
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychol. , 15 December 2022
Sec. Psycho-Oncology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyg.2022.960029
 Dirk Hofmeister1
Dirk Hofmeister1 Thomas Schulte2
Thomas Schulte2 Anja Mehnert-Theuerkauf1Kristina Geue1Markus Zenger3,4
Anja Mehnert-Theuerkauf1Kristina Geue1Markus Zenger3,4 Peter Esser1Heide Götze1
Peter Esser1Heide Götze1 Andreas Hinz1*
Andreas Hinz1*Objective: It is well-known that patients with cancer frequently experience sleep problems, and that sleep quality is associated with general quality of life (QoL). The aims of this study were to analyze the relationship between sleep problems and other components of QoL in more detail and to investigate sex and age differences in sleep quality in cancer patients in comparison with the general population.
Method: This study comprised one general population sample (n = 4,476) and eight samples with cancer patients (n between 323 and 4,020). Sleep Quality was measured using the QoL questionnaire EORTC QLQ-C30.
Results: All of the cancer patient groups reported more sleep problems than the general population. Sleep problems were associated with all facets of QoL both in cancer patients and in the general population. The highest associations were found in cancer patients for fatigue (r = 0.52) and emotional functioning (r = −0.47). The association between sleep quality and general QoL was lower in the cancer samples (r = −0.37) than in the general population (r = −0.46). Female cancer patients reported markedly more sleep problems than male patients did (d = 0.45), while this sex difference was lower in the general population (d = 0.15). In contrast to the general population, younger cancer patients had greater trouble sleeping than older patients did (d = −0.17).
Conclusion: The results underline the significance of the role mental factors play in sleep problems. Health care providers should pay special attention to female patients and younger patients concerning this issue.
According to the WHO, the number of cancer-related deaths is about 10 million worldwide, and the number is expected to increase markedly in the next decades (Sung et al., 2021).
Cancer patients often experience sleep disturbances (Ancoli-Israel, 2009; Akman et al., 2015; Otte et al., 2015; Strik et al., 2021), the prevalence of which ranges from 30 to 93% (Lin et al., 2020). Sleep problems often remain undetected in clinical practice (Kwak et al., 2020), and they are common among cancer survivors even after cancer treatment completion (Schieber et al., 2019; Aronsen et al., 2022). They are associated with reduced quality of life (QoL; Ancoli-Israel et al., 2014), depression (Hofmeister et al., 2020), concentration problems (Henneghan et al., 2018), fatigue (Medysky et al., 2017; Chartogne et al., 2021), and even reduced survival (Gottfried et al., 2020; Bach et al., 2021). However, it has yet to be systematically examined whether sleep problems are more strongly associated with physical health or with mental health problems, and previous studies have had inconsistent findings. While some found no difference between physical health and mental health in terms of how those dimensions were correlated with sleep problems (Kudielka et al., 2004), some detected stronger associations between sleep problems and physical health problems (Delgado-Guay et al., 2011; Sandadi et al., 2011), and others reported stronger associations with mental health factors (Nock et al., 2020; Pozzar et al., 2021).
Sex and age differences in sleep quality have been examined in both patient and general population samples. Most studies have found that females report having greater trouble sleeping than males do, while no consistent age effects were observed (Hinz et al., 2017a; Tibubos et al., 2020; Santoso et al., 2021; Schulte et al., 2021). Since cancer types and sex as well as age can be confounded, it is important to quantify sex and age differences when the impact of specific cancer types or treatments on sleep quality is to be examined. Therefore, it is relevant to investigate sex and age effects on sleep quality in cancer patients, and, for reasons of comparability, in the general population as well. A further issue is the question whether the strengths of the associations between sleep quality and general QoL depend on sex and age, e.g., whether sleep quality predicts QoL better or worse in samples of females in comparison with samples of males. This issue has not been addressed previously.
The relationship between sleep quality and other aspects of QoL, as well as age and sex effects, have been investigated in many studies that used a variety of questionnaires and many different samples of cancer patients. This makes it difficult to generalize the results. In our study, we used a single questionnaire, the EORTC QLQ-C30, which measures multiple components of QoL, including sleep quality, in a uniform way. Eight sufficiently large samples of cancer patients were included, making it possible to cover a wide range of cancers and settings. The results of the cancer samples are contrasted with a large sample of individuals from the general population to show the extent to which the associations of the QoL components and the age and sex effects found in the cancer samples are also present in the general population.
Summing up, the aims of this study were (a) to analyze the associations between sleep quality and other aspects of QoL in cancer patients, and to compare these results with the associations found in the general population, (b) to investigate sex and age effects on sleep quality in both types of samples, and (c) to explore sex and age effects of the correlations between sleep quality and general QoL assessments.
This study is a summarizing analysis of results obtained from several samples. The data set consists of eight German samples of cancer patients and one German general population sample. These samples have already been analyzed and featured in published studies with other objectives. Table 1 shortly describes the samples and references where further aspects of the studies such as sampling procedure, sociodemographic and clinical characteristics, time of examination, and response rate are described. The analyses were restricted to the respondents for whom sleep scale scores were available. Therefore, the sample sizes are not always exactly identical to those described in the reference papers. All of the studies were approved by corresponding ethics committees, and informed consent was obtained from all participants.
