 Julia C. Seelandt
Julia C. Seelandt Margarete Boos
Margarete Boos Michaela Kolbe
Michaela Kolbe Juliane E. Kämmer
Juliane E. Kämmer
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Psychol., 10 August 2023
Sec. Organizational Psychology
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1232331
This article is part of the Research TopicPromoting Teamwork in HealthcareView all 24 articles
The aim of this paper is to inspire team research to apply diverse and unconventional perspectives to study team dynamics and performance in healthcare settings. To illustrate that using multiple perspectives can yield valuable insights, we examine a segment of a team interaction during a heart-surgery, using five distinct interdisciplinary perspectives known from small group research: the psychodynamic, functional, conflict-power-status, temporal, and social identity perspectives. We briefly describe each theoretical perspective, discuss its application to study healthcare teams, and present possible research questions for the segment at hand using the respective perspective. We also highlight the benefits and challenges associated with employing these diverse approaches and explore how they can be integrated to analyze team processes in health care. Finally, we offer our own insights and opinions on the integration of these approaches, as well as the types of data required to conduct such analyses. We also point to further research avenues and highlight the benefits associated with employing these diverse approaches. Finally, we offer our own insights and opinions on the integration of these approaches, as well as the types of data required to conduct such analyses.
Communication, coordination and leadership in healthcare teams are essential for task performance and patient safety, especially during emergency situations (Tucker and Edmondson, 2003; Manser, 2009; Künzle et al., 2010; Fernandez Castelao et al., 2013; Kolbe and Grande, 2013; Tschan et al., 2014). Teamwork is especially challenging in large hospitals, where turnover rates are high, and for interdisciplinary and interprofessional ad-hoc teams lacking the experience of continuously working together as team (Pearce et al., 2006; Nemeth, 2008; St. Pierre et al., 2011; Fortune et al., 2012). Even the willingness and ability to work together do not guarantee success; frequent hurdles are diffuse responsibilities, role conflicts, unsuccessful communication, divergent assumptions about cooperation, skepticism toward other professional groups and the silo mentality that often prevails (Eichbaum, 2018; Rosen et al., 2018; Paige et al., 2019; Kämmer and Ewers, 2022).
How can we foster teamwork in the demanding and ever-changing healthcare environment? While past research has provided valuable insights into the input variables and processes that influence outcomes in healthcare teams (Schmutz and Manser, 2013), we still have much to learn about the temporal dynamics, power dynamics and interprofessional forces at play (Kolbe and Boos, 2019; Anderson et al., 2021). This is partly due to the fact that previous studies have tended to take a particular theoretical perspective when examining healthcare teams: applying what is called the functional perspective, they have examined how selected input factors function to influence group effectiveness (Härgestam et al., 2013; El-Shafy et al., 2018; Schmutz et al., 2018, 2019). However, the theoretical lens we use can influence our findings, and alternative perspectives may be create additional value to studying healthcare teams. Poole and colleagues (Poole et al., 2004) have identified nine interdisciplinary perspectives that can be applied to the study of small groups.
Based on our past research experience, we have noticed that we ourselves tend to act from a silo mentality: We conduct research from primarily one of these perspectives without much considering other perspectives. From our point of view, that “single-mindedness” of sticking to only one theoretical perspective is rather common in healthcare, resulting in reinventing the wheel or disregarding other relevant aspects of teamwork. We believe that using and linking diverse and unconventional perspectives for studying teams in healthcare can broaden our understanding and create additional value. This perspective article does not provide detailed how-to-instruction for conducting team research with each perspective. Instead, our intention is to provide “food for thought” to stimulate team researchers to think out of the box in their next research projects. We therefore present a thought experiment: using segments of the team interaction protocol from a heart-surgery, we demonstrate how we can extract different research questions emerge and offer unique insights when adopting five different perspectives—the functional, conflict-power-status, psychodynamic, temporal, and social identity perspectives. We have selected these five perspectives based on our own research interests, experience, and scientific curiosity; this selection does not claim to be exhaustive. By adopting these perspectives, we aim to shed light on how we can promote effective teamwork (research) in the complex and challenging healthcare environment. We hope that this illustration will offer team researchers who may feel stuck in one viewpoint a fruitful avenue to advance their research, combine certain points of view, and create new research insights that promote teamwork in healthcare. Notably, applying these different perspectives is not limited to healthcare but applicable to teams in other high risk organizations, as has been demonstrated (Hagemann et al., 2011).
The starting point is the transcript of an audio-recorded team interaction during a scheduled, conventional heart surgery at the University Medical Centre Goettingen (Germany). The surgery was chosen randomly from a control group of 11 surgeries used in another study (Leitsmann et al., 2021; Lehrke et al., 2022).
The surgical team consisted of six members: a primary surgeon (PS, male, age 50), an assisting surgeon (AS, male, 34), a scrub nurse (SN, female, 48), a circulating nurse (CN An, female, 61), an anesthesiologist (An, female, 49), and a perfusionist (HLM, male, 62). The MAGIX Samplitude Music Studio 2017 software (Magix Software GmbH, 2017., Berlin, Germany) was used to record and transcribe the communication, with the transcripts resulting in an Excel 2010 spreadsheet (Microsoft Corporation, 2018). The transcript was segmented into coding units (lines in Table 1) based on syntactic criteria (Kolbe et al., 2016).
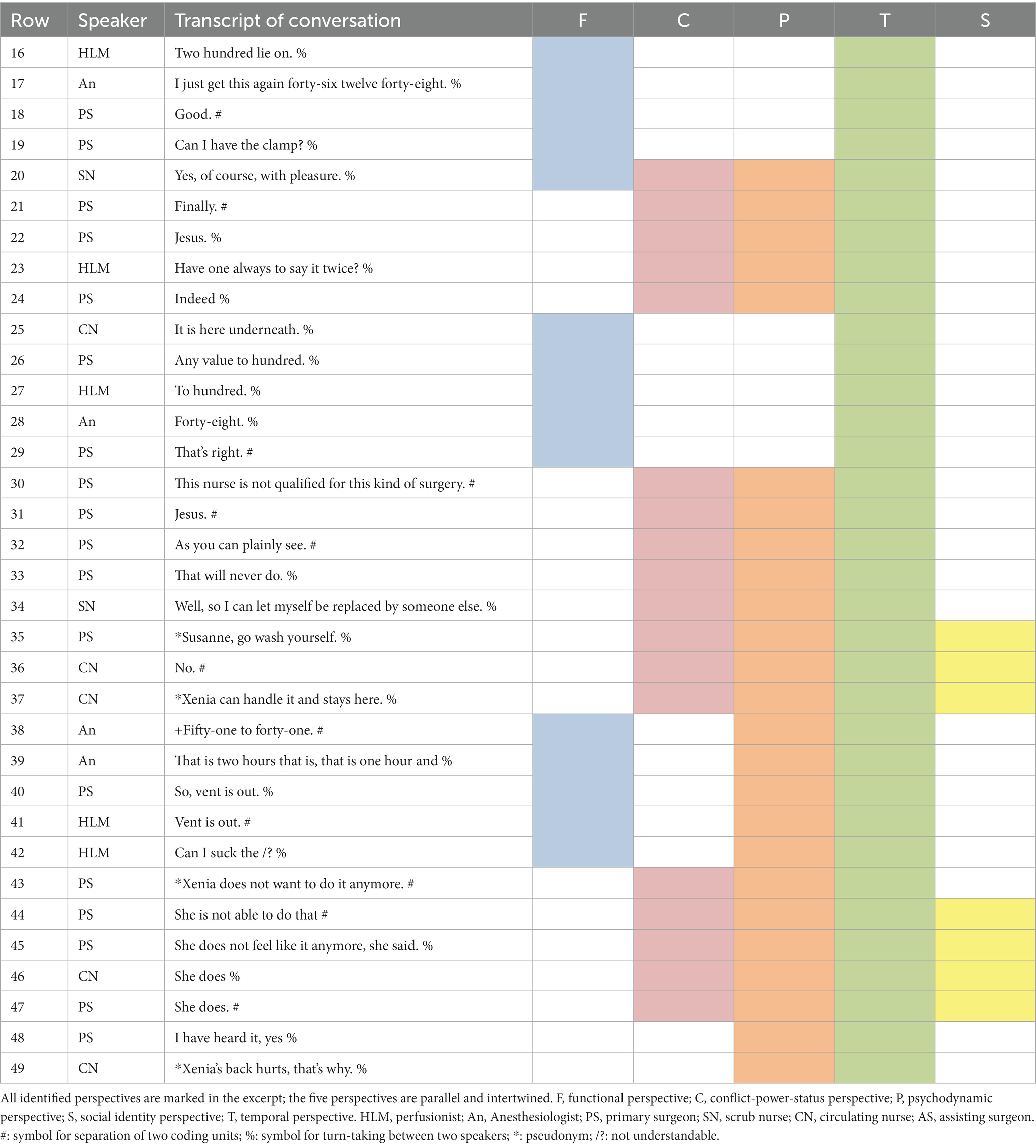
Table 1. Excerpt of a transcript of an audio-recorded team interaction during a conventional heart surgery with marked perspectives.
