
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 22 December 2023
Sec. Psychology for Clinical Settings
Volume 14 - 2023 | https://doi.org/10.3389/fpsyg.2023.1200685
 Juan P. Sanabria-Mazo1,2,3†
Juan P. Sanabria-Mazo1,2,3† Ariadna Colomer-Carbonell1,2,3†
Ariadna Colomer-Carbonell1,2,3† Óscar Fernández-Vázquez1,4
Óscar Fernández-Vázquez1,4 Georgina Noboa-Rocamora1,4
Georgina Noboa-Rocamora1,4 Gemma Cardona-Ros1
Gemma Cardona-Ros1 Lance M. McCracken5
Lance M. McCracken5 Antonio Montes-Pérez6
Antonio Montes-Pérez6 Juan R. Castaño-Asins6Sílvia Edo2
Juan R. Castaño-Asins6Sílvia Edo2 Xavier Borràs2,3
Xavier Borràs2,3 Antoni Sanz2
Antoni Sanz2 Albert Feliu-Soler3,7
Albert Feliu-Soler3,7 Juan V. Luciano1,3,7*
Juan V. Luciano1,3,7*Objective: Chronic pain frequently co-occurs with clinically relevant psychological distress. A systematic review was conducted to identify the efficacy of cognitive behavioral therapy-based interventions for patients with these comorbid conditions.
Methods: The systematic search was carried out in Medline, PsycINFO, Web of Science, and Scopus up to March 18th, 2023. Four reviewers independently conducted screenings, extraction, and quality assessment.
Results: Twelve randomized controlled trials and one non-randomized controlled trial involving 1,661 participants that examined the efficacy of Cognitive Behavioral Therapy (nine studies), Mindfulness-based Interventions (three studies), Acceptance and Commitment Therapy (one study), and Behavioral Activation Therapy for Depression (one study) were included. Compared to treatment as usual, six out of eight studies of traditional Cognitive Behavioral Therapy reported significant differences in the reduction of depressive symptoms at post-treatment (d from 1.31 to 0.18) and four out of six at follow-up (d from 0.75 to 0.26); similarly, five out of six reported significant differences in the reduction of anxiety symptoms at post-treatment (d from 1.08 to 0.19) and three out of four at follow-up (d from 1.07 to 0.27). Overall, no significant differences between traditional Cognitive Behavioral Therapy and treatment as usual were reported at post-treatment and follow-up in the studies exploring pain intensity and pain catastrophizing.
Conclusion: The available evidence suggests that traditional Cognitive Behavioral Therapy may produce significant benefits for the improvement of depression, anxiety, and quality of life, but not for pain intensity and pain catastrophizing. More evidence is needed to determine the effects of MBI, ACT, and BATD.
Systematic review registration: PROSPERO, CRD42021219921.
Chronic pain and psychological distress are common health conditions (Wittchen et al., 2011) with substantial healthcare and social impacts (Chopra and Arora, 2014). The prevalence of chronic pain ranges from 10% to 30% worldwide (Reid et al., 2011), generating a significant public health demand and economic burden (Baumeister et al., 2012). According to epidemiological studies, comorbidity between chronic pain and psychological distress in clinical practice is higher than 60% (Walker et al., 2014). Since this comorbidity is more treatment-resistant than either condition alone (Mansfield et al., 2016) and it generates a significant impact on the quality of life of patients with these conditions (McCracken et al., 2022), it has been considered a growing target for treatment in recent years (McCracken, 2023). The concurrent appearance of chronic pain and significant psychological distress is striking and requires attention from researchers, clinicians, and policymakers, as well as demands effective management strategies to improve the health and well-being of those affected by these conditions (Snyder and Handrup, 2018).
Due to the complexity and multifaceted nature of the construct, many definitions for psychological distress have been proposed in recent years. One of the most widely accepted defines this psychological construct as “state of emotional suffering characterized by the undifferentiated combinations of symptoms of depression (e.g., lost interest, sadness, hopelessness) and anxiety (e.g., restlessness, feeling tense) which are sometimes accompanied by somatic symptoms (e.g., insomnia, headaches, lack of energy)” (Drapeau et al., 2012, p. 125). Generally, psychological distress refers to a range of unpleasant emotional and mental experiences that can impact a person’s well-being and ability to function (Bisby et al., 2022; Gasslander et al., 2022). It is also considered a dimensional construct that has been truncated in most studies to employ it as a categorical construct to establish when it is or is not “clinically relevant,” with relevant meaning that scores on psychopathological measures exceed specific cut-off points.
Previous studies demonstrate that people with chronic pain are more likely to experience psychological distress, such as anxiety and depression, and individuals with psychological distress are more likely to report chronic pain (Rayner et al., 2016). The relationship between chronic pain and psychological distress is complex and bidirectional (Wittchen et al., 2011). The multidimensional nature of both chronic pain and psychological distress, with sensory, affective, and behavioral dimensions, is a challenge for intervention design and delivery (Roberts et al., 2018). Specifically, the presence of psychological distress in patients with chronic pain increases pain complaints and reduces quality of life (Snyder and Handrup, 2018). Comorbidity between psychological distress and chronic pain generates a higher degree of functional impairment than the presence of either condition alone (Mansfield et al., 2016) and negatively influences the response to pharmacological and non-pharmacological treatments (Kroenke et al., 2011). Chronic pain and clinical psychological distress involve shared neurobiological and psychosocial processes (Hooten, 2016).
Cognitive Behavioral Therapy (CBT) is the most applied psychological approach to chronic pain (McCracken, 2023). Different forms of CBT are frequently applied in chronic pain and related conditions (e.g., anxiety and/or depression), appearing effective when explored independently (Churchill et al., 2013; Cuijpers et al., 2013; Buhrman et al., 2016; Pasarelu et al., 2017). Traditional CBT has beneficial effects in adults with chronic pain (Williams et al., 2020) and is also effective in patients with emotional disorders (Lorenzo-Luaces et al., 2018; López-López et al., 2019). Concretely, recent evidence shows that Mindfulness-based Interventions (MBI), Dialectical Behavior Therapy (DBT), Rational Emotive Behavior Therapy (REBT), Acceptance and Commitment Therapy (ACT), and Behavioral Activation Therapy for Depression (BATD) also produce positive effects in patients with chronic pain (Jorn, 2015; Veehof et al., 2016; Hughes et al., 2017; Boersma et al., 2019; Khoo et al., 2019; Gloster et al., 2020; Pardos-Gascón et al., 2021).
Although the above-mentioned CBT-based interventions have generally demonstrated evidence in the management of chronic pain and related conditions, their specific efficacy in patients with comorbid pain and clinical psychological distress has been scarcely assessed. It appears that this is the first systematic review that aims to examine the efficacy of CBT-based interventions for comorbid chronic pain and clinically relevant psychological distress. Since chronic pain and psychological distress frequently co-occur, worsen one another, and resist therapy effects when they are both present, identifying effective CBT-based interventions for this complex set of conditions is critical work. In this systematic review, randomized controlled trials (RCTs) and non-randomized trials (non-RCTs) were selected for patients with chronic pain plus clinically relevant psychological distress, comparing CBT-based interventions to control conditions (active or inactive). Additionally, this research explored the risk of bias (RoB) of the included studies to assess their methodological quality.
This systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA; Page et al., 2021). The review protocol was registered in the Prospective Register of Systematic Reviews (PROSPERO), under identification number CRD42021219921. Supplementary Table S1 indicates some adjustments incorporated into the protocol of this systematic review and includes the PRISMA checklist.
To reduce publication bias, published and unpublished clinical trials were examined. For exploration of published clinical trials, searches were conducted in four electronic databases: Medline (PubMed), Web of Science (Core Collection), PsycINFO (ProQuest), and Scopus (Elsevier). The search strategy identified studies that included combinations of the population terms and the specific terms of psychological therapies. The search terms were selected according to a validation by experts and a review of the search strategies used in previous systematic reviews on CBT-based interventions for chronic pain (Lin et al., 2019; Williams et al., 2020; White et al., 2022). The specific Boolean searches were adjusted according to the Peer Review of Electronic Search Strategies (PRESS) guideline statement (McGowan et al., 2016). The following limits and filters were activated in all databases if possible: publication date (from inception until March 18th, 2023), type of publication (only studies of interest), species (humans), and languages (English and Spanish). The bibliographic database searches are detailed in Table 1.