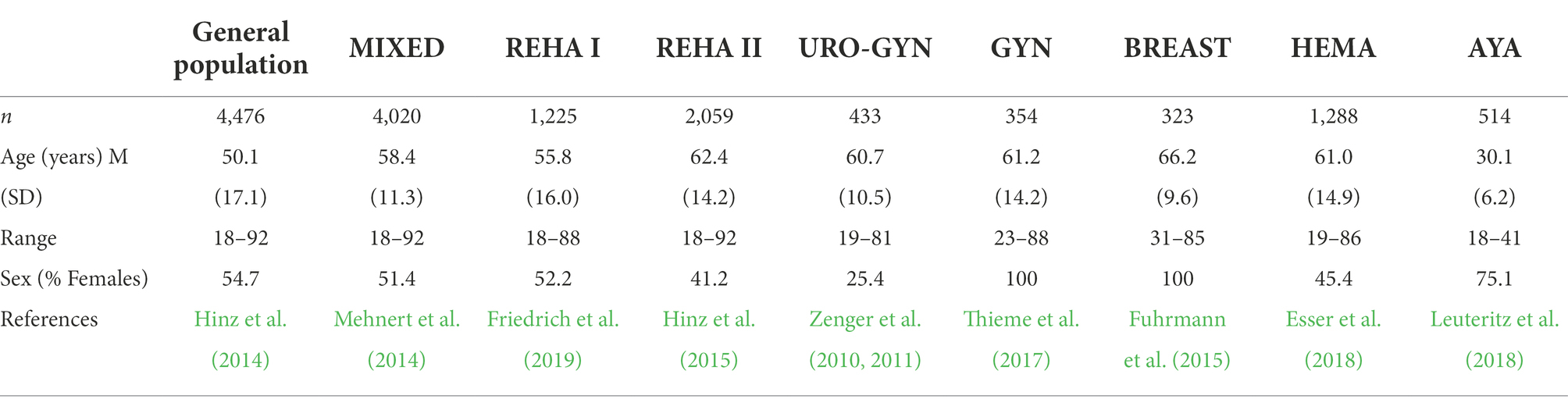
Table 1. Characteristics of the samples.
In all eight clinical samples, general inclusion criteria were a confirmed cancer diagnosis, age 18 years or older, and sufficient cognitive ability and language skills to complete the questionnaires. In samples 2 through 7, patients were visited in person and asked to participate; in samples 8 and 9, both personal visit and request to participate in an online survey were used. Samples 7 and 8 had completed treatments; the remaining clinical samples included patients with both completed and non-completed treatments. Samples 1, 2, 4, and 8 were cross-sectional studies; the remaining samples were longitudinal studies, but for these studies only the first measurement time point is considered here.
This sample was compiled from two surveys conducted in Germany. In both surveys, the samples were fairly representative of the German population living in private homes in terms of age and sex distribution. Both samples are described in more detail elsewhere (Hinz et al., 2014). The sample sizes were n = 2,448 for subsample 1 and n = 2,028 for subsample 2, resulting in a total sample of n = 4,476.
This multicenter study included 4,020 cancer patients receiving treatment in acute care hospitals, outpatient facilities, and rehabilitation clinics. The most frequent cancer localizations were: breast (22%), digestive organs (20%), and male genital organs (17%). Five study centers in Germany were involved in this project (Mehnert et al., 2014).
Sample 3 was composed of cancer patients enrolled in a rehabilitation program to regain physical fitness (n = 1,225). The most frequent cancer diagnoses were breast cancer (25%), prostate cancer (19%), and cancer of the gastrointestinal tract (18%; Friedrich et al., 2019).
Sample 4 also included cancer patients participating in a rehabilitation program (n = 2,059). The tumor sites with the highest frequency were prostate (31%), breast (17%), colon (9%), and kidney (6%). The participants of this study were sent the questionnaire 6 months after finishing the rehabilitation program (Hinz et al., 2015).
Sample 5 was composed of 323 male patients with urologic cancer (Zenger et al., 2010) and 110 female patients with gynecological cancer (Zenger et al., 2011) receiving treatment in a university hospital. In this analysis, we only use the data from the first measurement point (t1), obtained in hospital.
Patients with gynecological or breast cancer (n = 354) were consecutively recruited for this study in the gynecological clinics of three German hospitals. As in Sample 5, we only use the data from the first measurement point obtained in hospital (Thieme et al., 2017).
Sample 7 consists of 323 women who took part in a routine radiologic after-treatment (breast cancer) examination. Directly after the radiologic examination, the participants were asked to complete the questionnaires (Fuhrmann et al., 2015).
This sample included survivors of hematological malignancies (≥2.5 years after diagnosis) from two German cancer registries (Esser et al., 2017). The most frequent cancer types were non-follicular lymphoma (27%), lymphoid leukemia (15%), and follicular lymphoma (13%). While the publication describing the study methods (Esser et al., 2018) included only 922 patients, our sample was enlarged with further hematological survivors and reached a sample size of n = 1,288.
A sample of 514 AYAs (age 15–39 years at diagnosis) was included in this study. The most common tumor diagnoses were breast (27%), non-Hodgkin lymphoma (18%), gynecological tumors (9%), testicular tumor (8%), and hematological cancer (7%). Patients were recruited in 16 German acute care hospitals, four rehabilitation centers, and from two cancer registries (Leuteritz et al., 2018).
The 30 items of the EORTC QLQ-C30 (Aaronson et al., 1993) are distributed across five functioning scales, 9 symptom scales (including single symptom items and an item reflecting financial difficulties), and a 2-item global health/QoL scale. Items 1–28 have four possible response options (not at all, a little, quite a bit, very much), and the remaining two items have seven. High functioning scales, global health/QoL scale, and sum scores represent high QoL, while high scores on the symptom scales (including sleep problems) indicate low QoL. The EORTC Quality of Life Group proposed a summarizing score of higher order (sum score) which is composed of the five functioning scales and eight symptom scales (Giesinger et al., 2016).
In our analyses, we focused on the one-item sleep scale of the EORTC QLQ-C30:
“(During the past week): Have you had trouble sleeping?,” with the four response categories from “not at all” to “very much.” The raw scores are transformed linearly to a scale from 0 to 100, where a high score represents more sleep problems. The validity of this scale was underlined by the correlation between this one-item scale and the Jenkins Sleep Scale of 0.73 (Hofmeister et al., 2020) in a large sample of mixed cancer patients and between 0.74 and 0.81 in colorectal cancer survivors (Legg et al., 2022). Moreover, the association between the EORTC QLQ-C30 sleep scale and the 18-item Karolinska Sleep Questionnaire was characterized by an odds ratio of 8.2 (Lagergren et al., 2021) in a study with esophageal cancer patients. Normative values of the EORTC QLQ-C30 including the sleep scale are available for several countries (Hinz et al., 2014; Nolte et al., 2019).
