 Derek Farrell1,2*
Derek Farrell1,2* Johnny Moran1Zeynep Zat1
Johnny Moran1Zeynep Zat1 Paul W. Miller3
Paul W. Miller3 Lorraine Knibbs1
Lorraine Knibbs1 Penny Papanikolopoulos1Tessa Prattos1
Penny Papanikolopoulos1Tessa Prattos1 Iain McGowan2Derek McLaughlin2Ian Barron4
Iain McGowan2Derek McLaughlin2Ian Barron4 Cordula Mattheß1
Cordula Mattheß1 Matthew D. Kiernan5
Matthew D. Kiernan5- 1Department for Violence Prevention, Trauma and Criminology (VPTC), School of Psychology, University of Worcester, Worcester, United Kingdom
- 2School of Nursing and Midwifery, Queen’s University, Belfast, Northern Ireland, United Kingdom
- 3School of Nursing, Magee Campus, Ulster University, Northern Ireland, United Kingdom
- 4Centre for International Education, College of Education, University of Massachusetts, Amherst, MA, United States
- 5Northern Hub for Veteran and Military Families’ Research, Northumbria University, Newcastle upon Tyne, United Kingdom
Objective: Frontline mental health, emergency, law enforcement, and social workers have faced unprecedented psychological distress in responding to the COVID-19 pandemic. The purpose of the RCT (Randomized Controls Trial) study was to investigate the effectiveness of a Group EMDR (Eye Movement Desensitization and Reprocessing) therapy (Group Traumatic Episode Protocol—GTEP) in the treatment of Post-Traumatic Stress Disorder (PTSD) and Moral Injury. The treatment focus is an early intervention, group trauma treatment, delivered remotely as video-conference psychotherapy (VCP). This early intervention used an intensive treatment delivery of 4x2h sessions over 1-week. Additionally, the group EMDR intervention utilized therapist rotation in treatment delivery.
Methods: The study’s design comprised a delayed (1-month) treatment intervention (control) versus an active group. Measurements included the International Trauma Questionnaire (ITQ), Generalized Anxiety Disorder Assessment (GAD-7), Patient Health Questionnaire (PHQ-9), Moral Injury Events Scale (MIES), and a Quality-of-Life psychometric (EQ-5D), tested at T0, T1: pre—treatment, T2: post-treatment, T3: 1-month follow-up (FU), T4: 3-month FU, and T5: 6-month FU. The Adverse Childhood Experiences – International version (ACEs), Benevolent Childhood Experience (BCEs) was ascertained at pre-treatment only. N = 85 completed the study.
Results: Results highlight a significant treatment effect within both active and control groups. Post Hoc comparisons of the ITQ demonstrated a significant difference between T1 pre (mean 36.8, SD 14.8) and T2 post (21.2, 15.1) (t11.58) = 15.68, p < 0.001). Further changes were also seen related to co-morbid factors. Post Hoc comparisons of the GAD-7 demonstrated significant difference between T1 pre (11.2, 4.91) and T2 post (6.49, 4.73) (t = 6.22) = 4.41, p < 0.001; with significant difference also with the PHQ-9 between T1 pre (11.7, 5.68) and T2 post (6.64, 5.79) (t = 6.30) = 3.95, p < 0.001, d = 0.71. The treatment effect occurred irrespective of either ACEs/BCEs during childhood. However, regarding Moral Injury, the MIES demonstrated no treatment effect between T1 pre and T5 6-month FU. The study’s findings discuss the impact of Group EMDR therapy delivered remotely as video-conference psychotherapy (VCP) and the benefits of including a therapist/rotation model as a means of treatment delivery. However, despite promising results suggesting a large treatment effect in the treatment of trauma and adverse memories, including co-morbid symptoms, research results yielded no treatment effect in frontline/emergency workers in addressing moral injury related to the COVID-19 pandemic.
Conclusion: The NICE (2018) guidance on PTSD highlighted the paucity of EMDR therapy research used as an early intervention. The primary rationale for this study was to address this critical issue. In summary, treatment results for group EMDR, delivered virtually, intensively, using therapist rotation are tentatively promising, however, the moral dimensions of trauma need consideration for future research, intervention development, and potential for further scalability. The data contributes to the emerging literature on early trauma interventions.
Clinical Trial Registration:Clinicaltrials.gov, ISRCTN16933691.
Introduction
Frontline mental health, emergency, law enforcement, and social workers have faced unprecedented psychological distress in responding to the COVID-19 pandemic, with around 22% meeting the criteria for Post-Traumatic Stress Disorder [PTSD]–a mental health condition caused by a traumatic experience (Wild et al., 2016, 2022; Johnson et al., 2020; Greene et al., 2021; Nagarajan et al., 2022; Watson, 2022; Yunitri et al., 2022). Continued psychological distress potentially may result in adverse outcomes including substance misuse, suicide risk, burnout, compassion fatigue, and secondary traumatization (Arpacioglu et al., 2021; Hooper et al., 2021). Although the impact of psychological harm may have delayed onset, implementing effective early intervention measures that seek to mitigate the potential development of PTSD is essential (Haugen et al., 2012; Hooper et al., 2021; Brunet et al., 2022). Early intervention in the aftermath of psychological trauma is defined as a treatment administered at the earliest possible time, sometimes within hours of the traumatic event, but is considered any intervention within the first 3 months after exposure (Dyregrov and Regel, 2012) consider four important principles related to early trauma interventions: immediacy, proximity, expectancy, and flexibility. Acknowledging the COVID-19 pandemic has sharply increased the demand on frontline emergency workers; nonetheless, organizations require evidence-based information about available psychological programs to address the mental health needs of staff (Jecker et al., 2020; Rasheed et al., 2020; Sritharan et al., 2020; Beames et al., 2021; Billings et al., 2021; Do and Frank, 2021; Norman et al., 2021; Carmassi et al., 2022; Feingold et al., 2022; Ghahramani et al., 2022; Smith et al., 2022). COVID-19 risk factors on mental health depend on the individual and the context. These included the risk heightened stress and anxiety, limited resources and protection, exposure to the virus and fear of exposing family, partners, and relatives, long shift patterns, sleep disruption and deprivation, burnout, and broader impact on work/life balance (Johnson et al., 2020; Raudenská et al., 2020; Sasangohar et al., 2020; Shreffler et al., 2020; de Kock et al., 2021; Lasalvia et al., 2021). Additionally, pre-existing anxiety/depression, exposure to previous adverse life experiences, and dissociative symptoms may contribute to PTSD in frontline health and emergency workers (Greenberg et al., 2020; Williamson et al., 2020; Billings et al., 2021; Greene et al., 2021; Miguel-Puga et al., 2021).
Ruck et al. (2013) stipulate that early trauma interventions are designed to neither prevent, nor treat, PTSD. Early organization interventions are useful in facilitating mutual support, identifying those that may require additional assistance, improving social cohesion, reducing harmful responses, and improving occupational functioning (Creamer et al., 2012; Dyregrov and Regel, 2012; Richins et al., 2020). Bryant (2021, 2022) and Magruder et al. (2017) consider that despite the continued debate surrounding the optimal strategies used in the immediate period following trauma exposure, the specific objective should always be preventing the onset of PTSD and other co-morbidities.
The dynamic nature of PTSD in the immediate aftermath of trauma presents both opportunities and challenges concerning early trauma interventions (Price et al., 2018). Furthermore, the malleability of symptoms post-adversity exposure suggests that early interventions can alter the course of trauma sequelae, provided those interventions are both flexible and adaptive (Asmussen et al., 2019; Roberts et al., 2019; Hooper et al., 2021; Bryant, 2022). Therefore, the primary endeavor of any early trauma intervention response should be:
1. Reduce trauma stress reactions.
2. Provide authentic support.
3. Enhance coping.
4. Empower resilience.
5. Minimize the risk of burnout and vicarious traumatization.
6. Diminish the risk of developing other mental health and psychological difficulties with the potential to impact psychological well-being.
Roberts et al. (2019) published a systematic review of 61 studies of early psychological interventions. Their review supported trauma-focused cognitive behavioral therapy (CBT-TF), cognitive therapy without exposure, and eye movement desensitization and reprocessing (EMDR) for individuals reporting traumatic stress symptoms. They concluded that the research was more robust for CBT-TF. However, NICE guidance on PTSD (2018) highlights the lack of research supporting using EMDR as an early trauma intervention.
EMDR therapy is an empirically supported treatment for psychological trauma, endorsed by the World Health Organisation (2013), United Nations High Commission for Refugees (2022) and the International Society for Traumatic Stress Studies (2019). It is a psychological treatment for pathogenic (trauma) memories and their associated stress symptoms using a model of pathogenesis and change known as adaptive information processing (Hase et al., 2017; Hase, 2021; Farrell et al., 2022; Laliotis and Shapiro, 2022; Wippich et al., 2023). Shapiro (2017) considers EMDR to desensitize disturbing memories and stimulates the reprocessing of associated thoughts, feelings, and sensations towards adaptive resolution. Although a recent systematic review concluded EMDR is effective for first responders, they concurred with NICE (2018) in further indicating the quality of studies as weak or medium, highlighting several gaps and unanswered questions within the academic literature including high risk of bias, limited availability of data including safety and harm-related information (Oosterbaan et al., 2019; Bryant, 2021, 2022; Kaptan et al., 2021; Morris et al., 2022).
A humanitarian crisis emerges when an event threatens a population’s health, safety, and well-being. COVID-19 creates a familiar narrative frequently witnessed in humanitarian emergencies where demand for mental health provision outstrips the supply available (Carriere, 2014; Dunkley, 2018; Eichfeld et al., 2019; Mattheß et al., 2019, 2020; Farrell et al., 2020; Pupat et al., 2022). As Bryant (2022) highlighted earlier, interventions need adaptation to meet the needs of as many as possible. One such adaptation within EMDR therapy is Group Interventions. Kaptan et al. (2021) undertook a review of 22 studies using Group EMDR Interventions of which 13 studies examined the EMDR Integrative Group Treatment Protocol (IGTP), four studies the EMDR Group Traumatic Episode Protocol (G-TEP), four studies of EMDR Integrative Group Treatment Protocol for Ongoing Traumatic Stress and one study considered the EMDR Group Protocol with Children. Results suggested that Group EMDR protocols might effectively improve a wide range of mental health-related outcomes, including post-traumatic stress disorder (PTSD), depression and anxiety, compared with pre-treatment and control groups. However, Kaptan et al. (2021) concluded that the included studies are limited to methodological challenges with a high risk of bias.
The Group Trauma Episode Protocol [GTEP], developed by Shapiro and Laub (2008), is an evidence-based EMDR intervention used in the treatment of recent natural and human disasters (Acarturk et al., 2016; Roberts, 2018; Womersley and Arikut-Treece, 2019; Kaptan et al., 2021; Pink et al., 2022). An essential aspect of GTEP is that the client does not disclose any details regarding their trauma experiences. Within EMDR therapy this is known as ‘Blind 2 therapist (Farrell et al., 2020, 2022). There are distinct advantages to this. The rationale surrounding non-disclosure may potentially involve trauma memories that invoke shame, survivor guilt, moral injury, or fear of recrimination and stigma. Dimensions surrounding moral injury are pertinent as these either relates to inner core values, or external such as betrayal or breaches of trust.
For frontline and emergency workers, stigma remains a substantial barrier to seeking psychological support (Clement et al., 2015; Gronholm et al., 2021). Diop et al. (2022), in a study investigating 723 frontline workers, determined that 44% expressed concerns about being stigmatized and excluded from serving those affected by COVID-19, highlighting that stigma can be both internal and external. A study carried out in India with frontline healthcare workers in direct management of COVID-19 patients (Sachdeva et al., 2021) declared that 75% experienced self-stigma – primarily in the form of guilt in potentially exposing their families to the coronavirus.
In addition to Acute Stress Disorder [ASD] (Brunet et al., 2022) and PTSD, another critical issue to return to, is moral injury. In reviewing the academic literature outlined in Figure 1, moral injury results from an act, or failure to act, that creates an ethical transgression, either by self or witnessed, which damages one’s conscience or moral compass (Litz et al., 2009) refers to the impact of moral injury as emotional, psychological, social, behavioral, and spiritual. However, there is insufficient explanation of moral injury within the current understanding of PTSD and its subsequent treatment (Barnes et al., 2019; Griffin et al., 2019; Koenig et al., 2019, 2020). Treating core PTSD symptoms does not address moral trauma—the same is true vice-versa (Farnsworth, 2019; Borges et al., 2020). A further definition of moral injury provided by Brock and Lettini (2012) describes it as a ‘wound of the soul’ when existing core moral foundations cannot be justified, sufficiently processed, and integrated into a reliable identity and meaning system sustains relationships and human flourishing. A study carried out with military mental health nurses by Jamieson et al. (2020a,b) relates moral injury to frontline workers. They describe it as experiencing existential, psychological, social, emotional, and spiritual/religious damage arising from a violation or betrayal (by omission or commission) of the core moral framework and manifesting through feelings of shame, guilt, stigma, and self-condemning, or self-sabotaging behaviors. The core aspects of moral injury pertaining to the COVID-19 pandemic are highlighted in Figure 1 (Koenig et al., 2019; Borges et al., 2020; Williamson et al., 2020; Amsalem et al., 2021; Cartolovni et al., 2021).
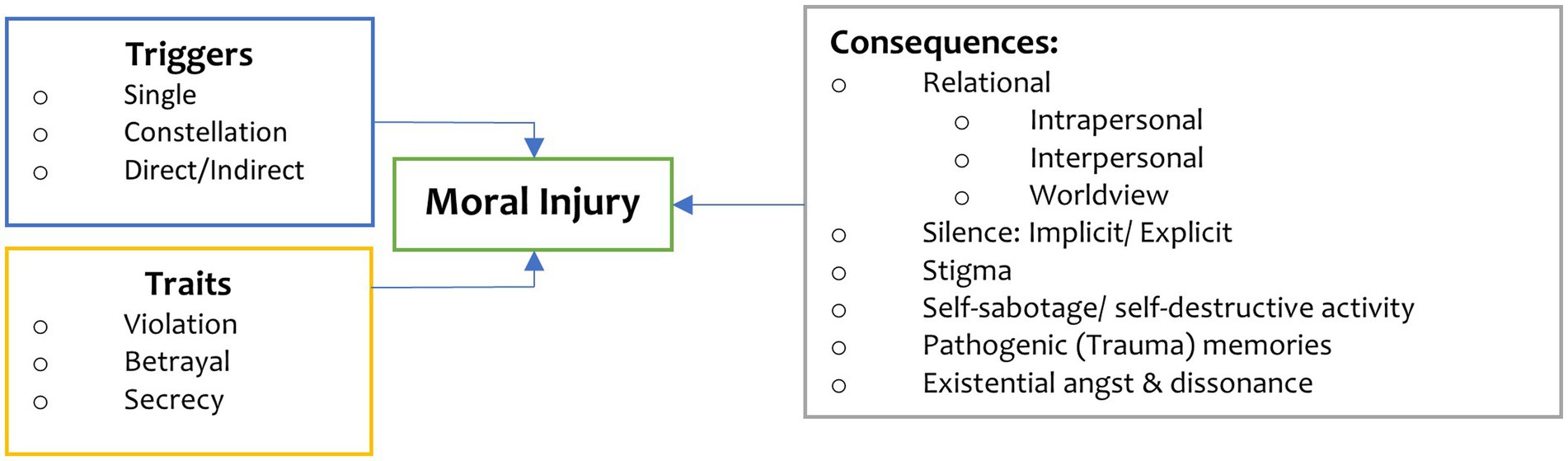
Figure 1. Key aspects of moral injury and COVID-19.
Implementing an early trauma intervention during COVID-19, and in government-enforced lockdown, presented several logistical challenges. Firstly, the public health management of COVID-19 involved social distancing to reduce risk of infection. One of the management strategies utilized to address this required a shift towards video-conferencing psychotherapy [VCP] (Crowe et al., 2020). As Healthcare providers closed their doors to face-to-face intervention, video-conferencing treatment platforms became, for many, the only viable option (Turgoose et al., 2018; Watts et al., 2020; Wind et al., 2020; Farrell et al., 2022). To date, several research studies indicate that psychological treatment, delivered remotely though video-conference platforms, are both safe and feasible. Furthermore, that they offer greater flexibility, and improve equity of access (Appleton et al., 2021; Broadbear et al., 2021; Cantone et al., 2021; Cataldo et al., 2021; Dharwadkar et al., 2021; Oudshoorn et al., 2021; Puspitasari et al., 2021; Shklarski et al., 2021a,b; Vera San Juan et al., 2021; Milosevic et al., 2022). Smith et al. (2022), however, considers that although the evidence-base is promising further interrogation and research is needed to further explore the ethical and moral dimensions of video-conference psychotherapy.
