 Annabel Maurer
Annabel Maurer Adrian Lieb2
Adrian Lieb2 Stephan Bongard
Stephan Bongard
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 12 July 2024
Sec. Pediatric Psychology
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1414852
Introduction: Due to an inhibited tryptophan resorption, patients with fructose malabsorption are expected to experience decreased serotonin synthesis. A deficiency of serotonin may cause internalizing mental disorders like depression and anxiety, and a fructose-oriented eating behavior may affect these symptoms.
Methods: The parents of 24 children and adolescents with a currently diagnosed fructose malabsorption aged 4;00–13;02 years (M = 8.10, SD = 2.05), the parents of 12 patients with a currently confirmed combination of fructose and lactose malabsorption aged 4;00–12;11 years (M = 8.07, SD = 2.11) and the parents of a comparative sample of 19 healthy participants aged 5;00 to 17;07 years (M = 9.06, SD = 3.04) were interviewed. The interviews were conducted using a screening questionnaire of the German “Diagnostic System of Mental Disorders in children and adolescents based on the ICD-10 and DSM-5 DISYPS-III” and a self-developed questionnaire on eating, leisure and sleeping behavior.
Results: On standardized scales parents of children with fructose malabsorption reported higher levels of Depression compared to symptoms of Attention-Deficit/Hyperactivity Disorders (ADHD) and Oppositional Defiant and Conduct Disorders (ODD/CD). Compared to healthy controls, for patients with fructose malabsorption, higher symptom levels of Depression and Anxiety were reported. With regard to eating behavior, within the group with a combination of fructose and lactose malabsorption, a strong positive association between an increased fruit sugar consumption and higher levels of Anxiety and Obsessive-Compulsive Disorders/Tics were found.
Discussion: These results suggest a close association between fructose malabsorption and elevated internalizing psychological symptoms in children and adolescents.
Clinical trial registration:https://drks.de/search/en/trial/DRKS00031047, DRKS-ID [DRKS00031047].
Fructose malabsorption is a common carbohydrate metabolism disorder. In Europe, about one third of adults and two out of three children are affected by fructose malabsorption (Kretschmer, 2022). The present study is based on the consideration that children and adolescents with an untreated fructose malabsorption may suffer from concomitant mental symptoms, which are associated with a reduced intestinal absorption of tryptophan and therefore dysregulated processes of the serotonergic system. It is generally assumed that there is an impaired tryptophan absorption in patients with fructose malabsorption (Ledochowski et al., 2001). The intestinal walls of affected individuals contain only few or impaired passive transport channels, so-called GLUT-5 transporters (Velten and Bayerl, 2007). Those are unable to react adequately to the entry of fructose. As a result, ingested fruit sugar enters virtually undigested into the large intestine, where it is metabolized—in parts—into short-chain fatty acids, hydrogen, and carbon dioxide (Ledochowski et al., 2000b). Among other symptoms, most of these metabolites can cause bloating, abdominal pain, nausea, and vomiting in individuals with fructose malabsorption (Escobar et al., 2014); constipation and diarrhea are also reported (Ledochowski et al., 2000b). Food high in fructose content, like various types of fruits and juices, as well as food enriched with fruit sugar, is described as causing the most discomfort in affected individuals (Latulippe and Skoog, 2011). While metabolized parts in the large intestine may lead to the mentioned gastroenterological complaints in individuals with a dietary fructose intolerance, remaining non-metabolized parts bind to the amino acid tryptophan. As a consequence, the essential amino acid is not available for further metabolic processes—such as the synthesis of serotonin (Huether et al., 1998)—to the same extent as in persons without fructose malabsorption (Ledochowski et al., 2001). Serotonin is known to modulate a variety of physiological processes (Berger et al., 2009) and a deficiency of serotonin can promote depressive symptoms (Mehler-Wex and Kölch, 2008; Jenkins et al., 2016). A study by Ledochowski et al. (2001) discovered lowered blood tryptophan levels in individuals with fructose malabsorption. Compared to a healthy sample, the female participants were also reported to have a higher expression of depressive symptoms. Varea et al. (2004) examined fourteen adolescents, eight of whom suffered from a combined fructose and lactose malabsorption, five from a lactose malabsorption, and one person was known to have an isolated fructose malabsorption. The results showed an association between depressive symptoms and the combined form of fructose and lactose malabsorption. A more recent study by Enko et al. (2018) revealed an association between fructose malabsorption and depressive symptoms. Other studies showed that a diet adapted to fructose malabsorption led most affected individuals to experience relief not only of physical symptoms (Litschauer-Poursadrollah et al., 2012; Berni Canani et al., 2016), but with regard to depression, also of psychological complaints (Ledochowski et al., 2000a). Based on these previous results, we hypothesized that an impaired absorption of tryptophan in children and adolescents with fructose malabsorption may promote psychological symptoms that can be associated with serotonergic processes. In addition to depressive symptoms (Ledochowski et al., 1998), special attention was given to anxiety (Deister, 2013) and obsessive-compulsive spectrum disorders (Kis et al., 2007). Because in some cases tic disorders have been reported to be associated with the serotonergic system (Steeves and Fox, 2008), they were also included in this study.