Associations between the sleep scale and other scales are expressed with Pearson correlation coefficients. Pearson correlations were used because they provide the best comparability with results from the literature. For characterizing group differences, we used effect sizes d, relating the mean score differences of the groups to the pooled standard deviations. The two age groups were defined as ≤59 years vs. ≥ 60 years for all of the samples except the AYA. Because of the non-normality of the distribution of correlation coefficients, the mean correlations across the eight cancer samples were calculated via Fisher’s z-transformation of the single coefficients. For this averaging procedure, we gave each sample the same weight and did not use weighting factors according to the sample sizes because we intended to represent each setting underlying the samples with the same weight. All calculations were performed with SPSS version 27.
Table 2 presents the correlations between the sleep scale and the other scales of the EORTC QLQ-C30. Sleep quality was significantly correlated with all components of QoL in all of the samples; positive correlations were found with the symptom scales, and negative correlations with the functioning scales, the global QoL scale, and the sum score. In both types of samples, the general population and the cancer patients, the strongest associations were found for fatigue and for emotional functioning. The correlations in the general population sample were generally stronger than those in the cancer patient samples.
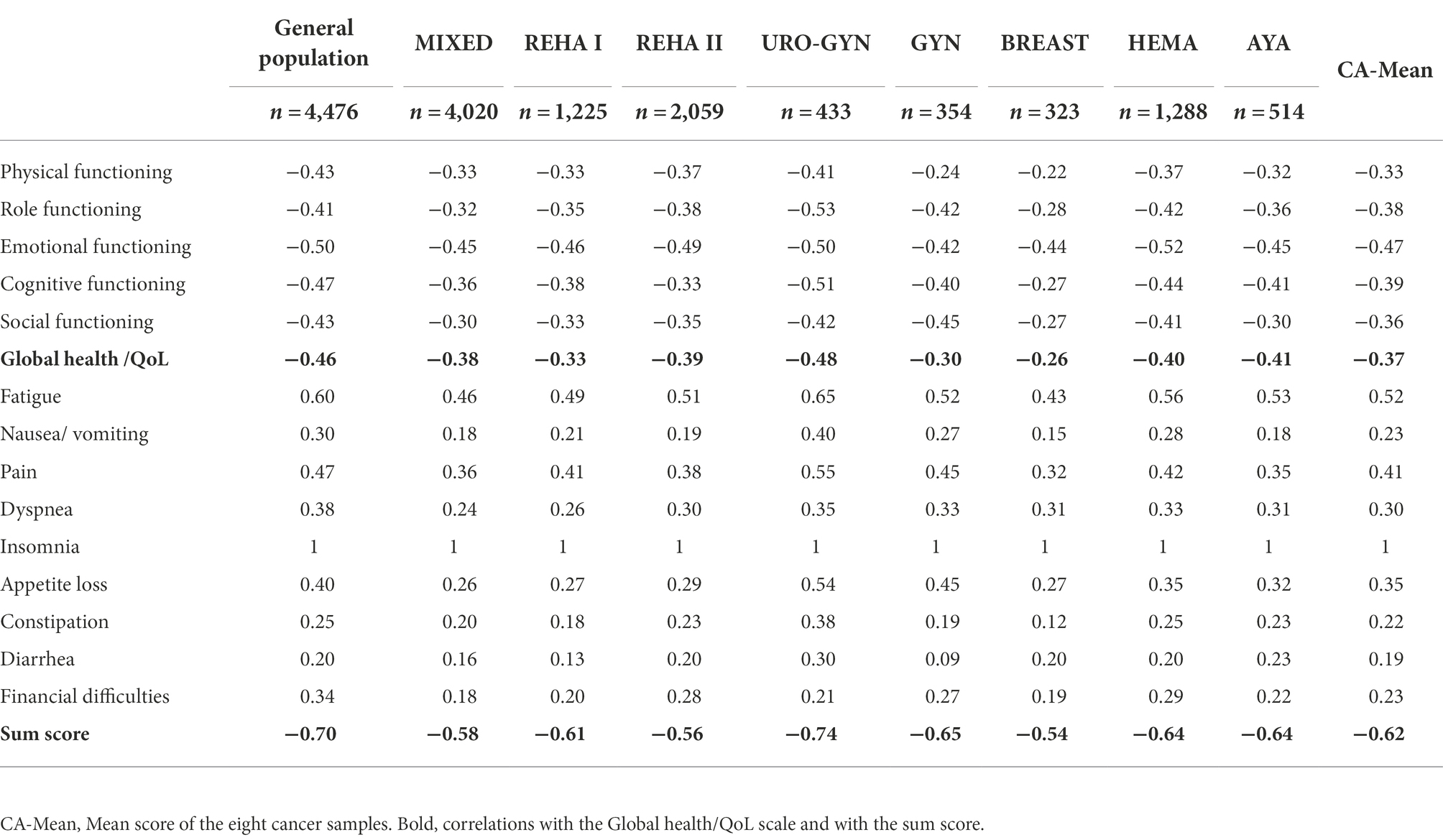
Table 2. Correlations between the sleep scale and the other scales.
Regarding the overall comparison between the clinical samples and the general population, the bottom rows of Table 3 show that sleep problems were markedly more frequent in all clinical samples (M between 32.6 and 54.7) than in the general population (M = 14.3).