According to Herman and Kallivayalil (2018), outcome research supports group interventions in the treatment of PTSD; however, they conclude that there is limited evidence to support the superiority of one group model over another. The research evidence exploring group trauma treatment for PTSD using VCP is limited, especially regarding COVID-19. One group trauma treatment approach is Eye Movement Desensitization and Reprocessing (EMDR). Most current research demonstrates its effectiveness with Post-Traumatic Stress Disorder [PTSD] and Complex PTSD. However, EMDR therapy has been used extensively as an early intervention as part of trauma capacity building throughout the world (Farrell et al., 2011, 2013, 2020; Eichfeld et al., 2019; Mattheß et al., 2019, 2020; Covers et al., 2021; Tarquinio et al., 2021). Table 1 highlights the advantages and disadvantages of using EMDR therapy as an early intervention using virtual platforms.
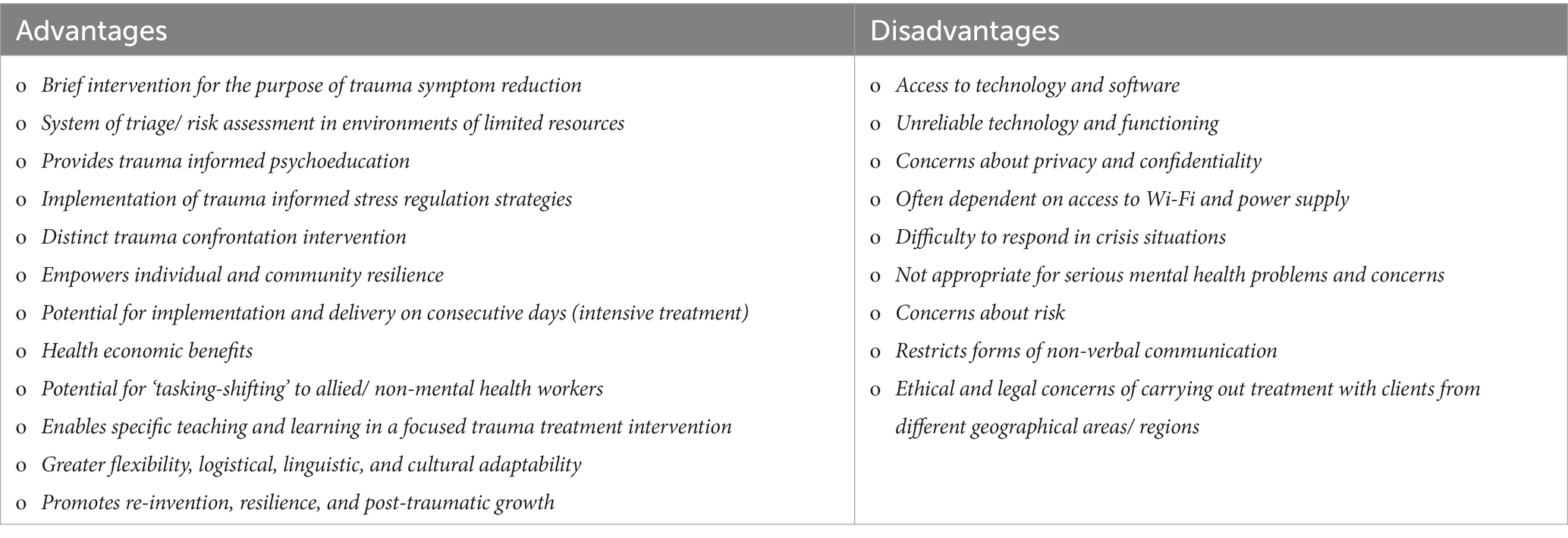
Table 1. Advantages and disadvantages of early intervention EMDR therapy using visual platforms.
Replicating an innovative approach used in the treatment of PTSD (van Minnen et al., 2018) utilized therapist rotation in delivering the treatment intervention. In this contemporary approach Trauma Therapists rotate between patients during the treatment intervention. As Table 2 accentuates, there are several distinct advantages and disadvantages to using therapist rotation (Krampe and Ehrenreich, 2012; van Minnen et al., 2018):
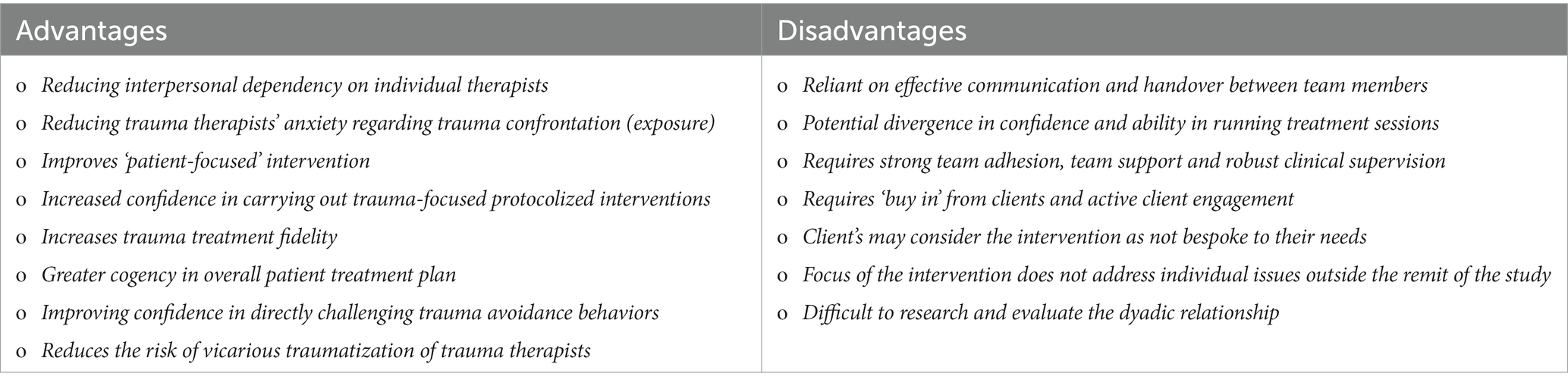
Table 2. Advantages and disadvantages of therapist rotation model in EMDR therapy.
As Kaptan et al. (2021) emphasized, more trauma-focused clinical trials, especially early intervention, incorporating robust methodology, larger sample sizes with participants who meet clear diagnostic criteria and including necessary follow-up data is essential. Addressing these salient issues was the primary driver in the inception of this COVID-19 randomized-control clinical trial. Mindful of the issues raised so far, this clinical trial wished to explore the following: early trauma intervention, use of video-conference psychotherapy, group treatment, Blind-2-therapist, intensive treatment, and therapist rotation – with a primary treatment target group Emergency Workers on the frontline of the COVID-19 pandemic who demonstrated trauma sequelae.
The broad research objectives for the study were:
1. Is Early Intervention EMDR Video Group Therapy (VGTEP) a safe, and efficient treatment intervention for Frontline/Emergency/Keyworkers, who experience psychological trauma in response to COVID-19 with regards to trauma sequalae and co-morbid symptoms.
2. Is Early Intervention EMDR Video Group Therapy (VGTEP) a relevant and effective treatment intervention for Frontline/Emergency/Keyworkers, who experience psychological trauma in response to COVID-19 with regards to both recruitment and retention to the study?
Materials and methods
Design
The University of Worcester (United Kingdom) granted ethical approval for the study [CBPS19200030]. The research study strictly adhered to the approval granted. Additionally, the study adhered to the British Psychological Society (BPS) Guidelines on ‘Conducting Research with Human Participants during COVID-19 (2020). The study registered as a clinical trial ID ISRCTN16933691 (2020) and hosted by the Trauma Response Network (TRN) – Ireland, an NGO organization offering early trauma interventions. Research participants recruited via a social networking and advertising strategy coordinated by TRN Ireland, which involved media outlets and radio stations in Ireland, Northern Ireland, and Great Britain. Interest in participation into the study was such that recruitment, although from the Island of Ireland, also included international participants from United States, Canada, Australia, New Zealand, Greece, and Turkey. The treatment intervention used for the clinical trial was the EMDR Group Traumatic Episode Protocol – version 9 (Shapiro, 2019–unpublished) used as a video-conference psychotherapy (VGTEP).
A Randomized Control Trial (RCT) Delayed Start Design used for the clinical study compared an active treatment intervention versus a control group (delayed treatment – 1 month) using the same intervention. The clinical trial conducted from July 2020 – March 2022 during the primary lockdown periods. The RCT consisted of two cohorts:
o Active Cohort 1: EMDR therapy VGTEP Treatment (4 sessions of approximately 2 h duration which equated to 8 h total treatment intervention) implemented as an intensive intervention for 1 week.
o Control Cohort 2: 4 weeks Delayed intervention of EMDR therapy VGTEP. Treatment involved an intensive intervention within 1 week.
The study incorporated six data points including T0 (control group), T1 (pre), T2 (post), T3 (1-month FU), T4 (3-month FU), and T5 (6-month FU) (Marcus et al., 2004; Ostacoli et al., 2018). All included research clients provided written consent before enrolment into the clinical trial.
The RCT generates six hypotheses to determine that the Virtual EMDR Group Intervention was safe, relevant, effective, and efficient:
Hypothesis 1: There is no difference between active and control (delayed) groups regarding trauma sequelae—measured with the International Trauma Questionnaire (ITQ) (Cloitre et al., 2018) when comparing T1, T2, T3, T4, and T5.
Hypothesis 2: There is no difference between active and control (delayed) groups regarding co-morbid sequelae – measured with the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001) and the Generalized Anxiety Disorder (GAD-7) (Williams, 2014) over the T1-T5 time periods.
Hypothesis 3: Treating the trauma sequelae will reduce the level of moral injury as demonstrated with the Moral Injury Events Scale (MIES) ((Nash et al., 2013), demonstrated between T1 and T5, for both active and control groups.
Hypothesis 4: Using Trauma-Focused Therapist rotation will demonstrate no change in clinical diagnosis between T1 and T5, for both active and control groups.
Hypothesis 5: A negative correlation exists, within the target population, between Adverse Childhood Experiences (ACEs) and Benevolent Childhood Experiences (BCEs) (Narayan et al., 2018) regarding evidence supporting resilience and posttraumatic growth.
Hypothesis 6: There is no difference between active and control groups regarding quality of life using the EQ-5D – generic measure of an individual’s health status when comparing between T1 and T5.
Participants
The clients used for this clinical trial were Frontline Health and Social Care workers or Emergency/First Responders directly working on the frontline of the COVID-19 pandemic utilizing the following inclusion/exclusion criteria:
Inclusion criteria:
o Adults (18 years and above).
o Front Line Health, Emergency and Social Care Workers experiencing Psychological Distress and Trauma in response to frontline working addressing the COVID-19 virus.
o Currently in active employment.
o Symptoms indicative of psychological distress and impact of psychological well-being and functioning measured using the Impact of Events Scale Revised Score of 24 and above.
Exclusion criteria:
o Non-trauma exposure.
o Impact of Events Scale Revised score of 23 or below.
o Undergoing current treatment (physical and/or psychological).
o Present evidence of psychosis.
As mentioned earlier as this was a Republic of Ireland Research initiative, research participants were recruited either from the Island of Ireland or internationally. A recruitment initiative was carried out utilizing media organizations within the Republic of Ireland. Recruitment to participate in the clinical trial used self-selection access through the Trauma Response Network (TRN) Ireland website through a secure platform. Each participant was also assessed by TRN Ireland administrative staff, who provided further information about the study outlining what participation involved. Those wishing to participate were provided with a detailed, research participant information sheet and research consent form.
The Impact of Events Scale–Revised (IES-R; Weiss and Marmar, 1997) was the primary screening tool used for the purpose of recruitment only. The IES-R has been tested for factor structure, internal consistency, concurrent validity, and discriminative validity by Beck et al. (2008). An IES-R score of 24 was used as the threshold for entering the study. The IES-R is an internationally recognized psychometric tool to assist in a diagnosis of Post-Traumatic Stress Disorder. The IES-R consists of 22 questions and provides four scores: total, intrusion, avoidance, and hyperarousal. The scoring is a maximum of 88. Asukai et al. (2002) stipulate that an IES-R score of 24–32 indicates clinical concern of either partial PTSD or at least some of its symptoms. Additionally (Creamer et al., 2003) advises that scores between 33 and 38 represent a cut-off score for a probable diagnosis of PTSD. A score of 39 and above is enough to suppress the immune system’s functioning (Izutsu et al., 2004, 2008).
Mirabilis Health Institute, Belfast, Northern Ireland, provided medical supervision for the clinical trial and was responsible for clinical risk assessment and triage.
In determining the sample size1 was used setting α = 0.05, β = 0.2. A power calculation indicated an initial sample size estimation of N = 72 with N = 36 in each arm of the study. This figure allowed for a 10% drop-out rate. Randomization done through sequence generation using a computer algorithm allocating each research participant a unique client number (UCN) to ensure anonymity to the clinical team. Figure 2 highlights N = 192 clients assessed for eligibility and N = 97 individuals excluded from the study as their IES-R scores were < 24, leaving a total of N = 95 subject to randomization.
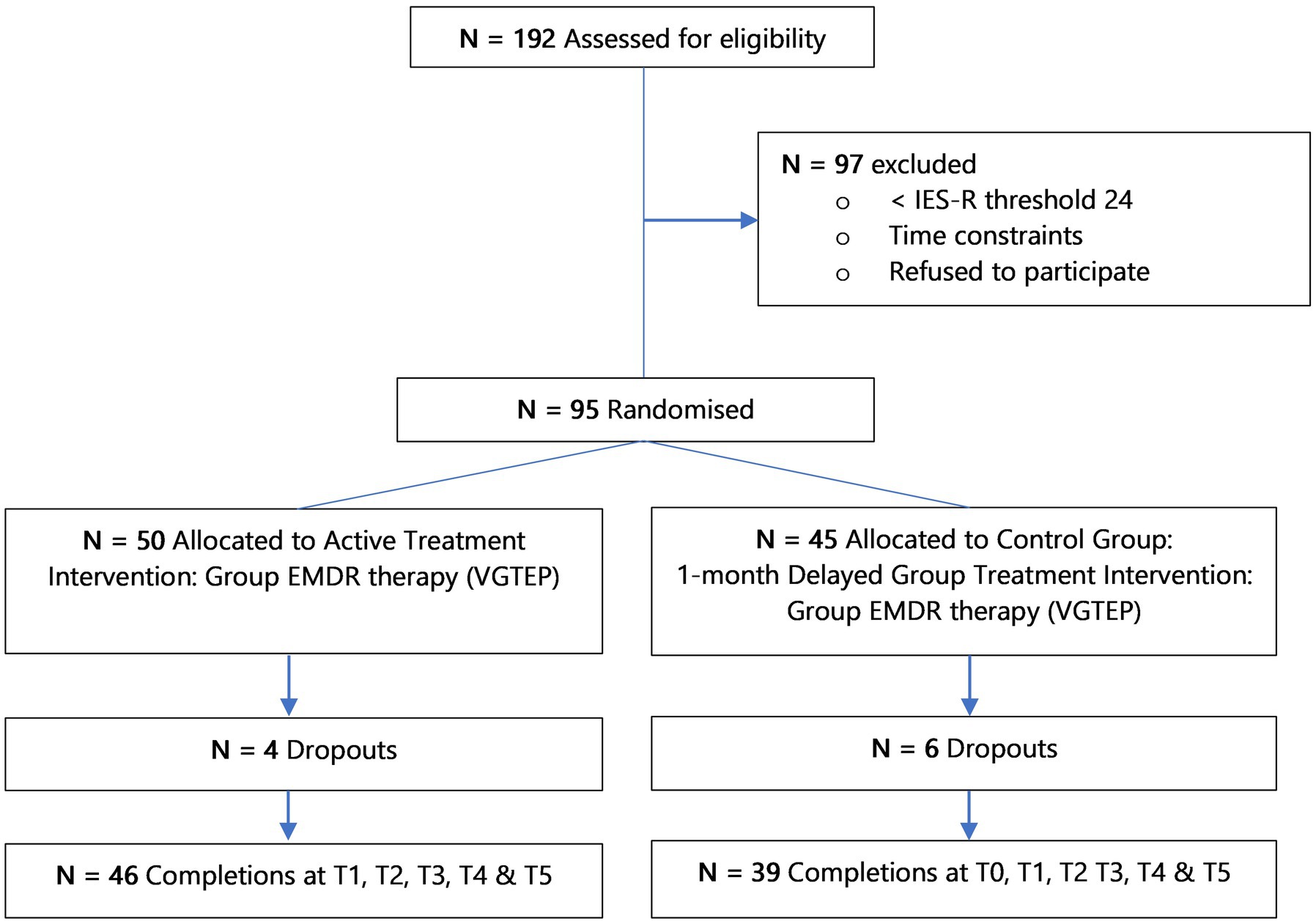
Figure 2. Flow of participants through the research clinical trial.