The following excerpt (Table 1) captures the beginning of a coronary bypass grafting procedure using conventional extracorporeal circulation. This procedure occurs during a phase of surgery when the aorta is reopened and the patient is under cardiopulmonary support by the heart lung machine. This phase is critical, as the main procedure (bypass grafting) is executed while the patient is in a vulnerable state. At the end of this phase, the heart must pump again without machine support and recover from its protracted metabolic disturbance.
In the following sections, we will delve into each of the five different perspectives on studying teams. Per perspective, we will provide a brief overview of its key assumptions, discuss how it could be applied to analyze the excerpt provided and describe for which research goal it is suitable. We also share potential insights and strengths when applying the perspectives to healthcare teams and we outline possible research questions for each perspective in Table 2. All identified perspectives are marked in the excerpt in Table 1. The five perspectives are parallel, intertwined and partly overlapping. Depending on which lens we have on, we can combine up to four different perspectives with each other to analyze this excerpt (Figure 1). For each perspective, different data sources are required (Table 2).
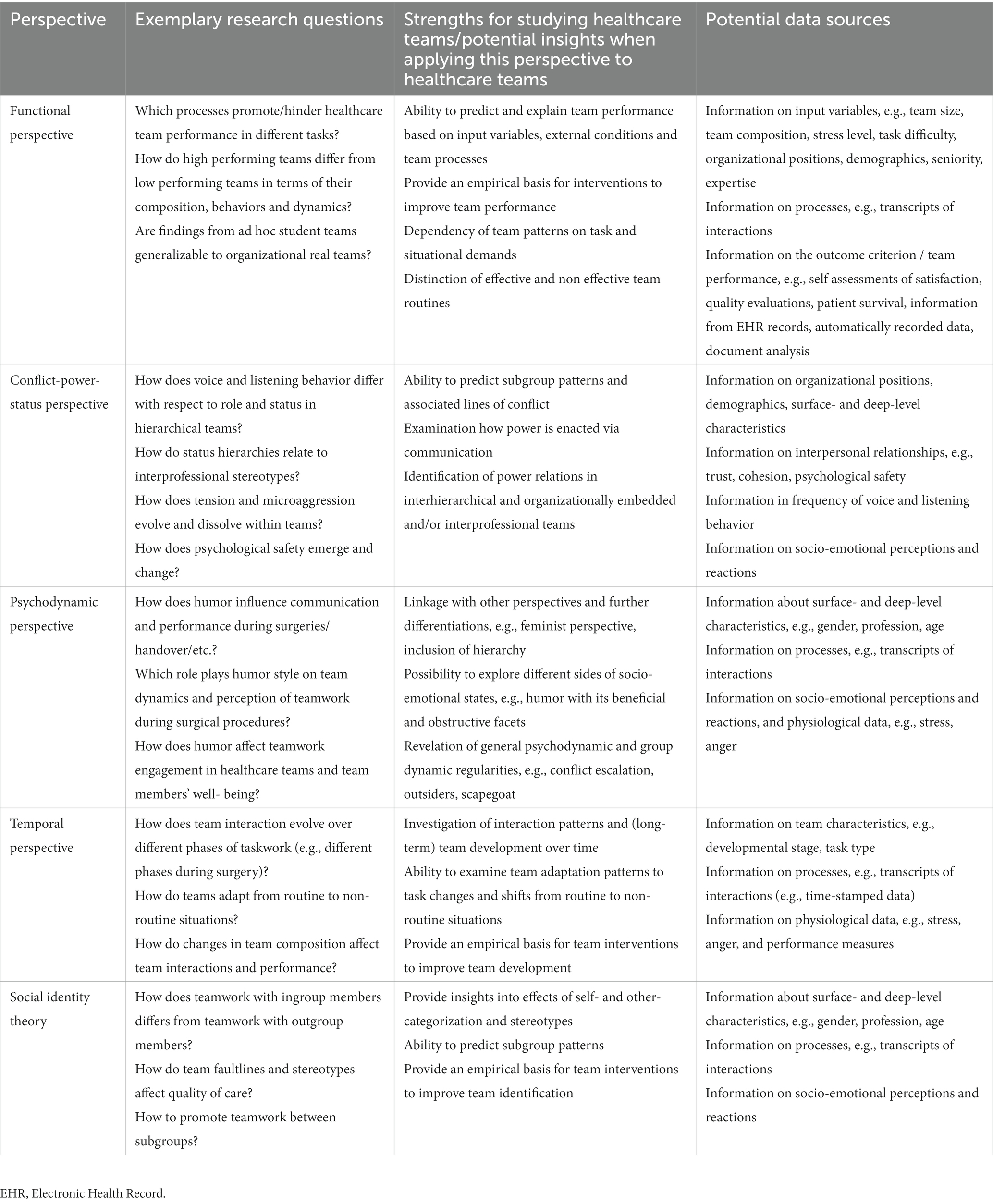
Table 2. Descriptions of possible research questions, strengths, and data requirements for each perspective.
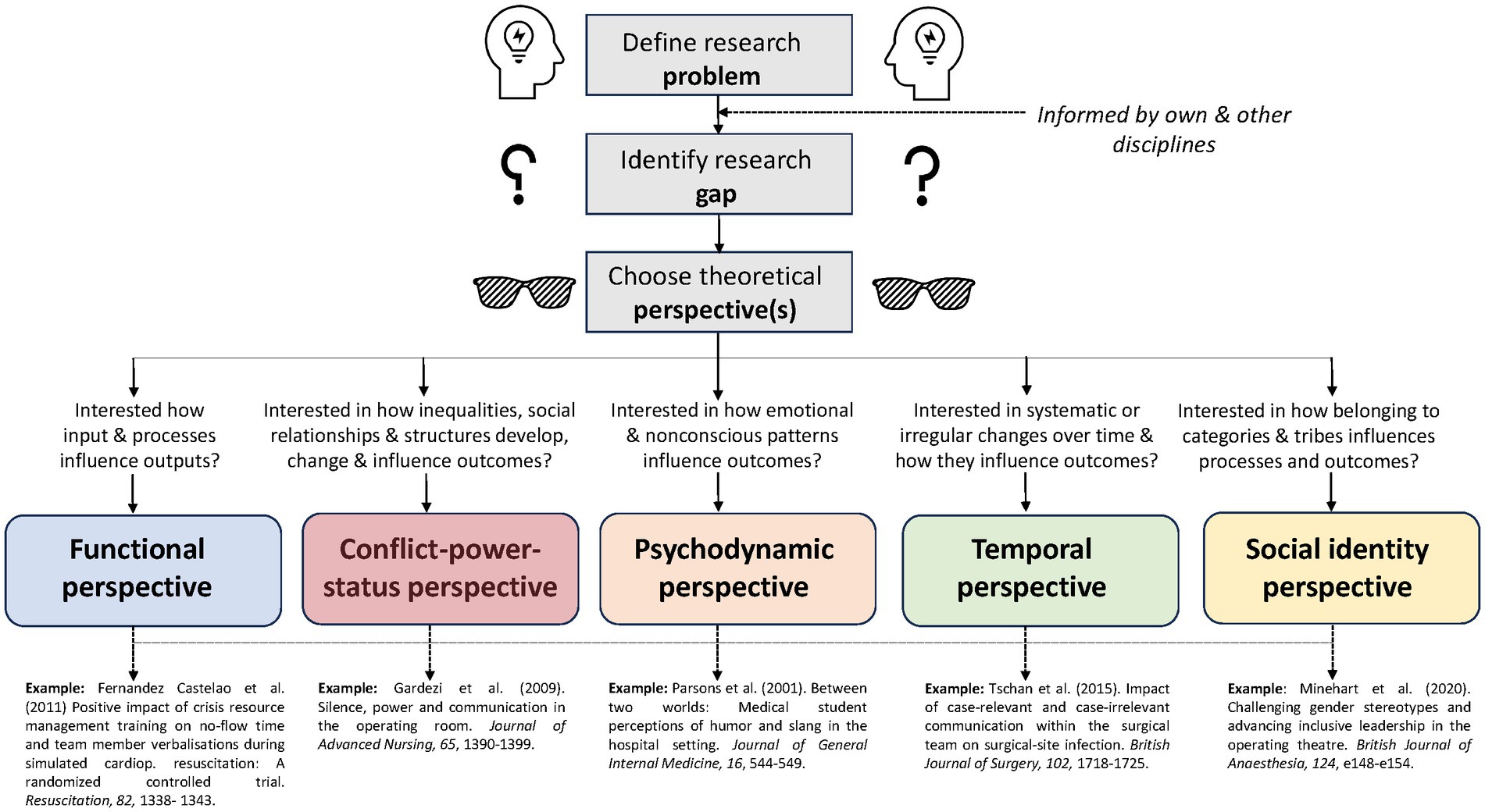
Figure 1. Five perspectives for analyzing team interactions.
