 Cristina Ene
Cristina Ene Vlad Burtaverde1*
Vlad Burtaverde1* Peter Karl Jonason
Peter Karl Jonason- 1Faculty of Psychology and Educational Sciences, University of Bucharest, Bucharest, Romania
- 2School of Psychology, University of Padua, Padua, Veneto, Italy
- 3Institute of Psychology, Cardinal Stefan Wyszynski University, Warsaw, Masovian, Poland
- 4Department of Neurosurgery, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania
- 5Department of Neurosurgery, Bagdasar-Arseni Clinical Emergency Hospital, Bucharest, Romania
According to evolutionary psychologists, an individual—consciously or not—who allocates resources for somatic effort focuses on homeostasis and the protection of themselves and others. During health crises, patients must choose between mobilizing their remaining resources to either recover or accepting the disease as inevitable. When patients choose to be proactive in terms of protecting their health, are conscientious, and compliant in the recovery process, a high level of patient activation is achieved. Therefore, we examined (N = 252) whether the patients’ K fitness strategies are predictors for engagement in patient activation-type behavior. In addition, we tested the mediating effect of pain catastrophizing and the moderating effect of romantic satisfaction. We found that people with a medical diagnosis, who were in a romantic relationship, and had high-K fitness were much more likely to be activated patients. Moreover, pain catastrophizing mediated the relationship between high-K fitness strategy and patient activation, while romantic satisfaction moderated this relationship, amplifying its intensity. The findings highlight the importance of identifying patients’ psychological resources (e.g., high-K strategy, romantic satisfaction, or pain perception) to keep them engaged in the health recovery process.
Introduction
The field of health psychology frequently explores the efficiency of intervention programs, the rate of patient recovery, patient involvement in the recovery process (Hibbard et al., 2007; Greene and Hibbard, 2012; Lee et al., 2022), and understanding the psychological factors that shape health-relevant behaviors (Martino et al., 2019; Ene et al., 2021). Evolutionary psychologists postulate that people are unconsciously motivated to protect themselves from health risk factors (e.g., disgust reaction to potential contamination and pregnancy sickness; Del Giudice, 2014), which is a manifestation of the human survival instinct (Figueredo et al., 2006; Tybur et al., 2012; Hill et al., 2016). Furthermore, these theories suggest that, given a favorable environment conducive to organism development, certain survival and adaptation strategies (High-K strategy) are developed. Individuals who align with this type of life history are characterized by attributes such as self-control, high aspirations, and risk avoidance. They tend to lead longer lives and have fewer offspring, on whom they prefer to focus their efforts and resources, being more inclined to undertake long-term endeavors (Dunkel Schetter, 2011). These strategies are presented on a continuum between two extremes: r strategies (unpredictable, risky environments, abuse, and hostility) and K strategies (predictable, prosperous environments, support, and emotional warmth).
However, research has traditionally focused on the general tendency of people to react involuntarily by withdrawing from or rejecting risk factors (Waynforth, 2012; Del Giudice, 2014) rather than on the health recovery process of those with medical diagnoses. In the present study, we investigate the adaptation strategies and somatic efforts of individuals who already have a medical diagnosis, depending on their life history. Therefore, we aim to explore the relationship between high-K fitness strategy and patient activation among those diagnosed with medical conditions. This includes examining the mediating role of pain catastrophizing and the moderating role of satisfaction in the couple’s relationship as explanatory mechanisms of this relationship.
Slow life/K-selected strategy and patient activation
According to evolutionary psychology, an individual—consciously or not—allocates resources toward somatic effort (e.g., growing a larger body) or reproductive effort (e.g., pursuing mates or investing in offspring; Figueredo et al., 2006; Giosan, 2006). The concept of fitness refers to the ability and potential of individuals to achieve reproductive success, their general adaptability to the environment, and their capacity to survive as long as possible (Giosan et al., 2018). Evolutionary psychologists show that, depending on the high-K fitness strategy, an organism’s life is shaped by several factors, including distinct mortality threats because the somatic effort is inherently limited (Figueredo et al., 2006; Hill et al., 2016). Therefore, organisms often face important trade-offs in distributing these resources among several competing life-sustaining components—growth, maintenance, and reproduction—at any given moment in time (Hill et al., 2016).
For individuals to reach a high level of fitness and avoid unfavorable strategies, it is necessary to adapt their strategies to the environment with its finite resources and make compromises in allocating energy to solve certain tasks relevant to fitness (Figueredo et al., 2006; Giosan, 2006). Life history theory postulates that under the influence of threatening factors unconsciously associated with mortality, people tend to allocate more motivational resources to survival than reproduction (Hill et al., 2016). People with a high-K fitness strategy are more oriented toward somatic effort and are long-term oriented (i.e., better health and increased lifespan; Figueredo et al., 2006). Therefore, once such individuals learn their health has deteriorated, they may be unconsciously motivated to protect themselves.
