 Snezana Corovic1Veroljub Vucic2Olgica Mihaljevic3
Snezana Corovic1Veroljub Vucic2Olgica Mihaljevic3 Jelena Djordjevic3
Jelena Djordjevic3 Sofija Colovic4
Sofija Colovic4 Snezana Radovanovic5
Snezana Radovanovic5 Svetlana Radevic5
Svetlana Radevic5 Ivana Simic Vukomanovic5
Ivana Simic Vukomanovic5 Katarina Janicijevic5
Katarina Janicijevic5 Marija Sekulic6
Marija Sekulic6 Svetlana Djukic7*
Svetlana Djukic7* Vladimir Vukomanovic8Ognjen Djordjevic9Gordana Djordjevic9
Vladimir Vukomanovic8Ognjen Djordjevic9Gordana Djordjevic9 Olivera Milovanovic10
Olivera Milovanovic10- 1Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 2Health Center Trstenik, Trstenik, Serbia
- 3Department of Pathophysiology, Faculty of Medical Sciences, University of Kragujevac, Kragujavac, Serbia
- 4Department of Communication Skills, Ethics and Psychology, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 5Department of Social Medicine, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 6Department of Hygiene and Ecology, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 7Department of Internal Medicine, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 8Department of Nuclear Medicine, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 9Depatment of Epidemiology, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 10Department of Pharmacy, Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
Introduction: Social support as a complex construct has a positive influence not only on a patient’s condition but also on the process of the patient’s emotional adjustment to cancer. The goal of this study is to investigate aspects of the level of social support in oncology patients and its interconnection with sociodemographic and medical variables.
Method: The study was conducted as a prospective observational study in 2020, including 250 patients aged 19 and over, both sexes, with a diagnosis of oncological disease. The research was conducted in the Department of General Medicine of the Health Center Trstenik, Central Serbia, after approval by the Ethics Committee of the Health Center Trstenik, Central Serbia. A social support assessment questionnaire (Oslo-3 Social Support Scale) was used as a research instrument.
Results: Data collected from the entire study population showed that bad social support was present in almost 90% of cases. Univariate and multivariate regression analysis showed a statistically significant influence of the following variables on the bad social support: education level, activity limitation, difficulties in performing daily activities, the impact of pain on the performance of activities, the need for additional help with activity, the need for help at home, unfulfilled needs for health care, means of information, anxiety score and depression score.
Conclusion: Interventions to increase social support may be important for enhancing mental health and quality of life in cancer patients.
Introduction
Social support is an interactive construct, an interpersonal transaction that occurs between those who need help and those who give the support. Most authors classify social support into three types: emotional support (when a person feels loved and has a person nearby whom he or she can trust), instrumental support (when a person has someone who can provide help in emergencies), and informational support (when he or she receives information or consultation) (Ruiz-Rodríguez et al., 2022).
According to the National Cancer Institute (NCI) definition, social support is a network of family members, friends, neighbors, and community members who provide cancer patients with psychological, physical, and financial support when they need it. Studies have shown that social support has a positive effect on cancer patient’s physical health, emotional state, well-being, and survival (Website National Cancer Institute, 2009). A cancer diagnosis has a significant impact and consequences for the patient and family. Most cancer patients successfully adjust to cancer diagnosis and treatment, but some initially struggle with a bad mood, feelings of vulnerability, sadness, and anxiety, which are usually followed by inability, weakness, depression, trauma, panic, and worries about existential survival. These feelings and concerns interfere with their normal functioning in daily activities and their quality of life (Daré et al., 2019). Knowing that they can count on the help and support of family and friends plays an important role in coping with the stress caused by disease diagnosis and treatment (Ruiz-Rodríguez et al., 2022). Social support as a complex system of different types of help has a huge constructive impact on patients’ well-being and emotionally stable acceptance of cancer diagnosis (Comijs et al., 2015; Chiu et al., 2017). It is important for cancer patients and is one of the most important psychosocial factors in cancer patients (Geue et al., 2019). Studies have shown that cancer patients who have higher levels of these kinds of support and social bonding have a better quality of life and lower mortality rates. At the same time, those who do not have all these types of support have poorer oncologic outcomes, a higher prevalence of cancer progression, and a lower overall survival rate (Mitchell et al., 2011; Lu et al., 2016; Zhu et al., 2018).
However, little is known in our country about the unmet need for social support among people with cancer and the factors associated with it. Therefore, the goal of our research was to investigate the level of social support in cancer patients and its correlation with sociodemographic and medical variables.
Materials and methods
Study design
The research was conducted in the form of a prospective observational study.