Measures
The clinical trial used the following measures:
o International Trauma Questionnaire (ITQ) – an 18 question, self-reporting measure focused on both PTSD and Complex PTSD, consistent with ICD-11 (Hyland et al., 2017; Cloitre et al., 2018; Redican et al., 2021).
o Generalized Anxiety Disorder Assessment (GAD-7) which objectifies and assesses the degree of anxiety severity (Williams, 2014).
o Patient Health Questionnaire (PHQ-9) which objectifies and assesses the degree of depression severity (Kroenke et al., 2001).
o Subjective Unit of Disturbance/Distress (SUD) – a scale of 0 to 10, measuring the subjective intensity of disturbance or distress currently experienced by an individual (Wolpe, 1969).
o Moral Injury Event Scale (MIES) – 9-point self-reporting scale exploring perceived transgressions, betrayals, or violations of an individual’s moral code (Nash et al., 2013).
o Adverse Childhood Experience International Questionnaire (ACE-IQ) – tested at Pre point only with the intention to measure exposure to adverse childhood experiences (< 18 years old).
o Benevolent Childhood Experiences Score (BCEs) (Narayan et al., 2017) – tested at Pre point only: this is a measure of exposure to benevolent factors that occurred in childhood that may impact on resilience and post-traumatic growth (< 18 years old).
o EQ-5D – generic measure of an individual’s health status. The EQ-5D is a preference based HRQL across five dimensions; mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.
Measure evaluated after each VGTEP session: SUD.
Measures evaluated at T1 only: ACE-IQ and BCEs.
Measures evaluated at T0, T1, T2, T3, T4, and T5: ITQ, GAD-7, PHQ-9, EQ-5D.
Measures evaluated at T1 and T5 only: MIES.
All psychometrics were sent out electronically to all research participants via the Trauma Response Network Ireland Administrators and was collected independent to the research team.
Treatment intervention
Once research participants met the study’s inclusion criteria the TRN administrative team randomly assigned participants using a random allocation software package to either the active group Immediate Treatment Group) or a 1-month Delayed Treatment Group. Each group intervention involved a 1-week block of intensive treatment consisting of four, two hours sessions of Group EMDR therapy, delivered as a remote treatment intervention. The platform used for the VGTEP sessions was ZOOM Enterprise version 5.9.1. The TRN Ireland administrative team emailed a ZOOM link for each of the treatment sessions – evenings of Monday, Wednesday, and Thursday, and Saturday morning. At the commencement of each treatment session research participants were instructed to only use the unique client number as a means of identification, and not their name. Clinical members of the research teams had no means of identifying any of the research participants. Participants were required to attend all four treatment sessions. Each session lasted approximately 2 h. Each group consisted of six participants who remained as a group for the duration of the treatment intervention. In addition, the VGTEP session lead, and the emotional protection worker (EPW), were also randomly allocated to the treatment sessions. As per the research protocol, session leads and EPWs introduced themselves at the start of each VGTEP treatment session, and importantly, however, the research participants revealed no information about themselves. Additionally, it was emphasized to the research participants that the VGTEP intervention required no disclosure of anything about the trauma memory – consistent with the EMDR Blind 2 therapist protocol. Clinical Leads and Emotional Protection workers were also randomly allocated to the VGTEP treatment intervention ensuring therapist rotation by the TRN Administrative team.
The EMDR Group Treatment Intervention delivered as video-conference psychotherapy (VGTEP) consisted of seven steps: 1. Trauma regulation exercise, 2. Trauma target selection, 3. Anchor to a past resource, 4. Identification of a future belief, 5. Trauma confrontation of the target trauma memory, 6. Enhancement of resilience and post-trauma growth, and 7. Closure grounding exercise. Dual attention, and bilateral stimulation, a distinct element of EMDR therapy, are used in steps 2 and 5. Step 5 addresses three of the significant points of disturbance relating to the target trauma memory. Trauma processing within the confrontation stage of VGTEP involves 27 occasions of focus on the trauma target material.
Each VGTEP session was digitally recorded and subjected to treatment fidelity checks carried out by an independent EMDR Europe Accredited Consultant/Clinical Supervisor. When necessary, the Emotional Protection worker utilized the breakout room within ZOOM to manage any participant if they needed I:I support or guidance. Before the commencement of the trial, training was provided for both the VGTEP clinical leads and Emotional Protection workers, this ensured familiarity with the clinical trial, treatment fidelity, triage and risk assessment procedures, welfare checks, team support, and clinical and research supervision. Mirabilis Health Institute, Belfast, Northern Ireland, provided onward referral and Consultant Medical Supervision for the clinical trial.
Regarding treatment fidelity and integrity a treatment protocol manual was created for the clinical trial, based on the Elan Shapiro GTEP Training Manual – version 9 (unpublished manual). Each treatment session was video recorded and was independently fidelity checked by an international expert in the Group Traumatic Episode Protocol (GTEP). Additionally, all psychometrics were acquired independently to the research team, with the entire data set only handed over to the team for data analysis once all the 6-month follow-up data had been obtained.
Data analysis
Data Analysis used the Jamovi (version 2.3.21.0) statistical software package. Descriptive data analyzed used either independent sample t-tests or fischer exact test. For further descriptive statistics, mean ±, standard deviation (±SD) for numerical variables and percentage (%) for categorical data. Tests for normality and homogeneity of variance determined no violations, therefore repeated measures RM-ANOVA analyzed each variable at T0, T1, T2, T3, T4, and T5 time points. The rationale for utilizing RM-ANOVAS is that they have been frequently used in various RCT studies testing EMDR therapy (de Roos et al., 2011; Jarero et al., 2018; Osorio, 2018; Ostacoli et al., 2018; Yurtsever et al., 2018). Skewness and kurtosis ensured normality of the ACEs and BCEs scores, as well as Pearson r to determine correlation coefficients. The p value of <0.05 considered significant. Using RM-ANOVA models Eta squared η2 is used as an indication of effect size (Olejnik and Algina, 2003).
Results
Within the research trial, 64 VGTEP treatment sessions were carried out during two periods of government lockdown during the COVID-19 pandemic. This equated to approximately 128 h of treatment intervention, including both active (N = 46) and control (N = 39) groups. Per the therapist rotation model, N = 11 EMDR therapists carried out the 64 treatment interventions, and N = 26 Emotional Protection Team members were utilized. VGTEP Therapists, Emotional Protection Workers, and research participants were blinded in the intervention.
Metric points conducted at T0 (control), and then T1 (pre-treatment), T2 (post—treatment), T3 (1-mth FU), T4 (3-mth FU), and T5 (6-mth FU). Table 3 highlights N = 85 completed the study up to, and including, T5.
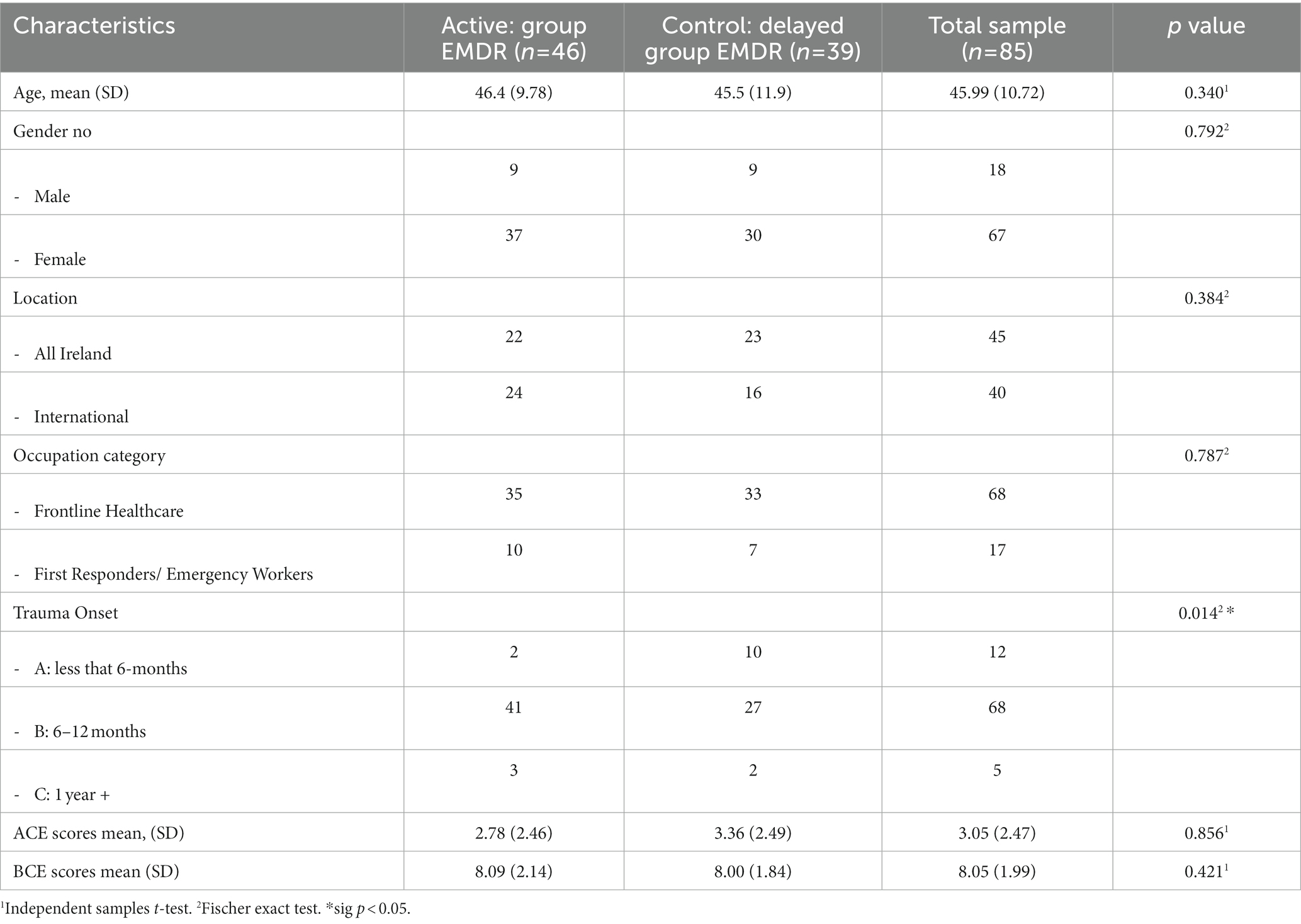
Table 3. Descriptive data.
In testing Hypothesis 1: There is no difference between active and control (delayed) groups regarding trauma sequelae—measured with the International Trauma Questionnaire (ITQ) when comparing T1, T2, T3, T4, and T5. As mentioned earlier results revealed no statistical change between T0 and T1 for the control group, therefore, Figure 3 highlights the descriptive results for the complete cohort N = 85 for periods T1, T2, T3, T4, and T5. A repeated measures RM-ANOVA conducted to compare the impact of the Virtual GTEP intervention on trauma symptoms using the International Trauma Questionnaire (ITQ) evaluated at T0 (control group), T1 – pre, T2 – post, T3–1-mth FU, T4–3-mth FU, and T5–6-mth FU. For the control (delayed) group there was no statistical difference between T0 and T1. Results, highlighted in Figure 3, demonstrated a significant difference in the reduction of the ITQ scores following the treatment intervention over time F(4–332) = 106.84, p < 0.001. Post Hoc comparisons of the ITQ demonstrated a significant difference between T1 pre (mean 36.8, SD 14.8) and T2 post (21.2, 15.1) (t11.58) = 15.68, p < 0.001). This was also seen between T1 pre and T3 1-mth FU (16.8; 14.5) (t13.77) = 20.06, p < 0.001; T1 pre and T4 3-mth FU (14.9, 15.7) (t14.02) = 21.98, p < 0.001; and T1 pre and T5 6-mth FU (12.9, 14.7) (t15.11) = 24.12, p < 0.001. Finally, there was a significant difference between T2 post and T4 3-mth FU d = 0.41, and T5 6-mth FU d. Figure 4 highlights the T1 and T5 scores, including outliers in the T5 dataset.
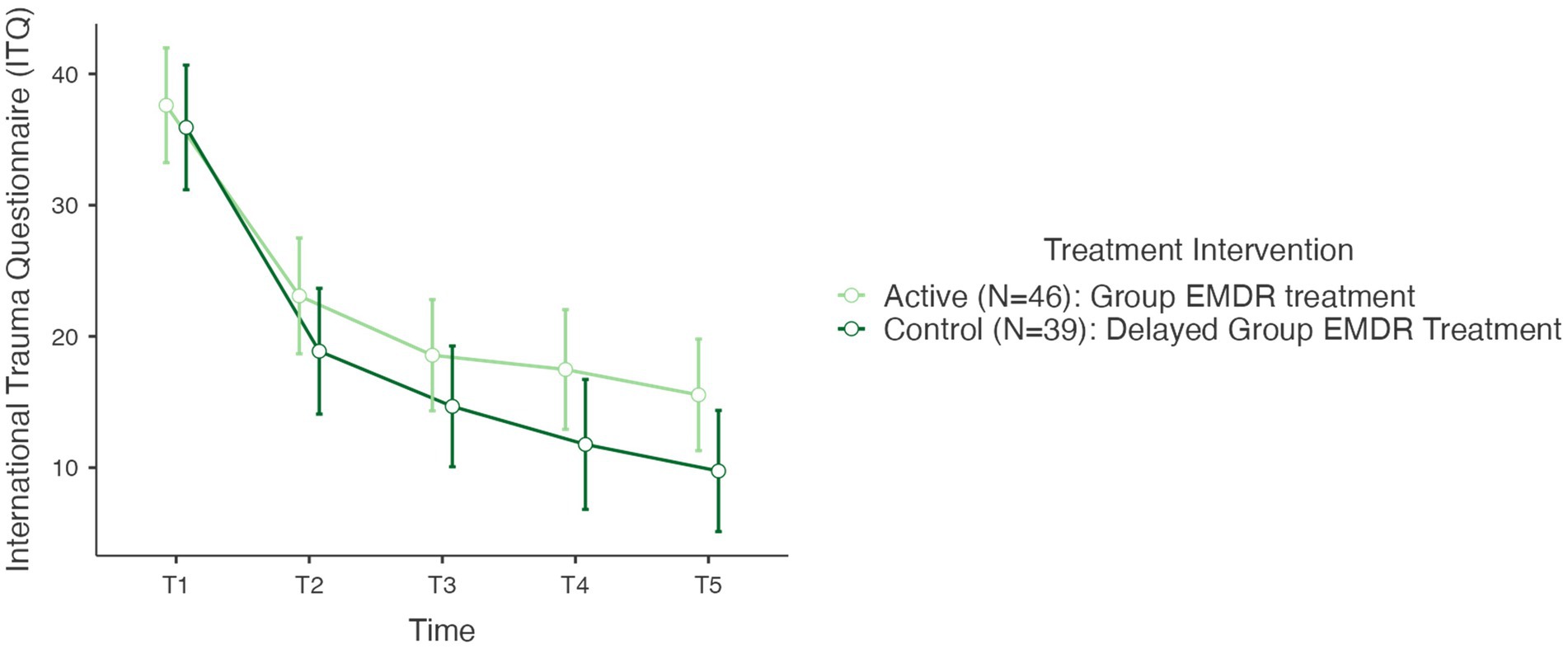
Figure 3. International trauma questionnaire (ITQ) T1–T5 active and control group (N=85) @ p < 0,001. T1, pre; T2, post; T3, 1-mth FU; T4, 3-mth FU; T5, 6-MTH FU.