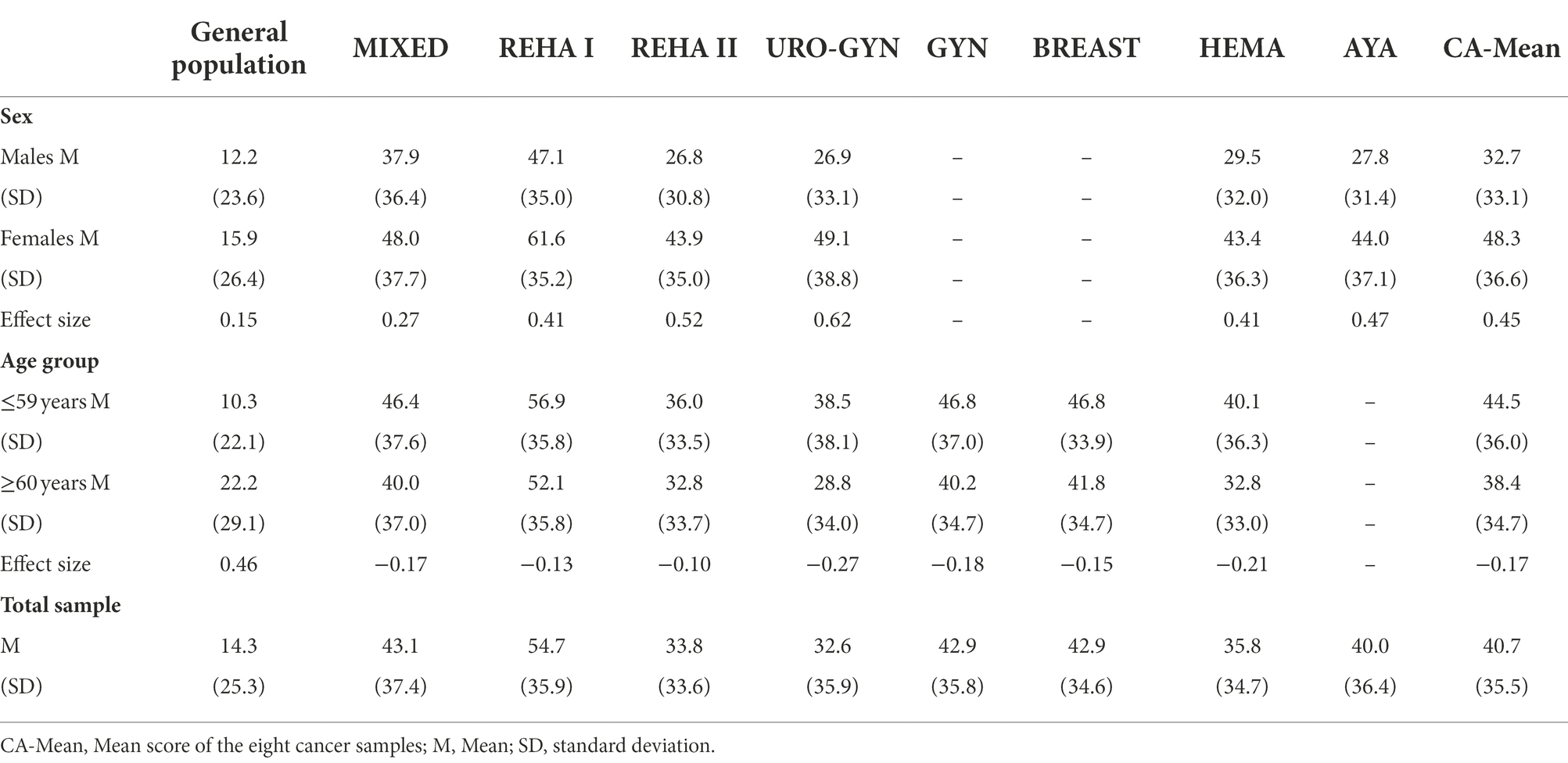
Table 3. Mean scores of the sleep scale, broken down by sex and age group.
Females reported more sleep problems than males in all samples (Table 3), and the effect sizes of this sex difference were higher in the clinical samples (d between 0.27 and 0.62) than in the general population (d = 0.15). Younger patients reported more sleep problems than older patients in all of the clinical samples, while the opposite was true of the general population sample. The GYN and BREAST samples included only women, and the AYA sample was composed entirely of young patients; therefore, the corresponding group differences could not be calculated in Table 3.
Table 4 presents the correlations between the sleep scale and the two-item global health/QoL scale, separately for males and females and for younger and older patients. All coefficients are negative, thus indicating decreasing QoL with increasing sleep problems. Correlations across the total samples are presented above in Table 2. In most of the samples, the correlations were slightly higher in the subsample of males compared those in the women’s groups, and the correlations among the younger patients were generally somewhat stronger than those among the older patients.
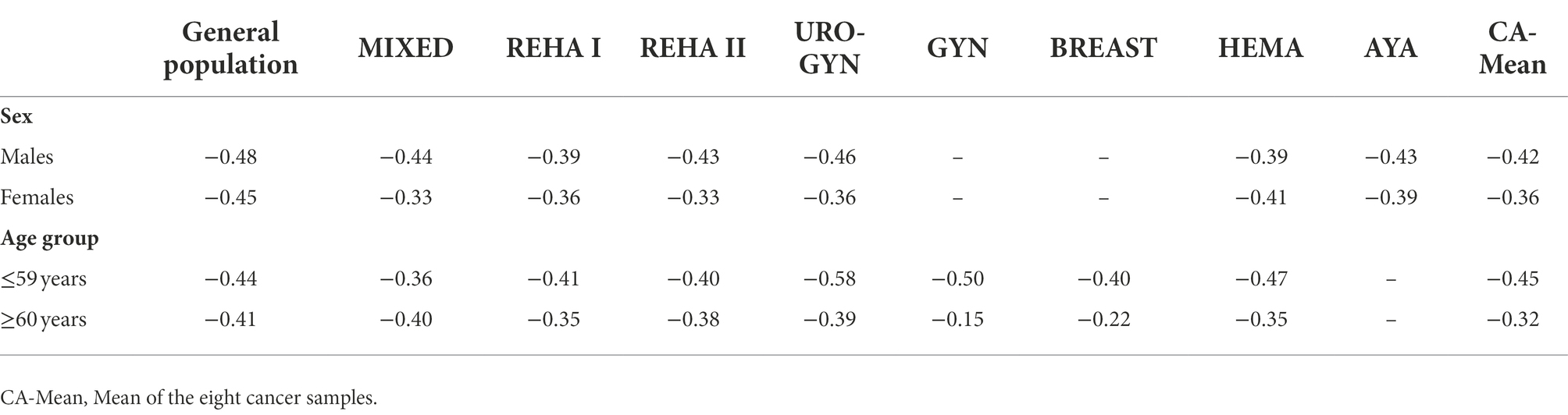
Table 4. Correlations between the sleep scale and global QoL, broken down by sex and age group.
