 Laís Ferreira1*
Laís Ferreira1* Milaine Dominici Sanfins2,3*
Milaine Dominici Sanfins2,3* Julia Dalcin Pinto5Piotr Henryk Skarzynski2,6,7,8
Julia Dalcin Pinto5Piotr Henryk Skarzynski2,6,7,8 Magdalena B. Skarżyńska4,7,9Eliara Pinto Vieira Biaggio1
Magdalena B. Skarżyńska4,7,9Eliara Pinto Vieira Biaggio1- 1Postgraduate Program in Human Communication Disorders, Department of Speech Therapy Federal University of Santa Maria, Santa Maria, Brazil
- 2Department of Teleaudiology and Screening, Institute of Physiology and Pathology of Hearing, Kajetany, Poland
- 3Albert Einstein Institute for Teaching and Research (IIEP), São Paulo, Brazil
- 4Department of Pharmacotherapy and Pharmaceutical Care, Pharmaceutical Department, Medical University of Warsaw, Warsaw, Poland
- 5ENT Department, Maria Curie-Skłodowska University, Lublin, Poland
- 6Center of Hearing and Speech Medincus, Kajetany, Poland
- 7Institute of Sensory Organs, Kajetany, Poland
- 8Marie Curie-Skłodowska University, Lublin, Lublin Voivodeship, Poland
- 9Center of Hearing and Speech, Nadarzyn, Poland
Background: Congenital toxoplasmosis (CT) occurs mainly by primary maternal infection during pregnancy. It is estimated that the incidence of vertical transmission to the fetus is 20% and that infected women are more likely to have a premature birth or low birth weight neonate since there is an association between CT and the rate of premature birth and low birth weight. In addition to severe neurological and ophthalmic consequences, hearing disorders such as hearing loss are also among the clinical manifestations seen in children with CT. Given the above, the objective of this study is to verify what are the auditory disorders seen in children with CT.
Methods: This literature review was structured according to the PRISMA statement and based on the terms of Study Target Population, Intervention, Comparison, Outcomes, and Study Types (PICOS). To obtain the studies, the following electronic databases were consulted: PubMed, Web of Science, Scopus, and Lilacs. The combined terms used for the search were: (“auditory evoked potentials” OR “hearing” OR “hearing loss”) AND (“congenital toxoplasmosis”). The selection of articles was carried out independently, blindly, by two of the authors, to minimize risk of bias.
Results: The search in the databases identified 172 articles, after excluding duplicate articles, 105 studies were identified. From the selection made by reading the titles and abstracts, 11 studies were selected for full-text reading. A total of 94 studies were excluded. An article was selected from the list of references. Therefore, 12 studies were included in the final analysis. It was observed that a significant percentage of studies sought to study the peripheral auditory pathway, verifying the occurrence or association between hearing loss and the presence of congenital infection. Only two studies evaluated the central auditory pathway, using the Brainstem Auditory Evoked Potential (BAEP) and the Frequency Following Response (FFR).
Conclusion: Toxoplasmosis affects not only the peripheral areas but central areas as well. Most studies suggest this pathology as a risk factor for both peripheral and central impairment. Research has found a greater association between CT and mild to moderate hearing loss, in addition to alterations in exams such as BAEP and FFR. These data recommend that CT be reported as a global public health problem and can help assess complications and impacts of hearing disorders as a result of CT. There is a gap about studies that retract the co-occurrence between CT and other Risk Indicators for Hearing Loss (RIHL), such as prematurity, permanence in the intensive care unit, and use of ototoxic medications, lack of longitudinal studies, that accompany the development of hearing and language of children with CT, since the consequences of this infection may be late.
1 Introduction
Congenital toxoplasmosis (CT) occurs mainly by primary maternal infection during pregnancy and brings an economic and health burden for affecting many pregnant women, especially those with low and middle income in underdeveloped countries. It is estimated that the incidence of vertical transmission to the fetus is 20% (Li et al., 2014) and that infected women are more likely to have a premature birth or the low birth weight neonate, since there is an association between CT and the rate of premature birth and low birth weight (Hurt et al., 2022). In addition, congenital and perinatal infections affect 0.5 to 2.5% of neonates and are the main causes of infant morbidity and mortality, complications of premature birth are the main cause of death in children under 5 years old (Liu et al., 2016).
