectations and therapy experience, as well as individual coping and resilience factors.
These defined criteria should not only capture the direct benefits and tolerability of EMDR therapy in chronic pain patients, but also contribute to the optimization of therapeutic approaches and the improvement of treatment quality.
The primary aim of the ‘EMDR Pain Therapy Network’ is to generate a high-quality dataset that facilitates the investigation of future effectiveness measures, response rates, and potential predictors for both response and non-response. This dataset will provide broad opportunities for exploratory analyses to address future research questions. Within the network, specific questions and analyses are pre-planned:
Descriptive Analysis: To characterise the sample, descriptive statistics will be employed, covering demographic data, clinical characteristics, and outcome criteria. Continuous variables will be described using means, standard deviations, medians, and interquartile ranges. Categorical variables will be presented through frequencies and percentages.
Effectiveness Outcome Analysis: The effectiveness of EMDR therapy will be evaluated by calculating effect sizes using Cohen’s d, with t-tests to determine these values. Response and non-response rates will be analysed using binary logistic regressions, with the PGIC and TGIC scales as dependent variables.
Adverse effect Outcome Analysis: Adverse effects will be quantified through frequency analysis for each item of the NEQ questionnaire, and serious adverse events (SAEs) will be described using descriptive statistics, analysing their correlation with EMDR therapy.
Therapist Influence: The impact of therapists on treatment outcomes will be explored using multivariate models or regression analyses, considering various contextual factors such as different therapy approaches, therapist experience.
Analysis of predictors: Predictors for therapy success will be identified through multivariate regression analyses, using data from multidimensional phenotyping as independent variables.
Feasibility and Practicability Assessment: The practicability of the evaluation process will be assessed by analysing dropout rates, missing values, and the variability of inclusion rates per therapist. An intention-to-treat analysis will be conducted, and satisfaction with the evaluation will be measured using z-scores.
The establishment of the ‘EMDR Pain Network Germany’ is a significant step towards promoting clinical exchange and deepening the understanding of EMDR in pain therapy. This interdisciplinary scientific-clinical platform includes standardised treatment protocols, an online data collection system with anonymised data and suggestions for a comprehensive core assessment set. It also enables regular professionals and promotes collaboration. These components are intended to personalise future therapies and create the basis for large-scale randomised clinical trials to enable systematic research into the mechanisms and effects of EMDR in pain treatment.
The network structure integrates scientists, therapists, and patients and is organised into three main levels: 1. a steering group that leads and organises the network; 2. participating therapists and associated scientists, who keep the network active; and 3. the patient group, which provides outcome data and forms the foundation of the network. This structure serves as a guide and an open system that promotes the continuous expansion of the network and the long-term exchange of experiences and expertise. The integration of these levels introduces considerable complexity, but it is crucial for gaining in-depth and long-term insights into treatment effects and paves the way for the discussion of analytical challenges.
The principle of opening the network to all interested scientists and therapists requires clear inclusion and exclusion criteria. To ensure a balance between the widespread use of EMDR and the maintenance of high-quality standards, basic therapeutic training and an officially recognised training certificate for EMDR (e.g., from the professional association) should be required. This ensures therapeutic standards and the generation of high-quality data for valuable analyses.
The planned analyses, especially predictor analyses, are challenging and require large sample sizes and longer study durations. These requirements fit with current big data initiatives that require early and systematic data collection. A proposed core assessment model will guide future research initiatives and studies, improve comparability and facilitate meta-analytical syntheses. Through continuous data collection and analysis, the network will provide valuable insights into the effectiveness of EMDR in pain management, deepen the understanding of this method and drive future research and clinical trials.
The network not only investigates the effectiveness and prediction of treatment response to EMDR in real clinical settings but also establishes a robust foundation for future randomised controlled multicentre studies. The systematic training and experience of therapists in the use of EMDR, along with standardised data collection methods, facilitate the development of a pool of qualified professionals essential for further clinical research. This pool of therapists will be a valuable resource for future studies aimed at testing the efficacy of EMDR on a larger scale and advancing its implementation in the treatment of complex pain disorders in clinical practice.