All cancer groups reported markedly higher levels of sleep problems than the general population. This finding is not new, and confirms results often reported in the literature. The first specific research question of the present study concerned analyzing the association between sleep quality and QoL. Sleep quality was significantly correlated with all components of QoL in all samples. In both types of sample groups, the general population and the cancer patients, the highest associations were found for fatigue and emotional functioning, while the lowest associations were observed for the specific symptoms diarrhea, constipation, nausea/vomiting, and financial difficulties. It is interesting to note that the psychological QoL dimensions, emotional and cognitive functioning, are more strongly correlated with sleep problems than are the more physical components, physical functioning and role functioning. The term fatigue comprises physical as well as mental components, and fatigue proved to be the scale with the highest associations with sleep problems of all of the nine samples. In a study on disruptive factors that may explain why cancer patients experience the sleep problems they do, psychological factors such as worrying had a stronger prognostic power than objective and physical factors such as nocturnal urination or pain (Schulte et al., 2021) did, a finding that further underlines the relevance of mental factors in the prognosis of sleep problems.
A further result was that all correlations between sleep quality and QoL in the general population group were higher than the mean correlations of the cancer patients. While the correlations between sleep problems and the 2-item general health/QoL scale was r = −0.46 in the general population sample, the mean correlation of the cancer samples was only r = −0.37. This indicates that sleep problems are more relevant for the prediction of general QoL in the general population as compared with cancer patient groups. At first glance, this seems to contradict the importance of sleep problems among cancer patients. In our study, the magnitude of sleep problems was markedly higher in all cancer patient samples than in the general population. However, the lower correlations in the cancer groups actually mean that the sleep disturbances are not as strongly associated with other detriments to QoL as they are in the general population, and that they cannot be predicted very well by the other variables. In contrast to cancer patients, sleep problems experienced by members of the general population may be the only problem that person has, and thus explains why a stronger association between sleep quality and general QoL exists in that general population group. Cancer patients, on the other hand, are faced with multiple other detriments in addition to having trouble sleeping. While this fact might reduce the relative importance of sleep quality for the general QoL assessment, it does not reduce the relevance of sleep problems per se.
The highest correlations found in Table 2 are those between sleep problems and the EORTC QLQ-C30 sum score. Here it must be taken into account however that the sleep problems are already included in the sum scores, and thus lead to a slight artificial inflation of the association. Nevertheless, a comparison between the different samples is possible, and, once more, the correlation is highest in the general population.
A further aim of the study was to investigate sex and age differences in sleep problems and their associations with QoL. It is well-known that females in general population samples report higher levels of sleep problems than males do (Hinz et al., 2017a). In our study, the relevant effect size was d = 0.15, a finding that is in line with other normative studies that have also used the EORTC QLQ-C30 for measuring sleep quality. Effect sizes with coefficients of d = 0.24 (Waldmann et al., 2013) and d = 0.13 (Nolte et al., 2020) can be inferred from two further German normative studies, and a large international normative study reported an effect size of d = 0.19 (Nolte et al., 2019). Females in our cancer samples also reported more sleep problems than males did. All eight samples showed more pronounced sex differences (mean effect size: d = 0.45) than the general population sample (d = 0.15), indicating that heightened sleep disturbances in female cancer patients are not only due to their sex. The threat of a cancer diagnosis provokes more sleep problems in female cancer patients in addition to their generally poorer sleep quality, a phenomenon which may be related to higher levels of anxiety (Hinz et al., 2017b) and fear of progression (Hinz et al., 2015) in females in comparison with males.
Regarding age, the cancer patient samples reported the opposite effect of that seen in the general population sample. In the latter, older people were more prone to sleep problems than younger ones, a fact that can also be observed in other normative studies (Hinz et al., 2014), while the younger cancer patients reported more sleep problems than the older ones. This confirms that a cancer diagnosis is particularly threatening for younger patients. Other studies have also found that, compared with their healthy peers, young cancer patients are more anxious and more depressed than older patients in relation to their healthy peers (Hinz et al., 2019).
As already mentioned above, our study confirmed severe sleep problems in cancer patients and clear associations between sleep quality and general QoL. While the QoL questionnaire EORTC QLQ-C30 has an item that measures sleep quality, the SF-36 does not. Unfortunately, most instruments for measuring supportive care needs such as the SCNS-SF34 (Boyes et al., 2009) or the CaSUN (Hodgkinson et al., 2007) do not cover sleep problems at all; therefore, these unmet needs may remain undetected. Many cancer patients find it easier to admit that they are having trouble sleeping than that they are experiencing depressive symptoms. Thus, talking about sleep problems can also serve as a path for facilitating support services for regaining mental health.
The take-away of this study for health care providers is that females and younger cancer patients deserve special attention concerning their sleep quality. This message is not new, but the compilation of the studies with different cancer types and different settings confirms the generalizability of this finding. Since sleep problems can become chronic when left untreated, health care providers should consider offering their patients who suffer from sleep problems intervention techniques for improving sleep quality such as physical exercise (Yang et al., 2021), behavioral or cognitive-behavioral treatment (Zhou et al., 2020; Savard et al., 2022), or stress reduction (Suh et al., 2021).
Some limitations of this study should be mentioned. The mean scores of the sleep scale for samples 2 and 4 have already been reported in previous publications (Hinz et al., 2017c; 2018), and for some of the samples mean scores of certain subsamples (but not the whole sample) have also been reported previously. However, the results on age and sex differences as well as the correlations between sleep problems and QoL, presented separately divided by sex and age, are new. The participants of the general population sample were on average somewhat younger than the cancer patients; therefore, some of the differences between the patients and the general population might, at least in part, be due to those mean age differences. The eight cancer samples were heterogeneous concerning multiple criteria such as tumor types, time since diagnosis, recruitment procedure, and other factors. Therefore, it is not possible to attribute differences between the eight cancer samples to just one cause. However, the heterogeneity of the cancer samples can also be seen as an advantage, as it allows for estimating the degree of generalizability of the results. The one-item sleep scale of the EORTC QLQ-C30 is less reliable than sleep scales with more items. However, the difference in accuracy between this single-item scale and more comprehensive scales is not severe (Hofmeister et al., 2020; Schulte et al., 2021), and the large sample sizes can compensate for inaccuracies in the sleep scale of the EORTC QLQ-C30 to a certain degree. In our analyses, we could not consider the influence of comorbidity (e.g., Ferro et al., 2020) and of medication (e.g., Voiss et al., 2019) on the relationship between sleep quality and QoL because the corresponding data on comorbidities and medication were not available.