Population under study
The studied population comprised 250 users of health care at the Health Center Trstenik, Central Serbia, aged 19 and over, both sexes, with a diagnosis of oncological disease. The study was conducted between July 2020 and December 2020. The study was conducted by general doctors at the Health Center Trstenik, Central Serbia.
Sampling
Using the statistical program G*Power for the chi-square (χ2) test, with the accepted values of the probable error of the first type α = 0.05 and the power of the study of 0.95, the total sample size was estimated at 250 subjects. The sample size was calculated according to data from studies of similar design (Geue et al., 2019). The sampling method was randomized population sample. The studied population comprised users of health care at the Health Center Trstenik, Central Serbia.
The protocols of this research were approved by the Ethics Committee of the Health Center Trstenik, Central Serbia (No 759/1 of 26.06.2020.). The study adhered to the ethical standards in line with the international (Helsinki Declaration) and national legislation. In addition, the privacy of the respondents and confidentiality of data were ensured by undertaking all necessary steps in line with the Law on the Protection of Personal Data (“Official Gazette of the RS” no. 97/08, 104/09), Law on Official Statistics (“Official Gazette of the RS” no. 104/09).
Participation in the research was voluntary. Before the start of the study, patients were introduced to the purpose and procedure of the study and gave informed consent to participate in this study. Inclusion criteria for participation in the study were patients with diagnosed oncological diseases who signed informed consent for participation in the study. Data on the presence of oncological diseases as well as the presence of other chronic non-communicable diseases (comorbidity), were collected by inspecting the medical documentation (health records), while exclusion criteria were patients under 19 years of age, the presence of psychiatric illness, the presence of acute infectious (infectious) disease, the presence of chronic infectious diseases, pregnant women and patients who did not give a written consent to participate in the study.
Assessment instruments
In addition to the general questionnaire on demographic and socio-economic characteristics (European Health Survey Questionnaire - Second Wave) (Eurostat, 2013), a questionnaire for assessing social support (Oslo-3 Social Support Scale) was used as a research instrument. The social support score (Oslo-3 Social Support Scale) was formed on the basis of three questions from the questionnaire: the first question “How many people are so close to you that you can count on them when you have serious personal problems?” [number of points from 1 (“None”) to 4 (“6 or more”)]; the second question “How much are people really interested in you, in what you do, what happens in your life?” [number of points from 1 (“They are not interested at all”) to 5 (“They are very interested”)] and the third question. “How easy is it to get practical help from neighbors if you need it?” [number of points from 1 (“Very difficult”) to 5 (“Very easy”)]. After collecting points, social support points were formed: strong social support (12–14 points), moderate (9–11 points) and bad (3–8 points) (Sarason et al., 1983). A research instruments to assess depressive and anxiety symptoms is used PHQ-9 (The Patient Health Questionnaire) questionnaire (Beck and Steer, 1990) and the Beck Anxiety Scale (BAI) (Kroenke et al., 2001).
The independent variables in the research were: sociodemographic characteristics (age, gender, family structure, marital status, education, material status, type of settlement, occupation, use of primary and hospital health care, unmet health care needs); determinants of health (alcohol and smoking use, hygiene habits, physical activity, eating habits, self-assessment of health, stress, ability to perform daily activities, presence of another chronic non-communicable disease), while the dependent variable in the study was social support in oncology patients.
Statistical analysis
Descriptive statistics methods were used to present the data: tabulation and graphical representation. Analysis of Variance (ANOVA) used to analyze the difference between the means of more than two groups. Independent sample t-test is used to analyze the mean comparison of two independent groups. The relationships between the dependent variable (social support) and the set of independent variables were examined by univariate and multivariate logistic regression. The risk was assessed using the size of the OR (odds ratio), with a 95% confidence interval. All results where the probability is less than 5% (p < 0.05) were considered statistically significant. All statistical calculations were done using the commercial, standard software package SPSS, version 20.0 (Chicago, IL, United States).
Results
The study included 250 patients diagnosed with cancer. All patients were aged 19 and over. Two thirds of the patients were women (69.6%), more often married 68.4%, with secondary education 39.6%. Based on the answers fto the questions from the questionnaire for the assessment of social support (Oslo-3 Social Support Scale) a social support score was obtained, the average value of which for the entire study population was (7.06 ± 1.25). The obtained values at the level of the entire study population point to poor social support in nearly 90% of cases. Sociodemographic and health characteristics of the respondents as well as differences in social support scores are shown in Tables 1, 2. In relation to gender, the mean value of the social support score for women was (6.94 ± 1.29), and for men (7.32 ± 1.12). Unmarried respondents, with less education and unemployed have a higher average social support score (Table 1). Major difficulties in performing daily activities (7.32 ± 0.99), severe limitation (7.37 ± 1.14), more than five chronic diseases/conditions in addition to cancer in 12 months (7.11 ± 1.36) were associated with higher average scores of social support. In relation to the stage of the disease, the existence of a statistically significant difference in the mean values of the social support score was not confirmed (p = 0.912), patients in the first stage 7.03 ± 1.25, patients in the second stage 7.11 ± 1.29, patients in in the third stage of the disease 7.0 ± 0.0. No statistically significant influence of the type of therapy on the average values of the social support score was shown (p = 0.963). Between operated and non-operated patients and the average score of social support no statistically significant difference (6.99 ± 1.32 vs. 7.14 ± 1.6) (p = 0.348), (Table 2).