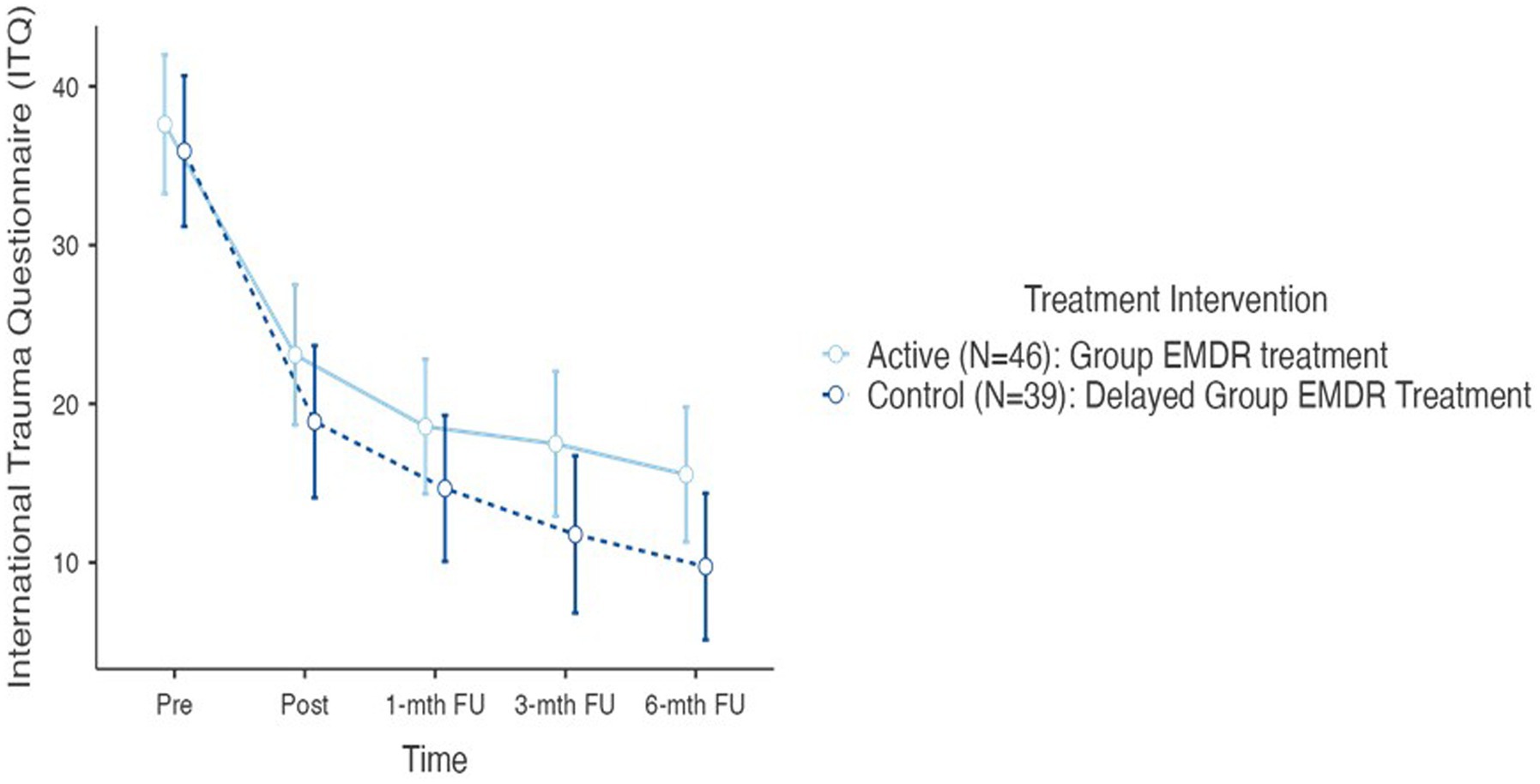
Figure 4. International trauma questionnaire (ITQ) T1–T5 active and control (delayed) groups (N=85) @ p < 0.001.
Concerning the ITQ, post hoc comparison determined no statistically significant difference between the active and the controlled (delayed) treatment interventions. In determining the overall effect size of the treatment intervention regarding the ITQ, as a repeated measures ANOVA used Lakens (2013) cites Cohen (1992) in providing a benchmark for η2 as an indication of effect size: η2 = 0.01 (small), η2 = 0.06 (medium), and η2 = 0.14 (large). Results of the ITQ treatment effect size calculated at η2 = 0.420 indicating a large treatment effect.
During the VGTEP session there are stages where the participants subjective unit of disturbance is assessed. This subjective measure ascertained in steps 1, 2, 5, and 6 of the VGTEP protocol, however, per the research protocol SUD measures obtained pre and post step 1, and at points step 2 and step 6. The rationale for this is to consider changes in subjective distress during both the trauma regulation (step 1) and trauma confrontation (steps 2–6) parts of the VGTEP protocol. Figure 5 highlights the alterations in the SUD during the trauma confrontation stage of the N = 340 participant episodes of VGTEP. The SUD treatment effect size calculated at η2 = 0.295, p < 0.001, indicating a large treatment effect.
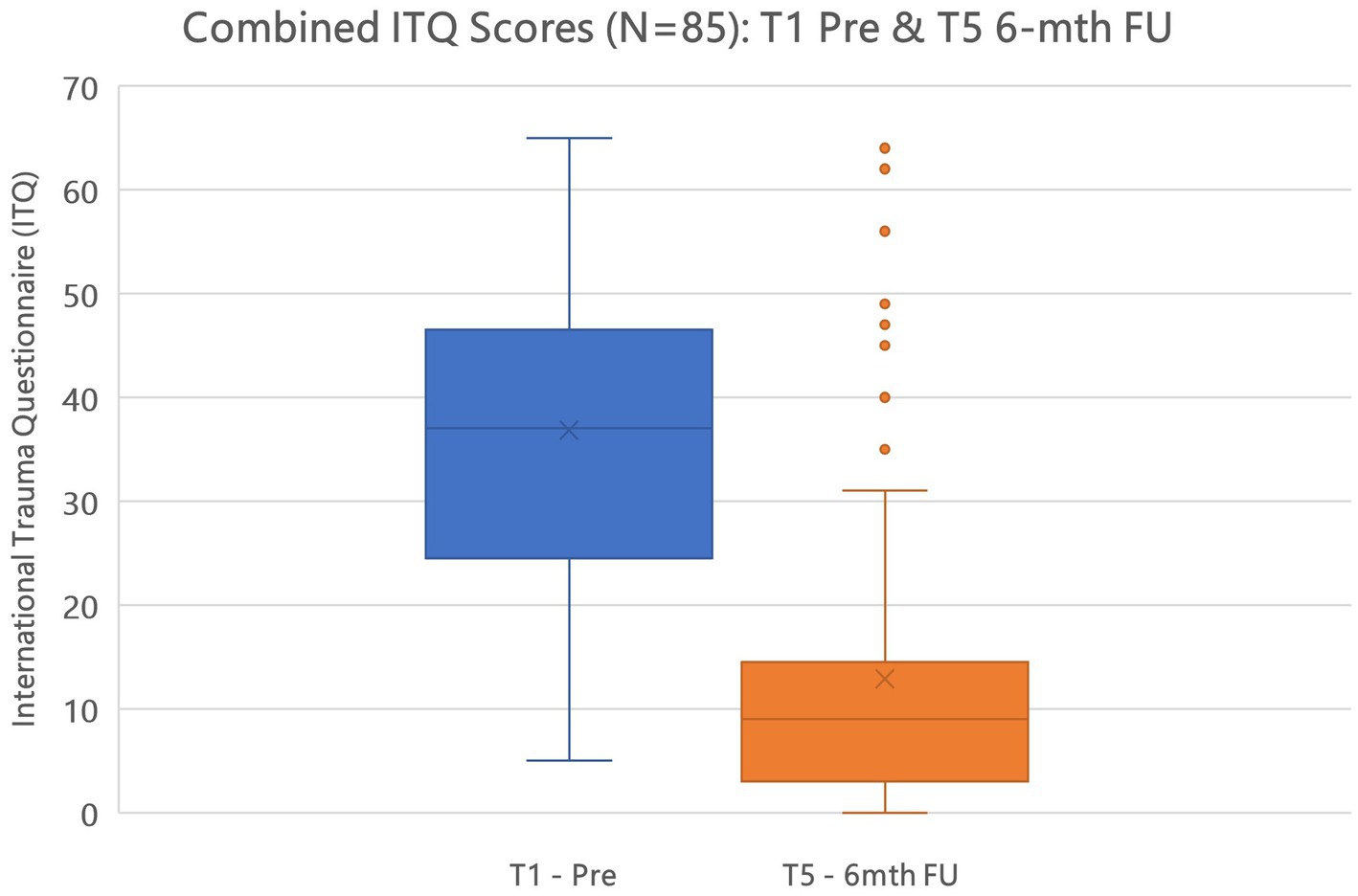
Figure 5. Combined ITQ T1 pre and T5 6-mth FU scores active and control (delayed) groups (N=85) @ p < 0.001.
Table 4 demonstrates alterations in the SUDs phenomenology (mean, SD, median) during the entire VGTEP session including both trauma regulation and confrontation stages. Results suggest that the Trauma Regulation element has a distinct treatment effect overall (η2 = 0.189, p < 0.001), and therefore is of clinical relevance and benefit.

Table 4. Descriptive data measuring Subjective unit of disturbance during VGTEP session (N = 340).
Figure 5 plots the alterations in SUD for both trauma regulation (Step 1 pre and post) and confrontation (Step 2 and 6). Results also highlight the range scores in that within each VGTEP session SUD scores decreased, increased, and flatlined, however, the general trend was a statistically significant (p < 0.001) decrease (Figures 6, 7).
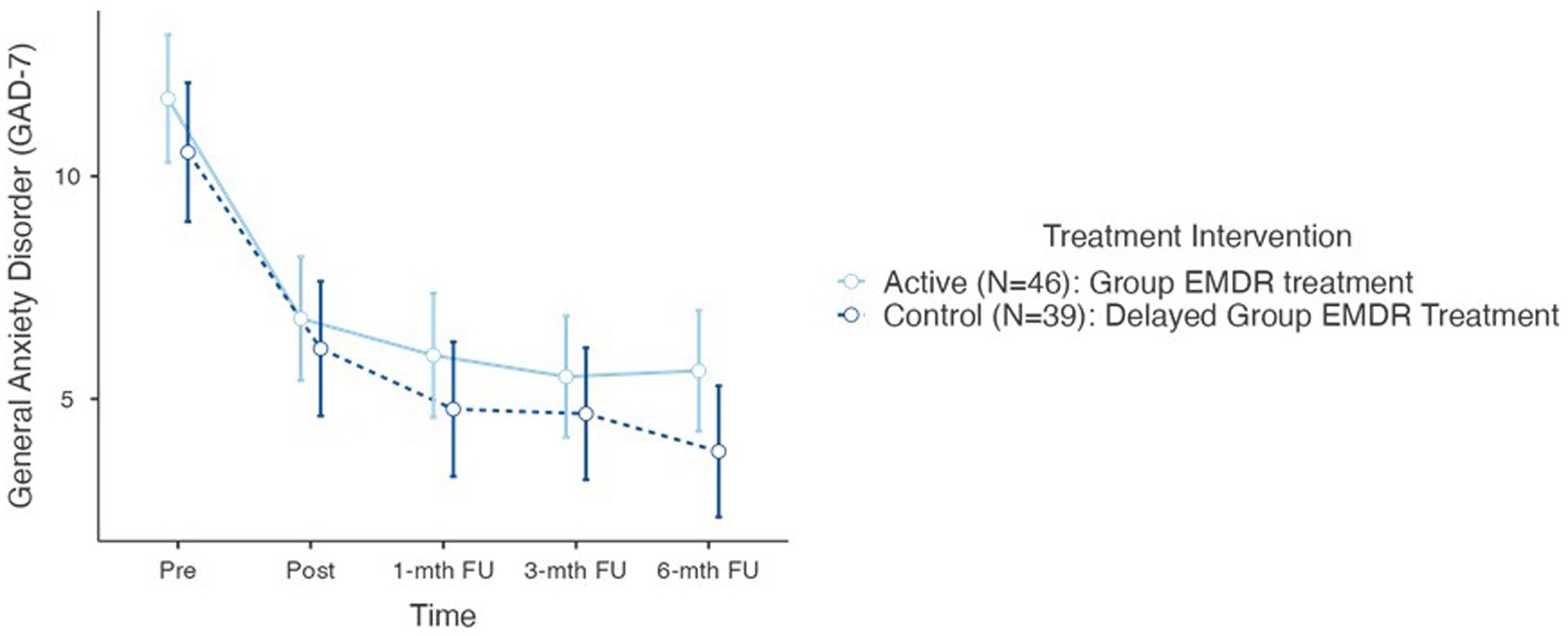
Figure 6. GAD-7 psychometric scores for active and control groups (total N=85).
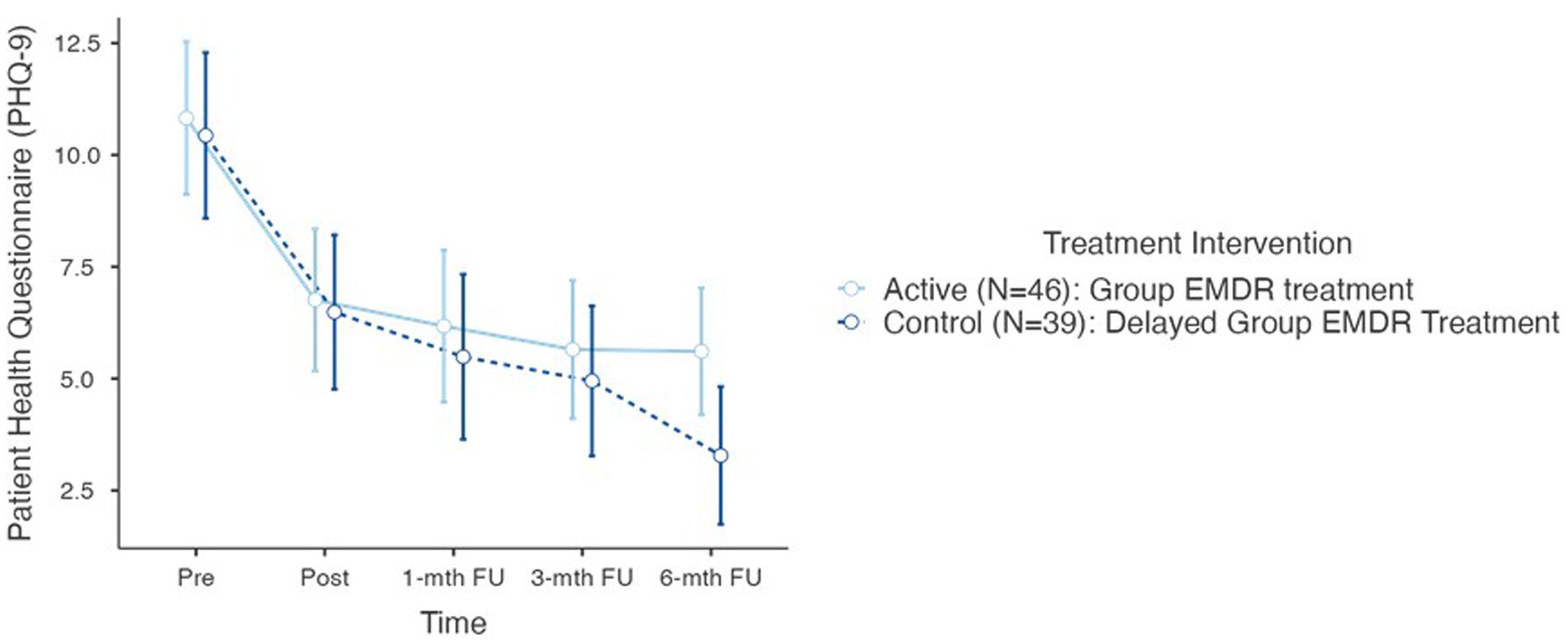
Figure 7. PHQ-9 psychometric scores for active and control groups (total N=85).
For the VGTEP SUD scores for the individual (N = 340) sessions results demonstrated a significant reduction in both groups over time for both trauma regulation (Step 1) and trauma confrontation (Step 2 and 6) with no statistical difference between the active and control (delayed) groups. The overall effect size for the trauma regulation piece @ p < 0.001, with an effect size calculated at η2 = 0.189, and trauma confrontation η2 = 0.295.
In summary, when reviewing hypothesis 1 the null is supported – no difference was observed between the active and control groups indicating that the VGTEP treatment intervention was effective for both groups.