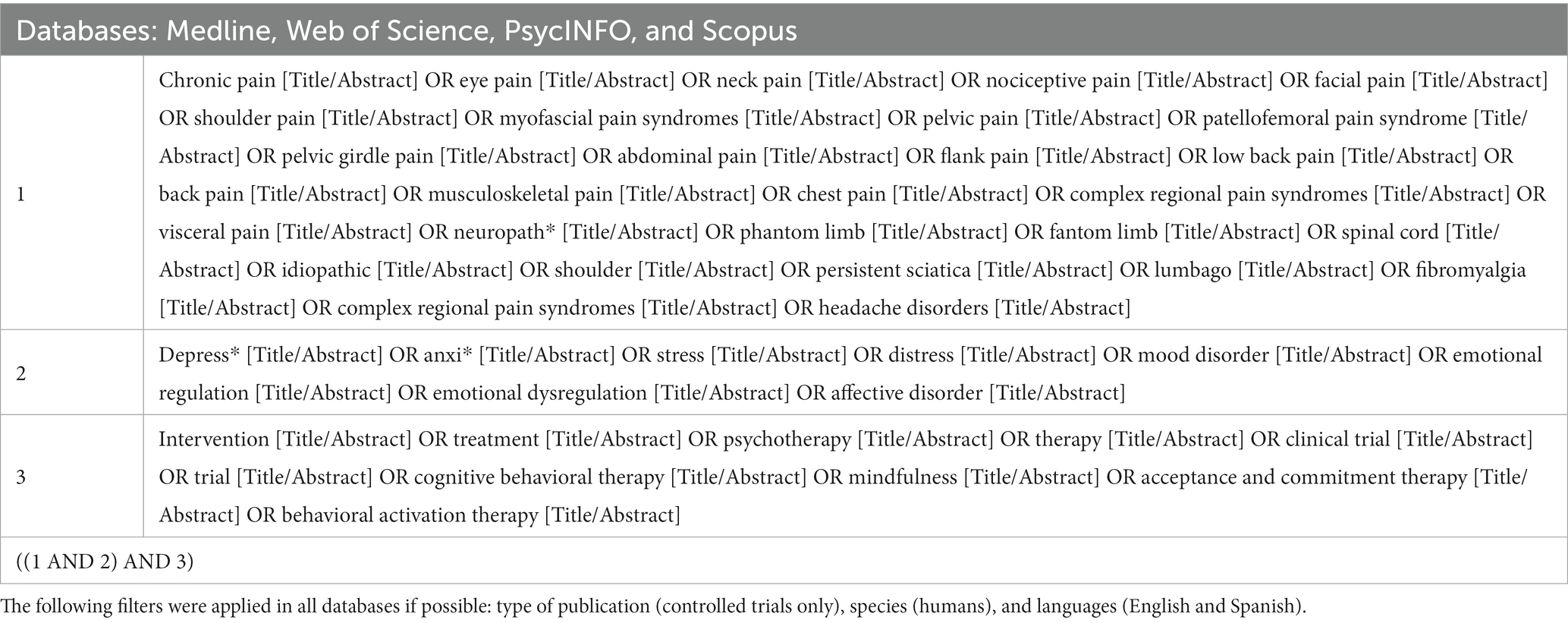
Table 1. Bibliographic database searches.
For the exploration of unpublished clinical trials, a search was conducted in ClinicalTrials.Gov, International Standard Randomized Controlled Trial Number register (ISRCTN), World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP), and PROSPERO (Lin et al., 2019). The reference list of included articles was also examined through a reverse citation search for further analysis. In addition, the reference list of published narrative reviews, systematic reviews, and meta-analyses, as well as grey literature (search carried out in Google Scholar), were consulted to ensure that all eligible studies were included (i.e., Buhrman et al., 2016; Hilton et al., 2017; Ahern et al., 2018; Haugmark et al., 2019; Khoo et al., 2019; López-López et al., 2019; Williams et al., 2020; Fordham et al., 2021; Pardos-Gascón et al., 2021; White et al., 2022).
To select the eligibility criteria, the “Population,” “Intervention,” “Comparison,” “Outcomes,” and “Study” (PICOS) approach was followed. Table 2 details the inclusion and exclusion criteria established in this systematic review.
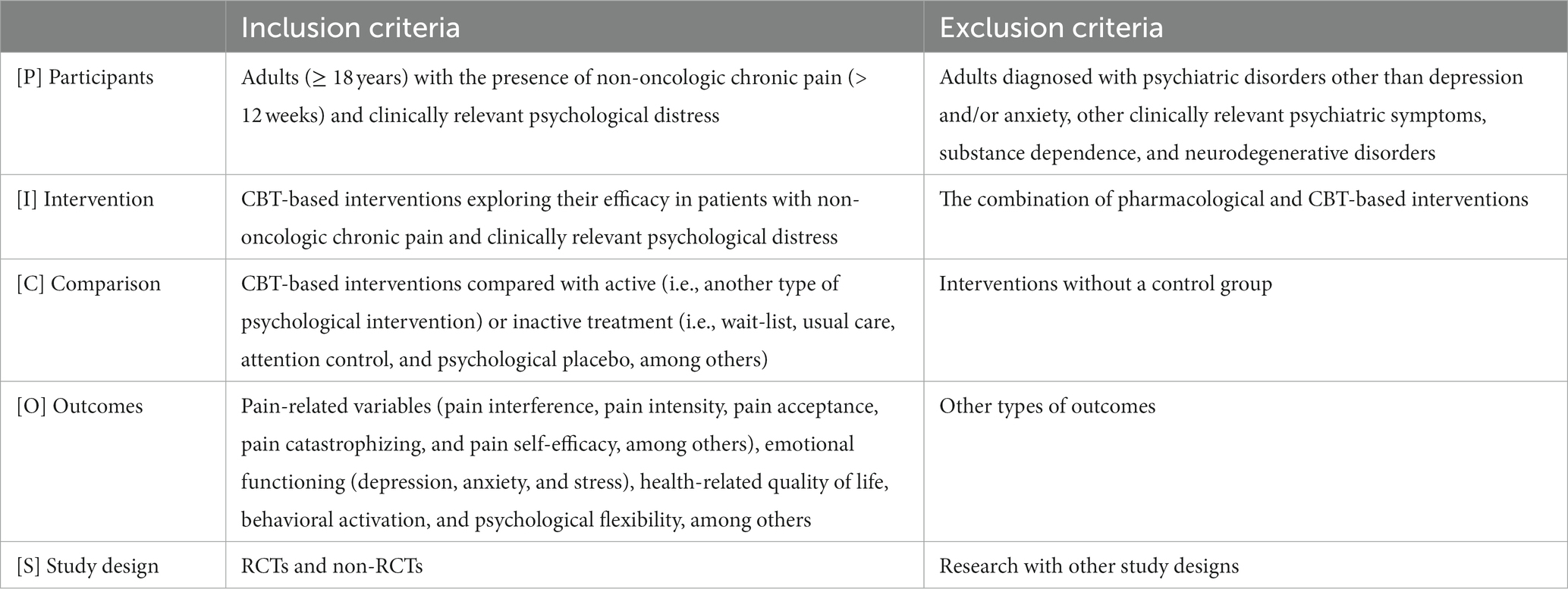
Table 2. Eligibility criteria according to PICOS strategy.
The population of interest consisted of adults (≥ 18 years) with the presence of non-oncologic chronic pain (> 12 weeks) and clinically relevant psychological distress, according to the clinical cut-off for depression and/or anxiety reported in the studies. Participants diagnosed with psychiatric disorders other than depression and/or anxiety, other clinically relevant psychiatric symptoms, substance dependence, and neurodegenerative disorders were excluded.
CBT-based interventions exploring their efficacy in patients with non-oncologic chronic pain and clinically relevant psychological distress, regardless of their mode of delivery (e.g., face-to-face, online, and blended format). To explore all available evidence in the literature, this systematic review synthesized the efficacy of all CBT-based interventions that met this eligibility criteria. The points analyzed for each outcome were the post-treatment and the follow-up assessment, examining differences between the groups. The combination of pharmacological and CBT-based interventions was excluded.
CBT-based interventions were included exclusively when the comparison group received active (i.e., another type of psychological intervention) or inactive treatment (i.e., wait-list, usual care, attention control, and psychological placebo, among others). Given the objective of this study, CBT-based interventions without a control group were excluded.
The selection of outcomes was based on recommendations from the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT; Dworkin et al., 2008). Specifically, pain-related variables (pain interference, pain intensity, pain acceptance, pain catastrophizing, and pain self-efficacy, among others), emotional functioning (depression, anxiety, and stress), health-related quality of life, behavioral activation, and psychological flexibility, among others, were explored in this systematic review.
RCTs and non-RCTs of any length of follow-up were included. Only data from studies that have received ethical approval and were published in English or Spanish were used. No studies were excluded based on publication status, date, or type (Lin et al., 2019).
Duplicate articles in the databases were automatically removed by Mendeley. Then, four reviewers independently screened all articles in Rayyan QCRI based on their titles and abstracts. The full texts were independently checked for compliance with the eligibility criteria. Finally, the reviewers entered key information from each study into a standardized data extraction form and assessed the RoB of included studies. During each phase, at least two reviewers were employed. No additional reviewer was needed to resolve a disagreement.
The RoB of the included studies was assessed using the Cochrane Collaboration’s risk of bias assessment tool (Higgins et al., 2011). This tool involves the assessment of RoB arising from each of six domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. Studies were classified as high risk (if at least one domain was assessed as high), unclear (if at least one domain was assessed as unclear and the other domains were low), or low risk of bias (if all individual domains were low).
Findings were described according to therapy type (CBT, MBI, ACT, and BATD). A narrative synthesis was carried out to describe the main characteristics of psychological therapies and the results obtained in the comparison of outcomes with control conditions (inactive or active). The statistical significance threshold was set at p < 0.05 and the magnitude of Cohen’s d was interpreted according to the following rule of thumb criterion (Sawilowsky, 2009): very small (0.10), small (0.20), medium (0.50), large (0.80), very large (1.20), and huge (2.00).
The initial database search yielded a total of 1,230 published articles. As shown in Figure 1, after removing duplicates and screenings, 14 articles based on 12 RCT and 1 non-RCT were included. Two studies were derived from the same sample (De Jong et al., 2016, 2018), although they presented evidence of different outcomes. The 14 articles that were excluded during the full-text screening are presented in Supplementary Table S2.