Activated patients in disease recovery are those who can manage their symptoms or difficulties, engage in activities that maintain optimal functioning, and are involved in treatment and diagnosis choices (Hibbard et al., 2004). Patient activation includes trusting in one’s own skills and knowledge, which helps manage their health and healthcare (Hibbard et al., 2004). There are favorable effects that patient activation can have on improving patients’ lives and on the physician–patient relationship (Hibbard et al., 2004, 2015; Feys et al., 2016). Few studies to date have focused on individual predictors of patients in disease management, such as personality, patient–physician relationship, resilience, self-efficacy, or race (Alexander et al., 2014; Crijns et al., 2019; Ene et al., 2021). However, to the best of our knowledge, we can affirm that greater patient activation is supported by a secure environment, trusting relationships, good social skills, conscientiousness, emotional stability, and a willingness to cooperate (Alexander et al., 2014; Crijns et al., 2019; Ene et al., 2021). Such aspects can further be associated with the high-K fitness strategy (Del Giudice et al., 2015), as somatic effort drives us to protect ourselves from threats, infections, or microbes. Therefore, the more patient activation, the slower the decline in health should be (Hibbard et al., 2015), thereby decreasing mortality risk.
By adopting an evolutionary lens to understand health behaviors, we contend that people who feel secure will be more motivated to make efforts that facilitate their survival. Growing up in an environment with satisfied needs (Ene et al., 2021), which help to develop self-esteem and a sense of security (e.g., resources allocated in somatic and parental efforts specify for slow life), will promote healthy and self-protective behaviors (Hill et al., 2016). In addition, individuals with a high-K fitness strategy, by nature, have a stronger self-preservation instinct, higher self-esteem, have easier access to good healthcare, and get involved more often in activities that improve their health or lifestyle (Buss, 2008; Giosan et al., 2018). These are all resources that individuals have easier access to, increasing their chances of going through an easier recovery, the prognosis to be more favorable, and the motivation for health to be almost always higher. Therefore, we expect a high-K fitness strategy to predict patients’ activation with a medical diagnosis and become more involved in the recovery process.
People with a high-K fitness strategy might lack important qualities as mating partners, leading to low chances of reproductive success, inappropriate adaptation to the environment, and low potential in the mating market (Buss, 2008). Those with a high-K fitness strategy who perceive threats as manageable (e.g., colds or flu) might favor increased somatic effort. However, serious or lifespan-shortening diseases, over which they feel little control (e.g., due to generally poor immune competence, chronic illness, or living in an environment rife with virulent pathogens), may accelerate their life history strategies (Hill et al., 2016). It appears that patients who come from disadvantageous early life conditions tend to exhibit elevated levels of pain catastrophizing, heightened perceived sensitivity to pain, and increased levels of pain-related fear (Simon et al., 2022), consequently finding themselves in unfortunate health situations, feeling trapped by fear, anxiety, or a sense of helplessness regarding their ability to improve their condition.
Pain catastrophizing
Pain catastrophizing is defined as a negative or exaggerated interpretation and orientation toward painful stimuli, often associated with health impairment, perceived disability, pain behavior, fear of movement, and depression (Sullivan et al., 1995; Suso-Ribera et al., 2017). Previous studies have shown that the burden of aging and functionality-limiting illness may be strongly associated with the adoption of a high-r strategy (McNamara et al., 1999; Hill et al., 2016). Growing up in an environment with socioeconomic disadvantages (e.g., low housing quality, high crowding, toxic exposure, and low social climate) reduces the likelihood that children will face adverse physical and psychosocial conditions, which can decrease emotional regulation, stress control, and cognitive functions (Simon et al., 2022). Environmental unpredictability, poor early life functioning, and stressful life events have also been associated with pain sensitivity, establishing memories, and associations for future adults (Waller et al., 2020). Therefore, individuals who were raised in such environmental and familial conditions develop a heightened state of alertness regarding pain and illness over time, feeling uncertain about how they will manage and whether they will find sufficient resources to cope or fully recover.
Given that all these risk factors are characteristic of a high-r fitness strategy, we expect that these patients will exhibit a higher perceived vulnerability to illness and catastrophizing if health risks are moderate or severe and if they perceive high levels of unpredictability and harshness. Individuals who are ill with a high-r fitness strategy may report high levels of pain catastrophizing because they might adopt emergency survival strategies, where danger is imminent and resources are dwindling. In such contexts, they allocate fewer resources to somatic efforts and healthcare, focusing instead on mating efforts and achieving reproductive success more quickly before the disease progresses, and of course, being much more accustomed to taking risks in general (Hill et al., 2016). Therefore, we expect that a high-K strategy has an indirect effect on patient activation through pain catastrophizing.
Romantic satisfaction
Survival and reproduction are fundamental evolutionary challenges, and humans have developed numerous strategies to maximize both (Salkicevic et al., 2014). These strategies encompass various mechanisms to achieve mating and somatic success. Previous studies indicate that high-K strategy indicators are significant predictors of couple satisfaction (Olderbak and Figueredo, 2010; Salkicevic et al., 2014). The potential moderating role of romantic satisfaction in the relationship between high-K fitness strategy and patient activation accurately reflects the effect of reproductive motivation and fulfilled reproductive success, which contributes to survival.