Testing Hypothesis 2: There is no difference between active and control groups regarding co-morbid sequelae – measured with the GAD-7 and the PHQ-9 at T1, T2, T3, T4, and T5.
Further repeated measures conducted to compare the impact of the trauma intervention on both the Generalized Anxiety Disorder Assessment (GAD-7) and the Patient Health Questionnaire (PHQ-9), evaluated at T0 (control group), T1 – pre, T2 – post, T3–1-mth FU, T4–3-mth FU, and T5–6-mth FU. Results determined no statistical difference between the two treatment group interventions for either the GAD-7 or the PHQ-9.
For the GAD-7 results demonstrated a significant reduction in both groups over time F(5–190) = 42.3, p < 0.001. There was no difference between T0 and T1. However, Post Hoc comparisons of the GAD-7 demonstrated significant difference between T1 pre (11.2, 4.91) and T2 post (6.49, 4.73) (t = 6.22) = 4.41, p < 0.001; T1 and T3 1-mth FU (5.42, 4.75) (t = 8.67) = 5.78, p < 0.001; T1 and T4 3-mth (5.12, 4.64) (t = 7.78) = 7.78, p < 0.001; T1 and T5 6-mth FU (4.73, 4.27) (t = 8.93) = 6.72, p < 0.001. In determining the overall effect size of the treatment intervention regarding the GAD-7, the overall effect size calculated as η2 = 0.202 indicating a large treatment effect.
For the Patient Health Questionnaire (PHQ-9) results also demonstrated a significant reduction in both groups over time F(5–190) = 43.3, p < 0.001. Furthermore, like the ITQ and GAD-7, there was no statistical difference between T0 and T1. However, post hoc comparison of the PHQ-9 demonstrated significant differences between T1 pre (11.7, 5.68) and T2 post (6.64, 5.79) (t = 6.30) = 3.95, p < 0.001, d = 0.71; T1 and T3 1-mth FU (5.86, 5.77) (t = 6.22) = 4.95, p < 0.001, d = 0.82; T1 and T4 3-mth FU (5.33, 5.24) (t = 6.39) = 5.49, p < 0.001; and T1 and T5 6-mth FU (4.54, 4.94) (t = 8.89) = 7.15, p < 0.001. In determining the overall effect size of the treatment intervention regarding the GAD-7, the overall effect size calculated as η2 = 0.136 which is on the threshold of a large treatment effect.
Regarding hypothesis 2 the null hypothesis is accepted – no difference was observed between the active and control groups demonstrating that the VGTEP intervention was influential in the treatment of co-morbid features of anxiety and depression.
Hypothesis 3: Treating the trauma sequelae will reduce the level of moral injury in active and control groups.
The Moral Injury Events Scale (MIES) was selected for this study as it has been adapted and applied within civilian research, has the advantage of measuring both events and symptoms, and, as a psychometric, is brief and straightforward in wording (Nash et al., 2013; Koenig et al., 2019). Although the MIES has a three-factor structure: moral violations either perpetrated or witnessed by the individual, and betrayal experiences results at this stage only focused on total scores. Further analysis will be presented in a future paper. Figure 8 demonstrate no treatment effect between T1 pre and T5 6-month FU, measured by the MIES, of the VGTEP intervention in both active and control groups.
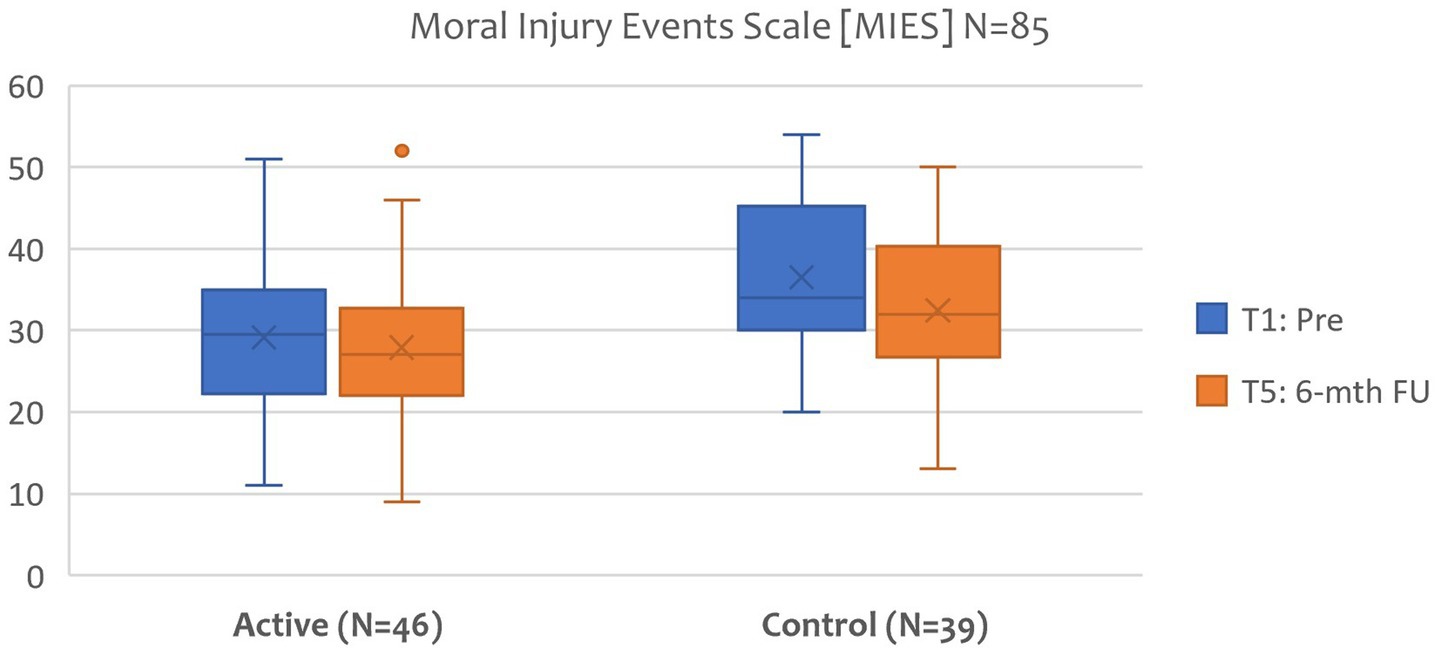
Figure 8. Moral injury events scale (MIES): T1 Pre and T5 6-mth FU (N=85).
Regarding hypothesis 3, the results do not support this hypothesis. Although the VGTEP intervention effectively treated trauma, anxiety, and depression symptoms, results demonstrate no discernible treatment effect on moral injury.
Hypothesis 4: Using Trauma-Focused Therapist rotation will demonstrate no change in clinical diagnosis between T1 and T5, for both active and control groups.
Regarding the diagnoses of PTSD and Complex PTSD, using the ITQ as a diagnostic indicator, Table 5 highlights the impact of the VGTEP treatment intervention at post-treatment (N = 85). At T1 N = 24 had sub-clinical PTSD, N = 28 PTSD, and N = 33 Complex PTSD. Of the research participants with sub-clinical PTSD at the start of the treatment intervention results indicated that 95.83% remained sub-clinical at T5 6-month FU, with 4.17% meeting the criterion for PTSD. Those meeting the criterion for Complex PTSD results suggest a 72.73% improvement to sub-clinical, however, 21.21% showed limited improvement from the VGTEP treatment intervention.
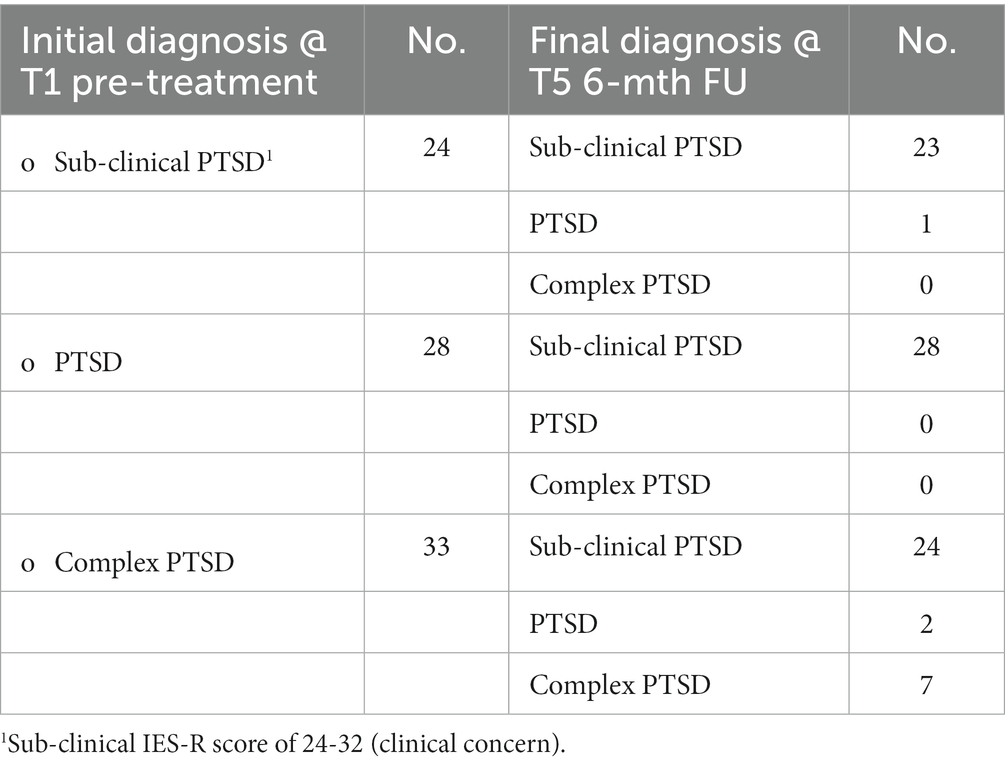
Table 5. Changes in clinical diagnosis following VGTEP intervention using the ITQ at T1 and T5 (N = 85).
Despite using a therapist rotation model within the clinical trial results highlight significant alterations in diagnosis at T5 6-mth FU. The VGTEP interventions had marked efficacy with both the sub-clinical and the PTSD research participants. In the sub-category, only one research participant was referred for additional help and support. With a dropout rate of 10.53% from the clinical trial, and 11.76% finding the treatment intervention insufficient, the overall recovery rate from the VGTEP intervention is estimated at 77.71%. Results confirm that hypothesis 4 is not supported – a favorable recovery rate was achieved using a therapist rotation model.
Hypothesis 5: There is no difference between active and control groups regarding quality of life using the EQ-5D – a generic measure of an individual’s health status and quality of life.
Figure 9 highlights that for the EQ-5D results demonstrated a significant reduction in both groups over time F(1–83) = 48.8, p < 0.001. Post Hoc comparisons of the EQ-5D demonstrated a significant difference between T1 pre (65.02, 17.99) and T5 (79.19, 14.84) t(−6.99) = −14.3, p < 0.001. In determining the overall effect size of the treatment intervention regarding the EQ-5D, calculated as η2 = 0.159 indicating a large treatment effect. There was not statistical difference between each of the groups. A more in-depth review of the health economic data will follow in a later paper.
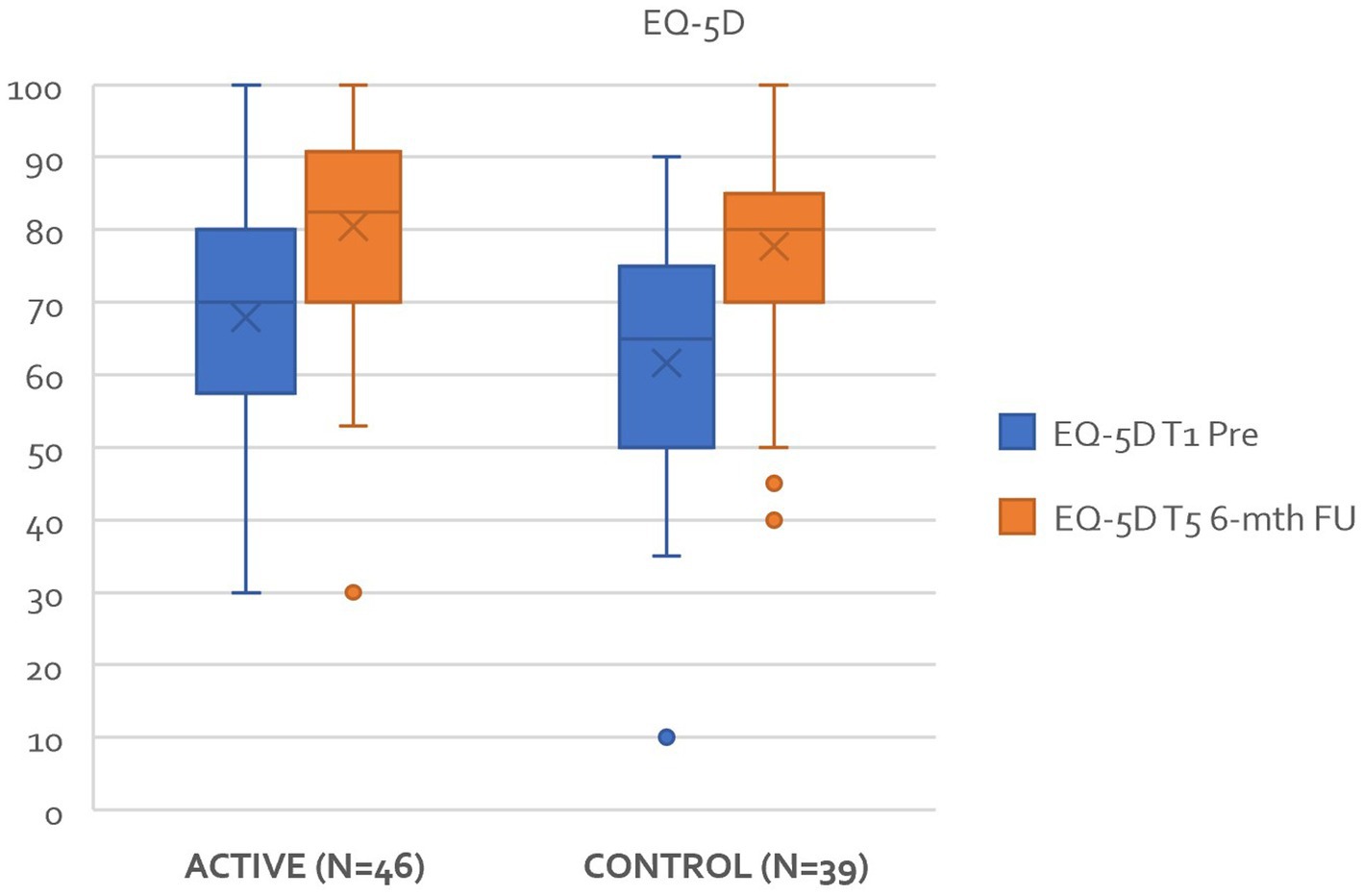
Figure 9. Improvements in EQ-5D between T1 and T5 active and control groups.
Hypothesis 6: A correlation exists, within the target population, between Adverse Childhood Experiences (ACEs) and Benevolent Childhood Experiences (BCEs) regarding evidence supporting resilience and posttraumatic growth.
A Pearson correlation coefficient was computed to assess the linear relationship between Adverse Childhood Experiences (ACEs) and Benevolent Childhood Experiences (BCEs). Results revealed a moderate, negative correlation between the two r = −0.312, **p = <0.01 as highlighted in Table 6. Bivariate analysis of either ACEs or BCEs revelated no other linear relationships with the ITQ, GAD-7, PHQ-9, MIES, or EQ-5D. Results indicate that the VGTEP treatment intervention was effective regardless of a research participants ACE or BCE scores.
