 Marion Robin1,2*
Marion Robin1,2* Luc Surjous1,3Jean Belbèze1,3Lucile Bonnardel1Claire Lamas1Jérôme Silva1Victoire Peres1
Luc Surjous1,3Jean Belbèze1,3Lucile Bonnardel1Claire Lamas1Jérôme Silva1Victoire Peres1 Maurice Corcos1,3
Maurice Corcos1,3- 1Department of Adolescent and Young Adult Psychiatry, Institut Mutualiste Montsouris, Paris, France
- 2CESP, INSERM U1178, Paris-Saclay University, Villejuif, France
- 3Paris Cité University, Paris, France
Introduction: Emotion regulation is altered in many psychiatric disorders in adolescence, but the understanding of mechanisms that underlie this alteration is still poor.
Methods: The PERCEPT study explores alexithymia, empathy, facial emotion recognition (FER) and defence mechanisms in a sample of adolescents in psychiatric care (n = 61, 74% of girls, mean age = 15.03 y.o.), in relation with participants’ attachment styles.
Results: Results revealed correlations between attachment dimensions and all of the emotion regulation variables, suggesting that attachment modalities have functional links with emotional regulation at its different levels: FER accuracy was inversely correlated with avoidant attachment, while affective empathy, difficulty in identifying feelings (alexithymia) and immature as well as neurotic defence mechanisms were positively correlated with anxious attachment. Moreover, attachment categories delineated distinct emotional perception profiles. In particular, preoccupied attachment included adolescents with the highest levels of facial emotion perception (sensitivity and accuracy) and of affective empathy, whereas detached attachment included adolescents with the lowest levels of these variables. Neurotic defence mechanisms and difficulty to identify feelings were correlated with preoccupied attachment; immature defence mechanisms and difficulty to describe feelings to others characterized fearful attachment.
Discussion: These results suggest that attachment categories underlie emotion regulation processes in psychiatric disorders in adolescence. Theoretical and clinical implications are discussed.
1. Introduction
Emotion regulation is the ability of an individual to cope with an emotion or a set of emotions, to respond to an emotional experience. It is a complex psychological process that covers both the ability to trigger, inhibit, maintain or modulate one’s own affects in a broad sense, which includes physiological processes (e.g., heart rate), behaviors (e.g., laughter), cognitive processes and subjective feelings (Thompson, 2008; McRae and Gross, 2020). Into this multi-layered process, the perception of emotion, of others or within oneself, constitutes one of the early and central stages of emotional regulation across human emotional and interpersonal experiences (Hildebrandt et al., 2012; Addabbo et al., 2018). Facial emotion is one of the non-verbal components of communication, which provides information about the affective states of the subject who expresses it, but also about his or her behavioral intentions (Ekman et al., 1976; de Bonis et al., 1999). It also speaks from a social perspective, in which each emotion has a specific functionality. The perception (or recognition or identification) of emotions is therefore central to any form of communication in relationships. The concept of alexithymia describes the inability to detect its own emotions. It is a personality construct characterized by difficulty in identifying and describing feelings, a lack of fantasy, and a concrete and externally oriented thinking style (Sifneos, 1973c Taylor et al., 2003). Empathy, another dimension of emotion regulation, refers not only to emotion perception, but also to the ability to identify with or understand the perspective, experiences, or motivations of another individual and to comprehend and share his/her emotional state (Thompson et al., 2019). Finally, defence mechanisms are historically the first dimension of emotion regulation described (Freud, 1936/2001; Bailey and Pico, 2022). They were envisaged as a modality of reducing or removing any modification likely to endanger the integrity and constancy of the biopsychological individual (Laplanche and Pontalis, 1967).
In the last two decades, emotion regulation has increasingly been incorporated into models of psychopathology (Berenbaum et al., 2003; Mennin and Farach, 2007), and a growing number of data have pointed toward the existence of an impairment in a wide range of psychiatric disorders, visible in children, adolescents and adults, and impacting on family and peer relationships (Britton et al., 2010; Svaldi et al., 2012; Collin et al., 2013; Simcock et al., 2020). Most studies report emotional regulation deficits by describing a single dimension into a single diagnostic category, whether they explore alexithymia, facial emotion recognition (FER), defence mechanisms or empathy (Domes et al., 2009; Mitchell et al., 2014; Green et al., 2015; Jáni and Kašpárek, 2018) in adults and in adolescents. A main limit pointed out by these studies is the impossibility of concluding to a specificity of the described emotional particularity, as the comorbidities are so numerous, and as the described dimensions seem to cross nosographic categories (Domes et al., 2009; Preißler et al., 2010; Jovev et al., 2011; Mitchell et al., 2014; England-Mason, 2020). A number of studies concluded that difficulties in emotion perception were not linked to a particular diagnosis category, but, instead, appeared to be a transdiagnostic risk and/or maintenance factor (Svaldi et al., 2012; Cludius et al., 2020). Moreover, the few studies that have excluded most of comorbidities, for example in BPD, have also clearly limited the generalizability of their findings to the community of patients and deplored it (Minzenberg et al., 2006; Domes et al., 2008). Fewer articles described emotion perception abilities in adolescents, particularly in patients with severe psychiatric disorders, in a transnosographic perspective. Adolescents hospitalized in psychiatry are representative of adolescents with a severe emotional and social dysfunction, partly due to cumulative adversity (Robin et al., 2021). Delineating emotions perception profiles at this age could allow a better understanding of psychopathology and possibly orientate prevention and treatment (Kumari, 2020).
Impairment in empathy and FER were clearly described in anxiety, depression, and neurodevelopmental disorders (Mendlewicz et al., 2005; Habel et al., 2006; Chan et al., 2008; Kohler et al., 2010; Green et al., 2015; Graziano and Garcia, 2016; Tseng et al., 2017; England-Mason, 2020). However, results were more heterogeneous in the context of Eating Disorders (ED) and Borderline Personality Disorders (BPD). In both of these diagnoses, which are highly comorbid, FER and empathy are alternatively described as higher, comparable or lower than in healthy controls in adults and in adolescents (Domes et al., 2009; Robin et al., 2012; Mitchell et al., 2014; Cardi et al., 2015; Tchanturia et al., 2015; Dapelo et al., 2016). Renwick et al. (2015) explored this discrepancy among adults with Anorexia Nervosa, and observed that three separate clusters emerged when analyzing social-cognitive measures (emotional theory of mind), with high, medium, and low-level groups. Some explanation of the discrepancy in social cognition in these patients has been searched in the distinction of FER skills or empathy dimensions. This attempt revealed for example that BPD patients are highly responsive to the feelings of others (affective empathy), but are deficient in identifying/describing feelings and in taking the perspective of others (cognitive empathy) (New et al., 2012; Dinsdale and Crespi, 2013).
Attachment modalities toward caregivers have been shown to influence emotion regulation (Fonagy and Luyten, 2009; Timpano and Port, 2021). Attachment orientations have important implications for emotion regulation and health, and attachment insecurity is associated with deficits in neural structure associated with emotion regulation (Mikulincer and Shaver, 2019). Although attachment disorders and emotional regulation have both been explored in a variety of diagnostic areas, their relationship has been most extensively studied in BPD. Indeed, patients with this diagnosis show significant emotional dysregulation (this is a diagnostic criterion) and in this disorder, attachment is particularly insecure (Miljkovitch et al., 2018). According to Bowlby’s (1969, 1982) concept of the internal working model, individuals develop models of self as more or less lovable and of others as more or less reliable and loving, depending on the quality of received care. In this line, both dimensional and categorical measures of attachment were built in a complementary way. Dimensional measures of attachment focus on attachment anxiety (negative model of the self, preoccupation with the availability and responsiveness of others with expectation of abandonment) and avoidance (negative model of others and devaluation of the importance of close relationships) (Main, 1995; Hazan and Shaver, 1987; Brennan et al., 1998). Bartholomew (1990) defined four prototypic attachment categories based on these underlying dimensions: secure (positive self and other model), fearful (negative self and other model), preoccupied (negative self model, positive other model) and dismissing (negative other model, positive self model). Thus, the negative model of self (fearful and preoccupied styles) relates to anxiety, while the negative model of others relates to avoidance (secure and dismissing styles). Attachment is considered disorganized when no category emerges in a stable manner. These two descriptive modalities of attachment (dimensions and categories) are used alternately according to the studies, which extends their interest but also makes comparisons difficult from one study to another, depending on whether the method is dimensional or categorical (Ravitz et al., 2010).
Studies have highlighted that BPD patients mostly show preoccupied, fearful and disorganized attachment patterns (Levy et al., 2005; Fonagy and Luyten, 2016), both of which have been hypothesized to influence emotion regulation in BPD (Skodol et al., 2002). Individuals with high levels of attachment anxiety, because of their hypersensitivity to rejection and abandonment, are supposed to develop hypersensitivity to external features in others, including affective facial expressions (Mikulincer and Shaver, 2007, 2008). Individuals high on attachment avoidance, by contrast, are often particularly poor at “reading” facial expression in others because of their tendency to deactivate attachment concerns (Van Heel et al., 2019). Studies on attachment modalities and FER are less frequent in other psychiatric diagnoses, but have also identified an influence of attachment modalities on emotion perception in Anorexia Nervosa (Doba and Nandrino, 2020). Studies on this topic are still lacking in other clinical areas and the understanding of the links between attachment and emotional regulation remains very partial. A review of the links between attachment and empathy, however, suggested a significant link between empathy and avoidant and secure attachment, but an insignificant link between empathy and anxious attachment (Xu et al., 2022). As for the links between alexithymia and attachment, several studies have shown negative correlations between alexithymia and attachment security (Troisi et al., 2001; Montebarocci et al., 2004; Wearden et al., 2005). This is consistent with Bowlby's (1969) view that secure attachment is fundamental to allowing exploration of internal emotional states.