Taken together, the present study contributes to clarifying the magnitude and role of sleep problems in the context of QoL. It underlines that sleep problems are severe in cancer patients, and it gives oncologists and other health care providers information concerning groups with specific needs, especially females and young cancer patients.
The data analyzed in this study is subject to the following licenses/restrictions: The datasets presented in this article are not readily available due to the heterogeneity of their origins. Requests for access to the datasets should be addressed to the corresponding authors of the original studies (Zenger et al., 2010, 2011; Hinz et al., 2014, 2015; Mehnert et al., 2014; Fuhrmann et al., 2015; Thieme et al., 2017; Leuteritz et al., 2018; Friedrich et al., 2019). Requests to access these datasets should be directed to YW5kcmVhcy5oaW56QG1lZGl6aW4udW5pLWxlaXB6aWcuZGU=.
The studies involving human participants were reviewed and approved by the Ethical Review Board Leipzig University. The patients/participants provided their written informed consent to participate in this study.
AH and DH designed the study, performed the statistical analyses, wrote the first draft, and wrote the final version. TS, AM-T, KG, MZ, PE, and HG recruited patients. AH obtained data from the general population. All authors contributed to the article and approved the final version.
The original research was funded and supported by German Cancer Aid (Grant Numbers: 70112267, 107 447, 107465, and 110948) and German Research Foundation (Grant Number HI 1108/5-1). The authors acknowledge the support by the Open Access Publishing Fund of Leipzig University, supported by the German Research Foundation within the program Open Access Publication Funding.
The research team gratefully acknowledges the patients who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aaronson, N. K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull, A., Duez, N. J., et al. (1993). The European-organization-for-research-and-treatment-of-cancer QLQ-C30- a quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 85, 365–376. doi: 10.1093/jnci/85.5.365
Akman, T., Yavuzsen, T., Sevgen, Z., Ellidokuz, H., and Yilmaz, A. U. (2015). Evaluation of sleep disorders in cancer patients based on Pittsburgh sleep quality index. Eur. J. Cancer Care 24, 553–559. doi: 10.1111/ecc.12296
Ancoli-Israel, S. (2009). Recognition and treatment of sleep disturbances in cancer. J. Clin. Oncol. 27, 5864–5866. doi: 10.1200/JCO.2009.24.5993
Ancoli-Israel, S., Liu, L., Rissling, M., Natarajan, L., Neikrug, A. B., Palmer, B. W., et al. (2014). Sleep, fatigue, depression, and circadian activity rhythms in women with breast cancer before and after treatment. A 1-year longitudinal study. Support Care Cancer 22, 2535–2545. doi: 10.1007/s00520-014-2204-5
Aronsen, S., Conway, R., Lally, P., Roberts, A., Croker, H., Beeken, R. J., et al. (2022). Determinants of sleep quality in 5835 individuals living with and beyond breast, prostate, and colorectal cancer: a cross-sectional survey. J. Cancer Surviv. 16, 1489–1501. doi: 10.1007/s11764-021-01127-2
Bach, L., Kalder, M., and Kostev, K. (2021). Depression and sleep disorders are associated with early mortality in women with breast cancer in the United Kingdom. J. Psychiat. Res. 143, 481–484. doi: 10.1016/j.jpsychires.2020.11.036
Boyes, A., Girgis, A., and Lecathelinais, C. (2009). Brief assessment of adult cancer patients’ perceived needs: development and validation of the 34-item supportive care needs survey (SCNS-SF34). J. Eval. Clin. Pract. 15, 602–606. doi: 10.1111/j.1365-2753.2008.01057.x
Chartogne, M., Rahmani, A., Landry, S., Bourgeois, H., Peyrot, N., and Morel, B. (2021). Neuromuscular, psychological, and sleep predictors of cancer-related fatigue in cancer patients. Clin. Breast Cancer 21, 425–432. doi: 10.1016/j.clbc.2020.12.002
Delgado-Guay, M., Yennurajalingam, S., Parsons, H., Palmer, J. L., and Bruera, E. (2011). Association between self-reported sleep disturbance and other symptoms in patients with advanced cancer. J. Pain Symptom Manag. 41, 819–827. doi: 10.1016/j.jpainsymman.2010.07.015
Esser, P., Kuba, K., Götze, H., and Mehnert, A. (2017). Long-term effects and psychological adjustment: study protocol of a large register-based study on quality of life among survivors of hematological malignancies. BMC Cancer 17:482. doi: 10.1186/s12885-017-3454-7
Esser, P., Kuba, K., Mehnert, A., Johansen, C., Hinz, A., Lordick, F., et al. (2018). Quality of life in survivors of hematological malignancies stratified by cancer type, time since diagnosis and stem cell transplantation. Eur. J. Haematol. 101, 340–348. doi: 10.1111/ejh.13104
Ferro, M., Katalin, M. O., Buonerba, C., Marian, R., Cantiello, F., Musi, G., et al. (2020). Type 2 diabetes mellitus predicts worse outcomes in patients with high-grade T1 bladder cancer receiving bacillus Calmette-Guérin after transurethral resection of the bladder tumor. Urol. Oncol. 38, 459–464. doi: 10.1016/j.urolonc.2020.02.016
Friedrich, M., Hinz, A., Kuhnt, S., Schulte, T., Rose, M., and Fischer, F. (2019). Measuring fatigue in cancer patients. A common metric for six fatigue instruments. Qual. Life Res. 28, 1615–1626. doi: 10.1007/s11136-019-02147-3
Fuhrmann, K., Mehnert, A., Geue, K., and Hinz, A. (2015). Fatigue in breast cancer patients: psychometric evaluation of the fatigue questionnaire EORTC QLQ-FA13. Breast Cancer 22, 608–614. doi: 10.1007/s12282-014-0527-1