It was hypothesized that children and adolescents with fructose malabsorption more likely show heightened serotonin-associated internalizing psychological symptoms (Anxiety and Depression extended by Obsessive-Compulsive Disorders/Tics) than externalizing ones (Attention-Deficit/Hyperactivity Disorders and Oppositional Defiant and Conduct Disorders). Additionally, it was hypothesized that they would show higher levels of internalizing mental symptoms than a healthy control group. Also, the degree of symptom expression was assumed to be related to eating behavior. It was expected, that within the group of children and adolescents with fructose malabsorption, the quantity of fruit sugar consumption would correlate with the degree of internalizing psychological symptoms.
Children and adolescents and their caregivers were recruited by support of the ambulatory gastroenterological department for children and adolescents of the Goethe-University Hospital in Frankfurt am Main, Germany. A total of 43 patients (n = 22 female, n = 21 male) who had been referred to the University Hospital due to a suspected fructose malabsorption or a combination of a fructose and lactose malabsorption formed the initial sample. Patients for whom tests disconfirmed the diagnosis of a malabsorption (n = 7) were obtained as a control sample. This was then supplemented by 12 additionally recruited children and adolescents without confirmed fructose and/or lactose malabsorption to a total of 19 persons (16 female).
The age of the group “Fructose Malabsorption” (n = 24) ranged from 4;00 to 13;02 years (M = 8.10, SD = 2.05) for 9 female and 15 male participants. The age of the group “Fructose and Lactose Malabsorption combined” (n = 12) ranged from 4;00 to 12;11 years (M = 8.07, SD = 2.11) for 6 female and 6 male participants. The control sample ranged in age from 5;00 to 17;07 years (M = 9.06, SD = 3.04), for sixteen female and three male participants. The described differences in gender distribution in the three aforementioned groups were statistically significant [F(2, 54) = 5.54; p = 0.007], but no group differences could be secured with regard to age [F(2, 54) = 0.99; p = 0.38]. Participation was voluntary and without compensation. Families were informed in advance—both verbally and in writing—about the study and how it would be conducted and gave written informed consent to participate. Parents were able to voluntarily provide their e-mail address in order to receive more detailed information about the study results after the survey was completed. The e-mail address was stored separately from the study data.
The study was approved by the ethics committee of the Department of Psychology and Sport Sciences, Goethe University Frankfurt, Germany.
Three different questionnaires were used which were completed in their parent-rating version in paper-pencil format. They are explained in the following.
At first the Questionnaire for the Screening of mental disorders FBB-SCREEN, a screening questionnaire of the German Diagnostic System of Mental Disorders in children and adolescents based on the ICD-10 and DSM-5 DISYPS-III (Döpfner and Görtz-Dorten, 2017) was filled out by the parents. The DISYPS-III is a diagnostic system that covers mental disorders in children and adolescents aged 4;00–17;11 years. The used FFB-SCREEN captures a broad spectrum of psychological symptoms in an economical way and provides results that can justify the administration of further disorder-specific instruments. With 49 items it records initial indications of the presence of mental disorders related to ICD-10 and DSM-5. Items are answered on a four-point Likert scale, on which symptom severity is rated from 0 to 3. The majority of items can be subsumed to the scales Screening Attention-Deficit/Hyperactivity Disorders (ADHD), Screening Oppositional Defiant and Conduct Disorders (ODD/CD), Screening Anxiety, Screening Depression, Screening Developmental and Excretory Disorders, Screening Autism and Screening Obsessive-Compulsive Disorders/Tics (OCD/Tics). Except for the scales Screening Developmental and Excretory Disorders and Screening Obsessive-Compulsive Disorders/Tics, sufficient internal consistencies between α = 0.67 and α = 0.92 are reported. For the two scales with less satisfactory internal consistencies, the scales’ authors recommend further data analysis on item level.
These so-called subscales can largely be assigned to the following superordinate scales: Screening External (Screening ADHD, Screening ODD/CD), Screening Internal (Screening Anxiety, Screening Depression), Screening Contact Behavior (Screening Autism plus items related to Social Anxiety, Mutism and Reactive Attachment Disorder), which all show internal consistencies of > 0.80. The 49 items can also be combined to calculate a total score for overall symptoms (α = 0.92). For parent reports, representative norms are available for girls and boys in the age ranges 4–6;11 years, 7–10;11 years, 11–13;11 years and 14–17;11 years.
