 Yi Xuan Ong1
Yi Xuan Ong1 Hye Kyung Kim1*
Hye Kyung Kim1* Benjamin O. Pelzer1
Benjamin O. Pelzer1 Ying Ying Tan2Wee Ping Lim2Annabelle Kai Lin Chua2Bei Yi Koh2
Ying Ying Tan2Wee Ping Lim2Annabelle Kai Lin Chua2Bei Yi Koh2- 1Wee Kim Wee School of Communication and Information, Nanyang Technological University, Singapore, Singapore
- 2DSO National Laboratories, Singapore, Singapore
In a public health crisis, communication plays a vital role in making sure policies and recommendations from the government level get disseminated accurately to its people and is only considered as effective when the public accepts, supports, complies to, and engages in policies or behaves as per governments’ recommendations. Adopting the multivariate audience segmentation strategy for health communication, this study uses a data-driven analytical method to (1) identify audience segments of public health crisis communication in Singapore based on knowledge, risk perception, emotional responses, and preventive behaviors; and (2) characterize each audience segment according to demographic factors, personality traits, information processing styles, and health information preferences. Results (N = 2033) from a web-based questionnaire executed in August 2021 have identified three audience segments: the less-concerned (n = 650), the risk-anxious (n = 142), and the risk-majority (n = 1,241). This study offers insights to how audiences of public health crisis communication perceive, process, and respond to information directed to them during the pandemic, thereby informing policy makers to tailor more targeted public health communication interventions in promoting positive attitude and behavior change.
1. Introduction
Since February 2020, the outbreak of COVID-19 has escalated to a global pandemic, with over 500 million cases and 6.28 million deaths to date (World Health Organization, 2022). Due to the nature of transmission and high virality of COVID-19, international health organizations and governments have rolled out preventive measures that include the closure of international and regional borders, lockdowns, and self-isolation. At the individual level, some governments have mandated the adoption of preventive behaviors such as handwashing, mask-wearing, and social distancing to maintain personal hygiene and reduce virus transmission. In such public health crises, communication plays a vital role in making sure policies and recommendations from the governmental level get disseminated accurately to the public. However, dissemination alone does not guarantee that the governments’ recommendations will be followed: Government health advisories are effective only when the public accepts, supports, and complies with the recommendations (Rogers and Storey, 1987; Slater, 1996; Warren and Lofstedt, 2021). Effective health communication should also consider how the public perceives, processes, and responds to information directed in these public health campaigns (Maibach et al., 1996; Slater, 1996). One important tool in understanding the public is audience segmentation (Slater, 1996).
Audience segmentation is the process of grouping audiences into smaller subgroups based on a set of variables that is indicative of an outcome (Slater, 1996). Audience segmentation is a useful communication strategy during a pandemic, as it helps to identify potential problems of current communication efforts for specific audience segments and offers insights to tailor public health communication for these groups (Maibach et al., 1996; Slater, 1996; Maibach et al., 2011). In this vein, the current study aims to capture and identify meaningful clusters of individuals who share similarities in risk attitudes, affective responses, and preventive behaviors during COVID-19. The clusters identified will then be characterized based on demographic and psychological traits, as well as health information preferences and attribution judgments relevant to COVID-19.
While prior research often used a variable-centered approach, which assumes a homogeneous sample, the current study instead adopts a person-centered approach to audience segmentation, using a more data-driven analytical method. This approach further employs Slater’s (1996) multivariate strategy, which enables a selection of variables from multiple theoretical frameworks as determinants of audience segmentation. The results of this study make it possible to uncover the demographic, psychographic, and behavioral characteristics of various audience segments in a population and offer useful insights into tailoring important health information to certain audience segments in order to improve the effectiveness of pandemic communication.
This study takes place in Singapore, a member of G20 with one of the world’s highest vaccination rates (91.4%; Reuters, 2022). Singapore was highly complimented for its crisis response to COVID-19, exemplified with high public trust and compliance to government-recommended preventive measures during the pandemic (Wong and Jensen, 2020; Yeo et al., 2022). Considering the above background, this study has three major objectives. First, this study attempts to identify audience segments on COVID-19 prevention based on Slater’s (1996) multivariate strategy. Specifically, using Latent Profile Analysis (LPA), we employ perceived knowledge, risk perception (inclusive of perceived severity and perceived vulnerability), perceived preventive efficacy, emotional responses, and intention to engage in preventive behaviors as key determinants of audience segments on COVID-19 prevention. Second, this study aims to characterize each identified audience segment regarding its demographic profiles (e.g., age, gender, race), personality traits, and information-seeking and processing styles. Lastly, this study will uncover differences between audience segments on health information preferences and attributions of responsibility in reducing transmission, in the specific context of COVID-19. Results of this study would bring insights to practitioners for tailoring health information to audiences’ characteristics, thus enhancing the effectiveness of communication efforts during a pandemic.
2. Literature review
The following review, divided into two sections, offers a critical understanding of the associations between the factors and justifies their use in this audience segmentation study. The first section reviews the overall strategy of audience segmentation and the theoretical explanation of the determinants used for audience segmentation. The second section gives an overview of the two different types of variables associated with audience profile characteristics. The first type focuses on demographic, personality, and behavioral characteristics associated with the audience segmentation determinants. The second type of variables are those that change during a pandemic to understand differences in health information preferences and inform future public health communication strategies.
2.1. Audience segmentation strategy—A person-centered approach
Audience segmentation involves the breakdown of a population into smaller clusters of audiences with similar patterns (for instance, in personality, media use habits, or cognitive styles) to achieve positive attitudinal and behavioral change via tailored communication efforts (Rogers and Storey, 1987; Grunig, 1989; Slater, 1996). Slater (1996) addresses two major approaches in audience segmentation: (a) the variable-centered approach based on theoretical typologies (Grunig, 1989), and (b) multivariate classification segmentation (one of the person-centered approaches; Maibach et al., 1996). Most extant studies take a variable-centered approach, examining how variables based on a framework (e.g., Risk Perception Attitude (RPA) Framework) relate to demographic factors to uncover segments within the sample (Rimal and Real, 2003; Rimal et al., 2009; Duong, 2022). However, this approach limits meaningful segmentation by treating the sample as homogenous on all other variables not used for segmentation (Slater, 1996; Kleitman et al., 2021). In contrast, the multivariate classification segmentation strategy approach, by acknowledging heterogeneity of all other variables within the sample, enables all variables to be used for a more rigorous and holistic identification of audience segments.
The person-centered approach has been employed in recent studies to examine individual differences on the impacts of COVID-19. For example, Ahmed et al. (2021) segmented the sample population to examine how people adapt to the impacts of COVID-19 based on their stress levels, sleep quality, and adoption of coping activities during a lockdown. Kleitman et al. (2021) also grouped the audience based on their risk attitudes and compliance with preventive behaviors during COVID-19, identifying the characteristics of each audience segment to inform future communication strategies. Similarly, Smith et al. (2021) clustered the population into five classes based on the audience’s intentions to engage in recommended behaviors during the COVID-19 pandemic to identify audiences for targeted messaging. These studies demonstrated the potential utility of a person-centered approach in audience segmentation for offering practical insights into effectively communicating with various segments during a pandemic.
Building on prior works, this study employs a person-centered method to identify subgroups based on shared target behaviors (Smith, 2017). Specifically, this study adopts Slater’s (1996) multivariate classification segmentation strategy, using perceived knowledge, risk perception, perceived preventive efficacy, emotional responses, and behaviors related to a given health domain as determinants of audience segmentation. In doing so, we advance prior literature by leveraging on the audience segmentation to capture differences in health information preferences and attributions of responsibility during the pandemic.
The adoption of preventive behaviors is the key communicative objective during the COVID-19 pandemic. Consequently, this study considered engagement in preventive behavior as a major predictor of audience segmentation. In addition, guided by theory and empirical evidence, we included various psychological factors (i.e., risk perception, perceived knowledge, perceived preventive efficacy, and emotional responses) that are predictive of protective behaviors.
Theoretical frameworks, such as the Health Belief Model (HBM) (Carpenter, 2010) and the RPA Framework (Rimal and Real, 2003), highlight the important roles of risk perception (i.e., perceived vulnerability and perceived severity) and perceived preventive efficacy in predicting preventive behaviors. When individuals have a higher risk perception and think they can engage in preventive behaviors, they are more likely to engage in the behaviors to reduce the risk. Beyond the analytic assessment of risk, affective responses also prominently impact how people interpret the risk at hand (risk as feeling, Slovic et al., 2013). Such emotional responses are theorized to influence individuals’ information processing and behavioral actions (Izard, 1993).
Empirically, emotional responses and risk perceptions have been found to predict positive behavioral changes and adherence to government-recommended measures (Weinstein, 1988; Brug et al., 2004; Leung et al., 2004). Kim and Niederdeppe (2013) found that both positive and negative emotional responses were associated with the respondents’ willingness to seek health-related information during the H1N1 pandemic. In the COVID-19 context, Anaki and Sergay (2021) found evidence that perceived severity, perceived susceptibility to COVID-19, and emotional responses predicted preventive behaviors. Kleitman et al. (2021) included risk attitudes and emotional responses toward COVID-19 to identify compliant and non-compliant audience segments to government-recommended measures.
Guided by the HBM and the Social Cognitive Theory (Bandura, 2000), prior works have identified perceived knowledge as a key antecedent of health behavioral intent (Rock et al., 2005; Zhang et al., 2015). As individuals are exposed to certain health information, they tend to retain the information for future evaluation or reference for producing protective behavior when sufficiently motivated (Bandura, 2000; Zhang et al., 2015). For example, Zhang et al. (2015) found that higher perceived knowledge attained from media exposure is associated with higher adoption of preventive behaviors during the H1N1 influenza outbreak. Moreover, the same study demonstrated that media exposure to pandemic information stimulates negative emotions and heightens the perceived knowledge of audiences, resulting in greater adoption of preventive measures (Zhang et al., 2015).
With the theoretical support and empirical evidence of existing literature, this study uses perceived severity, perceived preventive efficacy, and emotional responses experienced in pandemic situations as determinants of audience segments. Moreover, as an extension to Kleitman’s et al. (2021) segmentation study, we take a more holistic approach by including perceived knowledge of the virus (Zhang et al., 2015) and perceived vulnerability to COVID-19 (Duncan et al., 2009) to segment the audiences of COVID-19 communication.
2.2. Audience segment characteristics
2.2.1. Demographic traits
Meta-analyzes have highlighted gender and age as key factors directly associated with the adoption of preventive behaviors during pandemics (Bish and Michie, 2010). Specifically, women and older people tend to have greater risk perceptions and thus are more likely to engage in preventive behaviors (Bish and Michie, 2010). However, this meta-analysis did not provide any conclusive results on the association between ethnicity and the adoption of preventive behaviors (Bish and Michie, 2010). Likewise, international surveys have examined various demographic factors to elucidate group differences in risk perceptions related to infectious diseases (de Zwart et al., 2007, 2009). These studies suggested country, age groups, and gender as significant factors that associate with risk perception differences. However, there was still ambiguity from prior works investigating how these demographic factors are linked to preventive behaviors and risk perceptions (de Zwart et al., 2007, 2009; Bish and Michie, 2010). Thus, this study includes race, age, and gender to clarify their associations with audience segments grouped based on preventive behaviors and risk perceptions.