We know that individuals with a high-K fitness strategy tend to be oriented toward long-term relationships and have a greater need for stability in relationships (Figueredo et al., 2006; Del Giudice et al., 2015). Therefore, in contexts where people have safety, resources, and support, once they have reproduced, they can better connect to the goal of caring for and investing in their offspring (Del Giudice et al., 2015). Consequently, they find fulfillment and emotional resources in their children and family system, not merely a biological success motivated strictly by instinct.
There is evidence indicating that a slow strategy is frequently associated with long-term romantic orientation, active investment, and emotional involvement in the family system and child-rearing (Figueredo et al., 2006; Del Giudice et al., 2015). Therefore, a stable and satisfying relationship generally makes people feel that they have resources, support, and safety, thus creating a stronger motivation for the patient to focus more on somatic effort rather than reproductive effort. Patients thus have a higher tendency to take care of their health, recover, and regain functionality when all these conditions are met. Therefore, we expect that high relationship satisfaction serves as a reinforcing mechanism for individuals with increased fitness, aiding their physical recovery, enhancing their will to fight for survival, and making them active participants in protecting their health.
To sum up, considering that almost no research has investigated how life history strategies relate to health behavior, we aimed to examine whether individuals characterized by slow life history strategies are “good” patients who prioritize and value their health. Given the complexity of these relationships, we hypothesized that individuals with slow life history/high-K strategies, who also have a good romantic relationship, would be even more involved in patient activation behavior. In addition, we expect that patients with slow life/high-K strategies are more prone to catastrophizing pain, an effect that we anticipate will positively influence their mobilization and contribute to a high level of patient activation.
Method
Participants and procedure
We used G*Power to estimate the necessary sample size for significant effect sizes. The minimum required sample size was 197 participants for effect size (r) of 0.25, with an alpha set at 0.95 and the statistical power set at 0.95. For this study, 252 participants (Mage = 38.80, SD = 12.20, 67.9% women, 32.1% men) with an age range between 19 and 97 years were voluntarily recruited from several online groups based on the requirement that they have a medical diagnosis and are involved in a committed relationship. Participants who did not meet these conditions were excluded from the study. Participants reported relationship length in months (M = 155, SD = 128), with a minimum of 4 months and a maximum of 624 months (approximately 53 years).
The reported diagnoses were coded using the ICD-10-CM tabular list of diseases and injuries, and their frequency was reported as follows: 30.6% reported endocrine, nutritional, and metabolic diseases (E00-E89); 17.5% reported diseases of the musculoskeletal system and connective tissue (M00-M99); 11.1% reported diseases of the digestive system (K00-K95); 9.9% reported diseases of the genitourinary system (N00-N95); 7.1% reported diseases of the respiratory system (J00-J99); 6.0% reported neoplasms (C00-D49); 4.8% reported diseases of the skin and subcutaneous tissue (L00-L99); 4.4% reported diseases of the circulatory system (I00-I99); 4.0% reported diseases of the nervous system (G00-G99); 2.0% reported certain infectious and parasitic diseases (A00-B99); 2.0% reported diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50-D89); and 0.8% reported diseases of the ear and mastoid process (H60-H95). All participants were informed about the research objectives and provided consent to participate in the study. Data used in this research can be accessed at https://osf.io/uvxzm/.
Measures
Patient activation was assessed using the Patient Activation Measure (Hibbard et al., 2004). Participants indicated how much they identified with the items (1 = not at all, 5 = very much) with statements such as “How confident are you that you can follow through on medical treatments you need to do at home?.” The scale includes 22 items, and the items were summed to form a composite score (α = 0.92).
The high-K fitness strategy was assessed using the High-K Strategy Scale (Giosan, 2006), a measure of the high-K independent fitness criterion. Participants indicated how much they agreed with the items (1 = strongly disagree, 5 = strongly agree) with statements such as “I am in good physical shape.” The scale consists of 26 items, and all items were summed to form a composite score (α = 0.85).
Pain catastrophizing was assessed with the Pain Catastrophizing Scale (Sullivan et al., 1995). Participants indicated how frequently they experienced pain symptoms (1 = almost never, 5 = almost always) with statements such as “I cannot seem to keep it out of my mind” or “I feel I cannot go on.” The scale consists of 13 items, and all items were summed to form a composite score (α = 0.90).
Romantic satisfaction was assessed with the Relationship Assessment Scale (Hendrick, 1988). Participants indicated how satisfied they were with their romantic relationship (0 = very little/not at all satisfied, 4 = very much/very satisfied) with statements such as “In general, how satisfied are you with your relationship?.” The scale consists of seven items, and all items were summed to form a composite score (α = 0.90).
Data analysis
The analyses were conducted using SPSS (v25.0) and the MedMod package for R and Jamovi. Pearson’s correlations were used to analyze the relationships between the variables. Hierarchical linear regression was employed to investigate the predictive power of the high-K strategy within romantic relationships on patient activation. To test the mediation effect of pain catastrophizing and the moderation role of romantic satisfaction, we used the Medmod package for R and Jamovi.