Scholars taking a functional perspective assume that groups are goal-oriented and that inputs (e.g., the group task) and/or processes (e.g., communication) influence group performance (e.g., productivity, effectiveness, satisfaction) as well as external factors (e.g., organizational structures, regulations), all of which can be evaluated (Poole et al., 2004; Hollingshead et al., 2005). Their research goal is to identify relevant group features and behaviors (such as certain communication or coordination patterns) that promote or hinder group performance (Fernandez Castelao et al., 2011; Kolbe et al., 2014; Willmes et al., 2022). For example, one result obtained by taking this perspective is that closed-loop-communication (CLC), where a command is followed by a checkback and closing the loop (Härgestam et al., 2013; El-Shafy et al., 2018), correlates with higher task performance (e.g., lower hands-off time in resuscitation, better adherence to guidelines) and thus higher patient safety (Salas et al., 2008). Research from a functional perspective is suited to inform the testing of certain interventions (e.g., checklists)(Lingard et al., 2008; Russ et al., 2015), the development of interventions to improve team performance, such as crisis resource management principles (Oberfrank et al., 2019), different mnemonics to help teams quickly organize themselves (e.g., 10 s for 10 min) (Rall et al., 2008) and briefing and debriefing interventions (Lingard et al., 2008, 2011; Russ et al., 2015).
Consider the episode in lines 19–21, where the surgeon asked the scrub nurse to get the clamp and the nurse acknowledges it. Instruction-reaction episodes such as this one may be analyzed in terms of their completeness by comparing them to the “ideal” CLC cycle (Tschan, 1995, 2002). Additionally, one could check which internal and external factors prevent the correct implementation of the CLC cycles. This analysis could reveal the proportion of standard vs. non-standard forms of CLC and relate it to outcome measures such as the number of followed instructions or patient survival (Marzuki et al., 2019).
Another functional approach to the excerpt would be to code the content of utterances with an established coding scheme (i.e., assign pre-defined behavior and communication codes to sequences of the interaction). For example, researchers may code case-relevant communication (CRC) such as ‘instructions’, versus case-irrelevant communication (CIC) such as chitchatting (Seelandt et al., 2014; Lehrke et al., 2022). The proportions and patterns of CRC to CIC episodes could then be set in relation to outcome variables such as satisfaction with teamwork or team effectiveness [e.g., surgical site infections (Widmer et al., 2018)].
In sum, researchers interested in crucial inputs and processes influencing team performance outcomes are advised to adopt this perspective. Exemplary research questions as well as recommendations for data sources are highlighted in Table 2. However, focus on the functional perspective is often limited to “team performance,” disregarding other important outcomes such as well-being or system maintenance.
Scholars taking a conflict-power-status perspective assume that resources, status, and power are unequally distributed within groups (Poole et al., 2004; Sell et al., 2004). Their research goal is to understand how these inequalities, social relationships and associated group structures develop and change, and how they influence group processes (e.g., conflict management) and outcomes [e.g., member satisfaction (Poole et al., 2004)] Healthcare teams seem to be a logical place for adopting the conflict-power-status perspective (Janss et al., 2012) given that differences in (legitimate) power and occupational status are paramount (Hollenbeck et al., 2012). In our operating room team example, surgeons, anesthesiologists, perfusionists and nurses may each have certain explicit positional status and power, yet also have implicit, subtle and relational status and power based on experience, tenure and relationships (Yule et al., 2006; Gardezi et al., 2009).
Consider the episode in lines 30–37, where we witness how the surgeon expressed his dissatisfaction with the nurse, whereupon the nurse offered to be substituted by another nurse. While the surgeon agreed with this suggestion, instructing another nurse to enter, the circulating nurse overtly objected, instructing the first nurse to stay. Applying the conflict-power-status perspective to analyzing the excerpt offers the possibility to study how power is explicitly and implicitly enacted (e.g., by examining who instructs whom), how open (vs. subtle) conflicts are enacted, or which coalitions exist. Assumptions and discussion about responsibilities, performance or authority are a frequent source of tension in the operating room (Lingard et al., 2002, 2004). Tension, frustration and conflict influence the quality of team interactions. For example, while observing disrespectful behavior may cause team members to speak up with a concern, a general lack of psychological safety or of inclusive language may impede live-saving speaking up (Edmondson, 2003; Raemer et al., 2016; Weiss et al., 2018; Krenz et al., 2020; Vauk et al., 2022).
As healthcare is more and more provided by multidisciplinary teams whose professional members each have a unique identity with potentially differing priorities, roles and expectations of how care should be delivered, micropolitical interests have to be negotiated (Taplin et al., 2015; Kolbe et al., 2019). Politics refers to the use of power, authority and influence and is a relational process between people and within teams (Rogers et al., 2020). This excerpt also gives rise to the possibility to assess emotional reactions to and satisfaction with the manner in which hierarchy is acted out and which role sarcasm, humor and irony play in such power games (Krenz et al., 2019; Long et al., 2020; Koopman et al., 2023; Weiss et al., 2023).
In sum, researchers interested in understanding status and power inequalities, group structures and their impact on team performance outcomes are directed to this approach. However, research strongly following the conflict-power-status perspective may require high levels of reflexivity from researchers who have their own personal views on conflict, power and status dynamics.
Scholars taking a psychodynamic perspective assume that emotional and nonconscious processes exist within all human groups which impact their interactions and task performance (Mcleod and Kettner-Polley, 2004). Their research goal is to understand emotions and unconscious patterns of behavior (Mcleod and Kettner-Polley, 2004). To increase team performance, these nonconscious processes have to be brought to team members’ conscious awareness (Mcleod and Kettner-Polley, 2004). One of these nonconscious processes is humor (Newirth, 2006).
Humor can have different functions. On the one hand, humor takes on a conducive role and positive humor has many benefits. It may alleviate tension, fatigue, and improve work relationships (Crowe et al., 2016). Humor also has a relaxing function and can buffer the negative effects of stress on health and well-being (Martin, 1996; Karl et al., 2007). In addition, humor reduces perceived stress and the likelihood of burnout and strengthens resilience (Murden et al., 2018; Rose et al., 2021). On the other hand, humor and jokes can serve as a gateway for prejudices or to devalue other individuals (Prusaczyk and Hodson, 2020). Humor can be employed to define the status quo of a group or to maintain and consolidate the hierarchy within a team (Hodson and Prusaczyk, 2021). Interestingly, gender often plays a role regarding the negative form of humor, with women being the target of sexualized humor (Tabassum and Karakowsky, 2022).