Giesinger, J. M., Kieffer, J. M., Fayers, P. M., Groenvold, M., Petersen, M. A., Scott, N. W., et al. (2016). Replication and validation of higher order models demonstrated that a summary score for the EORTC QLQ-C30 is robust. J. Clin. Epidemiol. 69, 79–88. doi: 10.1016/j.jclinepi.2015.08.007
Gottfried, T., Kamer, I., Salant, I., Urban, D., Lawrence, Y. R., Onn, A., et al. (2020). Self-reported sleep quality as prognostic for survival in lung cancer patients. Cancer Manage. Res. 12, 313–321. doi: 10.2147/CMAR.S234523
Henneghan, A. M., Carter, P., Stuifbergan, A., Parmelee, B., and Kesler, S. (2018). Relationships between self-reported sleep quality components and cognitive functioning in breast cancer survivors up to 10 years following chemotherapy. Psycho Oncol. 27, 1937–1943. doi: 10.1002/pon.4745
Hinz, A., Glaesmer, H., Brähler, E., Löffler, M., Engel, C., Enzenbach, C., et al. (2017a). Sleep quality in the general population: psychometric properties of the Pittsburgh sleep quality index, derived from a German community sample of 9284 people. Sleep Med. 30, 57–63. doi: 10.1016/j.sleep.2016.03.008
Hinz, A., Herzberg, P. Y., Lordick, F., Weis, J., Faller, H., Brähler, E., et al. (2019). Age and gender differences in anxiety and depression in cancer patients compared with the general population. Eur. J. Cancer Care 28:e13129. doi: 10.1111/ecc.13129
Hinz, A., Klein, A. M., Brähler, E., Glaesmer, H., Luck, T., Riedel-Heller,, et al. (2017b). Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. J. Affect. Disord. 210, 338–344. doi: 10.1016/j.jad.2016.12.012
Hinz, A., Mehnert, A., Dégi, C., Reissmann, D. R., Schotte, D., and Schulte, T. (2017c). The relationship between global and specific components of quality of life, assessed with the EORTC QLQ-C30 in a sample of 2019 cancer patients. Eur. J. Cancer Care 26:e12416. doi: 10.1111/ecc.12416
Hinz, A., Mehnert, A., Ernst, J., Herschbach, P., and Schulte, T. (2015). Fear of progression in patients 6 months after cancer rehabilitation a validation study of the fear of progression questionnaire FoP-Q-12. Support Care Cancer 23, 1579–1587. doi: 10.1007/s00520-014-2516-5
Hinz, A., Singer, S., and Brähler, E. (2014). European reference values for the quality of life questionnaire EORTC QLQ-C30: results of a German investigation and a summarizing analysis of six European general population normative studies. Acta Oncol. 53, 958–965. doi: 10.3109/0284186X.2013.879998
Hinz, A., Weis, J., Faller, H., Brähler, E., Härter, M., Keller, M., et al. (2018). Quality of life in cancer patients-a comparison of inpatient, outpatient, and rehabilitation settings. Support. Care Cancer 26, 3533–3541. doi: 10.1007/s00520-018-4211-4
Hodgkinson, K., Butow, P., Hunt, G. E., Pendlebury, S., Hobbs, K. M., Lo, S. K., et al. (2007). The development and evaluation of a measure to assess cancer survivors’ unmet supportive care needs: the CaSUN (cancer survivors’ unmet needs measure). Psycho Oncol. 16, 796–804. doi: 10.1002/pon.1137
Hofmeister, D., Schulte, T., and Hinz, A. (2020). Sleep problems in cancer patients: a comparison between the Jenkins sleep scale and the single-item sleep scale of the EORTC QLQ-C30. Sleep Med. 71, 59–65. doi: 10.1016/j.sleep.2019.12.033
Kudielka, B. M., Känel, R. V., Gander, M.-L., and Fischer, J. E. (2004). Effort-reward imbalance, overcommitment and sleep in a working population. Work Stress 18, 167–178. doi: 10.1080/02678370410001731785
Kwak, A., Jacobs, J., Haggett, D., Jimenez, R., and Peppercorn, J. (2020). Evaluation and management of insomnia in women with breast cancer. Breast Cancer Res. Treat. 181, 269–277. doi: 10.1007/s10549-020-05635-0
Lagergren, P., Johar, A., Rosenlund, H., Arnberg, L., Haglund, L., Ness-Jensen, E., et al. (2021). Severe reflux, sleep disturbances, and health-related quality of life after esophageal cancer surgery. J. Cancer Surviv. 15, 818–824. doi: 10.1007/s11764-020-00974-9
Legg, M., Meertens, R. M., van Roekel, E., Breukink, S. O., Janssen, M. L., Keulen, E. T. P., et al. (2022). The association between sleep quality and fatigue in colorectal cancer survivors up until two years after treatment: a cross-sectional and longitudinal analysis. Cancers 14. doi: 10.3390/cancers14061527
Leuteritz, K., Friedrich, M., Sender, A., Nowe, E., Stoebel-Richter, Y., and Geue, K. (2018). Life satisfaction in young adults with cancer and the role of sociodemographic, medical, and psychosocial factors: Results of a longitudinal study. Cancer 124, 4374–4382. doi: 10.1002/cncr.31659
Lin, C.-Y., Cheng, A. S. K., Nejati, B., Imani, V., Ulander, M., Browall, M., et al. (2020). A thorough psychometric comparison between Athens insomnia scale and insomnia severity index among patients with advanced cancer. J. Sleep Res. 29:e12891. doi: 10.1111/jsr.12891
Medysky, M. E., Temesi, J., Culos-Reed, S. N., and Millet, G. Y. (2017). Exercise, sleep and cancer-related fatigue. Are they related? Neurophysiol. Clin. 47, 111–122. doi: 10.1016/j.neucli.2017.03.001
Mehnert, A., Brähler, E., Faller, H., Härter, M., Keller, M., Schulz, H., et al. (2014). Four-week prevalence of mental disorders in patients with cancer across major tumor entities. J. Clin. Oncol. 32, 3540–3546. doi: 10.1200/JCO.2014.56.0086
Nock, N. L., Dimitropoulos, A., Zanotti, K. M., Waggoner, S., Nagel, C., Golubic, M., et al. (2020). Sleep, quality of life, and depression in endometrial cancer survivors with obesity seeking weight loss. Support Care Cancer 28, 2311–2319. doi: 10.1007/s00520-019-05051-1