Results
The results presented in Table 1 show descriptive statistics and all correlations among the study variables. People with slow life history strategies reported high patient activation, low pain catastrophizing, and high romantic satisfaction, and people with high patient activation reported low pain catastrophizing. To test the predictive power of the high-K fitness strategies on patient activation, we conducted a hierarchical linear regression (Table 2). In Step 1, we introduced high-K strategies that predicted 11% of the variance of patient activation (R2 = 0.11; F [1, 218] = 28.1, p < 0.001). In Step 2, we included romantic satisfaction and pain catastrophizing. These variables added a 4% increment in the prediction of patient activation (ΔR2 = 0.04; F [3, 216] = 12.8, p < 0.001). Overall, the final model with high-K fitness strategies, romantic satisfaction, and pain catastrophizing explained 15% of the variance in patient activation.

Table 1. Bivariate correlations and descriptive statistics for all the variables of the study.

Table 2. Hierarchical linear regression on the predictive power of high-K fitness strategy, pain catastrophizing, and romantic relationship for patient activation.
We performed an analysis to test whether pain catastrophizing mediated the relationship between the high-K fitness strategies and patient activation (Figure 1). People with high-K fitness strategies reported low pain catastrophizing (β = −0.30, z = −4.52, p < 0.001). People with high pain catastrophizing reported low patient activation (β = −0.13, z = −2.59, p < 0.05). In addition, people with high-K fitness strategies reported high patient activation (β = 0.23, z = 4.42, p < 0.001). Moreover, slow life history strategies led to high patient activation through pain catastrophizing, suggesting partial mediation (indirect effect = β = 0.04, z = 2.25, p < 0.05; direct effect = β = 0.23, z = 4.42, p < 0.001).
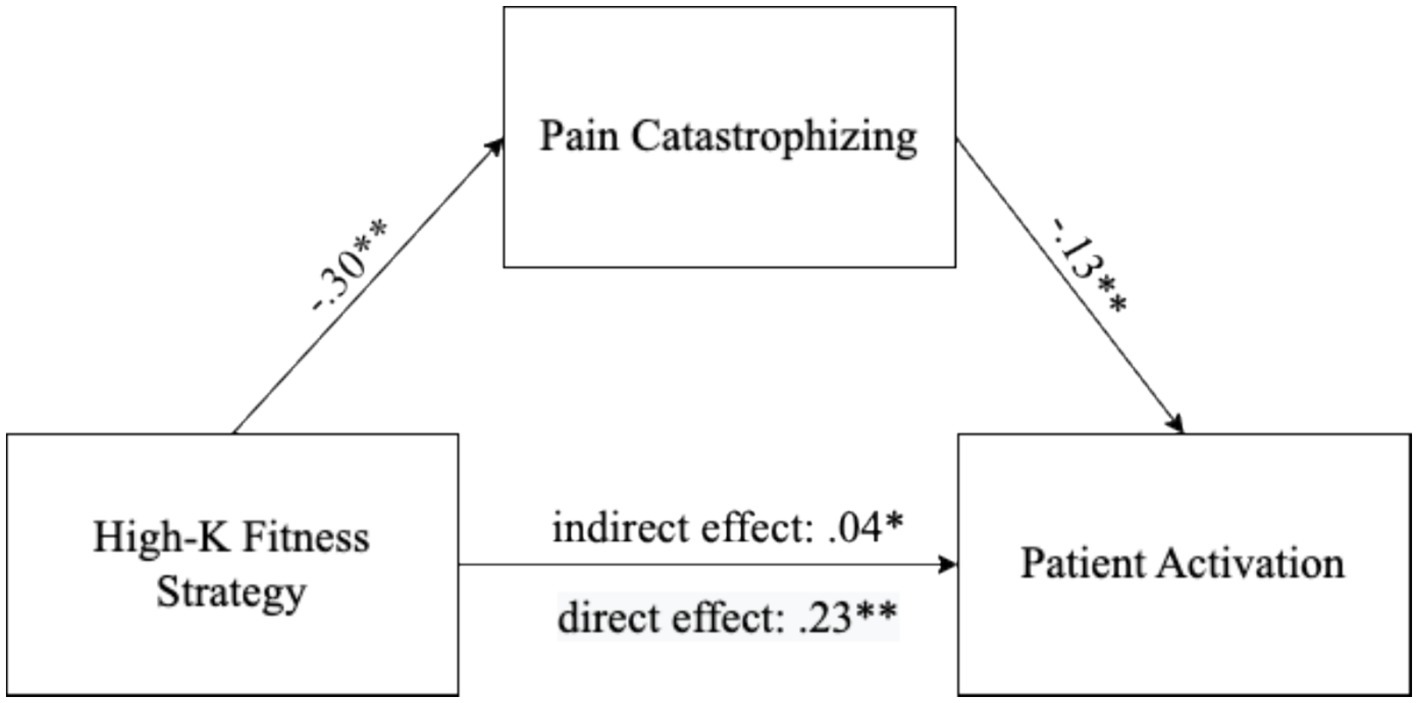
Figure 1. Mediator effect of pain catastrophizing on the relationship between high-K fitness strategy and patient activation. *p < 0.05 and **p < 0.01.