The network promotes the use of EMDR in pain therapy without commercial interests. Free working materials and free participation in the network support open science and patient-centred treatment. This approach aims to remove barriers to access and facilitate the dissemination of this effective therapy. This promotes a collaborative and inclusive model that benefits therapists and patients alike.
In summary, the developed framework promises to improve the understanding of the therapeutic effect of EMDR on chronic pain. It enables longitudinal analyses that describe the course of treatment success and identify individual differences in outcomes. This provides the basis for personalised treatment strategies that are tailored to the individual needs of patients with chronic pain in order to optimise therapeutic outcomes and improve quality of life.
In accordance with the ethical principles governing human research, all participants and therapists are required to provide written informed consent prior to enrolment. Ethical approval for data collection was obtained from the Research Ethics Committee II of the Medical Faculty of the University of Heidelberg (approval number S-696/2023), ensuring compliance with the ethical standards of the Declaration of Helsinki.
SV: Writing – review & editing, Writing – original draft, Supervision, Project administration, Methodology, Investigation, Formal analysis, Conceptualization. AH: Writing – review & editing, Supervision, Resources, Methodology, Funding acquisition, Conceptualization. ML: Writing – review & editing, Resources, Funding acquisition. KB: Writing – review & editing, Resources, Funding acquisition. SW: Writing – review & editing. GS: Writing – review & editing, Supervision. EB: Writing – review & editing, Methodology, Data curation, Conceptualization. MH: Writing – review & editing. H-CF: Writing – review & editing. WE: Writing – review & editing. JT: Writing – review & editing, Writing – original draft, Supervision, Resources, Project administration, Methodology, Investigation, Conceptualization.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. For the publication fee we acknowledge financial support by Heidelberg University.
Therapists in the EMDR Pain Network: Dr. Kristin Grupp, Dr. Ulla Raczinski, Martina Arrowsmith, Dr. Rahul Mukherjee, Dagmar Spurny, Dr. Dieter Stein, Dr. Karsten Krause, Manfred Hübner, Klaus Wild, Mathias Fauth, Dr. Marion Schowalter, Alexandra Selesnew, Dr. Simone Schneider, Simone Kandler, Monika Schwarz, Dr. Christina Eisenecker, Maria Prkno. ChatGPT was used to improve language style.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1449150/full#supplementary-material
ARM, Agnew Relationship Measure; BSI, Brief Symptom Inventory; CMSP, chronic musculoskeletal pain; CPG, Chronic Pain Grade Scale; CQR5, Compliance Questionnaire for Rheumatology; CTQ, Childhood Trauma Questionnaire; EMDR, eye movement desensitization and reprocessing therapy; FABQ, Fear Avoidance Belief Questionnaire; FPQ, Fear of Pain Questionnaire; FSS, Fatigue Severity Scale; HADS, Hospital Anxiety and Depression Scale; INEP, Inventory for Assessing Negative Effects of Psychotherapy (Inventar zur Erfassung negativer Effekte von Psychotherapie); MPI, Multidimensional Pain Inventory; NEQ, Negative Effects Questionnaire; PATHEV, Patients’ Therapy Expectations and Evaluations (Therapieerwartung und Therapieevaluation von Patienten); PDS, Posttraumatic Diagnostic Scale; PGIC, Patient’s Global Impression of Change; PRSS, Pain-Related Self Statement Scale; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale; RS-11, Resilience Scale (Resilienzskala); SAE, severe adverse effects; SCID-5, Structured Clinical Interview for the Diagnostic and Statistical Manual for Mental Disorders; SES, Pain Sensation Scale (Schmerzempfindungsskala); SF-12, Short Form 12; SSD-12, Somatic Symptom Disorder – B Criteria Scale; SSS-8, Somatic Symptom Scale; TGIC, Therapist’s Global Impression of Change; TICS, Trier Inventory of Chronic Pain (Trierer Inventar zum chronischen Schmerz); WI-7, Whiteley Index; WOMAC, Western Ontario and McMaster Universities Arthritis Index; WPI, Widespread Pain Index.