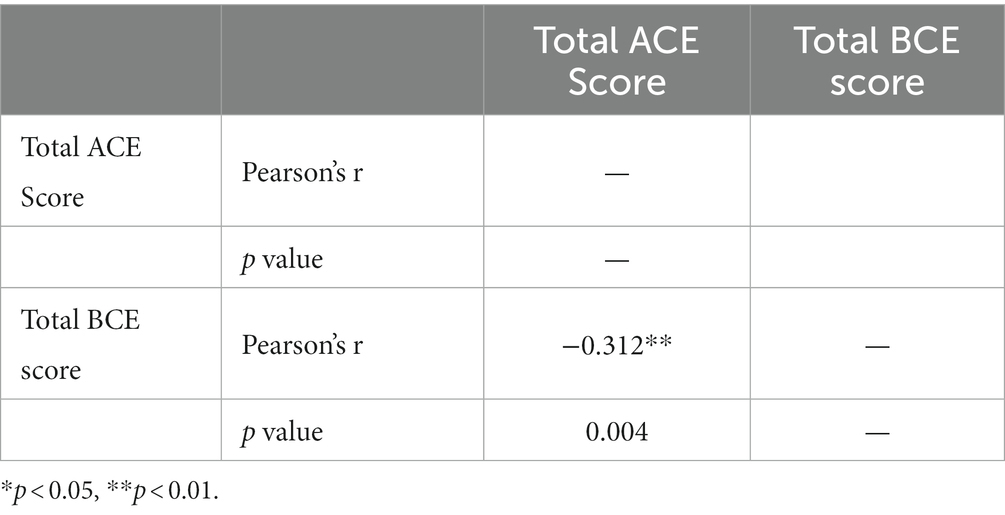
Table 6. Correlation matrix between ACEs and BCEs.
Table 7 highlights qualitative data related to the research participants which focused on the drop-outs from the study. Each participant was followed-up and offered further support and intervention. As their withdrawal impacted upon the T2 – T5 psychometric data their data removed from the overall data set. Although a 10.58% drop-out rate is low it is also reasonable to assume that not every client, once they have direct experience of working in this way, will find it useful.
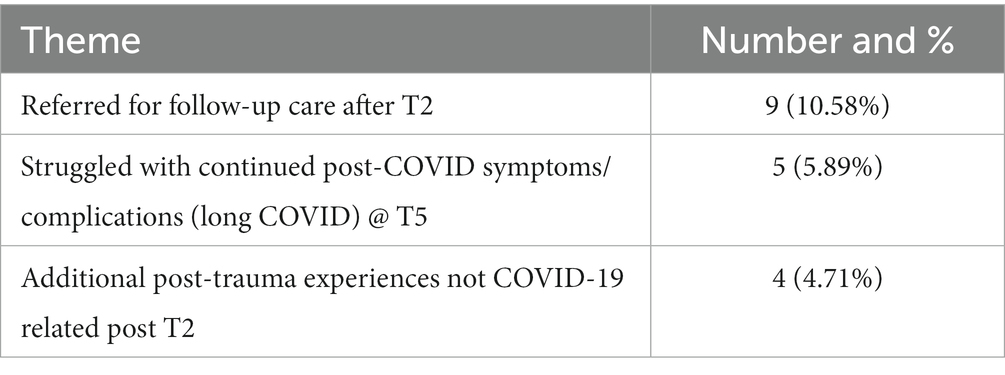
Table 7. Qualitative factors which impacted upon T2–T5 psychometric data.
At T5 6-month FU, every research participant contacted to provide brief feedback about their lived experience of undergoing the VGTEP intervention. A further research paper will explore this in more detail. However, Figure 10 highlights the primary response which clustered around 13 themes. The overwhelming feedback appeared to suggest the VGTEP intervention to have been effective, helpful, and timely.

Figure 10. Primary themes related to the qualitative feedback received from research participants post T5 (6-mth FU/end of treatment).
Discussion
Undertaking any large-scale, early intervention clinical trial is always difficult and present significant logistical challenges. Doing so during periods of Government-Imposed lockdown was also immensely demanding. The rationale for the study was to carry out a multi-component research project which focused on an important population at the frontline of the COVID-19 response. The realities of the COVID-19 pandemic, and carrying out clinical research, meant that everyone involved – the research participants, research team, and clinicians were all exposed to the ‘lived experience’ realities of COVID-19. Therefore, a reasonable conclusion is that the universality level for this whole study was extraordinarily high. As highlighted within the literature review, defining early intervention is not straight forward. Considering the ongoing nature of the pandemic for the entire duration of this RCT there is an argument cogent argument for this qualifying as an early intervention study.
An important reality of the current time was that lack of availability of trauma-informed early intervention for frontline emergency workers paradoxically assisted recruitment for our study. The consequence of this resulted in most research participants highly motivated, and appreciative to being included. Despite the eventual recruitment, a larger sample would have further enhanced the study’s findings. However, as this was an unfunded study, it was essential to make the limited resources we had stretch as far as possible.
The headline results from this RCT suggest that EMDR therapy, delivered remotely through a virtual platform was effective in the treatment of both PTSD and complex PTSD. This is an important finding considering the critical elements of group treatment, remote intervention, intensive delivery, and therapist rotation. When demand outstrips supply regarding access to trauma interventions research supporting the benefits of group treatment suggest significant resource benefits. Further research is needed to explore the potential benefits of this in relation to task-shifting.
However, based upon this data set, results do not support its efficacy as a treatment for Moral Injury. Although results are favorable regarding the ITQ, GAD-7, PHQ-9, SUD, and EQ-5D, demonstrating that the VGTEP intervention appeared relevant to the research population under investigation, results also suggest that the intervention was well tolerated, potentially safe, and effective as a treatment intervention. Intriguingly, there was no demonstrable difference between active and control (delayed) groups. Despite promising results, caution also needs to be exercised. The absence of another trauma-focused treatment intervention as a realistic comparator suggests that more research is required to ascertain a more reliable efficiency indicator. For example, future early intervention should consider comparing VGTEP with another Trauma-focused CBT Group Intervention.
Overall, the dropout rate for the study was just below 11%. There are two ways of looking at this; firstly, this level is particularly favorable to the context in which the research study operated – during a global pandemic. A contrary perspective relates to the tolerability of any psychological treatment intervention. There will always be dropouts related to factors unrelated to the study intervention – this was certainly the case for some but by no means all. However, following up on those that did drop out and relate to the treatment intervention highlighted that for some, it was too intense, too powerful, and too overwhelming, bearing in mind everything else going on in people’s lives at the time.
There are four other factors to consider. Firstly, treatment was delivered as video-conference psychotherapy. Overall results suggest that this was generally well tolerated. Although there were occasional technical glitches, fortunately, these were relatively infrequent. Indeed, the ZOOM platform performed robustly for much of the study—Secondly, the intense delivery of the treatment within 1 week. Again, results suggest that this was well tolerated, although admittedly, it does require a significant commitment from research participants. Further research needs to explore the potential health economic benefits of delivering trauma treatment in this manner. Thirdly, the VGTEP intervention involves non-disclosure of any trauma material. This aspect has advantages and disadvantages. Advantages include a greater willingness to work on traumatic material without the need for disclosure. This maximizes both power and control for the research participants. If trauma memories involve shame, fear of retribution, or a shattering of assumptive networks then there are clear benefits to non-disclosure. Disadvantages include a difficulty in demonstrating cause and effect. Although research participants were invited to work with recent material there was no means to accurately monitor this. This both a strength and limitation to this study. That said, previous research demonstrates qqclear benefits from working with non-disclosed trauma material (Farrell et al., 2020, 2022). Non-disclosure of trauma material does have another distinct advantage as non-disclosure of trauma material potentially reduces the risk of vicarious traumatization of therapists. However, more research is needed to explore this aspect further to ascertain if there is veracity in this argument.
The study’s results shed interesting light on the therapist rotation model. Instinctively, therapist rotation seems counterintuitive, considering the therapist relationship critical to outcome. Results from this study run counter to this narrative. Why is therapist rotation effective? There are several reasons to consider. The VGTEP intervention is highly structured – there are distinct benefits from this, reassurance, familiarity, containment, etc., however, the intervention is relatively passive. This argument may provide a rationale for why VGTEP was effective for PTSD/C-PTSD, but not Moral Injury (MI), is that MI requires more active engagement. This would require further investigation and study, and if proven correct, would necessitate further adaptation in EMDR group interventions.
The GTEP protocol involves 27 episodes of trauma confrontation and requires further research and investigation, particularly into its distinctive parts – which are essential, which not? Results from this study demonstrate an overall treatment effect; however, further dismantling studies need to explore whether there might be more effective or efficient means of achieving similar or better results.
Results from Table 5 are intriguing. Within the first category 28% were sub-clinical PTSD, and post-treatment 96% remained in this category. Could this potentially suggest that early intervention Group EMDR prevented the onset of PTSD? Further research is needed to explore this, however, even though results from this study are promising caution against over-reach is important. Of further interest relate to the PTSD and Complex PTSD data which suggest the favorability of the Group EMDR intervention. Again, these results are cautiously promising, however, further research is needed.
Roberts et al. (2019) conclude little evidence that most multiple-session trauma treatment interventions have little impact on primary outcome measures. However, our study’s results do not concur with this perspective. There is, nonetheless, an important narrative to consider at this juncture – results from this study suggest a significant treatment effect for PTSD but not for moral injury. Why might this be the case? This is an intriguing question. A potential consideration relates to the ‘unknowingness’ of the trauma memory clients use to target and reprocess. The EMDR GTEP and VGTEP interventions are ostensibly passive treatments. Within conventional EMDR therapy, moral dimensions are often addressed more actively with the utilization of Cognitive Interweaves, which are much more bespoke to the client’s lived experiences. However, more research is needed to explore this further, but results suggest a potential need for modifying the existing group EMDR protocols to address moral dimensions of trauma more effectively.
Another critical point of note relates to Adverse and Benevolent Childhood Experiences. Results from this study parallel an earlier study (Farrell et al., 2022) demonstrating a trauma treatment effect irrespective of either individual or collective ACEs or BCEs. Although results show a moderate, negative correlation between ACEs and BCEs, this certainly needs further research and exploration. The evidence from this study suggests that adverse memories process in EMDR therapy regardless of the form the adversity takes. The way benevolent factors potentially mitigate does require further investigation, particularly utilizing the theoretical framework of Adaptive Information Processing – the model underpinning EMDR therapy.
We recognize that follow periods reported within this RCT study are short (Dumoulin et al., 2018), however we took the pragmatic decision to use three-and six-month timeframes for follow up given the relative urgency to provide online psychological support to frontline workers during the pandemic (Drissi et al., 2021). A recent systemic review (Wilson et al., 2018) suggests follow up periods of between 4 weeks and 6 months is not uncommon in EMDR intervention research. For example, in what appears to be the only trial of online EMDR (Lenferink et al., 2020), Spence et al., 2013 used a 3 month follow up period when examine the use of internet delivered EMDR. We are therefore content that the design chosen for the study is in line with other EMDR related randomized controlled trials, however, acknowledge that the longer-term maintenance of benefits from the intervention may not be fully understood.
A further, distinct limitation of the study relates to the issue of moral injury. Further research is needed to adapt EMDR group interventions more specifically more sufficiently for this important issue. Secondly, with the benefit of hindsight, incorporating more qualitative data surrounding the participants experience would have been useful. Presently, there is no absolute clarity surrounding agents of change other than from the psychometric data. Thirdly, it would have been useful to ascertain better insight into the target memories worked on by the research participants. This was always going to be challenging based the critical aspect of non-disclosure. A further aspect related to this would have been to determine if research participants may indeed have been willing to disclose their trauma targets. Fourthly, would be to consider if more detailed debriefing sessions after the VGTEP intervention may have further enhanced the study’s findings. Fifthly, as the research participants were ‘self-selecting’ this leads to the possibility of bias and ambiguity. By not capturing or clarifying motivation for being part of the study there is a fair degree of uncertainty about this aspect. Furthermore, a distinct limitation was not being able to ascertain which trauma targets were moral injury, or not. A final limitation relates to the sub-clinical PTSD participants. The data set suggests that many from this group remained ‘sub-clinical’ post-intervention, however, there is not means to determine cause and effect, that the intervention prevented the onset of PTSD. To ascertain this with more clarity further research is needed.
A contemporary debate within the EMDR therapy literature relates to the value of trauma regulation. The data presented in Figure 5 suggests treatment benefits for trauma regulation and trauma confrontation phases with VGTEP; however, the effect size is more significant for trauma confrontation. Nevertheless, results suggest the clear advantage of utilizing trauma regulation strategies within the VGTEP intervention, even if this provides a grounding, presentness, or even a sense of community-building. Further dismantling studies need to explore this aspect in more detail.
Conclusion
The COVID-19 pandemic has presented significant challenges individually, collectively, and geopolitically. Ascertaining treatment interventions that can be delivered remotely safely, relevant to trauma populations, that are both effective and efficient, is paramount. In addition, the advantage of treatment given through video-conference platforms potentially increases availability and access. Critical to this relates to technical components, including availability, access, and functionality in making such treatment interventions viable on a fundamental level of scalability.
This research suggests the potential efficacy of the Group EMDR intervention; incorporating a therapist rotation model adds a contemporary facet that seems counterintuitive to the existing academic literature. In addressing the global burden of psychological trauma and the necessity for task-shifting, this study offers interesting findings to this debate.
The primary objective and rationale for this study were Frontline and Emergency colleagues working on the frontline of COVID-19 traumatized by their endeavors. This study contributes to the emerging knowledge base that Group EMDR therapy has something significant to contribute.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number (s) can be found in the article/supplementary material.
Ethics statement
The studies involving human participants were reviewed and approved by University of Worcester. The patients/participants provided their written informed consent to participate in this study.
Author contributions
DF conceived the study, was the chief investigator for the entire project, the principal data analyst, and the primary author of this research manuscript. JM was responsible for project management. MK was responsible for secondary data analysis, senior leadership, and support to the project. LK, PM, IM, DM, TP, PP, CM, and IB were vital research team members and treatment interventions. ZZ was responsible for treatment fidelity. DF, LK, JM, PM, IM, DM, TP, and PP were all clinical leads regarding the VGTEP treatment intervention. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank Trauma Response Ireland and Sonjia Maher for her invaluable contribution and administrative support. Additionally, we would like to thank Clare Smith, Adam Horner, Gus Murray, Bev Taylor, Carol Norris, Imelda Buckley, Yvonne Bayo, and the many colleagues who assisted this study as the Emotional Protection team. Finally, we thank EMDR All Ireland Board—President Gus Murray for the vital support of the research project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
Acarturk, C., Konuk, E., Cetinkaya, M., Senay, I., Sijbrandij, M., Gulen, B., et al. (2016). The efficacy of eye movement desensitization and reprocessing for post-traumatic stress disorder and depression among Syrian refugees: results of a randomized controlled trial. Psychol. Med. 46, 2583–2593. doi: 10.1017/S0033291716001070
Amsalem, D., Lazarov, A., Markowitz, J. C., Naiman, A., Smith, T. E., Dixon, L. B., et al. (2021). Psychiatric symptoms and moral injury among US healthcare workers in the COVID-19 era. BMC Psychiatry 21:546. doi: 10.1186/s12888-021-03565-9
Appleton, R., Williams, J., Needle, J. J., Schlief, M., Jordan, H., Sheridan Rains, L., et al. (2021). Implementation, adoption, and perceptions of Telemental health during the COVID-19 pandemic: systematic review. J. Med. Internet Res. 23:e31746. doi: 10.2196/31746
Arpacioglu, S., Gurler, M., and Cakiroglu, S. (2021). Secondary traumatization outcomes and associated factors among the health care workers exposed to the COVID-19. Int. J. Soc. Psychiatry 67, 84–89. doi: 10.1177/0020764020940742
Asmussen, K., McBride, T., and Waddell, S. (2019). The potential of early intervention for preventing and reducing ACE-related trauma. Soc. Policy Soc. 18, 425–434. doi: 10.1017/S1474746419000071
Asukai, N., Kato, H., Kawamura, N., Kim, Y., Yamamoto, K., Kishimoto, J., et al. (2002). RELIABILIGY and validity of the JAPANESE-language version of the impact of event scale-REVISED (IES-r-j): four studies of different traumatic events. J. Nerv. Ment. Dis. 190, 175–182. doi: 10.1097/00005053-200203000-00006
Barnes, H. A., Hurley, R. A., and Taber, K. H. (2019). Moral injury and PTSD: often co-occurring yet mechanistically different. J. Neuropsychiatry Clin. Neurosci. 31, A4–A103. doi: 10.1176/appi.neuropsych.19020036
Beames, J. R., Christensen, H., and Werner-Seidler, A. (2021). School teachers: the forgotten frontline workers of Covid-19. Australas. Psychiatry 29, 420–422. doi: 10.1177/10398562211006145
Beck, J. G., Grant, D. M., Read, J. P., Clapp, J. D., Coffey, S. F., Miller, L. M., et al. (2008). The impact of event scale-revised: psychometric properties in a sample of motor vehicle accident survivors. J. Anx. Disorders 22, 187–198.