Consider the episode in lines 33–49, where two female nurses and a male surgeon were part of what appears to be a humorous interaction. The surgeon questioned the performance of one nurse and made it sound as if she could not do her job and did not feel like doing it. He used a very colloquial formulation (“She does not feel like it anymore”) and this humorous interaction contains an ambiguity (which is typical for humor). He may have used humor to “soften” his message and to offer a more or less suitable excuse for what could otherwise be perceived as rude (Ringblom, 2022). Or, he may have used humor to put women (the nurses) in an inferior position and to maintain a gender- and/or status-based ingroup-outgroup distinction (Ringblom, 2022).
In this episode, it would be also interesting to examine the speaking up behavior of the participants. One might explore to what extent negative humor influences the speaking up behavior of the ironized group (the nurses) or the whole group and to clarify whether this behavior could be a hindrance or even beneficial for further speaking up (Parsons et al., 2001; Vauk et al., 2022).
Numerous studies on emotions, stress management, and burnout among health-care workers exist (e.g., during COVID-19 emergency (Di Giuseppe et al., 2021)) with only few studies on humor and well-being (e.g., effect of humor on nursing professionals’ well-being (Navarro-Carrillo et al., 2020)), albeit unrelated to healthcare teams. Therefore, investigating the role of humor in healthcare teams and its relation to well-being and speaking-up could not only be promising but applying the psychodynamic perspective may provide desired guidance for researchers who wish to identify emotional and nonconscious processes within teams and their impact on further interactions and performance. However, team research mainly following the psychodynamic perspective may struggle with the multiple and even conflicting socio-emotional processes, e.g., humor may have both a beneficial and obstructive impact (Tschan et al., 2015).
Scholars taking a temporal perspective assume that groups are systems that evolve over time and in which change is generic and arises across multiple time scales (Arrow et al., 2004). Their research goal is to discriminate changes that are systematic or even regular from changes that are episodic and particular. They also aim to understand how groups systematically change over time and how this group development can be described, explained and modeled (Harvey et al., 2023). On the micro level, the patterning of interaction in groups comes into focus and how these dynamics relate to relevant other factors like group performance, team member satisfaction etc.
Healthcare teams exhibit dynamics on both levels, the meso level of the dynamics of the team as a whole as well as the micro level of interaction patterns. For example, guideline-oriented teamwork as it is prevalent in resuscitation teams entrains the dynamics of the group as a whole, measurable by the degree of guideline adherence (Fernandez Castelao et al., 2015). Another example is an interaction pattern on the micro level who assumed that groups shift from behaviors focused primarily on the task to behaviors relating to the socio-emotional requirements of the group (Bales, 1950). This can be explained by Bales’ equilibrium model (Bales et al., 1953), which claims that a group must keep a balance between task-oriented and socio-emotional needs, in order to be successful. However, socio-emotional behavior might merge into CIC which, at some point, might cause distractions for team members and impair surgical outcomes (Tschan et al., 2015; Wheelock et al., 2015). Other temporal patterns found in healthcare teams are adaptation processes where implicit vs. explicit coordination mechanisms are situationally adapted to routine vs. non-routine requirements of the task (Burtscher et al., 2011; Riethmüller et al., 2012).
Consider the episode in lines 19 to 45, where we can apply the basic distinction between CRC and CIR outlined previously in the functional perspective. From the temporal perspective, we can state that this episode is composed of different micro episodes swaying from CRC and CIC communication. This shift back and forth between CRC and CIC creates a non-random interaction pattern relating systematically to task performance and well-being functions of the team. It would also be interesting to explore whether the CIC utterances in this group serve the tension-reduction function assumed in the equilibrium model (Bales, 1950) or – on the contrary – induce interpersonal conflict and thus impair team performance. Thus, researchers aiming at detecting and describing dynamic patterns in teams and relating these patterns to diverse functions of a team are recommended to apply the temporal perspective. However, research mainly driven by the temporal perspective may involve risks that such too fine-grained analyses of micro processes leaving out structural conditions on the meso (team as a whole) and macro (embedding organization, socio-political system) levels.
Scholars taking the social identity perspective assume that relations between large-scale social categories as nations, cultural groups etc. exist and analyze the cognitive aspects of self- and other-classifications of social groups and group membership (Hogg et al., 2004). Social identity is “the individual’s knowledge that he belongs to certain social groups together with some emotional and value significance to him of this group membership” (Tajfel, 1972, p. 292). These scholars’ research goal is to describe how the categorization of self and others define group memberships, the construction of group norms and the enactment of these norms in group and intergroup behavior (Turner, 1985; Turner et al., 1987; Hogg et al., 2004). For example, belonging to different professional groups impacts how healthcare team members react to inclusive language and speak up (Weller et al., 2014; Weiss et al., 2018). Even more, gender stereotypes woefully impact team interaction in the OR (Pattni et al., 2017; Minehart et al., 2020). That means, in a given situation a specific social category – in our example physician or nurse – might be salient due to the context, here the heart surgery in the operating theatre.
Consider the episode in lines 30–37, one could describe the interaction between the surgeon and the nurse(s) as an intergroup situation, primarily on the interprofessional dimension physician versus nurse. In the surgeon’s utterance “this nurse …,” the (scrub) nurse Xenia is addressed as a member of her social category. The physician addresses her not as an individual, but through the lens of the stereotype “nurse” which means the person become depersonalized. Although the nurse is present in the situation and working at the operating desk with the surgeon, she is addressed in the third person, not with her name but with her professional classification. Her colleague, the circulating nurse, immediately comes to her defense, says her name (“Xenia”) and provides cover. One could even go thus far that the circulating nurse tries to annulate the relational communication on the collective level (differentiating “we” from “them”) by trying to get back to the interpersonal level of “Xenia” interacting with the other team members. Applying the social identity perspective to analyze the excerpt, we could identify which social categories are salient in this team. Besides the interprofessional categorization – physician vs. nurse – there is also the gender-dimension, man versus women. In the ironic, sarcastic or even aggressive way the surgeon comments on the competencies of the nurse, one could even see a categorization on the dimension of hierarchy which parallels the other two dimensions. Thus, the social identity perspective provides theoretical guidance if research questions focus on the conditions and effects of identification with the team, with subteams or the discrimination or even competition toward other teams or larger social units and categories. However, research mainly based on the social identity perspective risks overlooking the variety and creativity of the behavior of team members as individual persons (rather than as members of social categories).
How team members work with one another, with other teams, with patients and their relatives impacts everybody’s well-being (Pronovost, 2013; WHO, 2021). Teams are not black boxes and exploring how team members manage teamwork in the complexity (Lingard et al., 2004) of healthcare systems will help identifying how to support them best (Kolbe and Boos, 2019; Anderson et al., 2021). Team science provides orientation, theoretical and methodological guidance, and resources for how to study teamwork. Reflecting on how we use these methodologies is important for drawing conclusions. In our perspective article we attempted to illustrate how our theoretical lens influences how we study teamwork in healthcare. It seems fascinating that a brief sequence of an operating room team conversation can be explored from many perspectives with varying foci: performance, power, identity, time and many more. Our purpose was to highlight the benefits of leaving static research behind but use the existing versatility of team theory to inspire team research in healthcare and other high responsibility domains.
Whether conscious or unconscious, our choice of a particular theoretical lens both sharpens our focus and leaves us blind to possible other phenomena. Applying the problem-gap-hook heuristic (Lingard and Watling, 2021), we hope that our illustration will provide guidance for studying teams in healthcare in identifying the problem, gap, and hook.
What is the problem that matters? Exposure to disrespectful team members? Impeded patient safety when team members do not share or listen to safety concerns? Lack of clarity on whether or how heart team meetings work? Precisely identifying the problem at hand is important because it will guide which theoretical lens(es) may fit best for studying it. For example, if in our heart surgery example (Table 1) the perceived stress and reduced well-being of the operating room team were problematic, applying not only the functional but also the conflict/power/status and psychodynamic perspectives might be fruitful and direct researchers to studying the tensions, potential toxic functions of humor and other forms of disrespectful communication in the OR (Lingard et al., 2004). Notably, the problem is not the same as the research gap.
What is already known about the problem and what is the current gap in the research, precisely? From our experience, a research review beyond the scope of one discipline and one theoretical perspective typically reveals plenty of existing research that will help sharpen the research question and methods. For example, when studying voice in healthcare teams, reviewing the voice literature in organizational behavior and psychology yields a variety of concepts, methods and results applicable to healthcare teams (Heaphy et al., 2022; Li and Tangirala, 2022). For broadening the research beyond healthcare, the dimensional model of Hagemann allows for identifying similarities, differences, and application (Hagemann et al., 2011). Notably, identifying the research gap can be a challenging step as research from different theoretical lenses and disciplines is frequently published in different kinds of journals; researchers may benefit from leaving the comfort zones of their field’s journals.