Asay, T. P., Lambert, M. J., Gregersen, A. T., and Goates, M. K. (2002). Using patient-focused research in evaluating treatment outcome in private practice. J. Clin. Psychol. 58, 1213–1225. doi: 10.1002/jclp.10107
Beiner, E., Baumeister, D., Buhai, D., Löffler, M., Löffler, A., Schick, A., et al. (2022). The PerPAIN trial: a pilot randomized controlled trial of personalized treatment allocation for chronic musculoskeletal pain-a protocol. Pilot Feasibility Stud, 8:251. doi: 10.1186/s40814-022-01199-6
Bellamy, N. (2005). Development, validation and globalisation of a health status measure for evaluating patients with osteoarthritis: University of Glasgow (United Kingdom).
Bernstein, D. P., Fink, L., Handelsman, L., and Foote, J. (1998). Childhood trauma questionnaire. Assessment of family violence: A handbook for researchers and practitioners.
Borst, M., Moeyaert, M., and van Rood, Y. (2024). The effect of eye movement desensitization and reprocessing on fibromyalgia: a multiple-baseline experimental case study across ten participants. Neuropsychol. Rehabil. 1-33, 1–33. doi: 10.1080/09602011.2024.2314883
Buysse, D. J., Reynolds, C. F. III, Monk, T. H., Hoch, C. C., Yeager, A. L., and Kupfer, D. J. (1991). Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh sleep quality index (PSQI). Sleep 14, 331–338
Cahill, J., Stiles, W. B., Barkham, M., Hardy, G. E., Stone, G., Agnew-Davies, R., et al. (2012). Two short forms of the Agnew relationship measure: the ARM-5 and ARM-12. Psychother. Res. 22, 241–255. doi: 10.1080/10503307.2011.643253
Dixon, D., Pollard, B., and Johnston, M. (2007). What does the chronic pain grade questionnaire measure? Pain 130, 249–253. doi: 10.1016/j.pain.2006.12.004
Dworkin, R. H., Turk, D. C., Wyrwich, K. W., Beaton, D., Cleeland, C. S., Farrar, J. T., et al. (2008). Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 9, 105–121. doi: 10.1016/j.jpain.2007.09.005
Fairbank, J. C., and Pynsent, P. B. (2000). The Oswestry disability index. Spine 25, 2940–2953. doi: 10.1097/00007632-200011150-00017
Ferguson, L., and Scheman, J. (2009). Patient global impression of change scores within the context of a chronic pain rehabilitation program. J. Pain 10:S73. doi: 10.1016/j.jpain.2009.01.258
First, M., Williams, J., Karg, R., and Spitzer, R. (2015). Structured clinical interview for DSM-5 disorders, research version. Arlington: American Psychiatric Association.
Flor, H., Behle, D. J., and Birbaumer, N. (1993). Assessment of pain-related cognitions in chronic pain patients. Behav. Res. Ther. 31, 63–73. doi: 10.1016/0005-7967(93)90044-U
Foa, E. B., Cashman, L., Jaycox, L., and Perry, K. (1997). The validation of a self-report measure of posttraumatic stress disorder: the posttraumatic diagnostic scale. Psychol. Assess. 9, 445–451. doi: 10.1037/1040-3590.9.4.445
Friedberg, F. (2004). Eye movement desensitization in fibromyalgia: a pilot study. Complement. Ther. Nurs. Midwifery 10, 245–249. doi: 10.1016/j.ctnm.2004.06.006
Galvez-Sánchez, C. M., De la Coba, P., Duschek, S., and Reyes del Paso, G. A. (2020). Reliability, factor structure and predictive validity of the widespread pain index and symptom severity scales of the 2010 American College of Rheumatology criteria of fibromyalgia. J. Clin. Med. 9:2460. doi: 10.3390/jcm9082460
Gandhi, S. K., Salmon, J. W., Zhao, S. Z., Lambert, B. L., Gore, P. R., and Conrad, K. (2001). Psychometric evaluation of the 12-item short-form health survey (SF-12) in osteoarthritis and rheumatoid arthritis clinical trials. Clin. Ther. 23, 1080–1098. doi: 10.1016/S0149-2918(01)80093-X
Gatchel, R. J., Peng, Y. B., Peters, M. L., Fuchs, P. N., and Turk, D. C. (2007). The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol. Bull. 133, 581–624. doi: 10.1037/0033-2909.133.4.581
Geisheim, C., Hahlweg, K., Fiegenbaum, W., Frank, M., Schröder, B., and von Witzleben, I. (2002). Das Brief Symptom Inventory (BSI) als Instrument zur Qualitätssicherung in der Psychotherapie [The German version of the Brief Symptom Inventory (BSI): Reliability and validity in a sample of outpatient psychotherapy patients]. Diagnostica. 48, 28–36. doi: 10.1026/0012-1924.48.1.28
Geissner, E. (1995). Die Schmerzempfindungsskala SES–Ein differenziertes und veränderungssensitives Verfahren zur Erfassung chronischer und akuter Schmerzen. Rehabilitation 34, 35–43.