Nolte, S., Liegl, G., Petersen, M. A., Aaronson, N. K., Costantini, A., Fayers, P. M., et al. (2019). General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15, 386 persons across 13 European countries, Canada and the unites states. Eur. J. Cancer 107, 153–163. doi: 10.1016/j.ejca.2018.11.024
Nolte, S., Waldmann, A., Liegl, G., Petersen, M. A., Groenvold, M., and Rose, M. (2020). Updated EORTC QLQ-C30 general population norm data for Germany. Eur. J. Cancer 137, 161–170. doi: 10.1016/j.ejca.2020.06.002
Otte, J. L., Carpenter, J. S., Manchanda, S., Rand, K. L., Skaar, T. C., Weaver, M., et al. (2015). Systematic review of sleep disorders in cancer patients. Can the prevalence of sleep disorders be ascertained? Cancer Med. 4, 183–200. doi: 10.1002/cam4.356
Pozzar, R. A., Hammer, M. J., Paul, S. M., Cooper, B. A., Kober, K. M., Conley, Y. P., et al. (2021). Distinct sleep disturbance profiles among patients with gynecologic cancer receiving chemotherapy. Gynecol. Oncol. 163, 419–426. doi: 10.1016/j.ygyno.2021.09.002
Sandadi, S., Frasure, H. E., Broderick, M. J., Waggoner, S. E., Miller, J. A., Gruenigen, V. E., et al. (2011). The effect of sleep disturbance on quality of life in women with ovarian cancer. Gynecol. Oncol. 123, 351–355. doi: 10.1016/j.ygyno.2011.07.028
Santoso, A. M. M., Jansen, F., Lissenberg-Witte, B. I., Baatenburg de Jong, R. J., Langendijk, J. A., Leemans, C. R., et al. (2021). Poor sleep quality among newly diagnosed head and neck cancer patients. Prevalence and associated factors. Support Care Cancer 29, 1035–1045. doi: 10.1007/s00520-020-05577-9
Savard, J., Filion, C., Gagnon, M.-P., Caplette-Gingras, A., Bélanger, L., and Morin, C. M. (2022). Barriers and facilitators to implementing a stepped care cognitive-behavioral therapy for insomnia in cancer patients: a qualitative study. Care Cancer 30, 6689–6698. doi: 10.1007/s00520-022-07094-3
Schieber, K., Niecke, A., Geiser, F., Erim, Y., Bergelt, C., Büttner-Teleaga, A., et al. (2019). The course of cancer-related insomnia: don’t expect it to disappear after cancer treatment. Sleep Med. 58, 107–113. doi: 10.1016/j.sleep.2019.02.018
Schulte, T., Hofmeister, D., Mehnert-Theuerkauf, A., Hartung, T., and Hinz, A. (2021). Assessment of sleep problems with the insomnia severity index (ISI) and the sleep item of the patient health questionnaire (PHQ-9) in cancer patients. Support Care Cancer 29, 7377–7384. doi: 10.1007/s00520-021-06282-x
Strik, H., Cassel, W., Teepker, M., Schulte, T., Riera-Knorrenschild, J., Koehler, U., et al. (2021). Why do our cancer patients sleep so badly? Sleep disorders in cancer patients: a frequent symptom with multiple causes. Oncol. Res. Treat. 44, 469–475. doi: 10.1159/000518108
Suh, H.-W., Jeong, H. Y., Hong, S., Kim, J. W., Yoon, S. W., Lee, J. Y., et al. (2021). The mindfulness-based stress reduction program for improving sleep quality in cancer survivors: a systematic review and meta-analysis. Complement. Ther. Med. 57:102667. doi: 10.1016/j.ctim.2021.102667
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., et al. (2021). Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA-Cancer J. Clin. 71, 209–249. doi: 10.3322/caac.21660
Thieme, M., Einenkel, J., Zenger, M., and Hinz, A. (2017). Optimism, pessimism and self-efficacy in female cancer patients. Jpn. J. Clin. Oncol. 47, 849–855. doi: 10.1093/jjco/hyx079
Tibubos, A. N., Zenger, M., Schmalbach, B., Beutel, M. E., and Brähler, E. (2020). Measurement invariance, validation and normative data of the Jenkins sleep Scale-4 (JSS-4) in the German general population across the life span. J. Psychosom. Res. 130:109933. doi: 10.1016/j.jpsychores.2020.109933
Voiss, P., Höxtermann, M. D., Dobos, G., and Cramer, H. (2019). Cancer, sleep problems, and mind-body medicine use: results of the 2017 National Health Interview Survey. Cancer 125, 4490–4497. doi: 10.1002/cncr.32469
Waldmann, A., Schubert, D., and Katalinic, A. (2013). Normative data of the EORTC QLQ-C30 for the German population: a population-based survey. PLoS One 8:e74149. doi: 10.1371/journal.pone.0074149
Yang, H., Yang, Z., Pan, H., and Zhou, Q. (2021). Effects of physical activity on sleep problems in breast cancer survivors: a meta-analysis. Support Care Cancer 29, 4023–4032. doi: 10.1007/s00520-020-05914-y
Zenger, M., Brix, C., Borowski, J., Stolzenburg, J., and Hinz, A. (2010). The impact of optimism on anxiety, depression and quality of life in urogenital cancer patients. Psycho Oncol. 19, 879–886. doi: 10.1002/pon.1635
Zenger, M., Glaesmer, H., Höckel, M., and Hinz, A. (2011). Pessimism predicts anxiety, depression and quality of life in female cancer patients. Jpn. J. Clin. Oncol. 41, 87–94. doi: 10.1093/jjco/hyq168
Keywords: cancer, insomnia, sleep loss, quality of life, age differences, sex differences
Citation: Hofmeister D, Schulte T, Mehnert-Theuerkauf A, Geue K, Zenger M, Esser P, Götze H and Hinz A (2022) The association between sleep problems and general quality of life in cancer patients and in the general population. Front. Psychol. 13:960029. doi: 10.3389/fpsyg.2022.960029
Edited by:
Eun-Jung Shim, Pusan National University, Republic of KoreaReviewed by:
Lauren Daniel, Rutgers University Camden, United StatesCopyright © 2022 Hofmeister, Schulte, Mehnert-Theuerkauf, Geue, Zenger, Esser, Götze and Hinz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreas Hinz, YW5kcmVhcy5oaW56QG1lZGl6aW4udW5pLWxlaXB6aWcuZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.