In the field of emotional regulation, defence mechanisms have been less explored than other aspects of emotion regulation in the last years. They constitute a modality of reducing or removing any modification likely to endanger the integrity and constancy of the biopsychological individual (Laplanche and Pontalis, 1967). They allow protecting the personality of the subject by decreasing the anguish, which can be felt in a given situation, thus they are a central element of the emotional regulation. Recent studies have demonstrated that defences can be arranged hierarchically based on their usual level of adaptiveness, and that defensive functioning tends to improve over the course of psychotherapy in stepwise fashion (Drapeau et al., 2003; Bond and Perry, 2004; Perry and Bond, 2012). Various authors have attempted to describe them precisely according to psychiatric diagnoses, most often using the Defence Style Questionnaire (Perry and Cooper, 1986; Bond, 1992; Paris et al., 1996; Koenigsberg et al., 2001), but their transnosographic role in emotion regulation and perception has still to be investigated. In this line, Ciocca et al. (2020) have recently demonstrated that attachment styles – preoccupied and fearful, and defence mechanisms – immature and neurotic, had a substantial impact on psychological distress in a sample of students.
In sum, there are a number of arguments to suggest that there is a link between attachment modalities and emotional regulation, a link that seems to underlie psychiatric diagnoses (Wearden et al., 2005; Mikulincer and Shaver, 2007, 2008). This link has so far been explored mainly separately for each dimension of emotional regulation (Ciocca et al., 2020; Xu et al., 2022), whereas we believe that a common analysis could be useful in order to understand psychiatric psychopathology in a more unified way. Similarly, research on attachment finds that the dimensions and categories make different but complementary contributions, which encourages their analysis in a single study (Bartholomew and Horowitz, 1991; Ravitz et al., 2010). Finally, these links between emotional regulation and attachment have not been explored in adolescents independently of their psychiatric diagnoses. For all these reasons, the aim of the present work is to explore, in an adolescent psychiatric sample, the links of attachment dimensions and categories with emotion regulation in a transnosographic perspective. Our first hypothesis is that the dimensions of attachment are correlated with all levels of emotional regulation explored: emotional recognition, empathy, alexithymia, defence mechanisms. Our second hypothesis is that it is possible to distinguish different modalities of emotional regulation according to the categories of attachment in these patients.
2. Materials and methods
2.1. Participants
The PERCEPT study included 61 inpatient adolescents admitted in an urban psychiatric crisis unit during 6 months, from October 2018 to April 2019 (Institut Mutualiste Montsouris, Paris, France). The unit receives adolescents referred by psychiatrists for any psychiatric crisis situation. The study was proposed to 65 patients successively hospitalized, in order to evaluate their emotion regulation with regard to their attachment styles. The inclusion criteria were all hospitalized patients who agreed to the research (as well as their parents); and the exclusion criteria were the impossibility for a patient to participate in an experimental test, either for a reason of refusal or for an incapacity related to their condition (incompatible state of agitation or incapacity to understand the task). The average length of hospitalization for these patients was 22 days and recruitment was done at the end of the hospitalization. The questionnaires were given to the patient during the last week of hospitalization, and they returned them to the investigator on the day of the experiment. Four patients refused to participate and one patient was not clinically able to. Procedures were approved by the Ethics Committee of Necker Hospital, Paris, France (CPP-IDFII-2013-09-10).
All participants were native European adolescents, including 74% of girls (sex assigned at birth), aged from 13 to 19 years old (m = 15.03 y.o., sd = 1.3). Most of them (52.9%) belonged to families with high economic status. Fifty-seven patients (93.4%) were currently under psychotropic medication, and fifty patients (81.9%) had received at least one psychotropic treatment prior to hospitalization. Twenty-seven patients (44.3%) had experienced self-injury, and thirteen patients (21.3%) had shown aggressive behaviors. Regarding patients’ medical profiles, the variety of diagnoses has led us to group them into categories: 36.1% of patients were diagnosed with an anxiety or depressive disorder, 39.3% with a BPD, 32.8% with Eating Disorders, and 22.9% with a psychosis (schizophrenia, autism, or pervasive developmental disorder). Most patients had more than one diagnoses (2.2 diagnoses on average per patient), and in this case, the main diagnosis that was retained was the most clinically invasive. Distribution of these diagnoses according to the four categories of attachment was measured for secure attachment (33% anxiety-depressive patients, 22% BPD patients, 22% of patients with ED, and 22% of patients with psychosis), fearful attachment (27% anx-dep, 33% BPD, 33% ED, 7% psychosis), preoccupied attachment (21% anx-dep, 33% BPD, 33% ED, 12% psychosis), and detached attachment (23% anx-dep, 23% BPD, 15% ED, 39% psychosis).
2.2. Procedure
All subjects completed a research protocol, including a self-reported questionnaire assessing socio-demographic, psychopathological data, and the behavioral task. Diagnoses of axis-I and axis-II disorders according to the DSM 5 criteria were collected from the patient’s records at the end of the hospitalization.
Alexithymia was assessed with the 20-item Toronto Alexithymia Scale (TAS-20; Bagby et al., 1994a,b), a 5 points Likert-scale questionnaire. The 20 items of the TAS are clustered into three factors corresponding to the theoretical dimensions of alexithymia: Difficulty Identifying Feelings (DIF), Difficulty Describing Feelings (DDF), and Externally Oriented Thinking (EOT). TAS-20 scores are reliable, and the three-factor structure is replicable (Bagby et al., 1994a). The TAS-20 is currently the most widely used measure of alexithymia, and considerable work has gone into testing its reliability and validity (Bagby et al., 1994b; Parker et al., 2003; Taylor et al., 2003).
For the self-reported assessment of empathic abilities, the Interpersonal Reactivity Index (IRI; Davis, 1983) was used. Participants had to rate 32 statements describing their empathic abilities with scores ranging from 0 (that does not describe me well) to 4 (that describes me very well). The questionnaire consists of two dimensions of affective and cognitive empathy, and has good reliability with a Cronbach’s alpha of 0.78.
Defence mechanisms were evaluated with the Defence Style Questionnaire (DSQ) (Bond and Vaillant, 1986), which is a 9-point Likert-scale that measures the conscious derivatives of different defence mechanisms through 88 items. The defence score is the average response of items contributing to the specific set. A higher score indicates greater use of the respective defence mechanism. According to Andrews et al. (1989), a factor analysis has identified 25 separate defences that cluster into three higher order defence styles by their functional adequacy: mature, including suppression, task orientation, anticipation, sublimation, and humour; neurotic, including reaction formation, undoing, inhibition, withdrawal, idealization, and pseudo-altruism; and immature, including projection, passive aggression, acting out, omnipotence/devaluation, help rejecting, fantasy, isolation, splitting, projective identification, regression, somatization, denial, affiliation, and consumption. The DSQ has been shown to discriminate control populations from psychiatric outpatients, as well as from patients with eating disorders (Steiger et al., 1989) and anxiety disorders (Bond and Vaillant, 1986; Andrews et al., 1989; Martin et al., 2019).
In order to assess attachment categories, we used the Relationship Questionnaire (RQ, Bartholomew and Horowitz, 1991), which consists of four paragraphs giving rise to both categorical and continuous data. The categorical measure is a forced-choice measure whereby participants select one of the four paragraphs indicating their attachment style as secure, preoccupied (anxious), fearful (anxious and avoidant), or dismissive (avoidant). The continuous measure, in which individuals indicate the extent to which they resemble each of the four attachment styles on a 7-point scale (1 = not like me at all to 7 = very much like me), gives rise to four continuous scales. The RQ has demonstrated adequate predictive validity and test–retest reliability, and is a widely used measure of attachment modalities (Scharfe and Bartholomew, 1994; Herzberg et al., 1999; Wongpakaran et al., 2021).
All these tools are frequently used in adolescent research samples.
2.3. Emotion recognition
Emotion recognition was assessed with a task that comprised 36 trials presented in a random order. The stimuli were taken from the empirically valid and reliable pictures of the facial affect series of Ekman and Friesen (1976). Each trial began with a neutral face gradually morphed into one of the six prototypical emotions—sadness, anger, happiness, disgust, surprise, and fear—according to forty 2.5% incremental stages. Each picture was presented for 500 ms followed immediately by the next morphed face in the sequence. Each trial therefore consisted of a 20 s continuum. We used the pictures of three men and three women, who were each expressing the six emotions of interest. Each emotion was thus presented six times. Participants were asked to report the emotion expressed whenever they thought they had identified it, by clicking on one of the six corresponding boxes. They were also told that they could change their initial response at any time and as often as necessary by clicking again, and that they had to indicate their final choice at the end of each trial (40th stage). With this paradigm, two FER skills were scored: accuracy was measured by the final success rate (i.e., percentage of correct response at 100% expression), and sensitivity by the precociousness of a right emotional recognition. It is measured by the difference between the final stage (40th stage) and the mean number of stages required for the accurate identification of facial emotions, across the trials in which the participants successfully recognized the final expression (Sensitivity = 40 − n). The greater is the difference between 40 and the number of images needed, the earlier the emotional recognition and the higher the sensitivity. The first variable describes the ability to recognize emotion independently of time, while the second describes its rapidity.
2.4. Data analysis
Emotional variables were first compared to age, sex and psychotropic number and using spearman correlations and student t-tests. Spearman correlations were also performed between emotional variables and attachment dimensions in the whole sample. We then used Kruskal-Wallis tests to determine statistically significant differences between mean levels of empathy, FER, Alexithymia and Defence mechanisms in the four attachment categories, as a one-way ANOVA non-parametric equivalence (R software).
3. Results
The effects of age, sex and medication on emotion variables are reported in Table 1. We observed significant positive effect of age on FER sensitivity, of gender on affective empathy and defence mechanisms: affective empathy, as well as immature and neurotic defences mechanisms were more frequent in young women than in young men.