The clinical diagnosis in this period is a challenge for professionals in the area since most cases are asymptomatic. However, the consequences are significant for the health of the child population and may occur in the neonatal period or late sequelae (Mirambo et al., 2019).
The clinical manifestations observed by this pathology depend on factors such as the mode of transmission, time of infection in relation to gestational age, maturity of the fetal immune system, and presence or absence of maternal immunity at the time of infection (Menson and Lyall, 2005).
In addition to severe neurological and ophthalmic consequences, hearing disorders are also among the clinical manifestations observed in children with CT (Al-Amari and Kameswaran, 1996; Andrade et al., 2008; de Resende et al., 2010; Vos et al., 2015; Besen et al., 2022). When analyzing the histopathology of the temporal bone in children with CT, researchers described that hearing loss in this infection may be a consequence of post-natal inflammation, since they found an inflammatory process, triggered by the parasite, in the inner ear (Salviz et al., 2013).
Although recommendations for children’s hearing health (Lewis et al., 2010; Joint Committee on Infant Hearing, 2019) cite CT and prematurity as Risk Indicators for Hearing Loss (RIHL), the results found in studies are variable. Thus, there is no consensus in the literature between the presence of hearing loss and this infection. While some authors report that such infection is a RIHL in children (Al-Amari and Kameswaran, 1996; Andrade et al., 2008; de Resende et al., 2010; Vos et al., 2015; Besen et al., 2022), other studies do not find this association (Lipka et al., 2002; Austeng et al., 2010).
Given the above, the objective of this study is to verify what are the auditory disorders observed in children with CT.
2 Materials and method
This literature review was structured according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and based on the terms of PICOS (Participants, Interventions, Comparators, Outcomes, and Study Design).
2.1 Eligibility criteria
Studies based on PICOS terms that evaluated the association between congenital toxoplasmosis and the presence of auditory disorders were included. PICOS stands for Study Target Population, Intervention, Comparison, Outcomes, and Study Types. Target population (P) corresponds to children; intervention (I) relates to congenital infections; comparison (C) was considered as children without congenital infections and typical audiological development; outcome (O) refers to the existence or not of auditory disorders; and the types of studies admitted (S) were observational, cohort, cross-sectional and randomized clinical trials. No restrictions were applied regarding language and year of publication. The studies should also obtain a score greater than 80% in the Study Quality Assessment Tools, showing that this is a high-quality study.
Studies that did not address the subject of this review, which were not carried out with the target population, reviews, letters, books, conference abstracts, case reports, case series, systematic and literature reviews, and opinion articles were excluded.
2.2 Search strategy
To obtain the studies, the following electronic databases were consulted: PubMed, Web of Science, Scopus and Lilacs. The research was carried out between May 2023 and June 2023, with individual search strategies by two researchers. Manual searches were also performed in bibliographic references in order to include relevant studies.
The combined terms used for the search were: (“auditory evoked potentials” OR “hearing” OR “hearing loss”) AND (“congenital toxoplasmosis”). Filters referring to the year of publication and language were not applied, however, filters related to the age of the sample were applied.
2.3 Selection of studies
The selection of articles was carried out independently, blindly, by two of the authors, avoiding any risk of bias. In this way, the names of authors and journals were masked to avoid any potential bias and conflict of interest. The articles were, at first, selected by title and abstract and were excluded for not respecting at least one of the inclusion criteria. The remaining articles were read in full and evaluated for eligibility. Any disagreement was resolved by discussion.
2.4 Risk of bias in individual studies
The risk of bias analysis was also performed independently, blindly, by two of the authors and subsequently agreed between them and a third author. For the analysis, the questionnaires of the Systematic reviews of etiology and risk instruments were used, specifically the Critical appraisal checklist for analytical cross-sectional studies and the Critical appraisal checklist for cohort studies. The final quality of each article was categorized by the following scores of answers “Yes,” “No” and “Little applicable,” being >70%, low risk of bias; between 50 and 69%, moderate risk of bias; <50%, high risk of bias.
2.5 Data extraction, synthesis and analysis
The information extracted from the studies were: authors, year of publication, age group studied, sample size, objective, results, and conclusion (Table 1) to then evaluate the association between congenital infections and hearing disorders. The extracted data were analyzed descriptively and comparatively. When any of this information was not available, the corresponding author was contacted by email.