Gerhardt, A., Leisner, S., Hartmann, M., Janke, S., Seidler, G. H., Eich, W., et al. (2016). Eye movement desensitization and reprocessing vs. treatment-as-usual for non-specific chronic back pain patients with psychological trauma: a randomized controlled pilot study. Front. Psych. 7:201. doi: 10.3389/fpsyt.2016.00201
Gierk, B., Kohlmann, S., Kroenke, K., Spangenberg, L., Zenger, M., Brähler, E., et al. (2014). The somatic symptom scale–8 (SSS-8): a brief measure of somatic symptom burden. JAMA Intern. Med. 174, 399–407. doi: 10.1001/jamainternmed.2013.12179
Gilam, G., Gross, J. J., Wager, T. D., Keefe, F. J., and Mackey, S. C. (2020). What is the relationship between pain and emotion? Bridging constructs and communities. Neuron 107, 17–21. doi: 10.1016/j.neuron.2020.05.024
Glöckner-Rist, A., Barenbrügge, J., and Rist, F. Deutsche version des Whiteley index (WI-d). Zusammenstellung Sozialwissenschaftlicher items Skalen ZIS [internet]; (2007)
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O'Neal, L., et al. (2019). The REDCap consortium: building an international community of software platform partners. J. Biomed. Inform. 95:103208. doi: 10.1016/j.jbi.2019.103208
Hashmi, J. A., Baliki, M. N., Huang, L., Baria, A. T., Torbey, S., Hermann, K. M., et al. (2013). Shape shifting pain: chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain 136, 2751–2768. doi: 10.1093/brain/awt211
Heuft, G., Senf, W., Bell, K., Cording, C., Geyer, M., Janssen, P. L., et al. (1998). Psy-BaDo: Kernmodul einer Basisdokumentation in der Fachpsychotherapie. Psychotherapeut 43, 48–52. doi: 10.1007/s002780050099
Hughes, L. D., Done, J., and Young, A. (2013). A 5 item version of the compliance questionnaire for rheumatology (CQR5) successfully identifies low adherence to DMARDs. BMC Musculoskelet. Disord. 14, 1–8. doi: 10.1186/1471-2474-14-286
Hurst, H., and Bolton, J. (2004). Assessing the clinical significance of change scores recorded on subjective outcome measures. J. Manip. Physiol. Ther. 27, 26–35. doi: 10.1016/j.jmpt.2003.11.003
Kerdijk, W., Tio, R. A., Mulder, B. F., and Cohen-Schotanus, J. (2013). Cumulative assessment: strategic choices to influence students’ study effort. BMC Med. Educ. 13:172. doi: 10.1186/1472-6920-13-172
Kerns, R. D., Turk, D. C., and Rudy, T. E. (1985). The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 23, 345–356. doi: 10.1016/0304-3959(85)90004-1
Klein, E. M., Brähler, E., Dreier, M., Reinecke, L., Müller, K. W., Schmutzer, G., et al. (2016). The German version of the perceived stress scale–psychometric characteristics in a representative German community sample. BMC Psychiatry 16, 1–10. doi: 10.1186/s12888-016-0875-9
Kocalevent, R.-D., Zenger, M., Heinen, I., Dwinger, S., Decker, O., and Brähler, E. (2015). Resilience in the general population: standardization of the resilience scale (RS-11). PLoS One 10:e0140322. doi: 10.1371/journal.pone.0140322
Konuk, E., Epözdemir, H., Atçeken, Ş., Aydın, Y., and Yurtsever, A. (2011). EMDR treatment of migraine. J. EMDR Pract. Res. 5, 166–176. doi: 10.1891/1933-3196.5.4.166
