
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 15 March 2024
Sec. Personality and Social Psychology
Volume 15 - 2024 | https://doi.org/10.3389/fpsyg.2024.1350133
 Fatemeh Shahri1
Fatemeh Shahri1 Abbas Zabihzadeh1*Alireza Taqipanahi2Morteza Erfani Haromi2Mobina Rasouli1†Asal Saeidi Nik1†
Abbas Zabihzadeh1*Alireza Taqipanahi2Morteza Erfani Haromi2Mobina Rasouli1†Asal Saeidi Nik1† Clare M. Eddy3*
Clare M. Eddy3*Introduction: While the relationship between narcissism and empathy has been well-researched, studies have paid less attention to empathic accuracy, i.e., appreciating the precise strength of another person’s emotions, and self-other distinction, in terms of the disparity between affective ratings for self and other in response to emotive stimuli. Furthermore, empathic responses may vary depending on whether the pain is physical or social.
Methods: We investigated empathic accuracy, affective empathy, and the distinction between pain, emotion and intensity ratings for self and other, in high (n = 44) and low (n = 43) narcissism groups (HNG and LNG, respectively) selected from 611 students, in response to both types of pain. Participants watched six videos where targets expressed genuine experiences of physical and social pain, and rated the perceived affect and pain experienced by the person in the video and their own empathic emotional responses.
Results and discussion: The HNG displayed lower affective empathy and empathic accuracy than the LNG for both pain types. Within the HNG there was higher empathic accuracy for social vs. physical pain, despite reduced affective empathy for social pain, in contrast to the LNG. In addition to this paradox, the HNG demonstrated greater differences between ratings for the self and for target others than the LNG, suggesting that narcissism is associated with higher self-other distinction in response to viewing other people describing social pain.
Narcissism is a dark personality trait (Smith et al., 2018), and its clinical manifestation, narcissistic personality disorder, is characterized by behavioral and thinking patterns including entitlement, a sense of superiority and uniqueness, excessive need for admiration, self-centeredness, and altered empathy (Bukowski and Samson, 2021; Eddy, 2021; Gruda et al., 2021). People with narcissistic traits have a hard time maintaining relationships (Back et al., 2013; Hart et al., 2018). Even though they may seem attractive to potential partners (Back et al., 2010), incompatible characteristics such as the strong desire for power and revenge (Wilson et al., 2017), betrayal and lack of commitment (Wurst et al., 2017), unwillingness to apologize (Leunissen et al., 2017), aggression (Hyatt et al., 2019), and a tendency to objectify others (Lachowicz-Tabaczek et al., 2021) can become apparent over time, leading to interpersonal difficulties (Campbell and Campbell, 2009). Despite ongoing debates regarding the definition and concept of trait narcissism (Miller et al., 2017), there is a consensus among researchers that it encompasses multiple dimensions, each with distinct forms or aspects (Krizan and Herlache, 2018) and varying implications for human behavior and well-being (Duffner et al., 2019). A critical and increasingly recognized distinction within the field is between grandiose and vulnerable narcissism (Wink, 1991). Grandiose narcissism is generally characterized by self-centered self-exaltation (Morf and Rhodewalt, 2001), aligning closely with everyday perceptions of narcissism, whereas vulnerable narcissism is associated with feelings of insufficiency and incompetence (Miller et al., 2011). The primary focus of this study was on the grandiose subtype of narcissism.
One critical feature of the narcissistic personality structure that may contribute to interpersonal difficulties is a reduced tendency to empathize with others (Hart et al., 2018). Empathy refers to the ability to understand and share the feelings and intentions of others (Decety and Jackson, 2004) and has two components, affective and cognitive (Decety and Jackson, 2004; Shamay-Tsoory et al., 2009). Whereas affective empathy (AE) is the emotional response within an individual that mirrors the emotional state of another person (Eisenberg and Miller, 1987), cognitive empathy (CE), is the capacity to recognize and understand the emotions, thoughts, and intentions of others (Davis, 1980; Bos and Stokes, 2019). CE can be measured in terms of empathic accuracy: the ability to accurately understand another person’s thoughts and emotions (Zaki and Ochsner, 2011). This concept is often measured by comparing the emotions and thoughts an individual reports with the inference made by another person observing them (Zaki and Ochsner, 2011).
Whereas research focusing on narcissism invariably reports a decline in AE, the results are less clear when it comes to CE (e.g., Wai and Tiliopoulos, 2012; Vonk et al., 2013; Pajevic et al., 2018; Turner et al., 2019; di Giacomo et al., 2023). Jonason and Krause (2013) observed that narcissism correlates with decreased affective empathy and difficulties in emotion recognition. However, more recent studies suggest that whereas narcissism negatively impacts affective empathy, it might be positively linked with cognitive empathy (Turner et al., 2019; Doyle, 2020; Wertag et al., 2021; Duradoni et al., 2023). One contributing factor to these inconsistencies is measurement methods, which range from self-report assessments to behavioral tasks. Data from different tasks show that empathy in narcissism is not solely characterized by deficiency but can also vary due to motivational factors (Baskin-Sommers et al., 2014; Hepper et al., 2014a; Jacobs, 2022). Pajevic et al. (2018) found that despite higher self-report cognitive empathy among narcissistic individuals, this did not translate to better performance in emotion recognition tasks, which showed a nonsignificant correlation. Additionally, a meta-analysis by Urbonaviciute and Hepper (2020) indicated that grandiose aspect of narcissism correlates negatively with AE and CE based on self-report measures. Similarly, objective, performance-based measures echoed this negative trend between grandiosity and AE. However, when CE was evaluated using performance-based measures, no clear relationship was found with this subtype of narcissism.
Empathic responses have been widely studied through observing another individual’s suffering, which can be caused by either physical (Benuzzi et al., 2008; Avenanti et al., 2010) or social (Zaki et al., 2009) pain stimuli. Whereas physical pain is associated with bodily injury, social pain refers to discomfort caused by the possible or actual loss of social bonds (Eisenberger, 2011), e.g., ostracism, betrayal, or rejection (Riva et al., 2016). Social and physical pain share commonalities in terms of evolutionary function (MacDonald and Leary, 2005) and involve partial overlapping brain circuitry (DeWall et al., 2010). Furthermore, both forms of pain can elicit fear and anxiety (Riva et al., 2014a,b), and lead to comparable psychological outcomes (Riva et al., 2011, 2014a,b). Whereas several studies have explored the disparities in the perception of these two types of pain in personal experiences (Eisenberger, 2011; Brunell et al., 2021), recent research has expanded to include how observers perceive and evaluate physical vs. social pain experienced by others (Riva and Andrighetto, 2012; Riva et al., 2014a,b, 2016; Atkins et al., 2016) as well as their empathetic responses to these types of pain (Flasbeck et al., 2017). In relation to the observation of pain experienced by others, understanding can be influenced by multiple factors, including racial differences (Avenanti et al., 2010; Riva and Andrighetto, 2012), gender (Riva et al., 2011), moral judgments (Riva et al., 2016), cultural background (Atkins et al., 2016), and the personality of both the observer and the person experiencing pain (Flasbeck et al., 2017). Given the inevitable nature of social pain within interpersonal relationships and its more lasting impact compared to physical pain (Chen et al., 2008), it is crucial to examine the differences in how individuals with grandiose narcissism respond to both physical and social pain stimuli. These people might suppress negative emotions related to social pain as a strategy to avoid feelings of failure, which are more prevalent in social contexts, thus experiencing this type of pain less intensely (Brunell et al., 2021). The current study explored empathic reactions toward the social and physical pain of others among individuals with grandiose narcissistic traits, given that grandiose narcissism might differentially influence the ability to recognize, accurately evaluate, and empathize with the physical and social pain experienced by others, suggesting that their diminished empathetic responses are notably more evident when confronting the social pain of others rather than physical pain.
The experience of empathy toward another’s pain appears to provoke neural responses similar to those we undergo when feeling pain personally (Singer et al., 2004; Riečanský et al., 2020), suggesting that we employ our own emotional systems to interpret and empathize with what another individual is experiencing and feeling. This is closely tied to the concept known as self-other distinction, i.e., our ability to differentiate between our own mental and physical states and those of others. Self-other distinction describes an intraindividual concept or experience, but it is likely to be closely linked to empathy and social behavior. Therefore while self-other distinction may be applied to different domains (e.g., motor, cognitive, and emotional: see Eddy, 2022), measuring self-other distinction may appear to overlap with affective empathy, when applied to emotional experience. For example, when self-other distinction within an individual is less pronounced, it may facilitate greater affective empathy or manifest as greater resonance with the emotion of another, such as experiencing personal distress in response to another person’s distress (e.g., Eddy, 2022). Intact CE in the context of lower AE, and many characteristics associated with narcissism, such as socially competitive emotions, seem to imply higher self-other distinction in highly narcissistic individuals (Eddy, 2022). However, self-other distinction may vary according to the subtype of narcissism, as one study (De Panfilis et al., 2019) found high personal distress (which may indicate low self-other distinction) in individuals with narcissistic traits who experience rejection sensitivity (suggestive of vulnerable narcissism) Consequently, the current study explored self-other distinction in individuals with more grandiose narcissistic traits, aiming to deepen our understanding of how this construct varies across narcissism subtypes.
Previous research exploring pain and empathy in those with narcissistic traits has not distinguished between physical and social pain. However, Brunell et al. (2021) explored the self-experience of these two types of pain in individuals with narcissism. Their research revealed that although grandiose narcissism is not directly associated with the sensation of physical pain, it is linked to a negative emotional response when experiencing it. Conversely, grandiose narcissistic individuals reported minimal impact in response to social pain and remained focused on cognitive tasks. This pattern of behavior arises from their tendency to place the blame for social discomfort on others, justifying their own innocence by adopting an “it’s them, not me” attitude (Brunell et al., 2021). Whereas this attitude cannot alleviate the sensation of physical pain, it plays a crucial role in diminishing the experience of social pain. Therefore, this difference in processing their own social pain relative to physical pain may reflect differential empathic responses to the social and physical pain of others. Based on these observations, the current study aimed to explore both empathy for physical and social pain in narcissism, and we expected that individuals with high levels of grandiose narcissism would exhibit lower affective empathy in response to social pain when compared to physical pain.
Given that self-report methods largely gauge motivation to empathize rather than actual capacity (Urbonaviciute and Hepper, 2020), we chose a video-task to assess empathy behaviorally. This approach provides a more ecologically valid measure of narcissists’ empathic behavior, which may be a better predictor of actual interpersonal skills. Due to the connection between affective empathy and self-other distinction (i.e., greater affective empathy may imply lower self-other distinction), and the possible tendency of individuals with grandiose narcissism to distance themselves to avoid engagement with others’ emotions (thereby lacking affective empathy), we were motivated to draw upon these experimental measures in order to explore self-other distinction. We expected that individuals with higher levels of grandiose narcissism would exhibit lower affective empathy, and greater self-other distinction (Eddy, 2022) than less narcissistic individuals. Taking our two hypotheses together, we also expected that the difference in self-other distinction between individuals with high versus low narcissism would be greater for social than physical pain stimuli.