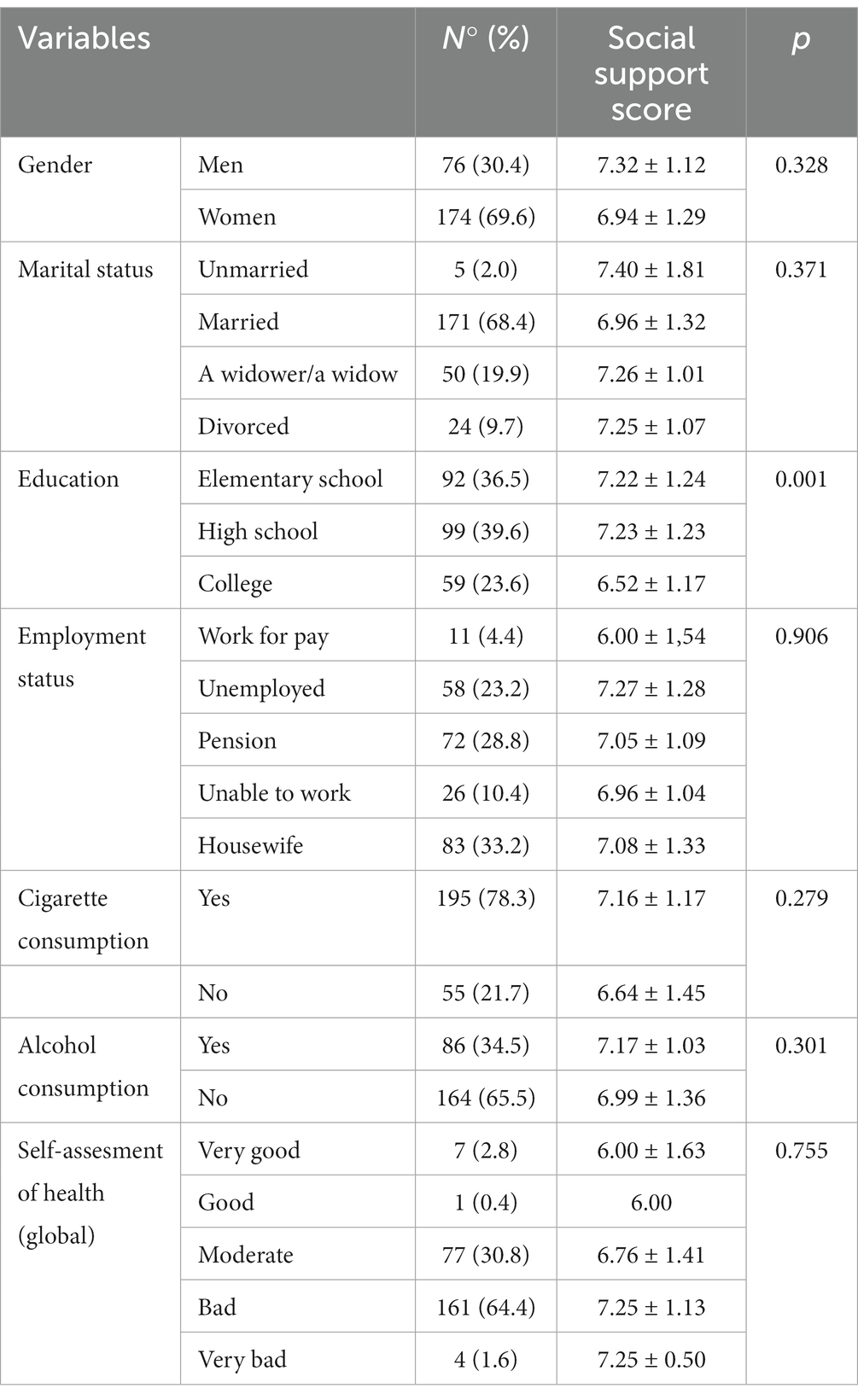
Table 1. Sociodemographic characteristics of cancer patients and social support score.