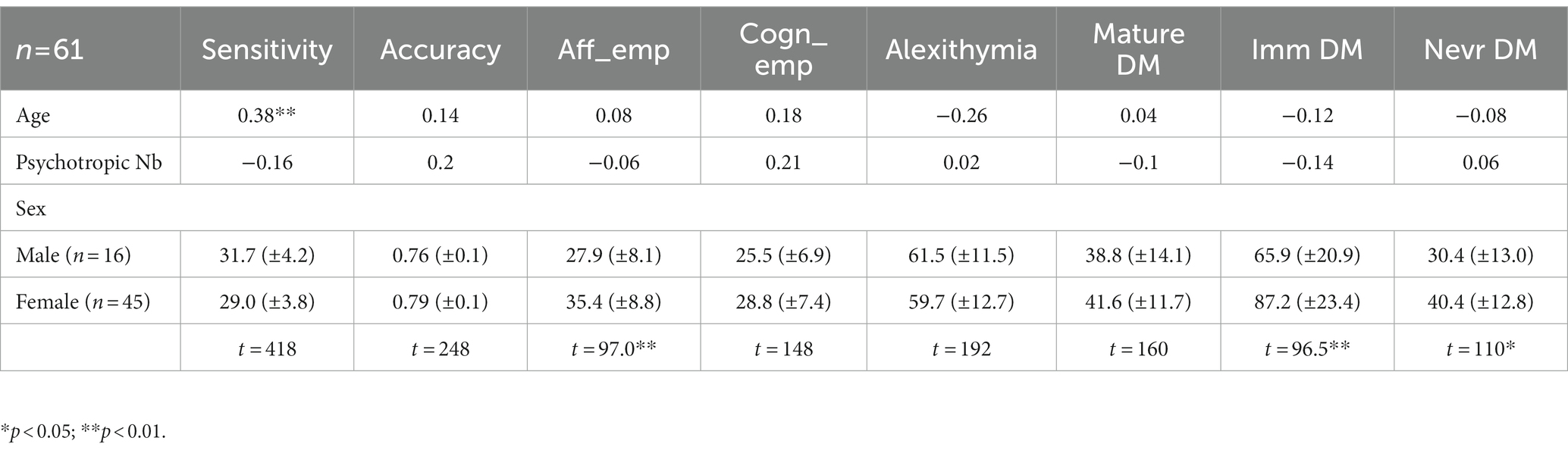
Table 1. Correlations between age, psychotropic number and emotion regulation variables, and t-tests of emotion regulation variables by sex: facial emotion recognition sensitivity and accuracy, affective empathy, cognitive empathy, alexithymia, mature, immature and nevrotic defence mechanisms (Aff_emp, Affective empathy; Cogn_emp, Cognitive empathy; DM, Defence Mechanisms; Nb, number).
3.1. Emotion regulation and attachment dimensions
Correlations between emotion regulation variables are reported in Figure 2:
• Anxious attachment was positively and significantly correlated to affective empathy, Nevrotic and Immature Defence mechanisms and Difficulty in Identifying Feelings.
• Avoidant attachment was negatively and significantly correlated to FER Accuracy.
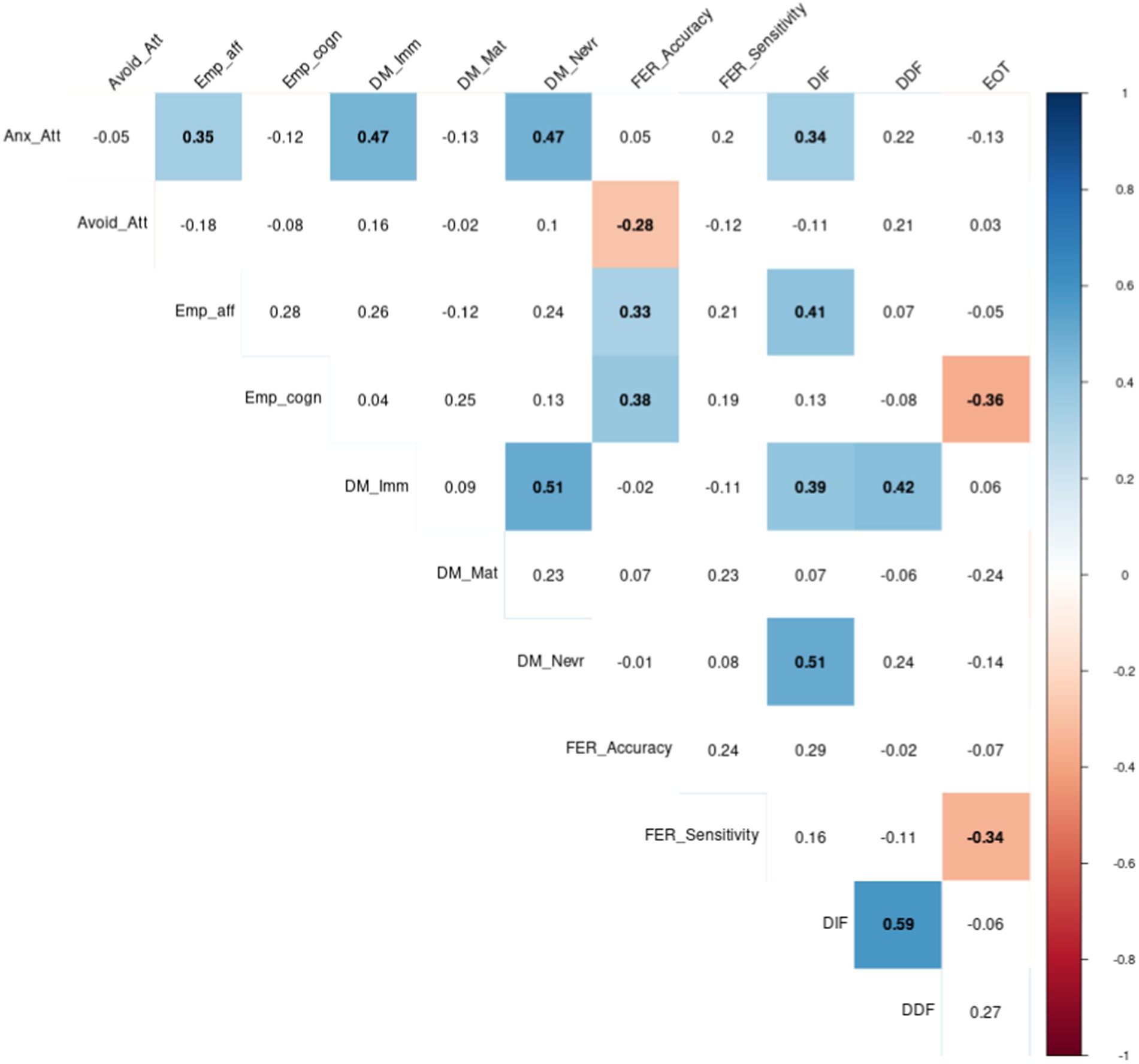
Figure 1. Correlations between emotion regulation variables: Attachment, Empathy, Defence Mechanisms, Facial Emotion Recognition and Alexithymia (Anx_att, Anxious attachment; Avoid_att, Avoidant attachment; Emp_aff, Affective Empathy; Emp_cogn, Cognitive Empathy; DM_Imm, Immature Defence Mechanism; DM_Mat, Mature Defence Mechanism; DM_Nevr, Nevrotic Defence Mechanism; FER_Accuracy, Facial Emotion Recognition Accuracy; FER_sensitivity, Facial Emotion Recognition Sensitivity; DIF, Difficulty Identifying Feelings; DDF, Difficulty Describing Feelings; EOT, External Oriented Thinking).p < 0.05.
We also observed correlations between emotional regulation variables. Among them:
• Empathy scores were positively correlated with DIF (affective empathy) and FER accuracy (affective and cognitive empathy), but negatively correlated with EOT (cognitive empathy).
• FER sensitivity was negatively correlated with EOT (alexithymia).
• Alexithymia was positively correlated with defence mechanisms: DIF score was correlated to Immature and Nevrotic defence mechanisms, while DDF score was correlated to Immature dimension. DIF score was also positively correlated with affective empathy, and EOT was negatively correlated with cognitive empathy.
3.2. Emotion regulation and attachment categories
Distribution of Empathy, Facial Emotion Recognition, Alexithymia and Defence Mechanisms levels by attachment categories and Kruskal-Wallis tests are reported in Table 2. It revealed contrasts, mostly for affective empathy and FER sensitivity among attachment categories, which, respectively, reached and tended to reach significance. Their highest scores were both observed in the preoccupied attachment category. It also revealed significant discrepancies in alexithymia (DIF and DDF) and defence mechanisms (total, neurotic and immature) among attachment categories. Considering the cut-off score of alexithymia, only preoccupied and fearful patients were alexithymic. The highest scores of DIF and DDF were observed in fearful attachment, as was the highest score of immature defence mechanisms, whereas highest scores of total and neurotic defence mechanisms were observed in the preoccupied attachment style.