The ethics committee of the Faculty of Psychology and Education of Shahid Beheshti University approved the procedure (IR.SBU.REC.1402.044). All participants gave written informed consent. The study involved two parts: the creation of physical and social pain stimuli, and then the testing of two subgroups of participants who had been screened and sub-grouped based on level of narcissism. Firstly, volunteers (i.e., targets) from the Faculty of Psychology at Shahid Behehsti University were recruited to form the stimulus creation sample, and provided ratings of pain, affect, and intensity for comparison to participants. To ensure targets were not familiar to participants who rated the videos, those participants were recruited from a separate student sample, divided into high and low narcissism groups, from other faculties at the University. Participants were paid to take part in the 40 min procedure, which included rating the degree of pain and affect experienced by the target and themselves in response to the video. They also completed measures to assess baseline emotional state, mental and physical health, and self-report empathy, described below.
The pool used to create high and low narcissism groups consisted of 611 students (337 females; Mage = 22.4, SD = 4.6). We used the Persian version (Mohammadzadeh, 2009) of the Narcissistic Personality Inventory-16 (NPI-16; Ames et al., 2006) to evaluate subclinical narcissism. The total score ranges from 0 to 16 and is positively associated with narcissism, focusing on more grandiose traits. There are no categories or cut-off points on the scale (Raskin and Hall, 1981; Raskin and Terry, 1988). The average NPI-16 score in the testing pool was 6.08 (SD = 3.08). The cut-off was mean + 1SD for the high narcissism group (“HNG”; N = 79, 32 females; Mage = 21.76, SD = 3.54; MNPI-16 = 11.23, SD = 1.39, Range = 10–16), and mean-1SD for the low narcissism group (“LNG”; N = 71, 48 females; Mage = 23.25, SD = 5.87; MNPI-16 = 1.51, SD = 0.65, Range = 0–2). Prior to the study, we determined to gather data from at least 100 participants—50 participants per group, using an established rule of thumb (see Nelson et al., 2018). From these two groups, 49 participants from the LNG and 50 from the HNG agreed to participate in the study. Participants who met any of the following criteria were excluded: current diagnosis of a psychiatric or neurological disorder, experiencing any physical or social pain at the time of assessment, taking medications that affect autonomic arousal or pain experience (e.g., mood stabilizers, analgesics), and exhibiting severe clinical levels of depression, anxiety, and stress, as assessed by the Depression and anxiety stress scale 21 (DASS-21) questionnaire (Lovibond and Lovibond, 1995). In total, 12 participants were excluded based on these criteria (two due to recent relationship breakdown, two due to medication usage, one diagnosed with bipolar disorder, four for depression, two for anxiety, and one for stress), resulting in a final sample of 87 participants, with 44 (15 females; Mage = 21.6, SD = 3.6; MNPI-16 = 11.27, SD = 1.59, Range = 10–16) classified as highly narcissistic and 43 (30 females, Mage = 21.7, SD = 4.1; MeanNPI-16 = 1.55, SD = 0.7, Range = 0–2) as low narcissistic. Following these exclusions, we confirmed that no extreme outliers were present in our data. Our sample scores were found to be consistent with previous studies (e.g., Casale et al., 2016; Aytaç and Akın, 2021) and all participants in the HNG scored above the previously suggested cut-off score (8) likely to indicate Narcissistic Personality Disorder (Vaziri-Harami et al., 2021). Sensitivity analyses using G*Power Version 3.1.9 (Faul et al., 2009) indicated our sample size to be sufficiently powered at 80% for detecting medium-sized within-between subject effects in analysis of variance (ANOVA) models (Cohen’s f = 0.15).
To create physical and social pain stimuli, we followed the protocol used by other researchers (Zaki et al., 2009; Atkins et al., 2016; Jospe et al., 2020). We invited 16 volunteers (nine females; Mage = 22.62, SD = 1.78) from the stimulus creation sample to the lab. We filmed them while they explained a physically or socially painful experience. Some who had experienced both types of pain were filmed twice (for physical pain, and social pain). These targets first completed the 16-item Berkeley Expressivity Questionnaire (BEQ; see Gross et al., 2000), which measures how much individuals believe their emotions are visible to others (e.g., “Whenever I feel negative emotions, people can easily see exactly what I am feeling”). This ensured uniformed expressivity across individuals explaining both social and physical pain stimuli. Following that, they were settled in a quiet room where they spent around 5 min reflecting on the pain they had experienced. To facilitate better memory retrieval, we asked them to give each story a title and write a short description of the incident. After that, we positioned the camera in front of them to capture their upper body. Once ready, we left the room, and they began describing their personal experience of pain in front of the camera, sharing their feelings and reflections for approximately 2–3 min. Immediately after the recording, targets watched their videos and rated the intensity (1 = not intense at all to 9 = extremely intense) and affective valence (1 = extremely negative to 9 = extremely positive) of the actual recall experience in the video, which were later used for video selection. They also completed the short form of Rejected Emotion Scale (Buckley et al., 2004), using a nine-point Likert scale ranging from (1 = not at all to 9 = extremely). They indicated the extent of pain and sadness, hurt feelings, anxiety, happiness, and anger experienced while recalling the physically or socially painful event. Targets were explicitly instructed to evaluate the affect they experienced while describing the pain rather than during the actual event or when watching the video replay (Jospe et al., 2020). They provided informed consent before the recording and again after recording to permit the use of their video in research.
A total of 26 videos were recorded involving 16 targets. Half captured physical pain experiences, and the other half social pain. The selection of videos for the current study was based on the following criteria; one video was selected from each target, and four videos were excluded for being shorter than 2–3 min. The resulting 12 videos included six for each type of pain. Next, ratings given by the targets were used to balance intensity and valence for each category, leaving 10 videos. The final selection of six videos was made to further ensure consistent video topic and ease of comprehension (Atkins et al., 2016). The social pain videos described losing a loving father, being ignored by a best friend, and being lonely. The physical pain stimulus videos described sustaining a cruciate ligament injury, a toe injury, and accidentally cutting fingers with a grate. Each video underwent editing in Adobe Premiere 6 software to remove background noise, standardize frame sizes, and incorporate the same opening sequence between them (see Table 1).
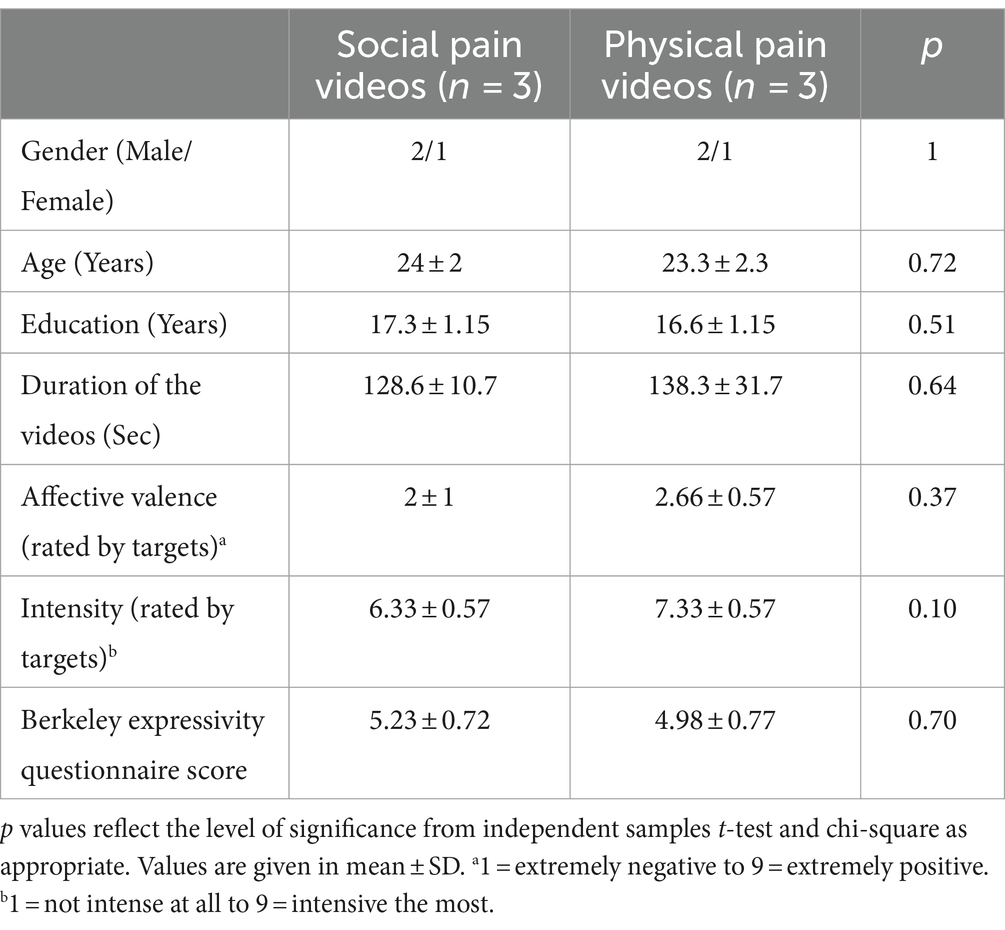
Table 1. Demographic variables and self-report measure scores for selected video stimulus.
All study participants from the LNG and HNG observed and rated the pain videos at the Psychology lab after completing the Positive and Negative Affect Schedule (PANAS; Watson et al., 1988) to establish parity of baseline emotional state across the groups. Next, they watched the six videos individually, in random order (using Psychopy 2020.2.4 software; Peirce et al., 2019), before rating the pain and intensity of each emotion the target in the video was feeling, using the same items and scales (i.e., for pain and specific emotions) as targets, in order to assess empathic accuracy (emotion and pain attribution). They provided self-ratings of their degree of pain (empathic pain) and concern (empathic concern) they felt toward the person in the video, as well as their own feelings (specific emotions: sadness; hurt; anxiety; happiness; and anger) and level of arousal (empathic arousal), to measure explicit and implicit affective empathy, respectively (see Dziobek et al., 2008; Figure 1). Participants also completed the Interpersonal Reactivity Index (IRI; Davis, 1980) to provide a general assessment of self-reported trait empathy.