We performed a moderation analysis (Table 3; Figure 2), and our results showed that patients with high-K fitness strategies and higher romantic satisfaction were found to be more activated in recovery and treatment (with 1 unit increase in SD, B = 0.33, z = 4.75, p < 0.01). We also found that for patients with high-K fitness strategies and lower romantic satisfaction, even if they reported less activated behavior in recovery and treatment process, the moderation effect has decreased, becoming almost insignificant (with 1 unit increase in SD, B = 0.07, z = 1.93, and p = 0.053).

Table 3. Moderator effect of romantic satisfaction on the relationship between high-K fitness strategy and patient activation.
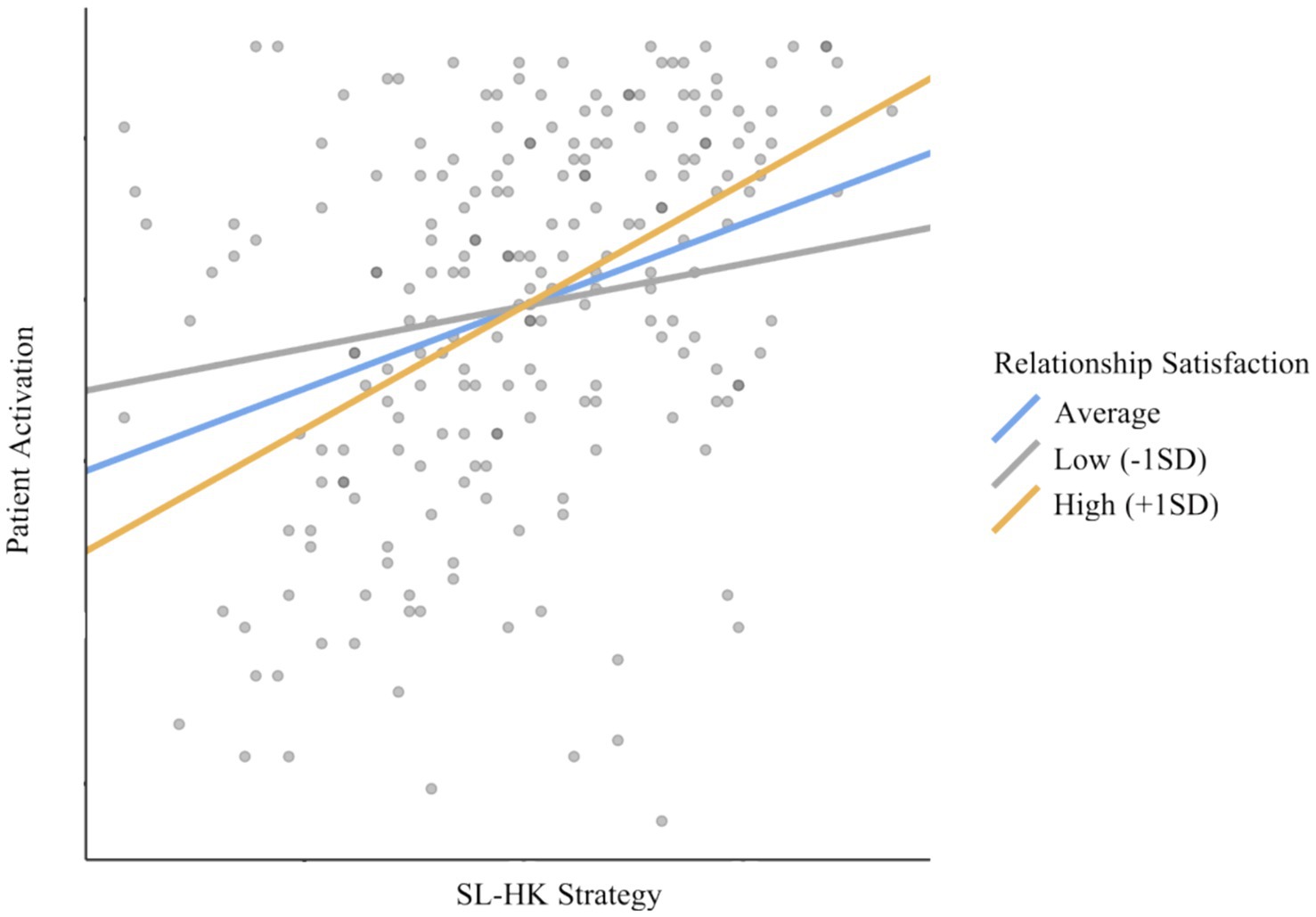
Figure 2. Simple slope plot for the moderating role of romantic satisfaction on the relationship between high-K fitness strategy and patient activation.