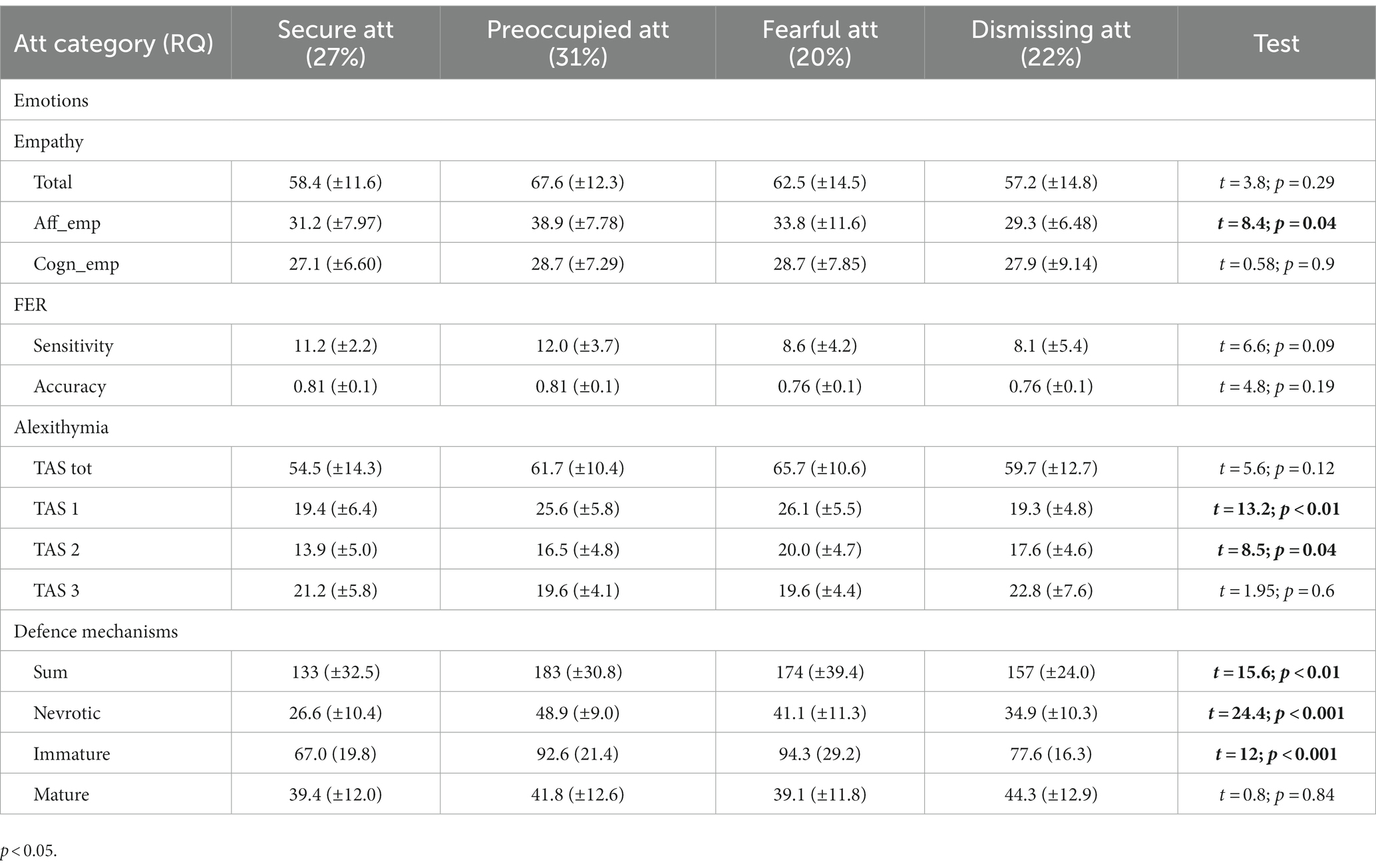
Table 2. Means of empathy, facial emotion recognition, alexithymia and defence mechanisms levels by attachment categories and Kruskal-Wallis tests results (Att, attachment; Emp_aff, Affective empathy; Emp_cogn, Cognitive empathy; FER, Facial Emotion Recognition; TAS, Toronto Alexithymia Scale; RQ, Relationship Questionnaire).
4. Discussion
Adolescents hospitalized in psychiatry are characterized by severe relational dysfunction, but so far little is known about the way these patients process emotion regulation.
4.1. Attachment modalities and emotion regulation
Our results revealed correlations between attachment dimensions and all of the emotion regulation variables: facial emotion recognition, empathy, alexithymia and defence mechanisms. While FER accuracy was correlated to avoidant dimension, the other three dimensions were correlated with the anxiety dimension of attachment. The fact that correlations were found on all the dimensions of emotional regulation explored suggests that attachment modalities have functional links with emotional regulation at its different levels.
The results also revealed that attachment categories might delineate distinct profiles of emotion regulation in this population sample. In particular:
• secure patients had the lowest scores of alexithymia and defence mechanisms, and intermediate levels of empathy and FER skills.
• preoccupied attachment included adolescents with high levels of alexithymia, FER skills (sensitivity and accuracy), affective empathy and defence mechanisms.
• dismissing patients showed low levels of alexithymia (DIF and DDF), FER skills, affective empathy and defence mechanisms.
• fearful attachment included adolescents with high levels of alexithymia and defence mechanisms, but medium or low levels of FER skills and empathic concern.
The distribution of psychiatric diagnoses according to the four categories of attachment revealed that anxiety-depressive patients were predominantly represented by secure attachment, while BPD and ED patients were mostly included in preoccupied and fearful categories. Psychotic troubles were more represented in detached attachment.
4.1.1. Attachment dimensions and categories with FER
The accuracy variable in FER was correlated with the avoidant dimension of attachment, in the sense that the more avoidant the subject’s attachment, the less able he or she was to identify emotions on another’s face. This study is in line with previous research on attachment dimensions and emotion recognition in BPD patients, which described individuals with BPD and healthy controls that score high on attachment avoidance showing impaired recognition of facial expressions in a RMET study (Van Heel et al., 2019). Authors commented that this result was consistent with findings that individuals with high avoidant attachment are often poor at recognizing facial emotions because they tend to deactivate attachment needs and concerns (Fonagy et al., 2003). However, other studies have shown different results. In previous studies, individuals with high levels of attachment anxiety had been described as developing hypersensitivity to affective facial expressions of others (Niedenthal et al., 2002; Mikulincer and Shaver, 2007, 2008). There is currently no consensus as to whether attachment phenomena are inherently categorical or dimensional (Ravitz et al., 2010), and it is perhaps the dual consideration of attachment via dimensions and categories at the same time that allows us to see the extent to which the two anxious and avoidant dimensions combine their effects with respect to facial emotion recognition. Statistical analyses suggested that attachment categories allowed a distinction of emotional profiles, although, probably due to the sample size, these results did not reach statistical significance for FER accuracy. Subjects with low-avoidant attachment had significantly better FER abilities (significant dimensional correlations), but between the two low-avoidant categories (secure and preoccupied), FER scores would be highest in the preoccupied style (tendency in categorical analyses). This suggests that the subjects with the best perception abilities have an insecure attachment, and it is consistent with the observations of Niedenthal et al. (2002) that insecure individuals showed better FER abilities than healthy subjects. Furthermore, it is those who meet both the condition of having a negative self-model and a positive other-model who would be most likely to observe others with acuity. This suggests that this is the relational situation that involves the most dependence and high motivation to seek closeness with a person deemed more reliable than oneself, which could lead one to look more intensely for signs of its availability to regulate one’s own emotions.
4.1.2. Attachment dimensions and categories with empathy
Our results revealed a positive correlation between anxious attachment and affective empathy. The highest level of affective empathy was also observed in the preoccupied style beyond the categorical analyses. These results reinforce the hypothesis that they are links between both attachment and empathy, even if the nature of these links is still unclear today. A recent meta-analysis of Xu et al. (2022) described a correlation between cognitive empathy and secure attachment in children and adolescents, and a low significant negative correlation between empathy and avoidant attachment. There is some evidence to support a link between empathy and attachment, but results vary widely depending on contextual, developmental, and methodological factors (Cassidy and Stern, 2018). Our results are not in line with the previous results, which, for the most part, are not based on clinical populations (Xu et al., 2022). Neurodevelopmental studies found that the development of affective empathy was related with that of the limbic amygdala, whereas the development of cognitive empathy was consistent with that of the prefrontal cortex, a brain region related to higher and more mature cognitive functions (Cui et al., 2008). Our results are consistent with the notion that in some psychological disorders such as BPD, amygdala hyperactivity develops in parallel with prefrontal disconnexion (New et al., 2007), and this could be associated with the excessive development of affective empathy unbalanced by cognitive empathy.
The predominant repartition of BPD in negative self-model attachment categories is in significant agreement with the literature, as many authors have described that adolescent or adult BPD patients show preoccupied or fearful attachment (Deborde et al., 2012). According to Fonagy and Bateman (2006), both insecure attachment and dysfunctional affect regulation constitute predisposing factors for the development of BPD. In our sample, negative self-model attachment categories (preoccupied and fearful), in which BPD were mostly represented, included high level of anxious attachment, alexithymia and defence mechanisms. While research consistently showed that BPD patients have biases in mental state attribution (e.g., evaluate others as malevolent) and are alexithymic, research focusing on emotion perception and empathy is less consistent (Preißler et al., 2010; Roepke et al., 2013; Kiliç et al., 2020; Németh et al., 2020). The empathy paradox refers to empirical evidence that BPD subjects may demonstrate enhanced empathy in spite of impaired interpersonal functioning (Krohn, 1974; Dinsdale and Crespi, 2013). A review of 28 studies on empathy in BPD reported comparable levels of evidence for enhanced, preserved, and reduced empathic skills in individuals with BPD (Dinsdale and Crespi, 2013). Similarly, studies have shown heterogeneous theory of mind abilities in ED (Renwick et al., 2015), with clusters of patients, which were not differing in ED symptoms, comorbidity features or treatment characteristics. In our study, the predominant repartition of AN and BPD in preoccupied and fearful categories of attachment suggests that the unexplained heterogeneity in social cognitions in some studies may be partly attributable to attachment heterogeneity, in AN as in BPD, which represents more than a high comorbidity, a very intricate common functioning (Khosravi, 2020). It suggests that heterogeneity in attachment in BPD and ED profiles may contribute to this discrepancy in literature data, with patients associating high empathic skills as a result of high anxious and low avoidant attachment, and patients with lower empathic skills as a result of lower anxious and higher avoidant attachment than in preoccupied category.