Table 2. Health characteristics of cancer patients and social support score.
Breast cancer (28.3%), bronchial and lung cancer (7.2%) and prostate cancer (5.6%). were the most common cancers in the studied population. Statistical data processing revealed the existence of a significant difference in the social support score among patients suffering from different types of cancer (One-Way ANOVA, df (30) = 2.217, p = 0.001). The highest average values of the social support score were found in patients with pancreatic cancer (8.2) and bladder cancer (8.1) (Table 3).
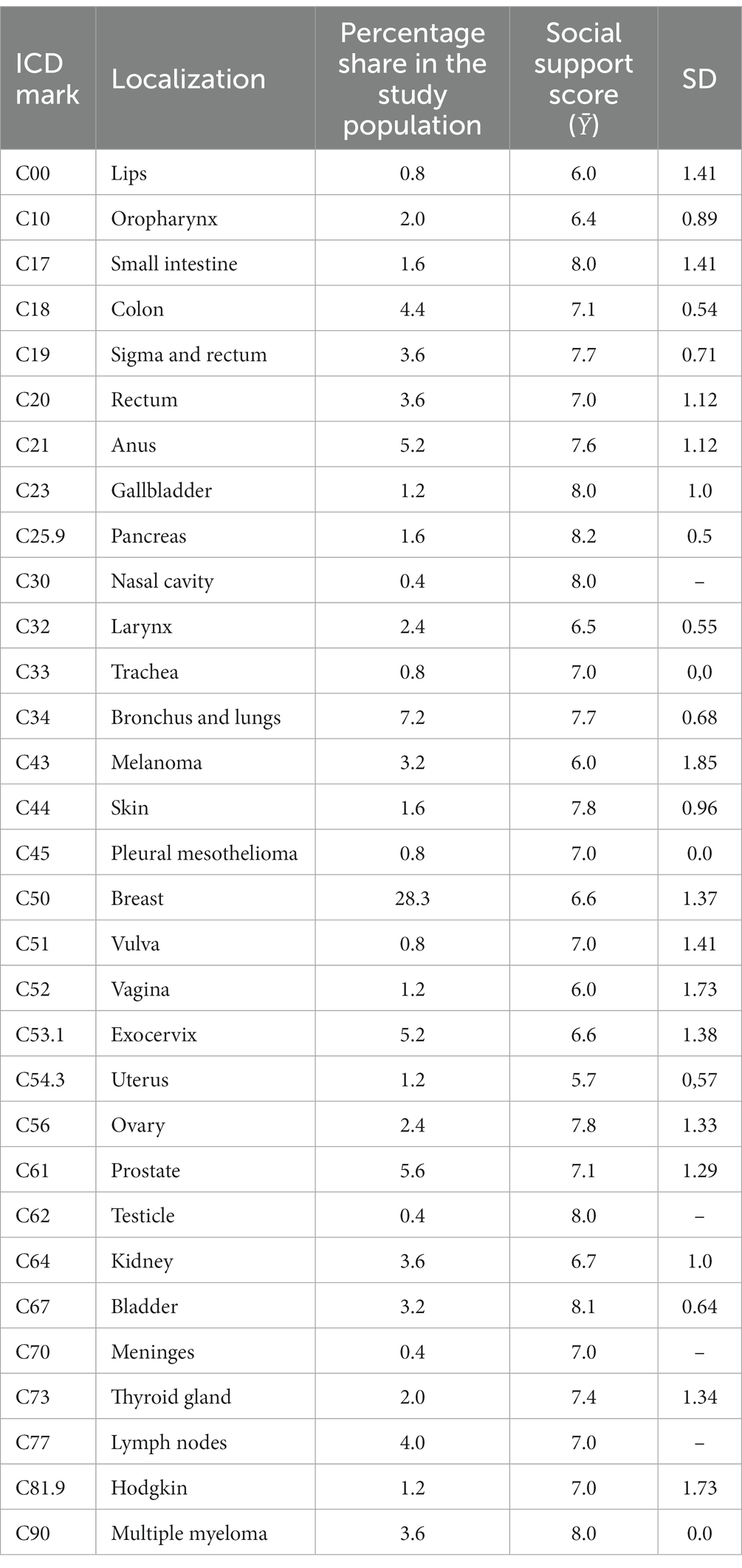
Table 3. Social support score in patients with different cancers.
Data collected from the entire study population showed that bad social support was present in almost 90% of cases. Univariate and multivariate regression analysis showed a statistically significant influence of the following variables on the bad social support: education level, activity limitation, difficulties in performing daily activities, the impact of pain on the performance of activities, the need for additional help with activity, the need for help at home, unfulfilled needs for health care, means of information, anxiety score and depression score (Table 4).