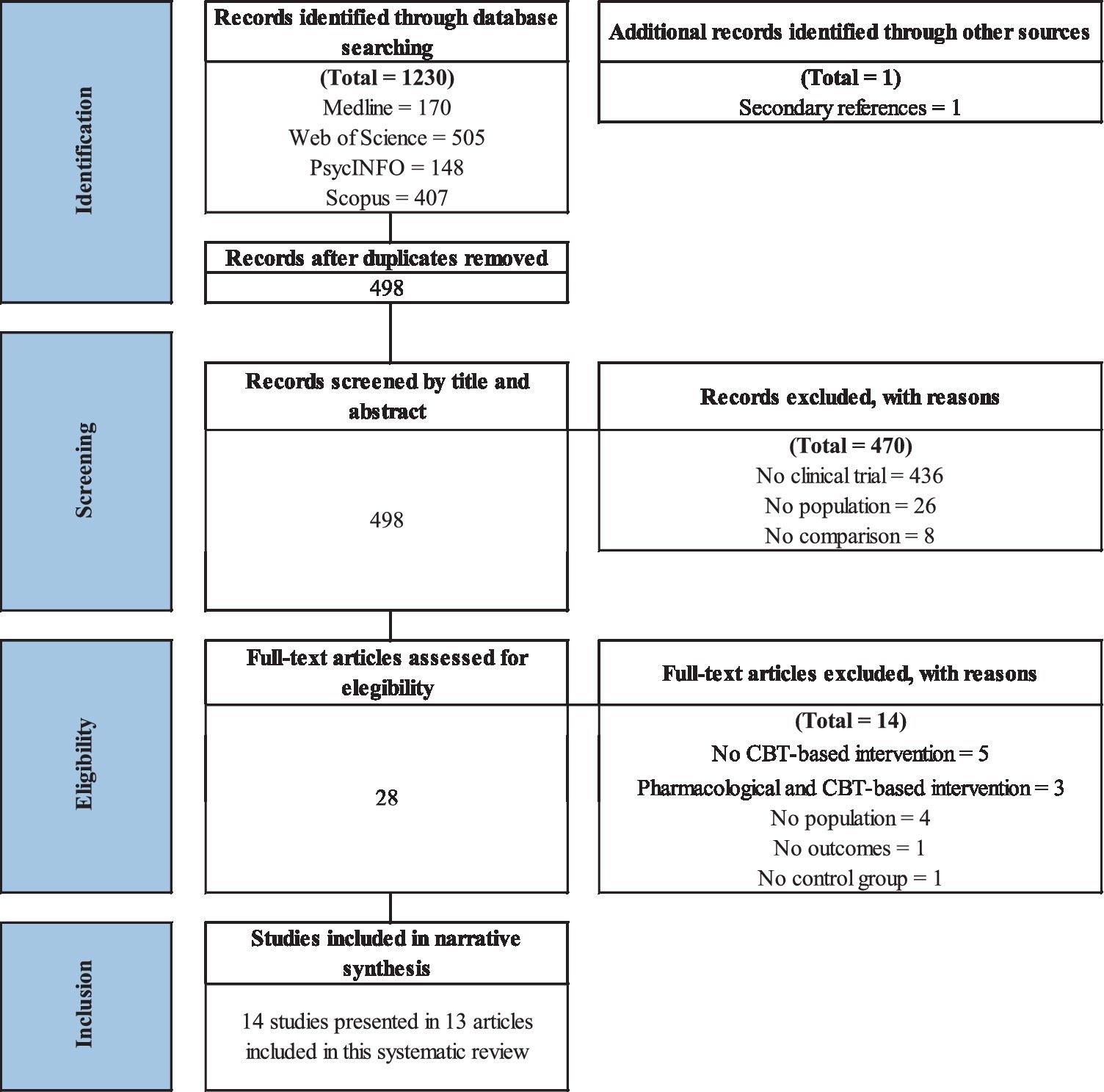
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flowchart from record identification to study inclusion.
The 13 articles included were published between 2011 and 2023. Three studies (23%) were conducted in Sweden, three (23%) in Spain, three (23%) in Germany, two (15%) in the United States of America, one (8%) in Australia, and one (8%) in Iceland. Five studies (38%) assessed patients with chronic pain (CP), three (23%) with chronic low back pain (CLBP), two (15%) with chronic musculoskeletal pain (CMP), one (8%) with chronic back pain (CBP), one (8%) with chronic spinal cord injury, and one (8%) with non-specific chronic pain (NSCP). Nine studies (69%) included CBT, three (23%) MBI, and one ACT and BATD (8%) as the main therapy of interest. Eleven studies (85%) employed inactive control groups (usual care or waitlist). All the studies (100%) carried out the therapy program weekly. The format of the therapy was face-to-face in six studies (46%), entirely online in five (38%), a blended format in one (8%), and combined face-to-face plus online versus online in one (8%).
The sample size of the study’s arms ranged from 26 to 167 in the intervention group (IG) and 24 to 161 in the control group (CG), and the mean age varied from 45 to 61 in IG and 46 to 59 years old in CG. In total, 1,661 participants were involved in this systematic review, of which 850 were in IG and 811 in CG. The proportion of women in all studies was higher than 50%, both in IG and CG, except for the IG in two (43.2% and 26%; Tlach and Hampel, 2011; Migliorini et al., 2016, respectively) and CG in one (32%; Migliorini et al., 2016). The employment status was reported in nine studies (69.2%) and medication consumption in eight studies (61.6%). The dropout rate at the end of the studies ranged from 17 to 67%. The number of sessions ranged from four to thirteen with a minimum duration of 50 min per session and a maximum of 150 min. The therapies were delivered by psychologists in ten studies (77.7%), other professionals in two (27.3%), and without therapists in one (7.7%). Details are described in Table 3.

Table 3. Characteristics of the controlled trials included in the systematic review.
Figure 2 shows the RoB for each included study. Twelve studies (92%) reported an adequate random sequence generation and provided sufficient information on the method of allocation concealment of patients. None of the studies (0%) blinded the participants and personnel to the intervention delivered. However, seven studies (54%) explicitly reported that they were able to blind outcome assessment from knowledge of which intervention a participant received. Incomplete outcome data were adequately managed in all cases (100%), and they were rated as free from selective outcome reporting bias in all included studies (100%). Considering the impossibility of blinding participants in psychological therapies, six studies (46%) reported a high (Tlach and Hampel, 2011; Ólason et al., 2018; Boersma et al., 2019; Schlicker et al., 2020; Baumeister et al., 2021; Torrijos-Zarcero et al., 2021) and seven (54%) an unclear RoB (Buhrman et al., 2015; De Jong et al., 2016, 2018; Migliorini et al., 2016; Aragonès et al., 2019; Gardiner et al., 2019; Gasslander et al., 2022; Sanabria-Mazo et al., 2023).
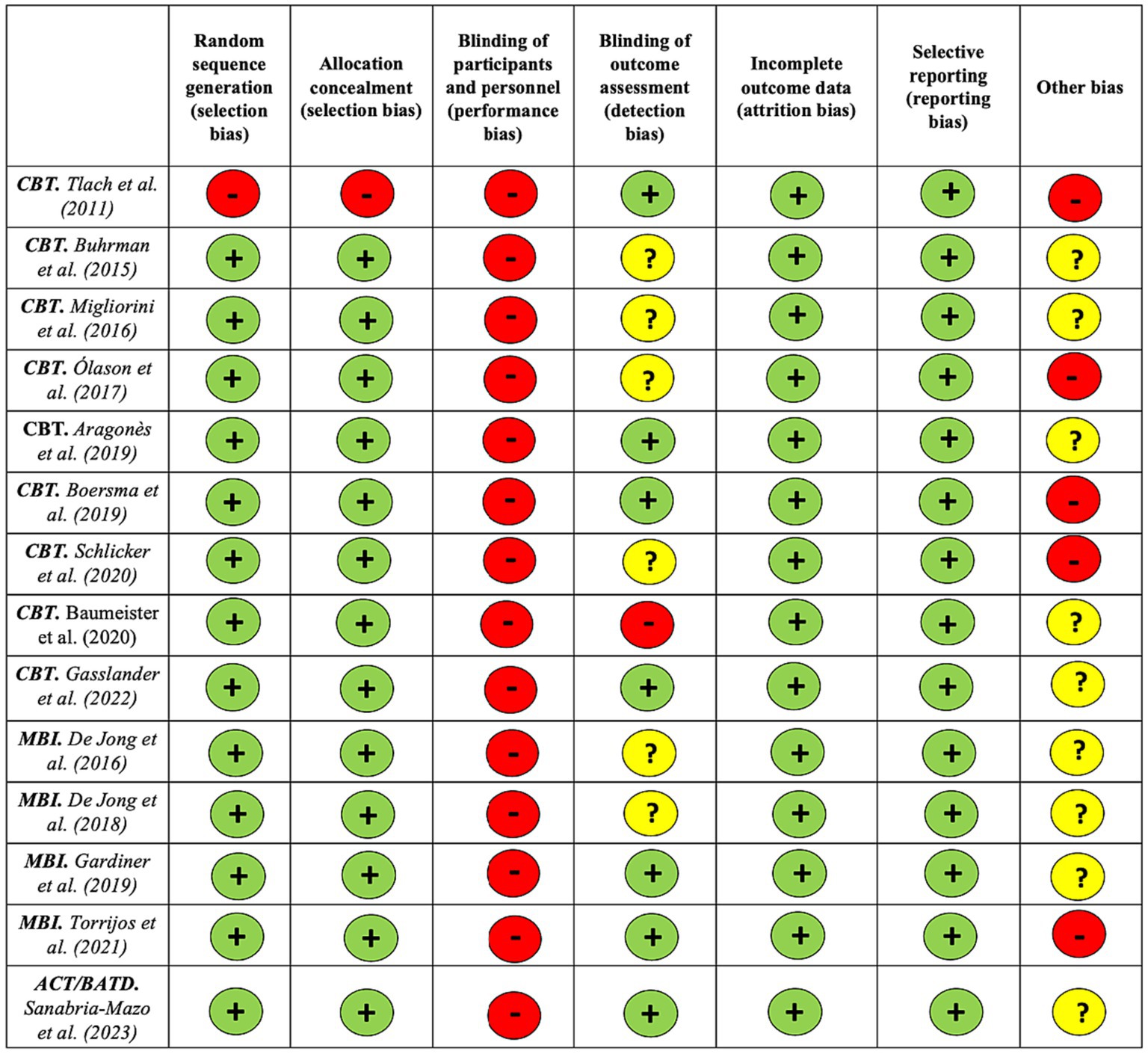
Figure 2. Risk of bias assessment for each included study using the Cochrane Collaboration’s tool for assessing risk of bias (Higgins et al., 2011).