4.1.3. Attachment dimensions and categories with alexithymia
Correlations between attachment dimensions and alexithymia total scores and subscales revealed that the difficulty in identifying feelings was linked with anxious dimension. Alexithymia, a personality construct characterized by this difficulty to identify and describe feelings, a lack of fantasy, and a concrete and externally oriented thinking style (Sifneos, 1973; Taylor et al., 2003), is largely described among psychiatric disorders in adults and adolescents (Bankier et al., 2001; Deborde et al., 2012; Leweke et al., 2012).
Among attachment categories, comparison of alexithymia total scores revealed that the difficulty in identifying feelings was mostly present in patients with anxious attachment (preoccupied and fearful), whereas the difficulty in describing feelings was more specifically described in fearful category of attachment. Our results echo previous studies describing that in young men with depressive symptoms, those with preoccupied or fearful categories had a higher prevalence of alexithymia than those with a dismissing category (Troisi et al., 2001). Wearden et al. (2005) also described association between negative model of the self, negative affectivity and fearful/preoccupied attachment categories. In this study, regression analyses showed that alexithymia particularly mediated the relationship between symptom reporting and fearful attachment. Our results reinforce arguments to consider more clearly alexithymia and alexithymia subscales with an attachment view, closely linked to preoccupied and fearful categories, but not to dismissive category. This result echo studies, which explored he links between alexithymia and psychotic or neurodevelopmental troubles (which in our sample mostly composed dismissive category of attachment), and which reported that these disorders are not associated with alexithymia or only in specific sub-groups (Henry et al., 2010; Kinnaird et al., 2019).
4.1.4. Attachment dimensions and categories with defence mechanisms
The distribution of defence mechanisms according to the axes of attachment in our study suggests a strong coherence between these two theoretical systems, which are described from different angles. However, there are very few studies in the literature to which our results can be compared, probably because of the important theoretical differences from which these concepts originate. By revealing correlations of neurotic and immature defence mechanisms with the anxious dimension of attachment, our results reinforces previous results, in which the effect of attachment style was mediated by defence mechanisms: 30% of the effect of fearful and preoccupied attachment styles on psychological distress in a sample of young healthy adults was mediated by immature and neurotic defences. Attachment style and defence mechanisms accounted for nearly 25% of the variance in psychological distress (Ciocca et al., 2020). Moreover, our study is in line with studies on BPD, in which described defence mechanisms included devaluation, passive aggression, omnipotence, primitive idealization, projective identification, retroactive cancelation, projection and cleavage. These immature mechanisms (Kernberg, 1975) had been linked to the BPD interpersonal skills impairment, including a strong dependency (Perry and Cooper, 1986; Presniak et al., 2010), the difficulty to express their needs to others, the tendency to project one’s internal states onto others, and the cleavage of the Ego with what it implies of devaluation of the self. Our results suggest a strong interaction between attachment dimensions or categories and defence mechanisms, and call for further investigation of these interactions.
4.2. Synthesis
In sum, our results suggest the existence of four emotional profiles. 1. In secure attachment, subjects are connected to their emotions, and to those of others. They have low levels of defence mechanisms, and may regulate emotions with the help of their internal resources and those of others: it is a self-and-other oriented emotion perception. 2. In preoccupied attachment, subjects are disconnected from their emotions (alexithymic) but strongly connected to the emotions of others: it is an other-oriented emotion perception. It suggests that the high level of neurotic defence mechanisms in these patients allows an adaptation to insecurity, by affiliation to others’ emotions and expectations, with a relative maintenance of reality testing. 3. In dismissing attachment, subjects are disconnected from others’ emotions and expectations, but have maintained a connection to their own emotions: it is a self-oriented emotion perception. The place of mature defence mechanisms in their functioning argues for autonomic attitudes, but, in this insecure context, it may be at the cost of a loss of reality resting. 4. In fearful attachment, patients are disconnected from their emotions, as well as from the emotions of others, with a high level of immature defence mechanisms. These patients have very few resources to cope with stressful situations: they are disconnected from emotions.
Our results echo theory and practical evidence that have described psychopathology in a transdiagnostic manner (Norton and Paulus, 2016; Norton and Roberge, 2017; Pearl and Norton, 2017). After having analyzed psychiatric disorders in a categorical way, some authors have, in line with Barlow et al. (2004), indeed defended the interest of a unified perspective of emotional disorders. Our observations pursue this reflection by highlighting the extent to which attachment could play an underlying but fundamental role.
4.3. Emotion regulation in adolescents
The adolescent status of patients in this study questions the effect of cerebral maturity in emotion regulation at an age where emotional consciousness in only emergent (Lerner and Steinberg, 2004). The large time lag between amygdala maturity and prefrontal cortex maturity, which characterizes neuronal development in healthy adolescents (Giedd et al., 1999; Sowell et al., 1999), has sometimes been suggested to play a role in adolescent difficulties in emotional information processing. In particular, parietal and frontal lobe areas have been shown to handle experiences of dynamic emotional stimuli, while temporal and limbic-related cortices process information about static emotional stimuli (Adolphs et al., 2003), raising the possibility that adolescents may be less sensitive to some stimuli than adults. Our results reinforce this hypothesis, in describing a positive correlation between age and sensitivity. Finally, patients’ sex ratio in this study has shown a possible influence on empathy and defence mechanisms, which is in agreement with the literature on gender and empathy or emotion recognition (McClure, 2000). Most published studies on emotion recognition have only included women and further studies should analyze emotional recognition in male adolescents, who are supposed to have more difficulties in facial expression processing in general as well as in BPD (McClure, 2000). Finally, the difference we observed in defence mechanisms scores between young men and women should be explored further, but echoes the study from Paris et al. (1996), in which men with BPD had comparable defence profiles to women with BPD (even if they did not have a lower adaptive profile score).
4.4. Limits and perspectives
The current study has certain limitations that must be considered. The sample size is limited to analyze the existence of subgroups. Some results failed to reach significance, probably due to this limit. However, descriptive data among attachment styles were interesting to observe independently of analyses, and were consistent with a number of data in the literature. Moreover, correlations analyses on the entire group were in line with data described in this four-classes analysis. Attachment categories were also measured using only a brief self-report questionnaire. Thus, participants’ responses reflected subjective evaluations rather than actual attachment strategies. Nevertheless, subjective representation is considered to be relevant to understanding the processes at work in psychopathology (Cassidy, 1994). Another limitation of the present study relates to the diagnosis assessment, which was not done after a structured interview, and is thus less reliable. Diagnostic instruments were not used for feasibility reasons (instability of patients). This prevented us from making more advanced comparisons between psychiatric diagnoses. Nevertheless, only one psychiatrist assessed the whole sample, according to DSM-5 criteria during their hospitalization, thus eliminating inter-rater discrepancy. Moreover, this psychiatrist is used to structured diagnostic interviews. The third main limitation was that most of our subjects were medicated, raising the question of the effect of medication on emotion perception. It is unclear whether psychotropic drugs can influence emotion identification, as the results of the few studies that looked at the impact of medication on emotion perception are very heterogeneous. Most of them however found no differences between medicated and unmedicated groups in adolescents and adults (Lynch et al., 2006; Dickstein et al., 2007; Guyer et al., 2007; Schenkel et al., 2007; Brotman et al., 2008a,b; Jänsch et al., 2009; Kalmar et al., 2009). In the present study, no link was found between the number of psychotropic treatments and emotion perception or defence mechanisms. It suggests that a potential medication effect on emotion perception would be secondary to attachment modalities. The convergence between FER skills and empathy, which have been measured in different ways – experimental and self-report questionnaire– (explicit knowledge is less easily influenced by medication than attention/perception modalities) argues for effects of psychopathology independently of medication. Finally, patients with heterogeneous medical diagnoses constitute this sample. Multiple data in the literature have pointed to the limitation of exploring emotional regulation within a diagnosis. Indeed, their results often showed heterogeneity of functioning within patients in one diagnosis, and the sample size (usually about 20–30 patients) did not allow the effect of comorbidities to be measured nor to conclude to a diagnostic specificity (Minzenberg et al., 2006; Domes et al., 2008; Kerr-Gaffney et al., 2019; McMahon et al., 2019). Thus, we voluntarily chose a transnosographic study for this reason, but recognize the inherent limitations of this choice in terms of the heterogeneity of the clinical sample. Despite these limitations, this study is, to our knowledge, the first to explore emotional perception and attachment styles in such a large sample of severe psychic troubles in adolescence in a transnosographic perspective. Patients in this sample are representative of typical adolescents hospitalized in a psychiatric department, with high severity and much comorbidity. These findings further our understanding of the differences in emotion perception in clinical conditions, including static and morphing stimuli, and constitute a basis of comparison for future research at this key period of development.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://doi.org/10.6084/m9.figshare.19292051.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of Necker Hospital, Paris, France (CPP-IDFII-2013-09-10). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
MR and MC performed the conceptualization. MR and VP performed the methodology. VP, LS, LB, and MR were performed material preparation, investigation, and data collection. MR and VP performed the formal analysis. MR performed the original draft preparation, and LS, JB, CL, and MC reviewed it. MC performed the supervision. MR wrote the manuscript and all co-authors approved it. All authors contributed to the study conception and design.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Addabbo, M., Longhi, E., Marchis, I. C., Tagliabue, P., and Turati, C. (2018). Dynamic facial expressions of emotions are discriminated at birth. PLoS One 13:e0193868. doi: 10.1371/journal.pone.0193868
Adolphs, R., Tranel, D., and Damasio, A. R. (2003). Dissociable neural systems for recognizing emotions. Brain Cogn. 52, 61–69. doi: 10.1016/s0278-2626(03)00009-5
Andrews, G., Pollock, C., and Stewart, G. (1989). The determination of defence style by questionnaire. Arch. Gen. Psychiatry 46, 455–460. doi: 10.1001/archpsyc.1989.01810050069011
Bagby, R. M., Parker, J. D., and Taylor, G. J. (1994a). The twenty-item Toronto alexithymia scale–I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 38, 23–32. doi: 10.1016/0022-3999(94)90005-1
Bagby, R. M., Taylor, G. J., and Parker, J. D. (1994b). The twenty-item Toronto alexithymia scale–II. Convergent, discriminant, and concurrent validity. J. Psychosom. Res. 38, 33–40. doi: 10.1016/0022-3999(94)90006-x
Bailey, R., and Pico, J. (2022). “Defence mechanisms” in StatPearls (Treasure Island, FL: StatPearls Publishing).