Discussion
Considering that almost no research investigated how life history strategies relate to health behavior, we aimed to investigate whether people characterized by slow life history strategies are “good” patients as they should prioritize and value their health. As there are hardly bivariate relationships, we hypothesized that pain catastrophizing mediates the relationships between life history strategies and patient activation, with relationship satisfaction playing a moderating role. We showed that people with slow life history strategies are “good” patients, as they are involved in patient activation behavior. In addition, pain catastrophizing partially mediated the relationship between slow life history strategies and patient activation. Romantic satisfaction moderated the relationship between high-K fitness strategies and patient activation, making it more intense.
Individuals who have a slow life history strategy were more likely to have more behaviors characteristic of the patient’s activation. Patients with a high-K strategy are people who grow in a secure environment and can have a higher mate value, more resources, and fewer risks. They can be more oriented toward somatic effort and are more interested and preoccupied with their health or direct threats to their survival (Figueredo et al., 2006; Giosan, 2006). Therefore, they can afford to manage a medical diagnosis with more care and involvement. As a result, they can easily become patients who are interested in or compliant with the doctor’s advice, follow the treatment, and do their research about the diagnosis. Therefore, we are referring to a life context in which patients know that if they follow these instructions and are conscientious and compliant with treatment, their chances of healing or survival are higher than if they acted otherwise.
Pain catastrophizing mediates the relationship, with patients using a high-K strategy tending to have more adaptive coping mechanisms related to the disease. These patients try to focus as little as possible on the intensity of the pain, thereby avoiding amplifying their perception of symptoms. This mediation effect is consistent with the argument that patients with a high-K strategy are concerned about their health and motivated to protect it as best as possible, not wanting to take additional risks with their health. Therefore, patients with emotional and financial resources, as well as those who actively experience a sense of security, have more coping strategies and become more easily concerned and conscientious in managing their illness.
On the other hand, we can recall previous studies that show us that people who grow up in fast-paced life environments tend to perceive themselves as unattractive, with few qualities (Dillon et al., 2013), and resign about their health with a high assumption of risks and, most likely, a strong orientation toward reproductive efforts (Giosan et al., 2018). People with such undesirable characteristics from the fast life environment were less likely to engage in preventive behavior and lower sense of self-efficacy in disease management (Nowak et al., 2020). Individuals from unpredictable environments are typically characterized by high risk-taking tendencies, an individualistic perspective on the world, and a strong orientation toward reproductive efforts, possibly even perceived as “insensitive” or dominant (Figueredo et al., 2006; Del Giudice et al., 2012). These are adaptive mechanisms to the reality in which they developed, helping them survive in a dangerous and unpredictable environment, and they tend to retain these mechanisms almost invariably into adulthood. However, this does not exclude the existence of emotions in the psychological system of patients from fast environments; rather, it is likely that they resort to adaptive and defensive mechanisms they have learned to be useful when faced with a challenge or danger (e.g., denial, dissociation, rationalization, and displacement; Colovic et al., 2016; Gori et al., 2023). They tend to use all these creative strategies to inhibit anxiety or fear that might otherwise overwhelm them, and sometimes, people may even underreport such emotional experiences.
Moreover, high-r individuals end up catastrophizing the pain because living in an unpredictable and poor environment they perceive illness and pain as a greater threat and evaluate risks as more difficult to manage (e.g., lower chances of recovery, higher long-term risks of mortality, or worsening of pain; Hill et al., 2016). Therefore, pain catastrophizing may act as an adaptive mechanism that signals to an individual the threats that are present in unstable environments, helping her/him avoid them. Therefore, they end up investing their limited resources and advantages in an objective that has more chances to be achieved, such as mating and reproductive efforts.
The importance of mating and romantic life is well known (Buss, 2008) and shows how strong people are guided by the “survival instinct.” The results showed that individuals with a slow life history strategy, once they have a satisfactory romantic relationship, will be even more motivated to allocate resources and importance to physical recovery. People know that they need energy and personal resources to fulfill their goals, in general (e.g., to raise their children). Therefore, when patients have a good romantic relationship, they notice that there are chances of success in terms of mating, and they manage to mobilize themselves to effectively manage the somatic aspect as well, as being active in the healing process.
These results have several practical implications. This information could be used in psychotherapy with clients who have health problems and end up being demotivated or frustrated because they have lost their physical functioning, or the process of recovery seems too arduous or protracted. Given that the motivation for survival and reproduction are powerful unconscious mechanisms (Buss, 2008), it is most likely that, under a suitable approach for each client, psychotherapists can help them recreate their goals and follow actions regarding their own lives.