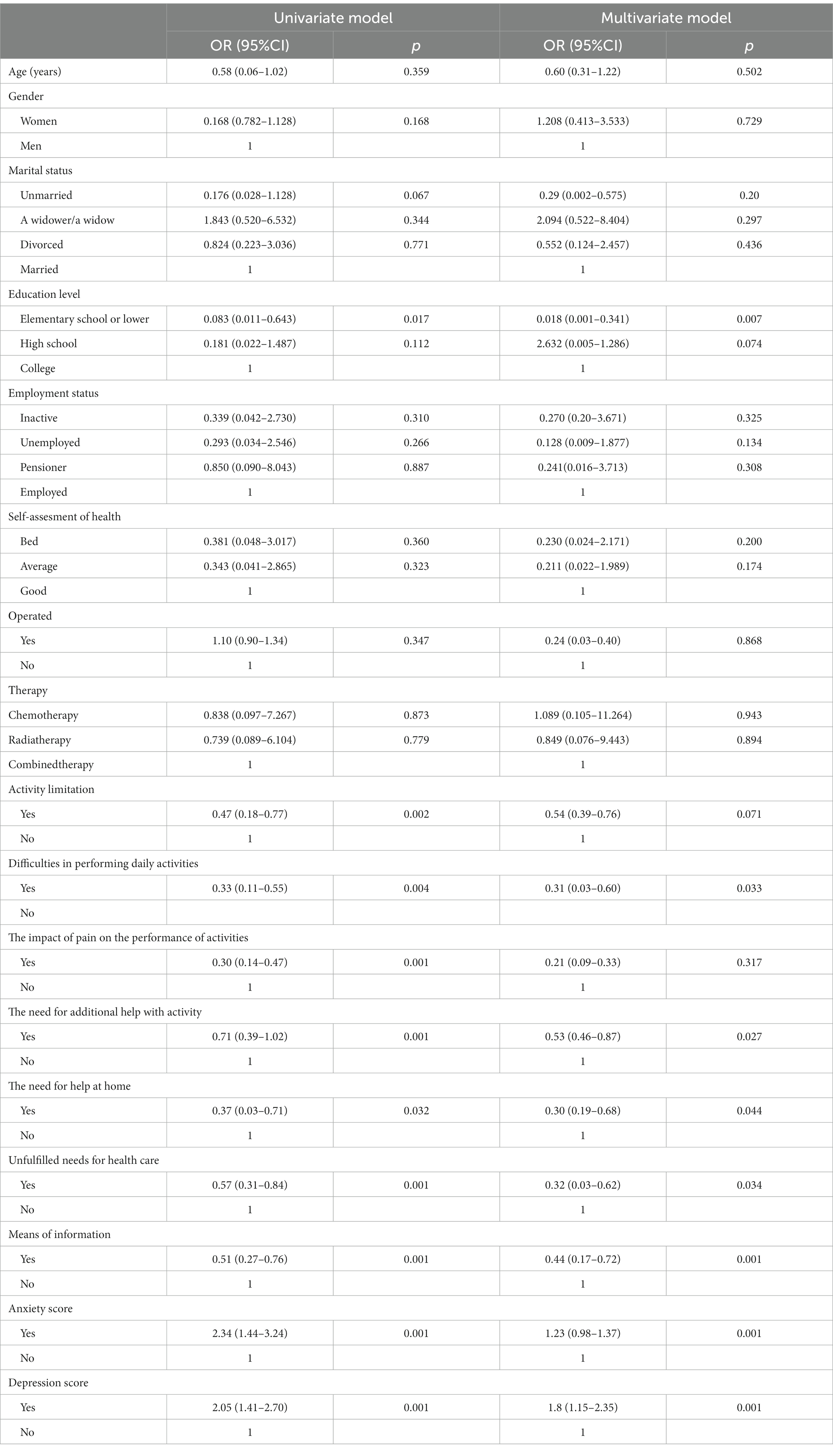
Table 4. Odds ratios (ORs) with the corresponding 95% confidence intervals (CIs) for the association between of social support score and patient characteristics.
Discussion
The concept of social support involves the willing or actual provision of relationships, information, advice, or assistance that enables a person to successfully cope with the day-to-day challenges of crisis in their personal life. Social support has a structural and a functional dimension. The structural dimension refers to the presence of social relationships, and the functional dimension refers to the various types of help provided by people within a person’s social network that one usually thinks of when one thinks of social support. In addition, there are other categories of functional measurements, such as emotional, instrumental, and counseling support (Ruiz-Rodríguez et al., 2022). Social support plays an important role in the daily life of cancer patients. Some studies have shown that social support contributes to coping, good mood, physical condition, emotional status, and overall quality of life while reducing disease-related stress (Usta, 2012).