The specific results of each of the studies included in this systematic review are presented in Supplementary Table S3. Information from these controlled trials is organized according to the type of intervention (CBT, MBI, ACT, and BATD).
Five out of the nine studies evaluated CBT as the only therapeutic component therapy (Tlach and Hampel, 2011; Ólason et al., 2018; Boersma et al., 2019; Baumeister et al., 2021; Gasslander et al., 2022) and the remaining four with other components (Buhrman et al., 2015; Migliorini et al., 2016; Aragonès et al., 2019; Schlicker et al., 2020). The time horizon of the assessment of eight out of the nine studies was pre-, post, and follow-up. Except for Tlach and Hampel (2011), Migliorini et al. (2016), and Ólason et al. (2018), all analyses of CBTs were based on ITT. Baseline comparisons were carried out in all nine CBT studies. Less Boersma et al. (2019), all studies compared CBT with an inactive control group (usual care).
All nine studies assessed depressive symptoms as the primary outcome (Buhrman et al., 2015; Migliorini et al., 2016; Ólason et al., 2018; Aragonès et al., 2019; Boersma et al., 2019; Schlicker et al., 2020; Baumeister et al., 2021; Gasslander et al., 2022) and three anxiety symptoms as the co-primary outcome (Tlach and Hampel, 2011; Buhrman et al., 2015; Ólason et al., 2018; Boersma et al., 2019). The characteristics of the CBT are detailed in Table 3 and the specific results of each study are presented in Supplementary Table S3. The evidence for each outcome is presented below.
Six out of eight studies (75%) found significant differences in the reduction of depressive symptoms at post-treatment with very large to very small effect sizes (d ranging from 1.31 to 0.18; Tlach and Hampel, 2011; Buhrman et al., 2015; Migliorini et al., 2016; Schlicker et al., 2020; Baumeister et al., 2021; Gasslander et al., 2022); and four out of six studies (66%) at follow-up with medium to small effect sizes (d ranging from 0.75 to 0.26; Tlach and Hampel, 2011; Ólason et al., 2018; Aragonès et al., 2019; Baumeister et al., 2021) in favor of CBT compared to treatment as usual (TAU).
Another study (Boersma et al., 2019) identified significant differences in the reduction of depressive symptoms at follow-up with a small effect size (d = 0.25) in favor of hybrid therapy (exposure in vivo and DBT) compared to CBT.
Five out of six studies (83%) also showed significant differences in the reduction of anxiety symptoms at post-treatment with large to very small effect sizes (d ranging from 1.08 to 0.19; Tlach and Hampel, 2011; Buhrman et al., 2015; Migliorini et al., 2016; Schlicker et al., 2020; Gasslander et al., 2022); and three out of four studies (75%) at follow-up with large to small effect sizes (d ranging from 1.07 to 0.27; Tlach and Hampel, 2011; Buhrman et al., 2015; Schlicker et al., 2020) in favor of CBT compared to TAU. No significant differences (0%) between these groups were found at post-treatment in two studies (Buhrman et al., 2015; Gasslander et al., 2022) and at follow-up in one study (Buhrman et al., 2015) exploring the fear of anxiety symptoms.
No significant differences (Boersma et al., 2019) were identified between CBT and hybrid therapy (exposure in vivo and DBT) in the reduction of anxiety symptoms at post-treatment and at follow-up.
One out of one study (100%) identified significant differences in improved stress symptoms at follow-up with a small effect size (d = 0.47) in favor of CBT compared to TAU (Migliorini et al., 2016).
Significant differences in improved pain intensity were identified at post-treatment in one out of four studies with a small effect size (d = 0.42; Baumeister et al., 2021) in favor of CBT compared to TAU. No differences at follow-up were found in any of the four studies exploring pain intensity (Migliorini et al., 2016; Ólason et al., 2018; Aragonès et al., 2019; Schlicker et al., 2020).
Similarly, no significant differences were also found in the study (Boersma et al., 2019) comparing pain intensity after CBT and hybrid therapy (exposure in vivo and DBT) at post-treatment and follow-up.
Two out of three studies (67%) found significant differences in the reduction of pain interference at post-treatment with small to very small (d ranging from 0.22 to 0.12; Buhrman et al., 2015; Gasslander et al., 2022), but not at the follow-up in the two studies (0%) that explored this outcome (Buhrman et al., 2015; Aragonès et al., 2019), in favor of the CBT compared to TAU.
Another study (Boersma et al., 2019) demonstrated significant changes in the reduction of pain interference in hybrid therapy (exposure in vivo and dialectical behavior therapy) compared to CBT at post-treatment with very small effect size (d = 0.02) and at follow-up with small effect size (d = 0.25).
No significant differences (0%) between CBT and TAU were found at post-treatment in two studies (Buhrman et al., 2015; Gasslander et al., 2022) and at follow-up in one study (Buhrman et al., 2015) exploring pain catastrophizing.
However, another study (Boersma et al., 2019) reported significant differences in the decrease of pain catastrophizing at post-treatment with a small effect size (d = 0.26), but not at follow-up, in favor of hybrid therapy (exposure in vivo and dialectical behavior therapy) compared to CBT.
Two out of two studies (100%) indicated significant differences in increased pain acceptance at post-treatment (Buhrman et al., 2015; Gasslander et al., 2022) with very small (d = 0.12) and small effect size (d = 0.30), but not at follow-up in one out of one study (0%) that explored this outcome, in favor of CBT compared to TAU.
Significant differences between CBT and TAU were found at post-treatment in one out of three studies (33%) with a small effect size (d = 0.39; Baumeister et al., 2021) and at follow-up in one out of two studies (50%) with small effect size (d = 0.33; Baumeister et al., 2021).
No significant differences (0%) between CBT and TAU were found post-treatment in two studies (Schlicker et al., 2020; Gasslander et al., 2022) and at follow-up in one study (Schlicker et al., 2020) exploring pain self-efficacy.
Four out of six studies (67%) found significant differences in improving quality of life at post-treatment with medium to invaluable effect sizes (d ranging from 0.78 to 0.02; Tlach and Hampel, 2011; Migliorini et al., 2016; Baumeister et al., 2021; Gasslander et al., 2022) and two out of four studies (50%) at follow-up with medium to small effect size (d = 0.78 and d = 0.33; Tlach and Hampel, 2011 and Baumeister et al., 2021, respectively) in favor of CBT compared to TAU.
One out of one study (100%) identified significant differences in improved social functioning at follow-up with a medium effect size (d = 0.51) in favor of CBT compared to TAU (Ólason et al., 2018). No differences were found between these groups at post-treatment in the three studies (Ólason et al., 2018; Schlicker et al., 2020; Gasslander et al., 2022) exploring this outcome.
One out of two studies (50%) indicated significant differences in coping strategy of ignoring and catastrophizing at post-treatment (Gasslander et al., 2022) with small effect sizes (d = 0.38 and d = 0.34), but not at follow-up in one out of one study (0%) that explored cognitive and behavioral coping strategies (Buhrman et al., 2015), in favor of CBT compared to TAU. One out of one study (100%) identified significant differences in improved pain-related disability at post-treatment with a small effect size (d = 0.35) in favor of CBT compared to TAU (Baumeister et al., 2021), but not at follow-up.
No differences were found between CBT and TAU in one out of one study examining kinesiophobia (Gasslander et al., 2022), fear avoidance (Ólason et al., 2018), and life control (Gasslander et al., 2022) at post-treatment. Two studies explored work capacity at post-treatment and follow-up (Schlicker et al., 2020; Baumeister et al., 2021), but neither found significant differences (0%).