Krupp, L. B., LaRocca, N. G., Muir-Nash, J., and Steinberg, A. D. (1989). The fatigue severity scale: application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 46, 1121–1123. doi: 10.1001/archneur.1989.00520460115022
Ladwig, I., Rief, W., and Nestoriuc, Y. (2014). What are the risks and side effects of psychotherapy?-development of an inventory for the assessment of negative effects of psychotherapy (INEP). Verhaltenstherapie 24, 252–263. doi: 10.1159/000367928
Laliotis, D., Luber, M., Oren, U., Shapiro, E., Ichii, M., Hase, M., et al. (2021). What is EMDR therapy? Past, present, and future directions. J. EMDR Pract. 15, 186–201. doi: 10.1891/EMDR-D-21-00029
Leisner, S., Gerhardt, A., Tesarz, J., Janke, S., Seidler, G. H., and Eich, W. (2014). Frühe Missbrauchserlebnisse bei chronischem Kreuzschmerz. Schmerz 28, 600–606. doi: 10.1007/s00482-014-1487-2
Lutz, W. (2003). Efficacy, effectiveness, and expected treatment response in psychotherapy. J. Clin. Psychol. 59, 745–750. doi: 10.1002/jclp.10169
Matthijssen, S., Lee, C. W., de Roos, C., Barron, I., Jarero, I., Shapiro, E., et al. (2020). The current status of EMDR therapy, specific target areas, and goals for the future. J. EMDR Pract. Res. 14, 241–284. doi: 10.1891/EMDR-D-20-00039
McNeil, D. W., and Rainwater, A. J. (1998). Development of the fear of pain questionnaire-III. J. Behav. Med. 21, 389–410. doi: 10.1023/A:1018782831217
Pfingsten, M., Kröner-Herwig, B., Leibing, E., and Kronshage, U. (2000). Validation of the German version of the fear-avoidance beliefs questionnaire (FABQ). Eur. J. Pain 4, 259–266. doi: 10.1053/eujp.2000.0178
Pinto, A. M., Geenen, R., Wager, T. D., Lumley, M. A., Häuser, W., Kosek, E., et al. (2023). Emotion regulation and the salience network: a hypothetical integrative model of fibromyalgia. Nat. Rev. Rheumatol. 19, 44–60. doi: 10.1038/s41584-022-00873-6
Rostaminejad, A., Behnammoghadam, M., Rostaminejad, M., Behnammoghadam, Z., and Bashti, S. (2017). Efficacy of eye movement desensitization and reprocessing on the phantom limb pain of patients with amputations within a 24-month follow-up. Int. J. Rehabil. Res. 40, 209–214. doi: 10.1097/MRR.0000000000000227
Rozental, A., Kottorp, A., Boettcher, J., Andersson, G., and Carlbring, P. (2016). Negative effects of psychological treatments: an exploratory factor analysis of the negative effects questionnaire for monitoring and reporting adverse and unwanted events. PLoS One 11:e0157503. doi: 10.1371/journal.pone.0157503
Schubert, S. J., Lee, C. W., and Drummond, P. D. (2011). The efficacy and psychophysiological correlates of dual-attention tasks in eye movement desensitization and reprocessing (EMDR). J. Anxiety Disord. 25, 1–11. doi: 10.1016/j.janxdis.2010.06.024
Schulte, D. (2005). Messung der therapieerwartung und Therapieevaluation von patienten (PATHEV). Z. Klin. Psychol. Psychother. 34, 176–187. doi: 10.1026/1616-3443.34.3.176
Schulz, P., Schlotz, W., and Becker, P. (2004). Trierer Inventar zum chronischen stress (TICS) [Trier inventory for chronic stress (TICS)].