Social support is very important in helping cancer patients alleviate the negative effects of cancer diagnosis and treatment and improve the consequences of cancer disease. An analysis of population diagnosed with cancer found that patients who experienced more social support had stronger mental health and quality of life (Taylor et al., 2007; Kadambi et al., 2020).
The results of our research indicate poor social support in patients with malignant diseases. Also, when viewed in relation to the sociodemographic and health characteristics of the subjects of our study, a low level of social support can be observed.
One study showed that married patients had a greater sense of hope and more social support than single patients (Ghazzawi et al., 2016). Another study that included cancer patients also found that patients who have a partner or are in a marriage have a better quality of life and more social support than single patients (Lavdaniti et al., 2017). This is supported by cancer patients’ statements that their spouse is the most important source of social support (Leung et al., 2014), which is contrary to the results of our study, where a bad score of social support was recorded for married respondents. Results obtained after analysing variables with social support dimensions corroborate findings of literature, in which men received more social support than women. The results showed that patients who had stronger social support had a greater sense of security and were less tired from chemotherapy (Karakoç and Yurtsever, 2010).
There is also a study that shows the connection between a lower level of social support and a significantly higher level of depression, suggesting that social support contributes to mental health and a higher quality of life (Eom et al., 2013). Studies have shown that patients with strong social support develop more optimistic feelings, which enable them to increase their confidence and hope that they can successfully fight and cure cancer (Kyriazidou et al., 2022). Studies examining the relationship between social support, depression, and quality of life in patients with various cancer diagnoses found that patients who did not have significant social support were more likely to suffer from depression, had lower functional abilities, and had a lower quality of life (Korotkin et al., 2019), which is in line with the results of our reaserch in a statistically significant influence of the anxiety and depression as a predictor the bad social support.
A study examining the types of social support patients considered important concluded that cancer patients most frequently expressed a desire for companionship, empathy, assistance with home care, information, equal treatment, and help to make appointments at healthcare facilities. Anxious patients were more likely to want companionship, and younger patients were more likely to want assistance with home care (Nausheen et al., 2009; Schroevers et al., 2010).
The results suggest that support from family and friends in the postdiagnosis period plays an important role in helping cancer patients develop a positive attitude toward cancer (Calderon et al., 2021).
A study examining was the associations between perceived social support and sociodemographic variables on coping showed that sociodemographic factors as age, education, and partnership status were associated with coping strategies. Hopelessness was more frequent in older people and lower educational level and single people. Support from family, friends, and partners was associated with a greater fighting spirit. In contrast, high psychological distress, anxiety and depression was associated with bad level social support (Faraci and Bottaro, 2021), which is in line with the results of our reaserch which also suggest the connection education, anxiety, depression and social support.
The value of social support is that it plays an important role in preventing and reducing anxiety and depression in cancer patients, contributes to mental health and a higher quality of life. Furthermore, social support has a direct impact on insecurity/uncertainty and the greater the support of family members and healthcare professionals, the lesser the uncertainty in relation to treatment and pathology. Twhen this support is received, patients develop a sense of importance in a social network, respond positively to challenges and adopt positive behavior, such as initiating or maintaining actions that promote wellbeing in their social circle and enhance the proposed treatment. Social support can come from bonds between people and groups, which include natural collaborators (family), informal groups (self-help) and formal and institutionalized groups, such as organizations for the sick, that can create the support networks of patients. This support refers to the help of others in case of need and also reflects access to healthcare services and actions from other people that help to solve practical activities. The acknowledgement that social support can help cancer patients to adapt and maintain a quality of life means accepting the need to identify the arrangement of a support network made available to users so that care can be planned and implemented with quality (Kolankiewicz et al., 2014).
Although several valuable findings were identified in the present study, we must acknowledge some limitations. First and foremost is that the nature of cross-sectional survey design limits the ability of establishing causality between the proposed variables. And thus, further study with longitudinal design will be necessary to prospectively clear the mechanism of social support. Second, the sample is not representative. Data were obtained from a specific population group, with its cultural, economic and social configurations which does not have the same characteristics and potentialities in all regions of Serbia. Third, we assessed social support, using self-reported questionnaires in the present study and the results may be inflated due to subjective bias from participants.
Implications for practice
Contributions of this study that should be emphasized are that the dimensions that make up social support should be topics of concern for healthcare professionals. Developing countries, such as Serbia, do not possess sufficient resources due to which it would be possible to provide adequate chosocial support to cancer-affected patients along with their family members. Practitioners can enhance the benefits of social support programs through strengthening. This study enhanced our understanding on the association social support in cancer patients Another contribution of the study is the acknowledgement that some groups are more vulnerable than others, and that socioeconimc factors should be observed in order to identify them and help these groups overcome difficulties in the initial stages of cancer. This study can serve as a model for investigations on other groups patients and for the characterization of social support.