Bankier, B., Aigner, M., and Bach, M. (2001). Alexithymia in DSM-IV disorder: comparative evaluation of somatoform disorder, panic disorder, obsessive-compulsive disorder, and depression. Psychosomatics 42, 235–240. doi: 10.1176/appi.psy.42.3.235
Bartholomew, K. (1990). Avoidance of intimacy: an attachment perspective. J. Soc. Pers. Relationsh. 7, 147–178. doi: 10.1177/0265407590072001
Bartholomew, K., and Horowitz, L. M. (1991). Attachment styles among young adults: a test of a four-category model. J. Pers. Soc. Psychol. 61, 226–244. doi: 10.1037//0022-3514.61.2.226
Berenbaum, H., Raghavan, C., Le, H.-N., Vernon, L. L., and Gomez, J. J. (2003). A taxonomy of emotional disturbances. Clin. Psychol. Sci. Pract. 10, 206–226. doi: 10.1093/clipsy.bpg011
Barlow, D. H., Allen, L. B., and Choate, M. L. (2004). Toward a unified treatment for emotional disorders. Behav. Ther. 35, 205–230. doi: 10.1016/S0005-7894(04)80036-4
Bond, M. (1992). “An empirical study of defensive styles: the Defence style questionnaire” in Ego mechanisms of defence: a guide for clinicians and researchers. ed. G. E. Vaillant (Washington: American Psychiatric Press), 127–158.
Bond, M., and Perry, J. C. (2004). Long-term changes in defence styles with psychodynamic psychotherapy for depressive, anxiety, and personality disorders. Am. J. Psychiatry 161, 1665–1671. doi: 10.1176/appi.ajp.161.9.1665
Bond, M. P., and Vaillant, J. S. (1986). An empirical study of the relationship between diagnosis and defence style. Arch. Gen. Psychiatry 43, 285–288. doi: 10.1001/archpsyc.1986.01800030103012
Bowlby, J. (1982). Attachment and loss: retrospect and prospect. Am. J. Orthopsychiatry 52, 664–678. doi: 10.1111/j.1939-0025.1982.tb01456.x
Brennan, K. A., Clark, C. L., and Shaver, P. (1998). “Self-report measures of adult romantic attachment” in Attachment theory and close relationships. eds. J. A. Simpson and W. S. Rholes (New York: Guilford Press), 46–76.
Britton, J. C., Stewart, S. E., Killgore, W. D., Rosso, I. M., Price, L. M., Gold, A. L., et al. (2010). Amygdala activation in response to facial expressions in pediatric obsessive-compulsive disorder. Depress. Anxiety 27, 643–651. doi: 10.1002/da.20718
Brotman, M. A., Guyer, A. E., Lawson, E. S., Horsey, S. E., Rich, B. A., Dickstein, D. P., et al. (2008a). Facial emotion labeling deficits in children and adolescents at risk for bipolar disorder. Am. J. Psychiatry 165, 385–389. doi: 10.1176/appi.ajp.2007.06122050
Brotman, M. A., Skup, M., Rich, B. A., Blair, K. S., Pine, D. S., Blair, J. R., et al. (2008b). Risk for bipolar disorder is associated with face-processing deficits across emotions. J. Am. Acad. Child Adolesc. Psychiatry 47, 1455–1461. doi: 10.1097/CHI.0b013e318188832e
Cardi, V., Corfield, F., Leppanen, J., Rhind, C., Deriziotis, S., Hadjimichalis, A., et al. (2015). Emotional processing, recognition, empathy and evoked facial expression in eating disorders: an experimental study to map deficits in social cognition. PLoS One 10:e0133827. doi: 10.1371/journal.pone.0133827
Cassidy, J. (1994). Emotion regulation: influences of attachment relationships. Monogr. Soc. Res. Child Dev. 59, 228–249. doi: 10.1111/j.1540-5834.1994.tb01287.x
Cassidy, J., Stern, J. A., Mikulincer, M., Martin, D. R., and Shaver, P. R. (2018). Influences on Care for Others: Attachment Security, Personal Suffering, and Similarity Between Helper and Care Recipient. Pers Soc Psychol Bull. 44, 574–588. doi: 10.1177/0146167217746150 [Epub 2017 Dec 22].
Chan, C. C., Wong, R., Wang, K., and Lee, T. M. (2008). Emotion recognition in Chinese people with schizophrenia. Psychiatry Res. 157, 67–76. doi: 10.1016/j.psychres.2006.03.028
Ciocca, G., Rossi, R., Collazzoni, A., Gorea, F., Vallaj, B., Stratta, P., et al. (2020). The impact of attachment styles and defence mechanisms on psychological distress in a non-clinical young adult sample: a path analysis. J. Affect. Disord. 273, 384–390. doi: 10.1016/j.jad.2020.05.014
Cludius, B., Mennin, D., and Ehring, T. (2020). Emotion regulation as a transdiagnostic process. Emotion (Washington, DC), 20, 37–42.
Collin, L., Bindra, J., Raju, M., Gillberg, C., and Minnis, H. (2013). Facial emotion recognition in child psychiatry: a systematic review. Res. Dev. Disabil. 34, 1505–1520. doi: 10.1016/j.ridd.2013.01.008
Cui, F., Nan, Y., and Luo, Y. (2008). A review of cognitive neuroscience studies on empathy. Adv. Psychol. Sci. 16, 250–254.
Dapelo, M. M., Surguladze, S., Morris, R., and Tchanturia, K. (2016). Emotion recognition in blended facial expressions in women with anorexia nervosa. Eur. Eat. Disord. Rev. 24, 34–42. doi: 10.1002/erv.2403
Davis, M. H. (1983). Measuring individual differences in empathy: evidence for a multidimensional approach. J. Pers. Soc. Psychol. 44, 113–126. doi: 10.1037/0022-3514.44.1.113
de Bonis, M., De Boeck, P., Pérez-Diaz, F., and Nahas, M. (1999). A two-process theory of facial perception of emotions. C R Acad Sci III 322, 669–675. doi: 10.1016/s0764-4469(99)80106-1
Deborde, A. S., Miljkovitch, R., Roy, C., Dugré-Le Bigre, C., Pham-Scottez, A., Speranza, M., et al. (2012). Alexithymia as a mediator between attachment and the development of borderline personality disorder in adolescence. J. Personal. Disord. 26, 676–688. doi: 10.1521/pedi.2012.26.5.676
Dickstein, D. P., Rich, B. A., Roberson-Nay, R., Berghorst, L., Vinton, D., Pine, D. S., et al. (2007). Neural activation during encoding of emotional faces in pediatric bipolar disorder. Bipolar Disord. 9, 679–692. doi: 10.1111/j.1399-5618.2007.00418.x
Dinsdale, N., and Crespi, B. J. (2013). The borderline empathy paradox: evidence and conceptual models for empathic enhancements in borderline personality disorder. J. Personal. Disord. 27, 172–195. doi: 10.1521/pedi.2013.27.2.172
Doba, K., and Nandrino, J. L. (2020). Cognitive and emotional empathy in anorexia nervosa: the role of attachment insecurity, intrapersonal, and interpersonal emotional competences. J. Nerv. Ment. Dis. 208, 312–318. doi: 10.1097/NMD.0000000000001130
Domes, G., Czieschnek, D., Weidler, F., Berger, C., Fast, K., and Herpertz, S. C. (2008). Recognition of facial affect in borderline personality disorder. J. Personal. Disord. 22, 135–147. doi: 10.1521/pedi.2008.22.2.135
Domes, G., Schulze, L., and Herpertz, S. C. (2009). Emotion recognition in borderline personality disorder-a review of the literature. J. Personal. Disord. 23, 6–19. doi: 10.1521/pedi.2009.23.1.6
Drapeau, M., De Roten, Y., Perry, J. C., and Despland, J. N. (2003). A study of stability and change in defence mechanisms during a brief psychodynamic investigation. J. Nerv. Ment. Dis. 191, 496–502. doi: 10.1097/01.nmd.0000082210.76762.ec
Ekman, P., and Friesen, W.V., (1976). Pictures of facial affect. Palo Alto, CA: Consulting Psychologists Press.
England-Mason, G. (2020). Emotion regulation as a transdiagnostic feature in children with neurodevelopmental disorders. Curr. Dev. Disord. Rep. 7, 130–138. doi: 10.1007/s40474-020-00200-2
Fonagy, P., and Bateman, A. W. (2006). Mechanisms of change in mentalization-based treatment of BPD. J. Clin. Psychol. 62, 411–430. doi: 10.1002/jclp.20241
Fonagy, P., and Luyten, P. (2009). A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder. Dev. Psychopathol. 21, 1355–1381. doi: 10.1017/S0954579409990198
Fonagy, P., and Luyten, P. (2016). “A multilevel perspective on the development of borderline personality disorder” in Developmental psychopathology. Vol. 3: Risk, disorder, and adaptation. ed. D. Cicchetti . 3rd ed (New York, NY: Wiley), 727–792.