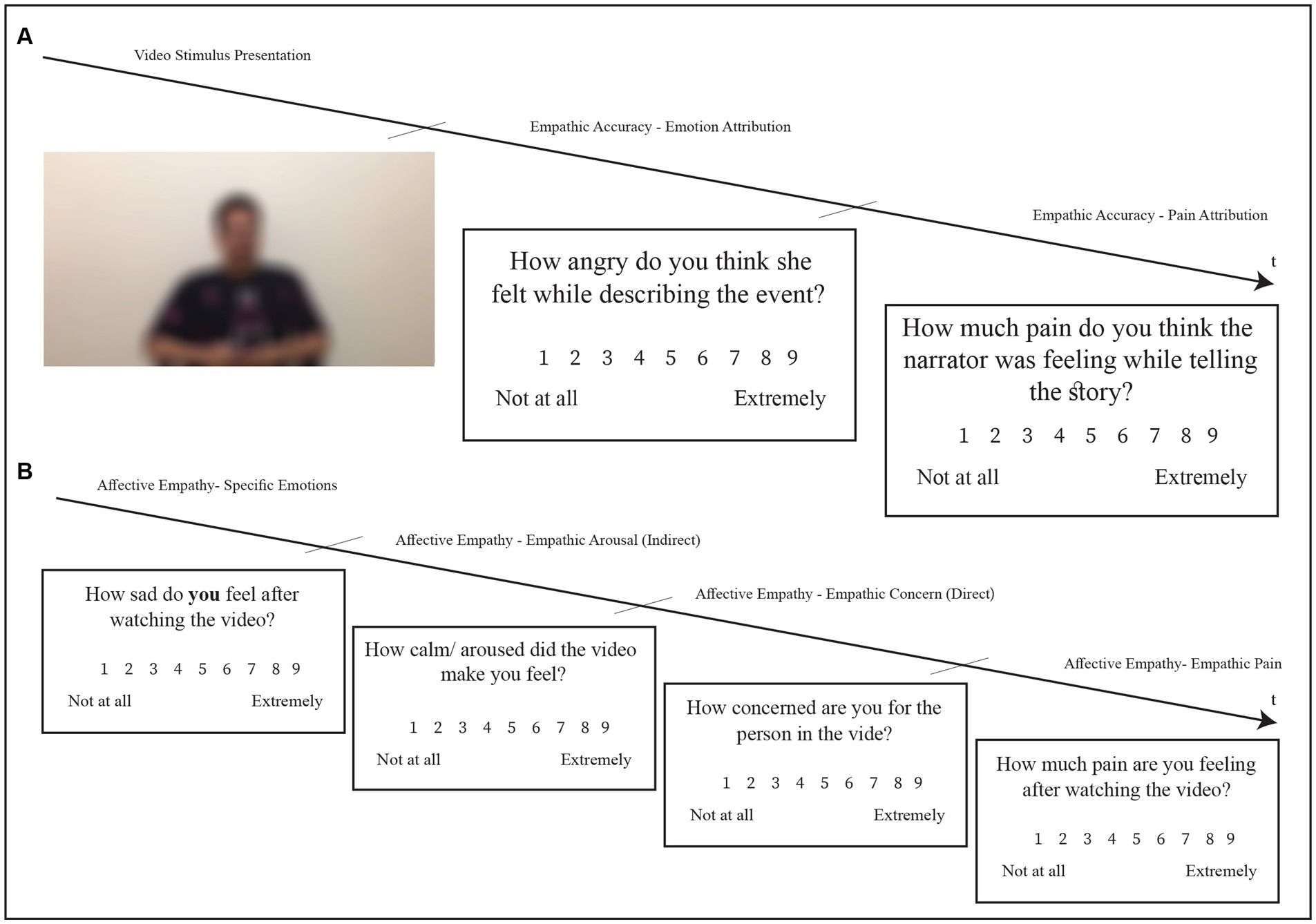
Figure 1. Rating process for each video completed by participants in high narcissism group (HNG) and low narcissism group (LNG). (A) Screen shots of the observers’ others-rating phase (Emotion Attribution and pain attribution). (B) Screen shots of the observers’ self-rating phase (Components of Affective Empathy).
The Positive and Negative Affect Schedule (PANAS) is a self-report measure that assesses general affect (Watson et al., 1988). Comprising 20 items, it has two subscales, each with 10 words describing positive (α = 0.88) and negative (α = 0.87) emotions. Respondents evaluate each item using a scale from 1 (“Very slightly or not at all”) to 5 (“Extremely”). The ratings from these items were averaged to generate separate positive and negative affect measures.
This self-report questionnaire assesses empathy’s cognitive and affective components as separate constructs (Davis, 1980). In this study, we utilized the Persian Version of the short form of the IRI, validated by Golbabaei et al. (2023). The scale consists of four subscales, each containing four items: Empathic Concern (α = 0.67) and Personal Distress (α = 0.71) measure affective empathy, whereas Perspective Taking (α = 0.67) and Fantasy (α = 0.69) assess cognitive empathy.
The DASS-21 is self-report and contains three subscales, each with seven items: depression (α = 0.81), anxiety (α = 0.73), and stress (α = 0.81) (Lovibond and Lovibond, 1995). Participants were asked to rate these items on a four-point scale, ranging from 0 (“did not apply to me at all”) to 3 (“applied to me very much, or most of the time”). Scores for each component were calculated by summing the responses for individual items within each subscale. In this study, participants in both groups were excluded if their scores exceeded the normal range, defined as >14 for depression, >12 for anxiety, and > 17 for stress. The normal range values for the subscales were determined based on the Iranian version of the DASS-21, validated by Sahebi et al. (2005).
We used a similar procedure to Jospe et al. (2020) to compute empathic accuracy scores. Firstly, distance was calculated between the participant’s ratings for the target and the target’s self-ratings for each of the five emotions on a nine-point scale (1–9). Scores were subtracted then reverse scored, e.g., a difference of 8 was scored 0; a difference of 0 was scored 8. Therefore, the range of possible distance scores extended from 0 to 40. Secondly, recognition score was assigned if the presence or absence of a specific emotion was accurately identified. Thus, if the participant gave a rating of 1 for a particular emotion (they believed the emotion was not present), and the target rated it 2 or higher (it was present), the participant would gain a 0, indicating they did not correctly identify the presence of the emotion. If they provided a rating of 2 or more, they would receive a score of 1, demonstrating successful emotion recognition. The same rule was applied when the target emotion was absent. The score of this measure was the proportion of correct recognition out of all 5 emotions, so the highest score would be 5/5 (1), representing perfect recognition, whereas the lowest score is 0/5 (0), indicating no correct recognition. The overall score for empathic accuracy was obtained by multiplying the distance score by the recognition score.
Demographic variables (gender, age, and year of study), trait empathy (IRI-16), and general affect (PANAS) were compared for the high and low narcissism groups using independent samples t-tests and chi-square. To examine whether the HNG and LNG differed in terms of empathic accuracy (measured by emotion attribution and pain attribution), affective empathy (measured by specific emotions, empathic concern, empathic arousal, and empathic pain), and self-other distinction in response to watching social pain and physical pain videos, we conducted a series of 2 × 2 repeated measures ANOVA with each outcome measure as dependent variables, trait narcissism group (high vs. low) as the between-subjects variable, and pain type (physical vs. social) as the within-subjects variable (see Table 2 for descriptive statistics).
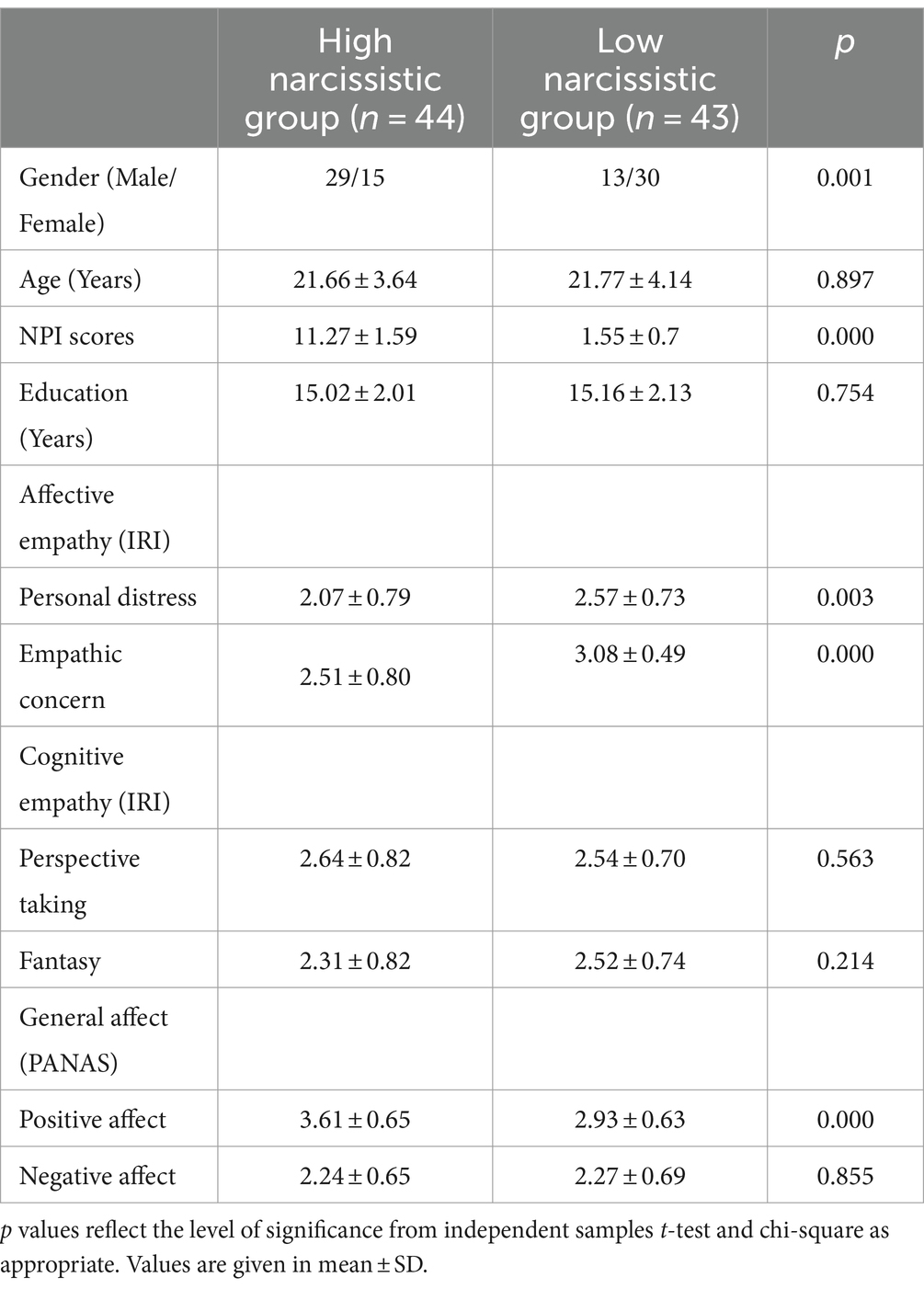
Table 2. Demographic variables and self-report measure scores for HNG (n = 43) and LNG (n = 43).