One of the MBI assessed the effects of Mindfulness-Based Cognitive Therapy (MBCT; De Jong et al., 2016, 2018), one of Integrative Medicine Group Visits (IMGV) with mindfulness techniques (Gardiner et al., 2019), and one of Mindful Self-Compassion (MSC) program (Torrijos-Zarcero et al., 2021). Two out of three studies evaluated MBI as the only therapeutic component (De Jong et al., 2016, 2018; Torrijos-Zarcero et al., 2021) and the remaining one as a multi-component (Gardiner et al., 2019) integrating mindfulness techniques, evidence-based integrative medicine, and medical group visits (Gardiner et al., 2019). The time horizon of the assessment of two of these studies was pre- and post (De Jong et al., 2016, 2018; Torrijos-Zarcero et al., 2021). All the analyses of MBIs were based on ITT. The efficacy of one study was tested in one RCT with results reported in two different publications (De Jong et al., 2016, 2018). Baseline comparisons were carried out in all MBI studies. Except for Torrijos-Zarcero et al. (2021), all studies compared MBI with an inactive control group (TAU).
Two studies assessed depressive symptoms as the primary outcome (De Jong et al., 2016, 2018; Gardiner et al., 2019); and one evaluated self-compassion (Torrijos-Zarcero et al., 2021) as the primary outcome and depressive and anxiety symptoms as the secondary outcome. The characteristics of the MBI are detailed in Table 3 and the specific results of each study are presented in Supplementary Table S3. The evidence for each outcome is detailed below.
One study out of two (50%) identified significant differences in the reduction of depressive symptoms at post-treatment (De Jong et al., 2016, 2018) with a very small effect size (d = 0.13) in favor of MBI compared to TAU. The only study (Gardiner et al., 2019) that assessed depressive symptoms at follow-up found no significant difference between MBI and TAU.
No significant differences were identified in the study (Torrijos-Zarcero et al., 2021) comparing depressive symptoms at post-treatment between MBI and CBT.
No differences were found between CBT and TAU in one out of one study examining anxiety symptoms at post-treatment and at follow-up (De Jong et al., 2016, 2018).
In contrast, one study (Torrijos-Zarcero et al., 2021) reported significant differences in the reduction of anxiety symptoms at post-treatment with a very small effect size (d = 0.17) in favor of MBI compared to CBT.
No significant differences between MBI and TAU (De Jong et al., 2016, 2018) and MBI and CBT (Torrijos-Zarcero et al., 2021) were reported at post-treatment in the reduction of pain intensity.
Neither of the two studies comparing pain interference between MBI and TAU at post-treatment (De Jong et al., 2016, 2018; Gardiner et al., 2019) and at follow-up (Gardiner et al., 2019) showed significant differences.
However, one study (Torrijos-Zarcero et al., 2021) indicated significant differences in the reduction of pain interference at post-treatment with a very small effect size (d = 0.07) in favor of MBI compared to CBT.
There was also no significant difference in the comparison between MBI and TAU in the reduction of pain catastrophizing in the only study (De Jong et al., 2016, 2018) that explored it at post-treatment.
One study (Torrijos-Zarcero et al., 2021) reported significant differences in decreasing pain catastrophizing at post-treatment with a very small effect size (d = 0.12) in favor of MBI compared to CBT.
One study (Torrijos-Zarcero et al., 2021) reported significant differences in increasing pain acceptance at post-treatment with a very small effect size (d = 0.19) in favor of MBI compared to CBT.
No significant differences between MBI and TAU (De Jong et al., 2016, 2018) were reported at post-treatment and follow-up in the reduction of pain self-efficacy.
One study (De Jong et al., 2016, 2018) out of two found significant differences in improving quality of life at post-treatment with a very small effect size (d = 0.19); and one (Gardiner et al., 2019), the only one featuring this comparison, found a significant effect at follow-up (RR = 1.07) in favor of MBI compared to TAU.
In contrast, no significant differences in quality-of-life improvement were identified (Torrijos-Zarcero et al., 2021) between MBI and CBT.
One study (De Jong et al., 2016, 2018) showed significant differences in increased self-regulation with a large effect size (d = 0.91) and emotional awareness with a medium effect size (d = 0.57) at post-treatment.
Another study (Torrijos-Zarcero et al., 2021) identified significant differences in self-compassion with a very small effect size (d = 0.05) at post-treatment in favor of the MBI compared to CBT.
No significant differences between MBI and TAU (De Jong et al., 2016, 2018) were reported at post-treatment and follow-up in the reduction of behavioral activation.
One study explored the efficacy of ACT and BATD compared to TAU (Sanabria-Mazo et al., 2023). The time horizon of the assessment of this study was pre-, post, and follow-up and the analyses were based on ITT. Baseline comparisons were carried out in this study. This study assessed pain interference as the primary outcome. The characteristics of the ACT and BATD are detailed in Table 3 and the specific results of these studies are presented in Supplementary Table S3. The evidence for each outcome is detailed below.
Significant differences were detected in the improvement of stress symptoms at post-treatment with medium effect size (d = 0.69), but not at follow-up, in favor of ACT compared to TAU. However, no significant differences between these groups were found in depressive and anxiety symptoms. Similarly, no significant differences between BATD and TAU and between ACT and TAU were found in the improvement of depressive, anxiety, and stress symptoms.
Significant differences between ACT and TAU were identified in the improvement of pain interference at post-treatment with a medium effect size (d = 0.64) and at follow-up with a medium effect size (d = 0.73). BATD was only statistically superior to TAU at follow-up with a medium effect size (d = 0.66). No significant differences between ACT and TAU, between BATD and TAU, and between ACT and BATD were found in pain intensity. A significant reduction in pain catastrophizing was reported by patients assigned to ACT and BATD at post-treatment with small and medium effect sizes (d = 0.45 and d = 0.59, respectively) and at follow-up with medium effect sizes (d = 0.59, in both) compared to TAU.
Significant differences were found in the improvement of pain acceptance at post-treatment with a small effect size (d = 0.34) and at follow-up with a small effect size (d = 0.42) in ACT compared to TAU. In contrast, no significant differences between BATD and TAU and between ACT and BATD were found in pain acceptance.
Significant differences were identified in the improvement of psychological flexibility at post-treatment with a medium effect size (d = 0.52) and at follow-up with a small effect size (d = 0.37) in ACT compared to TAU. Similarly, significant differences between BATD and TAU were found in psychological flexibility with a small effect size (d = 0.40), but not at follow-up. No significant differences between ACT and BATD were found in psychological flexibility.
Significant differences between ACT and TAU and between BATD and TAU were found in behavioral activation at post-treatment with small effect sizes (d = 0.30 and d = 0.46, respectively), but not at follow-up. No significant differences between ACT and BATD were found in behavioral activation.
Table 4 details a synthesis of all the evidence identified in the comparison between CBT, MBI, ACT, or BATD and TAU.
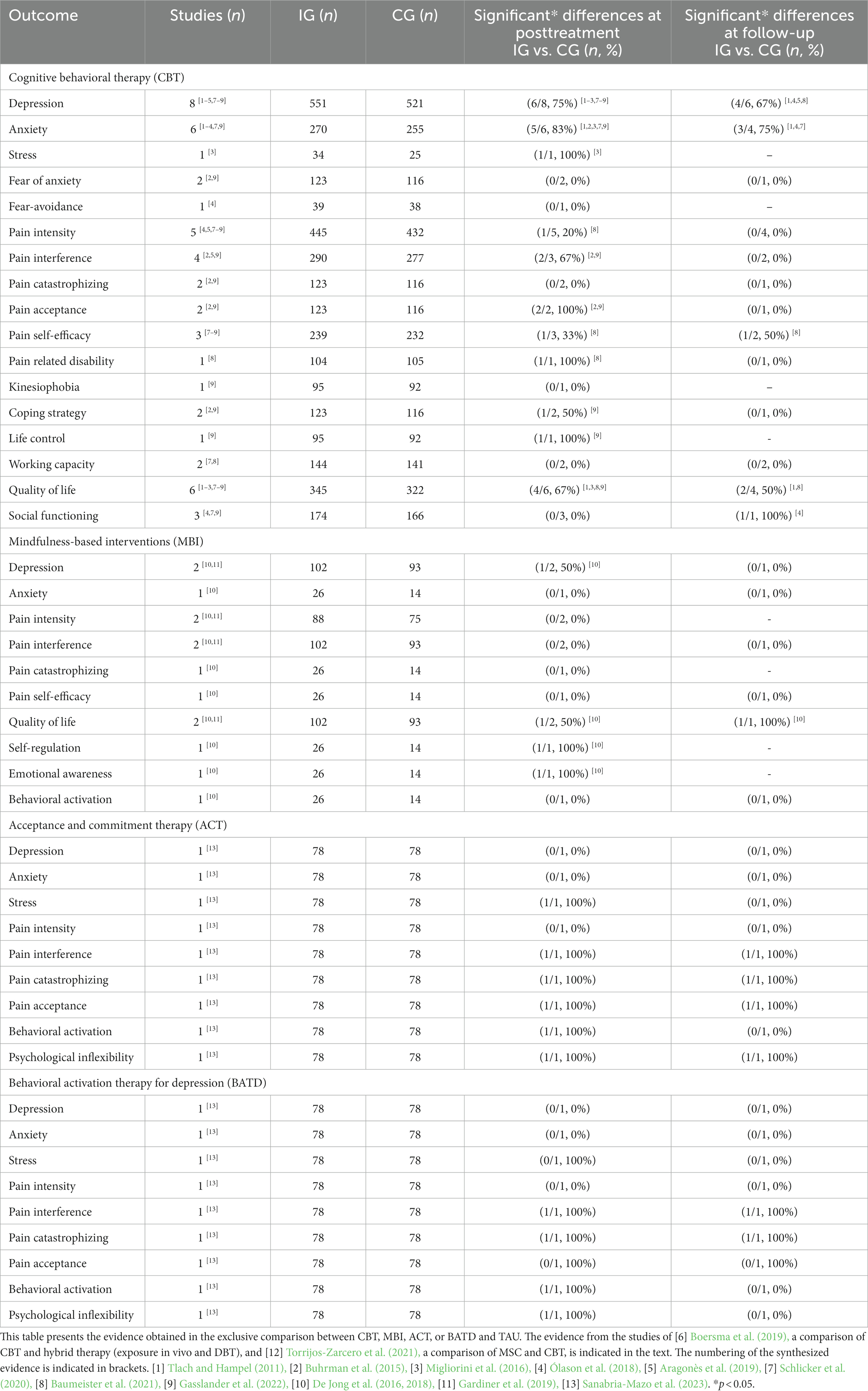
Table 4. Synthesis of all evidence identified in the comparison between CBT or MBI and TAU.