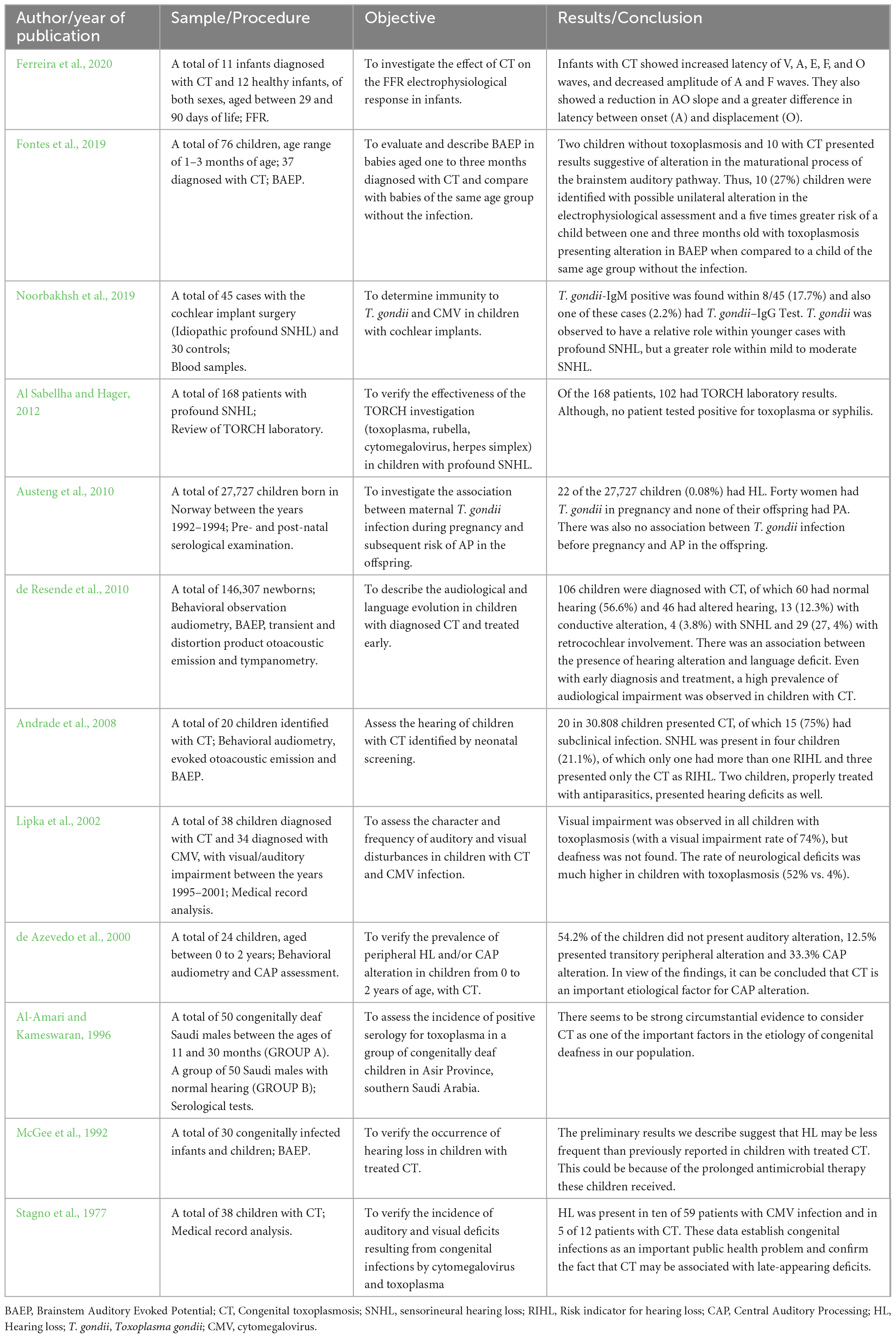
Table 1. Description of the included studies, presented in descending order of publication.