Why does the research gap and the chosen approach to closing it matter? The team research perspectives described in this article can be a considerable hook (Figure 1): A problem may be studied from a different perspective. For example, while voice in healthcare teams has typically been studied from the conflict/status/power perspective, applying a psychodynamic perspective may discover unconscious voice/silence patterns (Foulk et al., 2016). Alternatively, a problem may be studied combining different theoretical perspectives. For example, knowledge on facilitating voice in healthcare teams may be enhanced by combining the conflict/status/power with the psychodynamic perspective, linking power, status, patterns and voice communication (Weiss et al., 2017, 2018, 2023; Lemke et al., 2021). As another example, a behavioral observation study on teamwork and communication within surgical teams has shown that more case-irrelevant communication including humor during wound closure is related to worse patient outcomes, whereas case-relevant communication during the whole surgery seems to be a protective factor against surgical site infections (Tschan et al., 2015). This impressive study evolved through combining the psychodynamic, the temporal, and the functional perspectives. Further combinations of theoretical perspectives are conceivable: combining the functional with the conflict-power-status perspective may enrich our understanding of crucial relational aspects improving or undermining team effectiveness (Janss et al., 2012; Weiss et al., 2023). Combining the functional with the temporal perspective (Fernandez Castelao et al., 2015) to find out how effective and less effective behavioral patterns emerge and can be supported or avoided may be fruitful, e.g., by training or intervention. Similarly, the social identity perspective may fit well to the conflict-power-status and functional perspectives for exploring the effects of stereotyping on team and leadership effectiveness as well as on patient safety (Weller et al., 2014; Pattni et al., 2017; Minehart et al., 2020).
Thus, reflecting on which theoretical lenses we apply when studying dynamics in healthcare sharpens our focus. It sharpens what we are looking at, how we are looking at it and what literatures and methodologies we will use to inform our research (Weingart, 1997; Edmondson and Mcmanus, 2007).
Our analysis has limitations. First, there are more theoretical perspectives to studying team dynamics than we have discussed here (Poole et al., 2004). Our discussion is a starting point rather than a comprehensive exploration of each perspective. Further research is required; in particularly with respect to equity, diversity and inclusion in healthcare teams (Rosenkranz et al., 2021). For example, combining the psychodynamic with the so-called feminist perspective might yield important insights into how gender and privilege are enacted in team interaction (Minehart et al., 2020; Tramèr et al., 2020; Hochstrasser et al., 2022; Zwicky et al., 2022).
Second, we did not discuss why some theoretical perspectives (e.g., functional perspective) may, explicitly or implicitly, have been used more often than others (e.g., temporal perspective). Methodical constraints and required effort in accessing temporal data may play a significant role and new advances in collecting temporal team interaction may help (Weiss et al., 2023). Third, particularly the science of healthcare teams has to factor in two seemingly distinct mindsets of what constitutes “good data”: On the one hand, psychological and team science involve expertise in recording and describing social phenomena, such as perceptions, attitudes, or behavior in teams (Weingart, 1997; Brauner et al., 2018). Valid measurement instruments are developed to measure these data precisely and to be able to use them in behavioral observations, surveys/questionnaires, and interviews. This type of data collection may at first seem unusual to medical researchers, who, on the other hand, rely on more “objective” data such as physiological values. On the other hand, medical science considers randomized clinical trials the state of the art (Benson and Hartz, 2000). They may represent a particular form of the functional perspective and explain why much research on healthcare teams does indeed apply a functional perspective. In our view, it is precisely the diversity of interdisciplinary methods that would allow for other, new angles for research. Studying healthcare teams by translating and applying methods from medicine and nursing, organizational behavior, psychology, mechanical engineering and informatics seems now easier than a decade ago and allows for new avenues and methodologies for studying healthcare team dynamics (Rosen et al., 2014, 2018; Hałgas et al., 2023; Weiss et al., 2023). While we are aware of the enormous effort involved in planning, conducting and analyzing healthcare team research with any of the discussed perspectives, we believe in their potential for improving teamwork and patient care.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Open access funding was provided by ETH Zurich.
The authors would like to thank Jan Lehrke for transcribing and coding the conversation, and Paul J. Pritz for language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Anderson, J. E., Lavelle, M., and Reedy, G. (2021). Understanding adaptive teamwork in health care: Progress and future directions. J. Health Serv. Res. Policy 26, 208–214. doi: 10.1177/1355819620978436
Arrow, H., Poole, M. S., Henry, K. B., Wheelan, S., and Moreland, R. (2004). Time, change, and development: the temporal perspective on groups. Small Group Res. 35, 73–105. doi: 10.1177/1046496403259757
Bales, RF. Interaction process analysis: a method for the study of small groups. Oxford, UK: Addison-Wesley (1950).
Bales, RF, Parsons, T, and Shils, E. Working papers in the theory of action. New York Free Press (1953).
Benson, K., and Hartz, A. J. (2000). A comparison of observational studies and randomized, controlled trials. N. Engl. J. Med. 342, 1878–1886. doi: 10.1056/NEJM200006223422506
Brauner, E, Boos, M, and Kolbe, M, eds. The Cambridge handbook of group interaction analysis. Cambridge: Cambridge University Press (2018)
Burtscher, M. J., Manser, T., Kolbe, M., Grote, G., Grande, B., Spahn, D. R., et al. (2011). Adaptation in anaesthesia team coordination in response to a simulated critical event and its relationship to clinical performance. Br. J. Anaesth. 106, 801–806. doi: 10.1093/bja/aer039
Crowe, J., Allen, J. A., and Lehmann-Willenbrock, N. (2016). “Humor in workgroups and teams” in The psychology of humor at work (New York, NY: Routledge), 108–120.
Di Giuseppe, M., Nepa, G., Prout, T. A., Fabrizio, M. S., Orrù, G., and Conversano, C. (2021). Stress, burnout, and resilience among healthcare workers during the COVID-19 emergency: the role of defense mechanisms. Int. J. Environ. Res. Public Health 18:5258. doi: 10.3390/ijerph18105258
Edmondson, A. C. (2003). Speaking up in the operating room: how team leaders promote learning in interdisciplinary action teams. J. Manag. Stud. 40, 1419–1452. doi: 10.1111/1467-6486.00386
Edmondson, A. C., and Mcmanus, S. E. (2007). Methodological fit in management field research. Acad. Manag. Rev. 32, 1246–1264. doi: 10.5465/amr.2007.26586086
Eichbaum, Q. (2018). Collaboration and teamwork in the health professions: rethinking the role of conflict. Acad. Med. 93, 574–580. doi: 10.1097/ACM.0000000000002015
El-Shafy, I. A., Delgado, J., Akerman, M., Bullaro, F., Christopherson, N. A. M., and Prince, J. M. (2018). Closed-loop communication improves task completion in pediatric trauma resuscitation. J. Surg. Educ. 75, 58–64. doi: 10.1016/j.jsurg.2017.06.025
Fernandez Castelao, E., Boos, M., Ringer, C., Eich, C., and Russo, S. G. (2015). Effect of CRM team leader training on team performance and leadership behavior in simulated cardiac arrest scenarios: a prospective, randomized, controlled study. BMC Med. Educ. 15, 1–8. doi: 10.1186/s12909-015-0389-z
Fernandez Castelao, E., Russo, S. G., Cremer, S., Strack, M., Kaminski, L., Eich, C., et al. (2011). Positive impact of crisis resource management training on no-flow time and team member verbalisations during simulated cardiopulmonary resuscitation: a randomized controlled trial. Resuscitation 82, 1338–1343. doi: 10.1016/j.resuscitation.2011.05.009
Fernandez Castelao, E., Russo, S. G., Riethmüller, M., and Boos, M. (2013). Effects of team coordination during cardiopulmonary resuscitation: a systematic review of the literature. J. Crit. Care 28, 504–521. doi: 10.1016/j.jcrc.2013.01.005
Fortune, PM, Davis, M, Hanson, J, and Phillips, B. Human factors in the health care setting: a pocket guide for clinical instructors. New York John Wiley & Sons; (2012)
Foulk, T., Woolum, A., and Erez, A. (2016). Catching rudeness is like catching a cold: the contagion effects of low-intensity negative behaviors. J. Appl. Psychol. 101, 50–67. doi: 10.1037/apl0000037
Gardezi, F., Lingard, L., Espin, S., Whyte, S., Orser, B., and Baker, G. R. (2009). Silence, power and communication in the operating room. J. Adv. Nurs. 65, 1390–1399. doi: 10.1111/j.1365-2648.2009.04994.x
Hagemann, V., Kluge, A., and Ritzmann, S. (2011). High Responsibility Teams-Eine systematische Analyse von Teamarbeitskontexten für einen effektiven Kompetenzerwerb. J. Psychol. Alltagshandelns. 4, 22–42.