Comparisons specifically relevant to self-other distinction included within participant (1) differences between attributions of pain and emotions to the target vs. ratings of self-emotions and pain in response to the videos; and (2) the difference between the targets’ ratings of their pain/emotions/intensity during recording compared to the pain/emotion/arousal felt by observers (i.e., pain/emotional/intensity resonance), with more similar ratings for participant and target suggesting lower self-other distinction. Therefore, whereas our assessment of self-other distinction relied upon the same tasks used to assess affective empathy and empathic accuracy, this construct was explored in a distinct way by using specific within participant comparisons between numerous ratings for the self vs. the other. This first measure (1, above) was the primary measure of self-other distinction because it involved within-participant ratings. The resonance measures (2, above) are more similar to affective empathy and empathic accuracy as they compare ratings between targets and participants, but they are calculated differently to those measures. We would expect these latter measures to be closely tied to the within-participant rating of self-other distinction given that, e.g., feelings of greater separation from the other should be more likely when there is lower resonance with the other’s perceived state. However, they less directly reflect the current conceptualization of self-other distinction as an intra-individual construct.
Bonferroni correction was used to compare groups in terms of the mean estimated in empathic responses toward physical and social pain in post hoc tests with corrected p values. Instances of non-sphericity in Mauchly’s Test, we used Greenhouse–Geisser corrected p values. Statistical analyses were done in SPSS-26. For all tests, a significance level of p < 0.05 was chosen.
T-tests indicated no differences between groups in age, t(85) = 0.13, p = 0.897, 95% CI [−1.554, 1.770] and education t(85) = 0.314, p = 0.754, 95% CI [− 0.746, 1.026]. Nevertheless, according to the chi-square test, significant gender differences were found between the HNG and LGN. Descriptive statistics are shown in Table 2.
The HNG scored significantly lower than the LNG on the Empathic Concern, t(85) = 4.017, p < 0.001, 95% CI [0.29085, 0.86084] and Personal Distress, t(85) = 3.077, p = 0.003, 95% CI [0.17754, 0.82589] subscales of the IRI.
T-tests indicated no between-group differences for perspective-taking, t(85) = − 0.581, p = 0.563, 95% CI [− 0.42239, 0.23133] or Fantasy t(85) = 1.252, p = 0.214, 95% CI [− 0.12430, 0.54581] subscales of the IRI.
There were no differences between the HGN and LGN in negative affect, t(85) = 0.184, p = 0.855, 95% CI [− 0.26132, 0.31449]. However, the two groups significantly differed in the positive affect with higher scores in the HNG, t(85) = −4.925, p < 0.001, 95% CI [− 0.95925, − 0.40745].
Narcissism had a significant main effect, F(1, 85) = 4.2, p = 0.043, ηp2 = 0.047, such that individuals in the LNG were significantly more empathically accurate compared to those in the HNG in both pain types. Furthermore, a significant main effect of pain type was found, F(1, 85) = 6.12, p = 0.015, ηp2 = 0.067, indicating that participants in both groups had higher empathic accuracy for social pain videos than physical pain ones. The group × pain type interaction was insignificant, F (1, 85) = 0.165, p = 0.686 (see Table 3 for descriptive statistics).
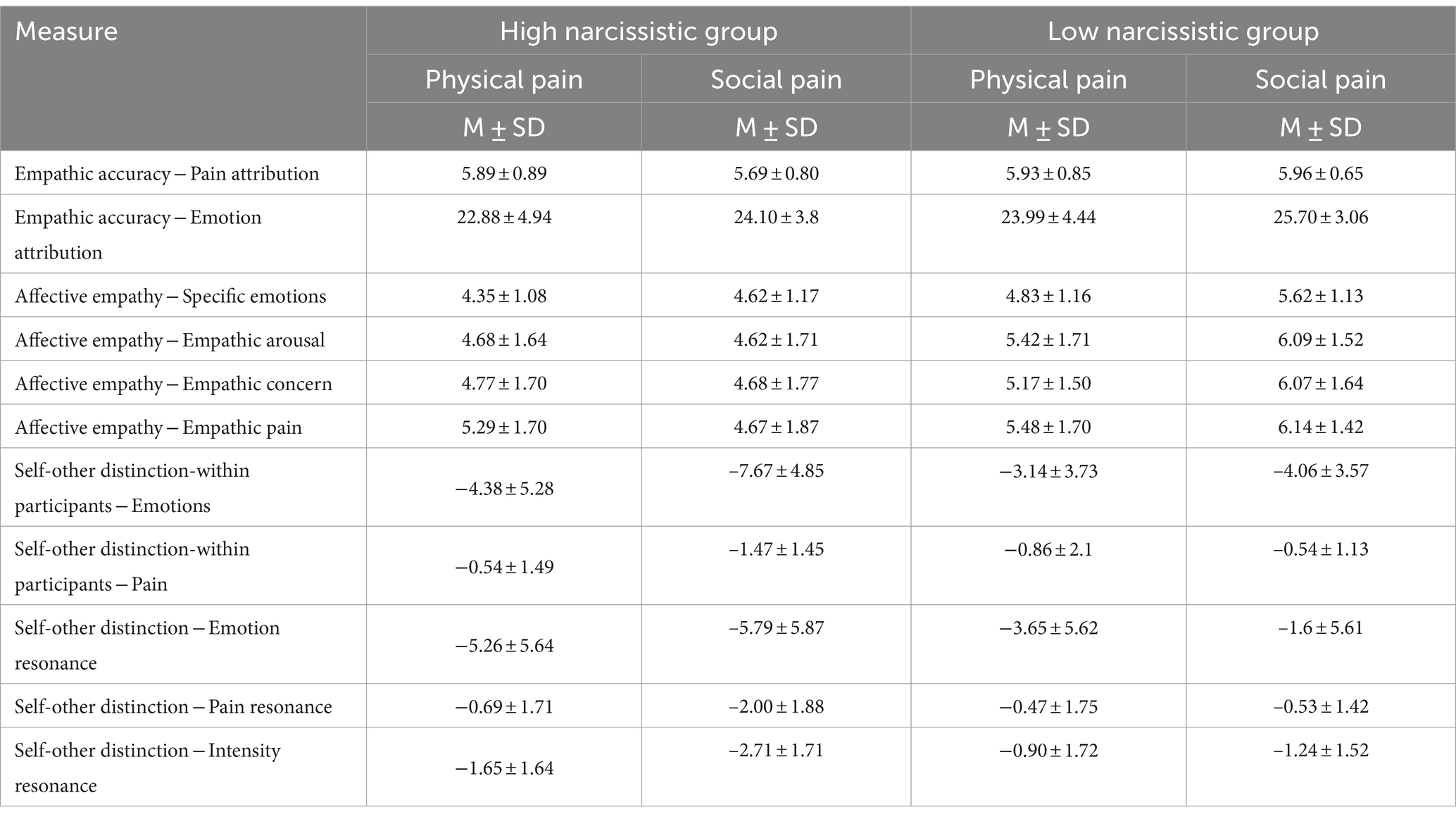
Table 3. Mean (SD) scores for component of empathic accuracy, affective empathy, and self-other distinction in response to physical and social pain separately for HNG and LNG.
There was no significant main effect of narcissism on pain ratings, F (1, 85) = 1.35, p = 0.248. Additionally, there was no significant effect of pain type, F (1, 85) = 0.615, p = 0.435. The interaction effect between narcissism level x pain type was also insignificant, F (1, 85) = 1.134, p = 0.29, suggesting that both groups perceived pain at comparable levels for each type of pain.
There was a significant main effect of narcissism, F(1, 85) = 11.58, p = 0.001, ηp2 = 0.12, demonstrating that participants in the LNG had higher levels of affective empathy. There was also a significant main effect of pain type, F(1, 85) = 23.85, p < 0.001, ηp2 = 0.219, i.e., both groups showed greater affective empathy toward social vs. physical pain videos. Additionally, pain type × group interaction effect was significant, with a group difference more apparent for social pain F(1, 85) = 5.8, p = 0.018, ηp2 = 0.064.
The HNG scored significantly lower in the arousal component of affective empathy, F (1, 85) = 13.93, p < 0.001, ηp2 = 0.141 for both pain types. However, the main effect of pain type was not significant F(1, 85) = 2.46, p = 0.121 and the interaction between the pain type x group was insignificant, F(1, 85) = 3.54, p = 0.063.
When asked about the person in the video, the LNG had significantly higher levels of empathic concern compared to the HNG, F(1, 85) = 9.75, p = 0.002, ηp2 = 0.103 in response to both types of pain. Furthermore, there was a significant main effect of pain type, F(1, 85) = 3.8, p = 0.054, ηp2 = 0.043, suggesting that participants in both groups reported greater empathic concern toward social pain than physical pain. The interaction of pain type × group was significant, with a group difference only apparent for social pain F(1, 85) = 5.68, p = 0.019, ηp2 = 0.063.
The HNG experienced significantly lower levels of pain than the LNG in response to both physical and social pain videos F(1, 85) = 7.62, p = 0.007, ηp2 = 0.082. In contrast, the main effect of pain type was insignificant within each group, F(1, 85) = 0.009, p = 0.926. Additionally, the pain type × group interaction was significant, with a group difference only apparent for social pain F(1, 85) = 9.98, p = 0.002, ηp2 = 0.105 (see Table 3 for descriptive statistics). Figures 2, 3 illustrate components of affective empathy and empathic accuracy in the HNG compared to the LNG in response to physical and social pain, respectively.
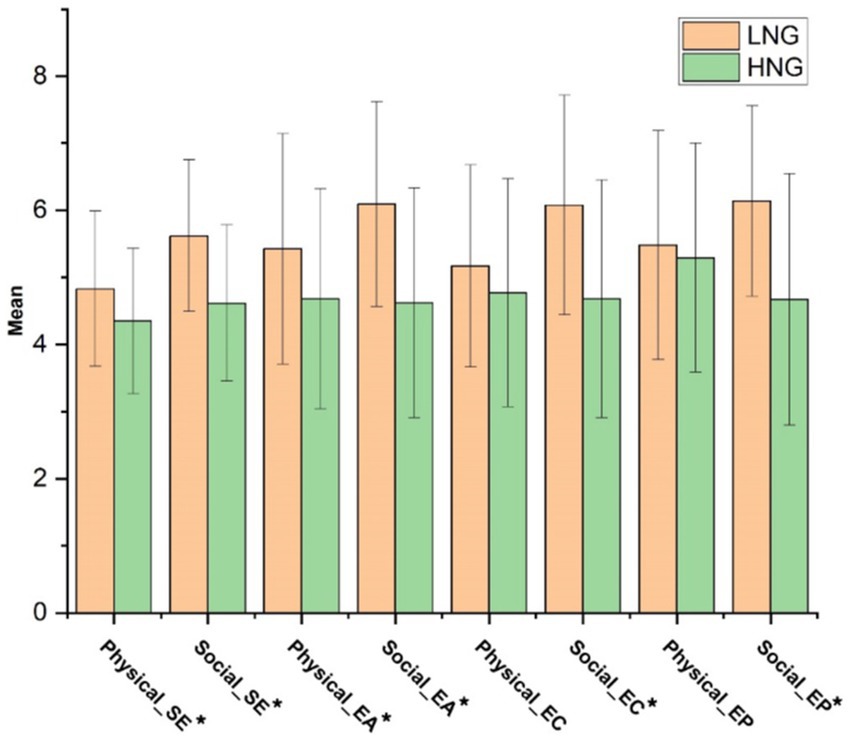
Figure 2. Mean of the components of affective empathy in two groups in response to physical and social pain. LNG, Low narcissistic group; HNG, High narcissistic group; SE, Specific emotions; EA, Empathic arousal; EC, Empathic concern; EP, Empathic pain. * indicates significant difference at p < 0.05.