2.2.2. Personality traits
Recent research on COVID-19 has begun to examine how individuals react to pandemic management measures differently depending on their psychological characteristics (Aschwanden et al., 2021). Personality traits can explain how a person thinks, perceives information, feels emotions, and behaves (McCrae and Costa, 2006), including during a pandemic (Aschwanden et al., 2021). In particular, the Big Five personality traits (openness, conscientiousness, extroversion, agreeableness, and neuroticism), introduced by McCrae and John (1992), have been suggested to be associated with health behaviors. For example, individuals who score high in conscientiousness tend to follow rules and regulations, have more self-discipline, and are more likely to adopt more preventive measures (Bogg and Roberts, 2004; Aschwanden et al., 2021; Blagov, 2021). Another trait, neuroticism, reflects the tendency to feel anxious, worried, fearful, or angry in a situation (McCrae and John, 1992). People who score higher in neuroticism tend to experience more negative emotions during the pandemic (Kroencke et al., 2020; Aschwanden et al., 2021). Individuals scoring high in agreeableness show more compliance with rules and regulations (John and Srivastava, 1999; Blagov, 2021; Kleitman et al., 2021). Similarly, individuals scoring high in openness tend to be more resilient, adaptive, and open to the policies set by the government (Aschwanden et al., 2021; Kleitman et al., 2021). Extroverted people tend to be more outgoing, and thus taking preventive measures such as self-isolation and social distancing may be more challenging for them (Aschwanden et al., 2021; Kleitman et al., 2021).
While existing studies include all five personality traits in their analyzes, most of them tend to focus on conscientiousness and neuroticism as these two traits were more significantly associated with adoption of preventive measures (Kroencke et al., 2020; Aschwanden et al., 2021; Blagov, 2021). However, there are inconsistencies in the relationship of each Big Five personality trait with preventive measure adoption or COVID-19-related attitudes. For example, Kleitman et al. (2021) found that conscientiousness and neuroticism did not show any significant differences between compliant and non-compliant groups, differing from previous studies. Likewise, Kleitman et al. (2021) found that non-compliant respondents tended to be more extroverted, in contrast to earlier studies which found that extraversion is associated with taking more precautions (Aschwanden et al., 2021; Blagov, 2021). With inconsistent results from prior works, this study will capture all five traits to clarify and extend findings in relation to personality differences in risk perceptions and preventive behaviors (Sutin and Terracciano, 2016).
2.2.3. Information processing styles—Need for cognition and need for affect
Need for Affect (NFA; Maio and Esses, 2001) and Need for Cognition (NFC; Petty and Cacioppo, 1982; Petty et al., 2009) are suggested to differ across individuals and are associated with the effectiveness of messages in persuasive communication (Haddock et al., 2008; Zhang et al., 2021). NFC and NFA, respectively, can indicate the cognitive and affective orientations which an individual is motivated to engage in when s/he is exposed to a message (Petty and Cacioppo, 1982; Haddock et al., 2008; Zhang et al., 2021). NFA looks at an individual’s tendency to engage in the affective process, relying upon affective information in attitude formation and behavioral intention (Haddock et al., 2008). Individuals with higher levels of NFA tend to be better persuaded when they engage with affect-based (emotionally charged) messaging. In contrast, NFC looks at an individual’s tendency to engage in effortful thinking. Individuals with higher levels of NFC are more likely to be persuaded when exposed to or engaged in cognition-based (informative, factual) messages (Haddock et al., 2008; Petty et al., 2009). Because these information processing styles are closely related to the type of persuasive messaging, it is important to consider how NFA and NFC differ between audience segments and their roles in characterizing the identified segments.
2.2.4. Health information seeking and information preferences during the COVID-19 pandemic
In the face of an ongoing COVID-19 pandemic, communication plays an integral role in managing the outbreak with preventive measures. Individuals often seek information on risks, preventive measures, and symptoms during a pandemic. Health information seeking is affected by various factors including health perceptions, health status, and demographic background (Lambert and Loiselle, 2007; Jacobs et al., 2017; Rayani et al., 2021). Existing studies have shown that engaging in health information seeking can help individuals feel more assured and be more active in adopting preventive measures (Shieh et al., 2010; Rayani et al., 2021). In prior research, time spent on seeking information and the number of pages of health information browsed were associated with higher levels of perceived susceptibility, fear, and anxiety (So et al., 2019). Kleitman et al. (2021) identified that compliant and non-compliant audience segments vary in their preferred information sources, frequency of information seeking, and the tendency to fact-check and compliance. Riding on existing literature, the current study seeks to better understand how the identified audience segments vary in health information-seeking patterns (frequency, time spent, preferred platforms, and intensity) during the pandemic.
Segmentation is the essence of developing a “consumer-oriented” communication (Lefebvre et al., 1995; Maibach et al., 1996, p. 262) that offers insights to policymakers in creating more persuasive messages by understanding their health information-seeking patterns. While current literature examined the health information-seeking patterns and source preferences (Kleitman et al., 2021), there is a research gap on audiences’ content preferences (e.g., topics, content types) during a pandemic, and how such preferences would be associated with audiences’ risk attitudes and behaviors (Avery, 2010; Park et al., 2019). During a pandemic that has persisted for more than 2 years, excessive exposure to health information tends to cause fatigue in the audiences, negatively affecting their attitudes and intention to adopt preventive measures (Ball and Wozniak, 2021). Thus, this study uncovers perceived importance and preferences for different types of COVID-19 information of each audience segment, providing insights for more targeted communication and preventing information fatigue.
2.2.5. Attributions of responsibility
The Attribution Theory (Weiner, 1986) posits that people search for the causes of a negative and unexpected event to make an attribution judgment (Weiner, 1986). An individual or an entity would search for relevant information to evaluate the level of responsibility the stakeholder has in an event or a crisis (Fiske and Taylor, 1991). The attribution of responsibility can be also influenced by various factors, such as the preference of information sources (Park and Lee, 2016), risk perceptions and crisis emotions (Kim and Niederdeppe, 2013), and political orientation (Zhang et al., 2021). The inclusion of this variable allows the examination of how segments of the audience attribute responsibility to different stakeholders (citizens, government, healthcare workers, schools, and workplaces) in reducing transmission during the COVID-19 pandemic. Understanding how an individual attributes responsibility during COVID-19 can inform policymakers on how to develop favorable responses and manage public opinion on the crisis (Coombs, 2016).
3. Methods
3.1. Sampling and data collection
This study was conceptualized and executed in Singapore, during the second global wave of the pandemic, where the Delta variant was the main variant of infection in Singapore. Participants were recruited with panels managed by local market research firms. We employed quota sampling according to Singapore’s population census in 2020 (Singapore Department of Statistics, 2021) to ensure demographic representativeness of the sample in terms of gender, age, and ethnicity. Only Singaporeans citizens aged 18 and above were eligible to take part in the study. The final sample consisted of 2,033 participants, including 1,038 (51.1%) females and 995 (48.9%) males. The sample consists of 266 (13.1%) respondents in the age group of 18–24, 361 (17.8%) in the 25–34 age group, 399 (19.6%) aged 35–44, 409 (20.1%) respondents aged 45–54, 379 (18.6%) from the 55–64 age group, and 219 (10.7%) respondents who are aged 65 and above. The sample’s racial distribution is representative of Singapore’s racial distribution, with 1,509 (74.2%) Chinese, 268 (13.2%) Malays, 197 (9.7%) Indians, and 59 (2.9%) respondents who identified as Eurasian or other ethnic groups. Participants recruited from the local market research agency were compensated at the discretion of the market research agency.
3.2. Measures
3.2.1. Determinants of audience segmentation
We assessed the following nine measures as determinants of the audience segmentation: preventive behaviors (nine items, Caress et al., 2010; 4-point scale, 1 = never to 4 = always, e.g., mask-wearing, handwashing, social distancing, M = 30.57, SD = 3.98); perceived knowledge (four items, Zhang et al., 2015; 7-point Likert scale, 1 = strong disagree, 7 = strongly agree, e.g., “I am knowledgeable about COVID-19.”; M = 5.21, SD = 1.01); perceived severity (three items, Rimal and Real, 2003; 7-point Likert scale, 1 = strong disagree, 7 = strongly agree, e.g., “COVID-19 is a deadly disease,” M = 5.25, SD = 1.31); perceived preventive efficacy (two items, Rimal and Real, 2003; 7-point Likert scale, 1 = strong disagree, 7 = strongly agree, e.g., “I can prevent myself from contracting COVID-19,” M = 5.12, SD = 1.31); perceived vulnerability (one item, Duncan et al., 2009; 5-point scale, 1 = extremely unlikely, 5 = extremely likely, “If you do not take any preventive actions against COVID-19, how likely do you think you may contract the virus within 3 months?”); emotional responses (nine items, Izard, 1977; Fredrickson et al., 2003; 5-point scale, 1 = never, 5 = all the time, e.g., “grateful” (four discrete positive emotions, M = 3.67, SD = 0.80), “anxious” (four discrete negative emotions, M = 3.05, SD = 0.95), and “sympathy,” M = 3.80, SD = 0.96). Responses from each variable were averaged to form their respective score.
3.2.2. Characteristics of audience segments
3.2.2.1. Demographic and personality traits
In addition to demographic traits such as age, gender, and race, we measured the Big Five personality traits and need for cognition and affect. Using the full 50-item scale of the Big Five Personality Traits (Goldberg, 1992), participants were asked to rate the extent to which they agree with each statement measuring their openness to experience, conscientiousness, extraversion, agreeableness, and neuroticism, on a scale from 1 (disagree) to 5 (agree). Responses from each variable were averaged to form its respective score.
3.2.2.2. Information processing styles
Using the ten-item measurement derived from Cacioppo et al. (1984), respondents indicated the extent of their need for cognition on a scale of −3 (strongly disagree) to 3 (strongly agree). We measured the need for affect with a ten-item scale derived from Maio and Esses (2001), for which respondents needed to indicate how similar the person in each statement is to the respondent from 1 (not like me at all) to 6 (very much like me). Responses from each variable were averaged to form its respective score.
3.2.2.3. Health information seeking
From a selection of 15 platforms provided (Majid and Rahmat, 2013), we asked the respondents to rank their top three preferred platforms they use when they want to find out health information. Based on their top three preferences, we asked the respondents to indicate the frequency of use for health information search in the past week on a 4-point scale (1 = never, 4 = often) and the duration spent in a day on average for searching health-related information on a 6-point scale (1 = less than 10 min, 6 = more than 3 h) (Ayers and Kronenfeld, 2007). Similarly, the intensity of the top three platform use was measured on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree) with four items derived from Ellison et al. (2007) (e.g., “This platform has become part of my daily routine”). Responses from each variable were averaged to form the respective scores.