Hałgas, E. A., van Eijndhoven, K. H. J., Gevers, J. M. P., Wiltshire, T. J., Westerink, J. H. D. M., and Rispens, S. (2023). A review of using wearable technology to assess team functioning and performance. Small Group Res. 54, 41–76. doi: 10.1177/10464964221125717
Härgestam, M., Lindkvist, M., Brulin, C., Jacobsson, M., and Hultin, M. (2013). Communication in interdisciplinary teams: exploring closed-loop communication during in situ trauma team training. BMJ Open 3:e003525. doi: 10.1136/bmjopen-2013-003525
Harvey, J.-F., Cromwell, J. R., Johnson, K. J., and Edmondson, A. C. (2023). The dynamics of team learning: harmony and rhythm in teamwork arrangements for innovation. Adm. Sci. Q. doi: 10.1177/00018392231166635
Heaphy, E., Lilius, J., and Feldman, E. (2022). Moved to speak up: how prosocial emotions influence the employee voice process. Hum. Relat. 75, 1113–1139. doi: 10.1177/00187267211007539
Hochstrasser, S. R., Amacher, S. A., Tschan, F., Semmer, N. K., Becker, C., Metzger, K., et al. (2022). Gender-focused training improves leadership of female medical students: a randomised trial. Med. Educ. 56, 321–330. doi: 10.1111/medu.14658
Hodson, G., and Prusaczyk, E. (2021). “Cavalier humor beliefs: dismissing jokes as ‘just jokes’ facilitates prejudice and internalizes negativity among targets” in The social psychology of humor. eds. M. Strick and T. E. Ford (New York: Routledge/Taylor & Francis), 170–188.
Hogg, M. A., Abrams, D., Otten, S., and Hinkle, S. (2004). The social identity perspective: intergroup relations, self-conception, and small groups. Small Group Res. 35, 246–276. doi: 10.1177/1046496404263424
Hollenbeck, J. R., Beersma, B., and Schouten, M. E. (2012). Beyond team types and taxonomies: a dimensional scaling conceptualization for team description. Acad. Manag. Rev. 37, 82–106. doi: 10.5465/amr.2010.0181
Hollingshead, A. B., Wittenbaum, G. M., Paulus, P. B., Hirokawa, R. Y., Ancona, D. G., Peterson, R. S., et al. (2005). “A look at groups from the functional perspective” in Theories of small groups: Interdisciplinary perspectives. eds. M. S. Poole and A. B. Hollingshead (Thousand Oaks, CA: Sage Publications, Inc), 21–62.
Janss, R., Rispens, S., Segers, M., and Jehn, K. A. (2012). What is happening under the surface? Power, conflict and the performance of medical teams. Med. Educ. 46, 838–849. doi: 10.1111/j.1365-2923.2012.04322.x
Kämmer, J. E., and Ewers, M. (2022). Stereotypes of experienced health professionals in an interprofessional context: results from a cross-sectional survey in Germany. J. Interprof. Care 36, 350–361. doi: 10.1080/13561820.2021.1903405
Karl, K. A., Peluchette, J. V., and Harland, L. (2007). Is fun for for everyone? Personality differences in healthcare providers' attitudes toward fun. J. Health Hum. Serv. Adm. 29, 409–447.
Kolbe, M., and Boos, M. (2019). Laborious but elaborate: the benefits of really studying team dynamics. Front. Psychol. 10, 1–16. doi: 10.3389/fpsyg.2019.01478
Kolbe, M., Boos, M., Stein, A., and Strack, M. (2016). SYNSEG—Eine Methode zur syntaxgeleiteten Segmentierung von Kodiereinheiten für die Analyse von Gruppenprozessen. Gruppe Interaktion Organisation Zeitschrift für Angewandte Organisationspsychologie (GIO). 47, 335–344. doi: 10.1007/s11612-016-0345-3
Kolbe, M., and Grande, B. (2013). Team coordination during cardiopulmonary resuscitation. J. Crit. Care 28, 522–523. doi: 10.1016/j.jcrc.2013.03.009
Kolbe, M., Grande, B., Marty, A., Manka, R., Taramasso, M., Nietlispach, F., et al. (2019). Making heart team discussions work. Struct. Heart. 3, 100–103. doi: 10.1080/24748706.2019.1572254
Kolbe, M., Grote, G., Waller, M. J., Wacker, J., Grande, B., and Burtscher, M. (2014). Monitoring and talking to the room: autochthonous coordination patterns in team interaction and performance. J. Appl. Psychol. 99, 1254–1267. doi: 10.1037/a0037877
Koopman, J., Lanaj, K., Lee, Y. E., Alterman, V., Bradley, C., and Stoverink, A. C. (2023). Walking on eggshells: a self-control perspective on workplace political correctness. J. Appl. Psychol. 108, 425–445. doi: 10.1037/apl0001025
Krenz, H., Burtscher, M. J., Grande, B., and Kolbe, M. (2020). Nurses’ voice: the role of hierarchy and leadership. Leadersh. Health Serv. 33, 12–26. doi: 10.1108/LHS-07-2019-0048
Krenz, H. L., Burtscher, M. J., and Kolbe, M. (2019). “Not only hard to make but also hard to take:” team leaders’ reactions to voice. Gr. Interakt. Org. 50, 3–13. doi: 10.1007/s11612-019-00448-2
Künzle, B., Kolbe, M., and Grote, G. (2010). Ensuring patient safety through effective leadership behaviour: a literature review. Safety Sci. 48, 1–17. doi: 10.1016/j.ssci.2009.06.004
Lehrke, J., Boos, M., Cordes, A., Leitsmann, C., and Friedrich, M. (2022). Effects of a technical solution on stress of surgical staff in operating theatres. Thorac. Cardiovasc. Surg. 70, 392–400. doi: 10.1055/s-0041-1741059
Leitsmann, C., Uhlig, A., Popeneciu, I. V., Boos, M., Ahyai, S. A., Schmid, M., et al. (2021). The silent operation theatre optimisation system (SOTOS©) to reduce noise pollution during da Vinci robot-assisted laparoscopic radical prostatectomy. J. Robot. Surg. 15, 519–527. doi: 10.1007/s11701-020-01135-x
Lemke, R., Burtscher, M. J., Seelandt, J. C., Grande, B., and Kolbe, M. (2021). Associations of form and function of speaking up in anaesthesia: a prospective observational study. Br. J. Anaesth. 127, 971–980. doi: 10.1016/j.bja.2021.08.014
Li, A. N., and Tangirala, S. (2022). How employees’ voice helps teams remain resilient in the face of exogenous change. J. Appl. Psychol. 107, 668–692. doi: 10.1037/apl0000874
Lingard, L., Garwood, S., and Poenaru, D. (2004). Tensions influencing operating room team function: does institutional context make a difference? Med. Educ. 38, 691–699. doi: 10.1111/j.1365-2929.2004.01844.x
Lingard, L., Regehr, G., Cartmill, C., Orser, B., Espin, S., Bohnen, J., et al. (2011). Evaluation of a preoperative team briefing: a new communication routine results in improved clinical practice. BMJ Qual. Saf. 20, 475–482. doi: 10.1136/bmjqs.2009.032326
Lingard, L., Regehr, G., Orser, B., Reznick, R., Baker, G. R., Doran, D., et al. (2008). Evaluation of a preoperative checklist and team briefing among surgeons, nurses, and anesthesiologists to reduce failures in communication. Arch. Surg. 143, 12–7; discussion 18. doi: 10.1001/archsurg.2007.21
Lingard, L., Reznick, R., Espin, S., Regehr, G., and DeVito, I. (2002). Team communication in the operating room: talk patterns, sites of tension, and implications for novices. Acad. Med. 77, 232–237. doi: 10.1097/00001888-200203000-00013
Lingard, L., and Watling, C. (2021). “Problem/gap/hook introductions” in Story, not study: 30 brief lessons to inspire health researchers as writers (Cham: Springer International Publishing), 7–14.