Limitations and conclusion
However, the study has several limitations. First, our study was cross-sectional, which does not allow us to reveal causal conclusions regarding the realities between the study variables. Second, given that high-K fitness strategies are related to higher reproductive success (Figueredo et al., 2006; Giosan et al., 2018), it would have been helpful to check whether participants had children, the time spent with the kids, the age of having become a parent to be able to observe if there are any differences at the level of motivation for somatic efforts, and the specific K orientation. Third, the implications of the participants’ diagnoses were not investigated. Each diagnosis can have a different level of severity, with different chances of recovery, which can lead to different attitudes of patients regarding the level of involvement they are willing to allocate to recovery. For future studies, we recommend that researchers investigate the impact of illness severity on the desire to allocate resources to somatic or reproductive efforts. In addition, the indirect effect within the mediation was quite weak, which is why the results should be interpreted with skepticism, and further replication studies will be necessary.
We aimed to bring together the patients’ activation in the recovery considering the aspects that concern life history theory and evolutionary psychology, thus having a more complex perspective on the life of individuals with a medical diagnosis. In this study, we can highlight again the importance of life history as a general framework for orientation in the way the individual chooses to mobilize his resources according to a cost–benefit analysis for success that he makes regarding his resources. We can also extract from this study the importance of a satisfactory couple relationship in the process of recovery from the disease, and this has a motivating role.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://osf.io/shmdg/?view_only=79d4471ef94e4d9c8581a59bc7102525.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the University of Bucharest. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CE: Writing – original draft, Methodology, Investigation, Conceptualization. VB: Writing – review & editing, Validation, Formal analysis, Data curation, Conceptualization. PJ: Writing – review & editing, Supervision, Conceptualization. FB: Conceptualization, Data curation, Formal analysis, Methodology, Resources, Writing – review & editing. VP: Conceptualization, Data curation, Methodology, Resources, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alexander, J., Hearld, L., and Mittler, J. N. (2014). Patient–physician role relationships and patient activation: the moderating effects of race and ethnicity. Med. Care Res. Rev. 71, 472–495. doi: 10.1177/1077558714541967
Buss, D. M. (2008). “Human nature and individual differences: evolution of human personality” in Handbook of personality: Theory and research. eds. O. P. John, R. W. Robins, and L. A. Pervin (New York: The Guilford Press), 29–60.
Colovic, O., Tosevski, D. L., Mladenovic, I. P., Milosavljevic, M., and Munjiza, A. (2016). Defense mechanisms in “pure” anxiety and “pure” depressive disorders. J. Nerv. Ment. Dis. 204, 746–751. doi: 10.1097/NMD.0000000000000559
Crijns, T. J., Liu, T. C., Ring, D., Bozic, K. J., and Koenig, K. (2019). Influence of patient activation, pain self-efficacy, and resilience on pain intensity and magnitude of limitations in patients with hip and knee arthritis. J. Surg. Orthop. Adv. 478, 1319–1329. doi: 10.1097/CORR.0000000000001170
Del Giudice, M., Gangestad, S. W., and Kaplan, H. S. (2015). “Life history theory and evolutionary psychology” in The handbook of evolutionary psychology, foundations. ed. D. M. Buss. 2nd ed (New York: Wiley), 88–114.
Del Giudice, M., Hinnant, J. B., Ellis, B. J., and El-Sheikh, M. (2012). Adaptive patterns of stress responsivity: a preliminary investigation. Dev. Psychol. 48, 775–790. doi: 10.1037/a0026519
Del Giudice, M. (2014). An Evolutionary Life History Framework for Psychopathology. Psychological Inquiry 25, 261–300. doi: 10.1080/1047840X.2014.884918
Dillon, H. M., Adair, L. E., Wang, Z., and Johnson, Z. (2013). Slow and steady wins the race: life history, mate value, and mate settling. Personal. Individ. Differ. 55, 612–618. doi: 10.1016/j.paid.2013.05.015
Dunkel Schetter, C. (2011). Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Annual review of psychology 62, 531–558.