Fonagy, P., Target, M., Gergely, G., Allen, J. G., and Bateman, A. W. (2003). The developmental roots of borderline personality disorder in early attachment relationships: a theory and some evidence. Psychoanal. Inq. 23, 412–459. doi: 10.1080/07351692309349042
Giedd, J. N., Blumenthal, J., Jeffries, N. O., Castellanos, F. X., Liu, H., Zijdenbos, A., et al. (1999). Brain development during childhood and adolescence: a longitudinal MRI study. Nat. Neurosci. 2, 861–863. doi: 10.1038/13158
Graziano, P. A., and Garcia, A. (2016). Attention-deficit hyperactivity disorder and children's emotion dysregulation: a meta-analysis. Clin. Psychol. Rev. 46, 106–123. doi: 10.1016/j.cpr.2016.04.011
Green, M. F., Horan, W. P., and Lee, J. (2015). Social cognition in schizophrenia. Nat. Rev. Neurosci. 16, 620–631. doi: 10.1038/nrn4005
Guyer, A. E., McClure, E. B., Adler, A. D., Brotman, M. A., Rich, B. A., Kimes, A. S., et al. (2007). Specificity of facial expression labeling deficits in childhood psychopathology. J. Child Psychol. Psychiatry 48, 863–871. doi: 10.1111/j.1469-7610.2007.01758.x
Habel, U., Krasenbrink, I., Bowi, U., Ott, G., and Schneider, F. (2006). A special role of negative emotion in children and adolescents with schizophrenia and other psychoses. Psychiatry Res. 145, 9–19. doi: 10.1016/j.psychres.2005.11.001
Hazan, C., and Shaver, P. (1987). Romantic love conceptualized as an attachment process. J. Pers. Soc. Psychol. 52, 511–524. doi: 10.1037//0022-3514.52.3.511
Henry, J. D., Bailey, P. E., von Hippel, C., Rendell, P. G., and Lane, A. (2010). Alexithymia in schizophrenia. J. Clin. Exp. Neuropsychol. 32, 890–897. doi: 10.1080/13803391003596462
Herzberg, D. S., Hammen, C., Burge, D., Daley, S. E., Davila, J., and Lindberg, N. (1999). Attachment cognitions predict perceived and enacted social support during late adolescence. J. Adol. Res. 14, 387–404. doi: 10.1177/0743558499144001
Hildebrandt, A., Schacht, A., Sommer, W., and Wilhelm, O. (2012). Measuring the speed of recognising facially expressed emotions. Cognit. Emot. 26, 650–666. doi: 10.1080/02699931.2011.602046
Jáni, M., and Kašpárek, T. (2018). Emotion recognition and theory of mind in schizophrenia: a meta-analysis of neuroimaging studies. World J. Biol. Psychiatry 19, S86–S96. doi: 10.1080/15622975.2017.1324176
Jänsch, C., Harmer, C., and Cooper, M. J. (2009). Emotional processing in women with anorexia nervosa and in healthy volunteers. Eat. Behav. 10, 184–191. doi: 10.1016/j.eatbeh.2009.06.001
Jovev, M., Chanen, A., Green, M., Cotton, S., Proffitt, T., Coltheart, M., et al. (2011). Emotional sensitivity in youth with borderline personality pathology. Psychiatry Res. 187, 234–240. doi: 10.1016/j.psychres.2010.12.019
Kalmar, J. H., Wang, F., Chepenik, L. G., Womer, F. Y., Jones, M. M., Pittman, B., et al. (2009). Relation between amygdala structure and function in adolescents with bipolar disorder. J. Am. Acad. Child Adolesc. Psychiatry 48, 636–642. doi: 10.1097/CHI.0b013e31819f6fbc
Kerr-Gaffney, J., Harrison, A., and Tchanturia, K. (2019). Cognitive and affective empathy in eating disorders: a systematic review and meta-analysis. Front. Psych. 10:102. doi: 10.3389/fpsyt.2019.00102
Khosravi, M. (2020). Eating disorders among patients with borderline personality disorder: understanding the prevalence and psychopathology. J. Eat. Disord. 8:38. doi: 10.1186/s40337-020-00314-3
Kiliç, F., Demirdaş, A., Işık, Ü., Akkuş, M., Atay, İ. M., and Kuzugüdenlioğlu, D. (2020). Empathy, alexithymia, and theory of mind in borderline personality disorder. J. Nerv. Ment. Dis. 208, 736–741. doi: 10.1097/NMD.0000000000001196
Kinnaird, E., Stewart, C., and Tchanturia, K. (2019). Investigating alexithymia in autism: a systematic review and meta-analysis. Eur. Psychiatry 55, 80–89. doi: 10.1016/j.eurpsy.2018.09.004
Koenigsberg, H. W., Harvey, P. D., Mitropoulou, V., New, A. S., Goodman, M., Silverman, J., et al. (2001). Are the interpersonal and identity disturbances in the borderline personality disorder criteria linked to the traits of affective instability and impulsivity? J. Personal. Disord. 15, 358–370. doi: 10.1521/pedi.15.4.358.19181
Kohler, C. G., Walker, J. B., Martin, E. A., Healey, K. M., and Moberg, P. J. (2010). Facial emotion perception in schizophrenia: a meta-analytic review. Schizophr. Bull. 36, 1009–1019. doi: 10.1093/schbul/sbn192
Krohn, A. (1974). Borderline “empathy” and differentiation of object representations: a contribution to the psychology of object relations. Int. J. Psychoanal. Psychother. 32, 142–165.
Kumari, V. (2020). Emotional abuse and neglect: time to focus on prevention and mental health consequences. Br. J. Psychiatry J. Ment. Sci. 217, 597–599. doi: 10.1192/bjp.2020.154
Laplanche, J., and Pontalis, JB. (1967), Vocabulaire de la psychanalyse, Paris, Presses Universitaires de France.
Lerner, R. M., and Steinberg, L. (2004). “The scientific study of adolescent development: past, present, and future” in Handbook of adolescent psychology. eds. R. M. Lerner and L. Steinberg (New York: John Wiley & Sons), 1–12.
Levy, K. N., Meehan, K. B., Weber, M., Reynoso, J., and Clarkin, J. F. (2005). Attachment and borderline personality disorder: implications for psychotherapy. Psychopathology 38, 64–74. doi: 10.1159/000084813
Leweke, F., Leichsenring, F., Kruse, J., and Hermes, S. (2012). Is alexithymia associated with specific mental disorders. Psychopathology 45, 22–28. doi: 10.1159/000325170
Lynch, T. R., Rosenthal, M. Z., Kosson, D. S., Cheavens, J. S., Lejuez, C. W., and Blair, R. (2006). Heightened sensitivity to facial expressions of emotion in borderline personality disorder. Emotion 6, 647–655. doi: 10.1037/1528-3542.6.4.647
Main, M. (1995). “Recent studies in attachment: Overview, with selected implications for clinical work” in Attachment Theory: Social, Developmental, and Clinical Perspectives, (Hillsdale, NJ: Analytic Press), 407–474.
Martin, L., Hargitai, R., Hupuczi, E., Rózsa, S., Birkás, B., Varga, J., et al. (2019). Defence style questionnaire: factors, validity and reliability. Psychiatr. Hung. 34, 19–33.
McClure, E. B. (2000). A meta-analytic review of sex differences in facial expression processing and their development in infants, children, and adolescents. Psychol. Bull. 126, 424–453. doi: 10.1037/0033-2909.126.3.424
McMahon, K., Kim, K., Fang, C. M., Neacsiu, A. D., and Rosenthal, M. Z. (2019). Blinded by our emotions: the impact of borderline personality disorder and affect on emotion recognition sensitivity. J. Exp. Psychopathol. 10:204380871881887. doi: 10.1177/2043808718818878
Mendlewicz, L., Linkowski, P., Bazelmans, C., and Philippot, P. (2005). Decoding emotional facial expressions in depressed and anorexic patients. J. Affect. Disord. 89, 195–199. doi: 10.1016/j.jad.2005.07.010
Mennin, D., and Farach, F. (2007). Emotion and evolving treatments for adult psychopathology. Clin. Psychol. Sci. Pract. 14, 329–352. doi: 10.1111/j.1468-2850.2007.00094.x
Mikulincer, M., and Shaver, P. R. (2007). Attachment in adulthood: Structure, dynamics, and change. New York, NY: Guilford Press.
Mikulincer, M., and Shaver, P. R. (2008, 2008). “Adult attachment and affect regulation” in Handbook of attachment: Theory, research, and clinical applications. eds. J. Cassidy and P. R. Shaver. 2nd ed (New York, NY: Guilford Press), 503–531.