3 Results
3.1 Selected studies
In the blind selection of articles, the researchers identified 172 articles. After removing duplicates, 105 studies were selected for eligibility according to the criteria previously established. Finally, 11 studies were selected for full-text reading after careful title and abstract screening. A total of 94 studies were excluded (16 for being a systematic review, eight for being case studies, one for not finding the full text and 70 for not addressing the proposed topic). An article was selected from the list of references. Therefore, 12 studies were included for the final analysis. Supplementary Figure 1 demonstrates the study selection process in detail.
3.2 Characteristics of the studies
The selected studies were published between 1977 and 2021, with a greater number of publications between 2000 and 2010. All studies were published in English, four of which are also available in Portuguese. As for the design of the studies, 13 cross-sectional studies and one cohort study were selected. The vast majority of studies evaluated children from 1 day of life to 2 years of age.
It was observed that a significant percentage of studies sought to study the peripheral auditory pathway, verifying the occurrence or association between hearing loss and the presence of congenital infection. Only two studies evaluated the central auditory pathway, using the Brainstem Auditory Evoked Potential (BAEP) and the Frequency Following Response (FFR).
The authors verified the existence of both hearing loss (Al-Amari and Kameswaran, 1996; de Azevedo et al., 2000; Andrade et al., 2008; de Resende et al., 2010) and increased latency values in the BAEP and FFR responses (de Resende et al., 2010; Fontes et al., 2019; Ferreira et al., 2020). Therefore, the auditory pathway of children with CT can be affected both at the peripheral and central hearing levels.
To illustrate the analyzed studies, a table was prepared with the description of each one of them, with the identification of authorship, year of publication, title, objective, results and conclusion (Table 1).
3.3 Quality assessment
The quality assessment of the studies indicated that most of the studies were considered at low risk of bias, two studies were categorized with moderate risk of bias and one with a high risk of bias. Table 2 shows the details of this analysis.
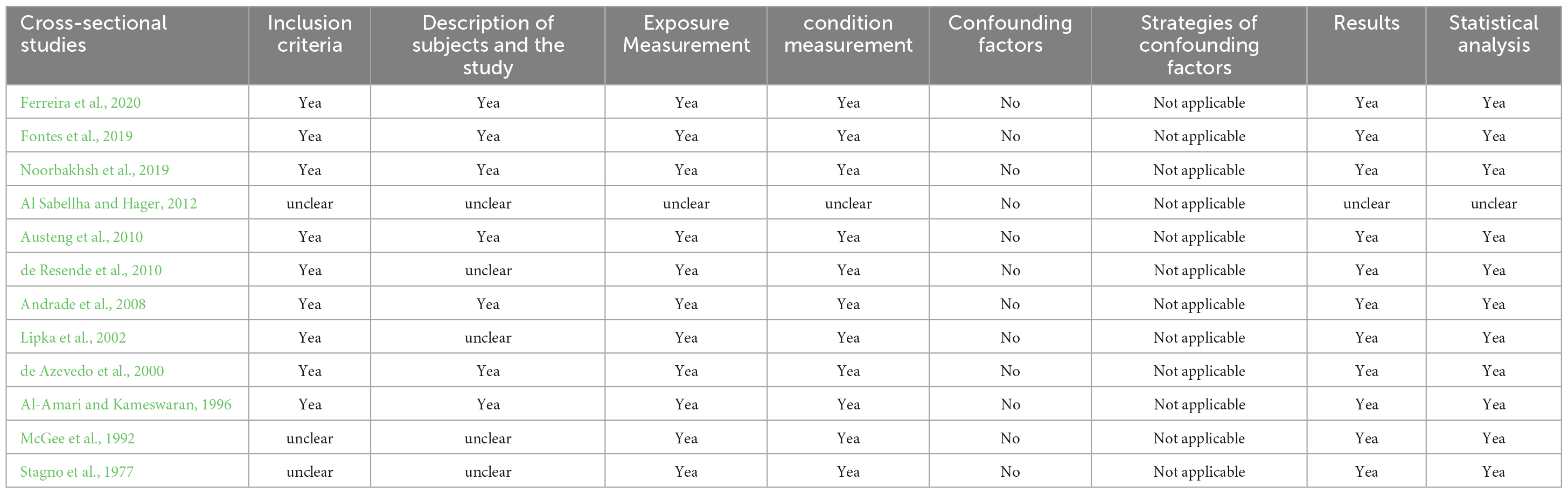
Table 2. Risk of bias analysis based on the instrument’s questionnaires.