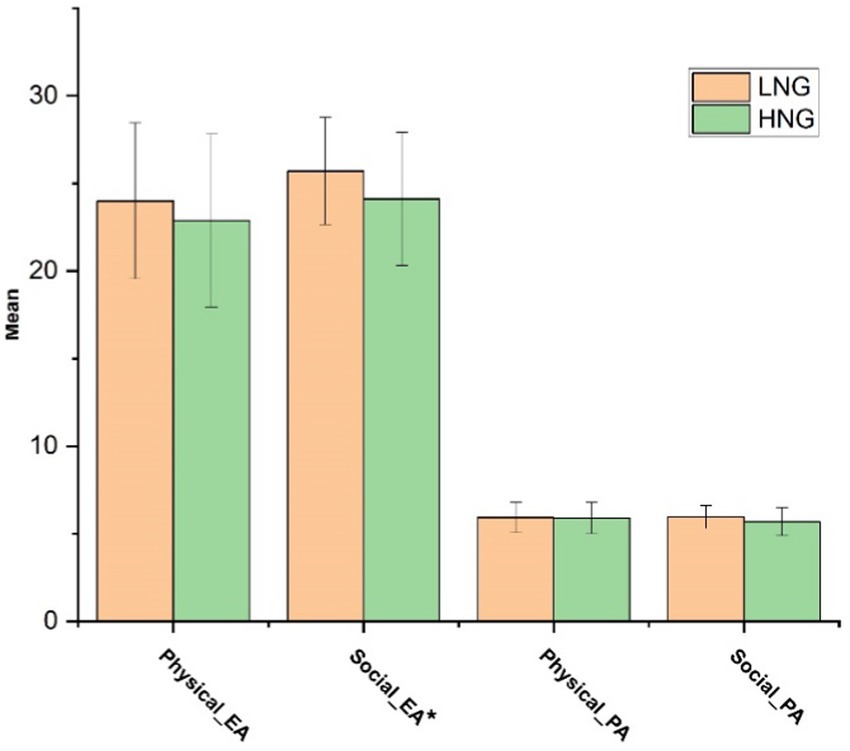
Figure 3. Mean of the components of empathic accuracy in two groups in response to physical and social pain. LNG, Low narcissistic group; HNG, High narcissistic group; EA, Emotion attribution; and PA, Pain attribution. * indicates significant difference at p < 0.05.
When comparing participants’ own emotional response to the videos, versus the emotions they rated for the target (the primary measure of self-other distinction), the HNG showed significantly greater disparity between these ratings F(1, 85) = 8.78, p = 0.004, ηp2 = 0.094. There was also a significant interaction between group and pain type, with a group difference only apparent for social pain F(1, 85) = 6.09, p = 0.016, ηp2 = 0.067. Although equivalent comparisons for pain did not reveal a significant main effect of group F(1, 85) = 1.24, p = 0.267, ηp2 = 0.014, and pain type F(1, 85) = 2.23, p = 0.139, ηp2 = 0.026, there was a significant interaction, with a greater disparity between ratings for the self and target for the HNG in relation to social pain videos only F(1, 85) = 9.23, p = 0.003, ηp2 = 0.098.
When comparing participants’ emotional reactions while watching the videos to the emotions targets felt when recording the videos, the LNG reported significantly greater emotion resonance with targets, F(1, 85) = 6.89, p = 0.010, ηp2 = 0.075. A significant interaction indicated a greater difference between groups for social pain only F(1, 85) = 6.12, p = 0.015, ηp2 = 0.067. Similar comparisons for pain, revealed the LNG also had significantly greater resonance with the targets in experiencing pain F(1, 85) = 7.81, p = 0.006, ηp2 = 0.084, with a significant interaction indicating a group difference only for social pain F(1, 85) = 9.5, p = 0.003, ηp2 = 0.101.
Finally, when considering participant arousal in response to videos and the target’s intensity ratings when recording the videos, the HNG again showed a significantly greater difference to targets versus the LNG F(1, 85) = 13.93, p = 0.000, ηp2 = 0.141. However the interaction between group and pain type was not significant F(1, 85) = 3.54, p = 0.063, ηp2 = 0.040 (see Table 3 for descriptive statistics).
As expected, the within-participant measure of self-other distinction was positively associated with the resonance measures, i.e., as the difference between the participants’ ratings for themselves and the target increased (primary measure) so did the difference between ratings taken from the participant and from the target (see Supplementary material 1).
In summary, both the primary measure of self-other distinction (within-participant measure) and resonance measures we expected to be closely linked to self-other distinction (between-participant comparisons) were suggestive of higher self-other distinction in the HNG for social pain. Figure 4 illustrates components of self-other distinction in the HNG compared to the LNG in response to physical and social pain, respectively.
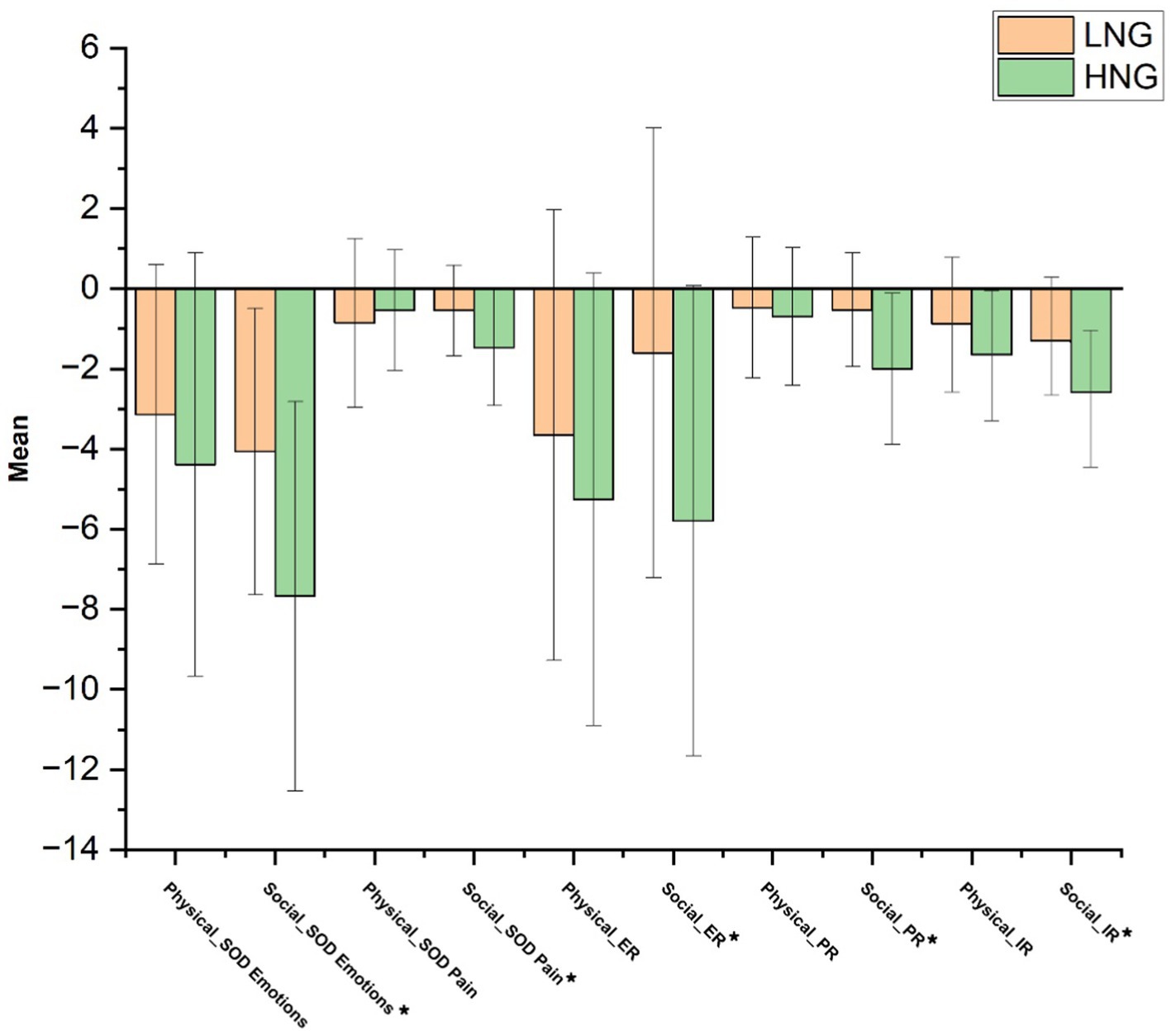
Figure 4. Mean of components related to self-other distinction for the high and low narcissism groups in response to physical and social pain. LNG, Low narcissistic group; HNG, High narcissistic group; ER, Emotional resonance; PR, Pain resonance; and IR, Intensity resonance. * indicates significant difference at p < 0.05.
Due to uneven gender distribution in our groups, we conducted further analyses with narcissism group and gender as between-subject factors, assessing their interactions across all dependent variables: subscales of empathic accuracy, affective empathy, and self-other distinction. These analyses did not reveal significant group × gender interactions, as indicated by the pairwise comparisons (see Supplementary material 2). In examining the interactions of gender x pain type, significant findings were limited to three variables: affective empathy—empathic concern [F (1, 84) = 5.95, p = 0.017, ηp2 = 0.066], and specific emotions [F(1, 84) = 3.93, p = 0.050, ηp2 = 0.045], and Self-other distinction—emotional resonance [F(1, 84) = 4.96, p = 0.029, ηp2 = 0.056], suggesting that women, overall and without considering the role of narcissism, tended to be more empathic and exhibited lower self-other distinction in response to the social pain of others. However, these interactions did not result in significant differences between genders within our groups; the significant differences were observed only across types of pain. Furthermore, the interaction of group × gender × pain type was not significant for any dependent variable. These results suggest gender does not significantly impact our primary outcomes (see Supplementary material 2).