3.2.2.4. Health information preferences
There are three variables measured for health information preferences. First, we asked the respondents to rank five out of 17 content types found in health news coverage in order of importance from 1 (most important) to 5 (least important). The items were derived from Majid and Rahmat (2013) and Wong and Sam (2010). Second, on a scale from 1 (most likely) to 6 (least likely), we asked the respondents to rate their likelihood of reading about news reporting from a selection of six news frame categories derived from Shih et al. (2008). Lastly, we derived nine news content types from Quandt et al. (2020) and asked the respondents to rank the top five topics in order of preference, with 1 being the most liked topic.
3.2.2.5. Attribution of responsibility
We derived the scale for attribution of responsibility from Kim and Niederdeppe (2013). The respondents were asked to indicate on a scale from 1 (not at all responsible) to 7 (totally responsible), the level of responsibility each of the five actors should bear for reducing the transmission of COVID-19 among the population (e.g., government, citizens, schools, healthcare workers, and workplaces).
3.3. Statistical analysis
A total of three analytic steps are followed to achieve the three research objectives. First, the Latent Profile Analysis (LPA), a method of the person-centered approach, is used to identify potential audience segments of individuals who share similar patterns of risk perception, perceived knowledge, perceived preventive efficacy, emotional responses, and preventive behaviors during COVID-19. To enable direct comparisons, variables were standardized before executing LPA with mclust on statistical software package Rstudio (Scrucca et al., 2016). The LPA classified the observations in a dataset into a set of profiles based on their homogenous characteristics across the set of estimated values of the determinants. The results of LPA offered a systematic grouping of the units of analysis based on the clustering of observations using standardized means. This data-driven approach allows researchers to assume heterogeneity within the sample while achieving conceptual validity with the use of widely explored variables in risk and health communication research as predictors of the audience profiles. Second, to characterize and examine differences between the identified audience segments in demographic factors, personality traits, information consumption, and information processing style, crosstab analysis with Chi-square tests were performed on categorical variables. We also performed a series of ANOVA tests, with Bonferroni post-hoc tests, on ordinal and continuous variables. Finally, to investigate the attribution of responsibility and health information preferences of different audience segments, a series of ANOVA tests were performed. The statistical software package IBM SPSS (Statistical Package for Social Sciences) V23.0 was used for the later analyzes testing for profile differences.
4. Results
4.1. Latent profile analysis
4.1.1. Model selection
LPA was performed for 2–6 class solutions, with 1 class as the default. Table 1 illustrates the model fit statistics and the proportion of class membership of 2–6 class solutions. To select the number of classes, this study inspected the Bayesian Information Criterion (BIC), the Integrated Completed Likelihood Criterion (ICL), and the Bootstrap Likelihood Ratio Test (BRLT), which is assessed based on the value of p associated with the log of this likelihood ratio (Nylund et al., 2007; Achterhof et al., 2019). Since the BRLT p-values are all less than 0.001 in all class solutions, BIC and ICL values were inspected for class selection. The BIC and log-likelihood values illustrated the trend that solutions with higher number of classes proved better model fit, with the 5-class solution having the greatest BIC value (Achterhof et al., 2019; Wardenaar, 2021). However, based on the ICL value, which penalizes solutions with classification uncertainty, the 3-class solution (bolded in Table 1) performed the best (Biernacki et al., 2000; Bertoletti et al., 2015).
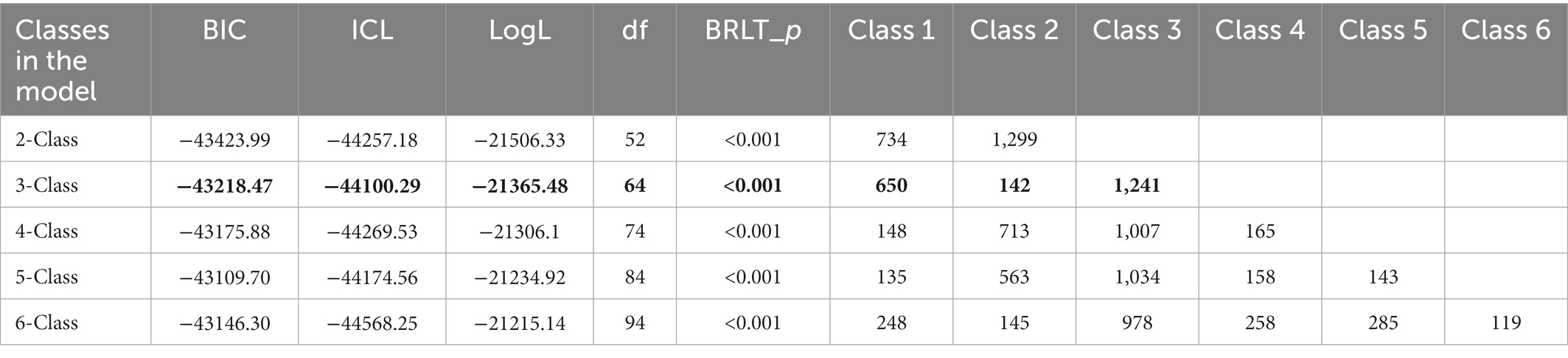
Table 1. Latent profile analysis model fit statistics and class membership.
Figure 1 presents the audience segmentation based on standardized mean scores for each of the three classes on the eight variables included in LPA. We confirmed that the three classes were significantly different from each other in all eight determinant variables using one-way ANOVA with Bonferroni post-hoc tests. Inspired by the RPA framework which posits four different groups of audiences based on their risk perception and efficacy beliefs to act on certain health-related actions (Rimal and Real, 2003), this study names the respective class based on its scores on the key determinants. Based on the 3-class profile selected, Class 1 (n = 650), consisting of 32% of the sample, is profiled to least engage in preventive behavior and scored the lowest for risk perceptions and emotional responses. They have the lowest mean scores of all the predictor measures related to risk perception and preventive behavior during COVID-19. Therefore, this group appeared to be less-concerned about COVID-19, having a lower likelihood to engage in preventive measures such as washing hands, wearing masks, and social distancing. They also appeared to feel positive and negative emotions less often as compared to other classes.
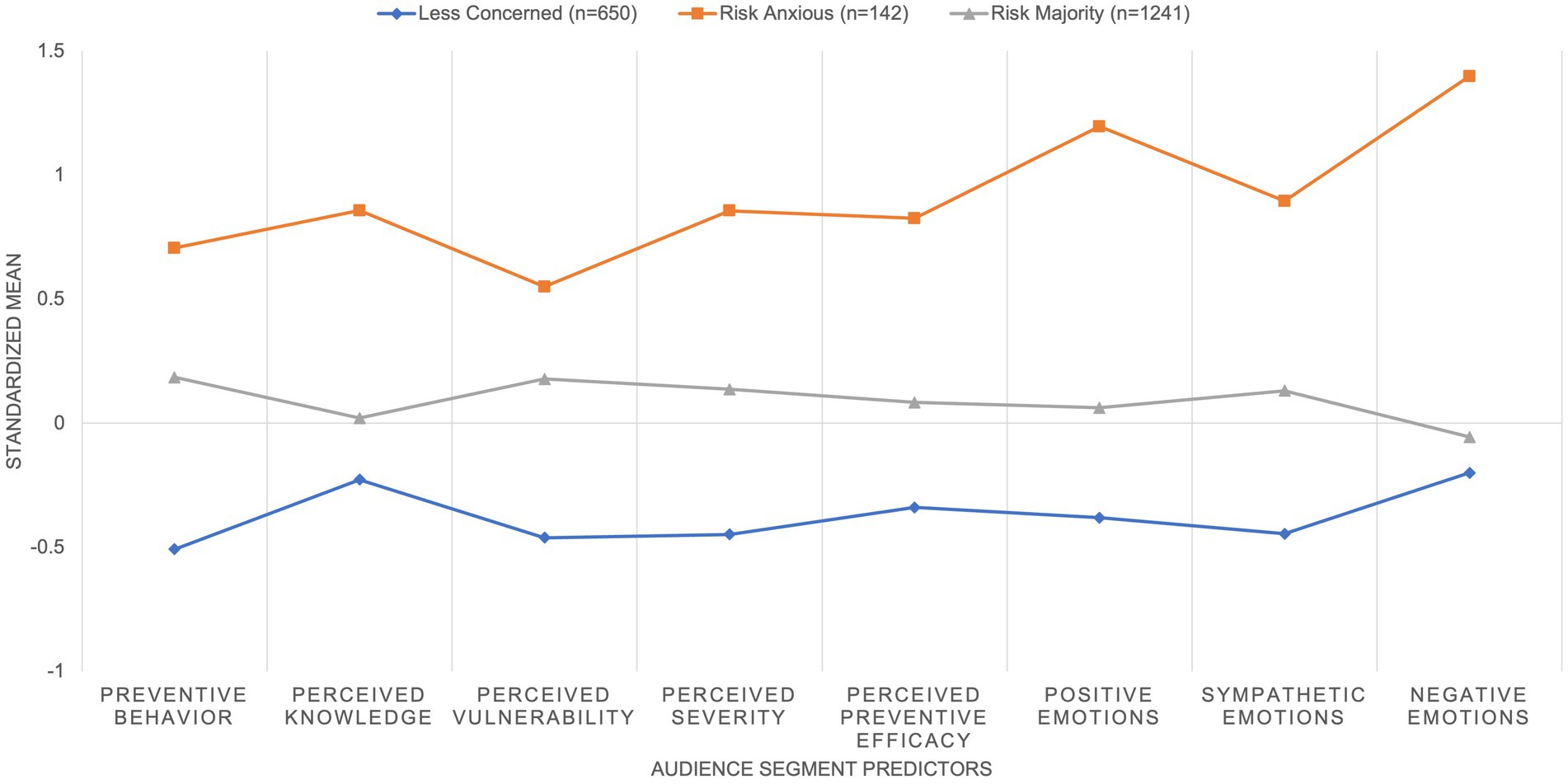
Figure 1. 3-class solution from LPA on audience segmentation.
Class 2 consists of the majority, with 61% of the sample (n = 1,241). Class 2 members are respondents who scored around the mean of determining variables, scoring only slightly higher than Class 1 members on perceived subjective knowledge on COVID-19, and the tendency to feel negative emotions during the COVID-19 pandemic. Class 2 members appeared to engage in preventive measures more actively than Class 1 members and perceived that they would be more likely to contract COVID-19 if they do not take any preventative measures, as compared to Class 1 members. However, they scored lower than Class 3 in the mean scores of all predictor variables. With Class 2 having mean scores that hover near the mean scores of all the measures used for predicting profiles in the LPA, this class is labeled as the risk-majority.