One upcoming RCT was identified. This RCT will evaluate the efficacy of internet-delivered ACT and internet-delivered CBT compared to attention control in patients with chronic non-cancer pain and major depression (Bell et al., 2020). The general characteristics of this study are detailed in Supplementary Table S4.
Depression and anxiety are among the most diagnosed mental health conditions in people with chronic pain. Identification of effective therapies is needed because of the poorer prognosis and higher therapy resistance entailed in comorbid pain and psychological distress compared to either condition considered alone. However, to date, no published systematic reviews have attempted to synthesize the efficacy of these interventions in patients with these combined conditions. The current systematic review demonstrates positive, but modest, results from CBT-based interventions for patients with chronic pain and clinically relevant psychological distress. A total of twelve RCTs and one non-RCT published between 2011 and 2023 were included in the analyses. In addition, it was noted that one RCT is upcoming that will explore the efficacy of ACT and traditional CBT in patients with chronic non-cancer pain and major depression, and results are expected soon (Bell et al., 2020). Taken together, the published and upcoming studies signal an increasing interest in examining how CBT-based therapies (CBT, MBI, ACT, and BATD) can improve the functional status and quality of life in patients with chronic pain experiencing clinically relevant depressive and/or anxiety symptoms. There is also an increasing interest in recognizing potential beneficial therapeutic processes of change in patients with this comorbidity in the second and third wave of CBTs (Hayes and Hofmann, 2021), such as acceptance of pain, psychological flexibility, and behavioral activation (Buhrman et al., 2015; Bell et al., 2020; Gasslander et al., 2022; Sanabria-Mazo et al., 2023).
Compared to TAU, traditional CBT reported significant differences in the reduction of depressive and anxiety symptoms and in the increase of quality of life at post-treatment and at follow-up, with very large to small effect sizes. These results are consistent with the reported efficacy of CBT-based interventions for depression or chronic pain in previous systematic reviews (Lorenzo-Luaces et al., 2018; López-López et al., 2019; Williams et al., 2020), but with a more modest magnitude. Nevertheless, in general, no significant differences between traditional CBT and TAU were identified at post-treatment and follow-up in the studies exploring pain intensity and pain catastrophizing. Although with a limited number of studies, there is also evidence that CBT could be beneficial in improving pain interference and pain acceptance (Buhrman et al., 2015; Gasslander et al., 2022) at posttreatment, but not at follow-up, with small effect sizes. In other pain-related variables, such as pain self-efficacy, pain-related disability, fear avoidance, kinesiophobia, working capacity, and social functioning, inconsistent results or insufficient evidence were obtained.
As in previous research in chronic pain (Veehof et al., 2016; Hilton et al., 2017; Khoo et al., 2019), compared to TAU, MBI produced a significant reduction at post-treatment in depressive symptoms, in one out of two studies (De Jong et al., 2018), and an increase in emotional awareness and self-regulation, in the one study that addressed this (De Jong et al., 2016). However, this evidence comes from a pilot RCT with a small sample size (De Jong et al., 2016, 2018). More evidence is needed to determine the overall efficacy of MBI in depression, anxiety, pain, and quality of life for populations with this comorbidity. Results from a single study (Torrijos-Zarcero et al., 2021) indicated significant differences in anxiety, pain interference, pain acceptance, pain catastrophizing, and self-compassion at post-treatment in favor of MBI compared to CBT.
Findings from a recent RCT provided evidence of the clinical utility of including remote synchronous video group-based ACT or BATD as adjuncts to TAU for the improvement of pain interference and pain catastrophizing after treatment and in the follow-up to patients with chronic low back pain (CLBP) and comorbid depressive symptoms. However, no significant differences in depressive or anxiety symptoms were found in ACT and BATD compared to TAU at any assessment time points. In both active therapies, improvements in pain interference at follow-up were significantly mediated by improvements at post-treatment in psychological flexibility (Sanabria-Mazo et al., 2023). Investigating the mediating role of psychological flexibility in the third wave of CBTs for chronic pain patients is important for understanding the mechanisms of change underlying treatment effectiveness, identifying effective treatment components, and enhancing treatment outcomes (McCracken et al., 2022). The results of the Bell et al. (2020) study, when available, could help provide stronger evidence for the findings known so far in the population with this comorbidity.
In most of the studies explored in this systematic review, CBT-based interventions were more effective than control groups in improving depression, anxiety, and quality of life, at both post-treatment and at follow-up, but not in the improvement of pain intensity. However, the findings of this systematic review should be interpreted with some caution, as they are based on few studies with high heterogeneity in terms of mode of delivery (e.g., face-to-face, online, and blended format), number of sessions, intervention components, compliance, and characteristics of therapists, among others. It is also important to consider the potential bias arising from studies with samples smaller than 50 participants per arm and the lack of information on the adverse effects of therapies (Moore et al., 2010). A recent Delphi study has pointed out the importance of recognizing what the main contents of CBT are. In this regard, three main components have been highlighted: (1) pain education; (2) increased activity; and (3) some form of cognitive challenge (Sharpe et al., 2020). In the studies included, there were also some differences in the types of CBT methods used or in the primary and secondary outcomes, which complicates the generalizability of these results.
Like previous meta-analyses in chronic pain (Williams et al., 2020) and depression (Lorenzo-Luaces et al., 2018), the efficacy of CBT-based interventions for comorbid pain and depression is clinically relevant on average (Sanabria-Mazo et al., 2020). As the findings of this study point out, the effects of CBT targeting the population with chronic pain and comorbid psychological distress are more modest than targeting one of the two conditions separately (Sanabria-Mazo et al., 2020). Psychological distress could potentially impact adherence to pain management interventions, leading to decreased engagement in self-care activities, and treatment plan compliance among patients with depression or anxiety, ultimately affecting treatment outcomes. Hence, it is crucial to evaluate and tackle depression in chronic pain populations for better treatment outcomes.
While the results of this systematic review fit with a wider conclusion that traditional CBT is beneficial for many varied conditions (Fordham et al., 2021), there appears substantial room for improvement. Considering the effects identified, it would be interesting to explore, when more robust evidence is available, the efficacy of third-generation therapies in patients with chronic pain and comorbid psychological stress. Although evidence is beginning to emerge on the effects of third-wave CBT therapies compared with TAU (De Jong et al., 2016, 2018; Gardiner et al., 2019; Bell et al., 2020; Torrijos-Zarcero et al., 2021; Sanabria-Mazo et al., 2023), more research is needed to compare which therapy is most effective, in which circumstances, and for whom.
These findings must be interpreted to understand the following limitations and strengths. First, given the lack of trials with low RoB, it might be premature to conclude the magnitude of the efficacy of CBT-based interventions for this comorbidity. Second, since the heterogeneity of available data in the included studies (e.g., mode of delivery, number of sessions, intervention components, and characteristics of therapists, among others), it was not possible to compute a meta-analysis. Third, although published and unpublished studies were explored, only published studies in English or Spanish were finally included in this systematic review, so other otherwise relevant evidence could have been omitted. Fourth, due to the limited number of RCTs, it was not possible to examine whether specific forms of CBT are more effective than others. The strengths of this study are the number of databases explored, the compliance with PRISMA guidelines, the validation of the Boolean searches according to PRESS guidelines, the use of Rayyan as a tool to minimize possible loss of evidence, and the consensual review between reviewers in the different phases of screening, extraction of the data, and RoB.
Further research is needed in this area when more studies are available. The need to identify the core elements of psychosocial therapies that drive their therapeutic effects is critical. To extend the knowledge on the relevant topic examined in this study, future studies should explore the ingredients that are indeed effective and for which patients, as well as what amount of variance is explained by universal factors shared by all therapies. These interventions should also strive to employ adequately powered randomized designs and compare the efficacy of psychological therapies to other empirically supported therapies.
The comorbidity of chronic pain and psychological distress represents a complex problem or set of problems, perhaps best conceived as having a multifactorial aetiology. Psychological research and treatment should address these because when they appear together, they cause substantial health and social impacts. This study shows that traditional CBT improves depression, anxiety, and quality of life in patients with comorbid chronic pain and clinically relevant psychological distress, but not for pain intensity and pain catastrophizing. Although some evidence is presented in this systematic review, more RCTs based on MBI, ACT, and BATD are needed to determine the overall efficacy of this intervention in these patients.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
JL, AS, SE, and JS-M designed the study. JS-M, AC-C, ÓF-V, and GN-R performed the eligibility criteria, data extraction, and study coding. JS-M and AC-C performed the data analysis and synthesized all extracted data. JS-M drafted the manuscript. GC-R, AM-P, JC-A, SE, XB, AS, AF-S, and JL revised and approved the final version of the manuscript. LM critically revised and supervised the final draft. All authors commented on, revised, and approved the draft and the final manuscript.