Tennant, C., and Andrews, G. (1976). A scale to measure the stress of life events. Aust. N. Z. J. Psychiatry 10, 27–32. doi: 10.3109/00048677609159482
Tesarz, J., Gerhardt, A., Leisner, S., Janke, S., Hartmann, M., Seidler, G. H., et al. (2013). Effects of eye movement desensitization and reprocessing (EMDR) on non-specific chronic back pain: a randomized controlled trial with additional exploration of the underlying mechanisms. BMC Musculoskelet. Disord. 14, 1–8. doi: 10.1186/1471-2474-14-256
Tesarz, J., Leisner, S., Gerhardt, A., Janke, S., Seidler, G. H., Eich, W., et al. (2014). Effects of eye movement desensitization and reprocessing (EMDR) treatment in chronic pain patients: a systematic review. Pain Med. 15, 247–263. doi: 10.1111/pme.12303
Tesarz, J., Seidler, G. H., and Eich, W. (2015). Schmerzen behandeln mit EMDR: das Praxishandbuch. Stuttgart: Klett-Cotta Verlag.
Tesarz, J., Wicking, M., Bernardy, K., and Seidler, G. H. (2019). EMDR therapy's efficacy in the treatment of pain. J. EMDR Pract. Res. 13, 337–344. doi: 10.1891/1933-3196.13.4.337
Toussaint, A., Murray, A. M., Voigt, K., Herzog, A., Gierk, B., Kroenke, K., et al. (2016). Development and validation of the somatic symptom disorder–b criteria scale (SSD-12). Psychosom. Med. 78, 5–12. doi: 10.1097/PSY.0000000000000240
Turk, D. C., Dworkin, R. H., Allen, R. R., Bellamy, N., Brandenburg, N., Carr, D. B., et al. (2003). Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 106, 337–345. doi: 10.1016/j.pain.2003.08.001
Vos, T., Lim, S. S., Abbafati, C., Abbas, K. M., Abbasi, M., Abbasifard, M., et al. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396, 1204–1222. doi: 10.1016/S0140-6736(20)30925-9
Watson, D., Clark, L. A., and Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. J. Pers. Soc. Psychol. 54, 1063–1070. doi: 10.1037/0022-3514.54.6.1063
Weldring, T., and Smith, S. M. S. (2013). Article commentary: patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs). Health Serv. Insights 6, HSI.S11093–HSI.S11068. doi: 10.4137/hsi.S11093
Wettstein, M., and Tesarz, J. (2023). Increasing pain prevalence and intensity among middle-aged and older adults: evidence from the German ageing survey. J. Psychosom. Res. 168:111233. doi: 10.1016/j.jpsychores.2023.111233
Williams, A. C., Eccleston, C., and Morley, S. (2012). Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 11:Cd007407. doi: 10.1002/14651858.CD007407.pub3
Zat Çiftçi, Z., Delibaş, D. H., Kaya, T., Külcü, D. G., Sarı, A., Nazlıkul, H., et al. (2024). A randomized controlled trial of eye movement desensitization and reprocessing (EMDR) therapy in the treatment of fibromyalgia. Front. Psych. 15:1286118. doi: 10.3389/fpsyt.2024.1286118
Keywords: chronic pain, eye movement desensitization reprocessing, EMDR, therapy, network
Citation: Vock S, Hofmann A, Lehnung M, Böhm K, Wieland S, Seidler GH, Beiner E, Hermes M, Friederich H-C, Eich W and Tesarz J (2024) Towards international collaboration of clinical research networks for EMDR: the EMDR Pain Network Germany. Front. Psychol. 15:1449150. doi: 10.3389/fpsyg.2024.1449150
Edited by:
Antonio Onofri, Scientific Director School of Specialization in Psychotherapy “Training School” in Rome, Jesi and Spoleto, ItalyReviewed by:
İbrahim Gündoğmuş, Ankara Etlik City Hospital, TürkiyeCopyright © 2024 Vock, Hofmann, Lehnung, Böhm, Wieland, Seidler, Beiner, Hermes, Friederich, Eich and Tesarz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: J. Tesarz, am9uYXMudGVzYXJ6QG1lZC51bmktaGVpZGVsYmVyZy5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.