The questionnaire on eating, leisure and sleeping behavior was specifically designed for this study. Thus, information on its psychometric properties is not yet available. With regard to eating habits, this questionnaire primarily records what the child usually eats and drinks at breakfast and during school break. In addition, questions are asked about snacks and beverages over the course of the day. All questions have different answer options that can be rated by parents using a four-point Likert scale from “never,” “rarely,” “frequently” to “always.” Additionally, it is requested how often the child asks for sweets on school days or weekends and how often he or she is actually allowed to eat them. Here the assessments are also made on four-point scales from “not at all,” “once,” “twice” to “three times and more” per day. The data on leisure time and sleep behavior was not analyzed in the context of this study, all related information will be presented elsewhere.
Finally, an also self-developed five-item-questionnaire for recording the type of malabsorption was used. It documented which form of malabsorption has been confirmed or excluded at the current appointment. Additionally, it asked whether a malabsorption has been diagnosed or disconfirmed at an earlier point in time and whether further test appointments are planned. It hereby assigned the subjects to the group “Fructose Malabsorption,” “Fructose and Lactose Malabsorption combined” or “Control Sample.”
A hydrogen breath test was used as diagnostic tool to confirm the presence of fructose or lactose malabsorption. In this test, after the administration of a liquid fructose or lactose concentrate adjusted to the patient’s weight, the hydrogen content of breath is measured every 30 min over a period of at least 120 min. Malabsorption is considered confirmed as far as the concentration of hydrogen rises to a critical value or significantly exceeds the baseline value (Jones et al., 2011).
The questionnaires of the study sample were completed by participants’ parents during their waiting time before and between examinations in the ambulatory gastroenterological department in following order: first, the FFB-SCREEN, then the questionnaire on eating, leisure and sleeping behavior and finally the questionnaire on type of malabsorption(s). To the caregivers of the later recruited control sample (n = 12) only the DISYPS-III FBB-SCREEN was handed out. The information sheet and the declaration of consent (including a duplicate to take home) for the study were provided for all participants on the first pages of a folder containing the questionnaire(s) to be completed. The folders of the study sample were handed out by the medical assistant to families whose child was suspected of suffering from fructose malabsorption. The folders of the later recruited control sample were given out to participating families by the investigator. The processing time of the study sample was about 30 min and that of the supplementary control sample took approximately 15 min.
Incomplete sheets of the DISYPS-III FBB-SCREEN were excluded from data analysis. Statistical analysis of this non-experimental questionnaire study was mainly performed by using SPSS 25.0 (Chicago, United States). First, data was tested for normal distribution using the Shapiro–Wilk-test. The analyses revealed that within the groups not all dependent variables could be assumed to be normally distributed. Therefore, the further inferential statistical analyses were performed non-parametrically. Post-hoc Holm-Bonferroni correction was carried out with an independent calculator to adjust the α-level (Hemmerich, 2016), as SPSS does not offer this procedure.
All scale-related data presented in the following refer to the screening scales of the DISYPS-III FBB-SCREEN, even if this is no longer explicitly stated for the sake of better readability.
Within the DISYPS-III FBB-SCREEN, stanine values higher than or equal to eight are considered as clinically relevant (Döpfner and Görtz-Dorten, 2017).
With regard to the superordinate scales a preliminary descriptive examination of the “Fructose Malabsorption” group’s data (see Table 1) showed a higher mean stanine value on the scale Internal than on the scale External which subsequently proved to be statistically significant (z = 2.85, p = 0.004, Wilcoxon-test). Further inferential statistical data analysis confirmed a significant discrepancy between symptom expression on the scale Depression and the scores on the scales Attention-Deficit/Hyperactivity Disorders ADHD (z = 2.79, p = 0.005) and Oppositional Defiant and Conduct Disorders ODD/CD (z = 2.82, p = 0.005). All other hypothesis-relevant analyses did not reveal significant median differences (all z < 1.92; all p > 0.055). In line with these results, with a mode score of eight, a value in clinically relevant range was recorded for the scale Depression. Twelve out of twenty-four (50%) participants with confirmed fructose malabsorption reached stanine scores of ≥8 on the scale Depression, respectively a clinically relevant degree of depressive symptoms.