4 Discussion
Together, the data found in this review show that children with congenital toxoplasmosis may have both hearing loss (Al-Amari and Kameswaran, 1996; de Azevedo et al., 2000; Andrade et al., 2008; de Resende et al., 2010) and alterations in central auditory pathways (de Resende et al., 2010; Fontes et al., 2019; Ferreira et al., 2020). Thus, this infection should be pointed out as a risk for disturbances in the peripheral and central auditory pathway. This finding suggests children with CT should undergo, besides typical audiological assessments, other more specific procedures for differential diagnosis.
Regarding the presence of hearing loss in children with CT, the literature does not demonstrate a consensus, as previously mentioned. While some authors found an association with hearing loss (Al-Amari and Kameswaran, 1996; de Azevedo et al., 2000; Andrade et al., 2008; de Resende et al., 2010) and language disorders (de Resende et al., 2010), another study did not find any association (Austeng et al., 2010).
Still regarding the degree of sensory auditory deficit, there is no significant relationship that children with congenital toxoplasmosis have profound hearing loss (Noorbakhsh et al., 2019). There is a greater correlation between children with CT and cases of mild to moderate hearing loss (Noorbakhsh et al., 2019).
Similar data were found in two studies that sought to understand the relationship between CT, hearing loss and possible changes in the Central Auditory Processing (CAP) (de Azevedo et al., 2000; de Resende et al., 2010). The results of these studies indicated that 54.2% to 56.6% of children with CT do not have auditory alterations, 12.3% to 12.5% have transient and conductive alterations, 3.8% have peripheral sensorineural alterations, 27.4% have retrocochlear changes and 33.3% have CAP changes (de Azevedo et al., 2000; de Resende et al., 2010).
In view of this, it is inferred that children with CT may demonstrate alterations in the basic diagnosis of hearing, evidenced by both conductive and sensorineural hearing loss. When performing differential assessments, children may also manifest changes in CAP.
The presence of clinical neurological manifestations in children with CT makes it essential to carry out the differential diagnosis of hearing. Through the evaluation of the central auditory nervous system, research has shown that children with CT may present alterations both at the brainstem level and at the subcortical and cortical levels (de Resende et al., 2010; Fontes et al., 2019; Ferreira et al., 2020).
At the brainstem level, the literature highlights that a child with CT, aged between 1 and 3 months, has a five times greater risk of manifesting an alteration in BAEP when compared to a child without the disease (Fontes et al., 2019). Furthermore, alterations at the subcortical and cortical level were verified through the FFR evaluation. The authors report that the group of children with CT showed a statistically significant increase in the latency of V, A, E, F, and O and a decrease in the amplitude of the A and F waves (Ferreira et al., 2020). Another interesting fact, when evaluating a group of children only exposed to toxoplasmosis during pregnancy, the authors observed that these children did not differ from the non-exposed group in terms of cochlear and conductive hearing loss, although they presented a higher occurrence of possible retrocochlear alteration (Leite Filho et al., 2017).
Researchers, who report neurophysiological delays in the central auditory pathway of children with CT when compared to neurotypical children, do not detail whether the group with the infection is behavior for term-born children. Considering that prematurity can cause immaturity in the auditory pathway and consequently delay in the latency of the waves of such potentials, this discussion would be interesting.
Given these data, the relevance of evaluations classified as differential diagnosis in this population is highlighted. It can be concluded that toxoplasmosis does not affect only the peripheral portion of the auditory pathway and that other evaluations deserve attention. However, more research is needed to establish in more detail the links and reflexes of congenital toxoplasmosis in the central auditory nervous system.
A limitation observed among the studies in this literature review is the restriction in relation to birth and health data and the demographic profile of the participants, which made it difficult to detail the characteristics of the population. There is a lack of research that portrays the co-occurrence between CT and other RIHLs, such as prematurity, permanence in the intensive care unit and use of ototoxic medications, in addition to reporting whether the existence of another RIHL increases or not the chances of hearing disorders.
In addition, another gap is the lack of longitudinal studies that follow the development of hearing and language of children with CT, since the consequences of this infection may be late. Therefore, it is recommended that studies be conducted to provide information regarding central auditory nervous system evaluations and to correlate the auditory disorders present in this population with their impact on the language of these children.