Class 3 (n = 142), consisting of 7% of the sample, is the group that equips itself with knowledge, scoring the highest out of the three classes in the mean scores of risk perception and preventive behaviors. They tend to feel crisis emotions (both positive and negative) more often during the pandemic. Thus, they are labeled as risk-anxious toward COVID-19.
4.2. Results for audience segment characteristics
Differences are observed between the identified audience segments in Age, Gender, and Race (Table 2). The risk-majority and the risk-anxious have a higher proportion of the female audience, following the gender distribution of the overall sample. The less-concerned profile differs from the other two audience segments with a higher proportion of male audience (53.7%) (male risk-majority = 46.3%, male risk-anxious = 48.6%), and the overall sample (48.8%). Looking at the audience in each age group, all audience segments generally follow the age distribution of the overall sample. The risk-anxious profile has a significantly lower proportion of the younger population (respondents in age groups 18–24 and 24–34) and a higher proportion of respondents aged between 55 and 74, who tend to face greater vulnerability against COVID-19 and perceive COVID-19 to be more severe, as compared to other classes and the overall sample. While the risk-majority members’ age profile follows that of the overall sample, the less-concerned members appear to have a higher proportion of respondents aged 25–34 as compared to members of the other segments and the overall sample. On the racial distribution of profiles, all audience segments show similar racial distribution as the overall sample, which is representative of Singapore’s racial distribution. However, the risk-anxious racial distribution differs slightly from the general racial distribution, with only 54.2% Chinese, 26.1% Malays, and 19.7% of Indian and other ethnic groups (e.g., Eurasian, Filipinos).
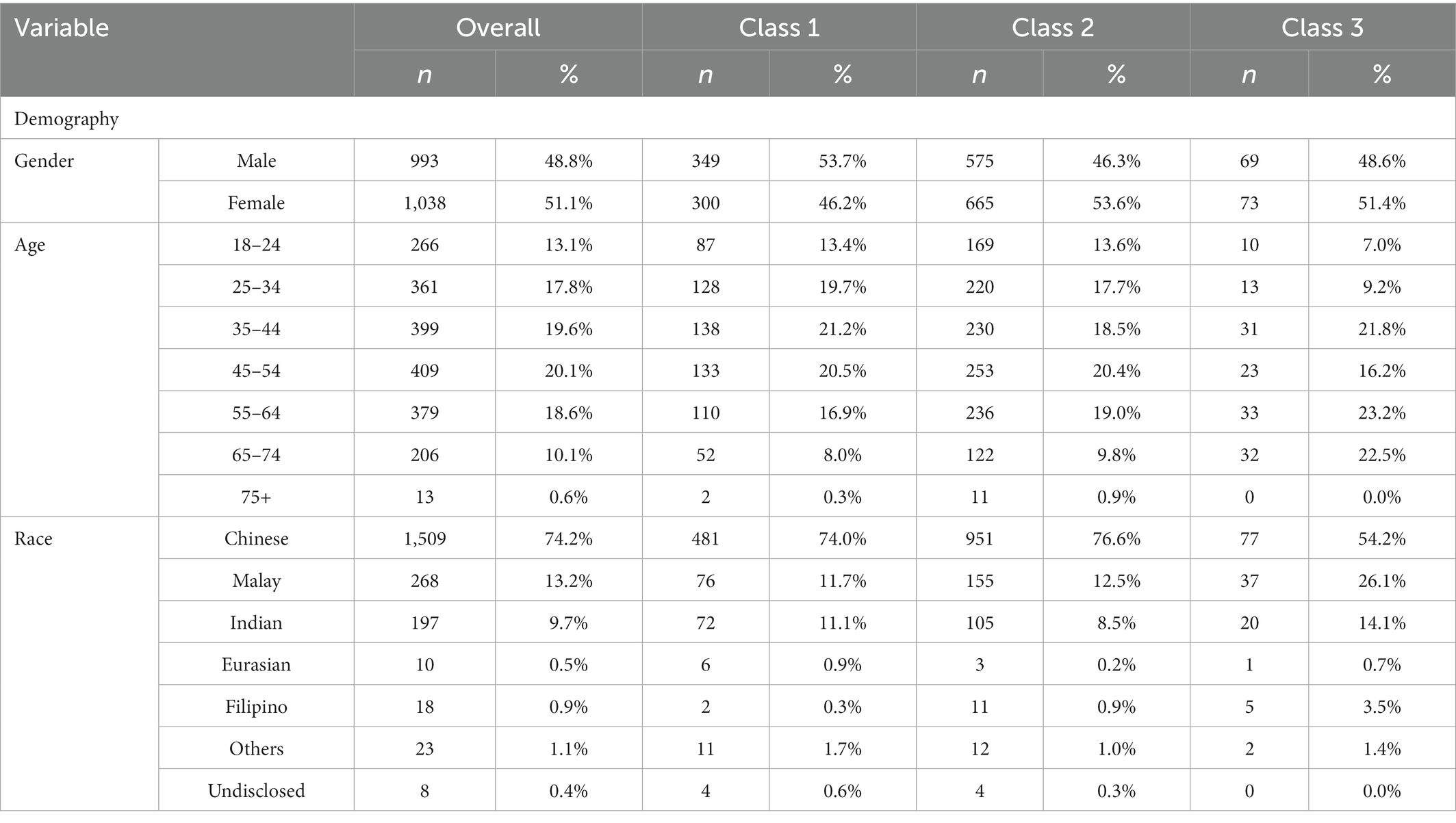
Table 2. Demographic differences between profiles.
Across the five personality traits, Extraversion and Neuroticism exhibited the lowest average score, while Conscientiousness exhibited the highest average (Table 3). Out of the Big Five Personality Traits, only Neuroticism does not show statistically significant differences between the audience segments. When compared pairwise, the less-concerned and the risk-majority profiles do not show significant differences from each other for Openness and Conscientiousness, while all classes differ from each other significantly for Extraversion and Agreeableness. Compared to the other two classes, the risk-anxious respondents score significantly higher on Openness, Conscientiousness, Extraversion and Agreeableness. The less-concerned respondents scored the lowest on Extraversion and Agreeableness as compared to the other two segments.
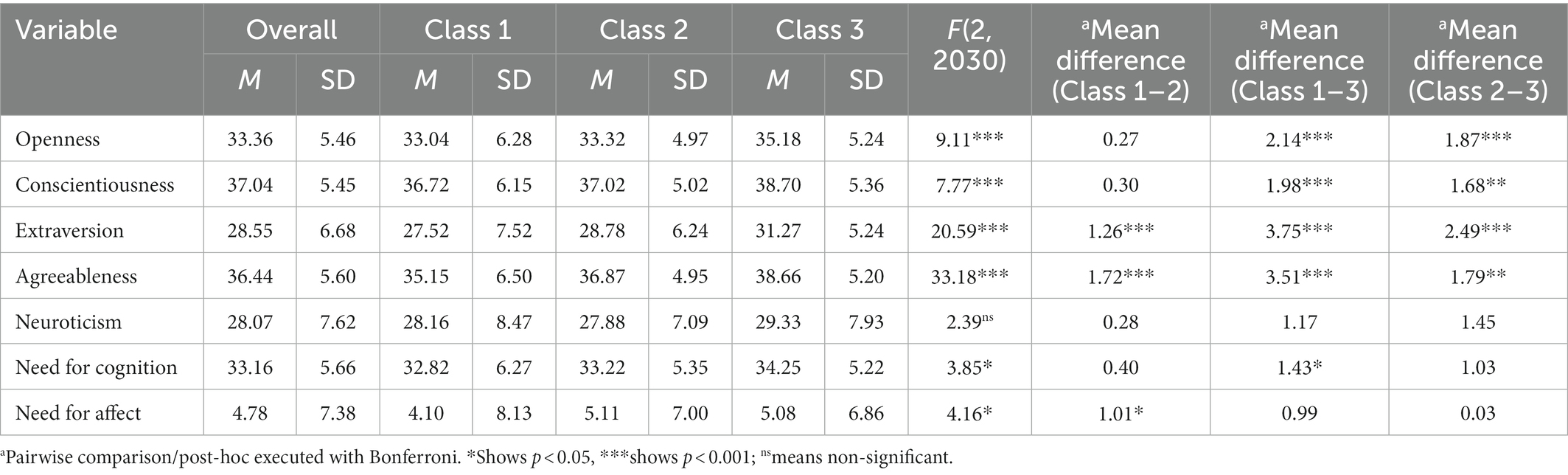
Table 3. Differences in big five personality traits and information processing styles.
There was a significant difference between the less concerned and the risk-anxious profiles on the need for cognition, where the latter scored significantly higher for the need for cognition than the former segment (Table 3). No class difference is observed between the other two comparisons. In contrast, there is a significant difference between the risk-majority and the less-concerned profiles, where the former scored significantly higher than the latter on the need for affect. No statistically significant difference is found between the other two pairwise comparisons.
Different health information-seeking behaviors during the pandemic are observed among the three identified audience segments (Table 4). The risk-anxious is found to have the highest frequency of health information seeking in a week (M = 3.52 out of 4). On the other hand, the less-concerned has the lowest frequency of health information seeking (M = 2.97 out of 4), while the risk-majority has the mean frequency that hovers close to that of the overall sample. In terms of the duration of health information seeking, the risk-anxious is found to spend about 10–60 min each day, the longest among the three classes of respondents (M = 2.51). However, no statistically significant difference is observed between the other two segments in the average time spent per day. Group differences are also observed between all three audience segments in health information platform intensity, with the risk-anxious having the highest intensity, followed by the risk-majority, and the less-concerned having the least intensity on health information.
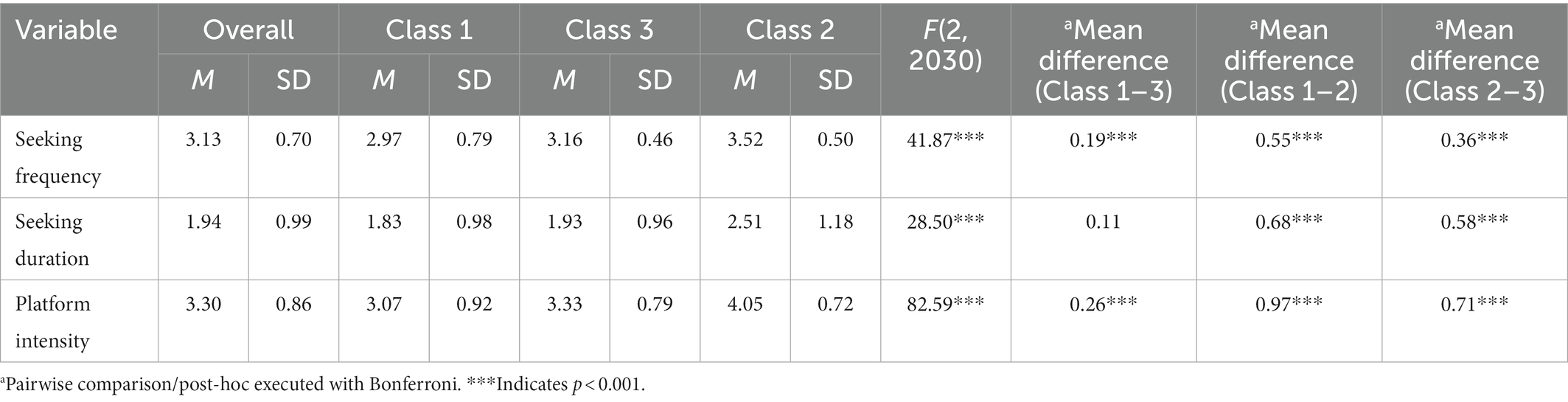
Table 4. Class comparison on health information seeking.