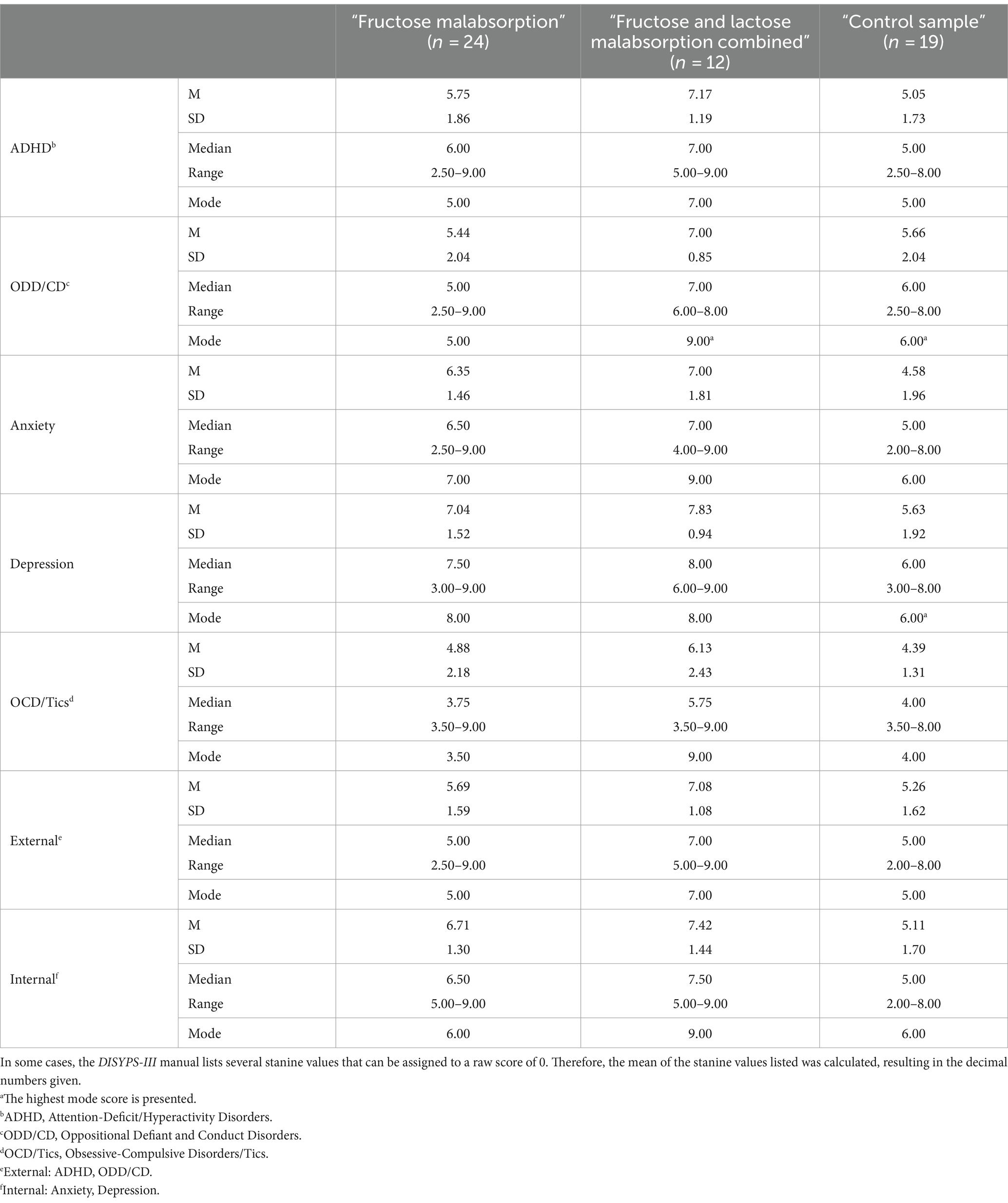
Table 1. Means (M), standard deviations (SD), medians and modes of the scales’ stanine scores for all groups in the observed scales (N = 55).
For the group “Fructose and Lactose Malabsorption combined,” descriptive statistics also showed a higher mean stanine value on the superordinate scale Internal than on the scale External (see Table 1). However, this discrepancy did not prove to be statistically significant (z = 0.92, p = 0.36). The inferential statistical analysis only confirmed a significant discrepancy between the expression on the symptom scale Depression compared to the scale ODD/CD (z = 2.49, p = 0.013, Wilcoxon-test) for the group of children and adolescents suffering from both fructose and lactose malabsorption. All other hypothesis-relevant discrepancy tests within this group did not identify significant median differences (all z < 1.71 all p > 0.088).
Considering the distribution of measurements within the group “Fructose and Lactose Malabsorption combined” according to clinically relevant modal values, it was shown that six out of twelve children achieved stanine values of ≥8 on the superordinate scale Internal. With further regard to the associated subscales eight out of twelve children (67%) showed a depression stanine score of ≥8 and five of twelve (42%) showed a stanine score of ≥8 on the scale Anxiety. On the symptom scale OCD/Tics, four out of twelve (33%) subjects reached a stanine value of ≥ 8. Although not hypothesized, it should be mentioned for completeness, that the distribution of stanines of the scale Screening ODD/CD showed that four out of twelve children (33%) reached a clinically relevant stanine value of ≥8. Overall, a striking clustering of clinically relevant scores on the hypothesis-relevant scales could be found in children and adolescents with a combination of fructose and lactose malabsorption-including the scale Obsessive-Compulsive Disorders/Tics.
Descriptive comparisons of the groups “Fructose Malabsorption” and “Control Sample” showed noticeable differences according to mean stanine scores on the superordinate scale Internal as well as on its subscales Depression and Anxiety with higher symptom severity observed in children and adolescents with fructose malabsorption. Within the control group, no modal value reached clinically relevant severity. The complete descriptive statistics of the control sample are presented in Table 1. Next, participants with a combined fructose and lactose malabsorption (n = 12) were compared to healthy controls (n = 19) by sight. Here, descriptive observation of the data showed elevated mean differences on almost all scales (see Table 1).