Ene, C., Rîndașu, C., and Ionescu, D. (2021). Patients’ personality in disease self-management. A self-determination perspective. Curr. Psychol. 42, 9618–9626. doi: 10.1007/s12144-021-02240-2
Feys, P., Giovannoni, G., Dijsselbloem, N., Centonze, D., Eelen, P., and Lykke Andersen, S. (2016). The importance of a multi-disciplinary perspective and patient activation programmes in MS management. Mult. Scler. J. 22, 34–46. doi: 10.1177/1352458516650741
Figueredo, A. J., Vasquez, G., Brumbach, B. H., Schneider, S. M. R., Sefcek, J. A., Tal, I. R., et al. (2006). Consilience and life history theory: from genes to brain to reproductive strategy. Dev. Rev. 26, 243–275. doi: 10.1016/j.dr.2006.02.002
Giosan, C. (2006). High-K strategy scale: a measure of the high-K independent criterion of fitness. Evol. Psychol. 4, 147470490600400–147470490600405. doi: 10.1177/147470490600400131
Giosan, C., Muresan, V., Wyka, K., Mogoase, C., Cobeanu, O., and Szentagotai, A. (2018). The evolutionary fitness scale: a measure of the independent criterion of fitness. EvoS J. 8, 1–28. doi: 10.59077/UAOL4054
Gori, A., Topino, E., and Musetti, A. (2023). The relationship among anxiety, worry, perceived stress, defense mechanisms, and high levels of post-traumatic stress symptoms: a discriminant analytic approach. J. Personal. Med. 13:237. doi: 10.3390/jpm13020237
Greene, J., and Hibbard, J. H. (2012). Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J. Gen. Intern. Med. 27, 520–526. doi: 10.1007/s11606-011-1931-2
Hendrick, S. S. (1988). A generic measure of relationship satisfaction. J. Marriage Fam. 50, 93–98. doi: 10.2307/352430
Hibbard, J. H., Greene, J., Shi, Y., Mittler, J., and Scanlon, D. (2015). Taking the long view. Med. Care Res. Rev. 72, 324–337. doi: 10.1177/1077558715573871
Hibbard, J. H., Mahoney, E. R., Stock, R., and Tusler, M. (2007). Do increases in patient activation result in improved self-management behaviors? Health Serv. Res. 42, 1443–1463. doi: 10.1111/j.1475-6773.2006.00669.x
Hibbard, J. H., Stockard, J., Mahoney, E. R., and Tusler, M. (2004). Development of the patient activation measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv. Res. 39, 1005–1026. doi: 10.1111/j.1475-6773.2004.00269.x
Hill, S. E., Boehm, G. W., and Prokosch, M. L. (2016). Vulnerability to disease as a predictor of faster life history strategies. Adapt. Hum. Behav. Physiol. 2, 116–133. doi: 10.1007/s40750-015-0040-6
Lee, C. S., Westland, H., Faulkner, K. M., Iovino, P., Thompson, J. H., Sexton, J., et al. (2022). The effectiveness of self-care interventions in chronic illness: a meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 134:104322. doi: 10.1016/j.ijnurstu.2022.104322
Martino, G., Langher, V., Cazzato, V., and Vicario, C. M. (2019). Editorial: psychological factors as determinants of medical conditions. Front. Psychol. 10:2502. doi: 10.3389/fpsyg.2019.02502
McNamara, J. M., Gasson, C. E., and Houston, A. I. (1999). Incorporating rules for responding into evolutionary games. Nature 401, 368–371. doi: 10.1038/43869
Nowak, B., Brzóska, P., Piotrowski, J., Sedikides, C., Żemojtel-Piotrowska, M., and Jonason, P. K. (2020). Adaptive and maladaptive behavior during the COVID-19 pandemic: the roles of dark triad traits, collective narcissism, and health beliefs. Personal. Individ. Differ. 167:110232. doi: 10.1016/j.paid.2020.110232
Olderbak, S. G., and Figueredo, A. J. (2010). Life history strategy as a longitudinal predictor of relationship satisfaction and dissolution. Personal. Individ. Differ. 49, 234–239. doi: 10.1016/j.paid.2010.03.041
Salkicevic, S., Stanic, A. L., and Grabovac, M. T. (2014). Good mates retain us right: investigating the relationship between mate retention strategies, mate value, and relationship satisfaction. Evol. Psychol. 12, 1038–1052. doi: 10.1177/147470491401200512
Simon, E., Zsidó, A. N., Birkás, B., and Csathó, Á. (2022). Pain catastrophizing, pain sensitivity and fear of pain are associated with early life environmental unpredictability: a path model approach. BMC Psychol. 10:97. doi: 10.1186/s40359-022-00800-0
Sullivan, M. J., Bishop, S. R., and Pivik, J. (1995). The pain catastrophizing scale: development and validation. Psychol. Assess. 7, 524–532. doi: 10.1037/1040-3590.7.4.524
Suso-Ribera, C., García-Palacios, A., Botella, C., and Ribera-Canudas, M. V. (2017). Pain catastrophizing and its relationship with health outcomes: does pain intensity matter? Pain Res. Manage. 2017, 1–8. doi: 10.1155/2017/9762864
Tybur, J. M., Bryan, A. D., and Hooper, A. E. (2012). An evolutionary perspective on health psychology: new approaches and applications. Evol. Psychol. 10, 855–867. doi: 10.1177/147470491201000508
Waller, R., Smith, A. J., O'Sullivan, P. B., Slater, H., Sterling, M., and Straker, L. M. (2020). The association of early life stressors with pain sensitivity and pain experience at 22 years. Pain 161, 220–229. doi: 10.1097/j.pain.0000000000001704
Keywords: high-K fitness strategy, patient activation, pain catastrophizing, romantic satisfaction, somatic effort
Citation: Ene C, Burtaverde V, Jonason PK, Brehar F and Pruna V (2024) Life history strategy and romantic satisfaction in patients’ behavior. Front. Psychol. 15:1346597. doi: 10.3389/fpsyg.2024.1346597
Edited by:
Béla Birkás, University of Pécs, HungaryReviewed by:
Ray Garza, Texas A&M International University, United StatesAndrea Zagaria, University of Trento, Italy
Copyright © 2024 Ene, Burtaverde, Jonason, Brehar and Pruna. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vlad Burtaverde, dmxhZC5idXJ0YXZlcmRlQGZwc2UudW5pYnVjLnJv