Out of the 15 platform choices for seeking health information on COVID-19, differences in platform preferences between the three audience segments can be seen in the following eight platforms (Table 5). The three audience segments shared similarities in their preference for formal sources of information. Official government websites, newspapers, and TV are the top three preferred platforms for seeking COVID-19 information for most of the less concerned and the risk-majority audiences. The risk-anxious preferred the TV, official government websites, and official government social media sites. However, the less concerned segment is found to have the highest proportion of respondents preferring informal sources (e.g., personal messaging applications, online forums, independent blogs) as compared to the other two segments and the overall sample.

Table 5. Differences in platform preferences.
Due to the nature of a ranked data measure for information preferences, this study executed nonparametric independent-samples Kruskal-Wallis’s test, with Bonferroni correction for pairwise comparisons (Table 6). Out of 17 listed content types, only seven indicated differences between the three audience segments for content type importance. The less-concerned and the risk-majority audiences showed differences in their topic importance for information on “the updated list of countries affected by COVID-19.” The less-concerned audience segment only differed from the risk-anxious on topic importance for information on “the current and future pandemic plans in Singapore.” The risk-majority and the risk-anxious differed in their topic importance on “the updated information of cluster areas in Singapore.” The risk-anxious audiences indicated differences from the other two segments in their perceived importance for information on “the spread of the outbreak in Singapore,” “information on proper procedures of washing hands,” “information on proper ways for putting on a mask,” and “the updated number of recovered patients infected by COVID-19 in Singapore.”
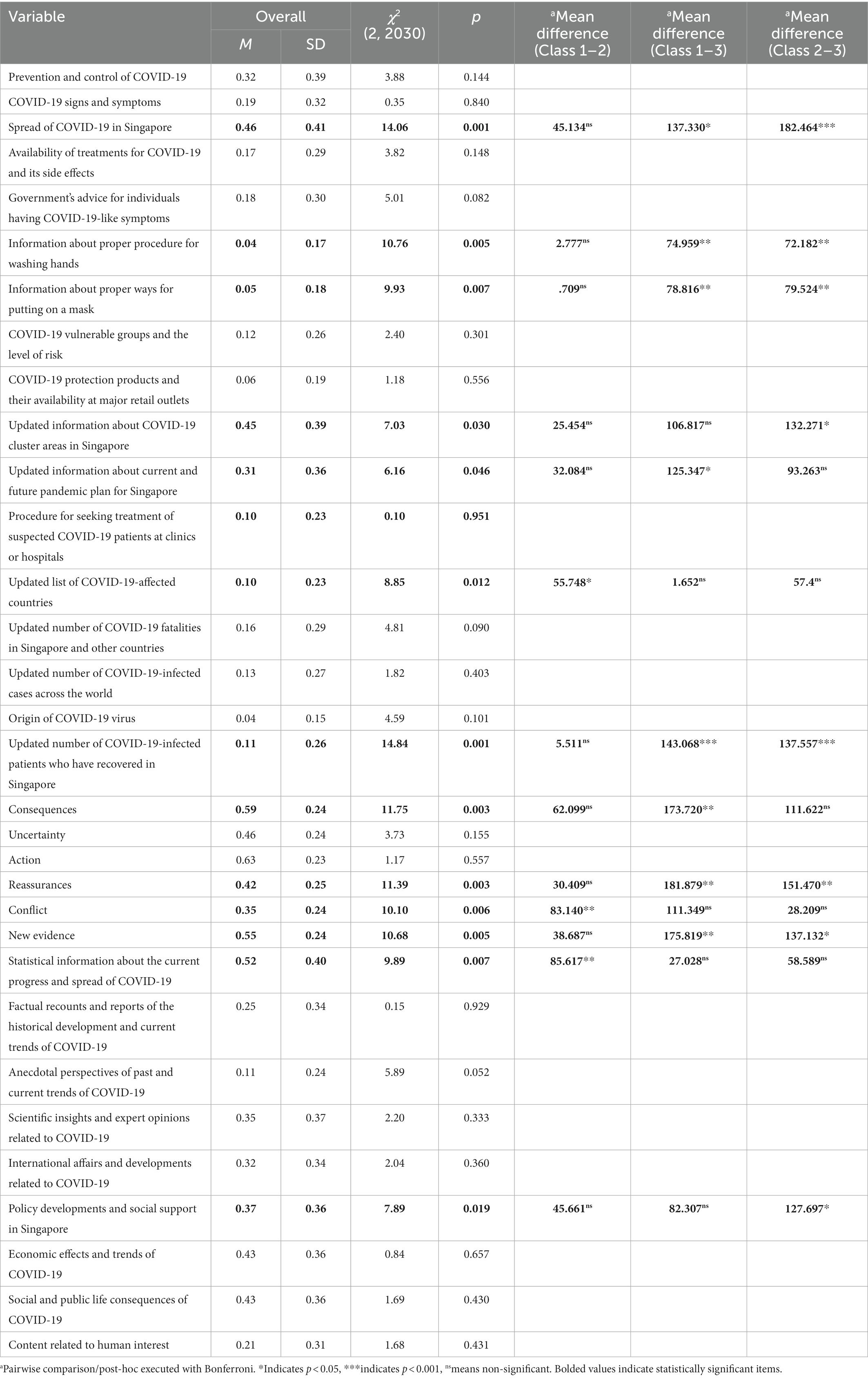
Table 6. Preference for COVID-19 information.
For reported news on COVID-19 that audiences are likely to read, all six news frame categories except for content related to “uncertainty of the disease” and “actions taken against COVID-19,” showed significant differences between the three audience segments. Risk-anxious audiences differ from the other audiences in their likelihood to read news reporting on “consequences of the disease,” “reassurances” and “new evidence on the disease.” The less-concerned and the risk-majority differ in their likelihood to read news reporting “conflicts on opinions on the pandemic,” but no other differences were identified from other pairwise comparisons.
Out of the nine content types that were provided, the audiences’ most liked topic was “statistical information about the current progress and spread of COVID-19″. This was followed by “the economic effects and trends of COVID-19”, “social and public life consequences of COVID-19”, “policy developments and social support in Singapore,” “scientific insights and expert opinions related to COVID-19,” and “international affairs and developments related to COVID-19.” However, only topics related to statistical information and policy developments showed statistically significant differences between the risk profiles. The difference is only observed for news based on statistical information between the less-concerned and the risk-majority. Difference between profiles is also observed between risk-majority and risk-anxious segments on the news related to “policy developments and social support in Singapore.” Other profile differences were not observed.
Out of the five stakeholders involved, health workers were attributed with the lowest responsibility, followed by schools and the workplace (Table 7). Citizens and government were attributed with the highest level of responsibility in reducing transmission during the pandemic. The less-concerned segment indicated a greater variance in their responsibility attribution, with the highest attributed to the government and the lowest to the health workers. On the other hand, the risk-anxious attributed the greatest extent of responsibility to all stakeholders, all scoring above 6.5 out of 7, with the greatest being the government, and the lowest being schools and the workplace. The risk-majority was more varied in the attributions of responsibility, showing a similar pattern to that of the less-concerned segment. Instead of attributing the government with the highest level of responsibility, risk-majority audiences attributed it to the citizens for reducing the transmission of COVID-19. Results based on ANOVA showed a significant difference between the three segments in the responsibility attributed to citizens, healthcare workers, and schools. However, significant differences were observed between the risk-anxious and the other two segments for responsibility attributed to the government and workplace, but not between the less-concerned and the risk-majority for these two entities. Thus, it can be inferred that the risk-anxious attributes more responsibility to the government and workplace in reducing the transmission of COVID-19.
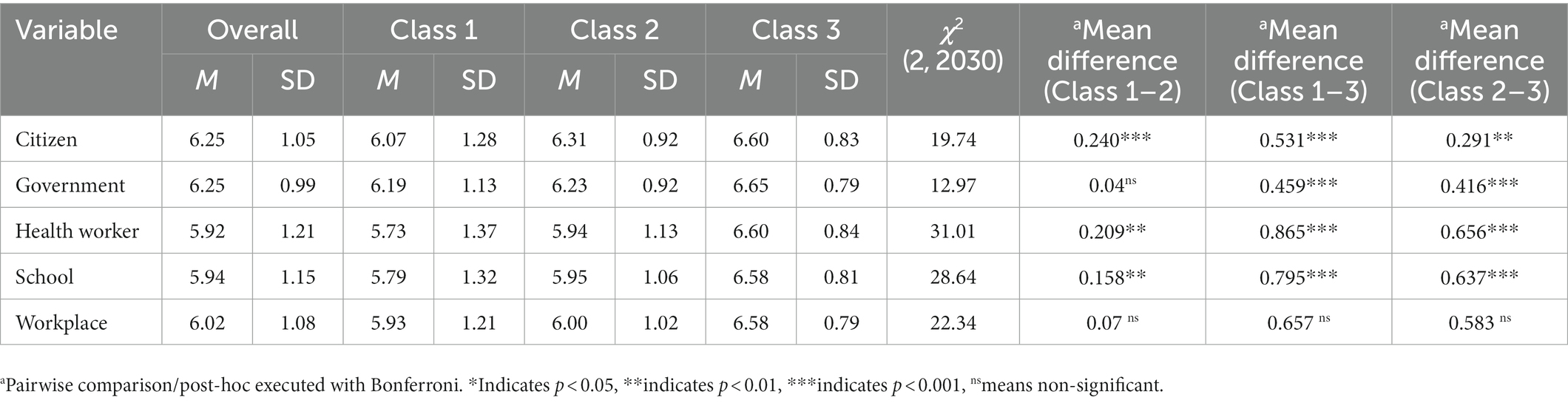
Table 7. Attributions of responsibility by each audience segment.
5. Discussion
The current study is one of the first that adopted Slater’s (1996) recommended strategy for multivariate audience segmentation. This study extends recent works on audience segmentation, such as Kleitman et al. (2021) and Smith et al. (2021) which clustered the sample primarily based on the engagement of preventive measures in COVID-19. Specifically, we took a more holistic approach by segmenting audiences based on their perceived knowledge, risk perceptions, and emotional responses, besides preventive behaviors during the COVID-19 pandemic.