In the current study, we used physical and social pain videos featuring targets expressing genuine emotion, in order to examine empathic accuracy, affective empathy, and differences in affective pain ratings for self and other for individuals with high and low levels of grandiose narcissism. Given our use of the NPI-16, moving forwards, our conclusions about narcissism are more likely to pertain to the grandiose subtype.
Our findings revealed that, when faced with either form of pain, individuals with high narcissistic traits displayed lower levels of affective empathy across all examined subcomponents (i.e., empathic concern, empathic arousal, empathic pain, and empathic emotions). The results remained consistent regardless of the measurement methods used, which included a video-task and the Interpersonal Reactivity Index (IRI). This finding aligns with recent studies including meta-analyses investigating the relationship between narcissism and affective empathy (Vonk et al., 2013; Chukwuorji et al., 2020; Urbonaviciute and Hepper, 2020; Eddy, 2021; Jacobs, 2022; Simard et al., 2022; di Giacomo et al., 2023).
In relation to cognitive empathy in narcissism, perhaps the picture is less clear. In our study, self-report data (IRI) revealed no difference between the high and low narcissistic groups in perspective-taking and fantasy, subcomponents of cognitive empathy. Yet, when we used the video-task method, individuals with high narcissistic traits showed a reduced ability in empathic accuracy in response to both types of pain, in terms of their attributions of degree of emotions felt by targets. This pattern is consistent with the findings of Pajevic et al., 2018, which showed a discrepancy between high self-reported cognitive empathy and actual performance in emotion recognition tasks. Such a difference could stem from a tendency among narcissists to overestimate their empathetic capabilities (Ronningstam, 2016; Bloxsom et al., 2021). Empathic accuracy (in terms of looking specifically at degree of specific emotions and pain) is an underexplored area. The current results are however consistent with Chukwuorji et al.’s (2020) finding of a negative correlation between all forms of empathy. Additionally, our study supports the idea that maladaptive aspects of narcissism, and perhaps those closely associated with grandiose narcissism, may hamper the accuracy of “mind reading” as suggested by emotion identification results (Hart et al., 2018). These disparities can be attributed not only to deficiencies but also to motivational factors in high narcissistic individuals (Baskin-Sommers et al., 2014; Hepper et al., 2014b; Lee and Kang, 2020), making it challenging to distinguish between the two.
Given the likely relationship between the ability to attribute emotions correctly to another person, and to feel and experience similar emotions in oneself, it is not unexpected to find narcissistic individuals exhibit deficits in both processes. However, when we consider measures more likely to reflect cognitive or affective empathy in the current study, we found more evidence for a significant issue with affective empathy. It is worth noting that narcissists still possess some level of empathic accuracy and what may distinguish them more clearly from people low in narcissism is their inner emotional resonance with others, or at least their self-awareness of any feelings that align with others’ emotional states.
Perceiving pain, or comprehending the level of pain another person is dealing with, was another rather novel focus of this study. Our findings suggest that people with narcissistic tendencies are adept at understanding both the physical and social pain that others experience. Essentially, it appears that whereas narcissistic individuals can correctly recognize others’ pain, they struggle to accurately attribute the degree of specific emotions linked to that pain. This may stem from the need for deeper engagement to comprehend another’s emotions rather than just their pain. The discrepancy may result from a reduced tendency to personally feel that pain and its related emotions in narcissism.
Another strength of the current study was that by measuring empathic accuracy in terms of the amount of emotions felt and perceived, we were able to calculate differences between self and other attributions. Our results showed that the HNG showed significantly greater differentiation between the pain and emotions attributed to targets in the pain videos and their own pain and emotions in response to observing those videos for social pain. This supported our initial hypothesis that more narcissistic people may show tendencies toward greater self-other distinction (Eddy, 2022). Greater self-other distinction aligns with diminished affective empathy, whereby highly narcissistic individuals may be less emotionally moved by others’ pain, and may focus more on themselves instead of empathizing with the distress of another person. This possibility is further supported by our other findings, including the lower arousal and emotional resonance in response to video targets expressing social pain, as well as lower empathic concern and personal distress in everyday life, as found in the HNG. However, because all of our measures were essentially self-report, it is not clear whether the lower ratings seen in the HNG truly reflect reduced ability to mirror the emotions of others, or whether these individuals were simply less attentive toward, accurate, or honest in relation to their affective responses to the videos. The fact that self-other distinction was only significantly greater for the HNG in relation to social pain is worthy of further exploration, but it may reflect the socially competitive nature of many narcissistic traits. High self-other distinction may characterize many social cognitive strategies used by individuals with narcissism to maintain their status and/or emotional equilibrium, and is perhaps more likely to predict low affective empathy than impairments in mentalising or cognitive empathy (Eddy, 2021, 2022).
It is notable that our findings indicated that both the HNG and LNG displayed greater empathic accuracy in response to videos depicting social pain as compared to those showing physical pain. This response reflects our shared sensitivity toward social pain, a common part of our everyday lives. Despite their accuracy in understanding others’ emotions during social pain, narcissists felt fewer empathic arousal, empathic concern, and empathic pain in these situations compared to those involving physical pain. This makes it all more interesting that self-other distinction was higher for social pain. It seems that for highly narcissistic individuals, the more adept they are at recognizing others’ social pain compared to physical pain, the less they empathize with them emotionally. This confirms our hypothesis that individuals with high narcissism traits disengaged more with the social pain of others compared to their physical pain. One explanation for this is that narcissists, despite their heightened sensitivity to social pain, suppress it more vehemently when witnessing it in others, and exhibit higher levels of self-other distinction to avoid experiencing a similar discomfort—an emotion they find highly undesirable. In other words, there is likely to be a motivational effect, e.g., a defensive mechanism intended to protect their ego. The second interpretation suggests that as grandiose narcissists remain relatively unaffected when facing social pain stimuli, often externalizing it as someone else’s problem, not theirs (Brunell et al., 2021), and so they find it challenging to empathize when others are going through such experiences. In other words, highly narcissistic individuals may either choose to detach from, or just be rather emotionally insensitive to, other’s affective states. Perhaps this may be more likely in the context of social pain as this is a more personally disturbing experience, whereas physical pain, which is a potential threat to themselves as well, draws their attention and engages them more effectively.
Understanding the social pain of others without feeling it may help to explain grandiose narcissistic characteristics such as the exploitation of others (Lamm et al., 2016; Di Pierro et al., 2018; di Giacomo et al., 2023; Duradoni et al., 2023), and the volatility often seen in narcissistic romantic relationships, where social pain as a result of rejection and abandonment (e.g., the “silent treatment”), is highly relevant, and may even be applied instrumentally by highly narcissistic individuals (Eddy, 2021).
Our study encountered certain limitations, notably our focus on the grandiose subtype of narcissism. Future research should also explore the vulnerable subtype and other conceptualizations of narcissism, such as the three-factor model (agentic extraversion, narcissistic neuroticism, and antagonism/entitlement; Simard et al., 2022), to provide a more comprehensive understanding. The second limitation pertains to the uneven distribution of gender within our sample, which can be attributed to the initial recruitment process and reflects the presence of narcissism within the sample population. Although our sample was in line with previous research suggesting that men tend to exhibit higher levels of narcissism compared to women (Grijalva et al., 2015; Chukwuorji et al., 2020), it is important to note that this imbalance in gender representation may influence the applicability of our findings to other populations. Another limitation of our study is the absence of control videos presenting neutral or positive situations, which could offer a comparison point to pain-related scenarios, similar to the methods employed by Atkins et al., 2016 and Riva et al., 2011. Our findings indicated that the baseline mood state of individuals with high narcissistic traits was more upbeat than those with low traits, aligning with previous research (Sedikides et al., 2004; Zuckerman and O'Loughlin, 2009). However, both groups displayed similar degrees of negative affect, which likely did not influence their empathic responses to others’ pain. Given that pain is typically unassociated with positive emotion and negative emotion plays a more significant role in dysfunctional interactions often linked with narcissism, this aspect was a focal point of our study. Nevertheless, it is important to acknowledge that the persistent positive mood observed in narcissistic individuals during their daily lives, introduces an uncontrollable element that could potentially influence their empathic responses in everyday situations. Therefore, exploring their responses to neutral and positive stimuli is a crucial area for future research, offering insight into the full spectrum of empathic responses in narcissistic individuals. In addition, it may be beneficial for future research to include a neutral group of referees to offer a more objective assessment of target expressivity. Studies could also explore whether self-other distinction varies according to narcissistic subtype, or mediates the association between narcissism and empathy, topics beyond the scope of our current study but which hold significant promise for advancing our understanding. Employing the validated, longer version of the Interpersonal Reactivity Index (IRI) in similar studies is also advisable. Furthermore, given that the current sample was limited to a healthy university population, future research should aim to replicate our findings in clinical samples among individuals diagnosed with Narcissistic Personality Disorder. Finally, we acknowledge that current conceptualizations of self-other distinction require refinement, and that there is no current consensus as to the best measure of this construct. Indeed, self-other distinction may be difficult to measure given that it could be intrinsically, and perhaps even differentially, linked to specific kinds of mental or physical states. An individual may say that they feel they are completely different from someone else, but at the same time, they may actually show evidence of significant resonance with another person, which may seem to suggest low self-other distinction. We hoped to help encompass this possibility by including both a within-participant measure of self-other distinction, and the resonance measures in the current study (which may be considered to represent explicit, and implicit measures of self-other distinction, respectively). At the same time, we accept the challenges associated with investigating such a complex construct, and the potential limitations associated with both intra- and inter-individual measures of self-other distinction.
In conclusion, highly narcissistic individuals can show lower affective empathy in response to observation of others’ social pain, and their attributions of the degree of emotion felt by those others may also be less accurate than the attributions made by individuals low in narcissism. We report preliminary evidence that grandiose narcissistic traits may also predict increased discrepancy between emotion ratings for self vs. other in response to observing those others’ social pain, in addition to reduced emotional resonance, personal distress and empathic concern, supporting the likelihood of higher self-other distinction in more narcissistic individuals.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://doi.org/10.6084/m9.figshare.23937063.
The studies involving humans were approved by Shahid Beheshti University (IR.SBU.REC.1402.044). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
FS: Conceptualization, Formal Analysis, Methodology, Investigation, Visualization, Writing – original draft. AZ: Conceptualization, Methodology, Supervision, Writing – review & editing. AT: Conceptualization, Methodology, Formal Analysis, Writing – review & editing. MEH: Formal Analysis, Software, Investigation, Visualization, Writing – review & editing. MR: Resources, Writing – review & editing. AS: Resources, Writing – review & editing. CE: Conceptualization, Methodology, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors wish to thank the participants in the study who contributed their time to assist our efforts to learn more about empathic capacities in narcissistic individuals.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1350133/full#supplementary-material
Supplementary Material 1: | Self-other Distinction Measures.