Long, J., Jowsey, T., Garden, A., Henderson, K., and Weller, J. (2020). The flip side of speaking up: a new model to facilitate positive responses to speaking up in the operating theatre. Br. J. Anaesth. 125, 1099–1106. doi: 10.1016/j.bja.2020.08.025
Magix Software GmbH (2017). The Magix Samplitude Music Studio. Available at: https://www.magix.com/de/unternehmen/
Manser, T. (2009). Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol. Scand. 53, 143–151. doi: 10.1111/j.1399-6576.2008.01717.x
Martin, R. (1996). Humour as therapeutic play: stress-moderating effects of sense of humour. J. Leisurab. Ont. 23, 8–15.
Marzuki, E., Rohde, H., Cummins, C., Branigan, H., Clegg, G., Crawford, A., et al. (2019). Closed-loop communication during out-of-hospital resuscitation: are the loops really closed? Commun. Med. 16, 54–66. doi: 10.1558/cam.37034
Mcleod, P. L., and Kettner-Polley, R. B. (2004). Contributions of psychodynamic theories to understanding small groups. Small Group Res. 35, 333–361. doi: 10.1177/1046496404264973
Microsoft Corporation (2018). Microsoft Excel. Availabel at: https://office.microsoft.com/excel
Minehart, R. D., Foldy, E. G., Long, J. A., and Weller, J. M. (2020). Challenging gender stereotypes and advancing inclusive leadership in the operating theatre. Br. J. Anaesth. 124, e148–e154. doi: 10.1016/j.bja.2019.12.015
Murden, F., Bailey, D., Mackenzie, F., Oeppen, R., and Brennan, P. (2018). The impact and effect of emotional resilience on performance: an overview for surgeons and other healthcare professionals. Br. J. Oral Maxillofac. Surg. 56, 786–790. doi: 10.1016/j.bjoms.2018.08.012
Navarro-Carrillo, G., Torres-Marín, J., Corbacho-Lobato, J. M., and Carretero-Dios, H. (2020). The effect of humour on nursing professionals’ psychological well-being goes beyond the influence of empathy: a cross-sectional study. Scand. J. Caring Sci. 34, 474–483. doi: 10.1111/scs.12751
Nemeth, CP. Improving healthcare team communication: Building on lessons from aviation and aerospace. Farnham Ashgate (2008).
Newirth, J. (2006). Jokes and their relation to the unconscious: humor as a fundamental emotional experience. Psychoanal. Dialogues 16, 557–571.
Oberfrank, S. M., Rall, M., Dieckmann, P., Kolbe, M., and Gaba, D. M. (2019). “Patient simulation” in Miller’s anesthesia. eds. M. A. Gropper, L. I. Eriksson, L. A. Fleisher, J. P. Wiener-Kronish, N. H. Cohen, and K. Leslie (Atlanta: Elsevier)
Paige, J., Garbee, D., Yu, Q., Kiselov, V., Rusnak, V., and Detiege, P. (2019). Moving along: team training for emergency room trauma transfers (T2ERT2). J. Surg. Educ. 76, 1402–1412. doi: 10.1016/j.jsurg.2019.03.013
Parsons, G. N., Kinsman, S. B., Bosk, C. L., Sankar, P., and Ubel, P. A. (2001). Between two worlds: medical student perceptions of humor and slang in the hospital setting. J. Gen. Intern. Med. 16, 544–549. doi: 10.1046/j.1525-1497.2001.016008544.x
Pattni, N., Bould, M. D., Hayter, M. A., McLuckie, D., Noble, L. M. K., Malavade, A., et al. (2017). Gender, power and leadership: the effect of a superior's gender on respiratory therapists’ ability to challenge leadership during a life-threatening emergency. Br. J. Anaesth. 119, 697–702. doi: 10.1093/bja/aex246
Pearce, S., Watts, F., Watkin, A., Walshe, K., and Boaden, R. (2006). “Team performance, communication and patient safety” in Patient safety: research into practice. eds. K. Walshe and R. Boaden (Berkshire: Open University Press), 208–216.
Poole, M. S., Hollingshead, A. B., McGrath, J. E., Moreland, R. L., and Rohrbaugh, J. (2004). Interdisciplinary perspectives on small groups. Small Group Res. 35, 3–16. doi: 10.1177/1046496403259753
Pronovost, P. (2013). “Teamwork matters” in Developing and enhancing teamwork in organizations: evidence-based best practices and guidelines. eds. E. Salas, S. I. Tannenbaum, D. Cohen, and G. Latham (San Francisco, CA: Jossey-Bass), 11–12.
Prusaczyk, E., and Hodson, G. (2020). “To the moon, Alice”: cavalier humor beliefs and women's reactions to aggressive and belittling sexist jokes. J. Exp. Soc. Psychol. 88:103973. doi: 10.1016/j.jesp.2020.103973
Raemer, D. B., Kolbe, M., Minehart, R. D., Rudolph, J. W., and Pian-Smith, M. (2016). Improving anesthesiologists’ ability to speak up in the operating room: a randomized controlled experiment of a simulation-based intervention and a qualitative analysis of hurdles and enablers. Acad. Med. 91, 530–539. doi: 10.1097/ACM.0000000000001033
Rall, M., Glavin, R., and Flin, R. (2008). The ‘10-seconds-for-10-minutes principle’ – why things go wrong and stopping them getting worse. Bull. R. Coll. Anaesth. 51, 2614–2616.
Riethmüller, M., Fernandez Castelao, E., Eberhardt, I., Timmermann, A., and Boos, M. (2012). Adaptive coordination development in student anaesthesia teams: a longitudinal study. Ergonomics 55, 55–68. doi: 10.1080/00140139.2011.636455
Ringblom, L. (2022). “It is just a joke!” informal interaction and gendered processes underground. NORA-Nordic J. Femin. Gen. Res. 30, 94–107. doi: 10.1080/08038740.2021.2009028
Rogers, L., De Brún, A., Birken, S. A., Davies, C., and McAuliffe, E. (2020). The micropolitics of implementation; a qualitative study exploring the impact of power, authority, and influence when implementing change in healthcare teams. BMC Health Serv. Res. 20:1059. doi: 10.1186/s12913-020-05905-z
Rose, S., Hartnett, J., and Pillai, S. (2021). Healthcare worker’s emotions, perceived stressors and coping mechanisms during the COVID-19 pandemic. PLoS One 16:e0254252. doi: 10.1371/journal.pone.0254252
Rosen, M. A., DiazGranados, D., Dietz, A. S., Benishek, L. E., Thompson, D., Pronovost, P. J., et al. (2018). Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am. Psychol. 73, 433–450. doi: 10.1037/amp0000298
Rosen, M. A., Dietz, A. S., and Kazi, S. (2018). “Beyond coding interaction” in The Cambridge handbook of group interaction analysis. eds. E. Brauner, M. Boos, and M. Kolbe (Cambridge: Cambridge University Press), 142–162.