Taking the person-centered approach, this study identifies and segments the sample into three main audience profiles: the less-concerned (32%), the risk-majority (61%), and the risk-anxious (7%). This study mirrors prior audience segmentation studies whereby people showcase complexity in patterns of behavior adoption. However, the current study brings originality in comparison with prior works. Instead of the identified traits of the resultant compliant and non-compliant audience segments in Kleitman’s et al. (2021), results of the current study identified three clusters of varying risk attitudes during the pandemic in a highly complaint sample. The results also differ from Smith et al. (2021), who identified five different audience classes based on their likelihood in engaging their preferred preventive measures, namely––the adherents, social distances, hygiene stewards, symptom managers and refusers, suggesting targeted campaigns for specific segments. In addition to characterizing traits of each identified audience segment, this study also highlighted the media and information preferences of each audience segment. Our finding shows that the less-concerned and the risk-anxious segments differ the most in perceived severity of COVID-19 and emotional responses felt during COVID-19. Possibly due to lower perceived severity and less emotional responses, the less-concerned also reported lower adoption of preventive behaviors compared to the risk-anxious segment.
5.1. Differences in audience segment characteristics
The three profiles differ from each other on several factors, including demographic characteristics, personality traits, information processing styles, health information seeking and preferences, and attributions of responsibility.
5.1.1. Demographic differences
Reflecting their highest risk perception and adoption of preventive measures, the risk-anxious consists of the highest proportion of respondents aged between 55 and 74. This finding is in line with recent studies which suggested that perceptions of COVID-19 severity increase with age (de Zwart et al., 2009; Bruine de Bruin, 2021; Rosi et al., 2021). Individuals in this age group perceive themselves to be more vulnerable to the complications brought by a COVID-19 infection due to pre-existing health conditions. Therefore, they tend to perceive greater severity and vulnerability toward COVID-19 and are more likely to engage in preventive measures (Bish and Michie, 2010).
On the other hand, gender differences in risk perception and adoption of preventive measures between segments corroborate with existing studies (Brug et al., 2004; Leung et al., 2004; Bish and Michie, 2010). Females are associated with higher perceived severity and higher adoption in preventive measures, as seen in the higher female audience proportion in risk-majority and risk-anxious segments. The less-concerned profile also consists of a higher proportion of male respondents. In terms of ethnicity, the risk-anxious indicated a higher proportion of Malays, Indians, and other ethnic groups in Singapore, as compared to other segments. This result could be influenced by other ethnic characteristics, and further studies should consider clarifying the association of ethnicity with risk perception and preventive measure adoption.
5.1.2. Personality differences
Out of the five personality traits, only neuroticism did not have any significant group differences, possibly due to the specific pandemic context that involves worry and anxiety. The risk-anxious audiences are found to be more open, conscientious, extraverted, and agreeable as compared to the less-concerned and the risk-majority. This finding suggests that the more extroverted respondents are more compliant with preventive measures, which counters the findings of Kleitman et al. (2021). Other personality traits like agreeableness, conscientiousness, and openness, in combination with extraversion, may exert an influence that delays gratification of social activities and adopt preventive measures (Aschwanden et al., 2021). The high scores in agreeableness, conscientiousness, and openness show that the risk-anxious audiences are more adaptable to changes in safety management measures and adhere to the regulations designed to reduce the transmission of COVID-19. Conversely, the less-concerned are shown to be less extraverted and agreeable than the risk-anxious and the risk-majority. Identifying these personality traits would be helpful for future campaigns when reaching out to people profiled under similar characteristics.
5.1.3. Information processing styles
Group differences are observed only between the less-concerned and the risk-anxious for NFC, consistent with Xu and Cheng’s (2021) findings on the association of NFC with engagement of preventive measures. That is, higher NFC is associated with enhanced risk perception, and higher adoption of preventive measures (Lachlan et al., 2021; Xu and Cheng, 2021). The higher scores of NFC in the risk-anxious audience segment also highlighted that this segment tends to use effortful, systematic information processing as compared to heuristic reasoning (Petty et al., 2009). The risk-majority scored significantly higher for NFA than the less-concerned and the risk-anxious. This shows that most of the audience are more likely to be persuaded by more emotionally charged messaging (Haddock et al., 2008). The less-concerned audience segment has low NFC and NFA as compared to other audience segments, which may prove to be a challenge for practitioners in making positive changes for this particular audience segment.
5.1.4. Differences in health information seeking and preferences
The risk-anxious differs from the other two profiles, with the highest frequency, and the longest time spent per day for health information seeking during COVID-19. A greater amount of time could be spent on fact-checking (Kleitman et al., 2021), given that they are identified as those who are more likely to perceive vulnerability to the disease (Brug et al., 2004; Bish and Michie, 2010; Bruine de Bruin, 2021). The less-concerned audiences are found to have lower frequency and intensity in seeking health information. Future studies should examine the motivations of each audience segment on their use of certain platforms for health information seeking during the pandemic.
Noteworthy findings related to health information preferences are observed. All three profiles reported a strong preference for official governmental sources and mainstream media for health information during the pandemic. This result similar to previous studies where the compliant group of respondents reported greater use of official sources, suggesting that respondents rely on credible sources for health information during the pandemic (Kleitman et al., 2021; Lwin et al., 2021). However, the less-concerned respondents also reported a significantly higher preference for informal sources like online forums, blogs and personal messaging applications as compared to the other two segments. This finding is in line with the concerns that previous studies have pointed out (Kleitman et al., 2021; Lwin et al., 2021). The use of both formal and informal sources for health information seeking during a pandemic would affect, positively and negatively, the effectiveness of campaigns used for managing the pandemic (Kleitman et al., 2021).
Each audience segment is found to have varied health information preferences. The risk-anxious segment indicated topics related to the spread of the pandemic and the proper procedures of preventive measures as important. This could be due to the higher perceived severity and vulnerability to COVID-19 and adoption levels of preventive behaviors found in the risk-anxious, thereby perceiving more importance should be placed on these topics to better manage the pandemic. Similar emphasis should also be placed on different topic preferences when tailoring messages for different clusters insofar as significant differences are observed between the risk-anxious and the risk-majority. Due to the progression of the pandemic situation in Singapore, updated information on clusters may not be seen as important by the risk-majority as compared to the risk-anxious. Further, the risk-anxious audiences are more likely to read stories reporting consequences of COVID-19, new evidence related to COVID-19, and reassurances on COVID-19. This could be associated to the risk perceptions and other characteristics of this audience segment. Moreover, the likelihood to read stories reporting reassurances can be associated with the higher frequency of positive emotions felt by the risk-anxious during the pandemic.
The less-concerned audience differed significantly from the risk-majority. They indicated greater importance on the “updated list of countries affected by COVID-19” and less importance on “current and future pandemic plans.” This difference could be indicated by personality traits characterizing the less-concerned, where they are less extroverted and less open, which would mean they are less open to changing policies or updates on the situation. In addition, the less-concerned segment indicated a greater likelihood to read conflict stories focusing on clash in opinions about COVID-19. This could be due to their preference of seeking health information on informal platforms such as blogs and online forums (Lachlan et al., 2021), or the need for stimulation from the infodemic/fatigue of prolonged exposure to COVID-19 information.
5.1.5. Differences in attributions of responsibility
The results have identified differences in responsibility attribution from each audience segment. The risk-anxious differs from the other two audience segments by attributing higher crisis responsibility to all stakeholders (citizens, government, health workers, school, and workplace) in reducing the transmission of COVID-19 in Singapore. This result could be linked to emotional reactions in this segment considering positive associations reported in prior work between attributions of responsibility and frequency of positive and negative emotions felt during a pandemic (Kim and Niederdeppe, 2013; Wong et al., 2021). The high responsibility attributed to all stakeholders by the risk-anxious audiences may not only be associated with the severity of the pandemic (Coombs, 1998; Lee, 2005; Choi and Lin, 2009; Kim and Niederdeppe, 2013), but also with perceived preventive efficacy toward the disease. This result echoes earlier works where perceived preventive efficacy to the disease may result in the respondents having more positive emotions (Kim and Niederdeppe, 2013). Conversely, moderate to high levels of responsibility were attributed across all stakeholders by the less-concerned and the risk-majority even when they less frequently felt positive and negative emotions during the pandemic. This may reflect these segments’ trust in the involved stakeholders and perceived importance of shared responsibility in reducing transmission, acknowledging that every entity plays their part in managing the crisis (Macnamara, 2021).
6. Study implications
6.1. Theoretical implications
This study extends research on audience segmentation of pandemic communication. Specifically, we used Slater’s (1996) recommendation of a multivariate classification which included knowledge, attitudes, and behaviors relevant to a given health domain. Existing research often relied solely on theoretical typologies (e.g., RPA framework) to perform audience segmentation during COVID-19 (e.g., Duong, 2022). In addition to risk attitudes and preventive behavior adoption, we included perceived knowledge and emotional responses felt during the pandemic as determinants of audience segmentation. The inclusion of audience profile predictors from a range of theoretically supported factors allows us to better capture differences in how various segments perceive and respond to a pandemic.
6.2. Practical implications
This study also has several practical implications for policymakers and practitioners of pandemic communication. Firstly, the identification of the less-concerned audience segment, which constitutes about one-third (32%) of the sample, may prove to be important in practice. The less-concerned audiences have considerably lower risk perceptions and engagement in preventive behavior, making them a primary target audience who needs an intervention. In doing so, practitioners could consider their characteristics, such as being less extroverted and less agreeable than the other audience segments, in designing tailored intervention strategies. It is also noteworthy that they have a higher tendency to seek health information from informal sources and prefer news or stories reporting conflicts which possibly indicates a higher likelihood of being more easily fatigued with constant messaging. In targeting the less-concerned, future strategies can use narrative messages or appeal to self-interest rather than social obligations to the community in promoting their positive attitude and behavior change (Kleitman et al., 2021).
On the other hand, the risk-anxious audience segment shows strong adherence to governmental recommendations due to their perceived severity of the disease. Characterized with high intensity, frequency and time spent on health information seeking, preference in mainstream media as health information sources, the risk-anxious also reported the highest frequency in positive and negative emotions felt during the pandemic. Future messaging targeting a risk-anxious segment should take a more reassuring stance to not encourage extreme behaviors such as panic buying or excessive information search and sharing.
6.3. Limitations and future studies
While this study provides useful insights into pandemic communication, this study is not without its limitations. First, this study focuses on Singapore, a country with high vaccination rates and compliance rates with preventive measures against COVID-19, which could be related to its unique cultural characteristics and sociopolitical environment. Thus, our findings should be cautiously interpreted and applied to different populations and pandemic contexts. Second, this study is based on a cross-sectional design that only represents one point in time in the pandemic. Due to the rapid progression of the COVID-19 pandemic, relaxation or tightening of preventive measures may change in the duration of weeks or months. Accordingly, individual perceptions and behavior may as well change with the updated measures over the course. Therefore, longitudinal studies may allow us more insights into the changes in risk perceptions and behaviors, as well as the stability of audience profiles identified over time.