Supplementary Material 2: | Gender-Related Analyses.
Ames, D. R., Rose, P., and Anderson, C. P. (2006). The NPI-16 as a short measure of narcissism. J. Res. Pers. 40, 440–450. doi: 10.1016/j.jrp.2005.03.002
Atkins, D., Uskul, A. K., and Cooper, N. R. (2016). Culture shapes empathic responses to physical and social pain. Emotion 16, 587–601. doi: 10.1037/emo0000162
Avenanti, A., Sirigu, A., and Aglioti, S. M. (2010). Racial bias reduces empathic sensorimotor resonance with other-race pain. Curr. Biol. 20, 1018–1022. doi: 10.1016/j.cub.2010.03.071
Aytaç, M. B., and Akın, E. (2021). Hatzfeld syndrome: narcissistic postpurchase state of mind. Canad. J. Administr. Sci. 38, 369–381. doi: 10.1002/cjas.1597
Back, M. D., Küfner, A. C., Dufner, M., Gerlach, T. M., Rauthmann, J. F., and Denissen, J. J. (2013). Narcissistic admiration and rivalry: disentangling the bright and dark sides of narcissism. J. Pers. Soc. Psychol. 105, 1013–1037. doi: 10.1037/a0034431
Back, M. D., Schmukle, S. C., and Egloff, B. (2010). Why are narcissists so charming at first sight? Decoding the narcissism–popularity link at zero acquaintance. J. Pers. Soc. Psychol. 98, 132–145. doi: 10.1037/a0016338
Baskin-Sommers, A., Krusemark, E., and Ronningstam, E. (2014). Empathy in narcissistic personality disorder: from clinical and empirical perspectives. Personal. Disord. Theory Res. Treat. 5, 323–333. doi: 10.1037/per0000061
Benuzzi, F., Lui, F., Duzzi, D., Nichelli, P. F., and Porro, C. A. (2008). Does it look painful or disgusting? Ask your parietal and cingulate cortex. J. Neurosci. 28, 923–931. doi: 10.1523/JNEUROSCI.4012-07.2008
Bloxsom, C. A. J., Firth, J., Kibowski, F., Egan, V., Sumich, A. L., and Heym, N. (2021). Dark shadow of the self: How the dark triad and empathy impact parental and intimate adult attachment relationships in women. Forensic Science International: Mind and Law, 2, 100045. doi: 10.1016/j.fsiml.2021.100045
Bos, J., and Stokes, M. A. (2019). Cognitive empathy moderates the relationship between affective empathy and wellbeing in adolescents with autism spectrum disorder. Eur. J. Dev. Psychol. 16, 433–446. doi: 10.1080/17405629.2018.1444987
Brunell, A. B., Buelow, M. T., and Trost, Z. (2021). Narcissism and the experience of pain. Personal. Individ. Differ. 169:109852. doi: 10.1016/j.paid.2020.109852
Buckley, K. E., Winkel, R. E., and Leary, M. R. (2004). Reactions to acceptance and rejection: effects of level and sequence of relational evaluation. J. Exp. Soc. Psychol. 40, 14–28. doi: 10.1016/S0022-1031(03)00064-7
Bukowski, H., and Samson, D. (2021). Automatic imitation is reduced in narcissists but only in egocentric perspective-takers. Acta Psychol. 213:103235. doi: 10.1016/j.actpsy.2020.103235
Campbell, W. K., and Campbell, S. M. (2009). On the self-regulatory dynamics created by the peculiar benefits and costs of narcissism: a contextual reinforcement model and examination of leadership. Self Identity 8, 214–232. doi: 10.1080/15298860802505129
Casale, S., Fioravanti, G., and Rugai, L. (2016). Grandiose and vulnerable narcissists: who is at higher risk for social networking addiction? Cyber Psychol. Behav. Soc. Netw. 19, 510–515. doi: 10.1089/cyber.2016.0189
Chen, Z., Williams, K. D., Fitness, J., and Newton, N. C. (2008). When Hurt Will Not Heal: Exploring the Capacity to Relive Social and Physical Pain. Psychological Science, 19, 789–795. doi: 10.1111/j.1467-9280.2008.02158.x
Chukwuorji, J. C., Uzuegbu, C. N., Agbo, F., Ifeagwazi, C. M., and Ebulum, G. C. (2020). Different slopes for different folks: gender moderates the relationship between empathy and narcissism. Curr. Psychol. 39, 1808–1818. doi: 10.1007/s12144-018-9881-z
Davis, M. H. (1980). A multidimensional approach to individual diferences in empathy. JSAS Catalog Select. Doc. Psychol. 10, 85–104.
Decety, J., and Jackson, P. L. (2004). The functional architecture of human empathy. Behav. Cogn. Neurosci. Rev. 3, 71–100. doi: 10.1177/1534582304267187
De Panfilis, C., Antonucci, C., Meehan, K. B., Cain, N. M., Soliani, A., Marchesi, C., et al. (2019). Facial emotion recognition and social-cognitive correlates of narcissistic features. J. Personal. Disord. 33, 433–449. doi: 10.1521/pedi_2018_32_350
DeWall, C. N., MacDonald, G., Webster, G. D., Masten, C. L., Baumeister, R. F., Powell, C., et al. (2010). Acetaminophen reduces social pain: behavioral and neural evidence. Psychol. Sci. 21, 931–937. doi: 10.1177/0956797610374741
di Giacomo, E., Andreini, E., Lorusso, O., and Clerici, M. (2023). The dark side of empathy in narcissistic personality disorder. Front. Psychol. 14:1074558. doi: 10.3389/fpsyt.2023.1074558
Di Pierro, R., Di Sarno, M., Preti, E., Di Mattei, V. E., and Madeddu, F. (2018). The role of identity instability in the relationship between narcissism and emotional empathy. Psychoanal. Psychol. 35, 237–243. doi: 10.1037/pap0000159
Doyle, L. (2020). Anti-social cognition: Exploring the relationships between the dark triad, empathy, and theory of mind. Doctoral dissertation. Trent University (Canada).
Duffner, M., Gebauer, J. E., Sedikides, C., and Denissen, J. A. (2019). Self-enhancement and psychological adjustment: a meta-analytic review. Personal. Soc. Psychol. Rev. 23, 48–72. doi: 10.1177/1088868318756467
Duradoni, M., Gursesli, M. C., Fiorenza, M., Donati, A., and Guazzini, A. (2023). Cognitive empathy and the dark triad: a literature review. Eur. J. Investig. Health Psychol. Educ. 13, 2642–2680. doi: 10.3390/ejihpe13110184
Dziobek, I., Rogers, K., Fleck, S., Bahnemann, M., Heekeren, H. R., Wolf, O. T., et al. (2008). Dissociation of cognitive and emotional empathy in adults with Asperger syndrome using the multifaceted empathy test (MET). J. Autism Dev. Disord. 38, 464–473. doi: 10.1007/s10803-007-0486-x
Eddy, C. M. (2021). Self-serving social strategies: a systematic review of social cognition in narcissism. Curr. Psychol. 42, 4362–4380. doi: 10.1007/s12144-021-01661-3
Eddy, C. M. (2022). The Transdiagnostic relevance of self-other distinction to psychiatry spans emotional, cognitive and motor domains. Front. Psychiatry. 13:797952. doi: 10.3389/fpsyt.2022.797952
Eisenberger, N. I. (2011). “The neural basis of social pain: findings and implications” in Social Pain: Neuropsychological and Health Implications of Loss and Exclusion. eds. G. MacDonald and L. A. Jensen-Campbell (Washington, DC: American Psychological Association), 53–78.
Eisenberg, N., and Miller, P. A. (1987). The relation of empathy to prosocial and related behaviors. Psychol. Bull. 101, 91–119. doi: 10.1037/0033-2909.101.1.91
Faul, F., Erdfelder, E., Buchner, A., and Lang, A. G. (2009). Statistical power analyses using G* power 3.1: tests for correlation and regression analyses. Behav. Res. Methods 41, 1149–1160. doi: 10.3758/BRM.41.4.1149
Flasbeck, V., Enzi, B., and Brüne, M. (2017). Altered empathy for psychological and physical pain in borderline personality disorder. J. Personal. Disord. 31, 689–708. doi: 10.1521/pedi_2017_31_276
Golbabaei, S., Barati, M., Haromi, M. E., Ghazazani, N., and Borhani, K. (2023). Development and construct validation of a short form of the interpersonal reactivity index in Iranian community. Curr. Psychol. 42, 14038–14050.
Grijalva, E., Newman, D. A., Tay, L., Donnellan, M. B., Harms, P. D., Robins, R. W., et al. (2015). Gender differences in narcissism: a meta-analytic review. Psychol. Bull. 141, 261–310. doi: 10.1037/a0038231
Gross, J. J., John, O. P., and Richards, J. M. (2000). The dissociation of emotion expression from emotion experience: a personality perspective. Personal. Soc. Psychol. Bull. 26, 712–726. doi: 10.1177/0146167200268006
Gruda, D., McCleskey, J., Karanatsiou, D., and Vakali, A. (2021). I'm simply the best, better than all the rest: narcissistic leaders and corporate fundraising success. Personal. Individ. Differ. 168:110317. doi: 10.1016/j.paid.2020.110317
Hart, C. M., Hepper, E. G., and Sedikides, C. (2018). “Understanding and mitigating narcissists’ low empathy” in Handbook of Trait Narcissism (Cham: Springer), 335–343.