Billings, J., Ching, B. C. F., Gkofa, V., Greene, T., and Bloomfield, M. (2021). Experiences of frontline healthcare workers and their views about support during COVID-19 and previous pandemics: a systematic review and qualitative meta-synthesis. BMC Health Serv. Res. 21:923. doi: 10.1186/s12913-021-06917-z
Brock, R. N., and Lettini, G. (2012). Soul repair: Recovering from moral injury after war. Beacon Press.
Borges, L. M., Barnes, S. M., Farnsworth, J. K., Bahraini, N. H., and Brenner, L. A. (2020). A commentary on moral injury among health care providers during the COVID-19 pandemic. Psychol. Trauma Theory Res. Pract. Policy 12, S138–S140. doi: 10.1037/tra0000698
Broadbear, J. H., Heidari, P., Dharwadkar, N. P., Cheney, L., and Rao, S. (2021). Telehealth psychotherapy for severe personality disorder during COVID-19: experience of Australian clinicians. Global J. Health Sci. 13:61. doi: 10.5539/gjhs.v13n12p61
Brunet, A., Rivest-Beauregard, M., Lonergan, M., Cipolletta, S., Rasmussen, A., Meng, X., et al. (2022). PTSD is not the emblematic disorder of the COVID-19 pandemic; adjustment disorder is. BMC Psychiatry 22:300. doi: 10.1186/s12888-022-03903-5
Bryant, R. A. (2021). A critical review of mechanisms of adaptation to trauma: implications for early interventions for posttraumatic stress disorder. Clin. Psychol. Rev. 85:101981. doi: 10.1016/j.cpr.2021.101981
Bryant, R. A. (2022). “Early intervention after trauma” in Evidence based treatments for trauma-related psychological disorders (Springrm, Cham: Springer International Publishing), 135–159. doi: 10.1007/978-3-030-97802-0_7
Cantone, D., Guerriera, C., and ARCHITRAVO, M., (2021). A sample of Italian psychotherapists express their perception and opinions of online psychotherapy during the covid-19 pandemic. Riv. Psichiatr. 56, 98–204. doi: 10.1708/3654.36347
Carmassi, C., Dell’Oste, V., Bui, E., Foghi, C., Bertelloni, C. A., Atti, A. R., et al. (2022). The interplay between acute post-traumatic stress, depressive and anxiety symptoms on healthcare workers functioning during the COVID-19 emergency: A multicenter study comparing regions with increasing pandemic incidence. J. Affect. Disord. 298, 209–216. doi: 10.1016/j.jad.2021.10.128
Carriere, R. C. (2014). Scaling up what works: using EMDR to help confront the World’s burden of traumatic stress. J. EMDR Pract. Res. 8, 187–195. doi: 10.1891/1933-3196.8.4.187
Čartolovni, A., Stolt, M., Scott, P. A., and Suhonen, R. (2021). Moral injury in healthcare professionals: A scoping review and discussion. Nurs. Ethics 28, 590–602. doi: 10.1177/0969733020966776
Cataldo, F., Chang, S., Mendoza, A., and Buchanan, G. (2021). A perspective on client-psychologist relationships in videoconferencing psychotherapy: literature review. JMIR Mental Health 8:e19004. doi: 10.2196/19004
Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N., et al. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 45, 11–27. doi: 10.1017/S0033291714000129
Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., et al. (2018). The international trauma questionnaire: development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatr. Scand. 138, 536–546. doi: 10.1111/acps.12956
Cohen, J. (1992). Statistical Power Analysis. Curr. Direct. Psychol. Sci. 1, 98–101. doi: 10.1111/1467-8721.ep10768783
Covers, M. L. V., de Jongh, A., Huntjens, R. J. C., de Roos, C., van den Hout, M., and Bicanic, I. A. E. (2021). Early intervention with eye movement desensitization and reprocessing (EMDR) therapy to reduce the severity of post-traumatic stress symptoms in recent rape victims: a randomized controlled trial. Eur. J. Psychotraumatol. 12:3188. doi: 10.1080/20008198.2021.1943188
Creamer, M., Bell, R., and Failla, S. (2003). Psychometric properties of the impact of event scale—Revised. Behav. Res. Ther. 41, 1489–1496. doi: 10.1016/j.brat.2003.07.010
Creamer, M. C., Varker, T., Bisson, J., Darte, K., Greenberg, N., Lau, W., et al. (2012). Guidelines for peer support in high-risk organizations: an international consensus study using the delphi method. J. Trauma. Stress. 25, 134–141. doi: 10.1002/jts.21685
Crowe, M., Inder, M., Farmar, R., and Carlyle, D. (2020). Delivering psychotherapy by video conference in the time of COVID-19: some considerations. J. Psychiat. Mental Health Nurs. 28, 751–752. doi: 10.1111/jpm.12659
de Kock, J. H., Latham, H. A., Leslie, S. J., Grindle, M., Munoz, S.-A., Ellis, L., et al. (2021). A rapid review of the impact of COVID-19 on the mental health of healthcare workers: implications for supporting psychological well-being. BMC Public Health 21:104. doi: 10.1186/s12889-020-10070-3
de Roos, C., Greenwald, R., den Hollander-Gijsman, M., Noorthoorn, E., van Buuren, S., and de Jongh, A. (2011). A randomized comparison of cognitive behavioral therapy (CBT) and eye movement desensitization and reprocessing (EMDR) in disaster-exposed children. Eur. J. Psychotraumatol. 2:5694. doi: 10.3402/ejpt.v2i0.5694
Dharwadkar, N. P., Broadbear, J. H., Heidari, P., Cheney, L., and Rao, S. (2021). Psychotherapy via Telehealth during the COVID-19 pandemic in australia–experience of clients with a diagnosis of borderline personality disorder. Global J. Health Sci. 14:29. doi: 10.5539/gjhs.v14n1p29
Diop, N., Anderson, I., Gwezera, B., Fihn, J., Gohar, F., Morgos, D., et al. (2022). Mental health and psychosocial support concerns among frontline workers within the eastern and southern Africa COVID-19 response. Pan African Med. J. 41:9032. doi: 10.11604/pamj.supp.2022.41.2.29032
Do, D. P., and Frank, R. (2021). U.S. frontline workers and COVID-19 inequities. Prev. Med. 153:106833. doi: 10.1016/j.ypmed.2021.106833
Drissi, N., Ouhbi, S., Marques, G., de la Torre Díez, I., Ghogho, M., and Janati Idrissi, M. A. (2021). A systematic literature review on e-mental health solutions to assist health care workers during COVID-19. Telemed. E-Health 27, 594–602. doi: 10.1089/tmj.2020.0287
Dumoulin, C., Cacciari, L. P., and Hay-Smith, E. J. C. (2018). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst. Rev. 2018:CD005654. doi: 10.1002/14651858.CD005654.pub4
Dunkley, F. (2018). Psychosocial support for humanitarian aid workers: a roadmap of trauma and critical incident care. London UK: Routledge.
Dyregrov, A., and Regel, S. (2012). Early interventions following exposure to traumatic events: implications for practice from recent research. J. Loss Trauma 17, 271–291. doi: 10.1080/15325024.2011.616832
Eichfeld, C., Farrell, D., Mattheß, M., Bumke, P., Sodemann, U., Ean, N., et al. (2019). Trauma stabilization as a sole treatment intervention for post-traumatic stress disorder in Southeast Asia. Psychiatry Q. 90, 63–88. doi: 10.1007/s11126-018-9598-z
Farnsworth, J. K. (2019). Is and ought: descriptive and prescriptive cognitions in military-related moral injury. J. Trauma. Stress. 32, 373–381. doi: 10.1002/jts.22356
Farrell, D., Fadeeva, A., Zat, Z., Knibbs, L., Miller, P., Barron, I., et al. (2022). A stage 1 pilot cohort exploring the use of EMDR therapy as a videoconference psychotherapy during COVID-19 with frontline mental health workers: A proof-of-concept study Utilizing a virtual blind 2 therapist protocol. Front. Psychol. 13:1855. doi: 10.3389/fpsyg.2022.901855
Farrell, D. P., Keenan, P. S., Ali, M. W., Bilal, S., Tareen, S. M., Keenan, L., et al. (2011). Training Pakistani mental health workers in EMDR in the aftermath of the 2005 earthquake in northern Pakistan. Couns. Psychol. Q. 24, 127–137. doi: 10.1080/09515070.2011.589599
Farrell, D., Keenan, P., Knibbs, L., and Hicks, C. (2013). A Q-methodology evaluation of an EMDR europe HAP facilitators training in Pakistan. J. EMDR Pract. Res. 7, 174–185. doi: 10.1891/1933-3196.7.4.174
Farrell, D., Kiernan, M. D., de Jongh, A., Miller, P. W., Bumke, P., Ahmad, S., et al. (2020). Treating implicit trauma: a quasi-experimental study comparing the EMDR therapy standard protocol with a “blind 2 Therapist” version within a trauma capacity building project in northern Iraq. J. Int. Human. Act. 5:3. doi: 10.1186/s41018-020-00070-8
Feingold, J. H., Hurtado, A., Feder, A., Peccoralo, L., Southwick, S. M., Ripp, J., et al. (2022). Posttraumatic growth among health care workers on the frontlines of the COVID-19 pandemic. J. Affect. Disord. 296, 35–40. doi: 10.1016/j.jad.2021.09.032
Ghahramani, S., Kasraei, H., Hayati, R., Tabrizi, R., and Marzaleh, M. A. (2022). Health care workers’ mental health in the face of COVID-19: a systematic review and meta-analysis. Int. J. Psychiatry Clin. Pract. 23, 1–10. doi: 10.1080/13651501.2022.2101927
Greenberg, N., Docherty, M., Gnanapragasam, S., and Wessely, S. (2020). Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 368:m1211. doi: 10.1136/bmj.m1211
Greene, T., Harju-Seppänen, J., Adeniji, M., Steel, C., Grey, N., Brewin, C. R., et al. (2021). Predictors and rates of PTSD, depression and anxiety in UK frontline health and social care workers during COVID-19. Eur. J. Psychotraumatol. 12:2781. doi: 10.1080/20008198.2021.1882781
Griffin, B. J., Purcell, N., Burkman, K., Litz, B. T., Bryan, C. J., Schmitz, M., et al. (2019). Moral injury: an integrative review. J. Trauma. Stress. 32, 350–362. doi: 10.1002/jts.22362
Gronholm, P. C., Nosé, M., van Brakel, W. H., Eaton, J., Ebenso, B., Fiekert, K., et al. (2021). Reducing stigma and discrimination associated with COVID-19: early-stage pandemic rapid review and practical recommendations. Epidemiol. Psychiatr. Sci. 30:e15. doi: 10.1017/S2045796021000056
Hase, M. (2021). The structure of EMDR therapy: A guide for the therapist. Front. Psychol. 12:753. doi: 10.3389/fpsyg.2021.660753
Hase, M., Balmaceda, U. M., Ostacoli, L., Liebermann, P., and Hofmann, A. (2017). The AIP model of EMDR therapy and pathogenic memories. Front. Psychol. 8:1578. doi: 10.3389/fpsyg.2017.01578
Haugen, P. T., Evces, M., and Weiss, D. S. (2012). Treating posttraumatic stress disorder in first responders: A systematic review. Clin. Psychol. Rev. 32, 370–380. doi: 10.1016/j.cpr.2012.04.001
Herman, J. L., and Kallivayalil, D. (2018). Group trauma treatment in early recovery. Guilford Publications. New York, United States.
Hooper, J. J., Saulsman, L., Hall, T., and Waters, F. (2021). Addressing the psychological impact of COVID-19 on healthcare workers: learning from a systematic review of early interventions for frontline responders. BMJ Open 11:e044134. doi: 10.1136/bmjopen-2020-044134
Hyland, P., Shevlin, M., Brewin, C. R., Cloitre, M., Downes, A. J., Jumbe, S., et al. (2017). Validation of post-traumatic stress disorder (PTSD) and complex PTSD using the international trauma questionnaire. Acta Psychiatr. Scand. 136, 313–322. doi: 10.1111/acps.12771
Izutsu, T., Shibuya, M., Tsutsumi, A., Konishi, T., and Kawamura, N. (2008). The relationship between past traumatic experience and sickness absence. Int. J. Soc. Psychiatry 54, 83–89. doi: 10.1177/0020764007083874
Izutsu, T., Tsutsumi, A., Asukai, N., Kurita, H., and Kawamura, N. (2004). Relationship between a traumatic life event and an alteration in stress response. Stress. Health 20, 65–73. doi: 10.1002/smi.997
Jamieson, N., Maple, M., Ratnarajah, D., and Usher, K. (2020a). Military moral injury: A concept analysis. Int. J. Ment. Health Nurs. 29, 1049–1066. doi: 10.1111/inm.12792
Jamieson, N., Usher, K., Maple, M., and Ratnarajah, D. (2020b). Invisible wounds and suicide: moral injury and veteran mental health. Int. J. Ment. Health Nurs. 29, 105–109. doi: 10.1111/inm.12704
Jarero, I., Givaudan, M., and Osorio, A. (2018). Randomized controlled trial on the provision of the EMDR integrative group treatment protocol adapted for ongoing traumatic stress to female patients with cancer-related posttraumatic stress disorder symptoms. J. EMDR Pract. Res. 12, 94–104. doi: 10.1891/1933-3196.12.3.94
Jecker, N. S., Wightman, A. G., and Diekema, D. S. (2020). Prioritizing frontline workers during the COVID-19 pandemic. Am. J. Bioeth. 20, 128–132. doi: 10.1080/15265161.2020.1764140
Johnson, S. U., Ebrahimi, O., and v., & Hoffart, A., (2020). PTSD symptoms among health workers and public service providers during the COVID-19 outbreak. PLoS One 15:e0241032. doi: 10.1371/journal.pone.0241032
Vera San Juan, N., Shah, P., Schlief, M., Appleton, R., Nyikavaranda, P., Birken, M., et al. (2021). Service user experiences and views regarding telemental health during the COVID-19 pandemic: A co-produced framework analysis. PLoS One 16:e0257270. doi: 10.1371/journal.pone.0257270
Kaptan, S. K., Dursun, B. O., Knowles, M., Husain, N., and Varese, F. (2021). Group eye movement desensitization and reprocessing interventions in adults and children: A systematic review of randomized and nonrandomized trials. Clin. Psychol. Psychother. 28, 784–806. doi: 10.1002/cpp.2549
Koenig, H. G., Youssef, N. A., Ames, D., Teng, E. J., and Hill, T. D. (2020). Examining the overlap between moral injury and PTSD in US veterans and active-duty military. J. Nerv. Ment. Dis. 208, 7–12. doi: 10.1097/NMD.0000000000001077
Koenig, H. G., Youssef, N. A., and Pearce, M. (2019). Assessment of moral injury in veterans and active-duty military personnel with PTSD: A review. Front. Psych. 10:443. doi: 10.3389/fpsyt.2019.00443
Krampe, H., and Ehrenreich, H. (2012). Therapeutic alliance and multiple psychotherapy in the context of therapist rotation: experiences with OLITA. Neurol. Psychiatry Brain Res. 18, 137–152. doi: 10.1016/j.npbr.2012.05.003
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). The PHQ-9. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lakens, D. (2013). Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front. Psychol. 4:863. doi: 10.3389/fpsyg.2013.00863
Laliotis, D., and Shapiro, F. (2022). “EMDR therapy for trauma-related disorders” in Evidence based treatments for trauma-related psychological disorders. eds. U. Schnyder and M. Cloitre (Springer, Cham: Springer International Publishing), 227–254.