Despite the reopening of economies and most international borders, the COVID-19 pandemic is still ongoing. Overexposure to messaging related to COVID-19 pandemic can lead to message fatigue. Future research could examine audience segmentation with message fatigue or examine how fatigue changes over time in audience segments. While we focused on prevention behaviors, future studies could investigate other behaviors relevant to a pandemic (e.g., panic buying and cyberchondria). Additionally, further research can investigate how various segments would perceive or act based on fake news and disinformation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by DSO-SAF Institutional Review Board (IRB). The patients/participants provided their written informed consent to participate in this study.
Author contributions
HK, BP, YT, and WL contributed to the conception and design of the study. YO performed the statistical analysis and wrote the first draft of the manuscript. HK and BP revised sections of the manuscript. All authors contributed to the manuscript revision, read, and approved the submitted version.
Funding
This research was supported by the DSO National Laboratories (DSOCL21088).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1085208/full#supplementary-material
References
Achterhof, R., Huntjens, R. J., Meewisse, M. L., and Kiers, H. A. (2019). Assessing the application of latent class and latent profile analysis for evaluating the construct validity of complex posttraumatic stress disorder: cautions and limitations. Eur. J. Psychotraumatol. 10:1698223. doi: 10.1080/20008198.2019.1698223
Ahmed, O., Hossain, K. N., Siddique, R. F., and Jobe, M. C. (2021). COVID-19 fear, stress, sleep quality and coping activities during lockdown, and personality traits: a person-centered approach analysis. Personal. Individ. Differ. 178:110873. doi: 10.1016/j.paid.2021.110873
Anaki, D., and Sergay, J. (2021). Predicting health behavior in response to the coronavirus disease (COVID-19): worldwide survey results from early march 2020. PLoS One 16:e0244534. doi: 10.1371/journal.pone.0244534
Aschwanden, D., Strickhouser, J. E., Sesker, A. A., Lee, J. H., Luchetti, M., Stephan, Y., et al. (2021). Psychological and behavioural responses to coronavirus disease 2019: the role of personality. Eur. J. Pers. 35, 51–66. doi: 10.1002/per.2281
Avery, E. (2010). Contextual and audience moderators of channel selection and message reception of public health information in routine and crisis situations. J. Public Relat. Res. 22, 378–403. doi: 10.1080/10627261003801404
Ayers, S. L., and Kronenfeld, J. J. (2007). Chronic illness and health-seeking information on the internet. Health 11, 327–347. doi: 10.1177/1363459307077547
Ball, H., and Wozniak, T. R. (2021). Why do some Americans resist COVID-19 prevention behavior? An analysis of issue importance, message fatigue, and reactance regarding COVID-19 messaging. Health Commun. 37, 1812–1819. doi: 10.1080/10410236.2021.1920717
Bandura, A. (2000). Exercise of human agency through collective efficacy. Curr. Dir. Psychol. Sci. 9, 75–78. doi: 10.1111/1467-8721.00064
Bertoletti, M., Friel, N., and Rastelli, R. (2015). Choosing the number of clusters in a finite mixture model using an exact integrated completed likelihood criterion. Metro 73, 177–199. doi: 10.1007/s40300-015-0064-5
Biernacki, C., Celeux, G., and Govaert, G. (2000). Assessing a mixture model for clustering with the integrated completed likelihood. IEEE Trans. Pattern Anal. Mach. Intell. 22, 719–725. doi: 10.1109/34.865189
Bish, A., and Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br. J. Heath Psychol. 15, 797–824. doi: 10.1348/135910710X485826
Blagov, P. S. (2021). Adaptive and dark personality in the COVID-19 pandemic: predicting health-behavior endorsement and the appeal of public-health messages. Soc. Psychol. Personal. Sci. 12, 697–707. doi: 10.1177/1948550620936439
Bogg, T., and Roberts, B. W. (2004). Conscientiousness and health-related behaviors: a meta-analysis of the leading behavioral contributors to mortality. Psychol. Bull. 130, 887–919. doi: 10.1037/0033-2909.130.6.887
Brug, J., Aro, A. R., Oenema, A., De Zwart, O., Richardus, J. H., and Bishop, G. D. (2004). SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerg. Infect. Dis. 10, 1486–1489. doi: 10.3201/eid1008.040283
Bruine de Bruin, W. (2021). Age differences in COVID-19 risk perceptions and mental health: evidence from a national US survey conducted in March 2020. J. Gerontol. B 76, e24–e29. doi: 10.1093/geronb/gbaa074
Cacioppo, J. T., Petty, R. E., and Kao, C. (1984). The efficient assessment of need for cognition. J. Pers. Asses. 48, 306–307. doi: 10.1207/s15327752jpa4803_13
Caress, A. L., Duxbury, P., Woodcock, A., Luker, K. A., Ward, D., Campbell, M., et al. (2010). Exploring the needs, concerns and behaviours of people with existing respiratory conditions in relation to the H1N1 'swine influenza' pandemic: a multicentre survey and qualitative study. Health Tech. Asses. 14, 1–108. doi: 10.3310/hta14340-01
Carpenter, C. J. (2010). A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 25, 661–669. doi: 10.1080/10410236.2010.521906
Choi, Y., and Lin, Y. H. (2009). Consumer responses to Mattel product recalls posted on online bulletin boards: exploring two types of emotion. J. Public Relat. Res. 21, 198–207. doi: 10.1080/10627260802557506
Coombs, W. T. (1998). An analytic framework for crisis situations: better responses from a better understanding of the situation. J. Public Relat. Res. 10, 177–191. doi: 10.1207/s1532754xjprr1003_02
Coombs, W. T. (2016). Reflections on a meta-analysis: crystallizing thinking about SCCT. J. Public Relat. Res. 28, 120–122. doi: 10.1080/1062726X.2016.1167479
de Zwart, O., Veldhuijzen, I. K., Elam, G., Aro, A. R., Abraham, T., Bishop, G. D., et al. (2007). Avian influenza risk perception, Europe and Asia. Emerg. Infect. Dis. 13, 290–293. doi: 10.3201/eid1302.060303
de Zwart, O., Veldhuijzen, I. K., Elam, G., Aro, A. R., Abraham, T., Bishop, G. D., et al. (2009). Perceived threat, risk perception, and efficacy beliefs related to SARS and other (emerging) infectious diseases: results of an international survey. Int. J. Behave. Med. 16, 30–40.
Duncan, L. A., Schaller, M., and Park, J. H. (2009). Perceived vulnerability to disease: development and validation of a 15-item self-report instrument. Personal. Individ. Differ. 47, 541–546. doi: 10.1016/j.paid.2009.05.001
Duong, H. T. (2022). Campaign message exposure, audience segmentation, and protective behaviors in the early stages of the COVID-19 pandemic in Vietnam. J. Commun. Health 15, 121–130. doi: 10.1080/17538068.2021.2021747
Ellison, N. B., Steinfield, C., and Lampe, C. (2007). The benefits of Facebook “friends:” social capital and college students’ use of online social network sites. J. Comp. Med. Commun. 12, 1143–1168. doi: 10.1111/j.1083-6101.2007.00367.x
Fredrickson, B. L., Tugade, M. M., Waugh, C. E., and Larkin, G. R. (2003). What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J. Pers. Soc. Psychol. 84, 365–376. doi: 10.1037/0022-3514.84.2.365
Goldberg, L. R. (1992). The development of markers for the big-five factor structure. Psychol. Asses. 4, 26–42. doi: 10.1037/1040-3590.4.1.26
Grunig, J. (1989). “Publics, audiences, and market segments: segmentation principles for campaigns,” in Information Campaigns: Balancing Social Values and Social Change. ed. C. Salmon (Newbury Park, CA: Sage), 199–228.
Haddock, G., Maio, G. R., Arnold, K., and Huskinson, T. (2008). Should persuasion be affective or cognitive? The moderating effects of need for affect and need for cognition. Pers. Soc. Psychol. Bull. 34, 769–778. doi: 10.1177/0146167208314871
Izard, C. E. (1977). “Differential emotions theory,” in Human Emotions. ed. C. E. Izard (Boston, MA: Springer), 43–66.
Izard, C. E. (1993). Four systems for emotion activation: cognitive and noncognitive processes. Psychol. Rev. 100, 68–90. doi: 10.1037/0033-295X.100.1.68
Jacobs, W., Amuta, A. O., and Jeon, K. C. (2017). Health information seeking in the digital age: an analysis of health information seeking behavior among US adults. Cogn. Soc. Sci. 3:1302785. doi: 10.1080/23311886.2017.1302785
John, O. P., and Srivastava, S. (1999). “The big-five trait taxonomy: history, measurement, and theoretical perspectives,” in Handbook of Personality: Theory and Research. eds. L. A. Pervin and O. P. John (New York: Guilford Press), 102–138.
Kim, H. K., and Niederdeppe, J. (2013). The role of emotional response during an H1N1 influenza pandemic on a college campus. J. Public Relat. Res. 25, 30–50. doi: 10.1080/1062726X.2013.739100
Kleitman, S., Fullerton, D. J., Zhang, L. M., Blanchard, M. D., Lee, J., Stankov, L., et al. (2021). To comply or not comply? A latent profile analysis of behaviours and attitudes during the COVID-19 pandemic. PLoS One 16:e0255268. doi: 10.1371/journal.pone.0255268
Kroencke, L., Geukes, K., Utesch, T., Kuper, N., and Back, M. D. (2020). Neuroticism and emotional risk during the COVID-19 pandemic. J. Res. Pers. 89:104038. doi: 10.1016/j.jrp.2020.104038
Lachlan, K. A., Hutter, E., Gilbert, C., and Spence, P. R. (2021). From what I've heard, this is bad: an examination of Americans' source preferences and information seeking during the COVID-19 pandemic. Prog. Dis. Sci. 9:100145. doi: 10.1016/j.pdisas.2021.100145
Lambert, S. D., and Loiselle, C. G. (2007). Health information–seeking behavior. Qual. Health Res. 17, 1006–1019. doi: 10.1177/1049732307305199
Lee, B. K. (2005). Hong Kong consumers' evaluation in an airline crash: a path model analysis. J. Pubic Relat. Res. 17, 363–391. doi: 10.1207/s1532754xjprr1704_3
Lefebvre, R. C., Doner, L., Johnson, C., Loughrey, K., Balch, G., and Sutton, S. (1995). “Use of database marketing and consumer-based health communication in message design: an example from the Office of Cancer Communication’s ‘5 a day for better health’ program” in Designing Health Messages. eds. E. Maibach and R. Parrott (Thousand Oaks, CA: Sage), 217–247.