Conclusion
Considering the significance and influence of social support on patients‘mental and physical health, it is necessary not only to conduct further research studies on the factors having influence on the level social support, but to implement various interventions for the the purpose of their promotion as well. In order to create adequate public health policies and strategies that are needed to improve social support it is essential to determine and expose different predictors of bad social support. Encouraging patients with malignant diseases to activate social and social engagement can help reduce anxiety and depressive symptoms, prevent suicidal ideation, improve cognitive and functional status and enable easier coping with the disease and psychosocial difficulties, which will result in a better quality of life for these patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Health Center Trstenik, Central Serbia (No 759/1 of 26.06.2020). The patients/participants provided their written informed consent to participate in this study.
Author contributions
SC, VlV, and SnR: design and writing manuscript. OM, JD, and SC conducted the statistical analyses, commented on the manuscript and contributed to the background, and discussion section. SnR, IV, KJ, MS, SD VlV, OD, GD, and OM contributed to investigation. SC, VeV, OM, JD, SC, SnR, SvR, IV, KJ, MS, SD, VlV, OD, GD, and OM: critical revision and approval of the final draft. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Calderon, C., Gomez, D., Carmona-Bayonas, A., Hernandez, R., Ghanem, I., Gil Raga, M., et al. (2021). Social support, coping strategies and sociodemographic factors in women with breast cancer. Clin. Transl. Oncol. 23, 1955–1960. doi: 10.1007/s12094-021-02592-y
Chiu, C. J., Hsu, Y. C., and Tseng, S. P. (2017). Psychological prognosis after newly diagnosed chronic conditions:socio-demographic and clinical correlations. Int. Psychogeriatr. 29, 281–292. doi: 10.1017/S1041610216001630
Comijs, H. C., Nieuwesteeg, J., Kok, R., van Marwijk, H. W., van der Mast, R. C., Naarding, P., et al. (2015). The two-year course of late-life depression; results from the Netherlands study of depression in older persons. BMC Psychiatry 15:20. doi: 10.1186/s12888-015-0401-5
Daré, L. O., Bruand, P., Gérard, D., Marin, B., Lameyre, V., Boumédiène, F., et al. (2019). Co-morbidities of mental disorders and chronic physical diseases in developing and emerging countries: a meta-analysis. BMC Public Health 19:304. doi: 10.1186/s12889-019-6623-6
Eom, C. S., Shin, D. W., Kim, S. Y., Yang, H. K., Jo, H. S., Kweon, S. S., et al. (2013). Impact of perceived social support on the mental health and health-related quality of life in cancer patients: results from a nationwide, multicenter survey in South Korea. Psychooncology 22, 1283–1290. doi: 10.1002/pon.3133
Eurostat (2013). European health interview survey (EHIS wave 2). Methodological manual, 2013. Luxembourg: Publications Office of the European Union.
Faraci, P., and Bottaro, R. (2021). A cross-sectional study examining the relationship between socio-demographics and coping styles in a group of Cancer patients. Clin. Neuropsychiatry 18, 3–12. doi: 10.36131/cnfioritieditore20210101
Geue, K., Göbel, P., Leuteritz, K., Nowe, E., Sender, A., Stöbel-Richter, Y., et al. (2019). Anxiety and depression in young adult German Cancer patients: time course and associated factors. Psychooncology 28, 2083–2090. doi: 10.1002/pon.5197
Ghazzawi, A., Kuziemsky, C., and Sullivan, O. (2016). T. Using a complex adaptive system lens to understand family caregiving experiences navigating the stroke rehabilitation system. BMC Health Serv. Res. 16:538. doi: 10.1186/s12913-016-1795-6
Kadambi, S., Soto-Perez-de-Celis, E., Garg, T., Loh, K. P., Krok-Schoen, J. L., Battisti, N. M. L., et al. (2020). Social support for older adults with cancer: young International Society of Geriatric Oncology review paper. J Geriatr Oncol. 11, 217–224. doi: 10.1016/j.jgo.2019.09.005
Karakoç, T., and Yurtsever, S. (2010). Relationship between social support and fatigue in geriatric patients receiving outpatient chemotherapy. Eur. J. Oncol. Nurs. 14, 61–67. doi: 10.1016/j.ejon.2009.07.001