However, understanding the importance of an integral peripheral and central auditory system for the child to have an adequate acquisition and appropriation of language, such findings lead to a concern regarding child development. For this reason, the importance of audiological and language monitoring within newborn hearing screening programs is highlighted, as already mentioned in the literature (Lewis et al., 2010; Joint Committee on Infant Hearing, 2019).
5 Conclusion
Given these data, the relevance of evaluations classified as differential diagnosis in this population is highlighted. It can be concluded that toxoplasmosis does not affect only the peripheral and most studies suggest that this pathology is a risk factor for peripheral and central impairment. Research has found a greater association between CT and mild to moderate hearing loss, in addition to alterations in exams such as BAEP and FFR. These data recommend that CT be reported as a global public health problem and can help assess complications and impacts of hearing disorders as a result of CT. In addition to serving as support for the development of guidelines for child health services.
Data availability statement
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
LF: Conceptualization, Data curation, Investigation, Methodology, Project administration, Writing−original draft, Writing−review and editing. MDS: Formal analysis, Supervision, Writing−review and editing. JP: Data curation, Investigation, Methodology, Writing−original draft, Writing−review and editing. PS: Funding acquisition, Methodology, Resources, Writing−review and editing. MS: Funding acquisition, Methodology, Resources, Writing−review and editing. EV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing−review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1286211/full#supplementary-material
References
Al Sabellha, R., and Hager, A. (2012). The value of TORCH screening in children with bilateral profound sensorineural hearing loss. Indian J. Otol. 18:62. doi: 10.4103/0971-7749.100696
Al-Amari, O., and Kameswaran, M. (1996). Toxoplasmosis and congenital sensorineural hearing loss in Saudi Arabia. Ann. Saudi Med. 16, 168–470. doi: 10.5144/0256-4947.1996.468
Andrade, G., Resende, L., Goulart, E., Siqueira, A., Vitor, R., and Januario, J. (2008). Hearing loss in congenital toxoplasmosis detected by newborn screening. Brazil. J. Otorhinolaryngol. 74, 21–28. doi: 10.1016/S1808-8694(15)30746-1
Austeng, M., Eskild, A., Jacobsen, M., Jenum, P., Whitelaw, A., and Engdahl, B. (2010). Maternal infection with toxoplasma gondii in pregnancy and the risk of hearing loss in the offspring. Int. J. Audiol. 49, 65–68. doi: 10.3109/14992020903214053
Besen, E., Paiva, K., Hillesheim, D., Cigana, L., and Haas, P. (2022). Congenital syphilis associated with hearing screening failure in southern Brazilian newborns. Braz. J. Otorhinolaryngol. 88, S20–S24. doi: 10.1016/j.bjorl.2021.07.003
de Azevedo, M. F., Silva, A. A., Guedes, A. P., Meneguello, J., Caneschi, S., and Succi, R. (2000). Audiological findings in congenital toxoplasmos. Minutes AWHO 19, 96–101.
de Resende, L., de Andrade, G., de Azevedo, M., Perissinoto, J., and Vieira, A. (2010). Congenital toxoplasmosis: auditory and language outcomes in early diagnosed and treated children. Sci. Med. 20, 13–19. doi: 10.15448/1980-6108.2010.1.5927
Ferreira, L., Valadão, M., Skarzynski, P., Sanfins, M., and Biaggio, E. (2020). Effect of congenital toxoplasmosis on the encoding of speech in infants. Int. J. Pediatr. Otorhinolaryngol. 129:109767. doi: 10.1016/j.ijporl.2019.109767
Fontes, A., Carvalho, S., Andrade, G., Carellos, E., Romanelli, R., and Resende, L. (2019). Study of brainstem auditory evoked potentials in early diagnosis of congenital toxoplasmosis. Braz. J. Otorhinolaryngol. 85, 447–455. doi: 10.1016/j.bjorl.2018.03.012
Hurt, K., Kodym, P., Stejskal, D., Zikan, M., Mojhova, M., and Rakovic, J. (2022). Toxoplasmosis impact on prematurity and low birth weight. PLoS One 17:e0262593. doi: 10.1371/journal.pone.0262593
Joint Committee on Infant Hearing (2019). Position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics 4, 1–44.