This study has been funded by the Institute of Health Carlos III (ISCIII; PI19/00112; ICI20/00080) and has been co-financed with European Union ERDF funds. JS-M has a PFIS predoctoral contract from the ISCIII (FI20/00034). AC-C has a FI predoctoral contract from AGAUR (FI_B/00216).
The authors are grateful to the CIBER of Epidemiology and Public Health (CIBERESP CB22/02/00052; ISCIII) for its support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1200685/full#supplementary-material
Ahern, E., Kinsella, S., and Semkovska, M. (2018). Clinical efficacy and economic evaluation of online cognitive behavioral therapy for major depressive disorder: a systematic review and meta-analysis. Expert Rev. Pharmacoecon. Outcomes Res. 18, 25–41. doi: 10.1080/14737167.2018.1407245
Aragonès, E., Rambla, C., López-Cortacans, G., Tomé-Pires, C., Sánchez-Rodríguez, E., Caballero, A., et al. (2019). Effectiveness of collaborative care intervention for managing major depression and chronic musculoskeletal pain in primary care: a cluster-randomized controlled trial. J. Affect. Disord. 252, 221–229. doi: 10.1016/j.jad.2019.04.004
Baumeister, H., Knecht, A., and Hutter, N. (2012). Direct and indirect costs in persons with chronic back pain and comorbid mental disorders: a systematic review. J. Psychosom. Res. 73, 79–85. doi: 10.1016/j.jpsychores.2012.05.008
Baumeister, H., Paganini, S., Sander, L. B., Lin, J., Schlicker, S., Terhorst, Y., et al. (2021). Effectiveness of a guided internet-and mobile-based intervention for patients with chronic back pain and depression (WARD-BP): a multicenter, pragmatic randomized controlled trial. Psychother. Psychosom. 90, 255–268. doi: 10.1159/000511881
Bell, L. V., Cornish, P., Flusk, D., Garland, S. N., and Rash, J. A. (2020). The INternet ThERapy for deprESsion trial (INTEREST): protocol for a patient-preference, randomised controlled feasibility trial comparing iACT, iCBT and attention control among individuals with comorbid chronic pain and depression. BMJ Open 10:e033350. doi: 10.1136/bmjopen-2019-033350
Bisby, M. A., Chandra, S. S., Dudeney, J., Scott, A. J., Titov, N., and Dear, B. F. (2022). Can internet-delivered pain management programs reduce psychological distress in chronic pain? Exploring relationships between anxiety and depression, pain intensity, and disability. Pain Med. 24, 538–546. doi: 10.1093/pm/pnac158
Boersma, K., Södermark, M., Hesser, H., Flink, I. K., Gerdle, B., and Linton, S. J. (2019). Efficacy of a transdiagnostic emotion–focused exposure treatment for chronic pain patients with comorbid anxiety and depression: a randomised controlled trial. Pain 160, 1708–1718. doi: 10.1097/j.pain.0000000000001575
Buhrman, M., Gordh, T., and Andersson, G. (2016). Internet interventions for chronic pain including headache: a systematic review. Internet Interv. 4, 17–34. doi: 10.1016/j.invent.2015.12.001
Buhrman, M., Syk, M., Burvall, O., Hartig, T., Gordh, T., and Andersson, G. (2015). Individualized guided internet-delivered cognitive behavior therapy for chronic pain patients with comorbid depression and anxiety. Clin. J. Pain 31, 504–516. doi: 10.1097/AJP.0000000000000176
Chopra, K., and Arora, V. (2014). An intricate relationship between pain and depression: clinical correlates, coactivation factors, and therapeutic targets. Expert Opin. Ther. Targets 18, 159–176. doi: 10.1517/14728222.2014.855720
Churchill, R., Moore, T. H., Furukawa, T. A., Caldwell, D. M., Davies, P., Jones, H., et al. (2013). 'Third wave' cognitive and behavioural therapies versus treatment as usual for depression. Cochrane Database Syst. Rev. 10:CD008705. doi: 10.1002/14651858.CD008705.pub2
Cuijpers, P., Berking, M., Andersson, G., Quigley, L., Kleiboer, A., and Dobson, K. S. (2013). A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. Can. J. Psychiatr. 58, 376–385. doi: 10.1177/070674371305800702
De Jong, M., Lazar, S. W., Hug, K., Mehling, W. E., Hölzel, B. K., Sack, A. T., et al. (2016). Effects of mindfulness-based cognitive therapy on body awareness in patients with chronic pain and comorbid depression. Front. Psychol. 7:967. doi: 10.3389/fpsyg.2016.00967
De Jong, M., Peeters, F., Gard, T., Ashih, H., Doorley, J., Walker, R., et al. (2018). A randomised controlled pilot study on mindfulness-based cognitive therapy for unipolar depression in patients with chronic pain. J. Clin. Psychiatry 79:15m10160. doi: 10.4088/JCP.15m10160
Drapeau, A., Marchand, A., and Beaulieu-Prévost, D. (2012). “Epidemiology of psychological distress” in Mental illnesses – understanding, prediction and control. ed. L. Labate (London: IntechOpen Limited), 105–133.
Dworkin, R. H., Turk, D. C., Wyrwich, K. W., Beaton, D., Cleeland, C. S., Farrar, J. T., et al. (2008). Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J. Pain 9, 105–121. doi: 10.1016/j.jpain.2007.09.005
Fordham, B., Sugavanam, T., Edwards, K., Stallard, P., Howard, R., Das-Nair, R., et al. (2021). The evidence for cognitive behavioral therapy in any condition, population, or context: a meta-review of systematic reviews and panoramic meta-analysis. Psychol. Med. 51, 21–29. doi: 10.1017/S0033291720005292
Gardiner, P., Luo, M., D’Amico, S., Gergen-Barnett, K., White, L. F., Saper, R., et al. (2019). Effectiveness of integrative medicine group visits in chronic pain and depressive symptoms: a randomised controlled trial. PLoS One 14:e0225540. doi: 10.1371/journal.pone.0225540
Gasslander, N., Andersson, G., Boström, F., Brandelius, L., Pelling, L., Hamrin, L., et al. (2022). Tailored internet-based cognitive behavioral therapy for individuals with chronic pain and comorbid psychological distress: a randomized controlled trial. Cogn. Behav. Ther. 51, 408–434. doi: 10.1080/16506073.2022.2065528
Gloster, A. T., Walder, N., Levin, M., Twohig, M., and Karekla, M. (2020). The empirical status of acceptance and commitment therapy: a review of meta-analyses. J. Contextual Behav. Sci. 18, 181–192. doi: 10.1016/j.jcbs.2020.09.009
Haugmark, T., Hagen, K. B., Smedslund, G., and Zangi, H. A. (2019). Mindfulness-and acceptance-based interventions for patients with fibromyalgia–a systematic review and meta-analyses. PLoS One 14:e0221897. doi: 10.1371/journal.pone.0221897
Hayes, S. C., and Hofmann, S. G. (2021). "Third-wave" cognitive and behavioral therapies and the emergence of a process-based approach to intervention in psychiatry. World Psychiatry 20, 363–375. doi: 10.1002/wps.20884
Higgins, J. P., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928. doi: 10.1136/bmj.d5928
Hilton, L., Hempel, S., Ewing, B. A., Apaydin, E., Xenakis, L., Newberry, S., et al. (2017). Mindfulness meditation for chronic pain: systematic review and meta-analysis. Ann. Behav. Med. 51, 199–213. doi: 10.1007/s12160-016-9844-2
Hooten, W. M. (2016). Chronic pain and mental health disorders: shared neural mechanisms, epidemiology, and treatment. Mayo Clin. Proc. 91, 955–970. doi: 10.1016/j.mayocp.2016.04.029
Hughes, L. S., Clark, J., Colclough, J. A., Dale, E., and McMillan, D. (2017). Acceptance and commitment therapy (ACT) for chronic pain. Clin. J. Pain 33, 552–568. doi: 10.1097/AJP.0000000000000425
Jorn, A. C. (2015). Elements of the biopsychosocial interview of the chronic pain patient: a new expanded model using rational emotive behavior therapy. J. Ration. Emot. Cogn. Behav. Ther. 33, 284–307. doi: 10.1007/s10942-015-0217-8
Khoo, E. L., Small, R., Cheng, W., Hatchard, T., Glynn, B., Rice, D. B., et al. (2019). Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioral therapy for the treatment and management of chronic pain: a systematic review and network meta-analysis. Evid. Based Ment. Health 22, 26–35. doi: 10.1136/ebmental-2018-300062
Kroenke, K., Wu, J., Bair, M. J., Krebs, E. E., Damush, T. M., and Tu, W. (2011). Reciprocal relationship between pain and depression: a 12-month longitudinal analysis in primary care. J. Pain 12, 964–973. doi: 10.1016/j.jpain.2011.03.003
Lin, J., Scott, W., Carpenter, L., Norton, S., Domhardt, M., Baumeister, H., et al. (2019). Acceptance and commitment therapy for chronic pain: protocol of a systematic review and individual participant data meta-analysis. Syst. Rev. 8, 140–110. doi: 10.1186/s13643-019-1044-2