Kolankiewicz, A. C. B., Souza, M. M., Magnago, T. S. B. S., and Domenico, E. B. L. D. E. (2014). Social support perceived by cancer patients and its relation with social and demographic characteristics. Revista gaucha de enfermagem 35, 31–38. doi: 10.1590/1983-1447.2014.01.42491
Korotkin, B. D., Hoerger, M., Voorhees, S., Allen, C. O., Robinson, W. R., and Duberstein, P. R. (2019). Social support in cancer: how do patients want us to help? J. Psychosoc. Oncol. 37, 699–712. doi: 10.1080/07347332.2019.1580331
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Kyriazidou, E., Alevizopoulos, N., Dokutsidou, E., Kavga, A., Kalemikerakis, I., Konstantinidis, T., et al. (2022). Health-related quality of life and social support of elderly lung and gastrointestinal Cancer patients undergoing chemotherapy. SAGE Open Nurs. 8:23779608221106444. doi: 10.1177/23779608221106444
Lavdaniti, M., Zyga, S., Vlachou, E., and Sapountzi-Krepia, D. (2017). Quality of life in elderly Cancer patients undergoing chemotherapy. Adv. Exp. Med. Biol. 989, 291–295. doi: 10.1007/978-3-319-57348-9_27
Leung, J., Pachana, N. A., and McLaughlin, D. (2014). Social support and health-related quality of life in women with breast cancer: a longitudinal study. Psychooncology 23, 1014–1020. doi: 10.1002/pon.3523
Lu, D., Andersson, T. M., Fall, K., Hultman, C. M., Czene, K., Valdimarsdottir, U., et al. (2016). Clinical diagnosis of mental disorders immediately before and after Cancer diagnosis: a Nationwide matched cohort study in Sweden. JAMA Oncol. 2, 1188–1196. doi: 10.1001/jamaoncol.2016.0483
Mitchell, A. J., Chan, M., Bhatti, H., Halton, M., Grassi, L., Johansen, C., et al. (2011). Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 12, 160–174. doi: 10.1016/S1470-2045(11)70002-X
Nausheen, B., Gidron, Y., Peveler, R., and Moss-Morris, R. (2009). Social support and cancer progression: a systematic review. J. Psychosom. Res. 67, 403–415. doi: 10.1016/j.jpsychores.2008.12.012
Ruiz-Rodríguez, I., Hombrados-Mendieta, I., Melguizo-Garín, A., and Martos-Méndez, M. J. (2022). The importance of social support, optimism and resilience on the quality of life of Cancer patients. Front. Psychol. 13:833176. doi: 10.3389/fpsyg.2022.833176
Sarason, I. G., Levine, H. M., Basham, R. B., and Sarason, B. R. (1983). Assessing social support: the social support questionnaire. J. Pers. Soc. Psychol. 44, 127–139. doi: 10.1037/0022-3514.44.1.127
Schroevers, M. J., Helgeson, V. S., Sanderman, R., and Ranchor, A. V. (2010). Type of social support matters for prediction of posttraumatic growth among cancer survivors. Psychooncology 19, 46–53. doi: 10.1002/pon.1501
Taylor, S. E., Welch, W. T., Kim, H. S., and Sherman, D. K. (2007). Cultural differences in the impact of social support on psychological and biological stress responses. Psychol. Sci. 18, 831–837. doi: 10.1111/j.1467-9280.2007.01987.x
Usta, Y. Y. (2012). Importance of social support in cancer patients. Asian Pac. J. Cancer Prev. 13, 3569–3572. doi: 10.7314/APJCP.2012.13.8.3569
Website National Cancer Institute . (2009) NCI dictionary of cancer terms. Available at: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/social-support (Accessed March 28,2022)
Keywords: tumors, social-, support, patients, score
Citation: Corovic S, Vucic V, Mihaljevic O, Djordjevic J, Colovic S, Radovanovic S, Radevic S, Vukomanovic IS, Janicijevic K, Sekulic M, Djukic S, Vukomanovic V, Djordjevic O, Djordjevic G and Milovanovic O (2023) Social support score in patients with malignant diseases—with sociodemographic and medical characteristics. Front. Psychol. 14:1160020. doi: 10.3389/fpsyg.2023.1160020
Edited by:
Paolo Fabbietti, National Institute of Science and Health for Aging (IRCCS), ItalyReviewed by:
Jiyoung Kim, Inha University, Republic of KoreaAleksandar Višnjić, University of Niš, Serbia
Copyright © 2023 Corovic, Vucic, Mihaljevic, Djordjevic, Colovic, Radovanovic, Radevic, Vukomanovic, Janicijevic, Sekulic, Djukic, Vukomanovic, Djordjevic, Djordjevic and Milovanovic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Svetlana Djukic, ZHJzdmV0bGFuYWRqdWtpY0BnbWFpbC5jb20=