Leung, G. M., Quah, S., Ho, L. M., Ho, S. Y., Hedley, A. J., Lee, H. P., et al. (2004). A tale of two cities: community psychobehavioral surveillance and related impact on outbreak control in Hong Kong and Singapore during the severe acute respiratory syndrome epidemic. Infect. Control. Hosp. Epidemiol. 25, 1033–1041. doi: 10.1086/502340
Lwin, M. O., Lee, S. Y., Panchapakesan, C., and Tandoc, E. (2021). Mainstream news media’s role in public health communication during crises: assessment of coverage and correction of COVID-19 misinformation. Health Commun. 38, 160–168. doi: 10.1080/10410236.2021.1937842
Macnamara, J. (2021). New insights into crisis communication from an “inside” emic perspective during COVID-19. Public Relat Inq. 10, 237–262. doi: 10.1177/2046147X21999972
Maibach, E. W., Leiserowitz, A., Roser-Renouf, C., and Mertz, C. K. (2011). Identifying like-minded audiences for global warming public engagement campaigns: an audience segmentation analysis and tool development. PLoS One 6:e17571. doi: 10.1371/journal.pone.0017571
Maibach, E. W., Maxfield, A., Ladin, K., and Slater, M. (1996). Translating health psychology into effective health communication: the American Healthstyles audience segmentation project. J. Health Psychol. 1, 261–277. doi: 10.1177/135910539600100302
Maio, G. R., and Esses, V. M. (2001). The need for affect: individual differences in the motivation to approach or avoid emotions. J. Pers. 69, 583–614. doi: 10.1111/1467-6494.694156
Majid, S., and Rahmat, N. A. (2013). Information needs and seeking behavior during the H1N1 virus outbreak. J. Inf. Sci. Theory Pract. 1, 42–53. doi: 10.1633/JISTaP.2013.1.1.3
McCrae, R. R., and Costa, P. T. (2006). Personality in Adulthood: A Five-factor Theory Perspective. 2nd. New York: Guilford Press.
McCrae, R. R., and John, O. P. (1992). An introduction to the five-factor model and its applications. J. Pers. 60, 175–215. doi: 10.1111/j.1467-6494.1992.tb00970.x
Nylund, K. L., Asparouhov, T., and Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct. Equ. Modeling 14, 535–569. doi: 10.1080/10705510701575396
Park, S., Boatwright, B., and Avery, E. J. (2019). Information channel preference in health crisis: exploring the roles of perceived risk, preparedness, knowledge, and intent to follow directives. Public Relat. Rev. 45:101794. doi: 10.1016/j.pubrev.2019.05.015
Park, H. J., and Lee, B. J. (2016). The role of social work for foreign residents in an epidemic: the MERS crisis in the Republic of Korea. Soc. Work Public Health 31, 656–664. doi: 10.1080/19371918.2016.1160352
Petty, R. E., Briñol, P., Loersch, C., and McCaslin, M. J. (2009). “The need for cognition” in In the Handbook of Individual Differences in Social Behavior. eds. M. R. Leary and R. H. Hoyle (New York: Guilford Press), 318–329.
Petty, R. E., and Cacioppo, J. T. (1982). The need for cognition. J. Pers. Soc. Psychol. 42, 116–131.
Quandt, T., Boberg, S., Schatto-Eckrodt, T., and Frischlich, L. (2020). Pandemic News: Facebook Pages of Mainstream News Media and the Coronavirus Crisis–a Computational Content Analysis. arXiv. Available at: https://arxiv.org/abs/2005.13290 (Accessed June 2, 2022).
Rayani, M., Rayani, S., and Najafi-Sharjabad, F. (2021). COVID-19-related knowledge, risk perception, information seeking, and adherence to preventive behaviors among undergraduate students, southern Iran. Environ. Sci. Pollut. Res. 28, 59953–59962. doi: 10.1007/s11356-021-14934-y
Reuters. (2022). Singapore to Drop Most Indoor Mask Requirements Next Week. Available at: https://www.reuters.com/world/asia-pacific/singapore-drop-most-indoor-mask-requirements-next-week-2022-08-24/ (Accessed August 2, 2022).
Rimal, R. N., Brown, J., Mkandawire, G., Folda, L., Böse, K., and Creel, A. H. (2009). Audience segmentation as a social-marketing tool in health promotion: use of the risk perception attitude framework in HIV prevention in Malawi. Am. J. Public Health 99, 2224–2229. doi: 10.2105/AJPH.2008.155234
Rimal, R. N., and Real, K. (2003). Perceived risk and efficacy beliefs as motivators of change: use of the risk perception attitude (RPA) framework to understand health behaviors. Hum. Commun. Res. 29, 370–399. doi: 10.1111/j.1468-2958.2003.tb00844.x
Rock, E. M., Ireland, M., Resnick, M. D., and McNeely, C. A. (2005). A rose by any other name? Objective knowledge, perceived knowledge, and adolescent male condom use. Pediatrics 115, 667–672. doi: 10.1542/peds.2004-0139
Rogers, E. M., and Storey, J. D. (1987). “Communication campaigns” in Handbook of Communication Science. eds. C. R. Berger and S. H. Chaffee (Beverly Hills: Sage Publications), 817–846.
Rosi, A., Van Vugt, F. T., Lecce, S., Ceccato, I., Vallarino, M., Rapisarda, F., et al. (2021). Risk perception in a real-world situation (COVID-19): how it changes from 18 to 87 years old. Front. Psych. 12:646558. doi: 10.3389/fpsyg.2021.646558
Scrucca, L., Fop, M., Murphy, T. B., and Raftery, A. E. (2016). Mclust 5: clustering, classification and density estimation using Gaussian finite mixture models. R. J. 8, 289–317. doi: 10.32614/RJ-2016-021
Shieh, C., Broome, M. E., and Stump, T. E. (2010). Factors associated with health information-seeking in low-income pregnant women. Women Health 50, 426–442. doi: 10.1080/03630242.2010.506152
Shih, T. J., Wijaya, R., and Brossard, D. (2008). Media coverage of public health epidemics: linking framing and issue attention cycle toward an integrated theory of print news coverage of epidemics. Mass Commun. Soc. 11, 141–160. doi: 10.1080/15205430701668121
Singapore Department of Statistics. (2021). Singapore Census of Population 2020, Statistical Release 1: Demographic characteristics, Education, Language and Religion. Available at: https://www.singstat.gov.sg/publications/reference/cop2020/cop2020-sr1 (Accessed June 1, 2022).
Slater, M. D. (1996). Theory and method in health audience segmentation. J. Health Commun. 1, 267–284. doi: 10.1080/108107396128059
Slovic, P., Finucane, M. L., Peters, E., and MacGregor, D. G. (2013). “Risk as analysis and risk as feelings: some thoughts about affect, reason, risk and rationality” in The Feeling of Risk. ed. P. Slovic (London: Routledge), 21–36.
Smith, R. A. (2017). “Audience segmentation techniques” in Oxford Research Encyclopedia of Communication: Health and Risk Message Design and Processing. ed. R. L. Parrott (Oxford: Oxford University Press), 1–12.
Smith, R. A., Myrick, J. G., Lennon, R. P., Martin, M. A., Small, M. L., Van Scoy, L. J., et al. (2021). Exploring behavioral typologies to inform COVID-19 health campaigns: a person-centered approach. J. Health Commun. 26, 402–412. doi: 10.1080/10810730.2021.1946218
So, J., Kuang, K., and Cho, H. (2019). Information seeking upon exposure to risk messages: predictors, outcomes, and mediating roles of health information seeking. Commun. Res. 46, 663–687. doi: 10.1177/0093650216679536
Sutin, A. R., and Terracciano, A. (2016). Five-factor model personality traits and the objective and subjective experience of body weight. J. Pers. 84, 102–112. doi: 10.1111/jopy.12143
Wardenaar, K. (2021). Latent profile analysis in R: A tutorial and comparison to mplus. PsyArXiv. doi: 10.31234/osf.io/wzftr
Warren, G. W., and Lofstedt, R. (2021). Risk communication and COVID-19 in Europe: lessons for future public health crises. J. Risk Res. 25, 1161–1175. doi: 10.1080/13669877.2021.1947874
Weinstein, N. D. (1988). The precaution adoption process. Health Psychol 7, 355–386. doi: 10.1037/0278-6133.7.4.355
Wong, C. M. L., and Jensen, O. (2020). The paradox of trust: perceived risk and public compliance during the COVID-19 pandemic in Singapore. J. Risk Res. 23, 1021–1030. doi: 10.1080/13669877.2020.1756386
Wong, L. P., and Sam, I. C. (2010). Public sources of information and information needs for pandemic influenza a (H1N1). J. Commun. Health 35, 676–682. doi: 10.1007/s10900-010-9271-4
Wong, J. C. S., Yang, J. Z., Liu, Z., Lee, D., and Yue, Z. (2021). Fast and frugal: information processing related to the coronavirus pandemic. Risk Anal. 41, 771–786. doi: 10.1111/risa.13679
World Health Organization. (2022). Coronavirus Disease (COVID-19) Pandemic. Geneva: World Health Organization. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (Accessed June 1, 2022).
Xu, P., and Cheng, J. (2021). Individual differences in social distancing and mask-wearing in the pandemic of COVID-19: the role of need for cognition, self-control and risk attitude. Personal. Individ. Differ. 175:110706. doi: 10.1016/j.paid.2021.110706
Yeo, S. L., Phua, D. Y., and Hong, Y. Y. (2022). The effects of dangerous world beliefs on COVID-19 preventive behaviors in Singapore: the moderating role of public health communication. Int. J. Strateg. Commun. 16, 485–498. doi: 10.1080/1553118X.2022.2036742
Zhang, L., Kong, Y., and Chang, H. (2015). Media use and health behavior in H1N1 flu crisis: the mediating role of perceived knowledge and fear. Atl. J. Commun. 23, 67–80. doi: 10.1080/15456870.2015.1013101
Keywords: audience segmentation, pandemic communication, risk perception, big five personality traits, health information preferences
Citation: Ong YX, Kim HK, Pelzer BO, Tan YY, Lim WP, Chua AKL and Koh BY (2023) Profile identification and characterization of risk perceptions and preventive behaviors during the COVID-19 pandemic: A latent profile analysis. Front. Psychol. 14:1085208. doi: 10.3389/fpsyg.2023.1085208
Edited by:
Changiz Mohiyeddini, Oakland University William Beaumont School of Medicine, United StatesReviewed by:
Qian Zhou, Huazhong University of Science and Technology, ChinaJunwei Cao, Yangzhou University, China
Ammar Redza Ahmad Rizal, National University of Malaysia, Malaysia
Copyright © 2023 Ong, Kim, Pelzer, Tan, Lim, Chua and Koh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hye Kyung Kim, ✉ SEtLaW1AbnR1LmVkdS5zZw==