Non parametric Kruskal-Wallis Test for independent samples revealed significant group differences on nearly all observed scales (Attention-Deficit/Hyperactivity Disorders: p = 0.005, Oppositional Defiant and Conduct Disorders: p = 0.039, Anxiety: p = 0.002, Depression: p = 0.003; External: p = 0.007, Internal: p = <0.001), except Obsessive-Compulsive Disorders/Tics (p = 0.113).
Pairwise comparisons of symptom expression between the group of children and adolescents with fructose malabsorption and the control sample primary confirmed higher symptom expression on the superordinate scale Internal for the clinical group “Fructose Malabsorption” (see Table 2). In addition, subjects with fructose malabsorption also showed significantly higher symptom expression than participants without confirmed malabsorption on both internalizing subscales, Depression and Anxiety.
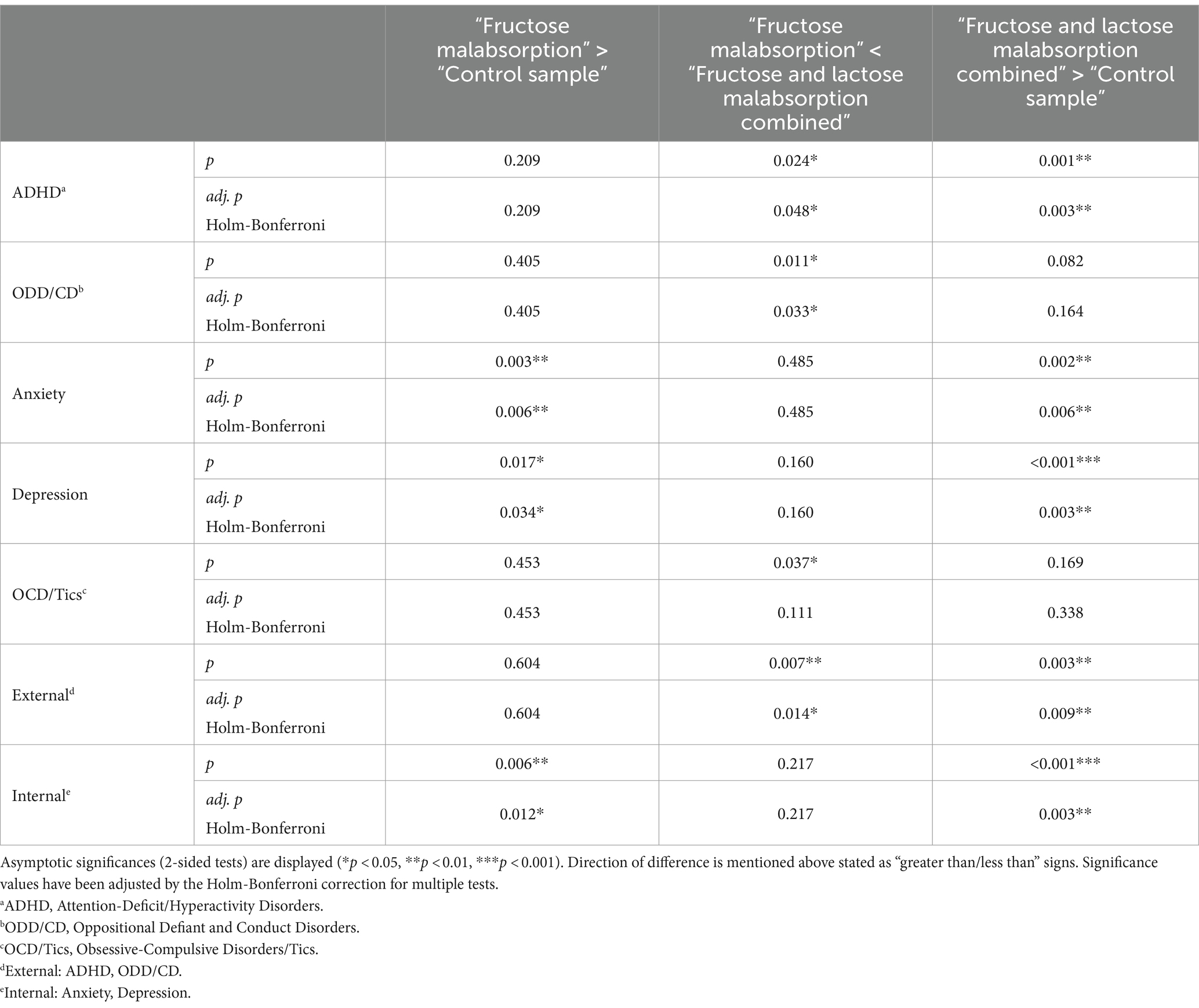
Table 2. Pairwise comparisons of symptom expression between all groups (N = 55).