Leite Filho, C. A., Lagreca, L. C. C., Jesus, N. O., Corvaro, C. P., Ferrarini, M. A. G., Monteiro, A. I. M. P., et al. (2017). Hearing loss in children exposed to toxoplasmosis during their gestation. Rev. CEFAC 19, 330–339.
Lewis, D. R., Marone, S. A. M., Mendes, B. C. A., and Cruz, O. L. M. Nóbrega, M. (2010). Comitê multiprofissional em saúde auditiva COMUSA. Braz. J. Otorhinolaryngol. 76, 121–128.
Li, X., Wei, H., Zhang, H., Peng, H., and Lindsay, D. (2014). A meta analysis on risks of adverse pregnancy outcomes in Toxoplasma gondii infection. PLoS One 9:e97775. doi: 10.1371/journal.pone.0097775
Lipka, B., Milewska-Bobula, B., Idzik, M., Marciński, P., Dunin-Wasowicz, D., Kassur-Siemieńska, B., et al. (2002). Visual and auditory impairment in children with congenital cytomegalovirus and Toxoplasma gondii infection. Przeglad Lekarski 59, 70–72.
Liu, L., Oza, S., Hogan, D., Chu, Y., Perin, J., Zhu, J., et al. (2016). Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet 388, 3027–3035. doi: 10.1016/S0140-6736(16)31593-8
McGee, T., Wolters, C., Stein, L., Kraus, N., Johnson, D., Boyer, K., et al. (1992). Absence of sensorineural hearing loss in treated infants and children with congenital toxoplasmosis. Otolaryngol. Head Neck Surg. 106, 75–80. doi: 10.1177/019459989210600131
Menson, E., and Lyall, H. (2005). Clinical presentation of congenital viral infections. Curr. Pediatr. 15, 163–170. doi: 10.1016/j.cupe.2004.12.004
Mirambo, M., Mshana, S., and Groß, U. (2019). Rubella virus, Toxoplasma gondii and Treponema pallidum congenital infections among full term delivered women in an urban area of Tanzania: a call for improved antenatal care. Afr. Health Sci. 19, 1858–1865. doi: 10.4314/ahs.v19i2.8
Noorbakhsh, S., Farhadi, M., Shokrollahi, M., Jomeh, H., and Ashouri, S. (2019). Cytomegalovirus and toxoplasma gondii: Common causes of profound sensori neural hearing loss in children with cochlear implant surgery in a highly immune population: Tehran, Iran. Open Neurol. J. 13, 45–49. doi: 10.2174/1874205X01913010045
Salviz, M., Montoya, J., Nadol, J., and Santos, F. (2013). Otopathology in congenital toxoplasmosis. Otol. Neurotol. 34, 1165–1169. doi: 10.1097/MAO.0b013e31828297b6
Stagno, S., Reynolds, D., Amos, C., Dahle, A., McCollister, F., Mohindra, I., et al. (1977). Auditory and visual defects resulting from symptomatic and subclinical congenital cytomegaloviral and toxoplasma infections. Pediatrics 59, 669–678. doi: 10.1542/peds.59.5.669
Keywords: hearing, electrophysiology, auditory evoked potentials, child development, congenital toxoplasmosis
Citation: Ferreira L, Sanfins MD, Pinto JD, Skarzynski PH, Skarżyńska MB and Vieira Biaggio EP (2024) Congenital toxoplasmosis and auditory disorders: a literature review. Front. Psychol. 14:1286211. doi: 10.3389/fpsyg.2023.1286211
Received: 31 August 2023; Accepted: 13 November 2023;
Published: 04 January 2024.
Edited by:
Sheila Andreoli Balen, Federal University of Rio Grande do Norte, BrazilReviewed by:
Ljiljana Jeličić, Research and Development Institute “Life Activities Advancement Center”, SerbiaSilvia Palma, AUSL Modena, Italy
Stela Maris Aguiar Lemos, Universidade Federal de Minas Gerais, Brazil
Copyright © 2024 Ferreira, Sanfins, Pinto, Skarzynski, Skarżyńska and Vieira Biaggio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laís Ferreira, bGFhaXNmZXJyZWlyYUBob3RtYWlsLmNvbQ==; Milaine Dominici Sanfins, bWlsYWluZWRzYW5maW5zQGdtYWlsLmNvbQ==