Mikulincer, M., and Shaver, P. R. (2019). Attachment orientations and emotion regulation. Curr. Opin. Psychol. 25, 6–10. doi: 10.1016/j.copsyc.2018.02.006
Miljkovitch, R., Deborde, A. S., Bernier, A., Corcos, M., Speranza, M., and Pham-Scottez, A. (2018). Borderline personality disorder in adolescence as a generalization of disorganized attachment. Front. Psychol. 9:1962. doi: 10.3389/fpsyg.2018.01962
Minzenberg, M. J., Poole, J. H., and Vinogradov, S. (2006). Social-emotion recognition in borderline personality disorder. Compr. Psychiatry 47, 468–474. doi: 10.1016/j.comppsych.2006.03.005
Mitchell, A. E., Dickens, G. L., and Picchioni, M. M. (2014). Facial emotion processing in borderline personality disorder: a systematic review and meta-analysis. Neuropsychol. Rev. 24, 166–184. doi: 10.1007/s11065-014-9254-9
Montebarocci, O., Codispoti, M., Baldaro, B., and Rossi, N. (2004). Adult attachment style and alexithymia. Personal. Individ. Differ. 36, 499–507. doi: 10.1016/S0191-8869(03)00110-7
Németh, N., Péterfalvi, Á., Czéh, B., Tényi, T., and Simon, M. (2020). Examining the relationship between executive functions and mentalizing abilities of patients with borderline personality disorder. Front. Psychol. 11:1583. doi: 10.3389/fpsyg.2020.01583
New, A. S., Hazlett, E. A., Buchsbaum, M. S., Goodman, M., Mitelman, S. A., Newmark, R., et al. (2007). Amygdala-prefrontal disconnection in borderline personality disorder. Neuropsychopharmacology 32, 1629–1640. doi: 10.1038/sj.npp.1301283
New, A. S., Rot, M., Ripoll, L. H., Perez-Rodriguez, M. M., Lazarus, S., Zipursky, E., et al. (2012). Empathy and alexithymia in borderline personality disorder: clinical and laboratory measures. J. Personal. Disord. 26, 660–675. doi: 10.1521/pedi.2012.26.5.660
Niedenthal, P. M., Brauer, M., Robin, L., and Innes-Ker, A. H. (2002). Adult attachment and the perception of facial expression of emotion. J. Pers. Soc. Psychol. 82, 419–433. doi: 10.1037/0022-3514.82.3.419
Norton, P. J., and Paulus, D. J. (2016). Toward a unified treatment for emotional disorders: update on the science and practice. Behav. Ther. 47, 854–868. doi: 10.1016/j.beth.2015.07.002
Norton, P. J., and Roberge, P. (2017). Transdiagnostic therapy. Psychiatr. Clin. North Am. 40, 675–687. doi: 10.1016/j.psc.2017.08.003
Paris, J., Zweig-Frank, H., Bond, M., and Guzder, J. (1996). Defence styles, hostility, and psychological risk factors in male patients with personality disorders. J. Nerv. Ment. Dis. 184, 153–158. doi: 10.1097/00005053-199603000-00003
Parker, J. D., Taylor, G. J., and Bagby, R. M. (2003). The 20-item Toronto alexithymia scale. III. Reliability and factorial validity in a community population. J. Psychosom. Res. 55, 269–275. doi: 10.1016/s0022-3999(02)00578-0
Pearl, S. B., and Norton, P. J. (2017). Transdiagnostic versus diagnosis specific cognitive behavioural therapies for anxiety: a meta-analysis. J. Anxiety Disord. 46, 11–24. doi: 10.1016/j.janxdis.2016.07.004
Perry, J. C., and Bond, M. (2012). Change in defence mechanisms during long-term dynamic psychotherapy and five-year outcome. Am. J. Psychiatry 169, 916–925. doi: 10.1176/appi.ajp.2012.11091403
Perry, J. C., and Cooper, S. H. (1986). A preliminary report on defences and conflicts associated with borderline personality disorder. J. Am. Psychoanal. Assoc. 34, 863–893. doi: 10.1177/000306518603400405
Preißler, S., Dziobek, I., Ritter, K., Heekeren, H. R., and Roepke, S. (2010). Social cognition in borderline personality disorder: evidence for disturbed recognition of the emotions, thoughts, and intentions of others. Front. Behav. Neurosci. 4:182. doi: 10.3389/fnbeh.2010.00182
Presniak, M. D., Olson, T. R., and Macgregor, M. W. (2010). The role of defence mechanisms in borderline and antisocial personalities. J. Pers. Assess. 92, 137–145. doi: 10.1080/00223890903510373
Ravitz, P., Maunder, R., Hunter, J., Sthankiya, B., and Lancee, W. (2010). Adult attachment measures: a 25 year review. J. Psychosom. Res. 69, 419–432. doi: 10.1016/j.jpsychores.2009.08.006
Renwick, B., Musiat, P., Lose, A., DeJong, H., Broadbent, H., Kenyon, M., et al. (2015). Neuro- and social-cognitive clustering highlights distinct profiles in adults with anorexia nervosa. Int. J. Eat. Disord. 48, 26–34. doi: 10.1002/eat.22366
Robin, M., Pham-Scottez, A., Curt, F., Dugre-Le Bigre, C., Speranza, M., Sapinho, D., et al. (2012). Decreased sensitivity to facial emotions in adolescents with Borderline Personality Disorder. Psychiatry Res. 200, 417–421. doi: 10.1016/j.psychres.2012.03.032
Robin, M., Douniol, M., Pham-Scottez, A., Gicquel, L., Delvenne, V., Nezelof, S., et al. (2021). J. pers. disord. 35(Supplement B), 94–110. Available at: https://doi.org/10.1521/pedi_2021_35_523
Roepke, S., Vater, A., Preißler, S., Heekeren, H. R., and Dziobek, I. (2013). Social cognition in borderline personality disorder. Front. Neurosci. 6:195. doi: 10.3389/fnins.2012.00195
Scharfe, E., and Bartholomew, K. (1994). Reliability and stability of adult attachment patterns. Pers. Relatsh. 1, 23–43. doi: 10.1111/j.1475-6811.1994.tb00053.x
Schenkel, L. S., Pavuluri, M. N., Herbener, E. S., Harral, E. M., and Sweeney, J. A. (2007). Facial emotion processing in acutely ill and euthymic patients with pediatric bipolar disorder. J. Am. Acad. Child Adolesc. Psychiatry 46, 1070–1079. doi: 10.1097/chi.0b013e3180600fd6
Sifneos, P. E. (1973). The prevalence of 'alexithymic' characteristics in psychosomatic patients. Psychother. Psychosom. 22, 255–262. doi: 10.1159/000286529
Simcock, G., McLoughlin, L. T., De Regt, T., Broadhouse, K. M., Beaudequin, D., Lagopoulos, J., et al. (2020). Associations between facial emotion recognition and mental health in early adolescence. Int. J. Environ. Res. Public Health 17:330. doi: 10.3390/ijerph17010330
Skodol, A. E., Gunderson, J. G., Pfohl, B., Widiger, T. A., Livesley, W. J., and Siever, L. J. (2002). The borderline diagnosis I: psychopathology, comorbidity, and personality structure. Biol. Psychiatry 51, 936–950. doi: 10.1016/s0006-3223(02)01324-0
Sowell, E. R., Thompson, P. M., Holmes, C. J., Jernigan, T. L., and Toga, A. W. (1999). In vivo evidence for post-adolescent brain maturation in frontal and striatal regions. Nat. Neurosci. 2, 859–861. doi: 10.1038/13154
Steiger, H., Van den Feen, J., Goldstein, C., and Leichner, P. (1989). Defence styles and parental bonding in eating-disordered women. Int. J. Eat. Disord. 8, 131–140. doi: 10.1002/1098-108X(198903)8:2<131::AID-EAT2260080202>3.0.CO;2-K
Svaldi, J., Griepenstroh, J., Tuschen-Caffier, B., and Ehring, T. (2012). Emotion regulation deficits in eating disorders: a marker of eating pathology or general psychopathology? Psychiatry Res. 197, 103–111. doi: 10.1016/j.psychres.2011.11.009
Taylor, G. J., Bagby, R. M., and Parker, J. D. (2003). The 20-Item Toronto Alexithymia Scale. IV. Reliability and factorial validity in different languages and cultures. J. Psychosom. Res. 55, 277–283. doi: 10.1016/s0022-3999(02)00601-3
Tchanturia, K., Dapelo, M. A., Harrison, A., and Hambrook, D. (2015). Why study positive emotions in the context of eating disorders? Curr. Psychiatry Rep. 17:537. doi: 10.1007/s11920-014-0537-x
Thompson, R. A. A. (2008). Emotion regulation: a theme in search of a definition. Monogr. Soc. Res. Child Dev. 59, 25–52. doi: 10.1111/j.1540-5834.1994.tb01276.x
Thompson, N. M., Uusberg, A., Gross, J. J., and Chakrabarti, B. (2019). Empathy and emotion regulation: an integrative account. Prog. Brain Res. 247, 273–304. doi: 10.1016/bs.pbr.2019.03.024
Timpano, K. R., and Port, J. H. (2021). Object attachment and emotion (Dys)regulation across development and clinical populations. Curr. Opin. Psychol. 39, 109–114. doi: 10.1016/j.copsyc.2020.08.013
Troisi, A., D'Argenio, A., Peracchio, F., and Petti, P. (2001). Insecure attachment and alexithymia in young men with mood symptoms. J. Nerv. Ment. Dis. 189, 311–316. doi: 10.1097/00005053-200105000-00007
Tseng, H. H., Huang, Y. L., Chen, J. T., Liang, K. Y., Lin, C. C., and Chen, S. H. (2017). Facial and prosodic emotion recognition in social anxiety disorder. Cogn. Neuropsychiatry 22, 331–345. doi: 10.1080/13546805.2017.1330190
Van Heel, M., Luyten, P., De Meulemeester, C., Vanwalleghem, D., Vermote, R., and Lowyck, B. (2019). Mentalizing based on external features in borderline personality disorder compared with healthy controls: the role of attachment dimensions and childhood trauma. J. Personal. Disord. 33, 736–750. doi: 10.1521/pedi_2019_33_373
Wearden, A. J., Lamberton, N., Crook, N., and Walsh, V. (2005). Adult attachment, alexithymia, and symptom reporting: an extension to the four category model of attachment. J. Psychosom. Res. 58, 279–288. doi: 10.1016/j.jpsychores.2004.09.010
Wongpakaran, N., DeMaranville, J., and Wongpakaran, T. (2021). Validation of the relationships questionnaire (RQ) against the experience of close relationship-revised questionnaire in a clinical psychiatric sample. Healthcare 9:1174. doi: 10.3390/healthcare9091174
Keywords: emotion regulation, attachment, adolescents, empathy, facial affect recognition, alexithymia, defense mechanisms
Citation: Robin M, Surjous L, Belbèze J, Bonnardel L, Lamas C, Silva J, Peres V and Corcos M (2023) Four attachment-based categories of emotion regulation in adolescent psychic troubles. Front. Psychol. 14:1133980. doi: 10.3389/fpsyg.2023.1133980
Edited by:
Inmaculada Méndez, University of Murcia, SpainReviewed by:
Wenhai Zhang, Hengyang Normal University, ChinaRute Brites, Autonomous University of Lisbon, Portugal
Copyright © 2023 Robin, Surjous, Belbèze, Bonnardel, Lamas, Silva, Peres and Corcos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marion Robin, bWFyaW9uLnJvYmluQGltbS5mcg==