With regard to the scale OCD/Tics the comparison of both groups did not yield statistical significance. The supplementary statistical comparisons of the expressions on the symptom scales Attention-Deficit/Hyperactivity Disorders and Oppositional Defiant and Conduct Disorders also determined no significant group differences.
Pairwise comparison of the group “Fructose and Lactose Malabsorption combined” and the “Control Sample” also confirmed a higher symptom expression on both the superordinate scale Internal and on its associated subscales Depression and Anxiety for the clinical group (see Table 2). Comparisons of the aforementioned groups in terms of recorded symptom severity on the scale External and on its subscale Attention-Deficit/Hyperactivity Disorders also showed significant differences with higher symptom levels for the group with combined malabsorption. The comparison of the central tendencies of the hypothesis-relevant scale OCD/Tics did not reveal significant group differences. With regard to the second External-subscale, ODD/CD, the comparison between the groups “Fructose and Lactose Malabsorption combined” and “Control Sample” did not reveal a significant difference as well.
Pairwise comparison between the clinical groups “Fructose Malabsorption” and “Fructose and Lactose Malabsorption combined” revealed a significantly higher symptom expression on the scale External as well as on its two subscales (ADHD, ODD/CD) for the group with combined malabsorption (see Table 2).
In a last set of analyses, possible relationships between eating habits and psychological symptoms were calculated via Spearman-Rho correlations (one-tailed tests). For the group “Fructose Malabsorption”, a medium-sized, positive relationship between a heightened fructose consumption and depressive symptoms was found [rs(24) = 0.35, p = 0.084]. The other correlations were rather low and insignificant [Anxiety (rs(24) = −0.176, p = 0.21); OCD/Tics (rs(24) = 0.146, p = 0.25); Internal (rs(24) = −0.071, p = 0.37)].
For the group, “Fructose and Lactose Malabsorption combined” (n = 12) a positive correlation was initially found between a heightened fructose consumption and symptom expression on the superordinate scale Internal [rs(12) = 0.560, p = 0.029]. With regard to the associated subscales, a strong positive influence of a high fructose diet on the related symptom expression could be demonstrated for the scale Anxiety [rs(12) = 0.620, p = 0.016]. Regarding the expression on the subscale Depression [rs(12) = 0.443, p = 0.074], a moderately strong but only tendentially significant correlation was found. Finally, for the group “Fructose and Lactose Malabsorption combined,” a high positive correlation between a fructose-oriented eating behavior and an increased symptom expression could be objectified on the symptom scale Obsessive-Compulsive Disorders/Tics [rs(12) = 0.527, p = 0.039].
The results of this study show that children and adolescents with an untreated fructose malabsorption frequently display internalizing psychological symptoms. For half of twenty-four patients a clinically relevant degree of depressive symptoms was recorded. In accordance with our initial hypothesis, children and adolescents with fructose malabsorption were reported higher symptom expression on the superordinate scale Internal (Depression, Anxiety Disorders) compared to the superordinate scale External (Attention-Deficit/Hyperactivity Disorders, Oppositional Defiant and Conduct Disorders). Compared to healthy controls, for children and adolescents with a currently diagnosed fructose malabsorption a higher symptom expression on the scale Internal and on its two subscales—Anxiety and Depression—was found. The presented results extend earlier results by Ledochowski et al. (1998, 2000c) and also findings by Enko et al. (2018), who mainly observed depressive symptoms in affected individuals. In accordance with Ledochowski et al. (2001) we assume that the reported internalizing psychological symptoms are likely the consequence of an impaired tryptophan absorption in affected patients, although we have not investigated this directly and thus are not able to prove it. Further research should address this assumption in more detail, although a former study by Varea et al. (2005) was not able to confirm evidence on this suggestion. Other factors that may have influenced the results should also be mentioned. For example, chronic abdominal pain as a result of carbohydrate metabolism disorder, may have an influence on the mental constitution of affected children and adolescents. Mention should also be made of a recent study where Enko et al. (2020) found a connection between Interleukin-6, tryptophan metabolism and depressive symptoms in patients with fructose malabsorption, lactose malabsorption or the combination of both. Compared to patients without signs of depression, increased serum levels of the inflammatory marker Interleukin-6 were found in patients suffering from depressive symptoms.
All this implies that further studies will be necessary to specify potential mechanisms.
After integrating all observations, it remains to be mentioned that further studies with an expanded sample size of children and adolescents with a combined fructose and lactose malabsorption also appear to be of importance. In terms of internalizing psychological symptoms within this group we only found a higher expression on the symptom scale Depression compared to Oppositional Defiant and Conduct Disorders. Nevertheless, descriptive data analyses of the group “Fructose and Lactose Malabsorption combined” revealed that for a majority (67%) of patients clinically relevant values of Depression were reported. For about half (42%) of the examined patients clinically relevant symptoms of Anxiety, and for notably one third of the sample (33%) clinically relevant symptoms of Obsessive-Compulsive Disorders/Tics were described. Additionally, the pairwise comparison of patients suffering from a combination of fructose and lactose malabsorption with healthy controls confirmed not only a higher expression of internalizing mental symptoms (scales Internal, Depression, Anxiety) but also of externalizing ones (scales External, Attention-Deficit/Hyperactivity Disorders) in the patient’s group. These observations extend previous outcomes by Varea et al. (2004, 2005) that only revealed increased depressive symptoms in children and adolescents with a combination of fructose and lactose malabsorption and may therefore lead to further studies.