Lasalvia, A., Amaddeo, F., Porru, S., Carta, A., Tardivo, S., Bovo, C., et al. (2021). Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: a cross-sectional study in a tertiary hospital of a highly burdened area of north-East Italy. BMJ Open 11:e045127. doi: 10.1136/bmjopen-2020-045127
Lenferink, L. I. M., Meyerbröker, K., and Boelen, P. A. (2020). PTSD treatment in times of COVID-19: A systematic review of the effects of online EMDR. Psychiatry Res. 293:113438. doi: 10.1016/j.psychres.2020.113438
Litz, B. T., Stein, N., Delaney, E., Lebowitz, L., Nash, W. P., Silva, C., et al. (2009). Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clin. Psychol. Rev. 29, 695–706. doi: 10.1016/j.cpr.2009.07.003
Magruder, K. M., McLaughlin, K. A., and Elmore Borbon, D. L. (2017). Trauma is a public health issue. Eur. J. Psychotraumatol. 8:1375338. doi: 10.1080/20008198.2017.1375338
Marcus, S., Marquis, P., and Sakai, C. (2004). Three-and 6-month follow-up of EMDR treatment of PTSD in an HMO setting. Int. J. Stress. Manag. 11, 195–208. doi: 10.1037/1072-5245.11.3.195
Mattheß, C., Farrell, D., Mattheß, M., Bumke, P., Sodemann, U., and Mattheß, H. (2019). The therapeutic value of trauma stabilization in the treatment of post-traumatic stress disorder – A southeast Asian study. Asian J. Psychiatr. 41, 45–49. doi: 10.1016/j.ajp.2018.09.010
Mattheß, C., Farrell, D., Mattheß, M., Bumke, P., Sodemann, U., and Mattheß, H. (2020). Trauma stabilization as an effective treatment for children with post-traumatic stress problems in South-East Asia. Int. J. Ment. Health Nurs. 29, 725–735. doi: 10.1111/inm.12707
Miguel-Puga, J. A., Cooper-Bribiesca, D., Avelar-Garnica, F. J., Sanchez-Hurtado, L. A., Colin-Martínez, T., Espinosa-Poblano, E., et al. (2021). Burnout, depersonalization, and anxiety contribute to post-traumatic stress in frontline health workers at COVID-19 patient care, a follow-up study. Brain Behav. 11:e02007. doi: 10.1002/brb3.2007
Milosevic, I., Cameron, D. H., Milanovic, M., McCabe, R. E., and Rowa, K. (2022). Face-to-face versus video teleconference group cognitive Behavioral therapy for anxiety and related disorders: A preliminary comparison. Can. J. Psychiatry 67, 391–402. doi: 10.1177/07067437211027319
Morris, H., Hatzikiriakidis, K., Savaglio, M., Dwyer, J., Lewis, C., Miller, R., et al. (2022). Eye movement desensitization and reprocessing for the treatment and early intervention of trauma among first responders: A systematic review. J. Trauma. Stress. 35, 778–790. doi: 10.1002/jts.22792
Nagarajan, R., Krishnamoorthy, Y., Basavarachar, V., and Dakshinamoorthy, R. (2022). Prevalence of post-traumatic stress disorder among survivors of severe COVID-19 infections: A systematic review and meta-analysis. J. Affect. Disord. 299, 52–59. doi: 10.1016/j.jad.2021.11.040
Narayan, A. J., Ippen, C. G., Harris, W. W., and Lieberman, A. F. (2017). Assessing angels in the nursery: A pilot study of childhood memories of benevolent caregiving as protective influences. Infant Ment. Health J. 38, 461–474. doi: 10.1002/imhj.21653
Narayan, A. J., Rivera, L. M., Bernstein, R. E., Harris, W. W., and Lieberman, A. F. (2018). Positive childhood experiences predict less psychopathology and stress in pregnant women with childhood adversity: A pilot study of the benevolent childhood experiences (BCEs) scale. Child Abuse Negl. 78, 19–30. doi: 10.1016/j.chiabu.2017.09.022
Nash, W. P., Marino Carper, T. L., Mills, M. A., Au, T., Goldsmith, A., and Litz, B. T. (2013). Psychometric evaluation of the moral injury events scale. Mil. Med. 178, 646–652. doi: 10.7205/MILMED-D-13-00017
Norman, S. B., Feingold, J. H., Kaye-Kauderer, H., Kaplan, C. A., Hurtado, A., Kachadourian, L., et al. (2021). Moral distress in frontline healthcare workers in the initial epicenter of the COVID-19 pandemic in the United States: relationship to PTSD symptoms, burnout, and psychosocial functioning. Depress. Anxiety 38, 1007–1017. doi: 10.1002/da.23205
Olejnik, S., and Algina, J. (2003). Generalized eta and omega squared statistics: measures of effect size for some common research designs. Psychol. Methods 8, 434–447. doi: 10.1037/1082-989X.8.4.434
Oosterbaan, V., Covers, M. L. V., Bicanic, I. A. E., Huntjens, R. J. C., and de Jongh, A. (2019). Do early interventions prevent PTSD? A systematic review and meta-analysis of the safety and efficacy of early interventions after sexual assault. Eur. J. Psychotraumatol. 10:2932. doi: 10.1080/20008198.2019.1682932
Osorio, A. (2018). Randomized controlled trial on the EMDR integrative group treatment protocol for ongoing traumatic stress with adolescents and young adults patients with cancer. Am. J. Appl. Psychol. 7:50. doi: 10.11648/j.ajap.20180704.11
Ostacoli, L., Carletto, S., Cavallo, M., Baldomir-Gago, P., di Lorenzo, G., Fernandez, I., et al. (2018). Comparison of eye movement desensitization reprocessing and cognitive behavioral therapy as adjunctive treatments for recurrent depression: the European depression EMDR network (EDEN) randomized controlled trial. Front. Psychol. 9:74. doi: 10.3389/fpsyg.2018.00074
Oudshoorn, C. E. M., Frielink, N., Riper, H., and Embregts, P. J. C. M. (2021). Experiences of therapists conducting psychological assessments and video conferencing therapy sessions with people with mild intellectual disabilities during the COVID-19 pandemic. Int. J. Dev. Disab. 10, 1–9. doi: 10.1080/20473869.2021.1967078
Pink, J., Ghomi, M., Smart, T., and Richardson, T. (2022). Effects of EMDR group traumatic episode protocol on burnout within IAPT health care professionals: A feasibility and acceptability study. J. EMDR Pract. Res. 16, 215–227. doi: 10.1891/EMDR-2022-0029
Price, M., van Stolk-Cooke, K., Brier, Z. M. F., and Legrand, A. C. (2018). mHealth solutions for early interventions after trauma: improvements and considerations for assessment and intervention throughout the acute post-trauma period. MHealth 4:22. doi: 10.21037/mhealth.2018.06.03
Pupat, A., Dewailly, A., Guidot, F., Duagani, Y., Kawesa, E., Carriere, R., et al. (2022). Global initiative for stress and trauma treatment—traumatic stress relief training for allied and Para-professionals to treat traumatic stress in underserved populations: A case study. Europ. J. Trauma Dissociation 6:100229. doi: 10.1016/j.ejtd.2021.100229
Puspitasari, A. J., Heredia, D., Coombes, B. J., Geske, J. R., Gentry, M. T., Moore, W. R., et al. (2021). Feasibility and initial outcomes of a group-based teletherapy psychiatric day program for adults with serious mental illness: open, nonrandomized trial in the context of COVID-19. JMIR Mental Health 8:e25542. doi: 10.2196/25542
Rasheed, J., Jamil, A., Hameed, A. A., Aftab, U., Aftab, J., Shah, S. A., et al. (2020). A survey on artificial intelligence approaches in supporting frontline workers and decision makers for the COVID-19 pandemic. Chaos, Solitons Fractals 141:110337. doi: 10.1016/j.chaos.2020.110337
Raudenská, J., Steinerová, V., Javůrková, A., Urits, I., Kaye, A. D., Viswanath, O., et al. (2020). Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 34, 553–560. doi: 10.1016/j.bpa.2020.07.008
Redican, E., Nolan, E., Hyland, P., Cloitre, M., McBride, O., Karatzias, T., et al. (2021). A systematic literature review of factor analytic and mixture models of ICD-11 PTSD and CPTSD using the international trauma questionnaire. J. Anxiety Disord. 79:102381. doi: 10.1016/j.janxdis.2021.102381
Richins, M. T., Gauntlett, L., Tehrani, N., Hesketh, I., Weston, D., Carter, H., et al. (2020). Early post-trauma interventions in organizations: A scoping review. Front. Psychol. 11:1176. doi: 10.3389/fpsyg.2020.01176
Roberts, A. K. P. (2018). The effects of the EMDR group traumatic episode protocol with cancer survivors. J. EMDR Pract. Res. 12, 105–117. doi: 10.1891/1933-3196.12.3.105
Roberts, N. P., Kitchiner, N. J., Kenardy, J., Lewis, C. E., and Bisson, J. I. (2019). Early psychological intervention following recent trauma: A systematic review and meta-analysis. Eur. J. Psychotraumatol. 10:1695486. doi: 10.1080/20008198.2019.1695486
Ruck, S., Bowes, N., and Tehrani, N. (2013). Evaluating trauma debriefing within the UK prison service. J. Forensic Pract. 15, 281–290. doi: 10.1108/JFP-09-2012-0018
Sachdeva, A., Nandini, H., Kumar, V., Chawla, R. K., and Chopra, K. (2021). From stress to stigma – mental health considerations of health care workers involved in COVID19 management. Indian J. Tuberc. 69, 590–595. doi: 10.1016/j.ijtb.2021.09.007
Sasangohar, F., Jones, S. L., Masud, F. N., Vahidy, F. S., and Kash, B. A. (2020). Provider burnout and fatigue during the COVID-19 pandemic: lessons learned from a high-volume intensive care unit. Anesth. Analg. 131, 106–111. doi: 10.1213/ANE.0000000000004866
Shapiro, F. (2017). Eye movement desensitization and reprocessing (EMDR) therapy: Basic principles, protocols, and procedures. Guilford Publications.
Shapiro, E., and Laub, B. (2008). Early EMDR intervention (EEI): A summary, a theoretical model, and the recent traumatic episode protocol (R-TEP). J. EMDR Pract. Res. 2, 79–96. doi: 10.1891/1933-3196.2.2.79
Shklarski, L., Abrams, A., and Bakst, E. (2021a). Navigating changes in the physical and psychological spaces of psychotherapists during Covid-19: when home becomes the office. Pract. Innov. 6, 55–66. doi: 10.1037/pri0000138
Shklarski, L., Abrams, A., and Bakst, E. (2021b). Will we ever again conduct in-person psychotherapy sessions? Factors associated with the decision to provide in-person therapy in the age of COVID-19. J. Contemp. Psychother. 51, 265–272. doi: 10.1007/s10879-021-09492-w
Shreffler, J., Huecker, M., and Petrey, J. (2020). The impact of COVID-19 on healthcare worker wellness: A scoping review. Western. J. Emerg. Med. 21, 1059–1066. doi: 10.5811/westjem.2020.7.48684
Smith, K., Moller, N., Cooper, M., Gabriel, L., Roddy, J., and Sheehy, R. (2022). Video counselling and psychotherapy: A critical commentary on the evidence base. Couns. Psychother. Res. 22, 92–97. doi: 10.1002/capr.12436
Spence, J., Titov, N., Johnston, L., Dear, B. F., Wootton, B., Terides, M., et al. (2013). Internet-delivered eye movement desensitization and reprocessing (iEMDR): an open trial. F1000Research 2:79. doi: 10.12688/f1000research.2-79.v2
Sritharan, J., Jegathesan, T., Vimaleswaran, D., and Sritharan, A. (2020). Mental health concerns of frontline workers during the COVID-19 pandemic: A scoping review. Global J. Health Sci. 12:89. doi: 10.5539/gjhs.v12n11p89
Tarquinio, C., Brennstuhl, M.-J., Rydberg, J. A., Bassan, F., Peter, L., Tarquinio, C. L., et al. (2021). EMDR in telemental health counseling for healthcare workers caring for COVID-19 patients: A pilot study. Issues Ment. Health Nurs. 42, 3–14. doi: 10.1080/01612840.2020.1818014
Turgoose, D., Ashwick, R., and Murphy, D. (2018). Systematic review of lessons learned from delivering tele-therapy to veterans with post-traumatic stress disorder. J. Telemed. Telecare 24, 575–585. doi: 10.1177/1357633X17730443
van Minnen, A., and Hendriks, L., Kleine, R. de, Hendriks, G.-J., Verhagen, M., and de Jongh, A. (2018). Therapist rotation: a novel approach for implementation of trauma-focused treatment in post-traumatic stress disorder. Eur. J. Psychotraumatol., 9,:1492836. doi:doi: 10.1080/20008198.2018.1492836
Watson, P. (2022). Stress, PTSD, and COVID-19: the utility of disaster mental health interventions during the COVID-19 pandemic. Curr. Treat. Opt. Psychiatry 9, 14–40. doi: 10.1007/s40501-021-00253-z
Watts, S., Marchand, A., Bouchard, S., Gosselin, P., Langlois, F., Belleville, G., et al. (2020). Telepsychotherapy for generalized anxiety disorder: impact on the working alliance. J. Psychother. Integr. 30, 208–225. doi: 10.1037/int0000223
Weiss, D. S., and Marmar, C. R. (1997). “The impact of event scale—revised,’’ in Assessing psychological trauma and post traumatic stress disorder: a handbook for practitioners. eds. P. Wilson and T. Keane (New York: Guilford Press), 399–411.
Wild, J., McKinnon, A., Wilkins, A., and Browne, H. (2022). Post-traumatic stress disorder and major depression among frontline healthcare staff working during the COVID-19 pandemic. Br. J. Clin. Psychol. 61, 859–866. doi: 10.1111/bjc.12340
Wild, J., Warnock-Parkes, E., Grey, N., Stott, R., Wiedemann, M., Canvin, L., et al. (2016). Internet-delivered cognitive therapy for PTSD: a development pilot series. Eur. J. Psychotraumatol. 7:1019. doi: 10.3402/ejpt.v7.31019
Williamson, V., Murphy, D., and Greenberg, N. (2020). COVID-19 and experiences of moral injury in front-line key workers. Occup. Med. 70, 317–319. doi: 10.1093/occmed/kqaa052
Wilson, G., Farrell, D., Barron, I., Hutchins, J., Whybrow, D., and Kiernan, M. D. (2018). The use of eye-movement desensitization reprocessing (EMDR) therapy in treating post-traumatic stress disorder-A systematic narrative review. Front. Psychol. 9:923. doi: 10.3389/fpsyg.2018.00923
Wind, T. R., Rijkeboer, M., Andersson, G., and Riper, H. (2020). The COVID-19 pandemic: the ‘black swan’ for mental health care and a turning point for e-health. Internet Interv. 20:100317. doi: 10.1016/j.invent.2020.100317
Wippich, A., Howatson, G., Allen-Baker, G., Farrell, D., Kiernan, M., and Scott-Bell, A. (2023). Eye movement desensitization reprocessing as a treatment for PTSD in conflict-affected areas. Psychol. Trauma Theory Res. Pract. Policy. 1–7. doi: 10.1037/tra0001430
Womersley, G., and Arikut-Treece, Y. (2019). Collective trauma among displaced populations in northern Iraq: A case study evaluating the therapeutic interventions of the free Yezidi foundation. Intervention 17:18. doi: 10.4103/INTV.INTV_56_18
Yunitri, N., Chu, H., Kang, X. L., Jen, H.-J., Pien, L.-C., Tsai, H.-T., et al. (2022). Global prevalence and associated risk factors of posttraumatic stress disorder during COVID-19 pandemic: A meta-analysis. Int. J. Nurs. Stud. 126:104136. doi: 10.1016/j.ijnurstu.2021.104136
Yurtsever, A., Konuk, E., Akyüz, T., Zat, Z., Tükel, F., Çetinkaya, M., et al. (2018). An eye movement desensitization and reprocessing (EMDR) group intervention for Syrian refugees with post-traumatic stress symptoms: results of a randomized controlled trial. Front. Psychol. 9:493. doi: 10.3389/fpsyg.2018.00493
Keywords: EMDR early intervention, group treatment, COVID-19, emergency and frontline workers, therapist rotation, posttraumatic stress disorder, moral injury
Citation: Farrell D, Moran J, Zat Z, Miller PW, Knibbs L, Papanikolopoulos P, Prattos T, McGowan I, McLaughlin D, Barron I, Mattheß C and Kiernan MD (2023) Group early intervention eye movement desensitization and reprocessing therapy as a video-conference psychotherapy with frontline/emergency workers in response to the COVID-19 pandemic in the treatment of post-traumatic stress disorder and moral injury—An RCT study. Front. Psychol. 14:1129912. doi: 10.3389/fpsyg.2023.1129912
Edited by:
Francisco Sampaio, Escola Superior de Enfermagem do Porto, PortugalReviewed by:
Selvira Draganovic, International University of Sarajevo, Bosnia and HerzegovinaWilis Srisayekti, Padjadjaran University, Indonesia
Yvette Hendrix, Onze Lieve Vrouwe Gasthuis (OLVG), Netherlands
Malindi Van Der Mheen, Amsterdam University Medical Center, Netherlands
Copyright © 2023 Farrell, Moran, Zat, Miller, Knibbs, Papanikolopoulos, Prattos, McGowan, McLaughlin, Barron, Mattheß and Kiernan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Derek Farrell, ZC5mYXJyZWxsQHdvcmMuYWMudWs=