Hepper, E. G., Hart, C. M., Meek, R., Cisek, S., and Sedikides, C. (2014a). Narcissism and empathy in young offenders and non–offenders. Eur. J. Personal. 28, 201–210. doi: 10.1002/per.1939
Hepper, E. G., Hart, C. M., and Sedikides, C. (2014b). Moving Narcissus: can narcissists be empathic? Personal. Soc. Psychol. Bull. 40, 1079–1091. doi: 10.1177/0146167214535812
Hyatt, C. S., Zeichner, A., and Miller, J. D. (2019). Laboratory aggression and personality traits: a meta-analytic review. Psychol. Violence 9, 675–689. doi: 10.1037/vio0000236
Jacobs, K. A. (2022). The concept of narcissistic personality disorder-three levels of analysis for interdisciplinary integration. Front. Psychol. 13:989171. doi: 10.3389/fpsyt.2022.989171
Jonason, P. K., and Krause, L. (2013). The emotional deficits associated with the dark triad traits: cognitive empathy, affective empathy, and alexithymia. Personal. Individ. Differ. 55, 532–537. doi: 10.1016/j.paid.2013.04.027
Jospe, K., Genzer, S., klein Selle, N., Ong, D., Zaki, J., and Perry, A. (2020). The contribution of linguistic and visual cues to physiological synchrony and empathic accuracy. Cortex 132, 296–308. doi: 10.1016/j.cortex.2020.09.001
Krizan, Z., and Herlache, A. D. (2018). The narcissism spectrum model: a synthetic view of narcissistic personality. Personal. Soc. Psychol. Rev. 22, 3–31. doi: 10.1177/1088868316685018
Lachowicz-Tabaczek, K., Lewandowska, B., Kochan-Wójcik, M., Andrzejewska, B. E., and Juszkiewicz, A. (2021). Grandiose and vulnerable narcissism as predictors of the tendency to objectify other people. Curr. Psychol. 40, 5637–5647. doi: 10.1007/s12144-019-00569-3
Lamm, C., Bukowski, H., and Silani, G. (2016). From shared to distinct self–other representations in empathy: evidence from neurotypical function and socio-cognitive disorders. Philos. Trans. Roy. Soc. B. Biol. Sci. 371:20150083. doi: 10.1098/rstb.2015.0083
Lee, E., and Kang, H. K. (2020). Narcissism and perspective taking: the mediating effect of need for control. Soc. Behav. Personal. Int. J. 48, 1–7. doi: 10.2224/sbp.9333
Leunissen, J. M., Sedikides, C., and Wildschut, T. (2017). Why narcissists are unwilling to apologize: the role of empathy and guilt. Eur. J. Personal. 31, 385–403. doi: 10.1002/per.2110
Lovibond, P. F., and Lovibond, S. H. (1995). The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav. Res. Ther. 33, 335–343. doi: 10.1016/0005-7967(94)00075-U
MacDonald, G., and Leary, M. R. (2005). Why does social exclusion hurt? The relationship between social and physical pain. Psychol. Bull. 131, 202–223. doi: 10.1037/0033-2909.131.2.202
Miller, J. D., Hoffman, B. J., Gaughan, E. T., Gentile, B., Maples, J., and Keith Campbell, W. (2011). Grandiose and vulnerable narcissism: a nomological network analysis. J. Pers. 79, 1013–1042. doi: 10.1111/j.1467-6494.2010.00711.x
Miller, J. D., Lynam, D. R., Hyatt, C. S., and Campbell, W. K. (2017). Controversies in narcissism. Annu. Rev. Clin. Psychol. 13, 291–315. doi: 10.1146/annurev-clinpsy-032816-045244
Mohammadzadeh, A. (2009). Validation of the narcissistic personality questionnaire (NPI). J. Mental Health Princip. 4, 276–281. doi: 10.22038/JFMH.2009.11313
Morf, C. C., and Rhodewalt, F. (2001). Unraveling the paradoxes of narcissism: a dynamic self-regulatory processing model. Psychol. Inq. 12, 177–196. doi: 10.1207/S15327965PLI1204_1
Nelson, L. D., Simmons, J., and Simonsohn, U. (2018). Psychology’s renaissance. Annu. Rev. Psychol. 69, 511–534. doi: 10.1146/annurev-psych-122216-011836
Pajevic, M., Vukosavljevic-Gvozden, T., Stevanovic, N., and Neumann, C. S. (2018). The relationship between the dark tetrad and a two-dimensional view of empathy. Personal. Individ. Differ. 123, 125–130. doi: 10.1016/j.paid.2017.11.009
Peirce, J. W., Gray, J. R., Simpson, S., MacAskill, M. R., Höchenberger, R., Sogo, H., et al. (2019). PsychoPy2: experiments in behavior made easy. Behav. Res. Methods 51, 195–203. doi: 10.3758/s13428-018-01193-y
Raskin, R., and Hall, C. S. (1981). The narcissistic personality inventory: alternative form reliability and further evidence of construct validity. J. Pers. Assess. 45, 159–162. doi: 10.1207/s15327752jpa4502_10
Raskin, R., and Terry, H. (1988). A principal-components analysis of the narcissistic personality inventory and further evidence of its construct validity. J. Pers. Soc. Psychol. 54, 890–902. doi: 10.1037/0022-3514.54.5.890
Riečanský, I., Lengersdorff, L. L., Pfabigan, D. M., and Lamm, C. (2020). Increasing self-other bodily overlap increases sensorimotor resonance to others’ pain. Cogn. Affect. Behav. Neurosci. 20, 19–33. doi: 10.3758/s13415-019-00724-0
Riva, P., and Andrighetto, L. (2012). “Everybody feels a broken bone, but only we can feel a broken heart”: group membership influences the perception of targets' suffering. Eur. J. Soc. Psychol. 42, 801–806. doi: 10.1002/ejsp.1918
Riva, P., Brambilla, M., and Vaes, J. (2016). Bad guys suffer less (social pain): moral status influences judgements of others’ social suffering. Br. J. Soc. Psychol. 55, 88–108. doi: 10.1111/bjso.12114
Riva, P., Wesselmann, E. D., Wirth, J. H., Carter-Sowell, A. R., and Williams, K. D. (2014a). When pain does not heal: the common antecedents and consequences of chronic social and physical pain. Basic Appl. Soc. Psychol. 36, 329–346. doi: 10.1080/01973533.2014.917975
Riva, P., Williams, K. D., and Gallucci, M. (2014b). The relationship between fear of social and physical threat and its effect on social distress and physical pain perception. Pain 155, 485–493. doi: 10.1016/j.pain.2013.11.006
Riva, P., Wirth, J. H., and Williams, K. D. (2011). The consequences of pain: the social and physical pain overlap on psychological responses. Eur. J. Soc. Psychol. 41, 681–687. doi: 10.1002/ejsp.837
Ronningstam, E. (2016). Pathological narcissism and narcissistic personality disorder: recent research and clinical implications. Curr. Behav. Neurosci. Rep. 3, 34–42. doi: 10.1007/s40473-016-0060-y
Sahebi, A., Asghari, M. J., and Salari, R. S. (2005). Validation of Depression Anxiety and Stress Scale (DASS-21) for an Iranian Population. Iran J Psychiatry. 4, 299–313.
Sedikides, C., Rudich, E. A., Gregg, A. P., Kumashiro, M., and Rusbult, C. (2004). Are normal narcissists psychologically healthy?: self-esteem matters. J. Pers. Soc. Psychol. 87, 400–416. doi: 10.1037/0022-3514.87.3.400
Shamay-Tsoory, S. G., Aharon-Peretz, J., and Perry, D. (2009). Two systems for empathy: a double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 132, 617–627. doi: 10.1093/brain/awn279
Simard, P., Simard, V., Laverdiere, O., and Descôteaux, J. (2022). The relationship between narcissism and empathy: a meta-analytic review. J. Res. Pers. 102:104329. doi: 10.1016/j.jrp.2022.104329
Singer, T., Seymour, B., O'Doherty, J., Kaube, H., Dolan, R. J., and Frith, C. D. (2004). Empathy for pain involves the affective but not sensory components of pain. Science 303, 1157–1162. doi: 10.1126/science.1093535
Smith, M. B., Hill, A. D., Wallace, J. C., Recendes, T., and Judge, T. A. (2018). Upsides to dark and downsides to bright personality: a multidomain review and future research agenda. J. Manag. 44, 191–217. doi: 10.1177/0149206317733511
Turner, I. N., Foster, J. D., and Webster, G. D. (2019). The dark Triad's inverse relations with cognitive and emotional empathy: high-powered tests with multiple measures. Personal. Individ. Differ. 139, 1–6. doi: 10.1016/j.paid.2018.10.030
Urbonaviciute, G., and Hepper, E. G. (2020). When is narcissism associated with low empathy? A meta-analytic review. J. Res. Pers. 89:104036. doi: 10.1016/j.jrp.2020.104036
Vaziri-Harami, R., Heidarzadeh, F., and Kheradmand, A. (2021). Relationship between mobile phone addiction and narcissistic personality disorder among medical students. Arch. Clin. Psychiatr. 48, 24–28.
Vonk, J., Zeigler-Hill, V., Mayhew, P., and Mercer, S. (2013). Mirror, mirror on the wall, which form of narcissist knows self and others best of all? Personal. Individ. Differ. 54, 396–401. doi: 10.1016/j.paid.2012.10.010
Wai, M., and Tiliopoulos, N. (2012). The affective and cognitive empathic nature of the dark triad of personality. Personal. Individ. Differ. 52, 794–799. doi: 10.1016/j.paid.2012.01.008
Watson, D., Clark, L. A., and Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. J. Pers. Soc. Psychol. 54, 1063–1070. doi: 10.1037/0022-3514.54.6.1063
Wertag, A., Ribar, M., and Sučić, I. (2021). Empathy of the devil: sex differences in the dark tetrad and empathy. Empir. Stud. Psychol. 42–45.
Wilson, S., Stroud, C. B., and Durbin, C. E. (2017). Interpersonal dysfunction in personality disorders: a meta-analytic review. Psychol. Bull. 143, 677–734. doi: 10.1037/bul0000101
Wink, P. (1991). Two faces of narcissism. J. Pers. Soc. Psychol. 61, 590–597. doi: 10.1037/0022-3514.61.4.590
Wurst, S. N., Gerlach, T. M., Dufner, M., Rauthmann, J. F., Grosz, M. P., Küfner, A. C. P., et al. (2017). Narcissism and romantic relationships: the differential impact of narcissistic admiration and rivalry. J. Pers. Soc. Psychol. 112, 280–306. doi: 10.1037/pspp0000113
Zaki, J., and Ochsner, K. (2011). Reintegrating the study of accuracy into social cognition research. Psychol. Inq. 22, 159–182. doi: 10.1080/1047840X.2011.551743
Zaki, J., Weber, J., Bolger, N., and Ochsner, K. (2009). The neural bases of empathic accuracy. Proc. Natl. Acad. Sci. 106, 11382–11387. doi: 10.1073/pnas.0902666106
Keywords: affective empathy, cognitive empathy, empathic accuracy, narcissism, physical pain, self-other distinction, social pain
Citation: Shahri F, Zabihzadeh A, Taqipanahi A, Haromi ME, Rasouli M, Saeidi Nik A and Eddy CM (2024) I understand your pain but I do not feel it: lower affective empathy in response to others’ social pain in narcissism. Front. Psychol. 15:1350133. doi: 10.3389/fpsyg.2024.1350133
Edited by:
Atsushi Oshio, Waseda University, JapanReviewed by:
Vesna Gojković, Faculty of Legal and Business Studies Dr. Lazar Vrtakić, SerbiaCopyright © 2024 Shahri, Zabihzadeh, Taqipanahi, Haromi, Rasouli, Saeidi Nik and Eddy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abbas Zabihzadeh, YV96YWJpaHphZGVoQHNidS5hYy5pcg==; Clare M. Eddy, Y2xhcmUuZWRkeTFAbmhzLm5ldA==; Yy5lZGR5QGJoYW0uYWMudWs=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.