Finally, for the group suffering from a combined malabsorption we were able to confirm a positive association between a fructose-rich diet and internalizing psychological symptoms. With regard to Anxiety, a strong influence of a fructose-rich diet on symptom severity was shown. For symptoms of Depression a moderate correlation was found. Relating to eating habits we finally confirmed for the group with combined malabsorption a positive correlation between a fructose-rich diet and an increased symptom expression concerning Obsessive-Compulsive Disorders/Tics. This has not been described previously and may also inspire further investigations.
The presented study has some limitations that need to be addressed. The small and unbalanced sample limits the generalizability. The use of a parent-rating questionnaire also represents sort of a restriction. Nevertheless, its use seemed necessary and reasonable to capture a broad spectrum of psychopathological irregularities without putting unnecessary strain on the participating children and adolescents. It was also regarded suitable to affirm initial suppositions to consider them more intensively at a later stage.
The obtained results suggest that children and adolescents with an untreated fructose malabsorption or a combined form of fructose and lactose malabsorption may suffer from internalizing psychological symptoms. For children and adolescents with a combined malabsorption also the presence of possible externalizing psychological symptoms cannot be excluded at the moment. In this regard a comparison of this group with the group “Fructose Malabsorption” also needs to be mentioned, where we found significantly higher levels of externalizing psychological symptoms related to the scale External and its two subscales ADHD and ODD/CD in patients with combined malabsorption.
According to our actual state of knowledge, it seems to be beneficial to record the history of psychological symptoms in the context of an initial gastroenterological investigation on suspicion of malabsorption(s). At the same time, it could also be advantageous to explore the presence of possible malabsorption(s) in the setting of initial psychological examinations. Finally—and in order to be able to offer optimal treatment options to affected children and adolescents—a close cooperation between clinicians from gastroenterology and psychology should be taken into account in the future.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study involving humans was approved by the ethics committee of the Department of Psychology and Sport Sciences, Goethe-University Frankfurt. Ethics approval number: 2017-31. The study was conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
AM: Conceptualization, Investigation, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, Data curation, Formal analysis, Methodology. AL: Investigation, Resources, Writing – review & editing, Data curation. SB: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Visualization, Writing – review & editing, Project administration.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by department resources.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Berger, M., Gray, J. A., and Roth, B. L. (2009). The expanded biology of serotonin. Annu. Rev. Med. 60, 355–366. doi: 10.1146/annurev.med.60.042307.110802
Berni Canani, R., Pezzella, V., Amoroso, A., Cozzolino, T., Di Scala, C., and Passariello, A. (2016). Diagnosing and treating intolerance to carbohydrates in children. Nutrients 8:157. doi: 10.3390/nu8030157
Deister, A. (2013). “Angst- und Panikstörungen,” in Duale Reihe - Psychiatrie, Psychosomatik und Psychotherapie. Eds. H. J. Möller, P. Falkai, G. Laux, and A. Deister (Stuttgart: Georg Thieme Verlag KG), 127–144.
Döpfner, M., and Görtz-Dorten, A. (2017). DISYPS-III. Diagnostik-System für Psychische Störungen nach ICD-10 und DSM-5 für Kinder und Jugendliche – III. Göttingen: Hogrefe.
Enko, D., Wagner, H., Kriegshäuser, G., Brandmayr, W., Halwachs-Baumann, G., Schnedl, W. J., et al. (2018). Assessment of tryptophan metabolism and signs of depression in individuals with carbohydrate malabsorption. Psychiatry Res. 262, 595–599. doi: 10.1016/j.psychres.2017.09.049
Enko, D., Zelzer, S., Wenninger, J., Holasek, S., Schnedl, W. J., Baranyi, A., et al. (2020). Interleukin-6 is associated with tryptophan metabolism and signs of depression in individuals with carbohydrate malabsorption. EXCLI J. 19, 1414–1422. doi: 10.17179/excli2020-2940
Escobar, M. A. Jr., Lustig, D., Pflugeisen, B. M., Amoroso, P. J., Sherif, D., Saeed, R., et al. (2014). Fructose intolerance/malabsorption and recurrent abdominal pain in children. J. Pediatr. Gastroenterol. Nutr. 58, 498–501. doi: 10.1097/MPG.0000000000000232
Hemmerich, W. (2016). StatistikGuru: Rechner zur Adjustierung des α-Niveaus. Available at: https://statistikguru.de/rechner/adjustierung-des-alphaniveaus.html (Accessed June 08, 2024).