Rosen, M. A., Dietz, A. S., Yang, T., Priebe, C. E., and Pronovost, P. J. (2014). An integrative framework for sensor-based measurement of teamwork in healthcare. J. Am. Med. Inform. Assoc. 22, 11–18. doi: 10.1136/amiajnl-2013-002606
Rosenkranz, K. M., Arora, T. K., Termuhlen, P. M., Stain, S. C., Misra, S., Dent, D., et al. (2021). Diversity, equity and inclusion in medicine: why it matters and how do we achieve it? J. Surg. Educ. 78, 1058–1065. doi: 10.1016/j.jsurg.2020.11.013
Russ, S., Rout, S., Caris, J., Mansell, J., Davies, R., Mayer, E., et al. (2015). Measuring variation in use of the WHO surgical safety checklist in the operating room: a multicenter prospective cross-sectional study. J. Am. Coll. Surg. 220, 1–11e4. doi: 10.1016/j.jamcollsurg.2014.09.021
Salas, E., Wilson, K. A., Murphy, C. E., King, H., and Salisbury, M. (2008). Communicating, coordinating, and cooperating when lives depend on it: tips for teamwork. Jt. Comm. J. Qual. Patient Saf. 34, 333–341. doi: 10.1016/S1553-7250(08)34042-2
Schmutz, J. B., Lei, Z., Eppich, W. J., and Manser, T. (2018). Reflection in the heat of the moment: the role of in-action team reflexivity in health care emergency teams. J. Organ. Behav. 39, 749–765. doi: 10.1002/job.2299
Schmutz, J., and Manser, T. (2013). Do team processes really have an effect on clinical performance? A systematic literature review. Br. J. Anaesth. 110, 529–544. doi: 10.1093/bja/aes513
Schmutz, J. B., Meier, L. L., and Manser, T. (2019). How effective is teamwork really? The relationship between teamwork and performance in healthcare teams: a systematic review and meta-analysis. BMJ Open 9:e028280. doi: 10.1136/bmjopen-2018-028280
Seelandt, J. C., Tschan, F., Keller, S., Beldi, G., Jenni, N., Kurmann, A., et al. (2014). Assessing distractors and teamwork during surgery: developing an event-based method for direct observation. BMJ Q. Saf. Healthcare 23, 918–929. doi: 10.1136/bmjqs-2014-002860
Sell, J., Lovaglia, M. J., Mannix, E. A., Samuelson, C. D., and Wilson, R. K. (2004). Investigating conflict, power, and status within and among groups. Small Group Res. 35, 44–72. doi: 10.1177/1046496403259813
St. Pierre, M, Hofinger, G, Buerschaper, C, and Simon, R. Crisis management in acute care settings. New York Springer (2011)
Tabassum, A., and Karakowsky, L. (2022). Do you know when you are the punchline? Gender-based disparagement humor and target perceptions. Gen. Manag. 38, 273–286. doi: 10.1108/GM-01-2021-0026
Tajfel, H. (1972). “Social stereotypes and social groups” in Introduction à la psychologie sociale. ed. S. Moscovici (Paris: Larousse), 272–302.
Taplin, S. H., Weaver, S., Chollette, V., Marks, L. B., Jacobs, A., Schiff, G., et al. (2015). Teams and teamwork during a cancer diagnosis: interdependency within and between teams. J. Oncol. Pract. 11, 231–238. doi: 10.1200/JOP.2014.003376
Tramèr, L., Becker, C., Schumacher, C., Beck, K., Tschan, F., Semmer, N. K., et al. (2020). Association of self-esteem, personality, stress and gender with performance of a resuscitation team: a simulation-based study. PLoS One 15:e0233155. doi: 10.1371/journal.pone.0233155
Tschan, F. (1995). Communication enhances small group performance if it confirms to task requirements: the concept of ideal communication cycles. Basic Appl. Soc. Psychol. 17, 371–393. doi: 10.1207/s15324834basp1703_6
Tschan, F. (2002). Ideal cycles of communication (or cognitions) in triads, dyads, and individuals. Small Group Res. 33, 615–643. doi: 10.1177/1046496402238618
Tschan, F., Seelandt, J. C., Keller, S., Semmer, N. K., Kurmann, A., Candinas, D., et al. (2015). Impact of case-relevant and case-irrelevant communication within the surgical team on surgical-site infection. Br. J. Surg. 102, 1718–1725. doi: 10.1002/bjs.9927
Tschan, F., Semmer, N. K., Hunziker, S., Kolbe, M., Jenni, N., and Marsch, S. U. (2014). Leadership in different resuscitation situations. Trends Anaesth. Crit. Care 4, 32–36. doi: 10.1016/j.tacc.2013.12.001
Tucker, A. L., and Edmondson, A. (2003). Why hospitals don't learn from failures. Calif. Manag. Rev. 45, 55–72. doi: 10.2307/41166165
Turner, J. C. (1985). “Social categorization and the self-concept: a social cognitive theory of group behavior” in Advances in group processes: theory and research. ed. E. J. Lawler, vol. 2 (Greenwich, CT: JAI Press), 77–122.
Turner, JC, Hogg, MA, Oakes, PJ, Reicher, SD, and Wetherell, MS. Rediscovering the social group: a self-categorization theory. Oxford, England: Blackwell; (1987).
Vauk, S., Seelandt, J. C., Huber, K., Grande, B., and Kolbe, M. (2022). Exposure to incivility does not hinder speaking up: a randomised, controlled high-fidelity simulation-based study. Br. J. Anaesth. 129, 776–787. doi: 10.1016/j.bja.2022.07.050
Weingart, L. R. (1997). How did they do that? The ways and means of studying group process. Res. Organ. Behav. 19, 189–239.
Weiss, M., Kolbe, M., Grote, G., Spahn, D. R., and Grande, B. (2017). Why didn’t you say something? Using after-event reviews to affect voice behavior and hierarchy beliefs in multi-professional action teams. Eur. J. Work Organ. Psy. 26, 66–80. doi: 10.1080/1359432X.2016.1208652
Weiss, M., Kolbe, M., Grote, G., Spahn, D. R., and Grande, B. (2018). We can do it! Inclusive leader language promotes voice behavior in multi-professional teams. Leader. Q. 29, 389–402. doi: 10.1016/j.leaqua.2017.09.002
Weiss, K., Kolbe, M., Lohmeyer, Q., and Meboldt, M. (2023). Measuring teamwork for training in healthcare using eye tracking and pose estimation. Front. Psychol. 14:1169940. doi: 10.3389/fpsyg.2023.1169940
Weiss, K. E., Kolbe, M., Nef, A., Grande, B., Kalirajan, B., Meboldt, M., et al. (2023). Data-driven resuscitation training using pose estimation. Adv. Simul. 8:12. doi: 10.1186/s41077-023-00251-6
Weiss, M., Morrison, E. W., and Szyld, D. (2023). I like what you are saying, but only if i feel safe: psychological safety moderates the relationship between voice and perceived contribution to healthcare team effectiveness. Front. Psychol. 14:1129359. doi: 10.3389/fpsyg.2023.1129359
Weller, J., Boyd, M., and Cumin, D. (2014). Teams, tribes and patient safety: overcoming barriers to effective teamwork in healthcare. Postgrad. Med. J. 90, 149–154. doi: 10.1136/postgradmedj-2012-131168
Wheelock, A., Suliman, A., Wharton, R., Babu, E. D., Hull, L., Vincent, C., et al. (2015). The impact of operating room distractions on stress, workload, and teamwork. Ann. Surg. 261, 1079–1084. doi: 10.1097/SLA.0000000000001051
WHO. Global patient safety action plan 2021–2030. Towards eliminating avoidable harm in health care. (2021) Geneva, Switzerland: WHO
Widmer, L. W., Keller, S., Tschan, F., Semmer, N. K., Holzer, E., Candinas, D., et al. (2018). More than talking about the weekend: content of case-irrelevant communication within the OR team. World J. Surg. 42, 2011–2017. doi: 10.1007/s00268-017-4442-4
Willmes, M., Sellmann, T., Semmer, N., Tschan, F., Wetzchewald, D., Schwager, H., et al. (2022). Impact of family presence during cardiopulmonary resuscitation on team performance and perceived task load: a prospective randomised simulator-based trial. BMJ Open 12:e056798. doi: 10.1136/bmjopen-2021-056798
Yule, S., Flin, R., Paterson-Brown, S., and Maran, N. (2006). Non-technical skills for surgeons in the operating room: a review of the literature. Surgery 139, 140–149. doi: 10.1016/j.surg.2005.06.017
Keywords: healthcare teams, theoretical perspectives, interaction analysis, group dynamics, small group research
Citation: Seelandt JC, Boos M, Kolbe M and Kämmer JE (2023) How to enrich team research in healthcare by considering five theoretical perspectives. Front. Psychol. 14:1232331. doi: 10.3389/fpsyg.2023.1232331
Edited by:
Tayana Soukup, Imperial College London, United KingdomReviewed by:
Vera Hagemann, University of Bremen, GermanyCopyright © 2023 Seelandt, Boos, Kolbe and Kämmer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michaela Kolbe, bWtvbGJlQGV0aHouY2g=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.