López-López, J. A., Davies, S. R., Caldwell, D. M., Churchill, R., Peters, T. J., Tallon, D., et al. (2019). The process and delivery of CBT for depression in adults: a systematic review and network meta-analysis. Psychol. Med. 49, 1937–1947. doi: 10.1017/S003329171900120X
Lorenzo-Luaces, L., Johns, E., and Keefe, J. R. (2018). The generalizability of randomised controlled trials of self-guided internet-based cognitive behavioral therapy for depressive symptoms: systematic review and meta-regression analysis. J. Med. Internet Res. 20:e10113. doi: 10.2196/10113
Mansfield, K. E., Sim, J., Jordan, J. L., and Jordan, K. P. (2016). A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain 157, 55–64. doi: 10.1097/j.pain.0000000000000314
McCracken, L. M. (2023). Personalized pain management: is it time for process-based therapy for particular people with chronic pain? Eur. J. Pain 27, 1044–1055. doi: 10.1002/ejp.2091
McCracken, L. M., Yu, L., and Vowles, K. E. (2022). New generation psychological treatments in chronic pain. BMJ 376:e057212. doi: 10.1136/bmj-2021-057212
McGowan, J., Sampson, M., Salzwedel, D. M., Cogo, E., Foerster, V., and Lefebvre, C. (2016). PRESS peer review of electronic search strategies: 2015 guideline statement. J. Clin. Epidemiol. 75, 40–46. doi: 10.1016/j.jclinepi.2016.01.021
Migliorini, C., Sinclair, A., Brown, D., Tonge, B., and New, P. (2016). A randomised control trial of an internet-based cognitive behaviour treatment for mood disorder in adults with chronic spinal cord injury. Spinal Cord 54, 695–701. doi: 10.1038/sc.2015.221
Moore, A. R., Eccleston, C., Derry, S., Wiffen, P., Bell, R. F., Straube, S., et al. (2010). “Evidence” in chronic pain–establishing best practice in the reporting of systematic reviews. Pain 150, 386–389. doi: 10.137110.1016/j.pain.2010.05.011
Ólason, M., Andrason, R. H., Jónsdóttir, I. H., Kristbergsdóttir, H., and Jensen, M. P. (2018). Cognitive behavioral therapy for depression and anxiety in an interdisciplinary rehabilitation program for chronic pain: a randomised controlled trial with a 3-year follow-up. Int. J. Behav. Med. 25, 55–66. doi: 10.1007/s12529-017-9690-z
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int. J. Surg. 88:105906. doi: 10.1016/j.ijsu.2021.105906
Pardos-Gascón, E. M., Narambuena, L., Leal-Costa, C., and Van-der Hofstadt-Román, C. J. (2021). Differential efficacy between cognitive-behavioral therapy and mindfulness-based therapies for chronic pain: systematic review. Int. J. Clin. Health Psychol. 21:100197. doi: 10.1016/j.ijchp.2020.08.001
Pasarelu, C. R., Andersson, G., Bergman Nordgren, L., and Dobrean, A. (2017). Internet-delivered transdiagnostic and tailored cognitive behavioral therapy for anxiety and depression: a systematic review and meta-analysis of randomized controlled trials. Cogn. Behav. Ther. 46, 1–28. doi: 10.1080/16506073.2016.1231219
Rayner, L., Hotopf, M., Petkova, H., Matcham, F., Simpson, A., and McCracken, L. M. (2016). Depression in patients with chronic pain attending a specialised pain treatment Centre: prevalence and impact on health care costs. Pain 157, 1472–1479. doi: 10.1097/j.pain.0000000000000542
Reid, K. J., Harker, J., Bala, M. M., Truyers, C., Kellen, E., Bekkering, G. E., et al. (2011). Epidemiology of chronic non-cancer pain in Europe: narrative review of prevalence, pain treatments, and pain impact. Curr. Med. Res. Opin. 27, 449–462. doi: 10.1185/03007995.2010.545813
Roberts, T., Esponda, G. M., Krupchanka, D., Shidhaye, R., Patel, V., and Rathod, S. (2018). Factors associated with health service utilisation for common mental disorders: a systematic review. BMC Psychiatry 18, 1–19. doi: 10.1186/s12888-018-1837-1
Sanabria-Mazo, J. P., Colomer-Carbonell, A., Borràs, X., Castaño-Asins, J. R., McCracken, L. M., Montero-Marin, J., et al. (2023). Efficacy of videoconference group acceptance and commitment therapy (ACT) and behavioral activation therapy for depression (BATD) for chronic low back pain (CLBP) and comorbid depressive symptoms: a randomized controlled trial (IMPACT study). J. Pain 24, 1522–1540. doi: 10.1016/j.jpain.2023.04.008
Sanabria-Mazo, J. P., Forero, C. G., Cristobal-Narváez, P., Suso-Ribera, C., García-Palacios, A., Colomer-Carbonell, A., et al. (2020). Efficacy, cost-utility and physiological effects of acceptance and commitment therapy (ACT) and behavioral activation treatment for depression (BATD) in patients with chronic low back pain and depression: study protocol of a randomised, controlled trial including mobile-technology-based ecological momentary assessment (IMPACT study). BMJ Open 10:e038107. doi: 10.1136/bmjopen-2020-038107
Sawilowsky, S. S. (2009). New effect size rules of thumb. J. Mod. Appl. Stat. Methods 8, 597–599. doi: 10.22237/jmasm/1257035100
Schlicker, S., Baumeister, H., Buntrock, C., Sander, L., Paganini, S., Lin, J., et al. (2020). A web-and mobile-based intervention for comorbid, recurrent depression in patients with chronic back pain on sick leave (get. back): pilot randomised controlled trial on feasibility, user satisfaction, and effectiveness. JMIR Ment. Health 7:e16398. doi: 10.2196/16398
Sharpe, L., Jones, E., Ashton-James, C. E., Nicholas, M. K., and Refshauge, K. (2020). Necessary components of psychological treatment in pain management programs: a Delphi study. Eur. J. Pain 24, 1160–1168. doi: 10.1002/ejp.1561
Snyder, M., and Handrup, C. T. (2018). Challenges in treatment of comorbid chronic pain, depression, and anxiety. J. Psychosoc. Nurs. Ment. Health Serv. 56, 17–21. doi: 10.3928/02793695-20180601-01
Tlach, L., and Hampel, P. (2011). Long-term effects of a cognitive-behavioral training program for the management of depressive symptoms among patients in orthopedic inpatient rehabilitation of chronic low back pain: a 2-year follow-up. Eur. Spine J. 20, 2143–2151. doi: 10.1007/s00586-011-1810-x
Torrijos-Zarcero, M., Mediavilla, R., Rodríguez-Vega, B., Del Río-Diéguez, M., López-Álvarez, I., Rocamora-González, C., et al. (2021). Mindful self-compassion program for chronic pain patients: a randomised controlled trial. Eur. J. Pain 25, 930–944. doi: 10.1002/ejp.1734
Veehof, M. M., Trompetter, H. R., Bohlmeijer, E. T., and Schreurs, K. M. G. (2016). Acceptance-and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cogn. Behav. Ther. 45, 5–31. doi: 10.1080/16506073.2015.1098724
Walker, A. K., Kavelaars, A., Heijnen, C. J., and Dantzer, R. (2014). Neuroinflammation and comorbidity of pain and depression. Pharmacol. Rev. 66, 80–101. doi: 10.1124/pr.113.008144
White, V., Linardon, J., Stone, J. E., Holmes-Truscott, E., Olive, L., Mikocka-Walus, A., et al. (2022). Online psychological interventions to reduce symptoms of depression, anxiety, and general distress in those with chronic health conditions: a systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 52, 548–573. doi: 10.1017/S0033291720002251
Williams, A. C. C., Fisher, E., Hearn, L., and Eccleston, C. (2020). Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2021:CD007407. doi: 10.1002/14651858.CD007407.pub4
Keywords: cognitive behavioral therapy, chronic pain, distress, depression, anxiety, systematic review
Citation: Sanabria-Mazo JP, Colomer-Carbonell A, Fernández-Vázquez Ó, Noboa-Rocamora G, Cardona-Ros G, McCracken LM, Montes-Pérez A, Castaño-Asins JR, Edo S, Borràs X, Sanz A, Feliu-Soler A and Luciano JV (2023) A systematic review of cognitive behavioral therapy-based interventions for comorbid chronic pain and clinically relevant psychological distress. Front. Psychol. 14:1200685. doi: 10.3389/fpsyg.2023.1200685
Edited by:
Valeria Cioffi, Phenomena Research Group (Italy), ItalyReviewed by:
Lucia Luciana Mosca, Scuola di Specializzazione in Psicoterapia Gestaltica Integrata (SIPGI), ItalyCopyright © 2023 Sanabria-Mazo, Colomer-Carbonell, Fernández-Vázquez, Noboa-Rocamora, Cardona-Ros, McCracken, Montes-Pérez, Castaño-Asins, Edo, Borràs, Sanz, Feliu-Soler and Luciano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan V. Luciano, anVhbnZpY2VudGUubHVjaWFub0B1YWIuY2F0
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.