Huether, G., Schmidt, S., and Rüther, E. (1998). Essen, Serotonin und Psyche: Die unbewußte nutritive Manipulation von Stimmungen und Gefühlen. Dtsch. Arztebl. 95, 477–479.
Jenkins, T. A., Nguyen, J. C. D., Polglaze, K. E., and Bertrand, P. P. (2016). Influence of tryptophan and serotonin on mood and cognition with a possible role of the gut-brain Axis. Nutrients 8:56. doi: 10.3390/nu8010056
Jones, H. F., Butler, R. N., and Brooks, D. A. (2011). Intestinal fructose transport and malabsorption in humans. Am. J. Physiol. Gastrointest. Liver Physiol. 300, G202–G206. doi: 10.1152/ajpgi.00457.2010
Kis, B., Gastpar, E., and Davids, E. (2007). Neurobiologie der Zwangsstörung. J. Neurol. Neurochir. Psychiatr. 8, 15–20.
Kretschmer, Ch. (2022). Intestinale Fructoseintoleranz. Available at: https://www.gelbe-liste.de/krankheiten/intestinale-fructoseintoleranz#Diagnostik (Accessed June 10, 2024).
Latulippe, M. E., and Skoog, S. M. (2011). Fructose malabsorption and intolerance: effects of fructose with and without simultaneous glucose ingestion. Crit. Rev. Food Sci. Nutr. 51, 583–592. doi: 10.1080/10408398.2011.566646
Ledochowski, M., Sperner-Unterweger, B., Widner, B., and Fuchs, D. (1998). Fructose malabsorption is associated with early signs of mental depression. Eur. J. Med. Res. 3, 295–298
Ledochowski, M., Widner, B., Bair, H., Probst, T., and Fuchs, D. (2000a). Fructose- and sorbitol-reduced diet improves mood and gastrointestinal disturbances in fructose malabsorbers. Scand. J. Gastroenterol. 35, 1048–1052. doi: 10.1080/003655200451162
Ledochowski, M., Widner, B., and Fuchs, D. (2000b). Fruktosemalabsorption. J. Ernährungsmed. 2, 10–14.
Ledochowski, M., Widner, B., Murr, C., Sperner-Unterweger, B., and Fuchs, D. (2001). Fructose malabsorption is associated with decreased plasma tryptophan. Scand. J. Gastroenterol. 36, 367–371. doi: 10.1080/003655201300051135
Ledochowski, M., Widner, B., Sperner-Unterweger, B., Propst, T., Vogel, W., and Fuchs, D. (2000c). Carbohydrate malabsorption syndromes and early signs of mental depression in females. Dig. Dis. Sci. 45, 1255–1259. doi: 10.1023/A:1005527230346
Litschauer-Poursadrollah, M., El-Sayad, S., Wantke, F., Fellinger, C., and Jarisch, R. (2012). Bauchschmerzen, Blähbauch, Diarrhoe: Fruktosemalabsorption, Laktoseintoleranz oder Reizdarmsyndrom? Wien. Med. Wochenschr. 162, 506–512. doi: 10.1007/s10354-012-0158-0
Mehler-Wex, C., and Kölch, M. (2008). Depressive Störungen im Kindes- und Jugendalter. Dtsch. Arztebl. 105, 149–155. doi: 10.3238/arztebl.2008.0149
Steeves, T. D., and Fox, S. H. (2008). Neurobiological basis of serotonin-dopamine antagonists in the treatment of Gilles de la Tourette syndrome. Prog. Brain Res. 172, 495–513. doi: 10.1016/S0079-6123(08)00924-2
Varea, V., de Carpi, J. M., Puig, C., Alda, J. A., Camacho, E., Ormazabal, A., et al. (2005). Malabsorption of carbohydrates and depression in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 40, 561–565. doi: 10.1097/01.MPG.0000153005.61234.28
Varea, V., Martin de Carpi, J., Puig, C., Alda, J., Vilaseca, M., Artuch, R., et al. (2004). Lactose and fructose malabsorption and depression in pediatric patients. J. Pediatr. Gastroenterol. Nutr. 39, S381–S382. doi: 10.1097/00005176-200406001-00977
Keywords: fructose malabsorption, tryptophan, serotonin, depression, anxiety, children, adolescents
Citation: Maurer A, Lieb A and Bongard S (2024) Internalizing psychological symptoms in children and adolescents with fructose malabsorption. Front. Psychol. 15:1414852. doi: 10.3389/fpsyg.2024.1414852
Edited by:
Magdalena Sowa-Kućma, College of Medical Sciences, PolandReviewed by:
Joanna Rog, Warsaw University of Life Sciences, PolandCopyright © 2024 Maurer, Lieb and Bongard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Annabel Maurer, YW5uYWJlbC5tYXVyZXJAZmlwc3ktc3R1ZGllLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.